Informating Health Care: EHRs, PHRs, and Diffusion Ritu Agarwal Professor and Robert H. Smith...
40
Informating Health Informating Health Care: EHRs, PHRs, and Care: EHRs, PHRs, and Diffusion Diffusion Ritu Agarwal Ritu Agarwal Professor and Robert H. Smith Dean’s Chair of Professor and Robert H. Smith Dean’s Chair of Information Systems Information Systems Director, Center for Health Information and Director, Center for Health Information and Decision Systems (CHIDS) Decision Systems (CHIDS) Corey Angst, Doctoral Candidate Corey Angst, Doctoral Candidate Associate Director, (CHIDS) Associate Director, (CHIDS) University of Maryland University of Maryland July 20, 2005 July 20, 2005
-
date post
20-Dec-2015 -
Category
Documents
-
view
213 -
download
0
Transcript of Informating Health Care: EHRs, PHRs, and Diffusion Ritu Agarwal Professor and Robert H. Smith...

Informating Health Care: Informating Health Care: EHRs, PHRs, and Diffusion EHRs, PHRs, and Diffusion
Ritu AgarwalRitu Agarwal
Professor and Robert H. Smith Dean’s Chair of Information SystemsProfessor and Robert H. Smith Dean’s Chair of Information SystemsDirector, Center for Health Information and Decision Systems Director, Center for Health Information and Decision Systems
(CHIDS)(CHIDS)
Corey Angst, Doctoral CandidateCorey Angst, Doctoral CandidateAssociate Director, (CHIDS)Associate Director, (CHIDS)
University of MarylandUniversity of MarylandJuly 20, 2005July 20, 2005

22© Professor R. Agarwal 2005© Professor R. Agarwal 2005
AgendaAgenda
The dilemma in health careThe dilemma in health careOpportunities afforded by ITOpportunities afforded by ITField studies of PHRsField studies of PHRs RespondentsRespondents Usage patternsUsage patterns Perceived valuePerceived value Drivers and outcomesDrivers and outcomes Delivery of PHRs for Maximum UtilityDelivery of PHRs for Maximum Utility
Facility level studiesFacility level studies

33© Professor R. Agarwal 2005© Professor R. Agarwal 2005
IT and HealthcareIT and Healthcare
Information intensive industries use IT Information intensive industries use IT extensivelyextensively Operational efficiencyOperational efficiency Strategic valueStrategic value
Yet, health care lags in realizing the Yet, health care lags in realizing the transformational potentialtransformational potential 15% of GDP15% of GDP Computerized records could save 600,000 lives, Computerized records could save 600,000 lives,
prevent 500,000 medical errors, and save $9.7 B prevent 500,000 medical errors, and save $9.7 B annually annually (Leapfrog Group 2004)(Leapfrog Group 2004)

44© Professor R. Agarwal 2005© Professor R. Agarwal 2005
IS Research in HealthcareIS Research in Healthcare
Technology use in healthcare is a fruitful Technology use in healthcare is a fruitful area of research area of research
Health systemsHealth systems Health insurance providersHealth insurance providers EmployersEmployers Individuals/PatientsIndividuals/Patients
Interesting areas for inquiry Interesting areas for inquiry IT adoption at various levels of analysisIT adoption at various levels of analysis Healthcare quality, cost, and efficiencyHealthcare quality, cost, and efficiency Value of ITValue of IT

55© Professor R. Agarwal 2005© Professor R. Agarwal 2005
Phenomenon of InterestPhenomenon of Interest
Why study PHRs?Why study PHRs? The National Committee on Vital and The National Committee on Vital and
Health Statistics and the Institute of Health Statistics and the Institute of Medicine have identified the “personal Medicine have identified the “personal health record” as a key dimension of a health record” as a key dimension of a national health information infrastructurenational health information infrastructure
Adoption of PHRs key to on-going Adoption of PHRs key to on-going diffusion of electronic health recordsdiffusion of electronic health records

66© Professor R. Agarwal 2005© Professor R. Agarwal 2005
The TechnologyThe TechnologyIn its purest form – it is a health record for an In its purest form – it is a health record for an individual – a personal health recordindividual – a personal health recordA tool for patients to self-manage their health. A tool for patients to self-manage their health. Ability to aggregate medical information.Ability to aggregate medical information.At a minimum, allows patients to see a copy of their At a minimum, allows patients to see a copy of their provider-based informationprovider-based informationPatient-centric form of the electronic medical Patient-centric form of the electronic medical record…the PHR itself is only a data set, and record…the PHR itself is only a data set, and perhaps a tool to see the dataperhaps a tool to see the dataCan be delivered by various means – e.g. an Can be delivered by various means – e.g. an individual’s PC, on the Internet (ASP), or a hybridindividual’s PC, on the Internet (ASP), or a hybrid

77© Professor R. Agarwal 2005© Professor R. Agarwal 2005
Some Issues with PHRsSome Issues with PHRs
The average American Internet users:The average American Internet users:Do not want their health information shared with anyone Do not want their health information shared with anyone else without their consentelse without their consent
Have a high level of concern about someone hacking Have a high level of concern about someone hacking into the site and gaining access to their informationinto the site and gaining access to their information
Have a high level of concern about access to personal Have a high level of concern about access to personal health information by insurers and employers who might health information by insurers and employers who might use the information against themuse the information against them
Online medical record keeping, even though a desired Online medical record keeping, even though a desired feature, is perceived as the greatest threat to individual feature, is perceived as the greatest threat to individual privacy on the Internetprivacy on the Internet
Ethics Survey of Consumer Attitudes about Health Web Sites (Grimes-Gruczka & Gratzer, 2000),

88© Professor R. Agarwal 2005© Professor R. Agarwal 2005
Goal of this ResearchGoal of this Research
Accelerate adoption of PHRsAccelerate adoption of PHRs
Understand barriers and facilitatorsUnderstand barriers and facilitators What value do patients perceive in a PHR?What value do patients perceive in a PHR? What do they use it for? How much do they What do they use it for? How much do they
use?use? What drives people to use PHRs?What drives people to use PHRs?
Behavioral characteristics?Behavioral characteristics?
Demographic characteristics?Demographic characteristics?

99© Professor R. Agarwal 2005© Professor R. Agarwal 2005
MethodologyMethodologyConduct preliminary studyConduct preliminary study Task characteristics: Interview users of healthcare Task characteristics: Interview users of healthcare
servicesservices Technology characteristics: Interview PHR developerTechnology characteristics: Interview PHR developer
Survey approximately 875 users of a PC-based Survey approximately 875 users of a PC-based PHR PHR ValueValue DemographicDemographic Tasks Technology featuresTasks Technology features UsageUsage Usefulness, Ease of Use, Intention for Future UseUsefulness, Ease of Use, Intention for Future Use

1010© Professor R. Agarwal 2005© Professor R. Agarwal 2005
Descriptive StatisticsDescriptive Statistics
Non-response bias1 test yielded no significant differences between several key indicators.
1Time trend extrapolation method by Armstrong and Overton (1977)
Description Value Surveys sent 875
Unusable or undeliverable 52 Usable surveys 199 Response Rate 24.2% Male/Female 69/31%
% of users with chronic illness 60% % taking multiple medications daily 76.8% Average number of visits to doctor per year 7.2
Average number of doctors seen per year 5-10

1111© Professor R. Agarwal 2005© Professor R. Agarwal 2005
The RespondentsThe RespondentsAge Distribution of PHR Users
0
10
20
30
40
50
60
<20
21-3
0
31-4
0
41-5
0
51-6
0
61-7
0
71-8
0
81 +
Age
Fre
qu
ency
Income Distribution of PHR Users
05
101520253035
<$2
0k
$20-
$29k
$30-
$49k
$50-
$69k
$70-
$89k
$90-
$109
k
$110
-12
9k
$130
-14
9k
$150
-17
4k
$175
k +
Household Income
Fre
qu
en
cy
Education Level of PHR Users
0
20
40
60
80
100
Fre
qu
en
cy
Breakdown of Users by Chronic Illness
Asthma8.2% Cancer
8.8%
Diabetes14.6%
Hypertension30.4%
Congestive Heart Failure
4.1%
HIV/AIDS0.6%
Unnamed33.3%

1212© Professor R. Agarwal 2005© Professor R. Agarwal 2005
Usage PatternsUsage PatternsHow Often Respondents Use PHR
0
10
20
30
40
50
60
70
A few timesa year
Monthly A few timesa month
Weekly A few timesa w eek
Daily
Fre
qu
en
cy
How Long Respondents Use PHR per Session
0
10
20
30
40
50
60
70
1-4
min
5-9
min
10-1
9 m
in
20-2
9 m
in
30-4
4 m
in
45-5
9 m
in
60+
min
Fre
qu
en
cy
Frequency of use
Duration of use

1313© Professor R. Agarwal 2005© Professor R. Agarwal 2005
Who Uses the PHR?Who Uses the PHR?
The typical user isThe typical user is Male Age 51-60 Has a chronic illness (hypertension most prevalent) Takes multiple medications daily Goes to the doctor 7.2 times annually Completed graduate studies Household income is $175k+ (2nd highest $70-89k) Typical usage – “Monthly for 30-44 min” or “A few
times/week for 5-9 min”

1414© Professor R. Agarwal 2005© Professor R. Agarwal 2005
Descriptive StatisticsDescriptive StatisticsMost Important Health Care Tasks
Store Tests, Evaluations.
6.1%
Track Vitals / Self-Monitor
5.2%
Manage Info/Knowledge
8.8%
Access to doctor reports
and lab 4.1%
Ability to organize data in useful way
18.6%
Medical History Archive
21.6%
Medication Tracking 10.9%
Track / Trend Lab Results
4.1%
Other20.7%
Primary Uses for PHR
Track Medications
18.7%
Track Lab Results14.1%Other
5.9%
Family Medical History26.4%
Track/Trend my health
13.5%
Track Doctor Visits21.4%
Tasks
Technologies

1515© Professor R. Agarwal 2005© Professor R. Agarwal 2005
Perceived ValuePerceived Value
1.1. Structure, organization, and compliance Structure, organization, and compliance
2.2. Relationship and connectedness with Relationship and connectedness with healthcare provider healthcare provider
3.3. Convenience and empowermentConvenience and empowerment
Using principal components analysis, the 18 items that make up perceived value were reclassified into three latent constructs:
Note: Six items were removed due to poor loadings

1616© Professor R. Agarwal 2005© Professor R. Agarwal 2005
Structure, Organization and Structure, Organization and ComplianceCompliance
Using the PHR helps me to perform my healthcare Using the PHR helps me to perform my healthcare activities (by reminding me to make and keep my activities (by reminding me to make and keep my appointments, etc.)appointments, etc.) Using the PHR helps me to stay on schedule with my Using the PHR helps me to stay on schedule with my healthcare activities (such as getting my regular healthcare activities (such as getting my regular checkup)checkup) Using the PHR helps me perform my healthcare Using the PHR helps me perform my healthcare activities at the appropriate times (such as refilling activities at the appropriate times (such as refilling prescriptions)prescriptions)Using the PHR helps me remember to perform my Using the PHR helps me remember to perform my healthcare activities (like testing my blood sugarhealthcare activities (like testing my blood sugarUsing the PHR allows me to accomplish more of my Using the PHR allows me to accomplish more of my healthcare objectives (such as losing weight)healthcare objectives (such as losing weight)

1717© Professor R. Agarwal 2005© Professor R. Agarwal 2005
Relationship & ConnectednessRelationship & Connectedness
Using the PHR improves communications between my Using the PHR improves communications between my care providers and mecare providers and me
Using the PHR improves my relationship with my care Using the PHR improves my relationship with my care providersproviders
Reducing the number of forms to fill-out during Reducing the number of forms to fill-out during registration by having the information available on my registration by having the information available on my PHR is valuable to mePHR is valuable to me

1818© Professor R. Agarwal 2005© Professor R. Agarwal 2005
Convenience & EmpowermentConvenience & Empowerment
It would be valuable to have my health information It would be valuable to have my health information available at all timesavailable at all timesIt would be valuable to have my complete medical record It would be valuable to have my complete medical record with me at all timeswith me at all timesIt is critical to have my emergency medical information It is critical to have my emergency medical information with me at all timeswith me at all timesIt would be valuable to have all of my healthcare It would be valuable to have all of my healthcare information located in one place information located in one place

1919© Professor R. Agarwal 2005© Professor R. Agarwal 2005
Drivers and OutcomesDrivers and Outcomes
Perceived Value of Using PHR
Behavioral Intentions to Use PHR
Demographics Age Income Education
Medical condition Chronic illness Multiple medications Number of doctor visits

2020© Professor R. Agarwal 2005© Professor R. Agarwal 2005
Perceived Value
ResultsResultsAge
Education
Chronic illness
Income
Multiple Medications
No. of Doctor Visits
Structure, Organization,and Compliance
Relationship andConnectedness
Convenience andEmpowerment
BehavioralIntentions to Use
(-)
(-)(-)
(+)(-)
(+)
(+)
(+)
(+)

2121© Professor R. Agarwal 2005© Professor R. Agarwal 2005
Overall FindingsOverall Findings
Patients believe that PHRs deliver multi-Patients believe that PHRs deliver multi-faceted valuefaceted value
Perceived value is a strong driver of usage Perceived value is a strong driver of usage intentionsintentions Strategies to amplify perceived valueStrategies to amplify perceived value
Value perceptions differ across patient Value perceptions differ across patient populationspopulations Target “opinion leaders” and championsTarget “opinion leaders” and champions

2222© Professor R. Agarwal 2005© Professor R. Agarwal 2005
More on PHRsMore on PHRs
Second field study related to privacy Second field study related to privacy concernsconcerns What messages alleviate concerns?What messages alleviate concerns?
Other findingsOther findings Desired features and capabilitiesDesired features and capabilities Adoption barriersAdoption barriers Influences on choicesInfluences on choices

2323© Professor R. Agarwal 2005© Professor R. Agarwal 2005
What Patients DesireWhat Patients Desire
What Features of PHR are Most Important?
Track/Trend Lab Results and Vitals
Record Medications and Immunizations
Record my Personal and Family Medical History
Assurance that my Medical Information is Safe and
Secure
Ability to Receive Electronic Data from Doctors/Hospitals
Having My Emergency Health Information Immediately Accessible
0 10 20 30 40 50 60 70 80
% R
esp
ondin
g

2424© Professor R. Agarwal 2005© Professor R. Agarwal 2005
Adoption BarriersAdoption Barriers
0
10
20
30
40
50
60
70
80
% Responding
Concerns that Keep Me From Using/Endorsing PHRs
Concerns about Privacy
Cost
Time Associated with Use
Computer or Internet Access
Accuracy of Information
I Have no Concerns

2525© Professor R. Agarwal 2005© Professor R. Agarwal 2005
Influence on ChoicesInfluence on Choices
Does IT Adoption by Doctors/Hospitals Influence Your Choice?
Yes, definitely, 8Yes, probably, 10
It might, 30
No, but it should, 20
No, probably not, 24
No, definitely not, 9

2626© Professor R. Agarwal 2005© Professor R. Agarwal 2005
ObservationsObservations
Record keeping functions are crucialRecord keeping functions are crucial
Digitization is not a key component of the Digitization is not a key component of the “mental model”“mental model”
Privacy and cost concerns dominatePrivacy and cost concerns dominate Giving the technology away?Giving the technology away?

2727© Professor R. Agarwal 2005© Professor R. Agarwal 2005
33rdrd PHR Study – Delivering PHRs PHR Study – Delivering PHRs
Research Questions:Research Questions: Does it matter who provides/sponsors the Does it matter who provides/sponsors the
PHR?PHR? Does the type of PHR chosen change Does the type of PHR chosen change
depending on the provider?depending on the provider?

2828© Professor R. Agarwal 2005© Professor R. Agarwal 2005
33rdrd Study - Defining the PHR Study - Defining the PHR Paper EntryPaper Entry. You enter, update, and manage your health . You enter, update, and manage your health information on paper and store it in binders, folders, or filing information on paper and store it in binders, folders, or filing cabinets. cabinets. **Primitive PHR****Primitive PHR**
PC-based softwarePC-based software. The software is installed on your home . The software is installed on your home computer and you enter, update, and manage your health computer and you enter, update, and manage your health information. information. **Detached PHR****Detached PHR**
USB Drive (Device-based)USB Drive (Device-based). Software is installed on the USB Drive . Software is installed on the USB Drive and you manage your health information, however, you can and you manage your health information, however, you can transport your entire record on the Key. Participating providers will transport your entire record on the Key. Participating providers will accept the Drive and populate it through the USB port. accept the Drive and populate it through the USB port. **Chauffeured PHR****Chauffeured PHR**
Internet PortalInternet Portal. The software resides on the Internet and you . The software resides on the Internet and you access it using a username and password from any computer with access it using a username and password from any computer with Internet access. Participating providers can populate your record Internet access. Participating providers can populate your record and you can grant access to others. and you can grant access to others. **Tethered PHR****Tethered PHR**
Hybrid - Internet Portal with USB DriveHybrid - Internet Portal with USB Drive. The software resides on the . The software resides on the Internet and you access it using a username and password from any Internet and you access it using a username and password from any computer with Internet access. You can also store all of your computer with Internet access. You can also store all of your information on the USB Drive so it is with you at all times. information on the USB Drive so it is with you at all times. Participating providers populate your record through the USB port, Participating providers populate your record through the USB port, and/or you can link to the Internet to send and receive information. and/or you can link to the Internet to send and receive information. **Ubiquitous PHR****Ubiquitous PHR**

2929© Professor R. Agarwal 2005© Professor R. Agarwal 2005
33rdrd PHR Study - Methodology PHR Study - Methodology
Conducted in Fall 2004Conducted in Fall 2004
Over 350 respondents Over 350 respondents
Sample included a general population of Sample included a general population of health care consumers and approximately health care consumers and approximately 100 individuals who identified themselves 100 individuals who identified themselves as being stakeholders in the adoption as being stakeholders in the adoption electronic health recordselectronic health records
3030© Professor R. Agarwal 2005© Professor R. Agarwal 2005
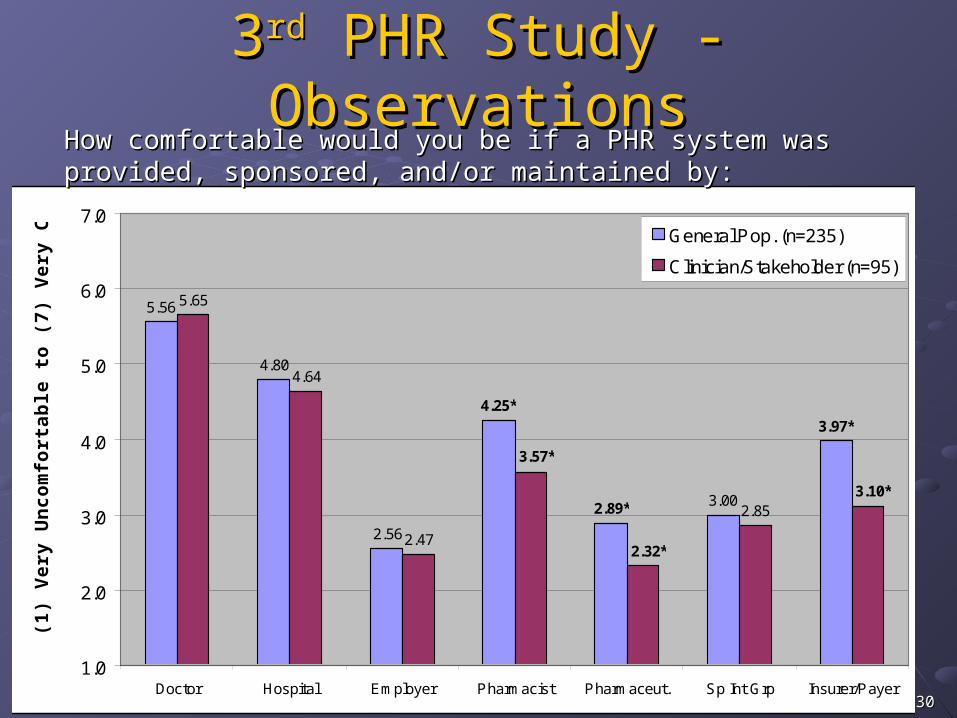
5.56
4.80
2.56
3.00
5.65
4.64
2.47
2.85
4.25*
2.89*
3.97*
3.57*
2.32*
3.10*
1.0
2.0
3.0
4.0
5.0
6.0
7.0
Doctor Hospital Employer Pharmacist Pharmaceut. Sp Int Grp Insurer/Payer
(1)
Ve
ry U
nc
om
fort
ab
le t
o (
7)
Ve
ry C
om
fort
ab
le General Pop. (n=235)
Clinician/Stakeholder (n=95)
How comfortable would you be if a PHR system was provided, How comfortable would you be if a PHR system was provided, sponsored, and/or maintained by:sponsored, and/or maintained by:
33rdrd PHR Study - Observations PHR Study - Observations
3131© Professor R. Agarwal 2005© Professor R. Agarwal 2005
33rdrd PHR Study - Observations PHR Study - ObservationsConsumers are far more comfortable receiving Consumers are far more comfortable receiving an electronic PHR from their PCP or hospital an electronic PHR from their PCP or hospital than they are from their employer, a than they are from their employer, a pharmaceutical company, health insurer, or a pharmaceutical company, health insurer, or a special interest groupspecial interest groupThe choice of what type of PHR the consumer The choice of what type of PHR the consumer would prefer is highly dependent on the source would prefer is highly dependent on the source of distribution of the PHR of distribution of the PHR As trust in an entity declines, consumer’s As trust in an entity declines, consumer’s choices regress towards stand-alone models choices regress towards stand-alone models such as paper- or home PC-based solutionssuch as paper- or home PC-based solutions

3232© Professor R. Agarwal 2005© Professor R. Agarwal 2005
Institution Level StudiesInstitution Level Studies
Data setData set Nationwide, longitudinal survey of Care Nationwide, longitudinal survey of Care
Delivery Organizations (CDOs)Delivery Organizations (CDOs) 2004-2005: 2,700 CDOs2004-2005: 2,700 CDOs
Type # of Facilities Ambulatory 17,697 Home Health 1,830 Hospital 3,983 Owned Payer 192 Sub-Acute 2,975 Total 26,994

3333© Professor R. Agarwal 2005© Professor R. Agarwal 2005
HIT Adoption in HospitalsHIT Adoption in Hospitals
Hospital Only (n=3983) Application Frequency % Adopt by '04 Electronic Claims - Clearing House Vendor 3860 96.9% Pharmacy Management System 3800 95.4% Laboratory Information System 3785 95.0% Clinical Decision Support System 2535 63.6% Radiology PACS 1383 34.7% EHR (RAND definition) 2223 34.2% Computerized Practitioner Order Entry (CPOE) 1026 25.8% Personal Health Record 170 4.3%
Electronic Claims used as a baseline. It is not an HIT but demonstrates validity of our data.

3434© Professor R. Agarwal 2005© Professor R. Agarwal 2005
Diffusion RatesDiffusion Rates
Diffusion Rates of HIT in Hospitals
0
10
20
30
40
50
60
70
80
90
100
1979 1984 1989 1994 1999 2004
% o
f H
os
pit
als
(n
=3
98
3)
Eclaims
CDSS
CPOE
PHR
LIS
PMS
RadPACS
EHR_RAND

3535© Professor R. Agarwal 2005© Professor R. Agarwal 2005
ObservationsObservations
Hospital EHR adoption is in the early stages of the Hospital EHR adoption is in the early stages of the diffusion curve. We may actually be seeing a drop-off diffusion curve. We may actually be seeing a drop-off due to:due to:
Potential government involvement in standards (consumers Potential government involvement in standards (consumers taking a wait-and-see approach)taking a wait-and-see approach)
Until the risk averse organizations (the highest percentage of Until the risk averse organizations (the highest percentage of organizations in the hospital market) see more ROI or benefit organizations in the hospital market) see more ROI or benefit from EHRs, they will not implement these solutions. from EHRs, they will not implement these solutions.
Some HITs diffuse rapidly, e.g. PACS (Picture Archiving Some HITs diffuse rapidly, e.g. PACS (Picture Archiving and Communication System) – why? ROI better? and Communication System) – why? ROI better? Easier to adopt? More useful? Value is better Easier to adopt? More useful? Value is better understood?understood?

3636© Professor R. Agarwal 2005© Professor R. Agarwal 2005
DescriptivesDescriptives
3983 Hospitals in analysis3983 Hospitals in analysis
3720 CIOs (93.4%), 158 No CIO, 104 3720 CIOs (93.4%), 158 No CIO, 104 VacantVacant
3106 Not-for-Profit (78%), 877 For Profit 3106 Not-for-Profit (78%), 877 For Profit (22%)(22%)
90% of hospitals have 400 or fewer beds, 90% of hospitals have 400 or fewer beds, 25% have 60 or fewer beds25% have 60 or fewer beds

3737© Professor R. Agarwal 2005© Professor R. Agarwal 2005
Does Size Matter? Does Size Matter? Variable Size N Mean
Statistical Signif (.05) Interpretation
HOSPOPEN 1 1000 1986.342 972 1978.133 999 1972.914 989 1965.28
Total 3960 1975.68NUMAPP12 1 1013 4.55
2 976 5.663 1002 5.994 990 6.54
Total 3981 5.68
AVGYRHIT1 1 911 1998.252 939 1997.993 950 1998.154 956 1998.09
Total 3756 1998.12
EARLYHIT2 1 911 1996.002 939 1995.663 950 1995.204 956 1994.22
Total 3756 1995.26Notes: 1 Of the 12 HIT applications examined, this is the average year of adoption of those that are used.2 Of the 12 HIT applications examined, this is the earliest year one was adopted.
Yes
Yes
There is not a statistically signficant difference in the average year of HIT adoption relative to size.
Largest hospitals are earliest adopters. No difference among other sizes.
No
Mixed
Older hospitals are larger.
Larger hospitals use more HIT applications.
3838© Professor R. Agarwal 2005© Professor R. Agarwal 2005
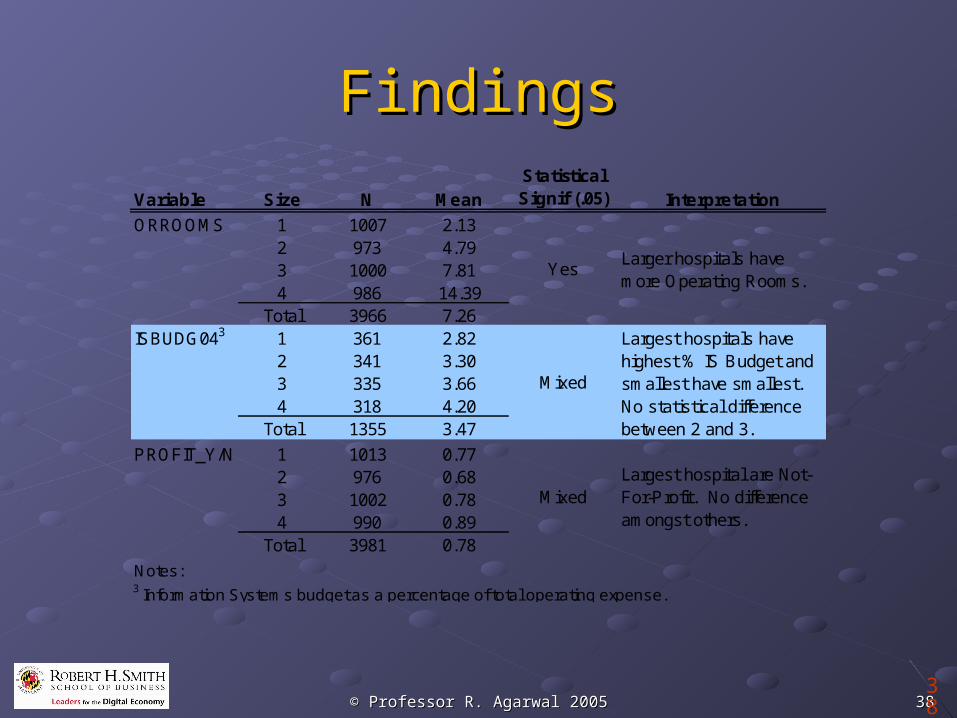
FindingsFindings
38
Variable Size N MeanStatistical Signif (.05) Interpretation
ORROOMS 1 1007 2.132 973 4.793 1000 7.814 986 14.39
Total 3966 7.26ISBUDG043 1 361 2.82
2 341 3.303 335 3.664 318 4.20
Total 1355 3.47
PROFIT_Y/N 1 1013 0.772 976 0.683 1002 0.784 990 0.89
Total 3981 0.78
Notes: 3 Information Systems budget as a percentage of total operating expense.
Mixed
Largest hospitals have highest % IS Budget and smallest have smallest. No statistical difference between 2 and 3.
MixedLargest hospital are Not-For-Profit. No difference amongst others.
YesLarger hospitals have more Operating Rooms.

3939© Professor R. Agarwal 2005© Professor R. Agarwal 2005
ConclusionConclusionHIT, particularly electronic records offer an HIT, particularly electronic records offer an opportunity to transform health careopportunity to transform health care Business case is compelling, but need more targeted Business case is compelling, but need more targeted
studies!studies!
PHR adoption is a critical prerequisite: patients PHR adoption is a critical prerequisite: patients see value but……see value but…… Information disseminationInformation dissemination Giving the technology “away”Giving the technology “away” Training and empowermentTraining and empowerment
Diffusion of HIT in CDOs needs further Diffusion of HIT in CDOs needs further investigation: intriguing patternsinvestigation: intriguing patterns

4040© Professor R. Agarwal 2005© Professor R. Agarwal 2005