Inhalers in Pediatric Asthma
53
-
Upload
kishore-chandki -
Category
Documents
-
view
235 -
download
0
description
Inhalers in Pediatric Asthma: Presentation for Pediatric Students & General Practitioners!
Transcript of Inhalers in Pediatric Asthma


Inhalers in Pediatric AsthmaInhalers in Pediatric Asthma
Dr. KISHORE Dr. KISHORE CHANDKICHANDKI
Kids’ Care Clinic,Kids’ Care Clinic,
Indore (M.P.) INDIAIndore (M.P.) INDIA

Asthma in ChildrenAsthma in Children
With 30 million asthmatics in the country, India With 30 million asthmatics in the country, India constitutes constitutes 10% of the world10% of the world asthmatics asthmatics
Most Most common chronic diseasecommon chronic disease of childhood of childhood
Up to 20%Up to 20% of children affected in various geographical of children affected in various geographical areasareas
Up to Up to one-fourth one-fourth of the children in the pre-school age in of the children in the pre-school age in Delhi are Delhi are recurrent wheezersrecurrent wheezers. . [Times of India, Dec 18, 2004][Times of India, Dec 18, 2004]
No age is exemptNo age is exempt from asthma & it can even start early from asthma & it can even start early in infancy.in infancy.
In most children, asthma develops In most children, asthma develops before age 5 yearsbefore age 5 years, , and, in more than half, asthma develops before age 3 and, in more than half, asthma develops before age 3 yearsyears

Asthma in ChildrenAsthma in Children
Unfortunately, Unfortunately, prevalence is increasingprevalence is increasing in India in India
Fortunately, asthma Fortunately, asthma can be effectively treatedcan be effectively treated & most & most patients can achieve good control of their diseasepatients can achieve good control of their disease
Most in India are either Most in India are either unaware, undiagnosed or are unaware, undiagnosed or are sub-optimally treatedsub-optimally treated for asthma. This is despite India for asthma. This is despite India having the latest, most effective and extremely affordable having the latest, most effective and extremely affordable inhaled medicines to control asthmainhaled medicines to control asthma
The The most effectivemost effective asthma treatment – Inhalation asthma treatment – Inhalation Therapy is available in India at a Therapy is available in India at a price as low asprice as low as Rs. 4 to Rs. 4 to Rs. 6 per day which means that a year’s supply of Rs. 6 per day which means that a year’s supply of medicine is less than the cost of 1 night’s stay at the medicine is less than the cost of 1 night’s stay at the hospital!hospital!

What is Asthma?What is Asthma?Asthma is a Asthma is a chronic inchronic inflammatory disorderflammatory disorder of the of the airways. Chronically inflamed airways are airways. Chronically inflamed airways are hyperresponsivehyperresponsive; they become obstructed & airflow is ; they become obstructed & airflow is limited (by bronchoconstriction, mucus plugs, & limited (by bronchoconstriction, mucus plugs, & increased inflammation) when airways are exposed to increased inflammation) when airways are exposed to various risk factorsvarious risk factorsAsthma attacks (or exacerbations) are episodic, but Asthma attacks (or exacerbations) are episodic, but airway airway inflammation is chronicallyinflammation is chronically present presentA A stepwise approachstepwise approach to pharmacologic treatment to to pharmacologic treatment to achieve & maintain control of asthma should take into achieve & maintain control of asthma should take into account the safety of treatment, potential for adverse account the safety of treatment, potential for adverse effects, & the cost of treatment required to achieve controleffects, & the cost of treatment required to achieve controlAsthma is Asthma is not a cause for shamenot a cause for shame. Olympic athletes, . Olympic athletes, famous leaders, other celebrities, & ordinary people live famous leaders, other celebrities, & ordinary people live successful livessuccessful lives with asthma with asthma

Components of AsthmaComponents of AsthmaAsthma Triggers
Smooth Muscle Dysfunction
Allergens Exercise Irritants Viruses Weather
Inflammation
Bronchial Constriction
Hypertrophy Hyperplasia
Inflammatory Mediator Release
Bronchial Hyperreactivity
Symptoms
Exacerbations
Inflammatory Cell Infiltration
Architectural Changes
Mucus Secretion
Epithelial Damage
Edema
Impaired Ciliary
Function
Adapted from Creticos. Adv Stud Med. 2002;2(14):499-503

Consequences of Inflammation in Consequences of Inflammation in AsthmaAsthma
StimulusStimulus(Antigen, virus, pollutant, occupational agent)(Antigen, virus, pollutant, occupational agent)
AcuteAcuteInflammationInflammation
ResolutionResolution
Chronic InflammationChronic Inflammation
RemodelingRemodeling(fixed changes in the (fixed changes in the structure of airway)structure of airway)
Injury RepairInjury Repair
Airway dysfunctionAirway dysfunction
““Permanently” alteredPermanently” alteredlung functionlung function
Altered airway physiologyAltered airway physiology Airflow obstruction Airflow obstruction

Triggers for acute exacerbationTriggers for acute exacerbation Bhave et Bhave et
alal
37%
9%
8%
8%
7%
11%
14%
5% 1%Viral infection
Colddrinks/icecreams
Food item
Dust exposure
Change of season
Picnics/camps
Physical stress
Emotional stressN = 1050

Outcome of WheezersOutcome of Wheezers
Among infants, 20% have wheezing with only URIs, & Among infants, 20% have wheezing with only URIs, & 60% 60% no longerno longer have wheezing have wheezing by age 6by age 6 years years
Children who have asthma (recurrent symptoms Children who have asthma (recurrent symptoms continuing at age 6 y) have airway reactivity later in continuing at age 6 y) have airway reactivity later in childhoodchildhood
Children with mild asthma who are Children with mild asthma who are asymptomatic asymptomatic between attacksbetween attacks are likely to are likely to improveimprove and be symptom- and be symptom-free later in lifefree later in life
Children with asthma appear to have less severe Children with asthma appear to have less severe symptoms as they enter adolescence, but symptoms as they enter adolescence, but half of these half of these children continue to havechildren continue to have asthma. Asthma has a asthma. Asthma has a tendency to remit during puberty, with a somewhat tendency to remit during puberty, with a somewhat earlier remission in girls. However, compared with men, earlier remission in girls. However, compared with men, women have more AHRwomen have more AHR

Inhalational Therapy in Pediatric Inhalational Therapy in Pediatric AsthmaAsthma
Inhalation: Inhalation: cornerstonecornerstone of asthma treatment of asthma treatment
Not very popularNot very popular among lay man because of some among lay man because of some misconceptionsmisconceptions
Although asthma can be well controlled by highly Although asthma can be well controlled by highly effective anti-inflammatory therapy (mainly ICS) in effective anti-inflammatory therapy (mainly ICS) in majority, majority, optimal control is not achieved in 50%optimal control is not achieved in 50% of of patients in daily practicepatients in daily practice
There is a confusing There is a confusing array of inhaler devicesarray of inhaler devices & & drug/device combinations available and it can be difficult drug/device combinations available and it can be difficult for a clinician to make informed prescribing decisions for a clinician to make informed prescribing decisions about all the possible permutationsabout all the possible permutations

Inhalational Therapy: AdvantagesInhalational Therapy: Advantages
Aerosol Aerosol doses are generally smallerdoses are generally smaller than systemic than systemic doses; e.g., oral Salbutamol is 2 to 4 mg; inhaled 0.2 mg doses; e.g., oral Salbutamol is 2 to 4 mg; inhaled 0.2 mg (MDI) to 2.5 mg (Nebulized)(MDI) to 2.5 mg (Nebulized)
Onset of effectOnset of effect with inhaled drugs is faster than with with inhaled drugs is faster than with oral dosing; e.g., oral albuterol is ≤ 30 min; inhaled oral dosing; e.g., oral albuterol is ≤ 30 min; inhaled albuterol is ~ 5 minalbuterol is ~ 5 min
Drug is delivered Drug is delivered directlydirectly to the target organ (lung), with to the target organ (lung), with minimal systemic exposureminimal systemic exposure
Systemic side effectsSystemic side effects are less frequent and severe with are less frequent and severe with inhalation compared to systemic delivery (injection, inhalation compared to systemic delivery (injection, oral); e.g., less muscle tremor, tachycardia with ß2-oral); e.g., less muscle tremor, tachycardia with ß2-agonists; lower HPA suppression with corticosteroidsagonists; lower HPA suppression with corticosteroids
Inhaled drug therapy is less painful and relatively Inhaled drug therapy is less painful and relatively comfortablecomfortable

Inhalational Therapy: Inhalational Therapy: DisadvantagesDisadvantages
Lung Lung deposition is a relatively lowdeposition is a relatively low fraction of the total fraction of the total aerosol doseaerosol dose
A number of A number of variablesvariables (correct breathing pattern, use of (correct breathing pattern, use of device) can affect lung deposition and dose device) can affect lung deposition and dose reproducibilityreproducibility
Difficulty coordinatingDifficulty coordinating hand action and inhalation with hand action and inhalation with MDIsMDIs
Lack of knowledgeLack of knowledge of correct or optimal use of aerosol of correct or optimal use of aerosol devices by patients and cliniciansdevices by patients and clinicians
The number and variability of device types confuses The number and variability of device types confuses patients and clinicianspatients and clinicians
Lack of standardizedLack of standardized technical information on inhalers technical information on inhalers for cliniciansfor clinicians

Inhalant Drugs: ListInhalant Drugs: ListBronchodilatorsBronchodilators
ArformoterolArformoterol
BitolterolBitolterol
EpinephrineEpinephrine
FormoterolFormoterol
IpratropiumIpratropium
IsoetharineIsoetharine
IsoproterenolIsoproterenol
LevalbuterolLevalbuterol
MetaproterenolMetaproterenol
PirbuterolPirbuterol
ProcaterolProcaterol
Racepinephrine (racemic Racepinephrine (racemic epinephrine)epinephrine)
SalbutamolSalbutamol
SalmeterolSalmeterol
TerbutalineTerbutaline
TiotropiumTiotropium
Anti-inflammatoryAnti-inflammatory
BeclomethasoneBeclomethasone
BudesonideBudesonide
CiclesonideCiclesonide
CromolynCromolyn
FlunisolideFlunisolide
FluticasoneFluticasone
DexamethasoneDexamethasone
FluticasoneFluticasone
MometasoneMometasone
NedocromilNedocromil
TriamcinoloneTriamcinolone
AntimicrobialsAntimicrobials
PentamidinePentamidine
RibavirinRibavirin
TobramycinTobramycin
ZanamivirZanamivir
MiscellaneousMiscellaneous
Aromatic ammoniaAromatic ammonia
Dornase alfaDornase alfa
GlutathioneGlutathione
InsulinInsulin
MethacholineMethacholine
NicotineNicotine
Sodium chlorideSodium chloride
MucolyticsMucolytics
AmbroxolAmbroxol
N-acetyl cysteineN-acetyl cysteine

Inhalant Drugs: EffectsInhalant Drugs: Effects

Asthma Treatment: EvolutionAsthma Treatment: Evolution

Evolution of Asthma ParadigmsEvolution of Asthma Paradigms
1970s–1980sBronchoconstriction
(Spirometry)
1980s–1990s
Inflammation
(PC20, Inflam cells, FeNO)
1990s–2000s
Remodeling
Relieve SymptomsPrevent Symptoms
Prevent AttacksPrevent Remodeling
Prevent SymptomsPrevent Attacks
Bronchial Hyperreactivity
Fixed ObstructionSymptoms

Therapy for Chronic Asthma in Therapy for Chronic Asthma in ChildrenChildren
Acute relief from symptoms Anti-inflammatory
Sustained bronchodilatorUnproven anti-inflammatory
Oral short acting ß2 agonists & xanthines: not for maintenance TxOral short acting ß2 agonists & xanthines: not for maintenance TxOther drugs: oral steroids, H1 antihistaminesOther drugs: oral steroids, H1 antihistamines
SABA
AnticholinergicIpratropium
Xanthine:Short Acting
ICS
ChromonesNa Cromoglycate
Nedocromil Na
SRTheophyllines
Leukotrieneantagonists
LABA
Slow release xanthines
Leukotrieneantagonists
PRN basis
Adjuncts
Aminophylline
Immunomodulators:Omalizumab (anti-IgE)
Adrenaline/Epi
Relievers Preventers
Controllers

Asthma Classification & Asthma Classification & ManagementManagement

Levels of Asthma Control > 5 yrs Levels of Asthma Control > 5 yrs GINA GINA
20112011
*Any exacerbation should prompt review of maintenance treatment to ensure that is adequate*Any exacerbation should prompt review of maintenance treatment to ensure that is adequateҰҰ By definition, an exacerbation in any week makes that an uncontrolled asthma week By definition, an exacerbation in any week makes that an uncontrolled asthma week¥ Without administration of bronchodilator, lung function is not a reliable test for children 5 years & ¥ Without administration of bronchodilator, lung function is not a reliable test for children 5 years & youngeryounger

Characteristic Controlled(All of the following)
Partly Controlled(Any measure present in any week)
Uncontrolled (3 or more of features of partly controlled asthma in any week)
Daytime symptoms: wheezing, cough, difficult breathing
None(less than twice/week, typically for short periods on the order of minutes and rapidly relieved by use of a rapid acting bronchodilator)
More than twice/week(typically for short periods on the order of minutes and rapidly relieved by use of a rapid-acting bronchodilator)
More than twice a week (typically last minutes or hours or recur, but partially or fully relieved with rapid-acting bronchodilator)
Limitations of activities
None(child is fully active, plays and runs without limitations or symptoms)
Any (may cough, wheeze, or have difficulty breathing during exercise, vigorous play, or laughing)
Any
Nocturnal symptoms/awakening
None(including no nocturnal coughing during sleep)
Any (typically coughs during sleep or wakes with cough, wheezing, and/or difficult breathing)
Any
Need for reliever/rescue Tx
≤2 days/week >2 days/week >2 days/week
Levels of Asthma Control ≤ 5 yrs Levels of Asthma Control ≤ 5 yrs GINA GINA
20092009

Management approach: Children > 5 years Management approach: Children > 5 years & Adults& Adults

Management approach: Children ≤ 5 yearsManagement approach: Children ≤ 5 years
GINA 2009GINA 2009
Controller:None
Controller:Low dose
ICS*
LT modifier
Controller:Double low-Dose ICS*
Low doseICS + LTModifier
Education, Environmental Control, As needed rapid-acting β2 agonist
ControlledPartly
Controlled
Uncontrolled orPartly Controlledon low dose ICS
When asthmaIs controlled:
Reduce therapyMonitor
*Preferred
Reliever: Rapid acting β2 agonist prn

Stepping Up: Inhalation Stepping Up: Inhalation therapytherapy
When asthma is When asthma is NOT controlledNOT controlled with: with:Rapid onset, short acting or LABA bronchodilatorsRapid onset, short acting or LABA bronchodilatorsRepeated dosing with bronchodilators in this class Repeated dosing with bronchodilators in this class provides temporary relief until the cause of the days provides temporary relief until the cause of the days signals the need for review and possible increase of signals the need for review and possible increase of controller therapycontroller therapyInhaled corticosteroidsInhaled corticosteroidsTemporarily doubling the dose of IGCS has not been Temporarily doubling the dose of IGCS has not been demonstrated to effective and is no longer recommended. demonstrated to effective and is no longer recommended. A fourfold or greater increase has been demonstrated to A fourfold or greater increase has been demonstrated to be equivalent to a short course of Oral GCSbe equivalent to a short course of Oral GCSCombination of ICS & LABACombination of ICS & LABAIn a single inhaler both as a controller and a reliever is In a single inhaler both as a controller and a reliever is effective in maintaining a high level of asthma control and effective in maintaining a high level of asthma control and reduces exacerbation requiring systemic GCS and reduces exacerbation requiring systemic GCS and hospitalizationhospitalization

Stopping Inhalation therapyStopping Inhalation therapy
When control is achieved with…When control is achieved with…
Low dose ICS Low dose ICS switch to switch to once dailyonce daily dosing dosing
Mod to high dose ICS Mod to high dose ICS reduce by reduce by 50% after 3 mo50% after 3 mo
ICS + LABA ICS + LABA Reduce ICS by 50% Reduce ICS by 50%
Bring ICS to lowest doseBring ICS to lowest dose
Omit LABAOmit LABA
ICS + Other ICS + Other Same as above Same as above
Stop when no symptoms for Stop when no symptoms for one yearone year

Equipotent Daily Doses of ICS: Age > 5 Equipotent Daily Doses of ICS: Age > 5 years/Adultsyears/Adults

Equipotent Daily Doses of ICSEquipotent Daily Doses of ICS
Beclomethasone 200-500 100-200 >500-1000 >200-400 >1000 >400
Budesonide 200-600 100-200 600-1000 >200-400 >1000 >400
Budesonide-Neb Inhalation Suspension
250-500 >500-1000 >1000
Ciclesonide 80 – 160 80-160 >160-320 >160-320 >320-1280 >320
Flunisolide 500-1000 500-750 >1000-2000 >750-1250 >2000 >1250
Fluticasone 100-250 100-200 >250-500 >200-500 >500 >500
Mometasone furoate
200-400 ?100-200 > 400-800 >200-400 >800-1200 >400
Triamcinolone acetonide
400-1000 ? 400-800 >1000-2000 >800-1200 >2000 >1200
Drug (µg) Low Daily Dose>5 y ≤ 5 y
Medium Daily Dose>5 y ≤ 5 y
High Daily Dose> 5 y ≤ 5 y

Combination InhalersCombination Inhalers
Steroid/LABASteroid/LABA Can improve complianceCan improve compliance Useful when asthma stableUseful when asthma stable Lack of flexibility to Lack of flexibility to or or dose dose
MultidosingMultidosing
Multiple puffsMultiple puffs (up to 10) of a short-acting (up to 10) of a short-acting ßß2 agonist via 2 agonist via a spacer device is a spacer device is as effectiveas effective as nebulised as nebulised
Children (& adults) with mild & moderate exacerbation Children (& adults) with mild & moderate exacerbation of asthma should be treated by bronchodilator given of asthma should be treated by bronchodilator given from a MDI + spacer with doses titrated according to from a MDI + spacer with doses titrated according to clinical responseclinical response

Inhalational Therapy: DevicesInhalational Therapy: Devices
Aerosol Aerosol devices includedevices include::
Metered-dose inhaler (MDI)Metered-dose inhaler (MDI)
Pressurized Metered Dose Inhaler (pMDI)Pressurized Metered Dose Inhaler (pMDI)
Breath-activated metered-dose inhalerBreath-activated metered-dose inhaler
Metered-dose inhaler with spacerMetered-dose inhaler with spacer
Dry powder inhaler (DPI) e.g. RotacapsDry powder inhaler (DPI) e.g. Rotacaps
NebulizerNebulizer

Metered Dose Inhalers Metered Dose Inhalers (MDI)(MDI)
Uses chemical propellants (hydro-fuoroalkane Uses chemical propellants (hydro-fuoroalkane instead of CFC) to deliver medication dose to instead of CFC) to deliver medication dose to lungslungs
Salbutamol (Asthalin, Ventorlin)Salbutamol (Asthalin, Ventorlin) Levosalbutamol (Levolin)Levosalbutamol (Levolin) Salmeterol (Serobid)Salmeterol (Serobid) Terbutaline (Bricanyl)Terbutaline (Bricanyl) Ipratropium (Ipravent)Ipratropium (Ipravent) Triotropium (Tiova)Triotropium (Tiova) Combinations (Duolin, Aerocort, Seroflo)Combinations (Duolin, Aerocort, Seroflo)

Metered Dose Inhalers Metered Dose Inhalers (MDI)(MDI)Reliever bronchodilatorsReliever bronchodilators
(usually blue)(usually blue)
Inhaled steroidsInhaled steroids(usually brown/orange)(usually brown/orange)
Long acting beta 2 Long acting beta 2 agonists (Always green)agonists (Always green)

MDI InhalersMDI Inhalers
Portable, compactPortable, compact
Short treatment timeShort treatment time
Reproducible dose Reproducible dose emitted per actuationemitted per actuation
Most medications are Most medications are available in this formavailable in this form
Hand-breathing Hand-breathing coordination & technique coordination & technique importantimportant
High oropharyngeal High oropharyngeal impaction without spacerimpaction without spacer
Failure to shake can alter Failure to shake can alter drug dosedrug dose
Foreign body aspiration Foreign body aspiration from debris-filled from debris-filled mouthpiecemouthpiece
No dose counterNo dose counter
AdvantagesAdvantages DisadvantagesDisadvantages

Dry Powder Inhalers Dry Powder Inhalers (DPIs)(DPIs)
RotahalerRotahaler DiskhalerDiskhaler DiskusDiskus

DPI: RotahalerDPI: Rotahaler
Small and portableSmall and portable
Built-in dose counterBuilt-in dose counter
Propellant-freePropellant-free
Breath-actuated (drug Breath-actuated (drug comes when patient comes when patient breaths in)breaths in)
Short preparation and Short preparation and administration timeadministration time
Dependence on patient’s Dependence on patient’s inspiratory flowinspiratory flow
Patients less aware of Patients less aware of delivered dosedelivered dose
Relatively high Relatively high oropharyngeal impaction oropharyngeal impaction can occurcan occur
Moisture sensitiveMoisture sensitive
Limited range of drugsLimited range of drugs
More expensive than MDIMore expensive than MDI
AdvantagesAdvantages DisadvantagesDisadvantages

Now Now recommended for administration recommended for administration of allof all MDI medications MDI medications
Spacers or holding Spacers or holding chamberschambers

SpacersSpacers
Less/No coordination Less/No coordination required required
Improved delivery of Improved delivery of drug to lower airwaysdrug to lower airways
May breathe in & out May breathe in & out several times to receive several times to receive complete dose complete dose
Faster delivery than Faster delivery than nebulizer & less nebulizer & less expensive expensive
Reduced Reduced oropharyngeal drug oropharyngeal drug impaction & lossimpaction & loss
Large, cumbersome than Large, cumbersome than MDI aloneMDI alone
Expensive wrt MDI aloneExpensive wrt MDI alone
Cleaning requiredCleaning required
Some assembly may be Some assembly may be neededneeded
Patient errors include Patient errors include firing multiple puffs into firing multiple puffs into chamber prior to chamber prior to inhaling, or delay inhaling, or delay between actuation and between actuation and inhalationinhalation
AdvantagesAdvantages DisadvantagesDisadvantages

SteroidsSteroids from a MDI from a MDI must always be prescribedmust always be prescribed with a spacer to with a spacer to improve drug delivery and diminish side-effectsimprove drug delivery and diminish side-effectsSmaller volume (250-300 ml) are suitable for children < 5 years and Smaller volume (250-300 ml) are suitable for children < 5 years and larger volume > 500 ml) for older childrenlarger volume > 500 ml) for older childrenShould be Should be washed weeklywashed weekly. To reduce the static electricity in plastic . To reduce the static electricity in plastic spacers the spacer should be washed with a liquid detergent, not spacers the spacer should be washed with a liquid detergent, not rinsed in water, and left to drip-dry overnightrinsed in water, and left to drip-dry overnightIf commercially available spacers are not available a If commercially available spacers are not available a 500 ml plastic500 ml plastic bottlebottle can be used as a spacer. A hole to fit the MDI is cut or melted can be used as a spacer. A hole to fit the MDI is cut or melted into the bottom of the bottle using the hot wire technique. into the bottom of the bottle using the hot wire technique. Polystyrene cups are not efficient spacersPolystyrene cups are not efficient spacersOne puff at a time should be actuated into the spacer and the child One puff at a time should be actuated into the spacer and the child should breathe 4-5 times before the next actuation. After inhalation should breathe 4-5 times before the next actuation. After inhalation of ICS, the of ICS, the mouth should be rinsedmouth should be rinsed..If a spacer with a facemask is used it should be applied tightly to If a spacer with a facemask is used it should be applied tightly to the face. The face should be washed after corticosteroid inhalation the face. The face should be washed after corticosteroid inhalation to prevent skin changes (spider nevi, atrophy)to prevent skin changes (spider nevi, atrophy)
SpacersSpacers

Nebulizers are principally used for Nebulizers are principally used for Children (<5 years) and adults (<55 years) who have Children (<5 years) and adults (<55 years) who have difficulty coordinating the use of MDIs and DPIsdifficulty coordinating the use of MDIs and DPIs
By patients with severe asthma or chronic obstructive By patients with severe asthma or chronic obstructive pulmonary disease (COPD)pulmonary disease (COPD)
In the emergency room for acute episodes of In the emergency room for acute episodes of bronchospasmbronchospasm
NebulizersNebulizers

NebulizersNebulizers
Use of passive Use of passive breathing: Any age breathing: Any age
Easy to teach & useEasy to teach & use
Patient coordination Patient coordination not requirednot required
High drug doses High drug doses possible, Many drugs possible, Many drugs
Can be used with Can be used with supplemental Osupplemental O2
Mixtures (>1 drug), if Mixtures (>1 drug), if drugs are compatibledrugs are compatible
Time intensiveTime intensive
Inefficient & Inefficient & cumbersomecumbersome
Equipment and power Equipment and power source requiredsource required
Cleaning requiredCleaning required
Variability in Variability in performanceperformance
Potential for drug Potential for drug delivery into eyes with delivery into eyes with maskmask
AdvantagesAdvantages DisadvantagesDisadvantages

How to choose delivery devices for How to choose delivery devices for asthmaasthma
Arch Dis Child 2000;82:185-187
NebulizerNebulizer Infants & toddlersInfants & toddlers EmergencyEmergency Poor coordination Poor coordination

Inhalational Drugs: Inhalational Drugs: MetabolismMetabolism
The fate of an inhaled drug. The total amount of drug in the The fate of an inhaled drug. The total amount of drug in the systemic circulation is the sum of the systemic absorption systemic circulation is the sum of the systemic absorption via the lungs and via the GI tractvia the lungs and via the GI tract

Inhaler Devices & Drug DeliveryInhaler Devices & Drug Delivery
NebulizerNebulizer 1 – 5% 1 – 5%
DPIDPI 5 – 10% 5 – 10%
MDIMDI 5 – 10%5 – 10%
MDI with Spacer (esp. Steroids)MDI with Spacer (esp. Steroids) 10 – 15% 10 – 15%
Disc DPIDisc DPI ~15%~15%
TurbuhalerTurbuhaler >30%>30%
Asthma By Consensus, IAP

Inhaler Devices & Drug DeliveryInhaler Devices & Drug Delivery

Device & Technique: Device & Technique: ConcernsConcerns
Up to 50%Up to 50% of patients are unable to use of patients are unable to use inhaler correctlyinhaler correctly
Most patients, nurse and doctors are Most patients, nurse and doctors are unable to use unable to use pMDIspMDIs correctly correctly
Patients forget instructions and Patients forget instructions and skills skills deteriorate over timedeteriorate over time – reassessment – reassessment and re-educationand re-education
Need forNeed for clear specific training for clear specific training for patients of correct inhaler techniquepatients of correct inhaler technique

Barriers to Inhalational Barriers to Inhalational TherapyTherapy
Fear about steroids Fear about steroids
Do not like public labeling as asthmaticDo not like public labeling as asthmatic
Fear of addiction Fear of addiction
Feel pumps reserved for serious or severe Feel pumps reserved for serious or severe attacks or will fail to act attacks or will fail to act
Misconception that costly Misconception that costly
Prefer oral medications Prefer oral medications
Physicians lack of knowledge and time Physicians lack of knowledge and time

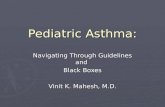
1 2 4 5 6 7 8 930 10 11 12
Age of Children (Years)
13 14 15 16+
Fluticasone MDI (HFA)
FDA = Food and Drug Administration; DPI = dry-powder inhaler; MDI = metered-dose inhaler; HFA = hydrofluoroalkane
Beclomethasone MDI
Budesonide DPI
Flunisolide MDI
Triamcinolone MDI
Beclomethasone MDI (HFA)
Budesonide Nebulization
Fluticasone DPI
Inhaled Corticosteroids: FDA-Inhaled Corticosteroids: FDA-ApprovalsApprovals
Mometasone DPI
Fluticasone/Salmeterol DPI

Inhaled CorticosteroidsInhaled Corticosteroids
Minimal effective doseMinimal effective dose to control asthma in the patient is to control asthma in the patient is always a goal of ICS therapyalways a goal of ICS therapy
In the past, patients were started on medium to high In the past, patients were started on medium to high doses of ICS until control is achieved & then step down to doses of ICS until control is achieved & then step down to the lowest dose that maintains control. The current the lowest dose that maintains control. The current guidelines recommend starting patients on guidelines recommend starting patients on dosages dosages based upon level of severitybased upon level of severity and then to titrate up or down and then to titrate up or down based upon responsiveness to therapybased upon responsiveness to therapy
Most patients' Most patients' symptoms will improve in 1–2 weekssymptoms will improve in 1–2 weeks of of therapy & will reach maximum improvement in 4–8 weeks. therapy & will reach maximum improvement in 4–8 weeks. Lung function improvement begins in 1–2 weeks and Lung function improvement begins in 1–2 weeks and usually plateaus at 4 weeks but may increase slightly usually plateaus at 4 weeks but may increase slightly thereafter for 6–8 weeks. Improvement in bronchial thereafter for 6–8 weeks. Improvement in bronchial hyperresponsiveness requires 2–3 weeks and approaches hyperresponsiveness requires 2–3 weeks and approaches maximum in 1–3 months but may continue to improve maximum in 1–3 months but may continue to improve over 1 yearover 1 year

Inhaled CorticosteroidsInhaled Corticosteroids
Many patients with mild persistent asthma can be Many patients with mild persistent asthma can be effectively treated with effectively treated with once-daily ICS therapyonce-daily ICS therapy, usually , usually more effective given in the evening.more effective given in the evening.
Currently, mometasone is the only ICS with approved Currently, mometasone is the only ICS with approved US-FDA labeling to begin therapy once daily & US-FDA labeling to begin therapy once daily & BudesonideBudesonide has once-daily approved labeling once has once-daily approved labeling once control is established on twice-daily dosing. All other control is established on twice-daily dosing. All other ICSs are labeled for twice-daily dosing.ICSs are labeled for twice-daily dosing.
The newest ICS, ciclesonide (CIC), is used in Europe on The newest ICS, ciclesonide (CIC), is used in Europe on a once-daily basis in adults and children, but only has a a once-daily basis in adults and children, but only has a twice-daily approved indication in adults in the United twice-daily approved indication in adults in the United States. The US pivotal trials for CIC in children 4–11 States. The US pivotal trials for CIC in children 4–11 years old with moderate-to-severe asthma gave once-years old with moderate-to-severe asthma gave once-daily dosing of 40, 80, & 160 μg.daily dosing of 40, 80, & 160 μg.
Current Opinion in Allergy & Clinical Immunology 2011;11(4):337-344

Common MDI PreparationsCommon MDI Preparations
Drug: Drug: NebulizedNebulized
AvailabilityAvailability DoseDose
SalbutamolSalbutamol Asthalin solAsthalin soln n 5 mg/mL, 5 mg/mL, respule 2.5 mg/2.5 mLrespule 2.5 mg/2.5 mL
0.15 mg/kg (Min 2.5 mg) as often as 20 0.15 mg/kg (Min 2.5 mg) as often as 20 min min × 3, then 0.15-0.3 mg/kg up to 10 mg × 3, then 0.15-0.3 mg/kg up to 10 mg q1-4h PRN, or up to 0.5 mg/kg/hr by q1-4h PRN, or up to 0.5 mg/kg/hr by continuous nebulizationcontinuous nebulization
LevosalbutaLevosalbutamolmol
0.31 mg, 0.63 mg, 1.25 0.31 mg, 0.63 mg, 1.25 mg/2.5 mL Respules mg/2.5 mL Respules Levolin / AerozestLevolin / Aerozest
0.075 mg/kg (Min 1.25 mg) q20 min 0.075 mg/kg (Min 1.25 mg) q20 min × 3, × 3, then 0.075 – 0.15 mg/kg up to 5 mg q1-4 h then 0.075 – 0.15 mg/kg up to 5 mg q1-4 h PRN, or 0.25 mg/kg/hr continuous PRN, or 0.25 mg/kg/hr continuous nebulization. 0.63 mg = 1.25 mg nebulization. 0.63 mg = 1.25 mg salbutamol for both efficacy & SEsalbutamol for both efficacy & SE
BudesonideBudesonide Respule 0.5 mg/2 mL, Respule 0.5 mg/2 mL, 1 mg/2 mL1 mg/2 mLMDI Bunase 100/200MDI Bunase 100/200
Initiating dose 0.5-1 mg BD, Maintenance Initiating dose 0.5-1 mg BD, Maintenance 0.25-0.5 mg BD0.25-0.5 mg BD
FluticasoneFluticasone 0.5 mg/2 mL, 2 mg/2 0.5 mg/2 mL, 2 mg/2 mLmL
1 mg BD1 mg BD
IpratropiumIpratropium Neb respirator Neb respirator solutionsolution0.25 mg/ml, Respule0.25 mg/ml, Respule0.5 mg/2 mL0.5 mg/2 mL
0.5 ml < 1 year, 1 ml >1 year every 20 mins 0.5 ml < 1 year, 1 ml >1 year every 20 mins for 3 doses, then every 6-8 hours solutionfor 3 doses, then every 6-8 hours solution

Common MDI PreparationsCommon MDI Preparations
DrugDrug AvailabilityAvailability DoseDose
SalbutamolSalbutamol Asthalin /Ventorlin Asthalin /Ventorlin MDI 100 MDI 100 µg/dose µg/dose (DPI 200 µg/dose)(DPI 200 µg/dose)
4-8 puff every 20 min 4-8 puff every 20 min × 3, then q1-4h. × 3, then q1-4h. Maintenance 1-2 puff q4-6hMaintenance 1-2 puff q4-6hAdults: 4-8 puffs every 20 min fo up to 4 Adults: 4-8 puffs every 20 min fo up to 4 hrs, then same.hrs, then same.Before exercise 1-2 puff 5 min before.Before exercise 1-2 puff 5 min before.
LevosalbutaLevosalbutamolmol
Levolin/ Aerozest 50 Levolin/ Aerozest 50 µg (DPI 100 µg)µg (DPI 100 µg)
Same puffs as above.Same puffs as above.
BudesonideBudesonide Budecort/Pulmicort Budecort/Pulmicort MDI 100/200 MDI 100/200 µg/dose µg/dose (DPI 100/200/400)(DPI 100/200/400)
FluticasoneFluticasone Flohale MDI Flohale MDI 25/50/125 25/50/125 µg/dose µg/dose (DPI 50/100/250 )(DPI 50/100/250 )
IpratropiumIpratropium Ipravent MDI 20 Ipravent MDI 20 µg/dose (DPI 40)µg/dose (DPI 40)
TiotropiumTiotropium MDI Aerotrop MDI Aerotrop µg µg (DPI 18µg )(DPI 18µg )

Common MDI PreparationsCommon MDI Preparations
DrugDrug AvailabilityAvailability DoseDose
Salmeterol + Salmeterol + FluticasoneFluticasoneS 25S 25µg + F 50/125/250µg + F 50/125/250
Seroflo & Flutrol Seroflo & Flutrol 50/125/250 50/125/250 (Macleods)(Macleods)
Seretide Evohaler Seretide Evohaler 50/125/250 (gsk)50/125/250 (gsk)
>4 yrs: 2 puffs of 50 >4 yrs: 2 puffs of 50 µg BD (up to µg BD (up to 100 BD)100 BD)
Formoterol + Formoterol + BudesonideBudesonideF 6F 6µg + B 100/200/400µg + B 100/200/400
Foracort 100/200/400Foracort 100/200/400
Budetrol 100/200/ 400 Budetrol 100/200/ 400 (Macloeds)(Macloeds)
Vent-FBVent-FB
For For maintenance & reliefmaintenance & relief!!
Formoterol + Formoterol + FluticasoneFluticasone
Flucort-F 125/250Flucort-F 125/250
Tiotropium + Tiotropium + FormoterolFormoterol
MDI Aerotrop-F (9 + 6 MDI Aerotrop-F (9 + 6 µg respectivelyµg respectively) DPI) DPI

Indications for ReferralIndications for ReferralThe The majoritymajority of asthmatics can be managed optimally in of asthmatics can be managed optimally in a a primary health care facilityprimary health care facility, provided the elements of , provided the elements of the asthma guidelines are followed.the asthma guidelines are followed.
ReferralReferral to a specialist is to a specialist is recommended ifrecommended if the goals of the goals of management are not achieved, or for following reasons:management are not achieved, or for following reasons:diagnosis in doubtdiagnosis in doubtunstable asthmaunstable asthmaparents or general practitioners need further supportparents or general practitioners need further supportchild on high dose ICS (>400 µg beclomethasone child on high dose ICS (>400 µg beclomethasone equivalent per day)equivalent per day)oral steroids are required regularlyoral steroids are required regularlyafter a life-threatening episodeafter a life-threatening episodefrequent hospitalizations or visits to an emergency frequent hospitalizations or visits to an emergency roomroom
http://www.pulmonology.co.za/guidelines/asthma%20paed.htm

Inhalational therapy remains the mainstay of Inhalational therapy remains the mainstay of treatment for asthma in children treatment for asthma in children (Preventers)(Preventers)
Medications can be safely and effectively Medications can be safely and effectively delivered to children at any age via MDI + delivered to children at any age via MDI + spacerspacer
Patient instruction is a key component in Patient instruction is a key component in determining the device; that a patient can determining the device; that a patient can use correctly & in teaching the patient how use correctly & in teaching the patient how to properly use the deviceto properly use the device
Take Home PointsTake Home Points

Thank you for your time & Thank you for your time & attention!attention!