Improving Pediatric Asthma Care and Outcomes...
11
Improving Pediatric Asthma Care and Outcomes Across Multiple Hospitals Flory Nkoy, MD, MS, MPH a , Bernhard Fassl, MD a , Bryan Stone, MD, MS a , Derek A. Uchida, MD a , Joseph Johnson, MD b , Carolyn Reynolds, MS, APRN b , Karen Valentine, MStat b , Karmella Koopmeiners, RN, MS b , Eun Hea Kim, BA a , Lucy Savitz, PhD b , Christopher G. Maloney, MD, PhD a abstract BACKGROUND AND OBJECTIVES: Gaps exist in inpatient asthma care. Our aims were to assess the impact of an evidence-based care process model (EB-CPM) 5 years after implementation at Primary Children’s Hospital (PCH), a tertiary care facility, and after its dissemination to 7 community hospitals. METHODS: Participants included asthmatics 2 to 17 years admitted at 8 hospitals between 2003 and 2013. The EB-CPM was implemented at PCH between January 2008 and March 2009, then disseminated to 7 community hospitals between January and June 2011. We measured compliance using a composite score (CS) for 8 quality measures. Outcomes were compared between preimplementation and postimplementation periods. Confounding was addressed through multivariable regression analyses. RESULTS: At PCH, the CS increased and remained at .90% for 5 years after implementation. We observed sustained reductions in asthma readmissions (P = .026) and length of stay (P , .001), a trend toward reduced costs (P = .094), and no change in hospital resource use, ICU transfers, or deaths. The CS also increased at the 7 community hospitals, reaching 80% to 90% and persisting .2 years after dissemination, with a slight but not significant readmission reduction (P = .119), a significant reduction in length of stay (P , .001) and cost (P = .053), a slight increase in hospital resource use (P = .032), and no change in ICU transfers or deaths. CONCLUSIONS: Our intervention resulted in sustained, long-term improvement in asthma care and outcomes at the tertiary care hospital and successful dissemination to community hospitals. Asthma is the most common reason for preventable emergency department (ED) and hospital admissions among children in the United States. 1–3 In 2009, .679 000 children with asthma were admitted to the ED or hospital. 1 Readmission rates of children to the ED or hospital are high and are associated with substantial health care costs. 2–4 Despite a major burden, significant gaps exist between the evidence of best asthma care practices and the actual care for children hospitalized with asthma. 5–8 Multiple quality improvement (QI) efforts to improve inpatient asthma care for children have been reported, but a positive impact on asthma outcomes is often not demonstrated. 3,9–18 No data exist about the sustainability or long-term impact of QI interventions. Furthermore, most of the successful pediatric inpatient asthma interventions are implemented at a tertiary care pediatric centers, with little information available about dissemination to community hospitals. 19–23 We previously reported suboptimal asthma care quality at Primary Children’s Hospital (PCH), 8 a tertiary care children’s hospital, and a Department of Pediatrics, University of Utah, Salt Lake City, Utah; and b Intermountain Healthcare, Salt Lake City, Utah Dr Nkoy conceptualized and designed the study, drafted the initial manuscript, and oversaw the analysis; Drs Fassl, Stone, Uchida, Johnson, Savitz, and Maloney, Ms Reynolds, and Ms Koopmeiners participated in the concept and design, interpretation of data, and review of the manuscript; Ms Valentine coordinated and supervised data collection, participated in data analysis, and critically reviewed the manuscript; Ms Kim coordinated and supervised data collection and critically reviewed the manuscript; and all authors approved the final manuscript as submitted. www.pediatrics.org/cgi/doi/10.1542/peds.2015-0285 DOI: 10.1542/peds.2015-0285 Accepted for publication Jun 11, 2015 Address correspondence to Flory L. Nkoy, MD, MS, MPH, Primary Children’ s Medical Center, Division of Pediatric Inpatient Medicine, University of Utah School of Medicine, 100 North Medical Drive, Salt Lake City, UT 84113. E-mail: fl[email protected] PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online, 1098-4275). Copyright © 2015 by the American Academy of Pediatrics QUALITY REPORT PEDIATRICS Volume 136, number 6, December 2015 by guest on May 17, 2018 http://pediatrics.aappublications.org/ Downloaded from
Transcript of Improving Pediatric Asthma Care and Outcomes...
Improving Pediatric Asthma Care andOutcomes Across Multiple HospitalsFlory Nkoy, MD, MS, MPHa, Bernhard Fassl, MDa, Bryan Stone, MD, MSa, Derek A. Uchida, MDa, Joseph Johnson, MDb,Carolyn Reynolds, MS, APRNb, Karen Valentine, MStatb, Karmella Koopmeiners, RN, MSb, Eun Hea Kim, BAa, Lucy Savitz, PhDb,Christopher G. Maloney, MD, PhDa
abstract BACKGROUND AND OBJECTIVES: Gaps exist in inpatient asthma care. Our aims were toassess the impact of an evidence-based care process model (EB-CPM) 5 yearsafter implementation at Primary Children’s Hospital (PCH), a tertiary carefacility, and after its dissemination to 7 community hospitals.
METHODS: Participants included asthmatics 2 to 17 years admitted at 8 hospitalsbetween 2003 and 2013. The EB-CPM was implemented at PCH betweenJanuary 2008 and March 2009, then disseminated to 7 community hospitalsbetween January and June 2011. We measured compliance using a compositescore (CS) for 8 quality measures. Outcomes were compared betweenpreimplementation and postimplementation periods. Confounding wasaddressed through multivariable regression analyses.
RESULTS: At PCH, the CS increased and remained at .90% for 5 years afterimplementation. We observed sustained reductions in asthma readmissions(P = .026) and length of stay (P , .001), a trend toward reduced costs(P = .094), and no change in hospital resource use, ICU transfers, or deaths.The CS also increased at the 7 community hospitals, reaching 80% to 90% andpersisting .2 years after dissemination, with a slight but not significantreadmission reduction (P = .119), a significant reduction in length of stay(P , .001) and cost (P = .053), a slight increase in hospital resource use(P = .032), and no change in ICU transfers or deaths.
CONCLUSIONS: Our intervention resulted in sustained, long-term improvement inasthma care and outcomes at the tertiary care hospital and successfuldissemination to community hospitals.
Asthma is the most common reason forpreventable emergency department(ED) and hospital admissions amongchildren in the United States.1–3 In2009, .679 000 children with asthmawere admitted to the ED or hospital.1
Readmission rates of children to the EDor hospital are high and are associatedwith substantial health care costs.2–4
Despite a major burden, significantgaps exist between the evidence of bestasthma care practices and the actualcare for children hospitalized withasthma.5–8 Multiple qualityimprovement (QI) efforts to improveinpatient asthma care for children have
been reported, but a positive impact onasthma outcomes is often notdemonstrated.3,9–18 No data existabout the sustainability or long-termimpact of QI interventions.Furthermore, most of the successfulpediatric inpatient asthmainterventions are implemented ata tertiary care pediatric centers, withlittle information available aboutdissemination to communityhospitals.19–23
We previously reported suboptimalasthma care quality at PrimaryChildren’s Hospital (PCH),8 a tertiarycare children’s hospital, and
aDepartment of Pediatrics, University of Utah, Salt Lake City,Utah; and bIntermountain Healthcare, Salt Lake City, Utah
Dr Nkoy conceptualized and designed the study,drafted the initial manuscript, and oversaw theanalysis; Drs Fassl, Stone, Uchida, Johnson, Savitz,and Maloney, Ms Reynolds, and Ms Koopmeinersparticipated in the concept and design,interpretation of data, and review of the manuscript;Ms Valentine coordinated and supervised datacollection, participated in data analysis, andcritically reviewed the manuscript; Ms Kimcoordinated and supervised data collection andcritically reviewed the manuscript; and all authorsapproved the final manuscript as submitted.
www.pediatrics.org/cgi/doi/10.1542/peds.2015-0285
DOI: 10.1542/peds.2015-0285
Accepted for publication Jun 11, 2015
Address correspondence to Flory L. Nkoy, MD, MS,MPH, Primary Children’s Medical Center, Division ofPediatric Inpatient Medicine, University of UtahSchool of Medicine, 100 North Medical Drive, SaltLake City, UT 84113. E-mail: [email protected]
PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online,1098-4275).
Copyright © 2015 by the American Academy ofPediatrics
QUALITY REPORT PEDIATRICS Volume 136, number 6, December 2015 by guest on May 17, 2018http://pediatrics.aappublications.org/Downloaded from
a significant improvement in qualityof care with reduction in asthmareadmissions 2 years afterimplementation of an evidence-basedasthma care process model(EB-CPM).21
Because of suboptimal baselineasthma care quality findings atcommunity hospitals and the desireto improve care throughout theregion, the specific aims of this studywere twofold: to evaluate the 5-year(or long-term) impact after EB-CPMimplementation at PCH and todetermine the impact ofdisseminating the EB-CPM to7 community hospitals. Specifically,we sought to assess changes frombaseline in provider compliance withevidence-based (EB) asthma inpatientquality measures and asthmahospitalization outcomes. Ourprimary outcome was 6-month ED orhospital asthma readmission,consistent with our previous work,21
and the current aim to assess long-term EB-CPM impact at PCH.Secondary outcomes were length ofstay (LOS), costs, hospital resourceuse, ICU transfer after inpatientadmission, and death.
METHODS
Setting
Our study included 8 IntermountainHealthcare hospitals. IntermountainHealthcare is a regional, not-for-profitintegrated health care deliverysystem, with 22 hospitals and160 clinics and urgent care facilitieslocated in Utah and southeasternIdaho,24 providing health care to∼1 680 000 patients. IntermountainHealthcare serves ∼60% of Utah’s 2.8million residents and 85% of Utah’schildren.25 Participating hospitalsinclude a 289-bed freestandingtertiary care children’s hospital (PCH)located in a major metropolitan area,staffed by pediatric hospitalists andsubspecialists, and both urban andrural general community hospitalswith pediatric wards, staffed by
general pediatricians and familyphysicians with limited pediatricresources.
PCH is affiliated with the Departmentof Pediatrics at the University of Utahand serves as a tertiary care pediatricreferral hospital for Utah and4 surrounding states (Wyoming,Nevada, Idaho, and Montana). The7 Utah community hospitals wereAmerican Fork Community Hospitalin American Fork, Dixie RegionalHospital in St George, LoganCommunity Hospital in Logan, McKayDee Hospital in Ogden, RivertonCommunity Hospital in Riverton, UtahValley Regional Medical Center inProvo, and Valley View Hospital inCedar City. Overall, the 8 hospitalsprovide care to ∼700 asthmaticchildren each year and serve bothurban (PCH, Riverton, McKay Dee,and Utah Valley) and rural (AmericanFork, Dixie, Valley View, and Logan)populations. The IntermountainHealthcare privacy and University ofUtah institutional review boardsapproved the study.
Planning the Intervention
EB-CPM implementation at PCH wasdescribed previously.21 Wedisseminated the EB-CPM to7 community hospitals by using theReplicating Effective Programsframework.26 We securedIntermountain Healthcare leadershipsupport, which led to prioritization ofour project as one of theorganizational clinical goals,identified local hospital physicianchampions, and assembleda multidisciplinary implementationteam with representatives from eachhospital, including physicianchampions; nursing, respiratorytherapy, and pharmacist leaders;hospital administrators; and QI staff.We obtained baseline compliancedata for each hospital, which showedsuboptimal asthma care, and sharedthese data with hospital clinical andadministrative leaders. We securedlocal administrative leadershipsupport, ensured buy-in of local
clinical staff (physicians, nurses,respiratory therapists, andpharmacists) through education andtraining, and adapted the PCHtraining manual and decision supporttools to fit local needs to facilitateEB-CPM integration into workflow.
The Intervention (Asthma EB-CPM)
Asthma EB-CPM Description
The EB-CPM was designed tostandardize asthma care and supporthospital compliance with EB asthmaquality measures.8 The EB-CPMincluded decision support tools(admission and discharge ordersets), with the followingcomponents: a standardizedassessment of both acute andchronic asthma severity and control,recommendations for acute care andchronic asthma control, algorithmsfor escalating and weaning fromalbuterol and oxygen, criteria forspecialist consultation, criteriafor pediatric ICU transfer, criteriafor discharge, and a standardizedtemplate and checklist to facilitatecare transition to the primary careprovider, including a written asthmaaction plan, patient and parentcompetency-oriented asthmaeducation modeled on the HomeManagement Plan of Care,27 andalgorithm-based stepwiseadjustment of controller therapy.28
Implementation and Dissemination ofthe EB-CPM
We began EB-CPM implementation21
at PCH in January 2008 and completedit in March 2009 by usinga Plan–Do–Study–Act rapid cycleapproach.29,30 To ensure EB-CPMsustainability at PCH, we replaced thepaper-based discharge order set withan electronic discharge process,21,31
allowing automated informationexchange and care continuity withprimary care providers.28 The EB-CPMdissemination to community hospitalsstarted in January 2011 and wascompleted in June 2011. We providedon-site education and training ofclinical and administrative staff and
PEDIATRICS Volume 136, number 6, December 2015 e1603 by guest on May 17, 2018http://pediatrics.aappublications.org/Downloaded from

data feedback during monthlymeetings with participating hospitalrepresentatives. Feedback data werealso shared with local hospital clinicaland administrative staff by localphysician champions. Finally, weprovided ongoing technical assistanceto physician champions and theirteams for troubleshooting theimplementation process.
Planning the Study
We used 8 EB quality measures fromour previous work to evaluate theEB-CPM impact.8 These included4 measures to assess compliancewith EB treatments for acuteexacerbations: (1) documented acuteasthma severity on admission, (2) useof quick reliever medications in thehospital, (3) use of systemiccorticosteroid medication in thehospital, and (4) restricted use ofipratropium bromide to ,24 hoursafter admission. They also included4 measures to assess compliance withEB measures intended to decreasereadmission risk: (5) documentedasthma education, (6) documenteddegree of chronic asthma control, (7)use of appropriate controller therapyprescription based on degree ofasthma control, and (8) documentedasthma action plan at discharge, withinstructions on how to recognize andavoid triggers and with follow-upappointment date and time.
Data Collection
This was a QI study of children aged 2to 17 years, discharged fromparticipating hospitals betweenJanuary 1, 2003, and December 31,2013, with the InternationalClassification of Diseases, NinthRevision primary diagnostic code ofasthma (493.xx). Data collectionincluded compliance with the 8quality measures and associatedasthma outcomes and was completedmanually for quality measures 1, 5, 6,7, and 8, and electronically (using theIntermountain Healthcare enterprisedata warehouse [EDW])32 for qualitymeasures 2, 3, and 4. Manual
collection of compliance metricswas facilitated by creation of a Web-based data collection form, anddata collection sources includedphysician and nursing documentationand medication administrationrecords.
The EDW was used to collect outcomevariables including asthmareadmission (ED revisit or hospitalreadmission with a primary diagnosisof asthma) at any of 22 Intermountainhospitals, hospital LOS in hours,variable hospitalization cost (directcost), hospital relative resource units(RRUs) used, ICU transfer within24 hours of admission, and death.Hospitalization cost was inflationadjusted for 2013. RRU isa standardized value adjusted forinflation and local market factors toallow comparison of resource usebetween hospitals and across years,reflecting the relative intensity ofresources used for each hospitalcharge.33 Finally, we used the EDW toretrieve demographic and othercovariates, including age, gender, race,insurance, calendar month ofhospitalization, and severity of illness(SOI) using All Patient RefinedDiagnosis Related Groups.34
For PCH, asthma discharges betweenJanuary 2003 and March 2009were defined as baseline(before implementation) withpostimplementation dischargesbetween April 2009 and December2013. For community hospitals,asthma discharges between January2003 and June 2011 were used asbaseline, with postimplementationdischarges including those betweenJuly 2011 and December 2013.
We included baseline data back to2003 to take into account anypreexisting secular trends.
Baseline data were collectedretrospectively andpostimplementation dataprospectively. For each patient, werecorded whether the care teamwas compliant with each measure(1 = yes and 0 = no). Individual
measure compliance per patient wassummed (ranging from 0 to 8) andused to calculate averagecompliance with individualmeasures and an average compositescore35 per hospital.
Data Analysis
We compared patient characteristicsbetween preimplementation andpostimplementation periods usingx2 for categorical and Wilcoxon t testfor continuous variables. We assessedchanges in compliance, by using thecomposite score, at PCHindependently and at communityhospitals as a group because oflimited sample size at individualcommunity hospitals. We used the“patient average” (cumulativepercentage of quality measuresachieved for each patient) method tocalculate the composite score.35 Weused statistical process control chartsto visually assess changes over timein 6-month asthma readmission andLOS between the preimplementationand postimplementation periods. Logtransformation was applied to LOS,cost, and RRU data, and log-linearregression analysis was used tocompare these outcomes betweenpreimplementation andpostimplementation periods. Thesemodels were adjusted for covariates.Finally, we used Fisher’s exact test toassess the EB-CPM impact on PICUtransfer.
RESULTS
There were 3510 children withasthma discharged from PCHand 1721 from community hospitalsduring the study period: 46.7%(1640/3510) and 74.3% (1279/1721)during preimplementation and53.3% (1870/3510) and25.7% (442/1721) during thepostimplementation period,respectively. Table 1 comparesdemographic characteristicsbetween preimplementation andpostimplementation populations. AtPCH, we noted significant differences
e1604 NKOY et al by guest on May 17, 2018http://pediatrics.aappublications.org/Downloaded from
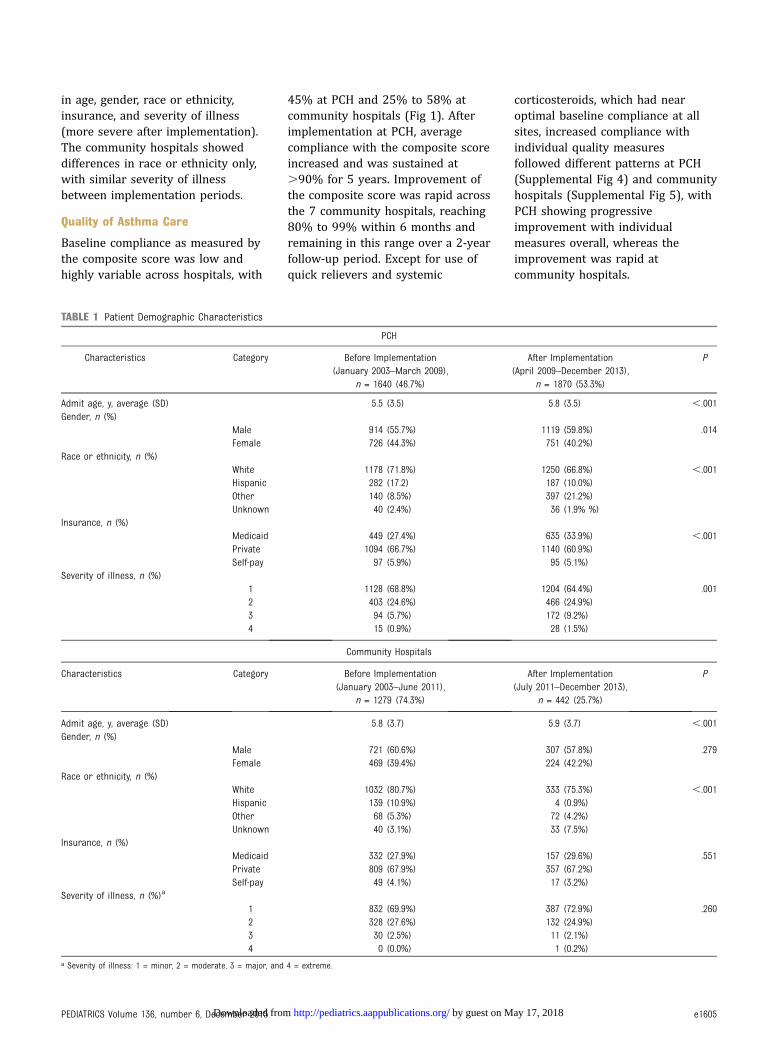
in age, gender, race or ethnicity,insurance, and severity of illness(more severe after implementation).The community hospitals showeddifferences in race or ethnicity only,with similar severity of illnessbetween implementation periods.
Quality of Asthma Care
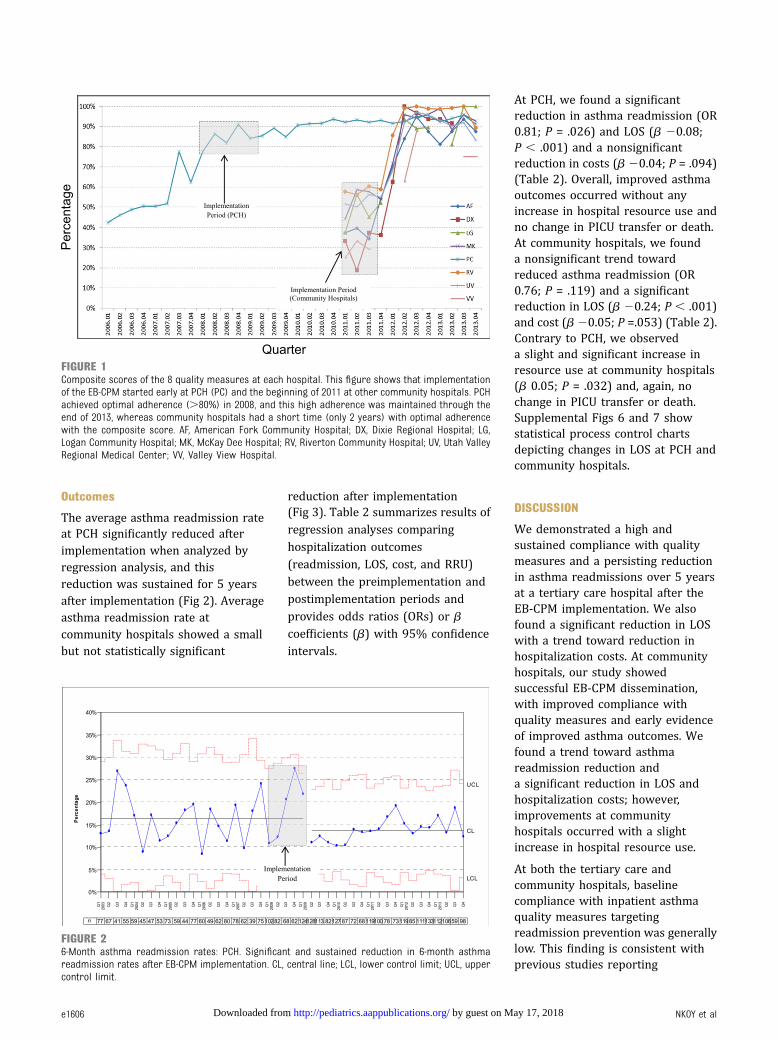
Baseline compliance as measured bythe composite score was low andhighly variable across hospitals, with
45% at PCH and 25% to 58% atcommunity hospitals (Fig 1). Afterimplementation at PCH, averagecompliance with the composite scoreincreased and was sustained at.90% for 5 years. Improvement ofthe composite score was rapid acrossthe 7 community hospitals, reaching80% to 99% within 6 months andremaining in this range over a 2-yearfollow-up period. Except for use ofquick relievers and systemic
corticosteroids, which had nearoptimal baseline compliance at allsites, increased compliance withindividual quality measuresfollowed different patterns at PCH(Supplemental Fig 4) and communityhospitals (Supplemental Fig 5), withPCH showing progressiveimprovement with individualmeasures overall, whereas theimprovement was rapid atcommunity hospitals.
TABLE 1 Patient Demographic Characteristics
PCH
Characteristics Category Before Implementation(January 2003–March 2009),
n = 1640 (46.7%)
After Implementation(April 2009–December 2013),
n = 1870 (53.3%)
P
Admit age, y, average (SD) 5.5 (3.5) 5.8 (3.5) ,.001Gender, n (%)
Male 914 (55.7%) 1119 (59.8%) .014Female 726 (44.3%) 751 (40.2%)
Race or ethnicity, n (%)White 1178 (71.8%) 1250 (66.8%) ,.001Hispanic 282 (17.2) 187 (10.0%)Other 140 (8.5%) 397 (21.2%)Unknown 40 (2.4%) 36 (1.9% %)
Insurance, n (%)Medicaid 449 (27.4%) 635 (33.9%) ,.001Private 1094 (66.7%) 1140 (60.9%)Self-pay 97 (5.9%) 95 (5.1%)
Severity of illness, n (%)1 1128 (68.8%) 1204 (64.4%) .0012 403 (24.6%) 466 (24.9%)3 94 (5.7%) 172 (9.2%)4 15 (0.9%) 28 (1.5%)
Community Hospitals
Characteristics Category Before Implementation(January 2003–June 2011),
n = 1279 (74.3%)
After Implementation(July 2011–December 2013),
n = 442 (25.7%)
P
Admit age, y, average (SD) 5.8 (3.7) 5.9 (3.7) ,.001Gender, n (%)
Male 721 (60.6%) 307 (57.8%) .279Female 469 (39.4%) 224 (42.2%)
Race or ethnicity, n (%)White 1032 (80.7%) 333 (75.3%) ,.001Hispanic 139 (10.9%) 4 (0.9%)Other 68 (5.3%) 72 (4.2%)Unknown 40 (3.1%) 33 (7.5%)
Insurance, n (%)Medicaid 332 (27.9%) 157 (29.6%) .551Private 809 (67.9%) 357 (67.2%)Self-pay 49 (4.1%) 17 (3.2%)
Severity of illness, n (%)a
1 832 (69.9%) 387 (72.9%) .2602 328 (27.6%) 132 (24.9%)3 30 (2.5%) 11 (2.1%)4 0 (0.0%) 1 (0.2%)
a Severity of illness: 1 = minor, 2 = moderate, 3 = major, and 4 = extreme.
PEDIATRICS Volume 136, number 6, December 2015 e1605 by guest on May 17, 2018http://pediatrics.aappublications.org/Downloaded from
Outcomes
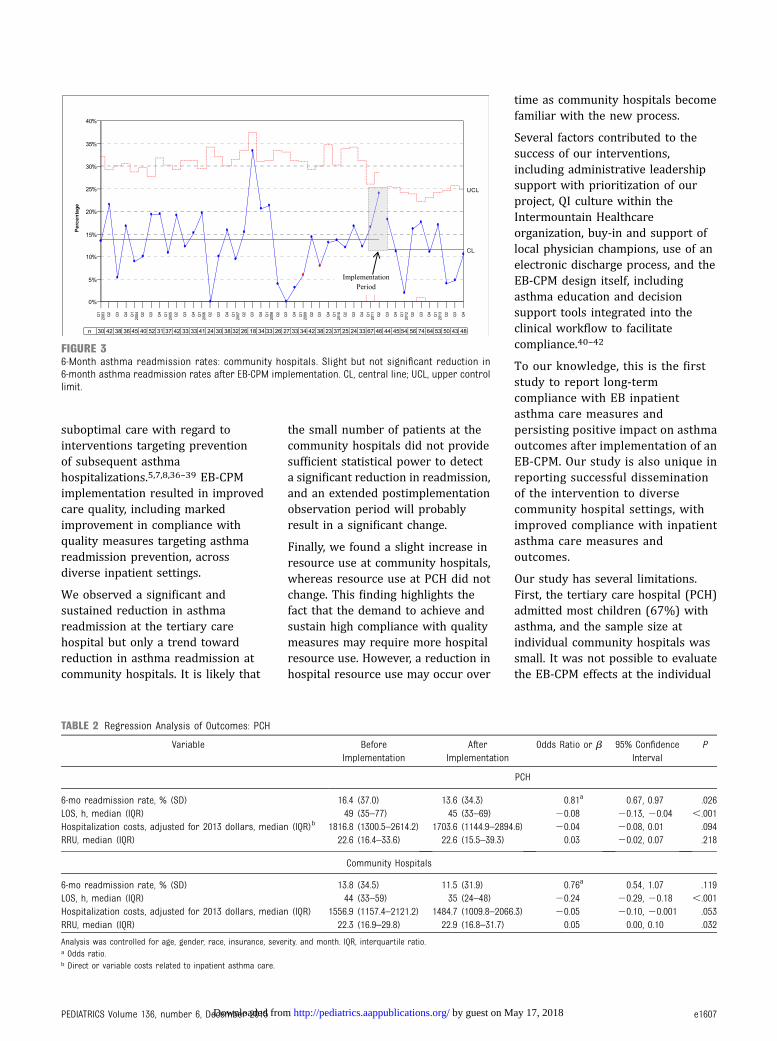
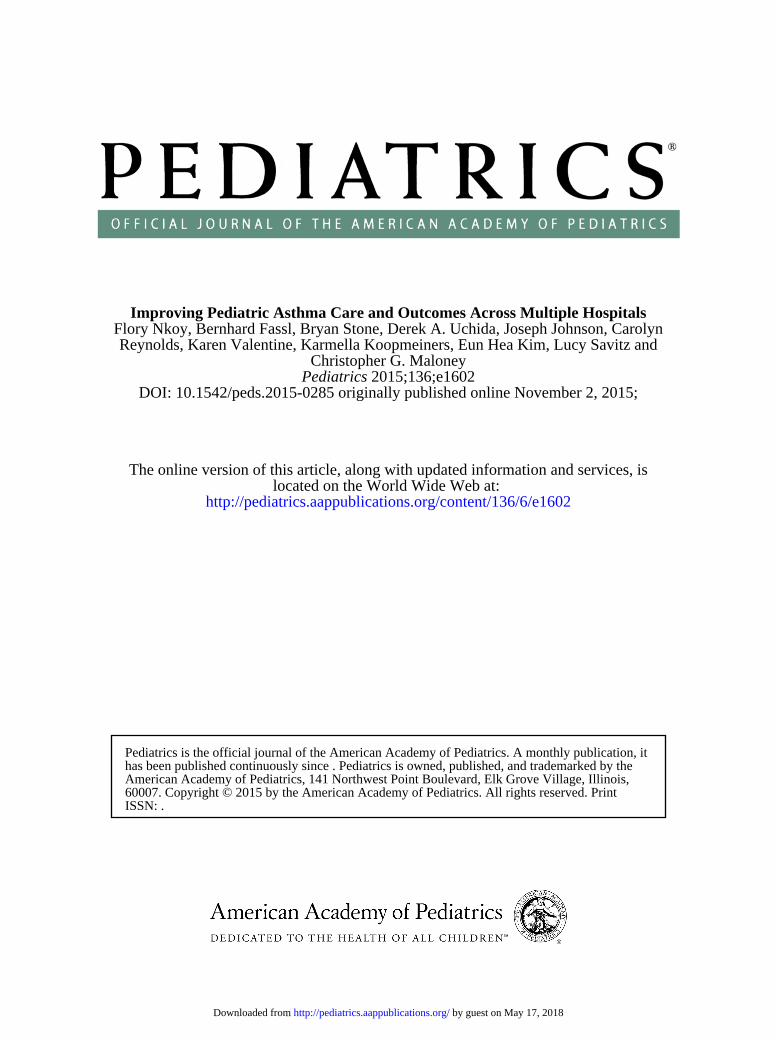
The average asthma readmission rateat PCH significantly reduced afterimplementation when analyzed byregression analysis, and thisreduction was sustained for 5 yearsafter implementation (Fig 2). Averageasthma readmission rate atcommunity hospitals showed a smallbut not statistically significant
reduction after implementation(Fig 3). Table 2 summarizes results of
regression analyses comparing
hospitalization outcomes
(readmission, LOS, cost, and RRU)
between the preimplementation and
postimplementation periods and
provides odds ratios (ORs) or b
coefficients (b) with 95% confidence
intervals.
At PCH, we found a significantreduction in asthma readmission (OR0.81; P = .026) and LOS (b 20.08;P , .001) and a nonsignificantreduction in costs (b 20.04; P = .094)(Table 2). Overall, improved asthmaoutcomes occurred without anyincrease in hospital resource use andno change in PICU transfer or death.At community hospitals, we founda nonsignificant trend towardreduced asthma readmission (OR0.76; P = .119) and a significantreduction in LOS (b 20.24; P , .001)and cost (b20.05; P =.053) (Table 2).Contrary to PCH, we observeda slight and significant increase inresource use at community hospitals(b 0.05; P = .032) and, again, nochange in PICU transfer or death.Supplemental Figs 6 and 7 showstatistical process control chartsdepicting changes in LOS at PCH andcommunity hospitals.
DISCUSSION
We demonstrated a high andsustained compliance with qualitymeasures and a persisting reductionin asthma readmissions over 5 yearsat a tertiary care hospital after theEB-CPM implementation. We alsofound a significant reduction in LOSwith a trend toward reduction inhospitalization costs. At communityhospitals, our study showedsuccessful EB-CPM dissemination,with improved compliance withquality measures and early evidenceof improved asthma outcomes. Wefound a trend toward asthmareadmission reduction anda significant reduction in LOS andhospitalization costs; however,improvements at communityhospitals occurred with a slightincrease in hospital resource use.
At both the tertiary care andcommunity hospitals, baselinecompliance with inpatient asthmaquality measures targetingreadmission prevention was generallylow. This finding is consistent withprevious studies reporting
FIGURE 1Composite scores of the 8 quality measures at each hospital. This figure shows that implementationof the EB-CPM started early at PCH (PC) and the beginning of 2011 at other community hospitals. PCHachieved optimal adherence (.80%) in 2008, and this high adherence was maintained through theend of 2013, whereas community hospitals had a short time (only 2 years) with optimal adherencewith the composite score. AF, American Fork Community Hospital; DX, Dixie Regional Hospital; LG,Logan Community Hospital; MK, McKay Dee Hospital; RV, Riverton Community Hospital; UV, Utah ValleyRegional Medical Center; VV, Valley View Hospital.
FIGURE 26-Month asthma readmission rates: PCH. Significant and sustained reduction in 6-month asthmareadmission rates after EB-CPM implementation. CL, central line; LCL, lower control limit; UCL, uppercontrol limit.
e1606 NKOY et al by guest on May 17, 2018http://pediatrics.aappublications.org/Downloaded from
suboptimal care with regard tointerventions targeting preventionof subsequent asthmahospitalizations.5,7,8,36–39 EB-CPMimplementation resulted in improvedcare quality, including markedimprovement in compliance withquality measures targeting asthmareadmission prevention, acrossdiverse inpatient settings.
We observed a significant andsustained reduction in asthmareadmission at the tertiary carehospital but only a trend towardreduction in asthma readmission atcommunity hospitals. It is likely that
the small number of patients at thecommunity hospitals did not providesufficient statistical power to detecta significant reduction in readmission,and an extended postimplementationobservation period will probablyresult in a significant change.
Finally, we found a slight increase inresource use at community hospitals,whereas resource use at PCH did notchange. This finding highlights thefact that the demand to achieve andsustain high compliance with qualitymeasures may require more hospitalresource use. However, a reduction inhospital resource use may occur over
time as community hospitals becomefamiliar with the new process.
Several factors contributed to thesuccess of our interventions,including administrative leadershipsupport with prioritization of ourproject, QI culture within theIntermountain Healthcareorganization, buy-in and support oflocal physician champions, use of anelectronic discharge process, and theEB-CPM design itself, includingasthma education and decisionsupport tools integrated into theclinical workflow to facilitatecompliance.40–42
To our knowledge, this is the firststudy to report long-termcompliance with EB inpatientasthma care measures andpersisting positive impact on asthmaoutcomes after implementation of anEB-CPM. Our study is also unique inreporting successful disseminationof the intervention to diversecommunity hospital settings, withimproved compliance with inpatientasthma care measures andoutcomes.
Our study has several limitations.First, the tertiary care hospital (PCH)admitted most children (67%) withasthma, and the sample size atindividual community hospitals wassmall. It was not possible to evaluatethe EB-CPM effects at the individual
FIGURE 36-Month asthma readmission rates: community hospitals. Slight but not significant reduction in6-month asthma readmission rates after EB-CPM implementation. CL, central line; UCL, upper controllimit.
TABLE 2 Regression Analysis of Outcomes: PCH
Variable BeforeImplementation
AfterImplementation
Odds Ratio or b 95% ConfidenceInterval
P
PCH
6-mo readmission rate, % (SD) 16.4 (37.0) 13.6 (34.3) 0.81a 0.67, 0.97 .026LOS, h, median (IQR) 49 (35–77) 45 (33–69) 20.08 20.13, 20.04 ,.001Hospitalization costs, adjusted for 2013 dollars, median (IQR)b 1816.8 (1300.5–2614.2) 1703.6 (1144.9–2894.6) 20.04 20.08, 0.01 .094RRU, median (IQR) 22.6 (16.4–33.6) 22.6 (15.5–39.3) 0.03 20.02, 0.07 .218
Community Hospitals
6-mo readmission rate, % (SD) 13.8 (34.5) 11.5 (31.9) 0.76a 0.54, 1.07 .119LOS, h, median (IQR) 44 (33–59) 35 (24–48) 20.24 20.29, 20.18 ,.001Hospitalization costs, adjusted for 2013 dollars, median (IQR) 1556.9 (1157.4–2121.2) 1484.7 (1009.8–2066.3) 20.05 20.10, 20.001 .053RRU, median (IQR) 22.3 (16.9–29.8) 22.9 (16.8–31.7) 0.05 0.00, 0.10 .032
Analysis was controlled for age, gender, race, insurance, severity. and month. IQR, interquartile ratio.a Odds ratio.b Direct or variable costs related to inpatient asthma care.
PEDIATRICS Volume 136, number 6, December 2015 e1607 by guest on May 17, 2018http://pediatrics.aappublications.org/Downloaded from

community hospital level. Second, weused the EDW data to track asthmareadmissions at any of the 22Intermountain Healthcare hospitals.Although Intermountain Healthcarecovers 85% of pediatric care in thestate, we may have missedreadmissions at non–IntermountainHealthcare facilities. The impact ofthis is unknown but unlikely tochange our results. Third,implementation and disseminationreceived leadership support fromIntermountain Healthcare and wasfacilitated by organizational changesat each facility to support compliance.The impact of leadership support andorganizational change is difficult toestimate. Efforts to disseminate theEB-CPM to facilities outsideIntermountain Healthcare may faceadditional challenges, although webelieve that our approach43 todissemination can be appliedanywhere.
Fourth, our EB-CPM is complex. Inour analysis we did not determinethe individual effect of EB-CPMcomponents on asthma outcomes.Fifth, the EB-CPM was introducedinto a dynamic real-world clinicalsetting in which many otherunmeasured variables may haveaffected the results, such as changesin access to asthma care,socioeconomic barriers to care, andimprovements in the quality ofasthma care resulting fromintroduction of the 2007 asthmaguidelines. However, Fig 1 showssuboptimal compliance with qualitymeasures at community hospitalsthat persisted ∼4 years after the2007 asthma guideline publicationand changed only after EB-CPMimplementation in 2011. We alsobelieve that including insurancetype, age, gender, race, underlying
asthma severity, and calendar monthin our adjusted analysis at leastpartially addressed unmeasuredconfounding factors. Sixth, weincluded SOI as a confounding factorin our regression analyses. SOI is animperfect marker of illness severityat presentation. It is also a reflectionof diagnoses coded and resourceuse.
Seventh, our study populationincluded only children with a primarydiagnosis of asthma, identifiedelectronically through the EDW, andwould exclude children with asthmadischarged with another primarydiagnosis, such as viral pneumonia.However, a review of our datasuggested that including only thosewith a primary diagnosis of asthmacaptures the great majority of cases.44
Lastly, previous studies have reportedthe effect of organizational factors onimplementation of QI interventionsand provider compliance with EBcare.42,45–47 Specifically, success of animplementation strategy is a functionof the relationship between thenature of the evidence, the context inwhich the proposed change isimplemented, and the methodsthrough which change isfacilitated.48–51 Our future planincludes assessing organizationalfactors associated with successfulimplementation and dissemination ofEB-CPMs. We hope to identify keyfactors that can be addressed tofacilitate implementation anddissemination of an EB interventionto more broadly improve asthma careand outcomes.
CONCLUSIONS
Our results showed not onlyimproved asthma care and outcomesbut also long-term sustainability of
the EB-CPM impact at PCH, a tertiarycare children’s hospital, andsuccessful dissemination to 7community hospitals, with evidenceof improvement in both the qualityof asthma care and clinical outcomes.Our study demonstrates thepotential use of EB-CPMs to achievesustained improvement in asthmacare and outcomes in varioushospital settings.
ACKNOWLEDGMENTS
We acknowledge the medical,nursing, respiratory therapy, andadministrative staff at participatinghospitals for their efforts anddiligence during the implementationand dissemination of the EB-CPM.We also thank the Pediatric ClinicalProgram leadership, includingDr Ed Clark and Ms CarolynReynolds, as well as Dr Brent Jamesof the Intermountain Institute forHealthcare Delivery Research fortheir support for this project. Finally,Dr Nkoy has full access to all thedata in the study and takesresponsibility for the integrity of thedata and accuracy of the dataanalysis.
ABBREVIATIONS
CS: composite scoreEB: evidence-basedEB-CPM: evidence-based care
process modelED: emergency departmentEDW: enterprise data warehouseLOS: length of stayOR: odds ratioPCH: Primary Children’s HospitalQI: quality improvementRRU: relative resource unitSOI: severity of illness
FINANCIAL DISCLOSURE: Drs Nkoy, Stone, and Fassl received salary and travel support through an Agency for Healthcare Research and Quality (AHRQ) grant.
Dr Maloney, Ms Koopmeiners, and Ms Kim received salary support through an AHRQ grant. The remaining authors have no financial relationships relevant to this
article to disclose.
e1608 NKOY et al by guest on May 17, 2018http://pediatrics.aappublications.org/Downloaded from

FUNDING: Supported by grant 1R18HS018166-01A1 from the Agency for Healthcare Research and Quality (AHRQ) to Drs Nkoy, Stone, and Fassl. Regarding funding
sources outside the scope of work for this publication, Drs Nkoy, Stone, Fassl, and Maloney are also supported by grant 1R18HS018678-01A1 (Improving Post-
Hospital Transitions and Ambulatory Care for Children With Asthma) from the AHRQ. Dr Stone is also supported by award KM1CA156723 from the National Cancer
Institute. None of the sponsors participated in design and conduct of the study; collection, management, analysis, and interpretation of the data; or preparation,
review, or approval of the manuscript. Its contents are solely the responsibility of the authors and do not necessarily represent the official view of the AHRQ or the
National Institutes of Health.
POTENTIAL CONFLICT OF INTEREST: Drs Nkoy, Fassl, Stone, and Maloney have a patent pending for an electronic tool (electronic AsthmaTracker) developed to support
asthma self-monitoring and management in children. The other authors have indicated they have no potential conflicts of interest to disclose.
REFERENCES
1. Akinbami LJ, Moorman JE, Liu X. Asthmaprevalence, health care use, andmortality: United States, 2005–2009. NatlHealth Stat Rep. 2011; Jan 12(32):1–14
2. Chung HS, Hathaway DK, Lew DB. Riskfactors associated with hospitalreadmission in pediatric asthma.J Pediatr Nurs. 2015;30(2):364–384
3. Kenyon CC, Melvin PR, Chiang VW, ElliottMN, Schuster MA, Berry JG.Rehospitalization for childhood asthma:timing, variation, and opportunities forintervention. J Pediatr. 2014;164(2):300–305
4. Barnett SB, Nurmagambetov TA. Costs ofasthma in the United States: 2002–2007.J Allergy Clin Immunol. 2011;127(1):145–152
5. Kattan M. Quality of inpatient care forasthma: challenges and opportunities.Pediatrics. 2008;122(6):1369–1370
6. Kattan M, Crain EF, Steinbach S, et al. Arandomized clinical trial of clinicianfeedback to improve quality of care forinner-city children with asthma.Pediatrics. 2006;117(6). Available at:www.pediatrics.org/cgi/content/full/117/6/e1095
7. Lantner R, Brennan RA, Gray L, McElroy D.Inpatient management of asthma in theChicago suburbs: the Suburban AsthmaManagement Initiative (SAMI). J Asthma.2005;42(1):55–63
8. Nkoy FL, Fassl BA, Simon TD, et al. Qualityof care for children hospitalized withasthma. Pediatrics. 2008;122(5):1055–1063
9. Bunik M, Federico MJ, Beaty B, Rannie M,Olin JT, Kempe A. Quality improvementfor asthma care within a hospital-basedteaching clinic. Acad Pediatr. 2011;11(1):58–65
10. Burgess SW, Sly PD, Devadason SG.Providing feedback on adherenceincreases use of preventive medication
by asthmatic children. J Asthma. 2010;47(2):198–201
11. Butz AM, Halterman J, Bellin M, et al.Improving preventive care in high riskchildren with asthma: lessons learned.J Asthma. 2014;51(5):498–507
12. Crane S, Sailer D, Patch SC. Improvingasthma care in emergency departments:results of a multihospital collaborativequality initiative in rural western NorthCarolina. N C Med J. 2011;72(2):111–117
13. Gold J, Reyes-Gastelum D, Turner J,Davies HD; Pediatric Asthma QualityTeam. A quality improvement study usingfishbone analysis and an electronicmedical records intervention to improvecare for children with asthma. Am J MedQual. 2014;29(1):70–77
14. Kuhlmann S, Mason B, Ahlers-SchmidtCR. A quality improvement project toimprove compliance with the JointCommission Children’s AsthmaCare–3 measure. Hosp Pediatr. 2013;3(1):45–51
15. Kwok R, Dinh M, Dinh D, Chu M.Improving adherence to asthma clinicalguidelines and discharge documentationfrom emergency departments:implementation of a dynamic andintegrated electronic decision supportsystem. Emerg Med Australas. 2009;21(1):31–37
16. Morse RB, Hall M, Fieldston ES, et al.Hospital-level compliance with asthmacare quality measures at children’shospitals and subsequent asthma-related outcomes. JAMA. 2011;306(13):1454–1460
17. Patel SJ, Longhurst CA, Lin A, et al.Integrating the home management planof care for children with asthma into anelectronic medical record. Jt Comm JQual Patient Saf. 2012;38(8):359–365
18. Shapiro A, Gracy D, Quinones W,Applebaum J, Sarmiento A. Putting
guidelines into practice: improvingdocumentation of pediatric asthmamanagement using a decision-makingtool. Arch Pediatr Adolesc Med. 2011;165(5):412–418
19. Andrews K, Esposito D, Taylor E, et al.Evaluation of the Business Case forQuality, Phase II: Cincinnati Children’sHospital Medical Center Case Study.Princeton, NJ: Mathematica PolicyResearch; 2013
20. Bergert L, Patel SJ, Kimata C, Zhang G,Matthews WJ Jr. Linking patient-centeredmedical home and asthma measuresreduces hospital readmission rates.Pediatrics. 2014;134(1). Available at:www.pediatrics.org/cgi/content/full/134/1/e249
21. Fassl BA, Nkoy FL, Stone BL, et al. TheJoint Commission Children’s AsthmaCare quality measures and asthmareadmissions. Pediatrics. 2012;130(3):482–491
22. McCarthy D, Cohen A. The CincinnatiChildren’s Hospital Medical Center’sAsthma Improvement Collaborative:Enhancing quality and coordination ofcare. Innovations in Care Transitions.The Commonwealth Fund Pub. 2013; 1660vol. 7: 1-19. Available at: http://www.commonwealthfund.org/∼/media/files/publications/case-study/2013/jan/1660_mccarthy_care_transitions_cincinnati_case_study_v2.pdf. Accessed September23, 2015
23. Vernacchio L, Francis ME, Epstein DM,et al. Effectiveness of an asthma qualityimprovement program designed formaintenance of certification. Pediatrics.2014;134(1). Available at: www.pediatrics.org/cgi/content/full/134/1/e242
24. James BC, Savitz LA. How Intermountaintrimmed health care costs throughrobust quality improvement efforts.Health Aff (Millwood). 2011;30(6):1185–1191
PEDIATRICS Volume 136, number 6, December 2015 e1609 by guest on May 17, 2018http://pediatrics.aappublications.org/Downloaded from

25. Byington CL, Reynolds CC, Korgenski K,et al. Costs and infant outcomes afterimplementation of a care process modelfor febrile infants. Pediatrics. 2012;130(1). Available at: www.pediatrics.org/cgi/content/full/130/1/e16
26. Kilbourne AM, Neumann MS, Pincus HA,Bauer MS, Stall R. Implementingevidence-based interventions in healthcare: application of the replicatingeffective programs framework.Implement Sci. 2007;2:42
27. The Joint Commission. SpecificationsManual for National Hospital InpatientQuality Measures. 2014; V4.3b_1.Available at: www.jointcommission.org/specifications_manual_for_national_hospital_inpatient_quality_measures.aspx. Accessed September23, 2015
28. National Heart Lung and Blood Institute.Expert panel report 3: guidelines for thediagnosis and management of asthma.Periodic Assessment and Monitoring:Essential for Asthma Management. 2007;(Section 3): 52-54. Available at: www.nhlbi.nih.gov/files/docs/guidelines/asthgdln.pdf. Accessed September 23,2015
29. Agency for Healthcare Research andQuality. Managing and evaluatingrapidcycle process improvements asvehicles for hospital system redesign.2011. Available at: http://archive.ahrq.gov/research/findings/final-reports/rapidcycle/rapidcycle1.html
30. Lau CY. Quality improvement tools andprocesses. Neurosurg Clin N Am. 2015;26(2):177–187, viii
31. Nkoy F, Stone B, Fassl B, et al.Development of a novel tool for engagingchildren and parents in asthma self-management. AMIA Annu Symp Proc.2012;2012:663–672
32. Evans RS, Lloyd JF, Pierce LA. Clinical useof an enterprise data warehouse. AMIAAnnu Symp Proc. 2012;2012:189–198
33. National Committee for QualityAssurance. The surprising health carecost–quality disconnect. Using NCQA’srelative resource use measures to getvalue: efficient, high-quality care. 2011.
Available at: http://www.ncqa.org/Portals/0/Newsroom/2013/NCQA%20RRU%20Fact%20Sheet.pdf
34. Lavernia CJ, Laoruengthana A, ContrerasJS, Rossi MD. All-patient refineddiagnosis-related groups in primaryarthroplasty. J Arthroplasty. 2009;24(6 suppl):19–23
35. Reeves D, Campbell SM, Adams J,Shekelle PG, Kontopantelis E, Roland MO.Combining multiple indicators of clinicalquality: an evaluation of differentanalytic approaches. Med Care. 2007;45(6):489–496
36. Davies G, Paton JY, Beaton SJ, Young D,Lenney W. Children admitted with acutewheeze/asthma during November1998–2005: a national UK audit. Arch DisChild. 2008;93(11):952–958
37. Lintzenich A, Teufel RJ II, Basco WT Jr.Younger asthmatics are less likely toreceive inhaled corticosteroids andasthma education after admission forexacerbation. Clin Pediatr (Phila). 2010;49(12):1111–1116
38. Ly CD, Dennehy CE. Emergencydepartment management of pediatricasthma at a university teaching hospital.Ann Pharmacother. 2007;41(10):1625–1631
39. Mattke S, Martorell F, Sharma P,Malveaux F, Lurie N. Quality of care forchildhood asthma: estimating impactand implications. Pediatrics. 2009;123(suppl 3):S199–S204
40. Gifford E, Tavakoli S, Wisdom J, Hamlett-Berry K. Implementation of smokingcessation treatment in VHA substanceuse disorder residential treatmentprograms. Psychiatr Serv. 2015;66(3):295–302
41. Nkoy FL, Fassl BA, Wolfe D, Colling D,Hales JW, Maloney CG. Sustainingcompliance with pediatric asthmainpatient quality measures. AMIA AnnuSymp Proc. 2010;2010:547–551
42. Quintanilha M, Downs S, Lieffers J, BerryT, Farmer A, McCargar LJ. Factors andbarriers associated with early adoptionof nutrition guidelines in Alberta,
Canada. J Nutr Educ Behav. 2013;45(6):510–517
43. Neumann MS, Sogolow ED. Replicatingeffective programs: HIV/AIDS preventiontechnology transfer. AIDS Educ Prev.2000;12(5 suppl):35–48
44. West S, Nkoy F, Fassl B, Stone B, HalbernS, Maloney C. Validity and reliability ofthe Joint Commission subjectidentification criteria for assessing thequality of children’s inpatient asthmacare. J Invest Med. 2011;59(1):158
45. Goldsack J, Bergey M, Mascioli S,Cunningham J. Hourly rounding andpatient falls: what factors boostsuccess? Nursing. 2015;45(2):25–30
46. Marchionni C, Ritchie J. Organizationalfactors that support the implementationof a nursing best practice guideline.J Nurs Manag. 2008;16(3):266–274
47. Moja L, Liberati EG, Galuppo L, et al.Barriers and facilitators to the uptake ofcomputerized clinical decision supportsystems in specialty hospitals: protocolfor a qualitative cross-sectional study.Implement Sci. 2014;9:105
48. Aarons GA, Ehrhart MG, Farahnak LR,Sklar M. Aligning leadership acrosssystems and organizations to developa strategic climate for evidence-basedpractice implementation. Annu RevPublic Health. 2014;35:255–274
49. Cummings GG, Estabrooks CA, MidodziWK, Wallin L, Hayduk L. Influence oforganizational characteristics andcontext on research utilization. Nurs Res.2007;56(4 suppl):S24–S39
50. Demby H, Gregory A, Broussard M,Dickherber J, Atkins S, Jenner LW.Implementation lessons: the importanceof assessing organizational “fit” andexternal factors when implementingevidence-based teen pregnancyprevention programs. J Adolesc Health.2014;54(3 suppl):S37–S44
51. Morden A, Ong BN, Brooks L, et al.Introducing evidence through research“push”: using theory and qualitativemethods [published online ahead ofprint February 5, 2015]. Qual Health Res.doi:1049732315570120
e1610 NKOY et al by guest on May 17, 2018http://pediatrics.aappublications.org/Downloaded from

DOI: 10.1542/peds.2015-0285 originally published online November 2, 2015; 2015;136;e1602Pediatrics
Christopher G. MaloneyReynolds, Karen Valentine, Karmella Koopmeiners, Eun Hea Kim, Lucy Savitz and
Flory Nkoy, Bernhard Fassl, Bryan Stone, Derek A. Uchida, Joseph Johnson, CarolynImproving Pediatric Asthma Care and Outcomes Across Multiple Hospitals
ServicesUpdated Information &
http://pediatrics.aappublications.org/content/136/6/e1602including high resolution figures, can be found at:
Supplementary Material
015-0285.DCSupplementalhttp://pediatrics.aappublications.org/content/suppl/2015/10/28/peds.2Supplementary material can be found at:
References
-1http://pediatrics.aappublications.org/content/136/6/e1602.full#ref-listThis article cites 44 articles, 11 of which you can access for free at:
Subspecialty Collections
munology_subhttp://classic.pediatrics.aappublications.org/cgi/collection/allergy:imAllergy/Immunologyprovement_subhttp://classic.pediatrics.aappublications.org/cgi/collection/quality_imQuality Improvementtion:practice_management_subhttp://classic.pediatrics.aappublications.org/cgi/collection/administraAdministration/Practice Managementfollowing collection(s): This article, along with others on similar topics, appears in the
Permissions & Licensing
https://shop.aap.org/licensing-permissions/in its entirety can be found online at: Information about reproducing this article in parts (figures, tables) or
Reprintshttp://classic.pediatrics.aappublications.org/content/reprintsInformation about ordering reprints can be found online:
ISSN: . 60007. Copyright © 2015 by the American Academy of Pediatrics. All rights reserved. Print American Academy of Pediatrics, 141 Northwest Point Boulevard, Elk Grove Village, Illinois,has been published continuously since . Pediatrics is owned, published, and trademarked by the Pediatrics is the official journal of the American Academy of Pediatrics. A monthly publication, it
by guest on May 17, 2018http://pediatrics.aappublications.org/Downloaded from
DOI: 10.1542/peds.2015-0285 originally published online November 2, 2015; 2015;136;e1602Pediatrics
Christopher G. MaloneyReynolds, Karen Valentine, Karmella Koopmeiners, Eun Hea Kim, Lucy Savitz and
Flory Nkoy, Bernhard Fassl, Bryan Stone, Derek A. Uchida, Joseph Johnson, CarolynImproving Pediatric Asthma Care and Outcomes Across Multiple Hospitals
http://pediatrics.aappublications.org/content/136/6/e1602located on the World Wide Web at:
The online version of this article, along with updated information and services, is
ISSN: . 60007. Copyright © 2015 by the American Academy of Pediatrics. All rights reserved. Print American Academy of Pediatrics, 141 Northwest Point Boulevard, Elk Grove Village, Illinois,has been published continuously since . Pediatrics is owned, published, and trademarked by the Pediatrics is the official journal of the American Academy of Pediatrics. A monthly publication, it
by guest on May 17, 2018http://pediatrics.aappublications.org/Downloaded from