Impact of POM + LoDEX on Disease Parameters and ...static9.light-kr.com/documents/IMW2013/Richardson...
20
Impact of POM + LoDEX on Disease Parameters and Cytogenetic Status in Relapsed and Refractory Multiple Myeloma (RRMM) Paul G. Richardson 1 , Sagar Lonial 2 , Andrzej Jakubowiak 3 , Rachid Baz 4 , Nizar Bahlis 5 , David S. Siegel 6 , Christine Chen 7 , Andrew Belch 8 , Martha Lacy 9 , Min Chen 10 , Mohamed H. Zaki 10 , Kenneth C. Anderson 1 1 Dana-Farber Cancer Institute, Boston, MA, USA; 2 Emory University School of Medicine, Atlanta, GA, USA; 3 University of Chicago Medical Center, Chicago, IL, USA; 4 H. Lee Moffitt Cancer Center and Research Institute, Tampa, FL, USA; 5 Southern Alberta Cancer Research Institute, University of Calgary, Calgary, AB, Canada; 6 John Theurer Cancer Center, Hackensack University Medical Center, Hackensack, NJ, USA; 7 Princess Margaret Hospital, Toronto, ON, Canada; 8 University of Alberta, Edmonton, AL, Canada; 9 Mayo Clinic, Rochester, MN, USA; 10 Celgene Corporation, Summit, NJ, USA
Transcript of Impact of POM + LoDEX on Disease Parameters and ...static9.light-kr.com/documents/IMW2013/Richardson...

Impact of POM + LoDEX on Disease Parameters and Cytogenetic Status in Relapsed and
Refractory Multiple Myeloma (RRMM)
Paul G. Richardson 1, Sagar Lonial 2, Andrzej Jakubowiak 3, Rachid Baz 4, Nizar Bahlis 5, David S.
Siegel 6, Christine Chen 7, Andrew Belch 8, Martha Lacy 9, Min Chen 10, Mohamed H. Zaki 10, Kenneth C. Anderson 1
1Dana-Farber Cancer Institute, Boston, MA, USA; 2Emory University School of Medicine, Atlanta, GA, USA; 3University of Chicago Medical Center, Chicago, IL, USA; 4H. Lee Moffitt Cancer Center and Research Institute,
Tampa, FL, USA; 5Southern Alberta Cancer Research Institute, University of Calgary, Calgary, AB, Canada; 6John Theurer Cancer Center, Hackensack University Medical Center, Hackensack, NJ, USA; 7Princess Margaret
Hospital, Toronto, ON, Canada; 8University of Alberta, Edmonton, AL, Canada; 9Mayo Clinic, Rochester, MN, USA; 10Celgene Corporation, Summit, NJ, USA

Disclosures
• Consultancy: Celgene, Millennium, Novartis, Bristol-Myers Squibb, Onyx, Merck

Background
• In patients with MM, clinical parameters and certain cytogenetic abnormalities are associated with poor prognosis1,2
• The MM-002 phase 2 study showed that POM is effectiveand well tolerated in RRMM patients3
• We assessed the impact of high-risk cytogenetics on the efficacy of POM + LoDEX:
– High-risk cytogenetic profile included Del(17p13) and/or t(4p16/14q32)
– Data cutoff was March 30, 2012
LoDEX, low-dose dexamethasone; MM, multiple myeloma ; POM, pomalidomide; RRMM, relapsed and refractory m ultiple myeloma.1. Kumar SK, et al. Mayo Clin Proc. 2004;79:867-74. 2. Avet-Loiseau H, et al. J Clin Oncol. 2012;30:194 9-52. 3. Richardson PG, et al. Blood. 2011;118:abstr act 634.
Richardson PG, et al. IMW 2013;Abstract 369.

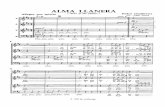
• Aspirin (80–100 mg) or equivalent was mandated for all patients• Patients aged > 75 yrs had a starting DEX dose of 2 0 mg/week
Ran
dom
izat
ion
N =
221
Option to add LoDEX
(40 mg/week) a
Discontinue and follow -up for survival
and subsequent treatment
Progressive disease
Progressive disease
POM (4 mg days 1–21 of each 28-day cycle)
+ LoDEX (40 mg/week)N = 113
POM (4 mg days 1–21 of each 28-day cycle)
N = 108
DEX, dexamethasone; DOR, duration of response; LoDEX , low-dose DEX; ORR, overall response rate; OS, overa ll survival; PFS, progression-free survival; POM, pomalidomide.1. Bladé J, et al. Br J Haematol. 1998;102:1115-23. 2. Richardson PG, et al. N Engl J Med. 2003;348:2609 -17.
Richardson PG, et al. IMW 2013;Abstract 369.
Progressive disease
• Primary end point : PFS• Secondary end points : ORR1,2, DOR, OS, and safety
MM-002: Study Design

MM-002: Key Eligibility Criteria
• Aged ≥ 18 years
• Patients with RRMM:– Measurable levels of M-protein in serum or urine
– Serum creatinine ≤ 3.0 mg/dL
– ≥ 2 prior therapies
– Prior therapy must have included ≥ 2 cycles of LEN and ≥ 2 cycles of BORT separately or in combination
– Documented progression ≤ 60 days after the last treatment (refractory disease)
BORT, bortezomib; LEN, lenalidomide; RRMM, relapsed/ refractory multiple myeloma.
Richardson PG, et al. IMW 2013;Abstract 369.

MM-002: Baseline Characteristics
Patient characteristicsPOM + LoDEX
(n = 113)POM
(n = 108)
Median age, years (range) 64 (34–88) 61 (37–88)
Male (%) 55 53
Durie-Salmon MM stage ≥ II (%) 93 93
ECOG performance status score (%)
0–1 88 88
2–3 12 12
Cytogenetic profile, n (%)
High-risk a 30 (27) 30 (28)
Del(17p13) 19 (17) 11 (10)
Standard-risk 57 (50) 43 (40)
a High-risk cytogenetic profile defined as those with abnormalities del(17p13) and/or t(4p16/14q32).ECOG, Eastern Cooperative Oncology Group; LoDEX, low-do se dexamethasone; MM, multiple myeloma; POM, pomalid omide.
Richardson PG, et al. IMW 2013;Abstract 369.

MM-002: Prior Therapy
Type of prior therapyPOM + LoDEX
(n = 113)POM
(n = 108)
Median number of prior therapies (range) 5 (2–13) 5 ( 1–12)
LEN / BORT / steroids (%) 100 100
LEN as last prior therapy (%) 39 31
BORT as last prior therapy (%) 50 47
Alkylators (%) 93 95
Stem cell transplantation (%) 73 76
Thalidomide (%) 67 67
Anthracyclines (%) 49 50
BORT, bortezomib; LEN, lenalidomide; LoDEX, low-dose dexamethasone; POM, pomalidomide.
Richardson PG, et al. IMW 2013;Abstract 369.

Discrepancies in totals are due to rounding. aResponse rate by investigator (based on best respon se assessment using EBMT criteria). bLoDEX was added in 64 patients (59%).cFor patients who achieved ≥ PR, efficacy evaluable population.CR, complete response; EBMT, European Group for Bloo d and Marrow Transplantation; ITT, intent-to-treat; LoDEX, low-dose dexamethasone; MR, minor response; ORR, overall response rate; PD, progressive disease; POM, pomalidomide; PR, partial response; SD, stable disease.
Richardson PG, et al. IMW 2013;Abstract 369.
• Median number of cycles received was 5 (range 1–28)
• Disease control ( ≥ SD) was observed in 81% of patients
Response a POM + LoDEX (n = 113)
POM (n = 108)b
ORR (≥ PR) (%) 34 15≥ MR (%) 45 31
CR 3 1PR 31 14MR 12 16
SD (%) 37 48PD (%) 6 10Median time to ORR c, months 1.9 3.7
MM-002: Best Response (EBMT Criteria) ITT Population

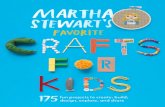
Median PFS (mos)
POM + LoDEX (n = 113) 4.6
POM (n = 108)a 2.6
aLoDEX was added in 64 patients (59%).DOR, duration of response; HR, hazard ratio; ITT, in tent-to-treat; LoDEX, low-dose dexamethasone; PFS, progression-free survival; POM, pomalidomide.
Richardson PG, et al. IMW 2013;Abstract 369.
HR = 0.67P = 0.002
0
20
40
60
80
100
0 5 10 15 20 25 30
Pat
ient
s (%
)
PFS (months) DOR (months)
0
HR = 0.89P = 0.734
20
40
60
80
100
0 5 10 15 20 25
Pat
ient
s (%
)
Median DOR (mos)
POM + LoDEX (n = 38) 8.3
POM (n = 16) 8.8
MM-002: PFS and DORITT Population

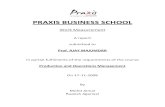
Median OS (mos)
POM + LoDEX (n = 113) 16.5
POM (n = 108)a 13.6
HR = 0.92P = 0.609
0
20
40
60
80
100
0 5 10 15 20 25 30
Pat
ient
s (%
)
OS (months)
aLoDEX was added in 64 patients (59%).DEX, dexamethasone; HR, hazard ratio; ITT, intent-t o-treat; LoDEX, low-dose DEX; OS, overall survival; POM, pomalidomide.
Richardson PG, et al. IMW 2013;Abstract 369.
• The OS of the POM alone arm includes 59% of patients who added LoDEX upon disease progression
MM-002: OS ITT Population

Grade 3–4 AEs of special interest (%)POM + LoDEX
(n = 112)POM
(n = 107)
HematologicNeutropenia 41 47Anemia 22 24Thrombocytopenia 19 22Leukopenia 10 7
Non-hematologicPneumonia 22 14Fatigue 14 11Dyspnea 13 8
AE, adverse event; DVT, deep-vein thrombosis; LoDEX , low-dose dexamethasone; POM, pomalidomide.
Richardson PG, et al. IMW 2013;Abstract 369.
MM-002: AEs All Patients Treated

MM-002: Baseline Characteristics by Cytogenetic Risk POM + LoDEX
a High-risk cytogenetic profile defined as those with abnormalities Del(17p13) and/or t(4p16/14q32).BORT, bortezomib; ECOG, Eastern Cooperative Oncology Gr oup ; LEN, lenalidomide; LoDEX, low-dose dexamethas one; MM, multiple myeloma; POM, pomalidomide; THAL, thalidomide.
Richardson PG, et al. IMW 2013;Abstract 369.
Patient characteristicsPOM + LoDEX
High-risk a
(n = 30)
POM + LoDEX Standard-risk
(n = 57)
Median age, years (range) 64 (52–88) 64 (34–83)
Male (%) 47 58
Durie-Salmon MM stage ≥ II (%) 93 91
ECOG Performance status score (%)
0–1 90 88
2–3 10 12
Median no. of prior therapies (range) 5 (3–11) 5 (2–1 2)
Prior LEN / BORT 100 100
Prior THAL 70 67

MM-002: Efficacy by Cytogenetic Risk POM + LoDEX
a For patients who achieved ≥ PR.CI, confidence interval; DOR, duration of response; LoDEX, low-dose dexamethasone; NR, not reached; ORR , overall response rate; OS, overall survival; PFS, progression-free survival; POM, pomalidomide; PR, pa rtial response; TTR, time to response.
Richardson PG, et al. IMW 2013;Abstract 369.
Efficacy outcomesPOM + LoDEX
High-risk(n = 30)
POM + LoDEX Standard-risk
(n = 57)
ORR (≥ PR), % (n) 23 (7) 40 (23)
TTRa, months (range) 1.2 (0.9–2.8) 1.9 (0.9–14.4)
DORa, months (95% CI) 4.9 (1.9–13.1) 10.1 (7.7–NR)
Median PFS, months (95% CI) 3.1 (1.9–3.9) 5.5 (3.7–8. 7)
Median OS, months (95% CI) 13.2 (4.7–19.8) 21.7 (12.4 –NR)
• Among patients with del(17p13), ORR was 21%

AE, adverse event; LoDEX, low-dose dexamethasone; P OM, pomalidomide.
Richardson PG, et al. IMW 2013;Abstract 369.
Grade 3–4 AEs of special interest (%)POM + LoDEX
High-risk (n = 29)
POM + LoDEX Standard-risk
(n = 57)
Hematologic
Neutropenia 48 40
Thrombocytopenia 31 16
Anemia 24 25
Non-hematologic
Pneumonia 21 28
Fatigue 10 18
Dyspnea 17 11
MM-002: AEs by Cytogenetic RiskPOM + LoDEX (All Patients Treated)

a Median values at cycle 8.b Number of patients with abnormal baseline values us ed to calculate percentages. c Normal values were 150–350 × 10 3/mm3, 8.3–10.6 mg/dL, and 0.9–1.5 mg/dL respectively.LoDEX, low-dose dexamethasone; POM, pomalidomide.
Richardson PG, et al. IMW 2013;Abstract 369.
Platelet count n = 50b,c
Serum calciumn = 15b,c
Serum creatininen = 36b,c
205.5 × 103/mm3,a
9 mg/dLa
1 mg/dLa
MM-002: Demonstration of Clinical BenefitPOM + LoDEX
Pat
ient
s (%
)

Pat
ient
s (%
)
Hemoglobin improvement a
≥ 1 g/dLAlbumin improvement a
≥ 0.5 g/dL
aAll the patients in the POM + LoDEX safety populatio n (n = 112) were evaluated to calculate percentages .LoDEX, low-dose dexamethasone; POM, pomalidomide.
Richardson PG, et al. IMW 2013;Abstract 369.
MM-002: Demonstration of Clinical BenefitPOM + LoDEX (All Patients Treated)

ECOG, Eastern Cooperative Oncology Group; LoDEX, low-do se dexamethasone; POM, pomalidomide.
Richardson PG, et al. IMW 2013;Abstract 369.
MM-002: ECOG Changes from BaselinePOM + LoDEX

• POM is currently approved by the US FDA for the treatment of RRMM patients with ≥ 2 prior therapies, including LEN and BORT, and who have demonstrated PD ≤ 60 days after their last therapy
• POM + LoDEX shows efficacy in RRMM patients with high-ri sk cytogenetics, including patients with Del(17p13)
• Overall efficacy and safety findings are associated wi th a consistent improvement in critical end-organ functional parameters
• The efficacy and safety data strongly favor future combi nation strategies, including proteasome inhibitors and other nov el agents, especially in high-risk RRMM patients
BORT, bortezomib; FDA, Food and Drug Administration; LEN, lenalidomide; LoDEX, low-dose dexamethasone; PD, progressive disease; POM, pomalidomide; RRMM, relapsed refractory multiple myeloma.
Richardson PG, et al. IMW 2013;Abstract 369.
MM-002: Conclusions & Future Directions

Phase 2 Investigators Including:Ravi Vij, Craig Hofmeister, Sundar Jagannath, Kevin Song, Noopur Raje, Joseph Mikhael,
Asher Alban A. Chanan-Khan, Suzanne Lentzsch, Jeffr ey Matous, Chaim Shustik
Our Patients and Their Families
Institutions With Study Sites
• Dana-Farber Cancer Institute
• John Theurer Cancer Center – Hackensack University Medical Center
• Washington University School of Medicine
• The Ohio State University – James Cancer Hospital
• H. Lee Mofitt Cancer and Research Institute
• Mount Sinai Medical Center
• Princess Margaret Hospital – UHN
• Cross Cancer Institute
• Emory University Hospital
• Multiple Myeloma Research Consortium
• University of Michigan, Comprehensive Cancer Center
• University of Calgary – Tom Baker Cancer Center
• Vancouver General Hospital, Diamond Health Care Centre
• Massachusetts General Hospital
• Royal Victoria Hospital – McGill University of Pittsburgh Cancer Institute
• Mayo Clinic Minnesota
• Mayo Clinic Arizona
• Rocky Mountain Cancer Centers
• St. Vincent’s Comprehensive Cancer Center
Medical writing assistance: Supported by Celgene Corpo ration and provided by Anna Georgieva, PhD, and Eva Polk, PhD (Excerpta M edica)
Acknowledgments

Thank you!Arigat ō!
ありがとうありがとうありがとうありがとう
谢谢谢谢谢谢谢谢 ขอขอบคุณคุณ