Human endometriosis is associated with plasma cells and ... · Human endometriosis is associated...
6
Human endometriosis is associated with plasma cells and overexpression of B lymphocyte stimulator Aniko Hever*, Richard B. Roth*, Peter Hevezi*, Maria E. Marin † , Jose A. Acosta † , Hector Acosta † , Jose Rojas † , Rosa Herrera † , Dimitri Grigoriadis*, Evan White*, Paul J. Conlon*, Richard A. Maki*, and Albert Zlotnik* ‡ *Neurocrine Biosciences, Department of Discovery Biology, San Diego, CA 92130; and † School of Medicine, University of Baja California, 21100 Mexicali, Baja California, Mexico Communicated by Philippa Marrack, National Jewish Medical and Research Center, Denver, CO, May 11, 2007 (received for review July 8, 2006) Endometriosis affects 10 –20% of women of reproductive age and is associated with pelvic pain and infertility, and its pathogenesis is not well understood. We used genomewide transcriptional profiling to characterize endometriosis and found that it exhibits a gene expression signature consistent with an underlying auto- immune mechanism. Endometriosis lesions are characterized by the presence of abundant plasma cells, many of which produce IgM, and macrophages that produce BLyS/BAFF/TNFSF13B, a mem- ber of the TNF superfamily implicated in other autoimmune dis- eases. B lymphocyte stimulator (BLyS) protein was found elevated in the serum of endometriosis patients. These observations sug- gest a model for the pathology of endometriosis where BLyS- responsive plasma cells interact with retrograde menstrual tissues to give rise to endometriosis lesions. autoimmunity cytokines microarrays E ndometriosis, adenomyosis, and uterine fibroids (leiomyo- mata) represent the most common benign gynecological diseases of women of reproductive age and are collectively responsible for significant morbidity. Affecting an estimated 10–20% of women in this age group (1), endometriosis is associated with pain and other discomforts and may play a role in infertility (2, 3). Despite its high prevalence, the underlying mechanism of endometriosis is still poorly understood. Diagno- sis of endometriosis is also difficult, relying primarily on symp- tomatology (i.e., dysmenorrhea or painful menstruation), with laparoscopic examination being the only definitive confirmation. Because the latter is a surgical procedure, the diagnosis and subsequent treatment of endometriosis are often delayed (4). Treatment options for endometriosis include surgery and/or suppression of ovarian steroids (5). However, these strategies may offer only temporary relief because the disease usually recurs (6). Endometriosis may be confused with other gyneco- logical disorders, such as adenomyosis or uterine fibroids. In endometriosis, endometrial tissue is found outside the uterus. In adenomyosis, the endometrium grows abnormally into the myo- metrium, while uterine fibroids are pathological outgrowths of the myometrium. The interrelationship of these diseases, if any, has not been well established (7). We have profiled endometri- osis at the molecular level by using genomewide genearrays. Our results indicate that endometriosis, in contrast to adenomyosis or leiomyomas, exhibits a unique molecular signature that reveals underlying immune system-associated pathology. Results Endometriosis Exhibits a Unique Gene Expression Pattern Character- ized by Underlying Immunological Pathways. We sought to under- stand endometriosis at the molecular level. Toward this end, we performed microarray analyses of these three diseases as well as control tissues (endometrium, myometrium, and ovary) by using the Affymetrix U133 Plus 2.0 genomewide gene array (Af- fymetrix, Santa Clara, CA). We compared ovarian endometriosis lesions with control endometrium obtained from the same patient at the same time to avoid detecting gene expression differences due to the menstrual cycle (8). Genes significantly up-regulated in endometriosis versus control endometrium were analyzed by using ingenuity pathway analysis (IPA) (9). This analysis determined that genes associated with immune re- sponses represent the most significant functional class in endo- metriosis, including 53 genes with altered expression that form two networks shown in Fig. 1. These genes are shown in supporting information (SI) Table 1. Network 1 identified genes associated with immune responses, cell-to-cell signaling/ interaction, and hematological system development/function; whereas Network 2 included genes associated with inf lammatory diseases, immune responses, and cellular movement. These results suggest that endometriosis has an immunological basis. SI Fig. 4 is a heat map indicating many genes up-regulated in endometriosis versus control endometrium. SI Table 2 lists the top 50 genes up-regulated in endometriosis versus normal en- dometrium. All these genes had false discovery rates of P 0.05 (Benjamini–Hochberg multiple testing correction), indicating that their induction in endometriosis was highly significant. Because all the endometriosis samples were ovarian, we also filtered out genes highly expressed in the ovary by using our database of gene expression that includes 93 female human tissues as described (10). We also compared endometriosis with uterine fibroids and adenomyosis (one-way ANOVA; P 0.00001) and observed that each of these diseases exhibits a discrete molecular signature of gene expression (SI Fig. 5). When adenomyosis or uterine fibroid-associated genes were analyzed by IPA, no immune response-associated pathways were detected (11). Endometriosis Gene Expression Pattern Indicates Presence of Plasma Cells and Activated Macrophages. The endometriosis-associated genes included several immunoglobulins, complement compo- nents, and cytokines such as PBEF (pre-B cell colony-enhancing factor) (12) and BlyS/BAFF/TNFSF13B (13). However, B cell markers like CD19, CD20, or the transcription factor PAX-5 were not detected in endometriosis lesions. The Ig switching mechanism involves the expression of activation-induced cyti- dine deaminase (14), which was not detected, indicating that there are few or no B cells undergoing Ig class switching in endometriosis lesions. Similarly, T cell-specific genes (T cell Author contributions: A.H. and R.B.R. contributed equally to this work; A.H., R.A.M., and A.Z. designed research; A.H., P.H., R.H., and E.W. performed research; J.A.A., H.A., and J.R. contributed new reagents/analytic tools; A.H., R.B.R., M.E.M., J.A.A., H.A., J.R., D.G., P.J.C., R.A.M., and A.Z. analyzed data; and A.H., R.A.M., and A.Z. wrote the paper. Conflict of interest statement: A.H., R.B.R., P.H., D.G., E.W., P.J.C., R.A.M., and A.Z. were employed by Neurocrine Biosciences and owned common stock of this company at the time this study was performed. Abbreviations: BlyS, B lymphocyte stimulator; IPA, ingenuity pathway analysis; SLE, sys- temic lupus erythematosus. ‡ To whom correspondence should be addressed. E-mail: [email protected]. This article contains supporting information online at www.pnas.org/cgi/content/full/ 0703451104/DC1. © 2007 by The National Academy of Sciences of the USA www.pnas.orgcgidoi10.1073pnas.0703451104 PNAS July 24, 2007 vol. 104 no. 30 12451–12456 IMMUNOLOGY
-
Upload
truongkhuong -
Category
Documents
-
view
216 -
download
0
Transcript of Human endometriosis is associated with plasma cells and ... · Human endometriosis is associated...

Human endometriosis is associated with plasma cellsand overexpression of B lymphocyte stimulatorAniko Hever*, Richard B. Roth*, Peter Hevezi*, Maria E. Marin†, Jose A. Acosta†, Hector Acosta†, Jose Rojas†,Rosa Herrera†, Dimitri Grigoriadis*, Evan White*, Paul J. Conlon*, Richard A. Maki*, and Albert Zlotnik*‡
*Neurocrine Biosciences, Department of Discovery Biology, San Diego, CA 92130; and †School of Medicine, University of Baja California,21100 Mexicali, Baja California, Mexico
Communicated by Philippa Marrack, National Jewish Medical and Research Center, Denver, CO, May 11, 2007 (received for review July 8, 2006)
Endometriosis affects 10–20% of women of reproductive age andis associated with pelvic pain and infertility, and its pathogenesisis not well understood. We used genomewide transcriptionalprofiling to characterize endometriosis and found that it exhibitsa gene expression signature consistent with an underlying auto-immune mechanism. Endometriosis lesions are characterized bythe presence of abundant plasma cells, many of which produceIgM, and macrophages that produce BLyS/BAFF/TNFSF13B, a mem-ber of the TNF superfamily implicated in other autoimmune dis-eases. B lymphocyte stimulator (BLyS) protein was found elevatedin the serum of endometriosis patients. These observations sug-gest a model for the pathology of endometriosis where BLyS-responsive plasma cells interact with retrograde menstrual tissuesto give rise to endometriosis lesions.
autoimmunity � cytokines � microarrays
Endometriosis, adenomyosis, and uterine fibroids (leiomyo-mata) represent the most common benign gynecological
diseases of women of reproductive age and are collectivelyresponsible for significant morbidity. Affecting an estimated10–20% of women in this age group (1), endometriosis isassociated with pain and other discomforts and may play a rolein infertility (2, 3). Despite its high prevalence, the underlyingmechanism of endometriosis is still poorly understood. Diagno-sis of endometriosis is also difficult, relying primarily on symp-tomatology (i.e., dysmenorrhea or painful menstruation), withlaparoscopic examination being the only definitive confirmation.Because the latter is a surgical procedure, the diagnosis andsubsequent treatment of endometriosis are often delayed (4).Treatment options for endometriosis include surgery and/orsuppression of ovarian steroids (5). However, these strategiesmay offer only temporary relief because the disease usuallyrecurs (6). Endometriosis may be confused with other gyneco-logical disorders, such as adenomyosis or uterine fibroids. Inendometriosis, endometrial tissue is found outside the uterus. Inadenomyosis, the endometrium grows abnormally into the myo-metrium, while uterine fibroids are pathological outgrowths ofthe myometrium. The interrelationship of these diseases, if any,has not been well established (7). We have profiled endometri-osis at the molecular level by using genomewide genearrays. Ourresults indicate that endometriosis, in contrast to adenomyosis orleiomyomas, exhibits a unique molecular signature that revealsunderlying immune system-associated pathology.
ResultsEndometriosis Exhibits a Unique Gene Expression Pattern Character-ized by Underlying Immunological Pathways. We sought to under-stand endometriosis at the molecular level. Toward this end, weperformed microarray analyses of these three diseases as well ascontrol tissues (endometrium, myometrium, and ovary) by usingthe Affymetrix U133 Plus 2.0 genomewide gene array (Af-fymetrix, Santa Clara, CA). We compared ovarian endometriosislesions with control endometrium obtained from the samepatient at the same time to avoid detecting gene expression
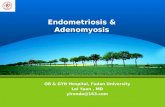
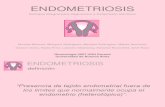
differences due to the menstrual cycle (8). Genes significantlyup-regulated in endometriosis versus control endometrium wereanalyzed by using ingenuity pathway analysis (IPA) (9). Thisanalysis determined that genes associated with immune re-sponses represent the most significant functional class in endo-metriosis, including 53 genes with altered expression that formtwo networks shown in Fig. 1. These genes are shown insupporting information (SI) Table 1. Network 1 identified genesassociated with immune responses, cell-to-cell signaling/interaction, and hematological system development/function;whereas Network 2 included genes associated with inflammatorydiseases, immune responses, and cellular movement. Theseresults suggest that endometriosis has an immunological basis.
SI Fig. 4 is a heat map indicating many genes up-regulated inendometriosis versus control endometrium. SI Table 2 lists thetop 50 genes up-regulated in endometriosis versus normal en-dometrium. All these genes had false discovery rates of P � 0.05(Benjamini–Hochberg multiple testing correction), indicatingthat their induction in endometriosis was highly significant.Because all the endometriosis samples were ovarian, we alsofiltered out genes highly expressed in the ovary by using ourdatabase of gene expression that includes 93 female humantissues as described (10). We also compared endometriosis withuterine fibroids and adenomyosis (one-way ANOVA; P �0.00001) and observed that each of these diseases exhibits adiscrete molecular signature of gene expression (SI Fig. 5).When adenomyosis or uterine fibroid-associated genes wereanalyzed by IPA, no immune response-associated pathways weredetected (11).
Endometriosis Gene Expression Pattern Indicates Presence of PlasmaCells and Activated Macrophages. The endometriosis-associatedgenes included several immunoglobulins, complement compo-nents, and cytokines such as PBEF (pre-B cell colony-enhancingfactor) (12) and BlyS/BAFF/TNFSF13B (13). However, B cellmarkers like CD19, CD20, or the transcription factor PAX-5were not detected in endometriosis lesions. The Ig switchingmechanism involves the expression of activation-induced cyti-dine deaminase (14), which was not detected, indicating thatthere are few or no B cells undergoing Ig class switching inendometriosis lesions. Similarly, T cell-specific genes (T cell
Author contributions: A.H. and R.B.R. contributed equally to this work; A.H., R.A.M., andA.Z. designed research; A.H., P.H., R.H., and E.W. performed research; J.A.A., H.A., and J.R.contributed new reagents/analytic tools; A.H., R.B.R., M.E.M., J.A.A., H.A., J.R., D.G., P.J.C.,R.A.M., and A.Z. analyzed data; and A.H., R.A.M., and A.Z. wrote the paper.
Conflict of interest statement: A.H., R.B.R., P.H., D.G., E.W., P.J.C., R.A.M., and A.Z. wereemployed by Neurocrine Biosciences and owned common stock of this company at the timethis study was performed.
Abbreviations: BlyS, B lymphocyte stimulator; IPA, ingenuity pathway analysis; SLE, sys-temic lupus erythematosus.
‡To whom correspondence should be addressed. E-mail: [email protected].
This article contains supporting information online at www.pnas.org/cgi/content/full/0703451104/DC1.
© 2007 by The National Academy of Sciences of the USA
www.pnas.org�cgi�doi�10.1073�pnas.0703451104 PNAS � July 24, 2007 � vol. 104 � no. 30 � 12451–12456
IMM
UN
OLO
GY

antigen receptor chains � and �, as well as CD3�) were notup-regulated in endometriosis. This paucity of mature B and Tcells was confirmed by immunohistochemistry, which revealedno CD20-positive cells and few CD3�-positive cells in the lesions(data not shown). Conversely, many genes associated withmacrophage activation were strongly up-regulated in endome-trial lesions such as CD163 (a macrophage scavenger receptorfor hemoglobin) (15), CD14 (lipopolysaccharide receptor) classII major histocompatibility complex molecules, and the intra-cellular adhesion molecule (ICAM-1) (SI Table 2). Last, noneutrophils were observed in the lesions.
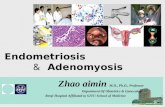
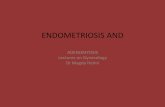
Histopathology of Endometriosis Lesions Confirmed Presence ofPlasma Cells and Macrophages. Tissue sections stained with H&Erevealed abundant plasma cells and macrophages (Fig. 2a) in theendometriosis lesions. Additional endometrial sections werestained with antibodies against IgM (Fig. 2b) (or �/� light chains,data not shown), revealing that �30% of the plasma cells wereproducing IgM. The rest of the plasma cells were likely producingIgG because we observed strong up-regulation of IgG mRNA(the gene array IgG data were unreliable, so we confirmed thisby PCR; data not shown), whereas no up-regulation of IgA orIgE mRNAs was detected. The presence of hemosiderin-containing macrophages was also evident in endometriosis le-sions (Fig. 2c). Staining for the macrophage-specific antigenCD68 (macrosialin/gp110) confirmed the presence of abundantmacrophages in endometriosis lesions (Fig. 2d). Histologicalexamination of control endometrium revealed no plasma cellswith few macrophages present. Thus, immunopathological ex-amination of endometriosis lesions confirmed the molecularresults, pointing to a strong presence of plasma cells (someproducing IgM) and activated macrophages.
Role for B Lymphocyte Stimulator (BlyS) in Endometriosis. Several ofthe cytokines up-regulated in endometriosis lesions are known to
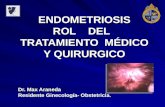
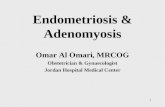
specifically activate B cells (16). BLyS was of particular interestbecause it was highly up-regulated, is a cytokine necessary fornormal B cell development, and also induces differentiation intoplasma cells (17). We confirmed that BLyS mRNA levels wereelevated in endometriosis lesions by real-time PCR (Fig. 3a).BLyS is capable of binding to three different receptors of theTNF superfamily (BAFF-R, TACI, and BCMA) (18). We ana-lyzed the expression of these receptors by real-time PCR. OnlyBCMA was strongly up-regulated in endometriosis lesions (Fig.3b). Interestingly, BCMA is expressed by plasma cells (19) andsupports their survival (18). These observations strongly suggestthat the BLyS/BCMA interaction supports the plasma cellsobserved in endometriosis (Fig. 2 a and b). Immunohistochem-ical staining revealed that the cells producing this cytokine weremacrophages present in the endometriosis lesions (Fig. 3c). Wethen measured BLyS protein in the sera of 31 endometriosispatients and found that its levels were significantly elevatedcompared to 21 healthy controls (Fig. 3d). Patients with adeno-myosis and uterine fibroids did not have elevated BLyS serumlevels compared to controls (data not shown). More important,BLyS levels are elevated in other autoimmune diseases, includ-ing rheumatoid arthritis, systemic lupus erythematosus (SLE),and Sjogren’s syndrome (20–23).
Complement System Is Altered in Endometriosis. Complement com-ponents were also strongly up-regulated in endometriosis lesions(Fig. 1 and SI Tables 1 and 2). The expression of some com-plement components fluctuates during the menstrual cycle, butthe levels observed in endometriosis are much higher than thoseinduced during the menstrual cycle (8). Several complementcomponents are produced by endometrial cells (24, 25), andchanges in complement levels have previously been reported tobe associated with endometriosis (26, 27). We measured theserum levels of C3, C4, C6, and C7 complement components inpatients with endometriosis, adenomyosis, and uterine fibroidscompared to normal controls. Although no changes in serum C4,C6, and C7 were observed between endometriosis patients andcontrols, serum levels of C3 were slightly reduced [endometriosis
Fig. 1. IPA was used to identify pathways altered in endometriosis comparedwith normal endometrium, and the two most significant networks associatedwith immune responses are shown (merged). The significance values of eachwere Network 1, P � 10�38, and Network 2, P � 10�26. For explanation ofsignificance values, see Materials and Methods.
Fig. 2. Endometriosis lesions contain macrophages and plasma cells. (a)Staining with H&E showing plasma cells in endometriosis lesions (arrows).(Magnification: �10.) (b) Immunohistochemical analysis shows that some ofthe plasma cells express IgM (arrows). (Magnification: �40.) (c) H&E stainingrevealed many macrophages with hemosiderin in the lesions of ovarianendometriosis. (Magnification: �10.) (d) Staining with anti-CD68 confirmedthe presence of macrophages in these lesions. (Magnification: �40.)
12452 � www.pnas.org�cgi�doi�10.1073�pnas.0703451104 Hever et al.

patients, 939 � 47 �g/ml; healthy controls, 1,352 � 23 �g/ml (n �26 and 11, respectively; P � 0.0001)]. Patients with adenomyosisor uterine fibroids had no significant changes in C3 levels. LowerC3 levels are consistent with findings from other autoimmunediseases, including SLE (28) as well as Sjogren’s syndrome (20).
Are There Atypical Plasma Cells in Endometriotic Lesions? Our resultsindicate that endometriosis lesions contain many activated mac-rophages and plasma cells with few or no mature B or T cells.Because typical B cell responses (those represented by B-2 cells)(29) require T cell help, these observations suggest that eitherthe development of these immune responses occurs elsewhere(and the plasma cells then migrate to the endometriotic lesions)or the plasma cells in endometriosis represent atypical B cellresponses similar to the B-1 or marginal zone cells that have beencharacterized in the mouse (29, 30). To further investigate this,we cloned and sequenced Ig � clones from the endometriosislesions and compared their sequences to Ig � clones amplifiedfrom tonsils (representing normal B-2 responses). As shown inSI Fig. 6 A and B, the IgM clones produced in endometriosislesions exhibit sharply reduced diversity when compared totonsil-derived IgMs (SI Tables 3 and 4), suggesting that theIgM-producing plasma cells in endometriosis lesions produce arestricted Ig repertoire.
DiscussionEndometriosis is a common gynecological disease affecting alarge number of reproductive age women. Treatment optionsinclude surgery (laparoscopy) as well as hormonal treatmenttargeting the GnRH receptor (1). Despite its high prevalence, itspathogenesis remains obscure. Although the exact origins ofendometriosis are unclear, a widely accepted model postulatesthat endometriosis originates when some endometrial tissue,which is normally eliminated with the menstrual f low, insteadundergoes retrograde flow (via the Fallopian tubes) to theovaries and peritoneum (5, 31). The endometrial tissues thendevelop into inflammatory foci that respond to hormonal cycles
and cause the symptoms associated with endometriosis. Previousendometriosis genomic studies focused on endometriosis-associated infertility (32), whereas another study identifiedCyr61 as an endometriosis-associated gene (33). The presentstudy represents the most comprehensive, genomewide analysisof ovarian endometriosis lesions to date. Given that endometri-osis is difficult to diagnose, we also compared endometriosis withadenomyosis and uterine fibroids, two other common gyneco-logical diseases that share symptoms with endometriosis. Ourresults indicate that these diseases can be readily differentiatedat the molecular level (SI Fig. 5), and that only endometriosisexhibits a gene expression signature reminiscent of other auto-immune disorders (Fig. 1 and SI Tables 1 and 2). It has beenpostulated that endometriosis has an autoimmune etiology (34),but the nature of this disorder has not been characterized.Patients with endometriosis have a higher incidence of autoan-tibodies of both IgM and IgG isotypes directed against phos-pholipids, histones, or DNA (35). Our molecular and patholog-ical analyses indicate that endometriosis lesions arecharacterized by the presence of abundant plasma cells andactivated macrophages. One of the most up-regulated cytokinesin these lesions is BLyS, a cytokine known to have importanteffects on B cells. Notably, BLyS has been shown to be criticalfor normal B-2 cell development (36), while high levels of BLySoverstimulate various B cell responses, leading to the initiationand exacerbation of autoimmune responses. Indeed, BLyS over-expression (using transgenic mice) has been shown to result inan autoimmune condition similar to SLE through the expansionof a population of B-1-related lymphocytes (29, 30). We shouldnote that the activation of macrophages present in endometriosislesions likely involves specific signals. For example, althoughmacrophages were found to produce BLyS, other genes like IL1or TNF� (present in diseases like SLE) (37), were not up-regulated, suggesting that endometriosis lesions represent aunique microenvironment.
B cell responses have been subdivided into thymus-independent (B1-like and related subsets) and thymus-
Fig. 3. BLyS and its receptor BCMA are significantly altered in endometriosis. (a) Qualitative RT-PCR (TaqMan) confirmed the overexpression of BLyS mRNAin endometriosis vs. control endometrium, as originally identified through microarray analysis. Relative expression values are expressed as mean of2(40�Ct) � SEM: endometrium, 100 � 15 (n � 16); endometriosis, 886 � 263 (n � 13). (b) BCMA mRNA was also found to be overexpressed in endometriosisvs. control endometrium by quantitative RT-PCR (TaqMan). Relative expression values are expressed as mean of 2(40�Ct) � SEM: endometrium, 43 � 13 (n �16); endometriosis, 290 � 89 (n � 13). (c) Immunohistochemical staining revealed that BlyS is produced by macrophages in endometriotic lesions.(Magnification: �100.) (d) Individual serum BlyS protein levels in 21 healthy control females and 31 patients with endometriosis were measured by ELISA.The data show the mean pg/ml values of each group � SEM: control, 523 � 74; endometriosis, 1,695 � 188.
Hever et al. PNAS � July 24, 2007 � vol. 104 � no. 30 � 12453
IMM
UN
OLO
GY

dependent (B2) responses. B1 and related cells may not requireT cell help to make antibodies, producing primarily IgM withsome IgG3 (29, 30). B1 cells typically recognize antigens thatinduce multivalent cross-linking of the B cell receptor. Theirrepertoire is likely selected by self-antigens, making them po-tentially autoreactive. In the mouse, B1 cells primarily reside inthe peritoneum, where they have been shown to be essential forresistance to certain pathogens and play an important role inmucosal immunity (38). B-1 cells are also known to exist in thehuman body and to produce autoreactive antibodies (38). Forexample, in arthritis, B1 cells make antibodies to self-antigens(i.e., DNA), which are involved in the disease process (39). Theperitoneal location of B1-like cells is ideal for them to interactwith retrograde menstrual tissues and to be involved in thepathogenesis of endometriosis (29, 30). The production oflimited repertoire IgM (SI Fig. 6 A and B) by endometriosis-associated plasma cells suggests that some of these may derivefrom atypical B cells. This hypothesis is also consistent with otherclinical findings of endometriosis, including the presence ofautoantibodies against endometrial antigens (29, 30).
Other characteristics of endometriosis, like its recurring na-ture, are suggestive of autoimmunity. Furthermore, epidemio-logical studies have already documented a higher incidence ofother autoimmune diseases among endometriosis patients (40).
Taken together, our results suggest the following model for thepathogenesis of endometriosis: The disease commences whenmenstrual tissue fails to exit the body and instead travels backthrough the fallopian tubes to the ovaries and/or peritonealcavity (retrograde menstruation). These tissues then interactwith B cells found in the peritoneal cavity (41). These cells likelyinclude the precursors of the plasma cells we have detected inendometriosis lesions. BlyS production may be of particularimportance for the plasma cells to develop and for the diseaseto become established. The fact that only BCMA mRNA isup-regulated in endometriosis lesions, along with the knownbiology of this receptor (18), strongly suggests that BLyS medi-ates the survival and activation of plasma cells through thisreceptor (35). This model predicts that neutralization of BLySmay have therapeutic effects in endometriosis.
Our results represent a significant advance in our understand-ing of the pathogenesis of endometriosis, but questions remain.First, it is unclear why only some women develop endometriosis,although retrograde menstrual f low likely occurs in most womenof reproductive age. Second, what is the connection betweendysmenorrhea and the plasma cells found in endometriosislesions? We should note that CD5� mouse B cells have beenreported to respond to estrogen by increased antibody produc-tion (42). Thus, it is important to know what happens to theplasma cells present in endometriosis lesions after hormonaltreatment (with GnRH agonists or antagonists). Finally, theplasma cells present in endometriosis lesions may representlineages related to B1, marginal zone, or other atypical B cellsubsets (29). The present study identified new directions that cannow be approached experimentally, and future studies shouldinvestigate the nature and role that the plasma cells and activatedmacrophages play in endometriosis.
Materials and MethodsHuman Samples. Ten ovarian endometriosis and 10 matchedcontrol endometrium from the same patients (follicular phase,n � 2; luteal phase, n � 8), 10 adenomyosis (follicular phase, n �2; luteal phase, n � 6; unknown phase, n � 2), and 10 uterinefibroid (leiomyoma) (follicular phase, n � 5; luteal phase, n �3; unknown phase, n � 1; postmenopausal, n � 1) samples wereobtained from Zoion Diagnostics (Hawthorne, NY). All donorswere Caucasian, were not taking medications, and had notreceived hormone therapy before surgery. All of the diseasedtissue samples were from discarded organs from scheduled
surgeries, following Institutional Review Board approvals andinformed consent. After removal, the samples were snap-frozenin liquid N2 and stored at �80°C. In addition to controlendometrium and ovary samples, our database of gene expres-sion (10) contains 93 tissues from five female donors. Flash-frozen tissue samples were obtained between 3 and 5 h post-mortem (Zoion Diagnostics).
RNA Extraction and Microarray Analysis. Total RNA was preparedfrom frozen samples by using TRIzol (43). Tissues were groundunder liquid nitrogen in a mortar and pestle, and the resultingpowder was solubilized in 1 ml of TRIzol (Invitrogen, Carlsbad,CA) in a FastPrep microfuge tube containing Lysing Matrix Dceramic beads. The RNA was subsequently isolated from theresulting TRIzol solution and further purified with an additionalRNeasy step (QIAGEN, Chatsworth, CA). Five micrograms oftotal RNA from each sample was used to direct cDNA synthesisby using a T7 oligo(dT)24 primer and PowerScript RT (BDClontech, Palo Alto, CA). After second-strand synthesis, double-stranded cDNA was used in a MEGAscript T7 RNA polymerasein vitro transcription reaction (Ambion, Austin, TX) containingbiotin-labeled ribonucleotides, CTP (Enzo Diagnostics, Farm-ingdale, NJ) and UTP (Roche, Indianapolis, IN). The biotin-ylated cRNA was fragmented and hybridized to the AffymetrixHuman Genome U133 Plus 2.0 gene array, stained with strepta-vidin phycoerythrin conjugate, and scanned in a GeneChipScanner 3000 as described in the Affymetrix technical manual.The data sets presented in this study have been deposited in theGEO database (accession no. GSE7305).
Statistical Analysis. All statistical analyses were performed byusing Genedata Expressionist Pro 2.0 software (Genedata,Basel, Switzerland). Raw data from Affymetrix U133 Plus 2.0 celfiles were uploaded to Expressionist Pro 2.0 and processed byusing robust multiarray analysis (44) and subsequently log-transformed. Ovarian endometriosis and control endometriumsamples were compared by using a two-sample paired t test witha significance threshold P value of 0.05. A Benjamini–Hochbergmultiple testing correction was applied with a false discovery ratethreshold of P � 0.05. Additionally, a fold-change filter wasapplied, with a minimum fold-change threshold of 2.0. Normalendometrium and ovary samples were also compared, withidentical thresholds for significance as described above. Toidentify probe sets significantly up-regulated in ovarianendometriosis compared to control endometrium, an additionalset of filters was applied because many probe sets were the resultof ovary tissue contamination in ovarian endometriosis samples.If a probe set was identified as differentially expressed betweennormal ovary and normal endometrium, indicating a nondisease-related difference in expression, it was removed from the ovarianendometriosis vs. control endometrium differentially regulatedlist of probe sets. In some instances, probe sets were not removedif (i) the fold-change ratios of endometriosis/control endome-trium and normal ovary/normal endometrium were of oppositesigns, or (ii) the fold-change ratios of endometriosis/controlendometrium and normal ovary/normal endometrium were atleast 3-fold different from one another. Endometriosis, adeno-myosis, and uterine fibroid samples were analyzed by using aone-way ANOVA (P � 0.00001) to identify significantly differ-entially regulated genes.
Ingenuity Pathway Analysis. The genes that were identified assignificantly up- or down-regulated in endometriosis vs. endo-metrium (two-sample paired t test, P � 0.01, filtered for ovary)were used for network and gene ontology analysis. Data setscontaining the Affymetrix probe set identifiers, fold changes,and P values were uploaded into IPA software (www.ingenuity-.com). The IPA program searches the Ingenuity Pathway Knowl-
12454 � www.pnas.org�cgi�doi�10.1073�pnas.0703451104 Hever et al.

edge Base for interactions (known from the literature) betweenthe uploaded genes and all other genes contained in the Inge-nuity Pathway Knowledge Base and generates a series of net-works. In addition, the program calculates a statistical score foreach network. The significance reflects the number of modu-lated genes represented in a given network and is calculated byusing Fisher’s exact test. A P value �0.01 is considered signif-icant.
Hierarchical Clustering. The robust multiarray analysis data set,including all ovarian endometriosis vs. control endometrium, orendometriosis vs. adenomyosis and uterine fibroids, was com-pared by using a paired t test (P � 0.05 plus 2-fold change) orone-way ANOVA (P � 0.00001), respectively. Clustering wasperformed by using GeneSpring GX 7.3 (Agilent Technologies,Palo Alto, CA) software by applying the standard correlationwith average linkage after per gene normalization.
Quantitative Real-Time PCR. Total RNAs from diseased or normalsamples were converted into single-stranded cDNAs by using thehigh-capacity cDNA Archive Kit (Applied Biosystems, FosterCity, CA) according to the manufacturer’s instructions. PCR wasperformed on the ABI PRISM 7900HT Sequence DetectionSystem in 384-well plates. TaqMan Universal PCR MasterMixand Assays-on-Demand Gene Expression probes (Applied Bio-systems) were used for the PCR step according to the manu-facturer’s instructions. Expression values obtained were cor-rected for loading by measuring 18S RNA relative expressionlevels and quantified by converting the cycle threshold (Ct) valueinto a numerical value by using the following formula: expressionvalue � 2(40�Ct).
IgM PCR and Sequence Analysis. Variable regions of IgM transcriptswere cloned from endometriosis and control tissues (tonsil) byusing SMART RACE cDNA amplification (Clontech, Moun-tain View, CA). 5�RACE-ready cDNA was prepared in atemplate-switching reaction using 500 ng of total RNA and theprotocol supplied by the manufacturer. Reverse primers specificfor IgM were: IGHM�1R 5�-TTCGTCTGTGCCCTGCAT-GACGTC and IGHM�2R 5�-AAGGCAGCAGCACCTGT-GAGGTG.
Next, 100 ng of RACE-ready cDNA was used in an initial30-cycle PCR using the manufacturer’s universal primer mix andthe 1R (outlying) gene-specific primers. The second 30-cycle
PCR contained one-tenth of the products from the first reactionand the nested primers (nested universal and gene-specific; 2R).Advantage 2 polymerase was used in both reactions. We havefound this proofreading polymerase to have a very low (�1mutation in 104 bases) error frequency. RACE products wereresolved by 1% low-melt agarose gel electrophoresis directlycloned into pCR2.1 TOPO (Invitrogen) and sequenced on bothstrands by using T3 and T7 primers.
Serum Samples from Endometriosis Patients. Serum samples werecollected from 31 patients confirmed to have endometriosis bylaparoscopy and before receiving any hormonal treatment (Lu-pron, etc.). Control samples were obtained from 21 age-matchedwomen who tested negative for routine clinical chemistry screen-ings and did not exhibit any symptoms of gynecological diseases.
Measurement of Serum Complement Factors. Individual serum com-plement components were measured in sera from patients byELISA (Abbott Laboratories, Chicago, IL) performed as per themanufacturer’s instructions.
Measurement of Serum BLyS. BLyS was measured by ELISA (R&DSystems, Minneapolis, MN) according to the manufacturer’sspecifications. The plates were read at an OD of 450 nm (witha correction wavelength set at 570 nm), and a standard curve wasgenerated by using recombinant human BLyS.
Immunohistochemistry. Paraffin-embedded sections were pro-cessed for epitope retrieval (heating under pressure). The sec-tions were stained with appropriate dilutions of antibodiesagainst human CD68 (clone 514H12; Serotec, Oxford, U.K.),polyclonal rabbit anti-human IgM (Dako, Glostrup, Denmark),or rat anti-human BLyS (ab16107; Abcam, Cambridge, MA).These antibodies were followed by appropriate anti-mouse,anti-rat, or anti-rabbit antibodies conjugated with biotin(CalTag, Burlingame, CA), followed by a streptavidin-biotin-peroxidase complex (Dako). The peroxidase was developed withdiaminobenzidine, and the stained slides were counterstainedwith hematoxylin and examined by microscopy.
We thank Dr. Leopoldo Santos for suggestions and critical review of themanuscript; Jerry Lee, Dorian Willhite, Anil Pahuta, and Xin-Jun Liufor technical support; and Drs. Hector Herrera, Wayne Muller, and JuanPablo Flores for help with the immunohistochemistry experiments.
1. Lebovic DI, Mueller MD, Taylor RN (2001) Fertil Steril 75:1–10.2. Giudice LC, Kao LC (2004) Lancet 364:1789–1799.3. Berkley KJ, Rapkin AJ, Papka RE (2005) Science 308:1587–1589.4. Brosens I, Puttemans P, Campo R, Gordts S, Brosens J (2003) Curr Opin Obstet
Gynecol 15:519–522.5. Valle RF, Sciarra JJ (2003) Ann NY Acad Sci 997:229–239.6. Frackiewicz EJ, Zarotsky V (2003) Expert Opin Pharmacother 4:67–82.7. Leyendecker G (2000) Hum Reprod 15:4–7.8. Talbi S, Hamilton AE, Vo KC, Tulac S, Overgaard MT, Dosiou C, Le Shay N,
Nezhat CN, Kempson R, Lessey BA, et al. (2006) Endocrinology 147:1097–1121.9. Calvano SE, Xiao W, Richards DR, Felciano RM, Baker HV, Cho RJ, Chen
RO, Brownstein BH, Cobb JP, Tschoeke SK, et al. (2005) Nature 437:1032–1037.
10. Lee J, Hever A, Willhite D, Zlotnik A, Hevezi P (2005) Faseb J 19:1356–1358.11. Hever A, Roth RB, Hevezi PA, Lee J, Willhite D, White EC, Marin EM,
Herrera R, Acosta HM, Acosta AJ, Zlotnik A (2006) Mol Hum Reprod12:737–748.
12. Samal B, Sun Y, Stearns G, Xie C, Suggs S, McNiece I (1994) Mol Cell Biol14:1431–1437.
13. Moore PA, Belvedere O, Orr A, Pieri K, LaFleur DW, Feng P, Soppet D,Charters M, Gentz R, Parmelee D, et al. (1999) Science 285:260–263.
14. Muramatsu M, Kinoshita K, Fagarasan S, Yamada S, Shinkai Y, Honjo T(2000) Cell 102:553–563.
15. Schaer DJ, Schaer CA, Buehler PW, Boykins RA, Schoedon G, Alayash AI,Schaffner A (2006) Blood 107:373–380.
16. Irvin BJ, Hanson CL, Smith LH, Daniels CK (2001) Exp Cell Res 265:73–79.
17. Schiemann B, Gommerman JL, Vora K, Cachero TG, Shulga-Morskaya S,Dobles M, Frew E, Scott ML (2001) Science 293:2111–2114.
18. O’Connor BP, Raman VS, Erickson LD, Cook WJ, Weaver LK, Ahonen C, LinLL, Mantchev GT, Bram RJ, Noelle RJ (2004) J Exp Med 199:91–98.
19. Tarte K, Zhan F, De Vos J, Klein B, Shaughnessy J, Jr (2003) Blood102:592–600.
20. Ramos-Casals M, Brito-Zeron P, Yague J, Akasbi M, Bautista R, Ruano M,Claver G, Gil V, Font J (2005) Rheumatology (Oxford) 44:89–94.
21. Zhang J, Roschke V, Baker KP, Wang Z, Alarcon GS, Fessler BJ, Bastian H,Kimberly RP, Zhou T (2001) J Immunol 166:6–10.
22. Stohl W, Metyas S, Tan SM, Cheema GS, Oamar B, Xu D, Roschke V, Wu Y,Baker KP, Hilbert DM (2003) Arthritis Rheum 48:3475–3486.
23. Groom J, Kalled SL, Cutler AH, Olson C, Woodcock SA, Schneider P,Tschopp J, Cachero TG, Batten M, Wheway J, et al. (2002) J Clin Invest109:59–68.
24. Isaacson KB, Coutifaris C, Garcia CR, Lyttle CR (1989) J Clin EndocrinolMetab 69:1003–1009.
25. Bischof P, Planas-Basset D, Meisser A, Campana A (1994) Hum Reprod9:1652–1659.
26. Tao XJ, Sayegh RA, Isaacson KB (1997) Fertil Steril 68:460–467.27. Vinatier D, Dufour P, Oosterlynck D (1996) Hum Reprod Update 2:371–384.28. Tsokos GC (2004) Arthritis Rheum 50:3404–3407.29. Herzenberg LA (2000) Immunol Rev 175:9–22.30. Lopes-Carvalho T, Kearney JF (2004) Immunol Rev 197:192–205.31. Vinatier D, Orazi G, Cosson M, Dufour P (2001) Eur J Obstet Gynecol Reprod
Biol 96:21–34.
Hever et al. PNAS � July 24, 2007 � vol. 104 � no. 30 � 12455
IMM
UN
OLO
GY

32. Kao LC, Germeyer A, Tulac S, Lobo S, Yang JP, Taylor RN, Osteen K, LesseyBA, Giudice LC (2003) Endocrinology 144:2870–2881.
33. Absenger Y, Hess-Stumpp H, Kreft B, Kratzschmar J, Haendler B, Schutze N,Regidor PA, Winterhager E (2004) Mol Hum Reprod 10:399–407.
34. Matarese G, De Placido G, Nikas Y, Alviggi C (2003) Trends Mol Med 9:223–228.35. Gleicher N, el-Roeiy A, Confino E, Friberg J (1987) Obstet Gynecol 70:115–122.36. Gross JA, Dillon SR, Mudri S, Johnston J, Littau A, Roque R, Rixon M, Schou
O, Foley KP, Haugen H, et al. (2001) Immunity 15:289–302.37. Rus V, Atamas SP, Shustova V, Luzina IG, Selaru F, Magder LS, Via CS (2002)
Clin Immunol 102:283–290.38. Berland R, Wortis HH (2002) Annu Rev Immunol 20:253–300.
39. Casali P, Burastero SE, Nakamura M, Inghirami G, Notkins AL (1987) Science236:77–81.
40. Sinaii N, Cleary SD, Ballweg ML, Nieman LK, Stratton P (2002) Hum Reprod17:2715–2724.
41. Nisitani S, Murakami M, Akamizu T, Okino T, Ohmori K, Mori T, ImamuraM, Honjo T (1997) Scand J Immunol 46:541–545.
42. Ansar Ahmed S, Dauphinee MJ, Montoya AI, Talal N (1989) J Immunol142:2647–2653.
43. Chomczynski P, Sacchi N (1987) Anal Biochem 162:156–159.44. Irizarry RA, Hobbs B, Collin F, Beazer-Barclay YD, Antonellis KJ, Scherf U,
Speed TP (2003) Biostatistics 4:249–264.
12456 � www.pnas.org�cgi�doi�10.1073�pnas.0703451104 Hever et al.