HMS Ganges HIA Report (final version) 2004
129
HMS Ganges Development Health Impact Assessment for Central Suffolk Primary Care Trust and Haylink Limited Undertaken by Salim Vohra, Sian Penner and Ben Cave
-
Upload
salim-vohra -
Category
Documents
-
view
113 -
download
5
Transcript of HMS Ganges HIA Report (final version) 2004

HMS Ganges Development Health Impact Assessment for Central Suffolk Primary Care Trust and Haylink Limited Undertaken by Salim Vohra, Sian Penner and Ben Cave

Front cover photographs courtesy of Shotley Peninsula Online - local community website - www.shotleypeninsula.org.uk Shotley Peninsula Online is a non-profit making site run by members of the community for the community. Lead Project Consultant: Dr. Salim Vohra Contact Details Seahorse IA Fl 2 24 Kings Avenue (Kings Court) Hounslow Middlesex TW3 4BL Mobile: 07 957 476 055 Tel/Fax: 020 8572 3608 Email: [email protected]

Executive Summary
Executive Summary
Haylink Ltd, who own the HMS Ganges site on the Shotley Peninsula, have proposed the
building of a mixed development that includes 500 houses of various types and a range of
commercial and community facilities. This report describes the potential positive and
negative health effects of the proposed development compared to leaving the site as it is. It
also outlines and assesses the options for meeting the health and social care needs of the new
community on the HMS Ganges site. The planning decision will be made in the next few
months and while it is not clear whether it will be given planning permission it is imperative
that a strategy to deal with the potential new residents is developed as a matter of urgency.
This site has been derelict for a number of years and has an extant planning permission for
just over 400 retirement homes. As derelict ‘brownfield’ land, the HMS Ganges site is a key
strategic development site within the Peninsula and the district of Babergh. There is also a
national, regional and local need for housing, which in the case of Babergh means providing
345 houses every year for the next thirteen years. Compared to the previous extant planning
permission for 400 retirement homes this proposal will build a mix of housing including
affordable and starter homes. This is likely to create a more balanced and sustainable
community of individuals, couples and families both from inside and outside the Peninsula and
Babergh.
The Shotley Peninsula is a rural community in South Suffolk, part of the district of Babergh.
The area has a population of 8000 people which is served by a single practice of four GPs who
own two purpose-built surgeries – one in Holbrook and the other in Shotley. The practice has
a primary care team that also includes three locum GPs. Emergency and acute hospital care is
provided by Ipswich Hospital. The general health of this population is good with a large
proportion of older people compared to children and young adults. There is a poor public
transport network on the peninsula and few retail and leisure amenities (especially for
children and young people). Three primary schools, a secondary school and a private boarding
school are located on the Peninsula. There is only one main road, the B1456, running the
length of the Peninsula that carries all traffic out of the Peninsula and towards Ipswich and
the rest of Suffolk. The residents work in a wide variety of different employment sectors –
manufacturing, retail, real estate and renting, education, agriculture and health and social
care - however the majority of these are located outside the Peninsula. The majority of
residents are heavily dependent on their cars as most work outside the peninsula using their
cars only or cars and trains. They also use their cars access key services such as food
shopping, banking and dental services which are also located outside the Peninsula.
The proposal to create a mixed development with a range of starter, affordable and other
homes as well as space for retail amenities and community facilities will have positive health
effects for the people who will move into the proposed development. The people moving in
Page 1

Executive Summary
are likely to be local people as well as people from outside the Peninsula. The existing
community will benefit from the landscaped public green space and the increase in retail
amenities and community facilities. The development will regenerate and bring back into use
a currently derelict and unused site. It will connect up Shotley village to the marina and its
associated development creating a more integrated physical community at the end of the
Peninsula that will allow more people to access the marina and the proposed museum by
road, cycle-paths and walking routes. Finally, it has the strong potential for improving the
quality of community relationships and interactions (social capital) by creating a focal point
for community activities through a village square that has a range of retail amenities and
community facilities.
The increase in population by 1,500 people within a two-year period will however cause
significant strains on the existing community and local services, especially primary and
secondary health care services. For existing residents there will be uncertainty and moderate
to major disruption during the construction period which is likely to last for up to two years.
There will be construction lorries moving through the community potentially causing more
road traffic accidents and more concern about road traffic accidents as well as bringing noise,
vibration, dirt and litter. For those living immediately adjacent to the site there will also be
noise and dust from the site and considerable loss of visual amenity as soil is excavated and
materials piled up on the site. There will also be more non-local strangers in the area –
largely but not exclusively workers on the construction site - which is likely to generate some
concerns about crime and safety. As new residents move into the HMS Ganges housing
development there will be increasing numbers of new people bringing different ways of doing
things and behaving, more traffic and greater pressures on local services and amenities. Apart
from road traffic accidents the majority of these individual health impacts will be relatively
small in scale however, their prolonged duration almost every day and over a number of years
is likely to create significant psychosocial stress in existing residents which may manifest in
physical disease as peace of mind, quality of life, sleep and daily routines are disrupted. This
could be more pronounced in those with pre-existing health conditions. Residents along the
whole of the Peninsula are likely to be effected in a moderate way during the construction
phase but those living adjacent to the entrance of the construction site are likely to face the
most disruption.
The new residents will most likely be younger couples with dependent children and older
couples without dependent children. In the short term moving to the area will be stressful for
them because of a: lack of a social support network of family and friends, lack of knowledge
of the area and where amenities are located, lack of familiarity with local customs and local
ways of living and doing things and in the case of children this could be especially difficult.
Over the long term, adapting to local ways and the local social, cultural and natural
landscape will have positive as well as negative mental health implications depending on how
quickly and how well the new residents adapt to the way of life on the Peninsula. Moving
house is one of the biggest causes of stress and loss of wellbeing and so, similar to existing
Page 2

Executive Summary
residents, new residents will also face significant psychosocial stress but for different reasons
and these again will be more pronounced in those with pre-existing poor health.
The development will generate considerable pressures in the local health services not just
because of the relatively sudden increase in the number of people on the Peninsula but also
because of the way the development will disrupt the lives of both existing and new residents.
These pressures will predominantly occur in children’s and older people’s services at primary,
secondary and intermediate levels and largely from those with pre-existing health conditions.
There are five major options for meeting the health needs of the incoming community and
maintaining the quality of health and social care services for existing residents (see Table
ES1).
The first is to assume that the increasing workload will be borne by the existing GP practice
team with emergency demand being dealt with by additional locum GPs. The second option is
to bring an additional GP and practice nurse into the existing practice with this GP providing
the majority of care to the development from there. The third option is to develop a
community nurse team that delivers clinic-based services from the community facilities
created on the development site thereby reducing the workload on the existing GP team and
so enabling them to increase their list sizes. The fourth option is a synthesis of options two
and three where the expanded practice delivers a range of outreach services based in the
community facilities on the development site. The fifth option would be to have a separately
contracted single-handed GP with a practice team based in the community facilities on the
HMS Ganges site.
Most of the options have strengths and weaknesses but option four offers the greatest
potential for delivering health positives whilst minimising the health negatives. This is
because while there is a strong need to expand the local health and social care services there
is also a strong need to make them as local and accessible as possible and to develop a
proactive health promotion and disease prevention approach for the people living at the end
of the Peninsula. This option is also the most in-line with the recommendations of the
Wanless Reports on the likely structure of the primary and public health care that is most
likely to deliver the greatest health benefits as well as meeting public expectations of the
National Health Service. Table ES1 shows the type and level of potential health impacts likely
for each of the five options.
Legend for Table ES1 + positive health impact +++ major ---- negative health impact ++ moderate --
~ no health impact + mild -
Page 3

Executive Summary
Table ES1: Potential health implications of the five options
Option Health Impact Comment
1. Existing practice copes with demand with emergency locums only.
--- The practice is already at the limits of its capacity and this is likely to lead to deteriorates and lower quality service to both new and exiting residents on the Peninsula.
2. An additional GP and practice nurse in the existing practice providing the majority of care from there.
++ This option will deal with the primary health care needs of the existing and new residents however it does little to move towards a more local community-based primary and public health care as advocated by the Wanless Report.
3. A community nurse team that delivers clinic-based services from the community facilities created on the HMS Ganges site.
++ This option moves strongly towards a community-based primary care and public health care approach but will easily act in isolation from the existing practice and create an un-integrated primary care service on the Peninsula with an increased potential for in-service conflicts
4. Expanded practice of additional GP and practice nurse delivers a range of outreach services based in the community facilities on the HMS Ganges site.
+++ This option, on balance is likely to have the best health gains for both the existing and new residents providing an integrated primary and public health care service that is local and community-based and moves in the direction the Wanless Report argues is likely to be the structure of primary care 2022
5. Separately contracted single-handed GP with practice team based in the community facilities on the HMS Ganges site.
-- This option is the least favourable as single-handed general practices are difficult to run, stressful and tend in the long run to deliver less effective care than group practices. This option will also lead to a les integrated service on the Peninsula with an increased potential for in-service conflicts.
The key recommendations are firstly, discussions between the primary care team on the
Peninsula, Central Suffolk PCT and Suffolk Social Services on how they will meet the needs of
the new residents whilst maintaining the quality of care and access to services of existing
residents. Secondly, discussions between Central Suffolk PCT, Suffolk Social Care Services,
Babergh Culture and Leisure Services, Babergh Planning Department and Haylink Ltd. on the
opportunities to develop a community centre and range of community facilities in the retail
and commercial space that has been proposed. Thirdly, discussions between Central Suffolk
PCT, Suffolk Social Care Services, Suffolk Environment and Transport Department and the
Police to investigate the best way of improving access and movement across the existing road
network through the use of traffic calming measures and reconfigurations of junctions that
have caused traffic incidents and accidents.
Page 4

Table of Contents
Table of Contents
Executive Summary 1
1. Introduction 9
2. Health and Health Impact Assessment 10
2.1 Definition of health impact assessment 10 2.2 Definitions of health 11 2.3 Determinants of health 12 2.4 Health inequalities 12
3. Methodology 14
3.1 Introduction 14 3.2 Stages 15 3.3 Methods used 16 3.4 Consultation 16 3.5 Strengths and limitations 17 3.6 Ethical issues 18
4. Background Context 19
5. Baseline Assessment 20
5.1 Introduction 20 5.2 Population characteristics 21 5.3 Deprivation and social inclusion 24 5.4 Employment and unemployment 25 5.5 Transport and mobility 27 5.6 Health, social care services and other key amenities 28 5.7 Community cohesion 29 5.8 Crime and community safety 29 5.9 Housing 30 5.10 Economic development 31 5.11 Education 32 5.12 Environment 33 5.13 Culture and leisure 33
6. Evidence Base 34
6.1 Introduction 34 6.2 The impact of health services provision on health and health inequalities 34 6.3 The impact of social exclusion on health and health inequalities 36 6.4 The impact of social capital on health and health inequalities 38
Page 5
Table of Contents
6.5 The impact of housing on health and health inequalities 41 6.6 The impact of transport on health and health inequalities 45 6.7 The impact of education on health and health inequalities 50 6.8 The impact of culture & leisure activities on health and health inequalities 51 6.9 The impact of the built environment on health and health inequalities 51 6.10 The impact of economic development on health and health inequalities 52 6.11 The impact of crime on health and health inequalities 52
7. Policy Context 55
7.1 Introduction 55 7.2 National Policy 55 7.3 Regional and local policy 59 7.4 National Health and social care services policy 61
8. Local Views and Knowledges 63
8.1 Introduction 63 8.2 Shotley parish council community consultation 63 8.3 Concerns of the Parish Councils 65
9. Appraisal of Current Trends without the Proposed New Housing Development 70
9.1 Introduction 70 9.2 Impact Appraisal 70 9.3 Mitigation measures & Enhancement opportunities 71
10. Appraisal of the Proposed New Housing Development 72
10.1 Introduction 72 10.2 Impact appraisal 72 10.3 Mitigation measures 74 10.4 Residual effects 75 10.5 Enhancement opportunities 75 10.6 Conclusion 75
11. Appraisal of the Options for Delivering Health and Social Care to the Proposed New Housing Development 91
11.1 Introduction 91 11.2 Background context 91 11.3 Appraisal 94 11.4 Mitigation measures 97 11.5 Residual effects 98 11.6 Enhancement opportunities 98 11.7 Conclusion 98
Page 6

Table of Contents
12. Conclusion and Recommendations 99
12.1 Introduction 99 12.2 Positive and negative health effects for existing residents 99 12.3 Positive and negative health effects for the potential new residents 100 12.4 Positive and negative implications for the health and social care services 101 12.5 Mitigation and enhancement measures for existing and new residents 101 12.6 Mitigation and enhancement measures for health and social care services 102 12.7 Monitoring and evaluation of the health impacts 103 12.8 Recommendations 103
References 115
Page 7

Table of Contents
Page 8
1. Introduction
1. Introduction
This report is prepared for Central Suffolk Primary Care Trust (PCT) and Haylink Ltd.
It describes a rapid health impact assessment (HIA) with a particular focus on the health
service implications of the potential health impacts associated with the development of the
HMS Ganges site on the Shotley Peninsula in Suffolk.
The key objectives of the health impact assessment were to identify:
1. the positive and negative health effects arising out of the development for existing local
residents living on the Shotley Peninsula,
2. the positive and negative health effects arising out of the development for residents of
the new housing development on the HMS Ganges site,
3. the positive and negative implications for the primary and secondary health services of
the new housing development,
4. key mitigation and enhancement measures to reduce the potential negative and positive
health effects for existing and new residents, and
5. key mitigation and enhancement measures for the local primary and secondary health
services for the Shotley Peninsula area.
The remainder of this report is structured as follows:
Chapter 2 explains health and health impact assessment;
Chapter 3 describes the methodology used for this HIA;
Chapter 4 describes briefly the background context of the proposed development;
Chapter 5 details the baseline conditions;
Chapter 6 describes key aspects of the evidence base used to appraise the potential positive
and negative health impacts;
Chapter 7 describes the key policy guidance evidence used to appraise the potential positive
and negative health impacts;
Chapter 8 describes the key concerns, views and experiences of local residents as expressed
through previous consultation exercises and interviews with key informants;
Chapter 9 assesses the health impacts of the proposed development if health and social care
services stay as they are;
Chapter 10 assesses the health impacts of two potential approaches to upgrading primary
care services for the development; and
Chapter 11 draws together the key conclusions and recommendations for mitigation and
enhancement.
Page 9

2. Health and Health Impact Assessment
2. Health and Health Impact Assessment
2.1 Definition of health impact assessment
Health impact assessment (HIA) is a relatively new impact assessment methodology. Statutory
legislation requires an environmental impact assessment (EIA) to be commissioned as part of
the planning process for significant developments. This legislation also prescribes the areas
which an EIA must cover (1,2). In contrast HIA is commissioned voluntarily, the methodology
is informed by national and international best practice and the focus determined by the
nature of the initiative (policy, programme, project, service or development) which is being
assessed.
The international consensus definition of health impact assessment is:
“A combination of procedures, methods and tools by which a policy,
program or project may be judged as to its potential effects on the health
of a population, and the distribution of those effects within the
population.”
WHO European Centre for Health Policy (3)
Our working definition of HIA that builds on the international consensus definition is that HIA
is the key systematic approach to identifying the health impacts of proposed and
implemented policies, programmes, projects and services within a democratic, equitable,
sustainable and ethical framework, so that negative health impacts are reduced and positive
health impacts increased (within a given population). It uses a range of structured and
evaluated sources of qualitative and quantitative evidence that includes public and other
stakeholders' perceptions and experiences as well as public health, epidemiological,
toxicological and medical knowledges.
This definition of HIA contains several key points, HIA:
• draws on many different techniques and sources of evidence;
• looks at the potential effects of an initiative i.e. it is carried out while the initiative is
at an early stage;
• identifies the potential positive as well a negative health effects;
• is concerned with the distribution of effects within a population because different
groups can be affected in different ways and the health inequalities this may give rise
to.
As with other forms of impact assessment HIA also attempts to identify mitigation measures
to help reduce the negative health effects and enhancement measures to help increase the
positive health effects of an initiative.
Page 10

2. Health and Health Impact Assessment
HIA also aims to contribute to developing a monitoring and evaluation strategy for the
initiative to ensure that the negative health effects are actually reduced. It can also enable
stakeholders to develop their own milestones and indicators for evaluating the health
positives and negatives of an initiative once it is built, implemented or in operation (4).
2.2 Definitions of health
Having a clear definition of what we mean by health and what definition of health we use
when undertaking a HIA is crucial as the definition will to a large extent determine what kind
of evidence needs to be collected and the kinds of health and illness factors that will be
considered.
Some people understand health as meaning curing diseases, more health services and new
medical technologies and procedures. HIA works with a broad model of health which includes,
but doesn’t stop at this medical model (5). It encompasses other determinants of health such
as housing, employment, social support, crime and community safety and education.
Health is difficult to define and ways of thinking about it have changed over the years and are
still changing (6). Three key models of health are the "medical model", the "holistic model",
and the "wellness or social model”: In its simplest form, the “medical model” views the body
as a machine that can be fixed when it does not work as it should. Its focus is on diagnosing
and treating specific physical conditions (diseases), and therefore tends to be reactive in
dealing with health problems rather than proactive in trying to prevent them. In this model
health is defined as the absence of disease and the presence of normal physical functioning.
The holistic model of health is exemplified by the 1947 WHO definition, "a state of complete
physical, mental and social wellbeing and not merely the absence of disease or infirmity".
This model uses a broader definition of what health is and also brings in the broader notion of
wellbeing.
The social model was developed from World Health Organisation (WHO) health promotion
initiatives of the 1970’s and 80’s. The definition argues that "[Health is] the extent to which
an individual or group is able to realise aspirations and satisfy needs, and to change or cope
with the environment. Health is therefore a resource for everyday life, not the objective of
living; it is a positive concept, emphasizing social and personal resources, as well as physical
capacities" (7).
Other definitions see health in terms of resilience. for example, "…the capability of
individuals, families, groups and communities to cope successfully in the face of significant
adversity or risk." and in ecological terms, health can be seen as "a state in which humans,
and other living creatures with which they interact, can coexist indefinitely" (8, 9).
Page 11

2. Health and Health Impact Assessment
The advantage of the medical model is that disease states can be relatively easily diagnosed
and measured. But this approach is narrow, seeing health as simply about physical disease, its
symptoms and consequences. The holistic and social models incorporate broader ideas of
wellbeing that take account of an individual’s subjective feelings of health, wellbeing and
illness. They allow for people with stable impairments to be seen as healthy e.g. a deaf or
blind person or someone with paraplegia who needs the aid of a wheelchair. However, these
conceptualisations are very broad and difficult to measure and assess.
2.3 Determinants of health
Health is affected by a wide range of factors, from what we eat and drink, to where we live
and work as well as the social relationships and connections we have with other people and
organisations. These factors are termed the wider determinants of health.
Figure 2.1 shows the Dalgren and Whitehead model of the wider determinants of health and
shows a visual diagram of the importance of social, cultural, spiritual and community factors
in affecting and influencing individual, family and community health and wellbeing alongside
genetic, lifestyle and personal factors such as age, gender and ethnicity.
HIA attempts to appraise these wider determinants and the potential impacts that an
initiative might have on these wider determinants and so on the health and wellbeing of the
affected population.
Figure 2.1 Wider determinants of health
Source: Dahlgren and Whitehead (10)
2.4 Health inequalities
Each of us is affected by the determinants of health described in the previous section.
However, the influence of these determinants is different with some playing a greater or
Page 12

2. Health and Health Impact Assessment
lesser role depending on personal, social and cultural factors. These differences in effect lead
to differences in health status (regardless of how we define health) so that we each possess
varying degrees of health and wellbeing. This creates a range of ‘health inequalities’ between
different individuals and different groups within a given community or society. These
inequalities in health due to personal circumstances such as gender, ethnicity, disability,
financial resources, housing, social support networks and self esteem can be exacerbated by
an initiative.
HIA therefore also considers how an initiative potentially widens or narrows these health
inequalities and how different groups will be affected within an affected community as a
whole.
Communities can therefore be categorised and compared in many different ways. Some of the
key ways of classifying and grouping communities that enable us to highlight health
inequalities are:
• Age – e.g. children, elderly people.
• Gender – e.g. male, female.
• Socio-economic status – e.g. unskilled, skilled, professional, income levels, education
levels, other.
• Ethnicity – e.g. White, Black, Asian, other.
• Culture (including religion) – e.g. Buddhist, Christian, Hindu, Muslim, Sikh, other
• Sexual orientation – i.e. heterosexual, homosexual, bisexual.
• Disability – e.g. physical, mental, other.
• Disease vulnerability/ susceptibility – e.g. thallassaemia, cystic fibrosis, sickle cell
anaemia, diabetes, other.
It is important to recognise that individuals can and do fall into more than one of these
categories. We have multiple identities and fit within multiple categories. The categories are
therefore useful rules of thumb but do not define and encompass what a person is. However,
categorising does provide a systematic approach to exploring the potential health impacts and
health inequalities by ensuring that key characteristics of both individuals and groups are
taken into account.
Page 13

3. Methodology
3. Methodology
3.1 Introduction
As noted previously health can be seen in narrow or broad ways. Health that is more than the
absence of disease is affected by many different determinants – direct and indirect. Alongside
these determinants people’s perception and experiences of their social, cultural and natural
environments are also central to their sense of health and well-being. This appraisal
incorporates a biomedical and social definition of health and wellbeing.
Health and wellbeing is more than the absence of disease or symptoms but incorporates the
indirect effects of education, employment, access to health and social care services and the
social, cultural and natural environments which through indirect pathways of impact produce
physical and psychological health effects.
To fully explore the potential impacts on residents’ health and wellbeing of the development
proposal it is necessary to develop an understanding of peoples’ perceptions, experiences,
daily routines, the ways they use their social and physical space and the types of social
interactions that occur within them.
Whereas health needs assessment moves from appraising the health needs of a population and
then developing policies, programmes, projects and services to meet those needs; health
impact assessment appraises policies, programmes, projects and services in terms of their
impacts on a population (see Figure 3.1).
Figure 3.1 Difference between health needs assessment and health impact assessment.
health needs assessment
PROJECT POPULATION
health impact assessment
An important point to bear in mind is that scientific criteria may not have democratic
legitimacy if they are inconsistent with considerations such as social values, moral criteria or
ethics (11). Firstly, by privileging quantitative evidence we can risk ignoring factors which we
cannot measure very reliably, but which are socially important e.g. spiritual aspects of
health, well-being and aesthetic aspects of the environment. Secondly, when there is
scientific uncertainty about risks to health, societal and community values can help ensure
Page 14

3. Methodology
that initiatives reduce the negatives and enhance the positives of an initiative by making
them more in keeping with social and cultural norms. An assessment which includes anecdotal
and experiential evidence as well as scientific evidence facilitates a more socially, morally
and scientifically justifiable decision (12).
3.2 Stages
In line with the majority of HIA models our methodology involves seven key stages (13):
• Scoping
• Baseline assessment
• Evidence base
• Appraisal
• Mitigation and enhancement measures
• Monitoring and evaluation
• Conclusions and recommendations
3.1.1 Scoping
This stage sets the ‘terms of reference’ for the HIA i.e. what aspects will be considered, what
areas and groups might need particular focus and what will be excluded from the HIA. A
scoping paper was produced which was amended and agreed upon by the commissioners (see
Appendix 1)
3.1.2 Baseline Assessment
This stage develops a specific local health and wellbeing profile of the community and is
developed using existing evidence from a range of sources to act as a baseline from which to
assess the potential positive and negative impacts.
3.1.3 Evidence Base
This stage involves the creation of a focussed and relevant collation of evidence on the
identified positive and negative health impacts of various aspects of the proposed
development, where this is available. This includes policy and lay evidence and knowledges as
well as more formal research evidence.
3.1.4 Appraisal
This stage undertakes a systematic appraisal of the potential impacts, the size and
significance of the impacts and the groups that are likely to be most affected.
3.1.5 Mitigation and Enhancement Measures
This stage identifies measures to reduce the potential negative health effects and increase
the positive health effects.
Page 15

3. Methodology
3.1.6 Monitoring and Evaluation
This stage identifies possible monitoring and evaluation measures to ensure that during the
implementation/construction and the implementation/operation phase negative health
effects are minimised and positive health effects maximised.
3.1.7 Conclusions and Recommendations
This stage details the significant conclusions and recommendations emerging from the
appraisal.
3.3 Methods used
A range of literature review techniques were used to gather information and evidence about
the potential positive and negative health effects of the development options. Routine
information about the Shotley Peninsula and Babergh was identified from the Office of
National Statistics, the Suffolk Observatory and district and county council websites. Policy
guidelines at national, regional and local levels relevant to the proposed development were
also referred to. Information about the concerns of local residents was gathered by examining
the findings of past consultations.
3.4 Consultation
Consultation is an important element of health impact assessment. Many community and
stakeholder consultations tend to be preference surveys eliciting the likes and dislikes of local
people.
There are three key reasons that residents’ and other stakeholders’ views and experiences
are used in HIAs:
• Residents both existing and new will face the direct positive and negative health
consequences of the development.
• Residents and other stakeholders have valuable experiential knowledge that they have
built up over years and decades about the locality in which they live and work.
• Not adequately and appropriately addressing residents’ concerns can and does lead to
residents experiencing stress and negative health effects.
• To allow residents and others to have a voice and influence in community processes and
thereby reduce a sense of social exclusion, democratic deficit and inequality.
Because of time constraints and the rapid nature of this HIA, only a limited consultation with
key informants who had particular knowledge and experience and an analysis of the findings
of relevant past consultations were undertaken.
Page 16

3. Methodology
3.5 Strengths and limitations
Both quantitative and qualitative approaches have strengths and limitations. In terms of
limitations both are based upon assumptions about how the world works. Table 3.1 shows how
quantitative approaches assess the rigour of research in terms of validity, reliability,
generalisibility and objectivity, while qualitative approaches assess the rigour of research in
terms of credibility, authenticity, transferability and confirmability (14).
This appraisal does not undertake any quantitative modelling of potential positive or negative
health impacts because they are only as good as the assumptions made and the quality of the
starting data. In the majority of cases the starting assumptions do not take account of
specific aspects of local context and the starting data is limited. An example in the case of air
pollution modelling is that most models make assumptions about geographical topography,
street configuration, climate and wind directions to estimate the likely peaks and average of
air pollution in a small area. In terms of data most use average estimates based on monitoring
sites that do not capture specific peaks and troughs and tend not to be based in the local area
concerned. Finally, quantitative modelling can give a false sense of precision and
forecastibility. These issues apply equally to traffic forecasting and modelling of traffic flows
for roads not yet built, street configurations not yet laid out and pedestrians not yet crossing
proposed roads.
By contrast, taking a qualitative approach and understanding the key factors that will be
acting regardless of what the eventual detailed layout of the development will be can provide
a clearer guide as to what is on balance likely to be better for health and what mitigating and
enhancement measures could be put in place to improve the initiative overall.
Table 3.1 Comparison of the quantitative and qualitative approaches to rigour (14)
Quantitative Qualitative Validity The degree to which people
taking part in the research are representative of the community as a whole.
Credibility The degree to which people taking part in the research recognise and agree with the findings of the research.
Generalisability The universality of the research findings and their application at other times and in other places.
Transferability The degree to which the research findings can be used in similar social and cultural contexts.
Reliability The repeatability of the research such that it gives the same results if done again on the same population with the same characteristics.
Dependability The degree to which other researchers would find the same results given the same population with the same characteristics.
Objectivity The degree to which emotion and the preferences of the researcher are removed from the research.
Confirmability The degree to which the research findings emerge from the research data rather than the emotion and preferences of the researcher.
Sources of bias in qualitative approaches are reduced by cross-checking or ‘triangulating’
information against other sources. This HIA used routine information, lay knowledges and
Page 17

3. Methodology
evidence, policy guidance and research evidence to build a coherent and consistent
understanding of the current conditions and the likely future implications.
3.6 Ethical issues
All information was gathered on the understanding that people's remarks would be presented
anonymously and would not be attributable to any one individual if they did not wish it.
We also endeavoured at all times to present no personal views about the proposed
development but to think and talk through all the issues raised during the HIA with other
people.
Page 18

4. Background Context
4. Background Context
HMS Ganges is a derelict naval base that has not been in use for the last three years. It
stopped being a naval training base many years ago and for a number of years was used by
Suffolk Police as a training centre for their cadets.
The site has extant planning permission for the building of 404 retirement homes however,
this was felt to be no longer appropriate and a more mixed development with a range of
homes and community facilities and commercial space has been drawn up.
The Master Plan states that:
“HMS Ganges will become part of an extended Shotley. It will offer a sustainable mix of
residential, (including starter and affordable homes), local shops, small business units, a
new naval heritage museum and 10 Ha of community open space.
The new development will be an exciting place to live, work and visit for all; it is
intended to be an inclusive development.
The Master Plan has at its heart a new village square, defined by a mix of commercial,
retail, workshop and cultural uses. This has been designed to link the new part of Shotley
to the existing Shotley village to the immediate west, and improve the range of local
facilities and services.
…
The development will create a community for residents of all ages, the young and old
alike, and for those working and living close by.
The extended community will be mixed and balance, giving a high quality residential
environment to all.”
Extract from the HMS Ganges Master Plan (15)
Considerable thought has already gone into the environmental suitability and sustainability of
this re-development, as evidenced by four key pieces of work:
• Planning Statement
• Master Plan Statement
• Environmental Statement
• Sustainability Appraisal
The site is a key brownfield site in Babergh and South Suffolk with the majority of local
people wanting to see some sort of good mixed development on the site. It is therefore a
strategic piece of land that has many stakeholders interested in how the site is developed.
Page 19

5. Baseline Assessment
5. Baseline Assessment
5.1 Introduction
This chapter describes the key baseline conditions as they relate to direct and indirect
determinants of health for Shotley Village in the context of the Shotley Peninsula and Babergh
as a whole. The majority of this data has been gathered from the Office of National Statistics
and the Suffolk Observatory (16, 17).
This is not intended to be an exhaustive profile of the current social, environmental and
economic conditions as they relate to health but a rapid assessment of readily accessible
information relating to the end of the Peninsula.
The Shotley peninsula is at the southern end of the district of Babergh in Suffolk. It is
encompassed by Central Suffolk PCT, Suffolk and Norfolk Strategic Health Authority and
Suffolk County Council (See Figure 5.1).
The focus of this baseline socio-economic and demographic profile will be the two wards most
directly affected by the proposed new development, Berners and Holbrook, and the parishes
within them, Shotley, Ewarton, Chelmondiston, Woolverstone, Freston, Harkstead and
Holbrook (see Appendix 2 for a detailed administrative map of Babergh).
This baseline will use data at the level of Babergh and the wards of Berners and Holbrook to
create as full a picture as possible of the current conditions in the community around the HMS
Ganges site.
Figure 5.1 Map of the Shotley peninsula and its relations to other key towns and cities
Page 20

5. Baseline Assessment
5.2 Population characteristics
5.2.1 Population size and growth
The resident population of Berners, Holbrook and Babergh is currently just under 3900, 2600
and 83500 respectively (16, 17).
Figure 5.2 Proportion of residents by age
0%
5%
10%
15%
20%
25%
30%
35%
40%
45%
50%
0 to 15 16 to 19 20 to 29 30 to 59 60 to 74 75 and
over
Berners
Holbrook
Babergh
England & Wales
Figure 5.2 shows that Berners has a similar demography to Babergh as a whole, in contrast to
Holbrook which has considerably greater numbers of children and young people
(proportionately 50% more under 16s and two to three times the number of 16-19 year olds)
with a corresponding lower number of 30-59 and 60-74 year olds.
Table 5.1 Population trends in Babergh 1999-2001
Age Census Change
1991 2001 Number %
0-19 20,287 20,146 -141 -7%
20-29 10,303 7,779 -2,524 -24.5%
30-59 31,322 35,579 -4,257 -14%
60-79 14,553 15,908 1,355 9%
80-89 3,167 4,050 883 28%
79,632 83,462 3,830 5%
Table 5.1 shows how the population of Babergh has changed over the 10 years between 1991
and 2001 (18). The main points are:
• total population grew by 5;
• number of young people under 20 went down by 7% with an almost 25% fall in the
numbers of young adults aged 20-29;
• the number of older people has increased in all age groups with an almost 10% increase
of those aged between 60-79 and an almost 30% increase in those aged 80-89; and
Page 21
Salim Vohra
Is there ward level data of population change

5. Baseline Assessment
• with the impact of the post-war baby boom in 10 years time there could be a 45%
increase in residents in their 60’s.
5.2.2 Ethnic Profile
10% of the population of England as a whole are ethnic minorities. In contrast, at 2%, 2.1%
and 2.5% respectively, the ethnic minority populations of Babergh, Berners and Holbrook are
tiny.
5.2.3 Family Structure
Marital status and household composition give a good indication of the family structure and
the likely personal and social care networks that residents have. The populations of Babergh,
Berners and Holbrook have very similar family structures, though Holbrook, as highlighted by
the age profile, has many more single people and fewer married or re-married people. This is
more in line with the profile for England & Wales as a whole (see Figure 5.3).
Figure 5.3 Marital status on the Peninsula compared to Babergh and England & Wales (all people
aged 16 and over)
0%
10%
20%
30%
40%
50%
60%
70%
Single
(never
married)
M arried or
re-married
Separated Divorced Widowed
Berners
Holbrook
Babergh
England & Wales
There are 1670 households in Berners, 758 in Holbrook and 34,865 in Babergh. Of these just
over 25% of households in Berners and Holbrook are one-person households, 15% are
pensioners living alone, 30% have dependent children and 5% are lone parents with children
(See Figure 5.4 next page).
There are 480 households in Berners with dependent children, of which 186 have children
aged 0-4. There are 233 households with dependent children in Holbrook, of which 71 have
children aged 0-4.
In Berners 516 households have one or more person with a limiting long term illness while in
Holbrook there are 229 households like this.
Page 22

5. Baseline Assessment
Figure 5.4 Household composition on the Peninsula compared to Babergh and England & Wales
0%
5%
10%
15%
20%
25%
30%
35%
1 person
households
Pensioners
living alone
Other All
pensioner
households
Contained
dependent
children
Lone parent
households
with
dependent
children
Berners
Holbrook
Brabergh
England & Wales
5.2.4 Religion
Over 73% of the population of Babergh, Berners and Holbrook call themselves Christians and
over 16% state that they have no religion (in Berners this is 20%) compared to 72% and 14% for
England and Wales as a whole.
5.2.5 Health status
Over 93% of the residents of Babergh, Berners and Holbrook described their perceived health
status as good to fairly good with 7% stating that their health was not good which is lower
than the England & Wales average. Holbrook with its younger population had over 95% of
residents stating that their health was good to fairly good with less than 5% stating that their
health was not good.
Figure 5.5 Health status and long term illness on the Peninsula compared to Babergh and England & Wales
0%
10%
20%
30%
40%
50%
60%
70%
80%
Good Fairly good Not good With a
limiting
long term
illness
People of
working
age with a
limiting
long term
illness
Berners
Holbrook
Babergh
England & Wales
Page 23

5. Baseline Assessment
Overall the population health of the people under the care of Central Suffolk PCT is very good
though there are likely to be local variations. Life expectancy in the Central Suffolk area is 78
years for men and 82 years for women. The infant mortality rate is 2 per 1000 live births
compared to the East of England rate of 4.5 per 1000 live births. Deaths and illness from
coronary heart disease, respiratory illness and cancer are lower than the Suffolk and England
& Wales averages. Teenage conception rates are very low. There is currently no routinely
analysed and anonymised general practice level data.
5.3 Deprivation and social inclusion
The Index of Multiple Deprivation 2000 (IMD) for England was published by the Department of
Environment, Transport and Regions (DETR) in 2000 (19). The IMD contains 6 'domains':
income; employment; health & disability; education, skills & training; housing; and
geographical access to services. Each ward is given a score and rank in each domain based on
its performance in respect of a range of relevant indicators. Wards are ranked from 1 to 8414
with 1 being most deprived and 8414 being least deprived.
Figure 5.6 Rank of the index of multiple deprivation, the six domains and child poverty out of 8414
0
1000
2000
3000
4000
5000
6000
7000
8000
9000
Index of
M ultiple
Deprivation
Income Employment Health Education Housing Access Child
Poverty
Ward Berners Rank
Ward Holbrook Rank
• The key domain of deprivation for both Berners and Holbrook is access where both score
approximately 2000 (out of 8414).
• Relative to England & Wales both Berners and Holbrook are not deprived in terms of
income, employment, health and child poverty though Berners is relatively more deprived
than Holbrook.
• Only in terms of education is Holbrook relatively more deprived than Berners.
In terms of the wards covered by Central Suffolk PCT Holbrook is the least deprived in terms
of income, employment and health and Shotley is the most deprived in terms of housing.
Page 24

5. Baseline Assessment
5.4 Employment and unemployment
Berners has a higher proportion of full-time and part-time employed residents, 41% and 10%
respectively, compared to Holbrook, 36% and 9% respectively, and is in line with the rates for
Babergh as whole. There are also higher numbers of retired residents in Berners (17%)
compared to Holbrook (12%).
There are almost 10% self-employed in both Berners and Holbrook. However in Holbrook there
are more economically inactive (15%) and economically active students than Berners (2% and
1% respectively). Though there are low levels of unemployment in Berners and Holbrook,
Berners (2%) has a higher rate than Holbrook (1%) and in both Berners and Holbrook these
unemployed residents are long-term unemployed. 3% of Berners and 2% of Holbrook residents
aged between 16-74 years are permanently sick or disabled.
Figure 5.7 Proportion of employed, unemployed, retired people and students on the Peninsula
compared to Babergh and England & Wales (all people aged 16-74)
0%
10%
20%
30%
40%
50%
60%
P art-timeemplo yed
Full-timeemplo yed
Self-emplo yed
Unemplo yed Eco no micallyactive full-
t ime student
Retired Eco no micallyinactivestudent
Lo o king afterho me/family
P ermanentlysick/disabled
Othereco no mically
inactive
Berners
Holbrook
Babergh
England
Approximately 50% of men in Berners (54%), Holbrook (46%) and Babergh (53%) are in full-time
employment compared to just under 30% of women (29%, 25% and 28% respectively).
There are many more women who work part-time than men with Berners having 26%,
Holbrook, 22% and Babergh 24% compared to less than 3% of men in all three areas.
Slightly more women are retired than men in Berners, Holbrook and Babergh and there are
many more women looking after homes and families (over 10%) compared to men (less than
1%).
There are an equal proportion of women and men in Babergh, Holbrook and Babergh who are
permanently sick or disabled.
Page 25

5. Baseline Assessment
The majority of men working full-time work on average between 38-48 hours per week but
there is a significant proportion, over 30% in Holbrook and just under this in Berners, who
work more than 49 or more hours per week.
The majority of women work part-time and most of these work for between 16-30 hours per
week though, like the men, there is a significant proportion, almost 15% in Holbrook, of
women working 49 or more hours per week.
Residents of Berners and Holbrook as in Babergh as a whole, are employed in a variety of
areas with high numbers in manufacturing; wholesale and retail trade; real estate and
renting; education and health and social care (see Figure 5.7). Fewer residents work in
construction; hotel and catering; transport storage and communication; financial
intermediation and public administration and defence. Fewer work in agriculture/forestry and
electricity/gas/water supply with a very small proportion working in fishing and mining/
quarrying.
Figure 5.8 Proportion of residents working in different employment-related fields on the Peninsula
compared to Babergh and England & Wales (all people aged 16-74)
0%
5%
10%
15%
20%
25%
Agr
icul
ture
; hu
ntin
g; f
ores
try
Fish
ing
Min
ing
& q
uarr
ying
Man
ufac
turi
ng
Elec
tric
ity;
gas
and
wat
er s
uppl
y
Con
stru
ctio
n
Who
lesa
le &
ret
ail t
rade
; re
pair
of
mot
or v
ehic
les
Hot
els
and
cate
ring
Tran
spor
t st
orag
e an
d co
mm
unic
atio
n
Fina
ncia
l int
erm
edia
tion
Real
est
ate;
ren
ting
and
bus
ines
s ac
tivi
ties
Publ
ic a
dmin
istr
atio
n an
d de
fenc
e
Educ
atio
n
Hea
lth
and
soci
al w
ork
Oth
er
Berners
Holbrook
Babergh
England
Over 20% of people in Holbrook work in education and over 10% in both Berners and Holbrook
work in health and social care compared to 7% and 9% for Babergh. Health and social care
work is predominantly undertaken by women, approximately 20% compared to less than 5% of
men. Men are predominantly found in manufacturing, wholesale and retail, real estate,
transport and storage and construction though in Holbrook over 17% of men work in
education. Women are predominantly found in health and social care, education, wholesale
and retail, hotel and catering and real estate and renting.
Page 26

5. Baseline Assessment
Figure 5.9 Proportion of residents in different occupational groups on the Peninsula compared to
Babergh and England & Wales (all people aged 16-74)
0%
5%
10%
15%
20%
25%
M anagers andsenio r o fficials
P ro fessio nalo ccupatio ns
A sso ciatepro fessio nal and
technicalo ccupatio ns
A dminstrativeand secretarialo ccupatio ns
Skilled tradeso ccupatio ns
P erso nalservice
o ccupatio ns
Sales andcusto mer
serviceo ccupatio ns
P ro cess; plantand machineo peratives
Elementaryo ccupatio ns
Berners
Holbrook
Babergh
England
Berners has a slightly higher proportion of residents who are managers or senior officials;
administrators or secretaries; sales and customers services staff; process and plant workers;
or in elementary occupations. Holbrook has twice as many residents in professional
occupations and a higher rate of associate professionals and personal service employees (see
Figure 5.8).
5.5 Transport and mobility
Public transport on the peninsula is poor with a limited bus service that runs hourly. There is
no local taxi service based on the Peninsula.
Table 5.2 Proportion of residents on the Peninsula having access to a care or van compared to Babergh and England & Wales (all people aged 16-74)
Berners Holbrook Babergh England & Wales Households 1,668 758 34,863 281,155
Have no car or van 13% 14% 16% 27% Have 1 car or van 44% 41% 42% 44% Have 2 or more cars or vans 43% 45% 42% 29% Total number of cars or vans 2363 1081 48,896 22,607,600
Berners and Holbrook has a lower proportion of no-car households compared to Babergh and
England & Wales as a whole. Over 85% of households have access to a car or van in Berners
and Holbrook which is greater than that for Babergh and England & Wales as a whole (See
Table 5.2).
On average distances travelled to a fixed place of work for Berners, Holbrook, Babergh and
England and Wales as a whole are 20km, 16km, 17km and 13km respectively. Over 50% of
working residents use a car or van to drive to their fixed place of work with Berners (68%)
having a higher rate than Holbrook (55%) compared to Babergh (62%) and England & Wales
Page 27

5. Baseline Assessment
(55%). Approximately 10% of residents in Berners, Holbrook and Babergh work from home.
There are a high proportion of residents in Holbrook (17% and 5%) who walk or cycle to work
compared to those in Berners (5% and 1%).
Figure 5.10 Residents on the Peninsula’s mode of travel to work compared to Babergh and England & Wales (all people aged 16-74)
0%
10%
20%
30%
40%
50%
60%
70%
80%
Work
mainly at
or from
home
Metro or
tram
Train Bus Motorcycle
or scooter
Drive car
or van
Passenger
in car or
van
Taxi or
minicab
Bicycle On foot Other
Berners
Holbrook
Babergh
England
5.6 Health, social care services and other key amenities
Overall, there are four post offices, five general stores, six pubs, one fish and chips shop, one
newsagent, two hairdressers and one dry-cleaner on the Peninsula. There are four primary
schools, one secondary school and one boarding school on the Peninsula (15).
Figure 5.11: Map of the key services and amenities located on the Shotley Peninsula
However the Babergh Local Plan identifies Holbrook and Shotley Village (Shotkey gate and
Shotley Street) as unsustainable villages though Holbrook just falls short of this being
classified as unsustainable (20).
Page 28

5. Baseline Assessment
The Plan identifies sustainable villages as those with:
• a primary school:
• good journey to work public/community transport to a town;
• convenience goods shop;
• community leisure and social facilities; and
• a variety of employment opportunities which have potential for further
development.
There is one general practice serving the whole peninsula of 8000 people. There are currently
four full-time and one part-time general practitioners (GPs) with an average list size of 2000
that provide a range of primary care services including immunisation, minor surgery, family
planning, maternity and specialist clinics. There are also three locum GPs. There is a total of
forty health care staff currently working from the Shotley and Holbrook practices. There are
existing pressures on the service and the service has had difficulties in recruiting
appropriately qualified staff at all levels in the past.
For 2003 the Commission for Health Improvement gave Central Suffolk Primary Care Trust 3
stars, East Anglia Ambulance Trust 3 stars, Ipswich Hospital 2 stars and the Social Services
Inspectorate gave Suffolk Social Services 1 star.
5.7 Community cohesion
This is difficult to gauge without the opportunity to undertake some specific local
consultation. The area has a strong rural identity and naval history. New people have been
slowly moving in over the years and some new housing developments have occurred in the
relatively recent past. The Peninsula is made up of long-standing residents who have ties to
the land and the Peninsula’s agricultural past and more recently arrived residents with less
agricultural and more urban histories. There are some concerns about a generation gap and
conflicting aspirations developing between children and young people on the Peninsula and
older residents. There have also been strong concerns and protests in the recent past about
proposals to use the HMS Ganges site as a centre to house refugees and asylum-seekers (21).
5.8 Crime and community safety
Levels of crime in Babergh compared to England Wales as a whole are, overall, lower across
the whole range of criminal offences. Figure 5.11 shows the notifiable offences recorded by
the Police between 2001-2003 (17).
• Both Berners and Holbrook have lower rates of all types of crime compared to Babergh as
a whole (except for theft and handling which is higher in Berners).
Page 29

5. Baseline Assessment
• Berners has a higher crime rate and higher rate for all types of crime compared to
Holbrook.
• However, the crime rate and certain types of crime – criminal damage and theft and
handling – are reducing in Berners but increasing in Holbrook and Babergh as a whole.
• Burglary and violent crime rates have increased in Berners, Holbrook and Babergh as a
whole.
• Drug offences and fraud and forgery rates are very low and stable in Berners and Holbrook
compared to small rises in Babergh as a whole.
Figure 5.12 Rates of various crimes on the Peninsula compared to Babergh and England & Wales
0
10
20
30
40
50
60
Crime rate Burglary Criminal
damage
Drug
offences
Fraud &
forgery
Theft &
handling
Violent
crime
Berners 2001-02
Berners 2002-03
Holbrook 2001-02
Holbrook 2002-03
Babergh 2001-02
Babergh 2002-03
5.9 Housing
The majority of the residents of Berners and Holbrook live in households; however 29% of the
residents of Holbrook live in communal establishments. Those that live in communal
establishments in Berners (27 residents) live in residential home accommodation and all have
limiting long term illness. Those in Holbrook live in local authority medical and care homes
(30 residents all have a limiting long term illness), residential care homes (5 residents all of
whom have a limiting long term illness) and other communal establishments (667 residents of
which 52 have a limiting long term illness).
Average house prices in Babergh are £115,000 for terraced and £136,000 for semi-detached
properties with the vast majority (94%) of houses having central heating and sole use of bath,
shower and toilet facilities.
The majority of residents in both Berners and Holbrook live in owner-occupied
accommodation with a significant proportion owning their homes outright (Berners 34% and
Holbrook 37% compared to Babergh 35% and England & Wales as a whole 24%).
Page 30

5. Baseline Assessment
Figure 5.13 Proportion of resident living in households compared to communal establishments
0%
20%
40%
60%
80%
100%
120%
People living inhouseholds
People living incommunual
establishments
Number of students awayfrom home*
BernersHolbrookBabergh
Approximately 15% of the residents of Berners and Holbrook rent their homes, with Berners
having a higher proportion of private renting and Holbrook having a higher proportion of
council renting. There is also a significant other rented sector in both Berners and Holbrook
(5% and 11%).
Figure 5.14 Rates of home ownership and renting on the Peninsula compared to Babergh and England & Wales
0%
5%
10%
15%
20%
25%
30%
35%
40%
45%
50%
Owner
occupied:
Owns
outright
Owner
occupied:
Owns with
a mortgage
Owner
occupied:
Shared
ownership
Rented:
Council
Rented:
Registered
Social
Landlord
Rented:
Private
landlord
Rented:
Other
Berners
Holbrook
Babergh
England
5.10 Economic development
It has not been possible given the time available to do an in-depth review of Berners and
Holbrook wards however the general themes that affect Suffolk and Babergh as a whole give
useful insights into what is likely to be happening in the Shotley Peninsula (22).
Page 31

5. Baseline Assessment
Rural Suffolk and the Shotley Peninsula are characterised by demographic growth combined
with a decline in the numbers of young people. The loss of young people is driven partly by
the lack of higher education opportunities within the county and partly by the lack of
affordable housing and good quality job opportunities.
Rural Suffolk and the Shotley Peninsula are characterised by an economy with low levels of
unemployment but the area is also one with relatively low wage levels and with a high
incidence of employment in sectors which are declining nationally. There has been a negative
economic growth rate in Babergh of -5.6% between 1998 and 2000. The key employment
sectors are manufacturing and wholesale and retail with only modest employment in the
‘high-tech’ area of telecommunications. Tourism (hotel and catering jobs) accounts for
around 10% of total rural employment.
Rural Suffolk and the Shotley Peninsula appear to be characterised by a lack of
entrepreneurship as evidenced by a low rate of new business start-ups.
5.11 Education
Less than 25% of Berners and Holbrook residents have no qualifications, with Berners having
more residents with no, level 1, level 3 and other qualifications. In contrast, Holbrook has a
greater proportion of level 2- and level 4/5-qualified residents.
Figure 5.15 Rates of home ownership and renting on the Peninsula compared to Babergh and England & Wales
0%
5%
10%
15%
20%
25%
30%
35%
No qualif icatio ns Highest qualif icatio nattained level 1*
Highest qualif icatio nattained level 2**
Highest qualif icatio nattained level 3***
Highest qualif icatio nattained level 4/5#
Otherqualif icatio ns/level
unkno wn
Berners
Holbrook
Babergh
England
There are a greater number and proportion of students in Holbrook than Berners in all age
categories (see Table 5.3).
Page 32

5. Baseline Assessment
Table 5.3 Total number and proportion of students aged 16-74 on the Peninsula compared to Babergh and England & Wales
Berners Holbrook Babergh England & Wales Total number of full-time students and schoolchildren aged 16 to 74
101 315 2805 2,648,992
% of total resident population
3% 12% 3% 5%
Total number aged 16 to 17 66 232 1,795 1,014,284
Total number aged 18 to 74 35 83 1,010 1,634,708
Of the students leaving Year 11 almost 85% in both Berners and Holbrook go on to further
education compared to 75% in Babergh as a whole. A further 7.7% and 11.5% respectively go
on to employment with training with 7.7% being unemployed in Berners compared to less than
1% in Holbrook and 6% in Babergh as a whole.
5.12 Environment
The natural environment on the Peninsula is excellent (23). It is an area of outstanding
natural beauty (AONB) and the Stour & Orwell Estuary is also an area of Special Scientific
Interest (SSI). Levels of air pollution are low and fall well within national air quality
guidelines.
5.13 Culture and leisure
There is one sports centre on the Peninsula, which is part of Holbrook High School. There are
no leisure facilities in Shotley Village itself. The facilities provided by Holbrook Sports Centre
are floodlit synthetic turf and tarmac tennis courts, floodlit multi-games area, gymnasium
playing fields, and an artificial cricket wicket (24).
There is a concerted community-based effort to enhance the community development and
youth work activities on the Peninsula but this has proved difficult and there continue to be
very poor amenities and facilities for young people at the end of the Peninsula (25, 26).
Page 33

6. Evidence Base
6. Evidence Base
6.1 Introduction
This section summarizes the ways in which the social and economic factors acting in rural
areas affect health and health inequalities. It is drawn from two key sources: the East London
evidence base sited at Queen Mary & Westfield College, University of London website and The
Health Impact Assessment Unit evidence base sited at the University of Northumbria website
(4, 27).
The ten key themes explored are the impact of:
• health services
• social exclusion
• social capital
• housing
• transport
• education
• culture & leisure
• built environment
• economic development
• crime
6.2 The impact of health services provision on health and health inequalities
It is widely accepted that health services improve the health of people; however there are a
number of key factors that determine how health services help to improve health and reduce
health inequalities.
One of the foremost factors affecting the relationship between health services provision, the
health of populations and health inequalities is access. Levels of access and need in rural
areas must be assessed in their own right. Distance-decay studies have drawn attention to the
possibilty of access problems for rural residents, but do not provide a solution to the problem
(28). Studies in the 1990s which have addressed the impact of distance and rurality on the
outcome of particular diseases (asthma, diabetic retinopathy, cancer) have shown poorer
outcomes for rural residents, often because disease is at a more advanced stage at diagnosis.
Although access problems are implicated in these studies, it is difficult to identify the
particular components of access which are to blame, for example is it poorer diagnostic
facilities, or a feature of rural populations that they present later.
Studies into the uptake of breast screening in remote areas also provide evidence that
decreased utilisation with increasing distance is caused by problems with access. These
Page 34

6. Evidence Base
studies included qualitative data which addressed various components of access. Distance was
found to be the most significant factor in non-attendance in these studies. Other factors
include lack of car ownership, full-time employment and being married.
The impact of distance on emergency care and outcomes from road traffic accidents is not so
clear-cut. Studies into the impact of distance on emergency care provide mixed results,
whilst studies into the role of distance on outcome from road traffic accidents have provided
little evidence that outcome is worse due to greater distances to hospital. More research is
required to answer these particular questions.
A second important issue is what features of rural areas are important in affecting access for
patients (29). There is strong evidence in the literature that distance, travel times and
transport are the most important factors in access for patients in rural areas. There is also
evidence that office hours, appointment times, rural culture, lack of anonymity and stigma
affect access. Stigma not only affects the patients (for example farmers accessing mental
health services), but there is evidence that it can also influence GP decision making on
whether to treat ‘emotionally charged’ diseases in the community.
It is clear that the particular problems rural residents face accessing health services do
impact upon their health. It is moreover to be expected that problems accessing health
services will be greater among particular groups, such as expectant mothers, those with
young children, lone parents, children and young people, the unemployed, those with
disabilities, and the elderly, i.e. upon the most vulnerable sections of the community, and
will therefore act to compound existing health inequalities.
Important factors other than access include:
• The availability of health care services and facilities
• The quality of health care
• Accessibility through the gate-keeping processes within health care facilities
• The diagnosis of conditions
• The availability of treatments
• The availability of after-care at home and in the community
• Access to drug and other treatments via local dispensary or pharmacies
• The availability of social care facilities and services
• The quality of social care
• Accessibility through the gate-keeping processes with the social care facility
• An appropriate level and length of social care
Page 35

6. Evidence Base
6.3 The impact of social exclusion on health and health inequalities
A recent UK government report (30) defined social exclusion as:
"covering those people who do not have the means, material or otherwise, to participate in
social, economic, political and cultural life"(30, p131).
This definition centres on not having a choice; true exclusion is therefore involuntary.
Barriers such as sustained low income brought about by unemployment, ill health, illiteracy,
being an informal carer or lack of personal skills, may exclude individuals from participating
in 'normal' life. A recent UK national survey (31) identified four aspects of social exclusion:
• Impoverishment or exclusion from adequate income
• Labour market exclusion
• Service exclusion, in particular financial, food, energy and health
• Exclusion from social relations
Impoverishment or exclusion from adequate income
Poverty and lack of income excludes people by reducing there opportunities to participate in
social and cultural activities and in taking part fully in social norms and cultural practices.
Labour market exclusion
Employment is a key resource for self-esteem and social status as well as income. This
exclusion from the labour market can occur through ill health, discrimination or lack of skills.
Service exclusion, in particular financial, food, energy and health
Financial services exclusion
Those with very low incomes tend not to have bank accounts with facilities such as cheque
guarantee cards and very few have an overdraft facility (32). Without bank accounts, credit is
difficult to get and expensive. Few people on low incomes have money to save, and loans are
often needed urgently (33). The problem has been further compounded by the closures of
neighbourhood bank and building society branches so that even for those who do have bank
accounts, access becomes problematic. Within deprived neighbourhoods, there tend to be
high levels of informal borrowing with high interest rates. Disadvantaged households,
excluded from mainstream financial services, have to rely on unregulated and expensive
alternatives (32).
Some people may experience short periods of financial exclusion at periods in their lives
whilst for a small number it may be a long-term or even a life-long problem (32).
Rowlinson's (34) qualitative research notes the recent shift in British government policy from
state planning to individual planning. For individuals suffering long-term financial exclusion,
future planning is limited by economic insecurity and lack of resources. People enduring less
security and low incomes tend to 'live in the present'.
Page 36

6. Evidence Base
Access to food outlets
Increasingly, out of town shopping provision, with its economies of scale, tends to provide
cheaper and fresher healthy food than neighbourhood food shops (35), and in many cases
contributes to the closure of local shops. Studies show that low-income groups may be denied
access to affordable and healthy food, and that this is for a number of reasons (36-38).
Specifically, low-income groups:
• Often rely on public transport
• May find the cost of public transport prohibitive
• Are hindered by transporting bulky goods on public transport
• Cannot always afford to buy a large range of goods during one shopping trip
• May have problems with storage (for example having only limited frozen food storage)
• May have problems with childcare
Energy services exclusion
There is concern about the relatively high costs of ensuring an adequate gas or electricity
energy supply for heating and cooking in the home. Poor quality housing is associated with
poor health (39). Damp housing may increase the prevalence of allergic and inflammatory
lung diseases such as asthma (39). Older persons are susceptible to hypothermia (40). Lack of
money may lead to inadequately heated housing; this has been referred to as 'fuel poverty'
(41). Whilst this aspect of social exclusion may be addressed through increasing state
benefits, Acheson (42) has recommended policies to improve insulation and heating systems
in new and existing buildings.
Private companies often deliver energy services such as gas and electricity. Privatisation and
restructuring have left less affluent neighbourhoods and social groups with only limited access
to services, which could be considered essential for full participation in contemporary society
(43). Non-availability of services ('collective exclusion') is a bigger barrier than non-
affordability ('individual exclusion') (44).
Health services exclusion
There may be low levels of health care provision, particularly of primary care, in deprived
areas that most need them (45). Some studies suggest that there is an unequal distribution of
the quality of care according to geography and social class (46).
A number of studies have investigated whether the development of fundholding in general
practice has led to a reluctance to deal with cases or social groups that are likely to add
disproportionately to costs (see for example Glennerster et al (47); Newton (48)). Generally
findings point to the disadvantage of patients of non-fundholders, particularly in terms of
hospital treatment (49), rather than to any discrimination by fundholders.
Page 37

6. Evidence Base
Exclusion from social relations
The term social relations encompasses interpersonal relations both within and outside of the
home. Studies consistently show a relationship between low levels of social networks and age-
adjusted adult mortality for almost every cause of death (see for example Avlund (50), House
et al (51)). Weak social ties have been particularly related to coronary heart disease mortality
(52, 53), although a small number of studies do not repeat this finding (see for example Olsen
et al (54)).
There has been a focus on the 'social support' aspect of social relationships, that is the
practical and emotional support that individuals feel they receive from family, friends,
neighbours and colleagues. Studies have shown that lack of, or perceived lack of, social
support is associated with symptoms of depression (see for example Bowling and Browne (55);
Holahan et al (56)). Evidence points to older persons who are socially isolated being at
increased risk of depression (57). The perceived adequacy of social support seems more
important than the availability (58).
Matthews et al (59) note that social support has been related to a range of positive health
outcomes for a number of conditions. These include:
• Improved immune status following drug therapy for cancer (60)
• Various chronic conditions such as rheumatoid arthritis (61)
• Perinatal health of mothers and children (62, 63)
• Diabetes (64)
• Anorexia and bulimia nervosa (65)
• Pregnancy outcome (66)
• Post-traumatic distress order (67)
• Well-being and depression (68,69)
6.4 The impact of social capital on health and health inequalities
Defining the term ‘community’ has received much attention in the literature, and an all-
encapsulating definition has yet to be found. Young and Willmot's (70) classic description
(summarized by Pereira (71) below) best captures the meaning with which the term is used in
this context:
"the existence of some kind of collective life that residents identify with, and a social life and
social relationships based on reputation rather than status (i.e. on who people are to each
other rather than how much they own or possess)" (71, p.5).
‘Social capital’ has been put forward (72, 73) as a useful concept for explaining how
community level social factors might influence health. The concept was first identified in
1961 by Jacobs (74) and subsequently updated by other authors (75, 76). It has since been
extensively developed by Coleman (77), Portes and Sensenbrenner (78), and Putnam (79-81).
Page 38
6. Evidence Base
Putnam's definition of social capital has been summarised (82) by its four defining
characteristics:
• The existence of community networks;
• Civic engagement (participation in community networks);
• Local identity and a sense of solidarity and equality with other community members;
• Norms of trust and reciprocal help and support.
Putnam (79) suggests that social capital can identify the human resources that members of a
community have access to. The higher the level of human resources, measured in terms of
the four characteristics cited above, the more likely it is that community members are
working together for the common good. The more people work together, the more social
capital is produced and the community becomes more 'cohesive', or more co-operatively
drawn together.
Social capital and health
Some authors have begun to address the question of establishing links between health and
social capital (see for example Gilles et al (83)). Different studies have looked at particular
aspects of social capital. In Scandinavia, surveys have measured social participation in terms
of actively taking part in organised groups and associations (84) and in terms of attending
cultural events (85). These surveys suggest that social participation may be a strong predictor
of longevity. In the US, a study (86) showed social and productive activities to be as effective
as fitness activities in lowering the risk of death among older Americans. Another study (87)
found that after controlling for individual psychosocial resources including mastery, self-
esteem and social support, membership in voluntary associations makes a significant
contribution to reducing distress. These studies corroborate the potential benefits of social
capital for health.
Campbell and colleagues (82) suggest that within the disciplines of the sociology of health and
social psychology, there is an extensive literature that could be drawn on to explicate the
mechanisms through which social capital might have beneficial health effects. They identify a
number of factors that may interact with each other at the individual, inter-individual,
organisational, community and macro-social level and which may promote or inhibit social
capital. These encompass:
• Self-efficacy at individual level;
• Social support and social networks at inter-individual level;
• Perceived inequalities at organisational level;
• Empowerment at community level;
• Macro-social factors at macro-social level.
Page 39

6. Evidence Base
Stansfeld (88) reviews the evidence for links between social support and health. His key
points may be summarized as follows:
• Social support may protect health by buffering against the effects of life events which
may be damaging to health. There may also be direct effects in promoting a sense of
control of one's life and self worth
• Social support may have physiological effects through the hormonal system, on the body's
response to stress and functioning of the immune system
• Social support reducing social isolation is associated with reduced levels of mortality from
cardiovascular disease, accidents, suicide
• Better social support is associated with reduced risk of cardiovascular disease
• People with better social support may cope with illness better and have better prognoses
when ill
• Better social support is beneficial to mental health; associated with lower levels of
anxiety, depression. There may be gender differences in the importance for health of
social support from different sources.
Social capital and income inequality
Social capital has been used, for example by Wilkinson (89, 90), as an explanatory construct
that defines the relationship between health and social inequalities in developed countries.
Epidemiologists (91) have used measures of social capital to indicate levels of social cohesion
in a community or society. They stress that social cohesion is undermined by increased
income inequality between rich and poor. Income inequality can cause hostility and mistrust
(92). This body of work may be beginning to point to social capital being an important
mediator of the association between income inequality and health.
Critics of social capital
The concept of social capital and its use as a measure and predictor of health has its critics.
Cross-disciplinary academics and practitioners (see for example (93-95)) suggest that a
community's social capital cannot as yet be measured, as the concept remains under-
theorised and poorly developed. These critics point out that:
• Social capital is too broad a concept to be empirically useful
• It has been presented as an unmitigated good without due consideration of the power of
coercive groups
• It is put forward as a panacea to public health problems, without an analysis of underlying
political and economic determinants
• It may ultimately encourage governments and policy makers to retreat from welfare
spending
Page 40

6. Evidence Base
Social capital and health promotion
Despite its critics, Hawe and Shiell (72) contend that the concept of 'social capital' encourages
health promoters to move away from individual level interventions aimed at redressing health
inequalities. Social capital also brings together practitioners, researchers and theorists from
sociology, ecology and geography, in order to counterbalance the dominance of the
behavioural sciences in much of the health promotion literature.
In summary, the concept of social capital may help trace the complex and interactive
mechanisms that link social inequalities and health, and may offer realistic solutions to health
inequalities.
6.5 The impact of housing on health and health inequalities
Shelter is a primary human requirement (96). It should be sufficient to provide protection
from the hazards of the outdoor environment, but without replacing them with new and
internal threats (96). Ambrose (97) considers 'housing quality', and uses the work of
Seedhouse (98) for a definition:
"A satisfactory housing standard is one that provides a foundation for, rather than a barrier
to, good physical health, personal development and the fulfilment of life objectives" (98,
p.7).
Housing policy in the 1930s and 1950s concentrated on slum clearance programmes in order to
eradicate some infectious diseases and improve population health. Subsequent policy
emphasised issues of home ownership, housing management, access, and costs (99). Currently
both housing and health government policies acknowledge that housing can have a significant
influence upon the physical and mental health of residents (100, 101).
Within the social rented sector, there is a tendency for concentrations of poor quality housing
to occur on the periphery of towns and cities (102). Unfit dwellings are occupied
disproportionately by older single persons and are often older, privately rented properties
(103).
Housing and its health impacts
Research evidence consistently identifies the following aspects of poor housing:
• Dampness and cold
• Indoor air quality
• Fires and accidents
• Infestation by pests
• Noise
• Overcrowding and density of housing units
Page 41
6. Evidence Base
Dampness and cold
Cold and poorly ventilated homes become damp as a result of condensation (104), which in
turn leads to mould growth (105). Damp housing conditions contribute to reduced indoor
temperatures (106). The major cause of damp in dwellings is a combination of location,
building fabric, type of building, and damp, rather than the behaviour of the inhabitants (107,
108).
The most vulnerable to damp and cold conditions are low-income groups: unemployed;
retired; single parents; chronically sick persons; people with disabilities (106). They have the
least income yet spend a greater percentage on heating than other groups. Inadequate,
inefficient, and uneconomic heating systems as well as insulation are implicated in excess
winter deaths (109).
Whilst there is some debate about inherent methodological limitations, a substantial body of
research suggests the following:
• Mould spores lead to respiratory problems (e.g. asthma, rhinitis (runny nose), alveolitis
(inflammation of the lung) and other allergies (105, 109, 110)
• Allergic reactions, infections and toxic reactions to spores develop with repeated exposure (105).
Children, older persons and those with existing illness are particularly at risk (105)
• Some bacteria and viruses that cause infection are more likely to thrive in damp conditions (105,
111, 112)
• Children are twice as likely to suffer from wheezing and chesty coughs as those who sleep in dry
homes (103) and are more likely to experience gastrointestinal upsets, aches and pains, fatigue and
nervousness (107)
• Adults are more likely to report aching joints, nausea, blocked nose, breathlessness and poor
mental health (112)
• Depression has been associated with damp housing , particularly in women (113).
A reluctance to invite friends or children's friends into the home because of the
embarrassment of deteriorating surfaces and associated smells may also lead to loneliness
and isolation (114).
Indoor air quality
Some materials widely used in building construction can expose residents to direct health
hazards (99). Asbestos materials have been used for insulation purposes and to reinforce
building materials (109). When asbestos is disturbed or deteriorates, it presents a risk to
respiratory health; blue asbestos in particular is more hazardous than white (109).
Formaldehyde has been widely used in foam insulation, synthetic carpets, and pressed wood
products (109). Efforts to make homes more airtight to conserve heat and reduce heating bills
e.g. double-glazing, may increase health risks by releasing formaldehyde vapours from cavity
walls (115). Formaldehyde can cause irritation of the mucous membranes (109).
Page 42

6. Evidence Base
Evidence reviewed by Ambrose et al (104) suggests that repeated exposure to nitrogen
dioxide from gas burning appliances may aggravate existing lung disorders; increase
susceptibility to respiratory infection particularly in children; and contribute to the
development of chronic pulmonary disease (116). However, comparing households that used
gas and those that used electricity for cooking, Kellar et al (117) found no difference in
respiratory illness.
In their review of the literature Ambrose et al (104) also found that radon gas, a colourless,
odourless gas that is present in almost all rocks and soils, but is especially high in areas where
granite occurs, has been linked to the incidence of death from lung cancer (118) and myeloid
leukaemia (119). An estimated 75,000 homes are in need of remedial attention to reduce
radon gas levels (120).
Fires and accidents
Annually, an estimated two million people, mostly children and older persons, seek hospital
treatment as a result of accidents in the home. Poor housing conditions are often implicated
(99). Over 4000 of these accidents are fatal and account for a third of all fatal accidents (99).
Housing-related accidents are the most common cause of death in children aged over one
year (121, 103). Almost half of all accidents involving children are associated with
architectural features in and around the home (121, 103). More than 300,000 people over the
age of 65 require hospital treatment following housing related accidents (122). Risk of falls,
burns and scalds in kitchen areas, electric shock, falling objects relating to structural
instability, injury from doors and windows, fire, explosions, are some examples of housing-
related hazards (123). Poor lighting is also associated with falls, and with injury from doors
and windows.
Infestation by pests
Housing type, design, and building materials are significant factors in encouraging pests that
negatively impact on residents' health (124). The degree to which food is available is a major
factor in buildings that become infested. The most common pests causing infestation are
cockroaches and rats.
Cockroach infestation is a particular problem in system-built housing e.g. high-rise dwellings
where construction methods used pre-formed concrete panels made off-site for rapid
assembly on site. This sort of construction provides ideal spaces for cockroaches to
congregate e.g. service ducts (124). The main threats to health are:
• Germs transferred from house to house (109)
• Cockroach allergy - symptoms can vary from those similar to mild hay fever to anaphylactic
shock (109)
• Secondary health effects following the use of pesticides to kill cockroaches (109)
• Stress and personal inconvenience of infestation procedures (109)
• Feelings of stigmatisation as a result of infestation eradication procedures (125)
Page 43

6. Evidence Base
Rat infestations occur in buildings when there are poor facilities for, and bad practice in,
waste disposal. Rat infestations impact on human health in a number of ways. Rats are (124):
• Transmitters of plague
• Carriers of food poisoning organisms because of their occupation of sewers and drains
• Transmitters of leptospirosis or Weil's disease
Noise
Noise is perceived as unwarranted, offensive, and quite often as an uncontrollable intrusion
(126-130). When noise can be controlled it is less stressful. Predictable noise is less disturbing
than isolated events. The more unpredictable and inconsistent the noise the more stressful it
is (126-130). Predictable noise can be anticipated, and as a result adaptations made to
minimise its impact. Unwanted noise commonly comes from neighbours' barking dogs and
house parties. Tensions from unwanted noise can cause conflict between neighbours and may
result in assaults (125).
The effects of noise on health are many and varied. Noise may distort perceptions of others
within the environment and increase the potential for aggression (although this may only
occur when a person is already angry) (126-130). Intermittent, unpredictable, or
uncontrollable noise can stimulate physiological changes, undermine psychological health,
and at night, can interfere with sleep patterns. Physiological effects include elevated blood
pressure, increased heart rate, and increases in adrenal hormone output. Psychological
effects include nervousness, irritability, and interference with concentration. The effects of
prolonged sleep disturbance include anxiety, headaches, and chronic fatigue (drawn from
Hunt & McKenna (131)).
Overcrowding and density
The connection between overcrowded housing conditions, high room densities, health, and
the spread of infections, notably tuberculosis, has been recognised since the slum clearance
programmes of the 19th century (125, 115). Overcrowding is still regarded as a risk to health
(115).
The consequences of overcrowding on physical health are:
• The spread of infectious diseases (125)
• Increased incidence of accidental deaths (132, 133)
• Increased incidence of asthma (132, 133)
• Increased incidence of cardiovascular diseases (99)
• Increased incidence of chronic bronchitis (132, 133)
• Increased incidence of dysentery (132, 133)
In relation to mental health, overcrowding may result in:
• Slow development in children (99)
• Stress (123)
• Depression (99)
Page 44
6. Evidence Base
Houses in multiple occupation (HMOs) have a long history of overcrowding and poor housing
conditions (115). HMOs are typically characterised by shared amenities i.e. washing facilities,
toilets, food storage, and cooking facilities. HMOs include houses that have been converted
into flats, student accommodation, and hostels (103, 115).
In addition to the above-mentioned health risks from overcrowding, homeless persons may
also be at risk of:
• Suicide
• Substance abuse
• Loneliness and boredom
• Loss of self-esteem
• Relationship breakdown
• Behavioural problems in children
• Increased levels of domestic violence
• Risk of assault
• Limited access to health education and primary care
(Drawn from Matthews (123))
Homeless persons who have no shelter and live on the streets have an increased risk from
many of the above mentioned health impacts. Life expectancy for those sleeping rough is 42
years compared to the national average of about 74 years for men and 79 years for women
(123).
Density
Density is distinct from overcrowding and more generally associated with high-rise housing. As
such it falls outside the scope of this review, which concentrates on those social and
economic determinants of health relevant to the HMS Ganges Housing Development Proposal
for the Shotley Peninsula.
6.6 The impact of transport on health and health inequalities
Transport plays an important in enabling people to reach key services like health care
facilities and schools; go to their place of work; and keep in touch with family and friends.
Access
Transport’s primary function is to enable access to people, goods and services ((134) cited in
(135)). In so doing transport also promotes health indirectly through the achievement and
maintenance of social networks and by enabling people to access employment opportunities.
Egan and Petticrew (136) state that the evidence on out-of-town bypasses indicates that they
reduce the incidence of injury accidents on main routes through or around towns. Secondary
roads within towns may be affected differently (e.g. Andersson’s study suggests that bypasses
Page 45

6. Evidence Base
lead to an increase in injuries on secondary roads and intersections (137)). Unfortunately,
detailed accident statistics are not always available for secondary roads (138). This perhaps
explains a relative lack of robust evidence on how new bypasses affect the distribution of
injury accidents across broader road networks.
As well as impacting directly on health, traffic also has a range of indirect health effects, for
example through its impact on social networks. As traffic volumes increase people’s sense of
neighbourliness and the geographic density of their friendships decreases (see (139) cited in
(140, p102)).
Certain population groups experience a lack of access to transport disproportionately more
than others. These include women, children and disabled people, people from minority ethnic
groups, older people and people with low socio-economic status. These groups find they have
limited access to services such as shops and health care and they tend to spend a higher
proportion of their resources on transport (135, p56).
Moreover, the same people who are forced to rely on public transport as their sole means of
transport are punished with higher transport costs. The cost of rail and local bus fares has
risen by nearly one third in real terms since 1980, whereas motoring costs have decreased by
5% over the same period (cited in 135, p56). Public transport must be affordable if it is to
contribute to social inclusion.
Accidents
The combined health effects of road traffic injuries and transport-related air pollution make
a significant contribution to overall morbidity. It has been estimated that they account for 1%
of all annual deaths in London, for example. (141). A community-based case-control study
(142) looking at traffic volume, speed and curb-side parking found that the risk of injury,
especially for child pedestrians, increased with traffic volume, a high density of curb parking
was associated with increased risk, and risk increased with mean traffic speeds over 40kph.
Worldwide, approximately one-half of the motor vehicle fatalities are due to pedestrian-
motor vehicle collisions. Children are among the groups at highest risk of pedestrian injuries,
especially when the amount of walking done by children is taken into consideration. The risk
to child pedestrians is very clearly related to the number of roads they cross (143). The
greater the number of roads crossed, the higher the risk of pedestrian injuries. Poorer
children under the age of 9 have higher rates of pedestrian injuries at least in part because of
their increased exposure to traffic. The reduction in pedestrian fatalities to children in the
US, UK, and other countries in recent years is probably largely due to a reduction in walking
by children (144).
Page 46

6. Evidence Base
Pedestrian injuries are most common among 5-9-year-old children, and in this age group,
pedestrian injuries are the most common cause of serious head trauma. Pedestrian motor
vehicle collisions are qualitatively different from other types of trauma in that very few of
the victims escape injury. In contrast, 94% of occupants of vehicles involved in crashes are
uninjured. Police data under-report pedestrian injuries by one-half to two-thirds. The most
common type of action by the child leading to pedestrian injuries is the mid-block dash/dart-
out and intersection dash actions. These account for 60-70% of the total for children under
the age of 10. Incidents in which children are run over by a vehicle backing up are limited
primarily to the youngest age group - toddlers.
Pedestrian injuries are a complex problem, for which no single intervention is completely
effective. Control requires intervention at local and regional levels, and involves changes in
the host, agent and environment. The evidence for the effectiveness of interventions at these
various levels is highly variable.
The difficulty with changing behaviour, particularly children’s behaviour, makes
environmental modification particularly attractive. Changes in the traffic environment have
been a traditional component of pedestrian safety programmes for many years.
Comprehensive programmes, such as those in Europe, often go under the rubric of "traffic
calming". Traffic calming refers to a group of measures designed to control traffic, usually in
an urban residential area. The definition of traffic calming adopted at the 1997 international
ITE conference is, "the combination of mainly physical measures that reduce the negative
effects of motor vehicle use, alter driver behaviour and improve conditions for non-motorized
street users" (145). Measures are designed to reduce the number of commuters using
residential streets and to reduce the speed of remaining traffic. Measures can include
establishing a hierarchical road system, improving main roads to carry additional traffic and
restricting or removing traffic from residential streets with road closures or one-way
designations. Environmental changes designed to reduce speed include vertical changes in the
street (speed cushions, humped pelican crossings, raised junctions), lateral changes in the
street (off-set intersections), constrictions (narrowings, pinch points, pedestrian refuges),
gateways at the entrances to the area, build-outs to protect on-street parking spaces, and
mini-roundabouts (traffic circles).
Epidemiological studies of environmental risk factors for child pedestrian injury indicate that
the likelihood of injury increases under the following conditions: increase in traffic volume
(13-14 times) or speed limit (6 times), absence of play areas (5.3 times), poorly protected
play area (3.5 times) and high proportion of kerbside parking (3.4 times) (146, 147) (Quoted
from Harborview Injury Prevention and Research Center (148). Accidents also show a social
class gradient (see for example (149) cited in (150). In the UK, road traffic accident deaths
for children in the poorest families (social class V) are more than 4 times greater than those
in the richest (social class I).
Page 47

6. Evidence Base
Children’s mobility is restricted through town-planning, road, and other safety information
and, importantly, the priority given to motorists in law (151). Children’s play territory has
been reduced as roads and pavements have become more and more dangerous. Children’s
psychological development may be impaired by curtailing their sense of independence and
personal mobility.
Carlin et al (152) conducted a cross sectional survey of six- and nine-year-old children in two
Australian cities to look at pedestrian activity in young children. They concluded that it is
important to measure unaccompanied street crossing as opposed to total streets crossed or
simply walking to school. All comparisons using indicators of socio-economic status show clear
trends toward less walking with higher socio-economic status. Unaccompanied street crossing
was associated with age, sex and maternal education. There was little difference in overall
walking levels between boys and girls but boys were significantly more likely to cross streets
unaccompanied. The predominant use of cars for transporting children may lead to an
increased risk of road traffic accident for children whose parents are unable, or less willing,
to drive their children.
One of the biggest problems facing rural villages is the very real problem of driver compliance
with speed limits (153). “The differential between the speed limits inside and outside the
village can be large, and so speed observed through such villages can be particularly high
compared to what is appropriate for the conditions. Thus potential for conflict between
pedestrians, cyclists and motor vehicles can be great” (154).
Air quality
Reducing air pollutants due to traffic benefits health. Exposure to air pollutants is associated
with earlier deaths and hospital admissions for respiratory and cardiovascular disease.
Evidence regarding the effects of particles, ozone and sulphur dioxide is sufficient for the size
of the effect to be quantified. For nitrogen dioxide and carbon dioxide there is insufficient
evidence to allow quantification but there is evidence to suggest exposure affects health
((155) cited in (156)).
The Government Committee on the Medical Effects of Air Pollution (COMEAP) (157) state that
air pollution:
• Has short term and long term damaging effects on health
• Can worsen the condition of those with heart disease or lung disease
• Can aggravate but does not appear to cause asthma
• In the longer term, probably has additional effects on individuals including some
reduction in average life expectancy, though the extent of this is not fully understood
at present
Page 48

6. Evidence Base
Key air pollutants include carbon monoxide, particulate matter, oxides of nitrogen and
sulphur, ozone, benzene and other hydrocarbons (157). Some are strong irritants, like sulphur
dioxide, and some are carcinogenic, notably benzene, 1,3-butadiene and some polycyclic
aromatic hydrocarbons (PAHs) (157). The size of the effect will vary depending, amongst
other things, on the concentration of the pollutant(s) and the period of exposure. An
individual’s exposure to pollutants can vary greatly. Most healthy individuals will not notice or
suffer from any serious or lasting ill effects of pollution that are commonly experienced in the
UK, even when levels are described as “high” or “very high” according to the current criteria.
However, our knowledge of the effects of air pollutants on individuals as a result of their
exposure both in the home and at work is incomplete. Some people with diseases of the
airways (such as Chronic Obstructive Pulmonary Disease [COPD] and asthma) may be adversely
affected by day-to-day changes in the levels of air pollutants. This is not surprising since
people with asthma are especially sensitive to a range of irritant substances.
Environmental Noise
A DETR (Department of Environment, Transport & Regions) report ((158) cited in (141, p54))
concludes there is sufficient evidence that exposure to noise has detrimental effects on
performance in school children; the evidence is not conclusive for adults. Road traffic noise
at an intensity of 50 to 60 dBA increases the time taken to fall asleep. In particular, the
number of noise events seems important in this effect ((159) cited in (160, p20)). The first
third of the night seems to be the time that is most vulnerable to sleep disturbance. A study
of Japanese women found that living less than 20 metres from a busy road predicts insomnia,
adjusting for many relevant confounding factors ((161) cited in (160, p20)).
Other authors have looked at the impact of noise on specific health conditions. Stansfeld et al
(160_68) write that “… noise per se, in the community at large, does not seem to be a
frequent, severe, pathogenic factor in causing mental illness but that it is associated with
symptomatic responses in selected subgroups of the population.” (161, p73) Many of these
studies have been carried out on aircraft noise but a British study of road traffic noise did find
a small association between one traffic noise level index and a mental health symptoms scale
(162). "Altogether, there is not strong evidence that noise causes mental ill-health although it
is possible that certain vulnerable groups, who are exposed to noise over which they have no
control, may be vulnerable to mental health problems. What is certain, is that those with
existing mental health problems, usually either depression or anxiety, are more prone to be
annoyed and disturbed by environmental noise exposure than the general population.” (160)
There is little evidence from community studies that environmental noise is related to high
blood pressure but there is some evidence to suggest that environmental noise may be a risk
factor for coronary heart disease, in people who live in noisy areas with outdoor noise levels
of more than 65-70 dBA, although the size of the effect is likely to be small (163,164).
Babisch and colleagues’ (164) careful analyses within the Caerphilly Study do suggest a small
Page 49

6. Evidence Base
increased risk of coronary events in relation to noise, but the association between noise and
coronary risk factors is inconsistent and may be confined to groups annoyed by noise (165,
166). Overall, the risk of coronary heart disease associated with road and aircraft noise
exposure is small, especially compared with other coronary risk factors such as smoking.
6.7 The impact of education on health and health inequalities
Education, training and learning play important roles in providing the basis for economic
growth, social cohesion and personal development (167). Education is positively correlated
with employment earnings. Independently of qualifications adult literacy has a strong impact
on earnings (168). Educational attainment in one generation has positive effects on the
educational attainment of the next generation: better schooled parents have children with a
higher level of cognitive development as well as children with higher future earnings
potential (169).
People with higher educational qualifications tend to be healthier and have a lower take of
social benefits (169). An additional year of schooling is associated with reduced average daily
cigarette consumption for both men and women (170). People with more schooling tend to be
less overweight and engage in more exercise per week than less educated people. People
with more schooling are better able to identify relevant health related information and using
this information in a constructive manner. Whitty et al (171) describe how improved
educational attainment in childhood is linked to a range of improved adult health outcomes.
The importance which a child’s parents and the child’s social network attach to learning have
a profound influence on children’s attitudes and behaviour (167). Coleman (168) emphasised
the importance of a surrounding community of adults for young people who are ‘embedded’
in enclaves of adults closest to them: social networks are important for learning. Different
types of supportive social relations among adults help learning e.g. help with homework, out
of school activities and direct parental involvement in school activities (168). Strong
neighbourhood connections can provide an environment which reinforces achievements in
school. Exchange and support between parents, schools and children can provide increased
resources necessary for improving children’s well-being (172).
An analysis of the British National Child Development Study (173) shows that during middle
childhood children spend less time at home and more time at school and with their peers.
During this time the quality of their interactions with teachers and other students becomes a
major contributor to their development. The period from about 10-16 years of age
encompasses the transition from childhood to adolescence (173).
Messages from school can undermine those at home (174) e.g. standards of cleanliness may be
lower at school than at home, the standard of school food may contradict messages to eat
Page 50

6. Evidence Base
healthily and messages to take exercise and take care on the roads may be weakened by
teachers who drive and on occasion pose a threat to children.
6.8 The impact of culture & leisure activities on health and health inequalities
Physical activity may play an important role in the management of mild-to-moderate mental
health diseases, especially depression and anxiety (175). Although people with depression
tend to be less physically active than non-depressed individuals, increased aerobic exercise or
strength training has been shown to reduce depressive symptoms significantly. Acute anxiety
responds better to exercise than chronic anxiety; studies of older adults and adolescents with
depression or anxiety have been limited, but physical activity appears beneficial to these
populations as well.
The list of health conditions associated with low levels of exercise includes some major
causes of death and disability (176). Exercise has the capacity to diminish morbidity and
mortality within the population, for example in relation to:
• Coronary artery disease
• Systemic hypertension
• Obesity
• Emotional disorders
• Incapacity of ageing
• Osteoporosis
• Diabetes mellitus
• Chronic back disease
• Athletic injuries
This list is composed almost exclusively of disorders that affect the health of adults, but it is
important to note that most involve lifelong processes that begin during the child or
adolescent years and surface clinically in later adulthood.
6.9 The impact of the built environment on health and health inequalities
The design of the built environment is important for psychosocial health. Feelings of safety
are enhanced if there are more people moving through an area; this suggests it is the isolated
areas that become vulnerable to crime (177). The majority of victims of property crime suffer
some degree of psychological harm (178). Crime Concern (179, p11) cite a study of UK
burglary victims which found that feelings of intrusion and emotional distress outweighed
feelings of loss or damage.
Access to open space can improve levels of exercise in a community, and thereby contribute
to reducing the current high rates of obesity, cardiovascular disease, diabetes and arthritis.
The impact on exercise levels is likely to be greatest in children. Access to green spaces can
Page 51
6. Evidence Base
improve social interaction and community activities. This can, in turn, contribute to reducing
levels of stress-related problems, and can contribute to reducing autistic spectrum disorders
and attention deficit disorder in children (180).
6.10 The impact of economic development on health and health inequalities
Economic development is an important factor in increasing social inclusion. Neighbourhoods
require local work opportunities to develop the bridging ties necessary to generate inclusive
social capital and better health (181). Most of London’s inner-city is within twenty minutes
travel of the largest employment catchment area in Europe, and regeneration programmes
should support and create potential for small and medium-size enterprises so they are able to
gain access to these opportunities (182).
The health consequences of employment and unemployment are directly contingent upon the
quality of the work available ((183) cited in (4): the existence of employment opportunities
does not necessarily lead to health improvement. The groups which face the highest risk of
experiencing the adverse effects of unemployment appear to be middle-aged men, young
people who have recently left school, the economically marginal such as women attempting
re-entry to the labour market and children in families in which the primary earner is
unemployed (184).
Likewise job creation does not necessarily 'trickle down' as job opportunities for the long-
term unemployed, and is neither a sufficient, nor necessary, condition for reducing long-term
unemployment (185). Ethnic minority unemployment is more than double that of comparable
white sub-populations (186). Employment policy should include measures to tackle possible
discrimination by employers and better targeting of vacancies to long-term unemployed
people.
6.11 The impact of crime on health and health inequalities
People who live in rural areas fall victims to the same types of crime and disorder as people
elsewhere and suffer the same types of problems. These problems may be compounded by
other aspects of rural life, for example, a lack of services, physical isolation and social
exclusion. There are also crimes that are peculiar to the countryside, such as thefts of
livestock and farm equipment, wildlife crime and mass trespass. Although evidence from the
British Crime Survey 2001 indicates that the level of general crime is lower in rural areas, the
survey also shows a widespread perception that crime rates in rural areas are rising (187).
There is a lack of research looking at the direct links between fear of crime and health. One
survey reports feelings of stress, smoking, drug dependence and loss of confidence ((188_123)
in (179)). A range of long-term health effects are associated with victimisation. Increased
Page 52

6. Evidence Base
rates of cigarette-smoking, alcohol and other substance abuse, health care neglect, risky
sexual behaviours and sleeping and eating disorders are all associated with physical and
sexual assault (in source 179, p6). Few studies consider intangible losses incurred by victims
of crime which include loss of quality of life, pain and suffering, impact on the health of
secondary victims, witnesses of crime and, the fear of crime (189). Witnesses of crime can
also suffer psychological and psychosomatic problems (189).
Young people face high levels of victimisation and also greater socialisation into fear having
grown up in an era in which crime influences parental control (190). This has resulted in far
fewer children exploring the outside world and as a consequence children have less
environmental knowledge, competence and confidence.
The risks of becoming criminally involved are higher for young people raised in disorganised
inner city areas, characterised by physical deterioration, overcrowded households, publicly-
subsidised renting and high residential mobility (191). It is not clear, however, whether this is
due to a direct influence on children, or whether environmental stress causes family
adversities which in turn cause delinquency.
Residential turnover
Researchers have found that residential mobility is associated with high levels of crime and
victimization (192). Residential mobility has one of the largest positive effects on violent
victimization of any neighbourhood characteristic, larger than poverty or racial composition
(193). Poverty contributes to criminality only in transient communities characterized by rapid
population turnover.
Design
Proponents of designing out crime justify it by stating that behaviour of offenders is highly
influenced by situational factors (194). Policy imperatives have tended to lead theory and
research rather than theory informing policy. Linking community safety entirely with the
design of the built environment shifts the focus away from the social and political causes of
crime (195). It is doubtful whether environmental changes can reduce attacks on women due
to most incidents taking place in the private realm, i.e. the home (195). Designing out fear is
underpinned by the assumption that most crime is opportunistic and offenders respond in a
mechanistic way to environmental stimuli (196).
One review (197, cited in 156) analyses the literature on the effectiveness of street lighting
improvements in preventing crime. The following conclusions are supported:
• Precisely targeted increases in street lighting generally have crime reduction effects;
• More general increases in street lighting seem to have crime prevention effects, but this
outcome is not universal. Older and US research yield fewer positive results than more
recent UK research;
Page 53

6. Evidence Base
• Even untargeted increases in crime prevention generally make residents less fearful of
crime or more confident of their own safety at night;
• In the most recent and sophisticated studies, street lighting improvements have been
associated with crime reductions in the daytime as well as during the hours of darkness;
and
• The debate about lighting effects has served to preclude a more refined analysis of the
means by and circumstances in which lighting might reduce crime.
Another review (198) analyses studies that have evaluated the effectiveness of closed-circuit
television (CCTV) in reducing crime, disorder and fear of crime in a variety of sites. CCTV can
be effective in deterring property crime, but the findings are more mixed in relation to
personal crime, public order offences, and fear of crime. (Cited in 156). Ditton (199) looked
at fear of crime and the effects of closed circuit television. The majority of people expressed
support for the CCTV installation. They thought it would make them feel safer. However,
when the actual as opposed to the prospective feelings of safety are compared over time
there was no improvement after installation: CCTV did not make people feel safer after it had
been installed. Respondents believed that CCTV is better than the police at detecting crime
but that police patrolling is more effective than CCTV in making people feel safer.
Neighbourhood incivilities
Neighbourhood incivilities are defined as low level breaches of community standards that
signal the erosion of accepted norms and values e.g. abandoned vehicles, litter, noise, street
homelessness, prostitution (200). These social and physical incivilities play a role in
generating feelings of fear but the role is modest and is mediated through perceptions of
crime risk.
School Environment
A survey of 2915 14-year-olds in a medium-sized county in Sweden looked at violent behaviour
and bullying and showed that bullying others in school was strongly linked to violent
behaviour and weapon-carrying on the streets, both among boys and girls. It was also found
that bullying others in school was related to being violently victimized on the streets. Bullying
behaviour in school is in many cases a part of a more general violent and aggressive behaviour
pattern and preventive efforts targeting individuals with bullying behaviour in school could,
according to the study, decrease violence among adolescents out in the community as well
(201).
Page 54

7. Policy Context
7. Policy Context
7.1 Introduction
This chapter summarises the policy context and policy evidence in relation to the proposed
HMS Ganges development, health and health and social care services.
The Government report Planning for the Communities of the Future (202) states that the
Government is pledged to making Britain better with decent homes for people and a good
environment for both town and country. In the report the Deputy Prime Minister argues that
“Planning is about more than statistics. It's about people. Local people living in local
communities”. (Foreword) Planning future communities and settlements is about the quality
of people's lives and providing decent homes, while ensuring a good quality environment for
people. Its vision is to accommodate the growing number of households while at the same
time protecting our precious countryside - without seeing rents, land and house prices or
homelessness spiralling.
Current planning policy guidance for housing encourages local authorities to ensure that they:
• Help meet the housing objective of offering everyone the opportunity of a decent home
and so promote social cohesion, well-being and self-dependence;
• Maximize the reuse of previously-developed land and buildings - through encouraging infill
and conversions - which assists regeneration and helps reduce the need for people to
travel; and
• Provide a mix of housing types and densities so as to meet the needs of different types of
households. (Context Point 12 ibid)
In planning for the projected increase in the number of households, the key issue should be
that of quality: the quality of life that we create, the quality of living environments we make
and the degree of choice that we can offer for all types of households. The most important
issue is not the precise numbers, but the quality of life in towns, cities and the countryside.
We need to provide enough housing, but it must be well designed and in the right place, to
create good living environments and more sustainable patterns of development. (Context
Point 14 ibid)
7.2 National Policy
PPG3 Housing (203)
The Government intends that everyone should have the opportunity of a decent home. They
further intend that there should be greater choice of housing and that housing should not
reinforce social distinctions. The housing needs of all in the community should be recognised,
including those in need of affordable or special housing in both urban and rural areas. To
Page 55

7. Policy Context
promote more sustainable patterns of development and make better use of previously-
developed land, the focus for additional housing should be existing towns and cities. New
housing and residential environments should be well designed and should make a significant
contribution to promoting urban renaissance and improving the quality of life.
PPG7 The countryside: environmental quality and economic and social development (204)
The Government's policies for the countryside are set out in the White Paper Rural England: A
Nation Committed to a Living Countryside. They are based on ensuring both rural prosperity
and the protection and enhancement of the character of the countryside. New building in
rural areas should contribute to a sense of local identity and regional diversity, and be of an
appropriate design and scale for its location. Modern designs should have proper regard to the
context for development, in relation to both the immediate setting and the defining
characteristics of the wider local area, including local or regional building traditions or
materials. Good design helps to maintain or enhance local distinctiveness, and can help to
make new development more acceptable to local people. Account should be taken of
feasibility and cost constraints when appraising development proposals. PPG1 provides
general guidance about design issues in relation to new development. People who live in rural
areas should have reasonable access to a range of services. Local planning authorities can
facilitate provision and help retain existing services by, for example, assessing the nature and
extent of rural needs, identifying suitable sites and buildings for development to meet these
needs, and promoting mixed and multi-purpose uses.
PPG10 Planning and Waste Management (205)
It is widely recognised that the way in which we, as a society, manage the waste we produce,
needs to change if we are to ensure that our environment is better protected both now and
for future generations. The Government intends to set out a policy framework for sustainable
waste management within which stakeholders can plan and take waste management
decisions, which reduces the amount of waste we produce, and, where waste is produced,
deals with it in a way that contributes to the economic, social and environmental goals of
sustainable development. The Government has recently published for consultation its revised
waste strategy “A Way With Waste”, with a view to final publication in late 1999 or early
2000. This will replace the 1995 White Paper “Making Waste Work: A Strategy for Sustainable
Waste Management in England and Wales” (Cm 3040, 1995). The land-use planning system has
an important role to play in achieving sustainable waste management.
PPG 13 Transport (206)
Our quality of life depends on transport and easy access to jobs, shopping, leisure facilities
and services; we need a safe, efficient and integrated transport system to support a strong
and prosperous economy. But the way we travel and the continued growth in road traffic is
damaging our towns, harming our countryside and contributing to global warming.
(http://www.planning.odpm.gov.uk/ppg/ppg13/01.htm)
Page 56

7. Policy Context
In response to this challenge, the Government set out its policy for the future of transport in
the White Paper “A New Deal for Transport: Better for Everyone” (July 1998), to extend
choice in transport and secure mobility in a way that supports sustainable development. The
“New Deal for Transport aims to deliver an integrated transport policy.
This means integration:
• Within and between different types of transport;
• With policies for the environment;
• With land use planning; and
• With policies for education, health and wealth creation.
PPG17 Open Space, Sport and Recreation (207)
Open spaces, sport and recreation all underpin people's quality of life. Well-designed and
implemented planning policies for open space, sport and recreation are therefore
fundamental to delivering broader Government objectives. Open space and sports and
recreational facilities that are of high quality, or of particular value to a local community,
should be recognised and given protection by local authorities through appropriate policies in
plans.
PPG24 Planning and Noise (208)
1. Noise can have a significant effect on the environment and on the quality of life enjoyed
by individuals and communities. The aim of this guidance is to provide advice on how the
planning system can be used to minimise the adverse impact of noise without placing
unreasonable restrictions on development or adding unduly to the costs and administrative
burdens of business. It builds upon the principles established in Circular 10/73 "Planning and
Noise", and takes account of the recommendations of the Noise Review Working Party which
reported in October 1990. It outlines some of the main considerations which local planning
authorities should take into account in drawing up development plan policies and when
determining planning applications for development which will either generate noise or be
exposed to existing noise sources.
2. The impact of noise can be a material consideration in the determination of planning
applications. The planning system has the task of guiding development to the most
appropriate locations. It will be hard to reconcile some land uses, such as housing, hospitals
or schools, with other activities which generate high levels of noise, but the planning system
should ensure that, wherever practicable, noise-sensitive developments are separated from
major sources of noise (such as road, rail and air transport and certain types of industrial
development). It is equally important that new development involving noisy activities should,
if possible, be sited away from noise-sensitive land uses.
Page 57

7. Policy Context
Development plans provide the policy framework within which these issues can be weighed
but careful assessment of all these factors will also be required when individual applications
for development are considered. Where it is not possible to achieve such a separation of land
uses, local planning authorities should consider whether it is practicable to control or reduce
noise levels, or to mitigate the impact of noise, through the use of conditions or planning
obligations.
Our Countryside: The Future - A Fair Deal for Rural England (209)
1.1. The countryside is important to all of us. Town and country are interdependent and the
needs of both have to be addressed together. But there are special problems in rural areas
which require a direct response and that is the focus of this paper.
1.2. The challenge for rural communities is clear. Basic services in rural areas are
overstretched. Farming has been hit hard by change. Development pressures are
considerable. The environment has suffered.
Circular 5/94: Planning out Crime (210)
Drawing from the previous disastrous attempts to renew inner cities and from the
characteristics exhibited by contemporary declining town centres, Circular 5/94 argues that:
"Desolate, sterile and featureless surroundings can engender feelings of hostility, anonymity
and alienation", but that "Used sensitively the planning system can be instrumental in
producing attractive and well-managed environments that help to discourage anti-social
behaviour. It can be used to make it harder for criminals to find targets" (DoE, 1994b, para.
4).
Circular 5/94 suggests that where large housing developments are being regenerated or new
development contemplated, they should feature distinct neighbourhoods of recognisable
character focused around necessary amenities.
Local Government Act (211)
The Local Government Act gives councils new powers to promote or improve the economic,
social or environmental well-being of their area. Councils are required to prepare
comprehensive community strategies with local strategic partnerships and to fully involve
local people in this process.
Quality of life is intimately bound up with the local environment. It is affected by the
availability of jobs, goods, educational and leisure opportunities. Individual health and
welfare depend on the quality of public services and the condition of the built and natural
environment. Community well-being means improving the conditions that help make healthy,
contented and prosperous local communities. (From the Office of the Deputy Prime Minister
(212))
Page 58

7. Policy Context
7.3 Regional and local policy
Suffolk Structure Plan (213)
• CS1 Provision will be made for development which helps sustain the economic and social
well-being of Suffolk, providing that the environment is safeguarded and development
does not give rise to problems of transport or service provision. Development will only be
acceptable where the community facilities and infrastructure necessary to serve it
already exist or will be made available at the appropriate time. In the latter case,
conditions will be attached to planning permissions and/or legal agreements entered into
to ensure that the necessary provision is made.
• CS3 (e) Other towns and villages with potential for housing development primarily
meeting the needs of their surrounding area will be identified in local plans. At these
settlements, new housing may be located within or, where indicated in the local plan,
adjoining the built-up area. Settlements identified for new housing under this policy
should have all of the following:
(i) primary school;
(ii) good journey to work public transport service to a town;
(iii) convenience goods shop;
(iv) community, leisure and social facilities; and
(v) a variety of employment opportunities which have potential for further
development.
(f) Housing development in most villages not identified under clause (e) will take the form
of small scale infilling within the built-up area. Local plan reviews will assess whether this
policy should be applied to those smaller settlements in which, by virtue of few or no
local facilities, remoteness and poor public transport, additional housing development
will be considered unsustainable.
• CS6 Measures will be taken to maintain the vitality of rural communities, seeking
(a) to reduce unemployment and diversify the range of jobs;
(b) to improve accessibility to jobs, services and facilities;
(c) to counter population loss in those areas experiencing decline;
(d) a better balance between the population of working and retirement age.
Particular attention will be given to the East Suffolk Rural Priority Area.
• CS7 New housing allocations will be made in local plans having regard to the following
sequential approach:
(a) Initially sites comprising previously developed land and buildings or vacant or under-
used land should be identified within built-up areas. Open land should not be allocated if
its development would do unacceptable harm to the townscape or the visual or historic
character of the settlement.
Page 59

7. Policy Context
• CS10 The County Council will pursue an integrated development and transport strategy
promoting the most effective use of the transport network through:
(a) development located and designed so as to minimise the need to travel;
(b) transport management and transport investment which help maximise the use of
environmentally sustainable and energy efficient modes of travel.
The County Council will seek to reduce demand for the use of private cars and lorries.
Babergh Local Plan (214)
• HS02 New housing development in villages will take the form of infilling (1-3 houses) in
the Built Up Area, although it is accepted that small groups of up to 5 dwellings within
the larger villages with a range of services and facilities may also be appropriate in the
Built Up Area providing that there is no significant adverse impact on:-
(i) the scale and character of the village;
(ii) residential amenity;
(iii) landscape characteristics, particularly Areas of
(iv) Outstanding Natural Beauty and Special Landscape Areas;·
(v) the availability of services and facilities;
(vi) highway safety;
(vii) the natural and built environment, particularly conservation areas, and listed
buildings, biodiversity and archaeological remains;
(viii) an open space which is important to the village scene or an important
recreational asset for the locality.
• HS04 In the interests of agriculture, rural amenity, road safety and the economy of
services, new housing will be integrated into the defined built-up areas of towns and
villages. In the countryside outside towns and villages it is intended that existing land
uses will remain for the most part undisturbed.
Central Suffolk PCT local health delivery plan (215)
Central Suffolk Primary Care Trust (PCT) has three key aims with regard to the heath and well
being of its population:
• To improve the health and well being of the responsible population within Central Suffolk
PCT and to reduce inequalities in health through the development of the Local Health
Delivery Plan.
• To integrate and effectively co-ordinate the development of Primary and Community
services as well as Health and Social Care services for the benefit of local people.
• To commission and provide high quality patient-centred services that are locally focussed,
involving other public bodies, the private and voluntary sectors, users, carers, clinicians
and all members of staff throughout the design and delivery process.
Page 60

7. Policy Context
Suffolk Health Strategy (216)
The Strategy emphasises the Council's commitment to improving health by mainstreaming
health in all its work and outlines the actions the County Council will be taking over the
forthcoming year. These actions are in five main areas
• Reducing accidents
• Improving Community safety
• Tackling smoking, promoting exercise and diet
• Reducing Teenage pregnancy
• Helping to reduce suicide
The actions have performance indicators and link the Policy and Performance Plan with the
Health Improvement Programme. Examples of key actions include training early years staff in
children's diet and exercise, investigating underage sales of cigarettes, supporting victims of
racial harassment, ensuring children who are looked after have access to sex and relationship
education, reducing the number of fires and engineering schemes to reduce road accidents.
7.4 National Health and social care services policy
The two Wanless reports ‘Securing our Future Health: taking the long term view’ and
‘Securing Good Health for the Whole Population’ are and will continue to have a key
influence in shaping health and social care over the next 20 years (217, 218). The Wanless
reports describe a vision of health and social care in 2022 as:
“When patients need to see their GP, or seek other forms of primary care, they get
appointments quickly with staff who are pro-active in identifying what care is required
and who is best placed to deal with it. Primary care delivers an increasingly wide range of
care, including diagnosis, monitoring and help with recovery. There is a focus on lifestyle,
disease prevention and screening. Choices are explained in a clear, jargon-free way.
Patients seek more advice from pharmacists who handle routine prescribing and help
patients to manage their medication effectively. Current service innovations such as NHS
Direct, Walk-in Centres and telemedicine are commonplace, enabling people to receive an
initial diagnosis in a variety of settings, moving beyond the traditional visit to the GP
surgery.
Social care is no longer a bottleneck preventing the NHS from working well. Patients leave
hospital quickly when they are medically fit to do so and are transferred speedily to the
most suitable setting. In many instances they will return home. If the need is there, they
are supported by health care professionals and paid carers, allowing people to enjoy
independent lives in their own homes for longer. They are monitored by regular GP check
ups designed to assess their all round needs. If necessary they move to a high quality
residential or nursing placement of their choice, or another quality ‘intermediate care’
setting.”
Page 61

7. Policy Context
The National Strategy for Neighbourhood Renewal (219) seeks to reduce the gap in services
and outcomes between poorer and richer areas in England and Wales. It has as its main
principles:
• A clear vision for improving the economic and social conditions in poorer areas;
• Addressing the causes of poverty and social exclusion;
• Integration of services across all sectors; and
• Improving the “unacceptable” level and quality of service provision in poorer areas.
This strategy focuses on improving public services serving poorer areas and populations. The
NHS will play a full part in the Government’s National Strategy for Neighbourhood Renewal
(Department of Health (220, p111)). The NHS Plan (220) is the key policy document driving
change in the National Heath Service; it is a potentially radical programme for the re-
structuring of the NHS. We will use this unprecedented investment to modernise NHS services
around the needs of patients. Department of Health (220, p42). It has as its main principles:
• Reducing health inequalities;
• A patient-led orientation;
• Increased access to services;
• Improved and integrated services; and
• Modern health care.
This includes extra investment in NHS staff and in NHS facilities, for example 500 new one-
stop primary care centres and over 3,000 GP premises modernised. There will be an emphasis
on access to healthcare and a shift to integrated health and social care services.
The Health Act 1999 enables local councils and the NHS to work more closely together… The
result will be a new relationship between health and social care… [This] will bring about a
radical redesign of the whole care system. Social services will be delivered in new settings,
such as GP surgeries, and social care staff will work alongside GPs and other primary and
community health teams as part of a single local care network. This co-location of services
will make easier the joint assessment of patients’ needs Department of Health (220, pp70-
71).
Shifting the balance of power: the next steps (221) describes the roles of public health in the
reorganised NHS. The focus of activity will be on local neighbourhoods and communities, and
public health will lead and drive programmes to improve health and reduce inequalities. They
will also play a powerful role in forging partnerships with, and influencing, all local agencies
to ensure the widest possible participation in the health and health care agenda.
The cross-cutting review on health inequalities (222) sets out the Government's long-term
strategy to reduce health inequalities. The approach is one of mainstreaming work on health
inequalities so that it is at the heart of Government policies rather than a marginal “add on”.
Page 62

8. Local Views and Knowledges
8. Local Views and Knowledges
8.1 Introduction
This health impact assessment did not have the opportunity to consult specifically on health
and social care issues; however, there has already been extensive consultation on a number
of issues, much of which is in written form. A community consultation carried out by Shotley
Parish Council was undertaken in Shotley in March 2001, when 810 questionnaires were
distributed and 140 households replied (223). The planning department of Babergh District
Council also undertook a consultation with the key statutory organisations and the local
community. They received written replies from the local parish councils and over 150
residents of the Peninsula. It has not been possible to systematically review and analyse the
letters from the residents at this time, so this chapter will detail the issues and concerns
emerging from the community consultation carried out by GSCC (a loose association of ex-
Ganges naval cadets and local residents) and the written responses of the parish councils
224).
8.2 Shotley parish council community consultation
The 140 households who replied included 331 residents or 12% of the resident population. The
questionnaire asked three main questions:
• What 3 things give you greatest cause for concern locally?
• Would you support a housing only or mixed use development of the HMS Ganges site?
• What would you like to see developed on the site?
The consultation highlighted fourteen concerns of which the top ten were: roads and traffic;
becoming an overdeveloped area; lack of and overburdened health facilities; lack of facilities
for young people; anti-social behaviour and lack of police; effect on the natural environment;
lack of sports, recreation or community facilities; lack of shops, pressure on primary school
and public transport (See Figure 8.1).
All these existing neighbourhood concerns are consistent with the findings from the baseline
assessment and, as will be seen in the next two chapters, reinforce some of the key health
and wellbeing issues that emerge from the appraisal of the potential health impacts of the
proposed development.
The second question produced a unanimous answer in favour of having a mixed development
rather than a housing-only development.
Page 63

8. Local Views and Knowledges
Figure 8.1 Residents current concerns about the neighbourhood of Shotley
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
The third question, about what residents would like on the site, showed a range of views with
some residents wanting no housing while others were happy to have either housing in general,
social housing or luxury housing. A significant majority of residents wanted the site to have a
general sports, swimming, recreation and community use. Others were also keen for the site
to be used for tourism-related activities, a museum or a park and a green environmental
area. There was also support for youth facilities, shopping, business space and health
facilities (see Figure 8.2).
Figure 8.2 Residents preferences for what should be built on the HMS Ganges site
0%
10%20%
30%
40%50%
60%
70%80%
90%
Page 64

8. Local Views and Knowledges
8.3 Concerns of the Parish Councils
The concerns of the majority of Councils (Brantham Parish Council are minded to approve the
proposal) fall into a number of categories:
• Construction
• Density
• Transport & mobility
• Health services
• Education
• Crime & safety
• Environment
• Contrary to local, regional and national planning guidance
Construction
• “There will be significant construction traffic during development.”
Density
• “500 houses is too many.”
Transport & mobility
• “The roads are inadequate, especially now that most homes have two cars.”
• “There is potential for a significant increase in traffic, not only on the B1456 but in
cross-Peninsula traffic. It is likely that there will be a number of journeys to
Manningtree station taking cars through Holbrook, Stutton and Brantham.”
• “In addition to those travelling to employment, it is also likely that there will be local
peninsular traffic at school times.”
• “Would like to have a firm commitment that the necessary upgrades to the roads will be
completed prior to commencement of any development work, especially at the Freston
crossroads junction by the Water Tower.”
• “Whilst supporting the promotion of non-car journeys through better use of public
transport, councillors do not believe that this will be sustainable.”
• “There is a risk that any improvements in public transport when the development has
been occupied may soon deteriorate if sufficient people do not make use of it or
timetables do not give necessary flexibility at times of travel to and from employment in
Ipswich.”
• “The B1456 is the only road entering this peninsular from Ipswich. Shotley is situated at
the end of the B1456 so all traffic going to and from Shotley will pass through Freston.”
• “Freston Crossroads (junction between B1456/ B1080 and road leading to Freston village)
could not safely accommodate any extra traffic going to and from Shotley. If this
development went ahead in our opinion this crossroads would become a major accident
Page 65

8. Local Views and Knowledges
spot. There has recently been two people killed at this junction. Residents would find it
very difficult to get in and out of the main village via this route.”
• “Many people living in Freston are unable to walk to the bus stop so the use of a car is
essential for them to have any quality of life, particularly as there are no shops in the
village.”
• “We are also concerned about the safety of our residents crossing both the B1456 and the
B1080 to use the bus service as this point.”
• “It is our belief that people moving into the area will most likely seek employment out
of Shotley. Although the plans indicate employment opportunities at Shotley it is
possible that this workforce will come from outside the peninsular and actually increase
the traffic along the B1456 and the B1456/B1080.”
• “We understand that it is envisaged that the route to Shotley from Manningtree station
which is normally used by residents commuting to Colchester, Chelmsford and London,
will be A137/B1080 and join at Freston crossroads. We are concerned that people in
Freston will be unable to bicycle or walk safely along the B1080 to Holbrook. Our
children are expected to make their own way to the Holbrook High School and therefore
this is the route they use.”
• “We would point out that much of Freston is an area of outstanding natural beauty and
that this extra traffic will be detrimental to the enjoyment and safety of people visiting
and living in the village.”
• “There are very limited lengths of footpaths along the B1456 through Freston. We are
concerned that with the extra traffic envisaged people will be in danger both on cycles
and as pedestrians. In certain parts of the B1456 there is not even a verge on which to
walk. The road between Freston Crossroads and the lane to Freston Tower is so narrow
that a car could not safely pass a pedestrian if there were an oncoming vehicle. The
B1456 has a number of bends where visibility is poor.”
• “Concerns about the safety of residents' and particularly children in terms of walking,
cycling and horse riding. The pavements are either too narrow or non existent in parts of
the village. The road itself is in places too narrow for passing large commercial vehicles
and coaches.”
• “Safety is further compromised by the ineffectiveness of the speed limit in the village
and the fact that it doesn't extend the full length. There is no consistent enforcement of
the limit, to the extent that the Parish Council is investigating the Community Speed
Watch Scheme.”
• “Residents are forced to drive their car to post a letter, causing a traffic incident as they
park and adding to the volume of traffic. Social interaction, particularly for children, is
severely handicapped by the road. Councillor Clarke advised at a recent Parish Council
meeting that delivering campaign leaflets for the local elections in May proved a
hazardous experience.”
Page 66

8. Local Views and Knowledges
• “Access from houses and side roads onto the B1456 is already difficult at peak times and
dangerous. It has been reported that it has taken a wait of 5 minutes before being able
to emerge.”
• “In the event of a road traffic accident, not only are the side roads inadequate to take
diverted traffic, there would also be difficulties for the emergency services to reach the
accident site.”
• “People will not give up the privilege of car ownership, the convenience it offers, the
comfort in bad weather, the fact that it is your own space, without it being severely
taxed. When Ipswich High School moved into Woolverstone Hall they reassured the
village that this would not impact on traffic greatly because pupils would be brought by
coach. Regretfully, whilst coaches are used, a significant number of pupils are brought to
school by car.”
Health and social care services
• “Doctors surgeries are now very busy in the area and according to local doctors it is
extremely difficult to employ new GPs.”
• “There will be a considerable increase in number of patients at Shotley surgery. We are
concerned that adequate provision of medical services (e.g. additional GPs and support
staff) has been fully addressed prior to the granting of planning permission, to ensure no
degradation in the current provision.”
• “There is only one practice with two surgery sites situated on the peninsular. As this
proposed development is at the end of the peninsular all the extra people will have to
be accommodated within these existing amenities. We are concerned as to whether there
is sufficient capacity to accommodate this increase in population. We are also concerned
as to whether the allied health services and social care could adequately support this
increase.”
• “Residents will be severely adversely affected by the increase of at least 1500 patients
on the Shotley/Holbrook practice. The current ratio of doctor/patient is at a maximum
of 1800 and this number is only manageable with the additional employment of a locum
on a regular weekly basis. Therefore the addition of in excess of 500 patients (and an
additional 1000-1500 are anticipated) would necessitate recruitment of an additional
doctor and nursing staff.”
• “Although it has been suggested that the nature of the location will attract applicants,
the fact is that when the practice last undertook a recruitment exercise about 8 years
ago, they only had 3 serious applications. The availability of general practitioners is now
significantly worse. It is believed that there are currently at least 5 GP vacancies in
Ipswich that have not been filled. This trend is also reflected in the availability of
competent nursing staff. A recent vacancy was advertised and only 4 applications were
made, of which only 1 applicant was suitable qualified.”
Page 67

8. Local Views and Knowledges
Education
• “Schools will be overstretched, which may mean that local children will have to travel
farther afield.”
• “Given the current climate with education funding, it would be imperative that funding
for the required improvements in local schools is agreed and finalised in advance,
especially if the developer will be expected to make any contribution.”
• “There could be a potential impact on Holbrook Primary if parents wish to exercise
choice of school.”
• “We would also like to see consideration given to improvements in community education,
with a focus on youth.”
• “Holbrook High School may not be able to accommodate the extra children from this
development. This could result in children over 11 years of age being sent to secondary
schools off the peninsular. We are of the opinion that children from this village must
have the opportunity to go to school on the peninsular if they wish.”
Crime & safety
• “We do not currently feel that we receive adequate policing in the village. Whilst there
has been mention of a policing facility being established on the peninsula, we would like
this to be a firm commitment prior to the granting of planning permission, to ensure no
further degradation in the current provision.”
• “This size of development would increase the chance of drug trafficking and illegal
immigrants entering the area.”
Economy
• “Consideration should also be given to the potential for creating local employment.”
• “It has been suggested that people moving into the new development at Shotley will
have the opportunity to gain employment in Harwich and commute using the Ferry. Our
understanding is that there are no employment opportunities in Harwich.”
Environment
• “Before planning permission is granted, there should be evidence of consultations with
environmental groups to minimise adverse impact on the peninsular environment.”
• “There is insufficient water supply in this area and unless improvements are made
hosepipe bans may become more frequent and water pressure could be adversely
affected.”
• “The extra number of people will have an adverse effect on the quality of the
environment in this area.”
• “An area of outstanding natural beauty should protect the character and tranquillity of
the village. Without any increase, the traffic is already too heavy for people to talk to
their neighbours in their gardens without shouting. The exhaust fumes from passing cars
Page 68

8. Local Views and Knowledges
is affecting use of gardens adjacent to the road and windows overlooking the road need
to be kept shut to avoid pollution.”
• “The increase in commercial vehicle traffic over the last few years and the vibration as
they rumble through the village brings the very real threat of causing subsidence to
houses and the consequent damage to the characteristic, waist high, red brick wall that
extends in various parts of the village is clearly visible. As a designated conservation
area, it is defined that the character and appearance of the village should be protected.
This is already not the case, and this proposal threatens it further.”
Contrary to local, regional and national planning guidance
The proposals are contrary to the:
• “…Babergh Local Plan policies HS02 (infilling villages), HS04 (existing land uses to remain
undisturbed outside built-up area villages)”.
• “…Suffolk Structure Plan policies CS1 (adequate infrastructure and facilities), CS3(f)
(small scale infilling in villages), CS10 (integral development and transport – minimising
need to travel).”
• “…National Planning Guidance Notes 1 and 3 (Housing) it does not accord with the
requirement to prioritise the re-use of previously developed land within urban areas; it
does not create a sustainable pattern of development; it does not follow the
Government's sequential approach to the allocation of housing land; it does not link the
new development with public transport and therefore minimise the need for car travel.”
Page 69

9. Appraisal of Current Trends without the Proposed New Housing Development
9. Appraisal of Current Trends without the Proposed New
Housing Development
9.1 Introduction
This chapter details the key health trends if no housing development were to take place on
the HMS Ganges site over the next ten years. The site would remain derelict and inaccessible.
There is likely to be a 5% increase in the resident population and an increasingly older age
profile. The health of the population will remain fairly-good to good but there would be an
increasing need for personal social care services and the long-term management of chronic
diseases.
9.2 Impact Appraisal
In line with national trends there will be a continuing increase in the number of cars on the
Peninsula. The road network and public transport are likely to remain the same but conditions
overall will worsen as the number of cars increase and there are fewer people using public
buses leading to pressures to further reduce the frequency and number of buses.
The development of the ports at Felixstowe and Harwich will generate visual, noise and light
pollution and significantly change the character of the visual landscape and seascape across
the estuary.
The availability of and access to sports, recreation and community facilities and the provision
of youth and community development activities is likely to remain the same but as children
and young people have greater expectations and those residents who have campaigned for
more provision have less time or are less able to undertake this work it is likely that young
people will feel this access has worsened.
There are some differences of view and disagreements between young people and older
residents which could over the long term lead to more anti-social behaviour and the reduction
and degradation of the quantity and quality of social interactions and relationships between
different generations.
The availability of and access to a wider range of amenities including shops, restaurants and
other leisure amenities is likely to remain unchanged though here again the pressures on the
rural economy and wider factors may make some amenities e.g. the local post office less
viable. There has been a recent planning application to build a community pharmacy in
Holbrook which shows that there is the potential for new amenities to establish themselves on
the Peninsula in the future; however, as has been the case with this proposal it is likely to
occur where there is already an existing amenity (In this case the GP dispensary) and an
Page 70

9. Appraisal of Current Trends without the Proposed New Housing Development
existing market so that new amenities are likely to push out existing ones rather than
enhance and complement existing amenities and services.
The environment will remain the same and residents will continue to enjoy the benefits of
their locality though their will be no improved access to the marina and maybe the building of
150 homes there. There will continue to be small scale development of between 1-15 houses
on the Peninsula.
The health and social care services are likely to remain the same overall, however, national
policy drivers will aim to improve rural access and to deliver more services within a primary
care setting and more community-based activities around health promotion and disease
prevention.
9.3 Mitigation measures & Enhancement opportunities
• Improving the local road network and developing traffic management and calming
measures on key parts of the road network.
• Developing a long-term youth and community development strategy with long-term (5
year) financial resources to improve the local provision of sports, recreation and other
community events and activities.
• Developing approaches to bridging the gap in understanding, values and needs between
younger and older residents of the Peninsula.
Page 71

10. Appraisal of the Proposed New Housing Development
10. Appraisal of the Proposed New Housing Development
10.1 Introduction
In total there are likely to be around 600 new homes in and around Shotley in the next two
years. These will be made up of 400 homes on the HMS Ganges site (the original planning
proposal was for 500), 150 homes on the marina development and a number of small pockets
of isolated developments of between 2 to 15 homes across the southern end of the Peninsula.
This will mean an increase of approximately 1500 new people (using the approximation of 600
households x 2.4 people – the England & Wales average numbers in a household), of which
between 300-480 are likely to be children under 16 and 60-195 are likely to be young people
aged between 16-19 years. It is likely that the new residents will have an age profile that is
closer to Holbrook than Berners ward with younger couples with dependent children and older
couples without dependent children. These new people will bring an average of 1.5 cars
(based on the current car owning profile for Berners and Holbrook) or 900 new motor vehicles
onto the Peninsula (see Table 10.1).
Table 10.1 Estimated age profile of the HMS Ganges residents based on Holbrook’s age profile
Berners profile
‘Berner Estimate’ population for HMS Ganges development
Holbrook profile
‘Holbrook Estimate’ population for HMS Ganges development
Under 16 20% 300 32% 480 16 to 19 4% 60 13% 195
20 to 29 9% 135 4% 60 30 to 59 43% 645 33% 495
60 to 74 15% 225 10% 150 75 and over 9% 135 8% 120
Total 1500 1500
People moving house, like those in employment, are likely to be healthier and less likely to
have chronic illnesses or serious disabilities than the general population as a whole.
10.2 Impact appraisal
All change involves uncertainty and uncertainty generates worries and fears about the future
in existing residents. This is the context within which the health impacts of the proposed
housing development need to be understood. For a detailed assessment of the health impacts
compared to doing nothing see Table 10.2 – the health impact appraisal matrix.
Page 72

10. Appraisal of the Proposed New Housing Development
Construction phase
Overall existing residents will face significant disruption during the construction period. This
will create some moderate to major medium term, temporary negative health effects on
existing residents’ sense of wellbeing and their general quality of life.
There are two key positive health benefits arising during the construction phase:
• the potential for employment and business opportunities for local people and
• the remediation of existing contamination on the HMS Ganges site.
There are four key negative health impacts from the construction phase:
• the disruption in access to health, social care and other services,
• the increase in heavy lorry traffic,
• the potential loss of social capital and cohesion and
• the noise, dust and dirt generated from the site and the lorries.
The majority of residents will benefit from the positive health benefits and be affected by
the negative health effects during the construction phase. Those likely to be the most
affected are those residents living adjacent to the site, especially those living near the
entrance and exit.
Operation phase
Overall the HMS Ganges site will come back into use with landscaped green and open public
space that is accessible to all residents – existing and new. The development will regenerate
and remediate this brownfield site and has the potential to provide regeneration for the
wider community through the provision of retail amenities and community facilities as well as
a museum. The development will also reconnect the existing marina development to Shotley
Village creating a more physically integrated community at the end of the Peninsula.
There are eight key positive health impacts of the development during its operation phase:
• the building of new modern housing that includes affordable and starter homes;
• the accessibility of the site and creation of new public green space;
• the protection of the local naval heritage; the creation of a more balanced community
with a wide range of ages;
• the increase in more retail amenities, and increased employment opportunities if the
retail and commercial space is let; the potential use of some of the commercial space for
community facilities; and
• the enhancement and protection of local flora and fauna on the site; and the re-use of a
key strategic ‘brownfield’ site for a mixed-use development.
There are three key negative health impacts of the development during its operation phase:
• the strain on existing health, social care, education and leisure services;
Page 73

10. Appraisal of the Proposed New Housing Development
• the increase in traffic and congestion caused by the increase in cars, leading to more road
traffic accidents and reduced access to key services; and
• the strain on social capital and cohesion because of the sense of ‘overcrowding’ created
by the influx of new people onto the Peninsula and the differing and potentially
conflicting ways of life and values of the new residents.
10.3 Mitigation measures
During the construction phase most of the worries, fears and complaints of residents can be
allayed and resolved by developing a good communication programme led by the local
(planning) authority. This should involve ongoing dialogue with the parish councils and public
meetings where necessary to deal with issues that arise during the construction phase. The
developer also needs to be proactive in listening to local complaints during the construction
phase. Complaints and concerns can be resolved at an early stage by having regular meetings
with a representative from Shotley Parish Council, Haylink, Babergh planning department and
Central Suffolk PCT. These meetings should initially be weekly and then become monthly as
the construction progresses and the community’s concerns are resolved and a trusting
relationship develops between the key stakeholders – community, developer and statutory
agencies.
A series of regular open meetings linked to parish council meetings that enable the wider
community to have their say directly will also develop and enhance the trust between the
community and Haylink thereby reducing the negative impact on social capital and social
cohesion.
Negotiation around and wide publicity of the times that construction work will take place,
especially when noisy or dusty work occurs as well as the times when lorry movement are
going to occur, will ensure that the negative impacts on residents are reduced. Consulting
residents in this way will also mean that they are likely to be more accepting of the
disruption caused by the construction work. Lorry movements should avoid ‘rush hour’ times
in the mornings and early evenings. Noisy construction work should not occur at weekends or
late evenings and early mornings when more individuals, families and children are at home
and relaxing. This will also ensure that disruption for local people is reduced.
A detailed review of the road traffic accident data over the construction and early operation
period will highlight increases in accidents on the B1456 and on other parts of the Peninsula’s
road network. This can be followed up with an investigation into the potential for traffic
calming measures and a re-configuration of existing accident ‘hot spots’.
Adherence to best practice in housing design, construction, occupational health and safety
and a secure and patrolled construction site will ensure that the hazards and potential
Page 74
10. Appraisal of the Proposed New Housing Development
negative health effects from the site itself will be mitigated. An example is the watering-
down of demolition work so that the dust thrown up into the air is localised to the site itself
and not to neighbouring homes and gardens.
Policies should be drawn up to enable local people – both those already involved in
construction and those who are unemployed - to access potential employment opportunities.
The new development should also be used as an opportunity to get young people into
employment-linked training and apprenticeship building and construction programmes.
10.4 Residual effects
These mitigation measures will reduce the majority of negative impacts but they will not
negate these impacts completely. Furthermore, these measures will not do much for those
residents who see any increase in people on the Peninsula as detrimental to their quality of
life and way of living and those who, while in favour of developing the HMS Ganges site, do
not feel that the proposed design is the right one.
10.5 Enhancement opportunities
There is an opportunity at this time to consider using some of the retail and commercial
space to develop a community centre-type facility where activities like health promotion
clinics, mother and toddler groups, a crèche, community internet café, indoor leisure
activities and youthwork and community development initiatives can operate from.
There is a good opportunity to explore the feasibility of siting a dental service and community
pharmacy which would also enhance the amenities in Shotley (this issue is discussed in more
detail in Chapter 11). All the above will serve to focus community activities and build both
social capital and cohesion between new and existing residents as both see and feel the
benefits of the new development.
Finally, more community development and youth work resources over the next three years
would help develop the resilience of the community to deal with the disruptions of the
construction and actualise the potential positive health benefits that the completed
development would have for existing residents in particular.
10.6 Conclusion
The development has overall positive health benefits especially if community amenities and
facilities are built into the site for both the new and existing residents however existing
residents will face moderate to major negative health impacts during the construction period.
Page 75

10. Appraisal of the Proposed New Housing Development
The key short term and long term negative impacts will be on access and mobility caused by
poor public transport and the increase in motor vehicle traffic on the relatively poor road
network.
There are a range of measures that could mitigate the negatives and enhance the positives
during the construction and operation phase of the proposed development.
Page 76

10. Appraisal of the Proposed New Housing Development
10.2 Health impact matrix for the construction and operation phases of the development compared to no development taking place Const Phase (0-2 years from date planning permission is given)
Construc e No development impact HMS Ganges development – CONSTRUCTION PHASE impact Overall The resident population will not face the
disruption caused by construction lorries moving through the community and the noise, dust and dirt generated from the building site and lorries.
~ The resident population will face significant disruption during the construction period.
These moderate, relatively short term and temporary negative health impacts on existing resident’s quality of life and sense of wellbeing will occur whilst construction is ongoing.
---
Disease Physical No change from current trends. The construction is unlikely to cause direct physical health problems in
local residents. The major physical health effects will be from accidents. Some workers may be injured on the construction site from falls, falling
objects, etc. There is potential for the additional traffic of heavy construction lorries
to result in an increase in road traffic accidents. Children gaining access to the site may also be injured.
--
Mental
Socio-ecoPopulati
Legend
+ positive health impact +++ major --- - negative health impact ++ moderate -- ~ no health impact + mild -
ruction
tion Phas
health
health No change from current trends. There is a string likelihood for varying degrees of psychosocial stress related to construction activities – noise, dust, dirt, traffic, other disruption – and manifested as worry, concern, frustration, anger and upset among existing residents.
---
nomics on profile: density No change from current trends. ~
The site is currently off-bounds and unused The site does not form part of the geographical space used by the community. Therefore there will be no change from current trends in the existing settlement of Shotley Village. As new residents move into the built phases of the new development the overall density of Shotley will remain similar to that of the existing village.
~
Page 77

10. Appraisal of the Proposed New Housing Development
Construction Phase No development impact HMS Ganges development – CONSTRUCTION PHASE impact Population profile: age structure No change from current trends.
The population is showing an ageing profile with fewer children and young people. While this is not inherently negative the lack of a balanced community with a range of ages does reduce the dynamism and sense of community and solidarity that children and young people can bring to communities.
- No change from current trends in the existing settlement. New residents will begin moving onto the HMS Ganges site. They are
likely to be young families and older couples. As new residents move into the built phases of the new development the overall age structure will change gradually during the construction to a younger profile with more children and young people.
This mixed use development has the potential of bringing new people into the area enhancing the local economy, help develop community activities and play a positive role in building a sense of community, and who can balance the overall ageing profile of the population on the Peninsula.
+
Health & social care services No change from current trends. ~- As most of the services are currently provided outside the immediate vicinity of the HMS Ganges site there will be no direct disruption to health and social service care services.
However the construction traffic will use the B1456 to get on and off the site. This is likely to create potentially significant local congestion and may lead to some disruption to service access.
The extent of this effect is difficult to predict as it will depend on the construction contractor and the size and type of vehicles they will use and the days and times of day that these vehicles will enter and exit the site. However as the B1456 is the major road that allows residents to access all of their health and social care services even small levels of disruption will have major impacts through delays in service access and psychosocial stress from any frustration caused by dealing with the construction traffic.
--
Crime and community safety No change from current trends. ~ Construction sites with their store of materials and the influx of new people can make an area more vulnerable to crime or at the very least be seen as more vulnerable to crime and less safe. However there is unlikely to be any significant increases in crime because of the construction.
~-
Employment & economy No change from current trends. ~ It is likely that most of the construction related employment will go to people from outside the Peninsula, however, there are likely to be some job opportunities for people living in Babergh as a whole. The local amenities - post office, shop, pubs - are likely to gain increased business from the construction workers on the site.
The effect on other local businesses on the Peninsula is limited because the majority of them are not related to the building and construction industry.
This will depend on the availability of local people with the relevant skills and the developer’s recruitment drive proactively focussing on local and district construction workers and skilled craftsmen.
+
Page 78

10. Appraisal of the Proposed New Housing Development
Construction Phase No development impact HMS Ganges development – CONSTRUCTION PHASE impact Education No change from current trends. ~ There is unlikely to be any disruption to the education of children going
to the schools on the Peninsula, which are situated away from the HMS Ganges site so that noise and vibration from the construction lorries and the site will not affect the schools and its pupils.
However, any congestion on the B1456 because of the construction traffic could disrupt the journeys, by both private and public transport, of children going to the schools.
~
Housing: general No change from current trends.
~ The new development will have a range of housing types including affordable housing.
There is unlikely to be any direct impacts on the existing houses in terms of vibration effects and structural damage due to the construction work . The phased nature of the new development should also make disruption of utility services – water, gas, electricity, waste and sewage disposal – unlikely.
+++
Housing: tenure and turnover No change from current trends. House prices will continue to rise in line with
district trends
~ No change from current trends in the existing settlement. On the new development as new residents move into the built phases of
the development the overall levels of tenure and turnover will change. It is unlikely that there will be large positive or negative changes in the
prices of existing housing because of the new development itself.
~
Housing: unsafe housing No change from current trends. ~ As stated in the housing section above vibration and the digging of foundations and laying of infrastructure e.g. sewage and gas pipes, electricity and telephone cables, etc is unlikely to have any effect on the physical structure of the existing housing in Shotley Village.
~
Housing: home accidents No change from current trends. ~ No change from current trends in the existing settlement. The new housing is being built to current safety standards and is
therefore unlikely to lead to an increase in home accidents.
++
Social capital No change from current trends. ~ The construction may cause some strains between the exiting residents and the developer and construction workers especially if there is considerable disruption caused by the construction work.
Residents and their families are likely to feel excluded and ‘pushed out’ from local amenities if construction workers use these amenities in any great numbers such as the local stores and pubs.
This may have mixed effects on social cohesion and capital with on the one hand uniting the community in their concerns and frustrations over the disruptions caused by the development as well as these frustrations straining and disrupting the existing the social interactions, connections and relationships that currently exist in Shotley.
-
Page 79

10. Appraisal of the Proposed New Housing Development
Construction Phase No development impact HMS Ganges development – CONSTRUCTION PHASE impact Culture and leisure No change from current trends. ~ The construction phase is on currently derelict land which is not being
used in any way by existing residents. There will therefore be no impacts on current cultural and leisure activities
There is likely to be some disruption to accessing culture and leisure facilities just as there is likely to be for other services.
~-
Traffic and access Transport No change from current trends. ~ There will be no direct effects on people’s access to private and public
transport. However the new development will generate construction traffic and this
is likely to have a significant impact on the movement of private and public transport vehicles on the Peninsula particularly Shotley Village.
--
Air quality: management No change from current trends. ~ Babergh has an established air quality management plan and implementation and monitoring system as well as construction and planning guidelines.
Dust from demolition and other work on the site is a potential pollutant. There will be additional construction traffic during the construction phase and this will give rise to increased levels of air pollution.
Both dust from the construction site and emissions from the construction vehicles are likely to have a negative effect on air quality. While the average levels of air pollutants are likely to be within air quality guidelines there is the potential for peaks in the concentration of air pollutants in the Shotley area. These peaks can have physical as well as psychological effects on residents’ sense of wellbeing. The increase in air pollution is unlikely to increase the number of people having respiratory illnesses.
The average levels of air pollution are unlikely to be above air quality guidelines however there may be peaks in air pollution at certain times.
~-
Air quality: respiratory & cardiovascular effects
No change from current trends. ~ Peaks in concentration may exacerbate the symptoms of those with existing respiratory and cardiovascular difficulties especially in older people and children.
~-
Traffic Injuries No change from current trends. ~ The increased construction traffic could pose a danger to adults and especially children.
On the Peninsula this is somewhat mitigated for pedestrians by the presence of footpaths that are separated from the traffic by hedges on many sections of the B1456.
~-
Page 80

10. Appraisal of the Proposed New Housing Development
Construction Phase No development impact HMS Ganges development – CONSTRUCTION PHASE impact Landscape & visual assessment
Urban & rural development planning No change from current trends. ~- This is a key strategic brownfield site that needs to be developed in a balanced way.
Babergh needs more mixed housing development over the next ten years.
The proposed development is mixed-use with affordable housing and commercial and community workspace.
+++
Noise and vibration Noise pollution No change from current trends. ~ Residents who are adjacent to the site will be most affected.. Noise and
vibration could give rise to psycho-social stress among these residents especially if there is continuous movement of heavy construction lorries.
-
Vibration & subsidence No change from current trends. ~ The lorries will also generate some vibration, however the building work and lorries are unlikely to damage the foundations of existing houses adjacent to the site.
~
Contamination & ground conditions
Contaminated land management No change from current trends. ~ Bedford has established planning and contaminated land management guidelines.
Some potential for heavy metals, hydrocarbons, asbestos and other chemical contamination to be present and to be thrown up as fine air particulates across the site and the surrounding area.
This is likely to be a greater hazard for the construction workers undertaking the removal than residents in the surrounding area. The extent of the hazard will depend on the safety protocols, clothing and equipment used to safely remove and dispose of these materials.
For existing residents the remediation of the site will remove hazardous substances from the site.
-++
Hazardous/toxic substances and poisonings
No change from current trends. ~ Construction sites can and do have hazardous substances on-site. This again is likely to be a greater hazard for construction workers than
for residents in the surrounding area. The extent of the hazard to construction workers will depend on the safety equipment and safe storage and usage of the substances.
The hazard to residents, especially children ingesting or coming into contact with hazardous chemicals, will depend on the secure storage and security measures to ensure no unauthorised access to the site.
~-
Page 81

10. Appraisal of the Proposed New Housing Development
Construction Phase No development impact HMS Ganges development – CONSTRUCTION PHASE impact Waste
Solid waste management No change from current trends. ~ Demolition and removal of solid waste will need to be managed carefully especially if it is contaminated with heavy metals, asbestos or other chemicals. The flow of materials entering and exiting the site during the construction phase will be significant. The key effects are likely to be the increase in construction traffic flows on the B1456 road and the potential for spillage and throwing up of materials outside the site and thereby creating new hazards for other vehicles and adult and child pedestrians.
~-
Hydrology Water supply and sanitation No change from current trends. ~ There is a potential for the disruption of the water and sewage facilities
of existing residents as connections are made for the new houses on the development site. If this occurs there is potential for bacterial and viral contamination which in turn could give rise to an increase in gastro-intestinal disorders i.e. acute diarrhoea and vomiting .
Weill’s disease (Leptospirosis) is a key hazard for construction workers working on the sewers. Leptospirosis is spread via direct contact with contaminated animals and a contaminated environment. Rats in the sewers excrete the spirochetes into the water. The extent of hazard will depend on the safety protocols and clothing worn by workers.
More water will be used on the Peninsula which will affect the levels of reservoirs and aquifers.
~-
Water quality monitoring No change from current trends. ~ Essex and Suffolk Water have established water quality monitoring. Essex and Suffolk Water will need to be informed and take part in
discussions about the water and sewage system design and construction to ensure that there is no disruption of fresh water supplies and sewage waste flows and reductions in water quality.
~
Other hazards Injuries to adults & children No change from current trends. ~ None identified.
~
Page 82

10. Appraisal of the Proposed New Housing Development
Page 83
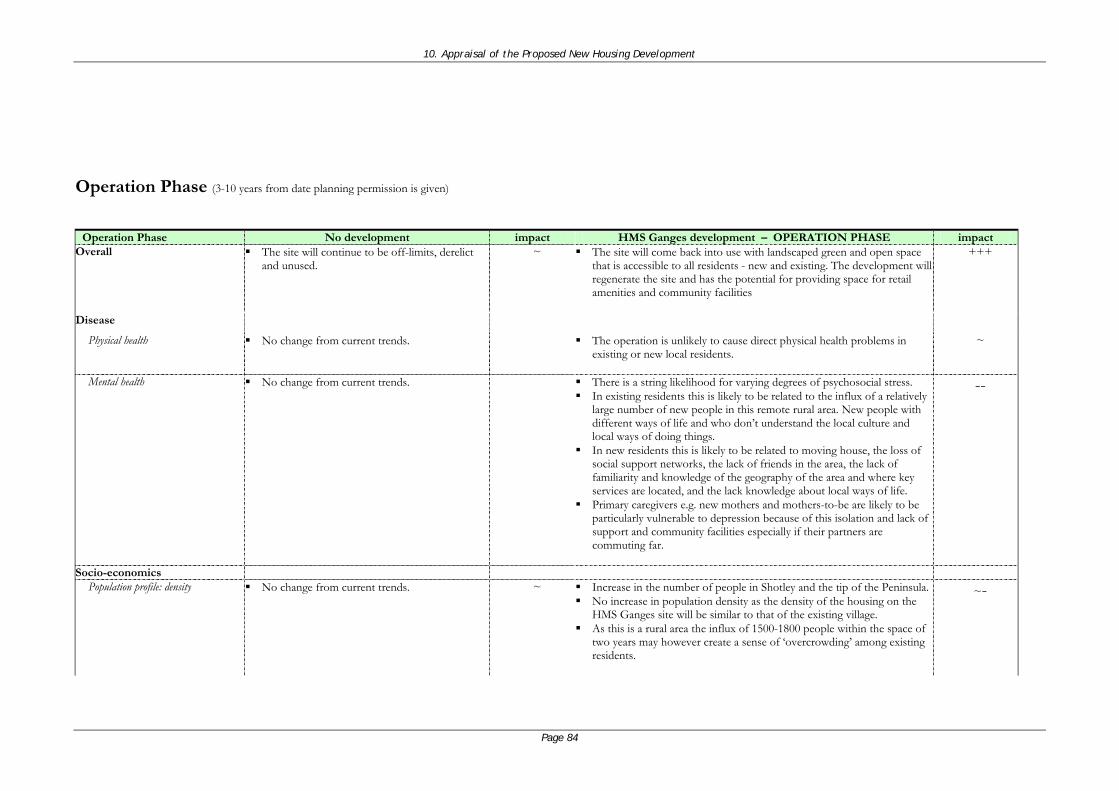
10. Appraisal of the Proposed New Housing Development
Operation Phase (3-10 years from date planning permission is given)
Operation Phase No development impact HMS Ganges development – OPERATION PHASE impact Overall The site will continue to be off-limits, derelict
and unused. ~ The site will come back into use with landscaped green and open space
that is accessible to all residents - new and existing. The development will regenerate the site and has the potential for providing space for retail amenities and community facilities
+++
Disease Physical health No change from current trends. The operation is unlikely to cause direct physical health problems in
existing or new local residents.
~
Mental health No change from current trends. There is a string likelihood for varying degrees of psychosocial stress. In existing residents this is likely to be related to the influx of a relatively
large number of new people in this remote rural area. New people with different ways of life and who don’t understand the local culture and local ways of doing things.
In new residents this is likely to be related to moving house, the loss of social support networks, the lack of friends in the area, the lack of familiarity and knowledge of the geography of the area and where key services are located, and the lack knowledge about local ways of life.
Primary caregivers e.g. new mothers and mothers-to-be are likely to be particularly vulnerable to depression because of this isolation and lack of support and community facilities especially if their partners are commuting far.
--
Socio-economics Population profile: density No change from current trends. ~ Increase in the number of people in Shotley and the tip of the Peninsula.
No increase in population density as the density of the housing on the HMS Ganges site will be similar to that of the existing village.
As this is a rural area the influx of 1500-1800 people within the space of two years may however create a sense of ‘overcrowding’ among existing residents.
~-
Page 84

10. Appraisal of the Proposed New Housing Development
Operation Phase No development impact HMS Ganges development – OPERATION PHASE impact Population profile: age structure No change from current trends.
The population is showing an ageing profile with fewer children and young people. While this is not inherently negative the lack of a balanced community with a range of ages does reduce the dynamism and sense of community and solidarity that children and young people can bring to communities.
- The majority of new residents are likely to be young families and older couples. As new residents move into the built phases of the new development the overall age structure will change gradually during the construction to a younger profile with more children and young people.
Over the long term this change in profile is likely to have positive benefits for the Shotley community by creating diversity and reversing the overall ageing profile of the population on the Peninsula.
++
Health & social care services No change from current trends. There is a potential for a new pharmacy to be
built in Holbrook which will mean that the GP dispensary which is currently based in Holbrook will become less viable which in turn is likely to have financial impacts on the GP practice as a whole and its two branches.
There is no local dentist on the Peninsula.
~-- The increase in population will strain existing primary care services and over the long term strain personal social care services.
There are no plans at present to deal with the creation of this new community.
This is likely to mean that there will be major negative effects both on the new residents as well as existing residents if the health and social care services are not expanded and/ or reconfigured in order to meet the health care needs of the new residents without compromising the quality of care that existing residents currently receive.
---
Crime and community safety No change from current trends. ~ The new housing development is designed using the latest guidance on creating safe communities so there is unlikely to be a greater increase in major crime.
However with the increase in children and young people there is a potential for anti-social and nuisance behaviour to increase as there are few social and leisure activities for these age groups on the Peninsula.
+-
Employment No change from current trends. ~ While there is commercial and retail space being developed on the site it is not clear as yet what kinds of businesses are likely to move in. This will be dependent on the cost of renting the facilities and the likelihood of existing local businesses needing space to expand.
There is a potential for retail businesses to move in and this is likely to create some reasonably good quality full-time and part-times jobs.
The building of the naval museum and the protection and enhancement of the Martello Tower and Fort alongside the better access to the marina are likely to increase he number of visitors, tourists and holiday-makers to the Peninsula.
+
Page 85

10. Appraisal of the Proposed New Housing Development
Operation Phase No development impact HMS Ganges development – OPERATION PHASE impact Education No change from current trends. ~ The number of new school- age children moving into the area is difficult
to predict at this stage but using the Holbrook ward as a comparable population group there are likely to be 480 children under 16 and between 195 young people aged between 16-19 years.
There is a section 106 agreement being worked out with the education department to ensure that there is appropriate and adequate provision forthese children and young people without effecting existing pupils.
As the children will move to the area over a two-year period any disruption because of them will be minimal.
Having a school with pupils from diverse backgrounds can be a richer social and educational experience.
On the other hand children going to a new school can be more vulnerable to bullying and the loss of existing friends may make the transition to the new school difficult for some children.
+-
Housing: management No change from current trends. ~ The new development will have a range of housing types including affordable housing. The majority of new residents are likely to be couples with families and older couples.
The houses will be built to the highest standards using sustainable construction techniques and materials.
The housing development will increase the attractiveness of the area and may cause prices to rise which will be positive for current home-owners but make houses less affordable in the longer term for local people especially those buying their first house.
+++-
Housing: tenure and turnover No change from current trends. ~ There will be some change in tenure and turnover as local people move into the some of the housing provided on the site and people from outside the Peninsula and on the Peninsula move onto the site.
~+
Housing: unsafe housing No change from current trends. ~ No change from current trends to the existing housing. The new housing will be built to high standards and follow current health
and safety regulations.
++
Housing: home accidents No change from current trends. ~ The new housing will be built to modern standards. This is likely to reduce the chance of home accidents in this accommodation.
++
Page 86

10. Appraisal of the Proposed New Housing Development
Operation Phase No development impact HMS Ganges development – OPERATION PHASE impact Social capital & cohesion No change from current trends.
There are already a number of smaller housing estates within the existing village creating a number of differing blocks of housing within Shotley.
There is a village hall but this acts as an administrative centre rather than a community centre where people can come together.
~ The development has been built to ensure the maximum physical integration of the new housing with the existing houses including using building materials that are sustainable and in keeping with the surrounding architecture.
However the amenities at the tip of the peninsula are poor and while there is some commercial and community space planned specific community facilities and services have not been planned.
There is green and open public space which is accessible to both new and existing residents and cycle and footpaths which will enable some mixing of the new and existing residents.
The development will also reconnect the existing marina and Shotley village creating a more physically integrated settlement at the end of the peninsula.
Existing residents find the influx of new people into this remote rural area difficult which may lead to difficulties in creating friendships and interacting with the new residents of the HMS Ganges site.
New residents may also find moving house, he loss of social support networks of family and friends, the initial send of isolation and lack of familiarity with where key services are located and local ways of doing things difficult. This may make them wary of interacting with long standing residents. Primary care givers at home looking after children may also find the lack of community facilities and isolation difficult leading to moderate forms of depression.
The lack of a community focus created by retail and community amenities means that it is likely that the new and existing residents will not mix very much which will impact negatively on social capital and cohesion in the first few years.
However mixed use nature of the development has the potential of bringing new people into the area enhancing the local economy, help develop community activities and play a positive role in building a sense of community and reversing the overall ageing profile of the population on the Peninsula.
++-
Page 87

10. Appraisal of the Proposed New Housing Development
Operation Phase No development impact HMS Ganges development – OPERATION PHASE impact Culture and leisure No change from current trends
There are some social, cultural or leisure amenities for children and young people including football and drama. However over time there has been a loss of established youth work and community development support. This is likely to continue.
~- There are no specific planned amenities on the site. There will be landscaped green open public space with a network of cycle
and foot paths which will increase the opportunities for children from all parts of Shotley to play outdoors.
A new naval museum will be built in the site and the Martello Tower and Fort will be protected and enhanced for local people and visitors from outside the Peninsula.
However there is no plan to provide indoor or covered facilities.
+-
Traffic and access Transport Traffic levels will continue to rise in line with
national trends.
~- It is likely that there will on average be 1.5 cars per new household which means approximately 900 additional cars on the Peninsula.
There are pathways throughout the development so that the development as a whole is accessible and traversable by cycle and foot.
There is likely to be greater congestion on the B1456 and surrounding roads especially during morning and evening rush hours between &.7.30-9.30am and 3.30-5.30pm.
--
Air quality: management No change from current trends. ~ There will be more motor vehicle traffic in the area this is likely to increase the air pollution in the area however because of the relatively open configuration of the settlements on the Peninsula this is likely to disperse quickly. The greatest concentrations of pollution are likely to be adjacent to roads especially those at junctions where traffic from the existing and new settlements meet..
The average levels of air pollution are unlikely to be above air quality guidelines however there may be peaks in air pollution at certain times.
~-
Air quality: respiratory & cardiovascular illness
No change from current trends. ~ The increase in air pollution is unlikely to exacerbate the symptoms of those with existing respiratory and cardiovascular conditions.
~
Road traffic injuries No change from current trends.
~ The increase in the number of motor vehicles on the unchanged road network on the peninsula will make road traffic injuries more likely.
--
Page 88

10. Appraisal of the Proposed New Housing Development
Operation Phase No development impact HMS Ganges development – OPERATION PHASE impact Landscape and visual assessment
Urban & rural development planning No change from current trends. HMS Ganges will remain a derelict and
inaccessible site
~ This development will play an important role in meeting the housing targets for Babergh.
There will also be more good quality affordable housing for local people.
++
Noise and vibration Noise Pollution No change from current trends. ~ The increase in the number of cars and the new housing will create more
noise for existing residents and may cause some nuisance.
-
Vibration & Subsidence No change from current trends. ~ There is unlikely to be any long term vibration or subsidence from the development.
~
Contamination & ground conditions
Contaminated land management No change from current trends.
~ The contaminated land on the HMS Ganges site will have been decontaminated.
The development will not create any non-domestic contamination though there is likely to be low levels of household chemical usage e.g. weedkiller.
+-
Hazardous/toxic substances and poisonings
No change from current trends. The small amounts of hazardous substances on
the site will remain over time this may leach and contaminate a larger area.
~- The toxic materials on the site will be removed from the site. The development will not create any non-domestic contamination
though there is likely to be low levels of household chemical usage e.g. weedkiller, bleaches, etc.
+
Waste Solid waste management No change from current trends. ~ The new homes will increase the overall domestic waste produced on the
peninsula. The development will be served by the waste disposal service that serves
the existing homes.
~
Hydrology Water supply and sanitation No change from current trends. ~ The development will upgrade the existing network used by the original
buildings on the site to connect the new homes to mains water and sewerage pipes.
~
Page 89

10. Appraisal of the Proposed New Housing Development
Operation Phase No development impact HMS Ganges development – OPERATION PHASE impact Environment and ecology
Flora No change from current trends. ~- The development will landscape and improve the green space on the site and maintain the existing natural habitats.
++
Fauna No change from current trends. ~- The development plan will take into account the local wildlife and ensure that habitats are maintained and reproduced.
++
Page 90

11. Appraisal of the Options for Delivering Health and Social care to the Proposed New Housing Development
11. Appraisal of the Options for Delivering Health and
Social Care to the Proposed New Housing Development
11.1 Introduction
There are five major options for meeting the health needs of the incoming community and
maintaining the quality of health and social care services for existing residents. The first is to
assume that the increasing workload will be borne by the existing GP practice team with
emergency demand being dealt with by additional locum GPs. The second option is to bring
an additional GP and practice nurse into the existing practice with this GP providing the
majority of care to the new residents from there. The third option is to develop a community
nurse team that delivers clinic-based services from community facilities on the HMS Ganges
site thereby reducing the workload on the existing GP team and so enabling them to increase
their list sizes. The fourth option is a synthesis of option two and three where an additional
GP and community nurse deliver surgery and outreach clinic services. The fifth option would
be to have a separately contracted single-handed GP and practice team based in the new
development.
There will also need to be an increase in the capacity of social care services delivered to the
Peninsula. Social care services already aim to provide as many services as possible to people
in their own homes however the poor road network and poor public transport have
implications for the delivery of high quality social care.
This chapter explores the positives and negatives of these outline options. While there are
differing cost implications and cost is an important factor it is one of a number of factors
including the long term sustainability of each of the options and range of positive health
benefits likely, any potential negatives, the acceptability of the options to existing health and
social care teams and the acceptability of the options to local residents who will use the
service.
11.2 Background context
There are ten key factors that influence capacity, configuration and delivery of health and
social care services (218). These fall into two categories - demand factors and supply factors,
see Table 11.1.
Page 91

11. Appraisal of the Options for Delivering Health and Social care to the Proposed New Housing Development
Table 11.1 Factors that impact on demand and supply
Demand Factors Supply Factors
• Demography
• Health status
• Health in old age
• Health promotion and disease prevention
• Health seeking behaviour
• Technology and medical advance
• Information and communication technology
• Health and social care workforce
• Pay and prices
• Productivity
All these factors need to be taken into account in developing and reconfiguring health and
social care services and estimating how the services will need to change over the long term.
These factors are discussed below in relation to the Shotley Peninsula and the HMS Ganges
development.
11.2.1 Demography
As described previously the key long term effect of the proposed development on the HMS
Ganges site will be to increase the population by 1500 people at the end of the Peninsula.
Overall this will increase the numbers of children and older people who tend to be the
heaviest users of health and social care services.
11.2.2 Health status
The overall health status of the people on the Peninsula is fairly good to good with low levels
of deprivation. The new residents to the Peninsula are also likely to be in fairly good to good
health as people who move are likely to have the financial and personal resources to enable
them to move themselves, their families, their possessions and their lives to another area.
The good health status of the new and existing residents will to an extent counteract the
demand generated by the increase in population however, over the very long term (beyond 10
years), these people will grow older and place greater demands on health and social services
especially personal social care services.
11.2.3 Health in old age
From the above, older residents on the Peninsula will not place great demands on health
services in the short term (0-3 years from the development being given planning permission)
however, over the longer term (4-10 years), there will be increasing demands to deal with
chronic diseases and to support older people to live independently in their own homes.
11.2.4 Health promotion and disease prevention
Health promotion and disease prevention activities e.g. screening, well person clinics and
chronic disease management clinics can ensure that the demands made on health and social
care services are reduced. Though health promotion and disease prevention activities at
primary care and community levels are crucial they are longer term measures and are unlikely
Page 92

11. Appraisal of the Options for Delivering Health and Social care to the Proposed New Housing Development
to reduce the demand for health services in the first three to five years. They also require a
long term plan and sustained resources – human and financial – to ensure long term success.
11.2.5 Health seeking behaviour
How people seek healthcare and their expectations and perceptions of health and social care
are important factors in influencing demand on health and social care services. The Peninsula
has an established primary care system with each person having a named GP. This is
consistent with the primary care system in the UK as a whole which means that people like to
have a long term relationship with a named medical practitioner who they can see over the
long term and who knows about their health and periods of illness. In this context new
residents and existing residents are likely to want to have a named GP who they can consult
regardless of what other primary care services are available. Patients derive a sense of
security and confidence by having someone they can talk to face-to-face and who knows their
past medical history.
11.2.6 Technology and medical advance
There are a range of innovative medical technologies and treatments in the field of genetics
which are likely to increase the treatments available for what are currently seen as incurable
illnesses e.g. a wide range of cancer, inherited conditions, Parkinson’s disease, etc. These are
likely to create pressures on drug budgets in particular. However, these cannot be planned
for, except in a very general sense of being aware of the new drugs and treatments that are
coming on-stream from pharmaceutical and biotechnology companies.
11.2.7 Information and communication technology
Information technologies in the form of tele-medicine; the electronic patient record (EPR);
online diagnostic results; integration of health and social care information systems; ongoing
collection and use of clinical information are likely to make health and social care more
efficient and more effective as long as the IT systems are robust, secure and error-free.
These technologies will affect the health services on the Peninsula but when and where will
only become clearer once these systems become more widespread and move from their early
pilot stages.
11.2.8 Health service workforce
The availability of appropriately qualified and skilled health and social care staff are a crucial
ingredient to providing high quality effective primary care. On the Peninsula there are
existing concerns about recruiting and retaining skilled staff. Long term workforce planning
has to occur at a regional level and does not tend to increase staffing in the short term.
Despite this, one important step is to develop the skills of local people to take on at least
some of the health and social care opportunities on the Peninsula.
Page 93

11. Appraisal of the Options for Delivering Health and Social care to the Proposed New Housing Development
11.2.9 Pay and prices
Difficulties in recruitment and shortages in certain health and clinical specialities tends to
push pay rates higher. The creation of newer and better drugs and treatments also pushes the
price of health care higher. Both pay and prices are influenced by national and regional
factors with little room for manoeuvre at the local level except in terms of productivity.
11.2.10 Productivity
Improving the efficiency of health services is also important to improving the health of local
people and the quality of the health care that they receive. By doing things differently and
making them more efficient and effective more people can be treated with the same amount
of human and financial resources. In the context of the peninsula there needs to be a balance
between efficiencies of scale and the need for locality of access.
11.2.11 Social care specific factors
The Social Services Inspectorate report ‘Care in the Country: Inspection of Community care in
Rural Areas’ found four key issues facing social care services in rural areas: lack of choice,
sometimes leading to service refusal; services being less accessible to country dwellers than
those living in towns; the use of inappropriate services because of their relative proximity to
the service user; and a reliance on historical distribution of services which do not necessarily
reflect known need. They also found that services are more expensive to deliver partly but
not wholly because of the increased travel and transport costs.
11.3 Appraisal
The five options to meet the health and social care needs of the potential new residents
whilst maintaining the quality of care for existing residents are:
Absorbing the increase within existing primary care capacity.
Additional GP and practice nurse.
Expansion of the community nursing team.
Additional ‘outreach’ GP and community nurse.
Separate single-handed GP team.
11.3.1 Absorbing the increase within existing primary care capacity
The current primary care team will be able to absorb the increasing population during the
first year of construction however it will become increasingly difficult to meet the needs of
the new residents whilst maintaining the quality of care and access available to existing
residents on the Peninsula.
Page 94

11. Appraisal of the Options for Delivering Health and Social care to the Proposed New Housing Development
The current GPs each have a list of approximately 2000 patients and the new residents are
likely to increase this by 375 patients to 2375 within two years. This is an almost 20%
expansion in list size within a two year period.
There are already three locum GPs who provide additional support to ensure that patients are
seen quickly. Leaving the service as it is will increase the demands on this locum service
which is both financially and strategically unsustainable over the longer term. The increase in
new residents will also place increasing pressures on the existing community and district
nursing team making visits and appointments shorter and more hurried reducing the indirect
health benefits of human contact and communication that community and district nursing in
the home can provide for elderly people and their carers.
Overall, this scenario is likely to lead to lower staff morale in primary care, longer waiting
times for appointments, shorter and more hurried appointments and visits both in the
surgeries and in the community. Its main advantage is that it will save money in the short
term but it is unclear whether these savings will continue over the long term.
11.3.2 Additional GP and practice nurse
Adding capacity with an additional GP and practice nurse would enable the new residents to
be under the care of a named GP without increasing the lists of the existing GPs. The
difficulties with this option are the need for an extension as there is currently a lack of space
for an additional GP in the Shotley surgery. Apart from the cost this is likely to take an
average of eighteen months from design and planning permission to building and handover.
The recruitment and induction of a new GP is also likely to take six to nine months.
The positives of this option are its expansion of an established approach to primary care
delivery, its understanding and acceptance by patients and the enhanced capacity it would
bring to the existing primary care team. However, while it is very likely to meet the core
health care needs of the new residents this option will not take forward the health promotion
and disease prevention agenda that will be key to improving health and reducing demand on
health and social care services in the future.
11.3.3 Expansion of the community nursing team
The development of an enhanced community nursing team that provided clinic services from
facilities on the new development would provide a proactive health promotion and disease
prevention programme that would enhance health and reduce demand on health services over
the medium to long term. Recruitment of these community nurses and the management of
this team will be key issues alongside the purchasing or leasing of the facilities where these
clinics will take place. The implications of this approach are that the existing GPs will take
the new residents on their lists and increase their workload in the short term but this would
reduce over the medium to long term as the health promotion and disease prevention
activities take effect.
Page 95

11. Appraisal of the Options for Delivering Health and Social care to the Proposed New Housing Development
The negatives of this option are that people tend to be conservative with regard to their
healthcare and are likely to show a strong preference to visit their GP when they need health
advice and are likely to listen and act on the advice of their GP more than any other health
care professional. This option also assumes that these community nursing activities will
significantly reduce the demand on primary health care services within three years and that
the short term demands made on the existing primary care team will not lead to a loss of
morale and conflicts between the two teams.
11.3.4 Additional ‘outreach’ GP with community nurse
This option is a synthesis of options two and three with an additional GP recruited to provide
a traditional GP service to the residents of the new development and to lead on the
development of a health promotion and disease prevention community nurse-led outreach
clinic service from facilities located on the new development.
This option will marry the advantages of options two and three whilst minimising the
negatives of both these options. The benefits of this option is that it provides a traditional
‘face’ with new residents having a named GP who will also lead on the development of a
health promotion and disease prevention outreach programme that is community nurse-led.
This is likely to ensure that there is co-operation between the existing primary care team and
the new ‘outreach’ health care team. The focus on developing services on the site could
obviate, or at least significantly reduce, the urgent need to extend the existing surgery in
Shotley though it is likely to mean some reconfiguration of space within it there will be costs
to refurbishing the retail and commercial space on the development and the needs to make
this part of any Section 106 agreement.
11.3.5 Separate single-handed GP team
This option would involve recruiting a GP and setting up a single-handed practice. Besides the
recruitment and setting up of a separate practice this option goes against the latest good
practice guidance on delivering primary care. It will also disjoint what is currently an
integrated service on the Peninsula and may cause conflicts between the existing and new
practice. A single-handed GP is also likely to face more pressure and stress without having
adequate support to help her/him cope over the longer term.
Table 11.2 (next page) provides a summary of the type and level of the potential health
impacts, on the new and existing residents, likely for each of the five options. Overall Option
4 is likely to provide the highest degree of positive health impacts, whilst reducing the
negative impacts, for both the new and existing residents on the Shotley Peninsula.
Page 96

11. Appraisal of the Options for Delivering Health and Social care to the Proposed New Housing Development
Table 11.2: Potential health implications of the five options
Option Health Impact Comment
1. Existing practice copes with demand with emergency locums only.
--- The practice is already at the limits of its capacity and this is likely to lead to deteriorates and lower quality service to both new and exiting residents on the Peninsula.
2. An additional GP and practice nurse in the existing practice providing the majority of care from there.
++ This option will deal with the primary health care needs of the existing and new residents however it does little to move towards a more local community-based primary and public health care as advocated by the Wanless Report.
3. A community nurse team that delivers clinic-based services from the community facilities created on the HMS Ganges site.
++ This option moves strongly towards a community-based primary care and public health care approach but will easily act in isolation from the existing practice and create an un-integrated primary care service on the Peninsula with an increased potential for in-service conflicts
4. Expanded practice of additional GP and practice nurse delivers a range of outreach services based in the community facilities on the HMS Ganges site.
+++ This option, on balance is likely to have the best health gains for both the existing and new residents providing an integrated primary and public health care service that is local and community-based and moves in the direction the Wanless Report argues is likely to be the structure of primary care 2022
5. Separately contracted single-handed GP with practice team based in the community facilities on the HMS Ganges site.
-- This option is the least favourable as single-handed general practices are difficult to run, stressful and tend in the long run to deliver less effective care than group practices. This option will also lead to a les integrated service on the Peninsula with an increased potential for in-service conflicts.
11.4 Mitigation measures
• Early proactive planning is key to ensuring that there is minimal disruption in health and
social care services to the new and existing residents of the Peninsula.
• Consensus between the PCT and the primary health care team on the Peninsula is crucial.
• A health promotion and disease prevention programme involving the whole primary care
team serving the Peninsula is vital for the long term improvement of the health of local
people and the reduction in demand of secondary health care.
• The above is likely to mean an increase in personal social care services and community-
based management of long term illnesses and disabilities so that discussions to coordinate
and integrate social care services are also very important.
Page 97

11. Appraisal of the Options for Delivering Health and Social care to the Proposed New Housing Development
11.5 Residual effects
Whatever option is chosen there is no guarantee that it will meet all future needs of the local
people of Shotley and the wider Peninsula. The objective must therefore be to build capacity
that is flexible, accessible and proactive as well as cost-effective.
11.6 Enhancement opportunities
There are a number of opportunities to enhance the positive health benefits of any proposed
expansion and reconfiguration of the Peninsula’s health and social care services.
• Starting discussions on the potential to lease, on a peppercorn rent, some of the retail
and commercial space for some community facilities to provide the outreach clinic
services and other health promotion and disease prevention activities. These could also
provide space for the community development and youth work activities that already take
place in Shotley.
• Starting discussion on the feasibility of the community pharmacy currently being proposed
in Holbrook within the retail and commercial space provided by the new development.
This would provide a complementary service to that already provided by the GP
dispensary and enhance the pharmacy provision on the Peninsula.
• Exploring the feasibility of putting an NHS dental service within the retail and commercial
space provided by the new development.
11.7 Conclusion
Whatever option is chosen, early planning and the building of consensus between all health
and social care agencies is crucial for long term success.
All the options require the recruitment of a range of health staff and the provision of
additional premises from which to work.
Ensuring easy and local access to services is an important consideration given the poor levels
of public transport and poor road network making access to health and social care services
prone to disruption given the increase in people and cars without a corresponding increase in
the capacity of the road network on the Peninsula.
For the long term, option four, a synthesis of options two and three, is likely to provide the
most positive health benefits, the fewest negatives and the greatest degree of flexibility in
dealing with the long term health and social care needs of the potential new and existing
residents of the Shotley Peninsula.
Page 98

12. Conclusion and Recommendations
12. Conclusion and Recommendations
12.1 Introduction
This chapter summarises the key themes emerging from the health impact assessment (HIA)
on the development proposed by Haylink Ltd for the HMS Ganges site.
This HIA has assessed:
• the positive and negative health effects arising out of the development for existing local
residents living on the Shotley Peninsula,
• the positive and negative health effects arising out of the development for residents of
the new housing development on the HMS Ganges site,
• the positive and negative implications for the primary and secondary health services of
the new housing development,
• key mitigation and enhancement measures to reduce the potential negative and positive
health effects for existing and new residents, and
• key mitigation and enhancement measures for the local primary and secondary health
services for the Shotley Peninsula area.
Communities, settlements and landscapes are never static but are undergoing continual
change. The majority of these wanted and unwanted changes are gradual and allow
adaptation to the new conditions and circumstances. However, there are times in the lives of
communities, settlements and landscapes when these changes are major such that the
resources and resilience needed to cope and adapt to these changes are strained. This is
especially so when not all the members of a community or set of communities want these
changes.
The aim must therefore be to ensure that the community, settlements and landscapes are
supported and enabled on the one hand to have adequate resources to cope with the
disruptions caused by any proposed change whilst on the other hand ensuring that these
disruptions are minimised; that there is continuous communication on the likely changes in
intensity and duration of the disruptions; and that there are positive tangible short term and
long term benefits for existing communities and settlements.
12.2 Positive and negative health effects for existing residents
Overall existing residents will face significant disruption during the construction period. This
will create some moderate to major, medium term, temporary negative health effects on
existing residents’ sense of wellbeing and their general quality of life.
Page 99

12. Conclusion and Recommendations
There are two key positive health impacts for existing residents during the construction
phase: the potential employment and business opportunities for the local people and the
remediation of the existing contamination on the HMS Ganges site.
There are four key negative health impacts from the construction phase: the disruption in
access to health and social care services, the increase in heavy lorry traffic, the loss of social
capital and cohesion and the noise, dust and dirt generated from the site and the lorries.
The majority of residents will benefit from the positive health benefits and be affected by
the negative health effects during the construction phase. Those likely to be the most
affected are those residents living adjacent to the site especially those living near the
entrance and exit.
The four key positive health impacts for existing residents will be: that the HMS Ganges site
will come back into use with landscaped green and open public space that will be accessible
to existing residents; the remediate this brownfield site which has some contaminated land,
the potential easy access to retail amenities and community facilities in a new village square;
the protection and enhancement of the local cultural heritage through the preservation of the
Martello Tower, the Fort and the building of the Ganges museum; and the development will
also reconnect the existing marina development to Shotley Village creating a more physically
integrated community at the end of the Peninsula.
The key three negative health impacts for existing residents will be: the strain on existing
health, social care, education and leisure services; the increase traffic and congestion caused
by the increase in cars leading to more road traffic accidents and reduced access to key
services; and the strain on social capital and cohesion because of the sense of ‘overcrowding’
created influx of new people onto the Peninsula and the differing potentially conflicting ways
of life and values of the new residents.
12.3 Positive and negative health effects for the potential new residents
Some residents of the new development especially those who move into the first phase of the
development will the same disruptions as existing residents however they will have chosen to
live in an area where construction work is taking place and hence are likely to face less
psychosocial stress than long-standing residents.
The key three positive health impacts for new residents on the development will be: access to
good quality starter, affordable and other homes; access to public green space and the
opportunity to live in a rural area with a high quality natural environment and rich cultural
heritage; and the potential easy access to retail amenities and community amenities in the
village square.
Page 100

12. Conclusion and Recommendations
The key three negative health impacts for new residents on the development will be: the
strain on existing health, social care, education and leisure services; the increase traffic and
congestion caused by the increase in cars leading to more road traffic accidents and reduced
access to key services; and the difficulties in building a relationship with existing residents
strain on social capital and cohesion because their differing ways of life and values which may
make it hard for them to adapt to the ways of life and community routines and norms built up
by existing residents.
12.4 Positive and negative implications for the health and social care services
The four key positives implications on health and social care services will be that: the new
residents are likely to be in fairly good to good health; the negative health impacts during the
construction phase will largely be temporary and for the majority of residents of mild to
moderate severity; there will be more open public green space that will be accessible to new
and existing residents; and the potential retail amenities and community facilities that will
improve access to such amenities and facilities for both new and existing residents
The three key negatives health implications on health and social care services will be that:
the existing primary care team will not be able to meet the needs of the new residents; any
option to provide health and social care services to these new residents whilst maintaining
the quality of care to existing residents needs has resource implications – financial, human
and organisational and the existing poor public transport and road network will further reduce
the accessibility of some health and social care services
12.5 Mitigation and enhancement measures for existing and new residents
A good communication programme led by the local (planning) authority needs to be
developed and implemented before the start of construction. This should involve ongoing
dialogue with the parish councils and public meetings where necessary to deal with issues
that arise during the construction phase. The developer also needs to be proactive in listening
to local complaints during the construction phase. Complaints and concerns can be resolved
at an early stage by having regular meetings with a representative from Shotley Parish
Council, Haylink, Babergh planning department and Central Suffolk PCT. These meetings
should initially be weekly and then become monthly as the construction progresses and the
community’s concerns are resolved and a trusting relationship develops between the key
stakeholders – community, developer and statutory agencies.
Investigation and commitment to traffic calming measures and re-configuration of existing
accident ‘hot spots’. A detailed review of the road traffic accident data over the construction
and early operation period will highlight increases in accidents on the B1456 and on other
parts of the Peninsula’s road network.
Page 101

12. Conclusion and Recommendations
Adherence to best practice in housing design, construction, occupational health and safety
and a secure and patrolled construction site will ensure that the hazards and potential
negative health effects from the site itself will be mitigated. An example is the watering
down of demolition work so that the dust thrown up into the air is localised to the site itself
and not to neighbouring homes and gardens.
It is also important to ensure at this early stage that some of the retail and commercial
space, on a peppercorn rent, is used to develop a community centre-type facility where
activities like health promotion clinics, mother and toddler groups, a crèche, community
internet café, indoor leisure activities and youth work and community development initiatives
can operate from. It is also important at this stage to explore the feasibility of siting a dental
service and community pharmacy on the development as these would also enhance access,
increase the amenities available and reduce the impacts on the road network. All the above
will serve to focus community activities and build both social capital and cohesion between
new and existing residents as both see and feel the benefits of the new development.
Finally, more community development and youth work resources over the next three years
would help develop the resilience of the community to deal with the disruptions of the
constructions and actualise the potential positive health benefits that the completed
development would have for existing residents in particular.
12.6 Mitigation and enhancement measures for health and social care services
There are five major options for meeting the health needs of the incoming community and
maintaining the quality of health and social care services for existing residents. The first is to
assume that the increasing workload will be borne by the existing GP practice team with
emergency demand being dealt with by additional locum GPs. The second option is to bring
an additional GP and practice nurse into the existing practice with this GP providing the
majority of care to the new residents from there. The third option is to develop a community
nurse team that delivers clinic-based services from community facilities on the HMS Ganges
site thereby reducing the workload on the existing GP team and so enabling them to increase
their list sizes. The fourth option is a synthesis of option two and three where an additional
GP and community nurse deliver surgery and outreach clinic services. The fifth option would
be to have a separately contracted single-handed GP and practice team based in the new
development.
Whatever option is chosen, early planning and the building of consensus between all health
and social care agencies is crucial for long term success. All the options require the
recruitment of a range of health staff and the provision of additional premises from which to
work. Ensuring easy and local access to services is an important consideration given the poor
levels of public transport and poor road network making access to health and social care
Page 102

12. Conclusion and Recommendations
services prone to disruption given the increase in people and cars without a corresponding
increase in the capacity of the road network on the Peninsula. For the long term, option four,
a synthesis of options two and three, is likely to provide the most positive health benefits,
the fewest negatives and the greatest degree of flexibility in dealing with the long term
health and social care needs of the potential new and existing residents of the Shotley
Peninsula.
12.7 Monitoring and evaluation of the health impacts
There a number of ways of monitoring the construction phase to ensure that negative health
impacts are reduced and positive health impacts enhanced. Our suggestion are:
Construction phase
1. Monitoring the number of written and phone complaints (and compliments) received by the construction team and sub-contractors.
2. Monitoring the number of local people who are employed on the development site.
3. Regular meetings with the parish councils to get feedback on informal community comments and concerns.
4. Monitoring the number of crimes and nuisance occurring that are related to the development.
5. Monitoring the number of road incidents and the places where traffic problems are occurring.
Operation phase
6. Monitoring the accessibility and activities occurring in the open green space created especially by existing residents.
7. Monitoring the number and type of retail amenities and businesses moving onto the development.
8. Regular meetings with the parish councils to get feedback on informal community comments and concerns.
9. Monitoring the number of crimes and nuisance occurring that are related to the development.
10. Monitoring the number of road incidents and the places where traffic problems are occurring.
12.8 Recommendations
This report outlines some of the key issues that need to be taken forward to ensure that the
negative health impacts of the proposed developed are minimised and the positive health
impacts are maximised. These are:
• Discussions between the primary care team on the Peninsula, Central Suffolk PCT and
Suffolk Social Services on how they will meet the needs of the new residents whilst
maintaining the quality of care and access to services of existing residents.
Page 103

12. Conclusion and Recommendations
• Discussions between Central Suffolk PCT, Suffolk Social Care Services, Babergh Culture
and Leisure Services, Babergh Planning Department and Haylink on the opportunities to
develop a community centre and range of community facilities in the retail and
commercial space that has been proposed.
• Discussions between Central Suffolk PCT, Suffolk Social Care Services, Suffolk
Environment and Transport Department and the Police to investigate the best way of
improving access and movement across the existing road network through the use of
traffic calming measures and reconfigurations of junctions that have caused traffic
incidents and accidents.
A suggested health and social care action plan for the Shotley Peninsula based on the
above recommendations is described on the next page.
On a wider and more strategic note it would be useful for Central Suffolk PCT to undertake:
• A wider strategic review based on the Suffolk Structure Plan and the Babergh and Mid-
Suffolk Local Plans to assess the health and social care implications of other new housing
developments that are likely to be occurring within the area served by Central Suffolk
PCT.
• A wider strategic review based on the Babergh and Mid Suffolk Transport Plans of the
transport needs and initiatives in the area served by Central Suffolk PCT and its
implications in terms of traffic incidents and access for health and social cares services
especially but not restricted to the new housing developments that are likely to be
occurring within its area.
Page 104

12. Conclusion and Recommendations
Table 12.1 Shotley Peninsula health and social care development action plan
Date (2004) Task Stakeholders involved
April Take as a starting point the working proposition that planning permission will be given for the HMS Ganges development proposed by Haylink Ltd.
Central Suffolk PCT Suffolk Social Services Shotley Peninsula GPs Shotley Parish Council
April Explicitly agree on and sign up, in principle, to one of the five options for dealing with the health and social care needs of the new incoming (1500 within two years of planning permission being given) and existing (8000) residents of the Shotley Peninsula.
Central Suffolk PCT Suffolk Social Services Shotley Peninsula GPs
May-Jul Create a steering group led by Central Suffolk PCT that has strategic planning and delivery representatives from the PCT and from Suffolk Social Services with at least one GP partner from the GP practice on the Peninsula, a member of Shotley Parish Council and a representative from a voluntary sector health and social care agency. Other representatives can be co-opted as and when necessary.
The agenda would be to use the health impact assessment report to develop a detailed costed action plan for managing the construction phase and the final agreed upon option for dealing with the health and social care needs of new and existing residents during the operation phase of the proposed development.
Central Suffolk PCT Suffolk Social Services Shotley Peninsula GPs Shotley Parish Council Age Concern or other voluntary sector agency Suffolk Ambulance Trust
June-Aug The steering group, once it has drawn up an outline plan and costings, starts discussions with Haylink Ltd through planning consultant Philippa Mason to develop a communication strategy, what principles of good construction practice should be used and a Section 106 agreement to deal with as many of the health and social care issues as possible.
Central Suffolk PCT Suffolk Social Services Haylink Ltd Babergh Planning Dept.
Sep Agree a communication strategy and principles of good construction practice that should be abided by and the Section 106 agreement with Haylink Ltd.
Central Suffolk PCT Suffolk Social Services Haylink Ltd Babergh Planning Dept.
Oct-onwards Steering group through a project leader coordinates activities to ensure that the action plan is implemented if/when planning permission is given.
Central Suffolk PCT Suffolk Social Services Haylink Ltd Babergh Planning Dept. Shotley Peninsula GPs Shotley Parish Council
Page 105

Appendix 1: Scoping Paper
Appendix 1
Scoping Paper
Page 106

Appendix 1: Scoping Paper
Table of Contents
1 Introduction 108
2 Scoping of the key HIA sections 109
Health and social care access .................................................... 109 Social cohesion...................................................................... 110 Housing............................................................................... 110 Transport and mobility ............................................................ 111 Employment ......................................................................... 111 Education ............................................................................ 111 Crime ................................................................................. 111 Culture and leisure................................................................. 112 Lifestyle, daily routines and amenities ......................................... 112 Environment......................................................................... 112
Page 107

Appendix 1: Scoping Paper
INTRODUCTION The aim of this paper is to do a rapid scoping of the health issues related to the HMS Ganges development using as much readily available information as possible. This scoping has identified that the health impact assessment (HIA) should focus on the health impacts of the residents of the Shotley peninsula and in particular those residents living in Shotley village immediately adjacent to the proposed new development. In order of priority the key sections of the HIA should be the potential positive and negative impacts on:
1. health and social care services 2. social cohesion 3. housing 4. transport and mobility 5. employment 6. education 7. crime 8. culture and leisure 9. lifestyle, daily routines and amenities 10. environment
The following pages describe in more detail the first five key sections and what should be addressed within each. It is worthwhile re-stating the five objectives of the health impact assessment before moving on. The HIA will investigate
6. the positive and negative health effects arising out of the development for existing local residents living on the Shotley Peninsula,
7. the positive and negative health effects arising out of the development for residents of the new housing development on the HMS Ganges site,
8. the positive and negative implications for the primary and secondary health services of the new housing development,
9. key mitigation and enhancement measures to reduce the potential negative and positive health effects for existing and new residents, and
10. key mitigation and enhancement measures for the local primary and secondary health services for the Shotley Peninsula area.
Page 108

Appendix 1: Scoping Paper
SCOPING OF THE KEY HIA SECTIONS HEALTH AND SOCIAL CARE ACCESS The Babergh Council data shows that there are approximately 3000 residents of Shotley parish. The new development of 400 houses or so will mean that the local population will increase by between 800-1200 people – older people especially couples, some young families and some young couples with no children. The majority of these people will come from outside Shotley and many are likely to come from outside the district of Babergh i.e. the new residents of the development will not be simply existing residents of Babergh moving house. The local health services, in particular the primary care team in the area, will need to cope with an increase of between 25-40% of the existing population within a two year period from when the homes are completed. The characteristics of the population are mainly white, with a small number of ethnic minorities, and a predominance of older people. The health of this community overall is good to very good. There is currently one primary care team based in Shotley with five GPs. Key issues that the HIA will aim to address are: • What are the current primary facilities and services offered by the primary care
team? • What are the current pressures on these services? • What are the likely future health needs and health service pressures associated with
the changing demographic profile of more old people and fewer younger people of working age within the current resident population?
• What is the likely population profile of the new development in terms of gender and
age ranges? What are their potential health needs? • How can current facilities and services be modified and expanded to cope with the
likely increase in population due to the new development? • What resource implications are there – in human, time, and financial terms? Is there a
need for more health professionals; if so what kind? Do health facilities need to be upgraded?
• What concerns, if any, do local health professionals have about the proposed
development? • The same set of questions will need to be asked about the social care services in the
area. This issue is important for central Suffolk PCT and also for Haylink as having good health and social care services in the area will be a strong selling point for the homes on the HMS Ganges site.
Page 109

Appendix 1: Scoping Paper
SOCIAL COHESION The Master Plan shows a good physical layout of the proposed development that is in line with best housing layout practice. However physical layout and integration with the existing housing is only one strand in creating and maintaining an integrated and socially cohesive community. The Master Plan objective is to create a balanced community with a mix of privately owned and social housing of various sizes. Creating a socially inclusive and cohesive community both within the new development and between the new development and the older existing community is vital in producing a health-promoting social environment. New developments can often create an ‘us’ and ‘them’ mentality which separates and cuts off people thereby reducing the potential regenerative benefits of the new developments. Key issues that the HIA will aim to address are: • What concerns, if any, have local people expressed about the proposed development?
Are there specific health or social concerns? • What are the physical pathways of access between the existing settlement and the
new development? • Where are potential new amenities located within the new development? Are they
accessible to existing residents of the existing settlement? • Are the existing amenities accessible to the new people moving into the new
development? • How is the new community integrated and included in the daily life and routines of
the existing settlement? • Does transport and mobility infrastructure enhance or reduce social cohesion and
integration? • What are the potential positive and negative effects on the existing local people’s
sense of identity and community? HOUSING The Master Plan follows established best practice in housing design and construction. This section will largely highlight the positive health benefits of regenerating brownfield areas and building new homes that are balanced with a mix of privately owned houses and social housing of various sizes as determined by identified local needs. Investment and redevelopment of areas when sensitively done can enhance a local area community. Key issues that the HIA will aim to address are: • What are the health and social benefits of new housing developments in rural areas? • How many residents of Shotley and Babergh are likely to benefit from the new
housing? • How will the new housing influence the local housing market? Will it stimulate
further demand from people outside the area and hence make it more difficult for local people to buy in the local area?
Page 110

Appendix 1: Scoping Paper
• What is the previous track record of the developers on previous developments? TRANSPORT AND MOBILITY The ability to travel easily is crucial to accessing health and social care services as well as leisure and other amenities including local shops. Having extensive and integrated pedestrian paths, cycle ways, private car and public bus, ferry, train and tram links are vital in indirectly ensuring the health and wellbeing of communities. Key issues that the HIA will aim to address are: • What are the current transport links for the existing settlement? • What are the proposed transport links for the new development and are they
integrated with the existing settlement? • Is the public transport network extended into the new development? • Are current amenities and employment accessible by foot, cycle and public transport
and are any new amenities being planned to be accessible by foot, cycle and public transport?
EMPLOYMENT Employment and the lack of it is a key determinant of good or poor health. Key issues that the HIA will aim to address are: • How will the new residents potentially affect the local employment market? Could
they push existing residents out of jobs? • What new jobs will be temporarily and permanently created in the area? What will be
the quality of those jobs? EDUCATION The developer is already having discussions with the education department and therefore educational issues will only be touched upon. CRIME Crime and the implications of the new housing development on crime are difficult to gauge. The Master Plan follows established best practice in housing design and layout to build out crime. There is a potential during the construction phase for there to be significant disruption which could generate crime in and around the construction site. This needs to be balanced by the several instances of arson, vandalism and minor accidents to trespassers at the site, despite the on-site security provided by the current owner, since the Police stopped using the site for training 10 or so years ago.
Page 111

Appendix 1: Scoping Paper
CULTURE AND LEISURE Cultural and leisure activities and amenities have direct and indirect influence on health. The key question that this section will address is whether cultural and leisure activities will be enhanced or reduced by the proposed development. LIFESTYLE, DAILY ROUTINES AND AMENITIES Disruptions to individual and family lifestyles and daily routines especially during the construction phase can have severe temporary negative effects on health and wellbeing. This section will investigate how daily routines and lifestyles might be affected by the proposed new development. ENVIRONMENT This has been extensively covered by the environmental statement and sustainability appraisal and will not be investigated except for specific aspects of environmental health which have not been discussed in the other two documents.
Page 112

Appendix 2: Administrative Map of Babergh District
Appendix 2
Administrative Map
of Babergh District
Page 113

Appendix 2: Administrative Map of Babergh District
Page 114

References
References
1. The Town and Country Planning (Environmental Impact Assessment) (England and Wales) Regulations 1999. No. 293. 1999. available at http://www.hmso.gov.uk/si/si1999/19990293.htm
2. Office of the Deputy Prime Minister. Circular 02/99: environmental impact assessment. 2002. Available at http://www.planning.odpm.gov.uk/circulars/02_99/01.htm
3. WHO European Centre for Health Policy. 1999. Health impact assessment: main concepts and suggested approach. Gothenburg consensus paper. 1-10. Brussels, WHO Regional Office for Europe, ECHP. Available: http://www.who.dk/document/PAE/Gothenburgpaper.pdf
4. Cave, B., Curtis, S. et al. Health impact assessment for regeneration projects. Volumes I-III. 2001. London, East London and the City Health Action Zone and Queen Mary, University of London . 27-1-2003. Available at http://www.geog.qmul.ac.uk/health/guide.html
5. Cave, B. and Penner, S. Frequently asked questions about HIA. 2001. London, Queen Mary, University of London. Available at http://www.geog.qmul.ac.uk/health/guide.html
6. University of Ottawa. 2003. Measurement on health. Epi5251 online course notes. Available at http://courseweb.edteched.uottawa.ca/epi5251/Index_notes/Definitions%20of%20Health.htm
7. Health promotion: a discussion document. Copenhagen, WHO, 1984
8. Vingilis & Sarkella, Social Indicators Research 1997; 40:159
9. Last JM. Dictionary of epidemiology. IEA, 1995:73
10. Dahlgren, G. and Whitehead, M. Policies and strategies to promote social equity in health. 1991. Stockholm, Institute for Future Studies.
11. Royal Commission on Environment and Pollution. 21st report: setting environmental standards. 2003. Available at http://www.rcep.org.uk/reports2.html
12. Funtowicz, S. O and Ravetz, J. R. "Three types of risk assessment and the emergence of post-normal science" in Social theories of risk eds. Krimsky, S. and Golding, D. Westport, Conn. ; London: Praeger. 1992.
13. Ison, E., NHS Executive, Resource for health impact assessment. London. 2000. Available at http://www.londonshealth.gov.uk/allpubs.htm#hia
14. Guba, G. E. and Lincoln, Y. S. 1994. "Competing paradigms in qualitative research," in Handbook of qualitative research. Edited by N. K. Denzin and Y. S. Lincoln, Thousand Oaks: Sage.
15. BUJ Architects. 2003. HMS Ganges master plan. Available at http://www.babergh-south-suffolk.gov.uk/planctrl/planapps/ganges/mastplan.htm
16. Office of National Statistics. 2003. Census 2001 neighbourhood statistics. Available at http://www.ons.gov.uk
17. Suffolk Development Agency 2003. Suffolk observatory. Available at http://www.suffolkobservatory.info/
18. Geoff Kistner. 2003. Report.C97. Babergh District Council. Available at http://www.babergh-south-suffolk.gov.uk/legaladm/ccpapers/reports/c097-pt1.htm
19. Department of Transport, Environment and Regions. 2000. Indices of Deprivation. Available at http://www.odpm.gov.uk/stellent/groups/odpm_urbanpolicy/documents/page/odpm_urbpol_608140.hcsp
20. Babergh District Council. Babergh Local Plan. 2003. Second Deposit Draft. Alteration No. 2. Available at http://www.babergh-south-suffolk.gov.uk/planplcy/blp2dep/text.htm
Page 115

References
21. Informal interviews with key informant residents on the Shotley Peninsula. 2004.
22. SQW Ltd. 2003. A profile of the rural Suffolk economy. Suffolk Development Agency. Available at http://www.suffolkobservatory.info/Reports.asp?ThemeID=2
23. Haylink Ltd. 2003. HMS Ganges Environmental Statement. Available at http://www.babergh-south-suffolk.gov.uk/planctrl/planapps/ganges/ganges.htm
24. Leisure and Community Services. 2004. Babergh Disrict Council. Available at http://www.babergh-south-suffolk.gov.uk/leiscoms/leisure/leisure.htm
25. Carr, C. and Steel G. 1997. Developing Work with Young People in the Holbrook and East Bergholt Areas
26. Steel G. 2003. Recruiting Volunteer Youth Workers on the Shotley Peninsular – some discussion points.
27. Milner, S et al. 2004. Health Impact Assessment Research and Development Programme. School of Health, Community and Education Studies, Northumbria University. Available at http://online.northumbria.ac.uk/faculties/hswe/hia/index.htm
28. Deaville, J. A. 2001. The nature of rural general practice in the UK: preliminary research. Institute of Rural Health and the General Practitioners Committee of the BMA. Available at http://www.rural-health.ac.uk/publications/respub.php
29. Deaville, J. A. 2001. The nature of rural general practice in the UK: preliminary research. Institute of Rural Health and the General Practitioners Committee of the BMA. Available at http://www.rural-health.ac.uk/publications/respub.php
30. Scottish Office. Social inclusion: opening the door to a better Scotland. Edinburgh: Scottish Office; 1999. (Secondary Citation) Cited in Brennan A, Rhodes J, Tyler P. The nature of local area social exclusion in England and the role of the labour market. Oxford Review of Economic Policy 2000;16(1):129-146.
31. Gordon D, Adelman L, Ashworth K, J B, Levitas R, Middleton S, et al. Poverty and social exclusion in Britain. York: Joseph Rowntree Foundation; 2000.
32. Kempson E, Whyley C. Keep out or opted out?: understanding and combating financial exclusion: Policy Press; 1999.
33. Collard S, Kempson E, Whyley C. Tackling financial exclusion: an area based approach: The Policy Press; 2001.
34. Rowlinson K. Fate, hope and insecurity: future orientation and forward planning: Policy Studies Institute; 2000.
35. Dowler E. Food and poverty: the present challenge. Benefits 1999;24:3-6.
36. Caraher M, Dixon P, Lang T, Carr-Hill R. Barriers to accessing healthy foods: differentials by gender, social class, income and mode of transport. Health Education Journal 1998;53(3):191-201.
37. Ellaway A, Macintyre S. Shopping for food in socially contrasting localities. British Food Journal 2000;102(1):52-59.
38. Robinson N, Caraher M, Lang T. Access to shops: the views of low income shoppers. Health Education Journal 2000;59:121-136.
39. Burridge R, Ormandy D, editors. Unhealthy housing: research, remedies and reform. London: E and FN Spon; 1993.
40. Christopherson O. Mortality during the 1996/7 winter. Population Trends 1997;90:11-17.
41. Markus T. Cold, condensation and housing poverty. In: Burridge R, Ormandy D, editors. Unhealthy housing: research, remedies and reform. London: E and FN Spon; 1993.
42. Acheson D. Independent inquiry into inequalities in health: report. London: Stationery Office; 1998.
Page 116

References
43. Speak S, Graham S. Service not included: social implications of private sector service restructuring in marginalised neighbourhoods: Polity Press; 2000.
44. Gordon D. Inequalities in income, wealth and standard of living in Britain. In: Pantazis C, Gordon D, editors. Tackling inequalities: where are we now and what can be done? Bristol: The Policy Press; 2000. p. 25-59.
45. Baggott R. Public health: policy and politics: Macmillan; 2000.
46. Macintyre S. Geographical inequalities in mortality, morbidity and health-related behaviour in England. In: Gordon D, Shaw M, Dorling D, Davey Smith G, editors. Inequalities in health: the evidence presented to the Independent Inquiry into Inequalities in Health, chaired by Sir Donald Acheson: The Policy Press; 1999.
47. Glennerster H, Matsaganis M, Owens P, Hancock S. GP fundholding: wild card or winning hand? In: Robinson R, Le Grand J, editors. Evaluating the NHS reforms. London: King's Fund; 1993. p. 74-107.
48. Newton J. Fundholding in the Northern Region: the first year. British Medical Journal 1993;306:375-378.
49. Beecham L. Fundholders' patients are treated quicker. British Medical Journal 1994;308:11.
50. Avlund K, Damsgaard M, Holstein B. Social relations and mortality: an eleven year follow up study of 70-year old men and women in Denmark. Social Science and Medicine 1998;47(5):635-643.
51. House J, Landis K, Umberson D. Social relationships and health. Science 1988;241:540-5.
52. Kaplan G, Salonen J, Cohen R, et al. Social connections and mortality from all causes and cardiovascular disease: prospective evidence from eastern Finland. American Journal of Epidemiololgy 1988;128:370-380.
53. Kawachi I, Colditz G, Ascherio A, Rimm W, Giovannucci E, Stampfer M, et al. A prospective study of social networks in relation to total mortality and cardiovascular disease in men in the USA. Journal of Epidemiology and Community Health 1996;50:245-51.
54. Olsen R, Olsen J, Gunner-Svennson F, Waldstrom B. Social networks and longevity: a 14 year follow up study among elderly in Denmark. Social Science and Medicine 1991;33:1189-1195.
55. Bowling A, Browne P. Social networks, health and emotional well-being amongst the oldest old in London. Journal of Gerontology 1991;46:S20-32.
56. Holahan CJ, Moos R, Holahan CK, Brennan P. Social support, coping and depressive symptoms in a late-middle-aged sample of patients reporting cardiac illness. Health Psychology 1995;14:152-163. (Secondary Citation) Cited in Berkman L, Glass T. Social integration, social networks, social support and health. In: Berkman L, Kawachi I, editors. Social epidemiology: Oxford University Press; 2000. p. 137-173.
57. Murphy E. Social origins of depression in old age. British Journal of Psychiatry 1982;141:135-42.
58. Henderson S. Social relationships, adversity and neurosis: an analysis of prospective observations. British Journal of Psychiatry 1981;138:391-8.
59. Matthews S, Stansfield S, Power C. Social support at age 33: the influence of gender, employment status and social class. Social Science and Medicine 1999;49:133-142.
60. Lekander M, Fuerst C, Rotstein S, Blomgren H, Fredikson M. Social support and immune status during and after chemotherapy for breast cancer. Acta Oncologica 1996;35(1):31-37. (Secondary Citation) Cited in Matthews S, Stansfield S, Power C. Social support at age 33: the influence of gender, employment status and social class. Social Science and Medicine 1999;49:133-142.
61. Fitzpatrick R, Newman S, Archer R, Shipley M. Social support disability and depression: a longitudinal study of rheumatoid arthritis. Social Science and Medicine 1991;33(5):605-611. (Secondary Citation) Cited in Matthews S, Stansfield S, Power C. Social support at age 33: the influence of gender, employment status and social class. Social Science and Medicine 1999;49:133-142.
Page 117

References
62. Oakley A, Hickey D, Rigby A. Love or money?: social support, class inequality and the health of women and children. European Journal of Public Health 1994;4:265-274. (Secondary Citation) Cited in Matthews S, Stansfield S, Power C. Social support at age 33: the influence of gender, employment status and social class. Social Science and Medicine 1999;49:133-142.
63. Oakley A, Rigby A, Hickey D. Life stress, support and class inequality: explaining the health of women and children. European Journal of Public Health 1994; 4:81-91. (Secondary Citation) Cited in Matthews S, Stansfield S, Power C. Social support at age 33: the influence of gender, employment status and social class. Social Science and Medicine 1999;49:133-142.
64. Kaplan R, Hartwell S. Differential effects of social support and social networks on physiological and social outcomes in men and women with type 11 diabetes mellitus. Health Psychology 1987;6(5):387-398. (Secondary Citation) Cited in Matthews S, Stansfield S, Power C. Social support at age 33: the influence of gender, employment status and social class. Social Science and Medicine 1999;49:133-142.
65. Tiller J, Sloane G, Schmidt U, Troop N, Power M, Treasure J. Social support in patients with anorexia nervosa and bulima nervosa. International Journal of Eating Disorders 1997;21(1):31-38. (Secondary Citation) Cited in Matthews S, Stansfield S, Power C. Social support at age 33: the influence of gender, employment status and social class. Social Science and Medicine 1999;49:133-142.
66. Rogers M, Peoples-Sheps M, Suchindran C. Impact of a social support program on teenage prenatal care use and pregnancy outcomes. Journal of Adolescent Health 1996;19:132-140. (Secondary Citation) Cited in Matthews S, Stansfield S, Power C. Social support at age 33: the influence of gender, employment status and social class. Social Science and Medicine 1999;49:133-142.
67. Stephens C, Long N. The impact of trauma and social support on post traumatic stress disorder: a study of new Zealand police officers. Journal of Criminal Justice 1997;25(4):303-314. (Secondary Citation) Cited in Matthews S, Stansfield S, Power C. Social support at age 33: the influence of gender, employment status and social class. Social Science and Medicine 1999;49:133-142.
68. Brugha T, Bebbington P, MacCarthy B, Sturt E, Wykes T, Potter J. Gender, social support and recovery from depressive disorders: a prospective clinical study. Psychological Medicine 1990;20:147-156. (Secondary Citation) Cited in Matthews S, Stansfield S, Power C. Social support at age 33: the influence of gender, employment status and social class. Social Science and Medicine 1999;49:133-142.
69. Stansfield S, Rael E, J H, Shipley M, Marmot M. Social support and psychiatric sickness absences: a prospective study of British civil servants. Psychological Medicine 1998;27: 35-48. (Secondary Citation) Cited in Matthews S, Stansfield S, Power C. Social support at age 33: the influence of gender, employment status and social class. Social Science and Medicine 1999;49:133-142.
70. Young M, Willmott P. Family and kinship in East London. London: Routledge & Kegan Paul; 1957. (Secondary Citation) Cited in Pereira C. Anthology: the breadth of community. In: Bornat J, Pereira C, Pilgrim D, Williams F, editors. Community care: a reader: Macmillan; 1993.
71. Pereira C. Anthology: the breadth of community. In: Bornat J, Pereira C, Pilgrim D, Williams F, editors. Community care: a reader: Macmillan; 1993. p. 5-20.
72. Hawe P, Shiell A. Social capital and health promotion: a review. Social Science and Medicine 2000;51:871-885.
73. Kelly M, Campbell C. Social capital - making the links with community health. Healthlines 1999(June):24-25.
74. Jacobs J. The life and death of great American cities. New York: Random House; 1961. (Secondary Citation) Cited in Woolcock M. Social capital and economic development: toward a theoretical synthesis and policy framework. Theory and Society 1998;27:151-208.
75. Loury G. A dynamic theory of racial income differences. In: Wallace P, LeMund A, editors. Women, minorities and employment discrimination. Lexington, Mass.: Lexington Book; 1977. (Secondary Citation) Cited in Woolcock M. Social capital and economic development: toward a theoretical synthesis and policy framework. Theory and Society 1998;27:151-208.
76. Bourdieu P, Passeron J-C. Reproduction in education, society and culture. London: Sage; 1977. (Secondary Citation) Cited in Woolcock M. Social capital and economic development: toward a theoretical synthesis and policy framework. Theory and Society 1998;27:151-208.
Page 118
References
77. Coleman J. Social capital in the creation of human capital. American Journal of Sociology 1988;94:S95-S120.
78. Portes A, Sensenbrenner J. Embeddedness and immigration: notes on the social determinants of economic action. American Journal of Sociology 1993;98(6):1320-1350. (Secondary Citation) Cited in Woolcock M. Social capital and economic development: toward a theoretical synthesis and policy framework. Theory and Society 1998;27:151-208.
79. Putnam R. Making democracy work: civic traditions in modern Italy. New Jersey: Princeton University Press; 1993.
80. Putnam R. Bowling alone: America's declining social capital , cited in Woolcock (1998). Journal of Democracy 1995;6:65-78. (Secondary Citation) Cited in Woolcock M. Social capital and economic development: toward a theoretical synthesis and policy framework. Theory and Society 1998;27:151-208.
81. Putnam R. The strange disappearance of civic America. The American Prospect 1996;7(24). http://www.prospect.org/print/V7/24/putnam-r.html [Accessed on 2001/11/19]
82. Campbell C, Wood R, Kelly M. Social capital and health. London: Health Education Authority; 1999.
83. Gilles P, Tolley K, Wolstenhome J. Is AIDS a disease of poverty? AIDS Care 1996;8(3):351-63. (Secondary Citation) Cited in Campbell C, Wood R, Kelly M. Social capital and health. London: Health Education Authority; 1999.
84. Dalgard O, Haheim L. Psychosocial risk factors and mortality: prospective study with special focus on social support, social participation and locus of control in Norway. Journal of Epidemiology and Community Health 1998;52:476-81.
85. Byrgen L, Benson B, Johansson S. Attendance at cultural events, reading books or periodicals, and making music or singing in a choir as determinants for survival: Swedish interview survey of living conditions. British Medical Journal 1996;313:1577-80. 86. Glass T, Mendes de Leon C, Marottoli R, Berkman L. Population based study of social and productive activities as predictors of survival among elderly Americans. British Medical Journal 1999;319: 478-83.
87. Rietschlin J. Voluntary association membership and psychological distress. Journal of Health and Social Behaviour 1998;39:348-355.
88. Stansfeld, S. A. "Social support and social cohesion" in Social determinants of health eds. Marmot, M. and Wilkinson, R. G. Oxford, Oxford University Press. 1999: pp.155-178.
89. Wilkinson R. Unhealthy societies: the afflicitions of inequality. London: Routledge; 1996.
90. Wilkinson R. Health inequalities : relative or absolute material standards? British Medical Journal 1997;314:591-595.
91. Kawachi I, Kennedy B. Health and social cohesion: why care about income inequality? British Medical Journal 1997;314(5th April):1037-1040.
92. Cooper H, Arber S, Fee L, Ginn J. The influence of social support and social capital on health: a review of British data: Health Education Authority; 1999.
93. Lynch J, Due P, Muntaner C, Smith G. Social capital: is it a good investment strategy for public health? Journal of Epidemiology and Community Health 2000;54(June):404-408.
94. Muntaner C, Lynch J. Income inequality, social cohesion and class relations. International Journal of Health Services 1999;29(1):59-81.
95. Woolcock M. Social capital and economic development: toward a theoretical synthesis and policy framework. Theory and Society 1998;27:151-208.
96. Burridge R, Ormandy D, editors. Unhealthy housing: research, remedies and reform. London: E and FN Spon; 1993.
97. Ambrose P. A drop in the ocean: the health gain from the Central Stepney SRB in the context of national health inequalities: University of Brighton, Health and Social Policy Research Centre; 2000.
Page 119

References
98. Seedhouse D. Health: the foundation for achievement: John Wiley & Sons; 1986. (Secondary Citation) Cited in Ambrose P. A drop in the ocean: the health gain from the Central Stepney SRB in the context of national health inequalities: University of Brighton, Health and Social Policy Research Centre; 2000.
99. Conway J. Housing policy: The Guildredge Press; 2000.
100. Department of the Environment Transport and the Regions. Quality and choice: a decent home for all: the way forward for housing: DETR; 2000.
101. Department of Health. Saving lives: our healthier nation: Cm 4386: http://www.ohn.gov.uk/ohn/intro.htm. London: Stationery Office; 1999.
102. McGregor A, McConnachie M. Social exclusion, urban regeneration and economic reintegration. Urban Studies 1995;32:1587-1600. (Secondary Citation) Cited in Gaffron P, Hine JP, Mitchell F. The role of transport on social exclusion in urban Scotland: Scottish Executive Central Research Unit; 2001.
103. Best R. The housing dimension. In: Benzeval M, Judge K, Whitehead M, editors. Tackling health inequalities: an agenda for action: King's Fund; 1995.
104. Ambrose P, Barlow J, Bonsey A, Pullin M. The real cost of poor homes: a critical review of the literature: University of Sussex and University of Westminster for the Royal institute of Chartered Surveyors; 1996.
105. Hunt S. Damp and mouldy housing: a holistic approach. In: Burridge R, Ormandy D, editors. Unhealthy housing: research, remedies and reform: E and FN Spon; 1993.
106. Collins KJ. Cold- and heat-related illnesses in the indoor environment. In: Burridge R, Ormandy D, editors. Unhealthy housing: Research, remedies and reform: E and FN Spon; 1993.
107. Martin C, Platt S, Hunt S. Housing conditions and ill health. British Medical Journal 1987;294:1125-1127. (Secondary Citation) Cited in Ambrose P, Barlow J, Bonsey A, Pullin M. The real cost of poor homes: a critical review of the literature: University of Sussex and University of Westminster for the Royal institute of Chartered Surveyors; 1996.
108. Strachan D, Elton R. Relationship between respiratory morbidity in children and the home environment. Family Practice 1986;3:137-142. (Secondary Citation) Cited in Ambrose P, Barlow J, Bonsey A, Pullin M. The real cost of poor homes: a critical review of the literature: University of Sussex and University of Westminster for the Royal institute of Chartered Surveyors; 1996.
109. Arblaster L, Hawtin H. Health, housing and social policy: towards equality in health: Socialist Health Association; 1993.
110. Hosen H. Mould in allergy. Journal of Asthma Research 1978;15:151-156. (Secondary Citation) Cited in Ambrose P, Barlow J, Bonsey A, Pullin M. The real cost of poor homes: a critical review of the literature: University of Sussex and University of Westminster for the Royal institute of Chartered Surveyors; 1996.
111. Kingdom K. Relative humidity and airborne infections. American Review of Respiratory Disease 1960;81:504-512. (Secondary Citation) Cited in Ambrose P, Barlow J, Bonsey A, Pullin M. The real cost of poor homes: a critical review of the literature: University of Sussex and University of Westminster for the Royal institute of Chartered Surveyors; 1996.
112. Hunt SM, Martin C, Platt S. Damp housing, mould growth and health status: Part 1: report to the funding bodies. Edinburgh: RUHBC, University of Edinburgh; 1988. (Secondary Citation) Cited in Hunt SM, McKenna SP. The impact of housing quality on mental and physical health. Housing Review 1992;41(3):47-49.
113. Brown GW, Harris T. Social origins of depression: a study of psychiatric disorders in women: Tavistock; 1978. (Secondary Citation) Cited in Marsh A, Gordon D, Pantazis C, Heslop P. Home sweet home?: the impact of poor housing on health: The Policy Press; 1999.
114. Markus T. Cold, condensation and housing poverty. In: Burridge R, Ormandy D, editors. Unhealthy housing: research, remedies and reform. London: E and FN Spon; 1993.
115. Lowry S. Housing and health inequalities: review and prospects for research; 1991.
Page 120

References
116. Sneddon J. The oxides of nitrogen. In: Leslie G, Lunau F, editors. Indoor air: Cambridge University Press; 1992. (Secondary Citation) Cited in Ambrose P, Barlow J, Bonsey A, Pullin M. The real cost of poor homes: a critical review of the literature: University of Sussex and University of Westminster for the Royal institute of Chartered Surveyors; 1996.
117. Kellar M, et al. Respiratory illness in households using gas and electricity for cooking 1: survey of incidence. Environmental Research 1979;19:495-503. (Secondary Citation) Cited in Ambrose P, Barlow J, Bonsey A, Pullin M. The real cost of poor homes: a critical review of the literature: University of Sussex and University of Westminster for the Royal institute of Chartered Surveyors; 1996.
118. O'Riordan MC. Human exposure to radon in homes: recommendations for the practical application of the Board's statement. Chilton: National Radiological Protection Board; 1990. (Secondary Citation) Cited in Arblaster L, Hawtin H. Health, housing and social policy: towards equality in health: Socialist Health Association; 1993.
119. Henshaw DL, Eatough JP, Richardson RB. Radon as a causative factor in induction of myeloid leukaemia and other cancers. Lancet 1990;335:1008-1012. (Secondary Citation) Cited in Arblaster L, Hawtin H. Health, housing and social policy: towards equality in health: Socialist Health Association; 1993.
120. Hooton S. A point to prove: why housing matters: Chartered Institute of Housing; 1995. (Secondary Citation) Cited in Ambrose P, Barlow J, Bonsey A, Pullin M. The real cost of poor homes: a critical review of the literature: University of Sussex and University of Westminster for the Royal institute of Chartered Surveyors; 1996.
121. Best R. Health inequalities: the place of housing. In: Gordon D, Shaw M, Dorling D, Davey Smith G, editors. Inequalities in health: the evidence presented to the independent inquiry into inequalities in health chaired by Sir Donald Acheson. Bristol: Policy Press; 1999.
122. Ransom R. Accidents at home: the modern epidemic. In: Burridge R, Ormandy D, editors. Unhealthy housing: research, remedies and reform: E and FN Spon; 1993.
123. Matthews G. Why should public health include housing? In: Griffiths S, Hunter DJ, editors. Perspectives in public health: Radcliffe Medical Press; 1999.
124. Howard M. The effects on human health of pest infestation in houses. In: Burridge R, Ormandy D, editors. Unhealthy housing: research, remedies and reform: E and FN Spon; 1993.
125. Ineichen B. Homes and health: how housing and health interact: E and FN Spon; 1993.
126. Topf M. Sensitivity to noise, personality hardiness, and noise induced stress in critical care nurses. Environmental Behavior 1989;21:717-733. (Secondary Citation) Cited in Rice PL, editor. Stress and health. 3rd ed. Pacific Grove Publishing: Brooks/Cole Publishing; 1999.
127. Cohen S, Evans GW, Krantz DS, Stokols D. Physiological, motivational, and cognitive effects of aircraft noise on children. American Psychologist 1980;35:231-243. (Secondary Citation) Cited in Rice PL, editor. Stress and health. 3rd ed. Pacific Grove Publishing: Brooks/Cole Publishing; 1999.
128. Siegle JM, Steele CM. Environmental distractions and interpersonal judgements. British Journal of Social and Clinical Psychology 1980;19:23-32. (Secondary Citation) Cited in Rice PL, editor. Stress and health. 3rd ed. Pacific Grove Publishing: Brooks/Cole Publishing; 1999.
129. Konecni VJ, Libuser,L., Morton,H and Ebbesen,E.B. Effects of a violation of personal space on escape and helping responses. Journal of Experimental Social Psychology 1975;11:288-299. (Secondary Citation) Cited in Rice PL, editor. Stress and health. 3rd ed. Pacific Grove Publishing: Brooks/Cole Publishing; 1999.
130. Bonzaft AL, McCarthy DP. The effects of elevated train noise on reading ability. Environment and Behavior 1975;7:517 - 529. (Secondary Citation) Cited in Rice PL, editor. Stress and health. 3rd ed. Pacific Grove Publishing: Brooks/Cole Publishing; 1999.
131. Hunt SM, McKenna SP. The impact of housing quality on mental and physical health. Housing Review 1992;41(3):47-49.
132. Barker D, Osmond C. Inequalities in health in Britain: specific explanations in three Lancashire towns. British Medical Journal 1987;294(6574):749-752. (Secondary Citation) Cited in Ambrose P, Barlow
Page 121
References
J, Bonsey A, Pullin M. The real cost of poor homes: a critical review of the literature: University of Sussex and University of Westminster for the Royal institute of Chartered Surveyors; 1996.
133. Kellet J. Health and housing. Journal of Psychosomatic Research 1989;33:255-268. (Secondary Citation) Cited in Ambrose P, Barlow J, Bonsey A, Pullin M. The real cost of poor homes: a critical review of the literature: University of Sussex and University of Westminster for the Royal institute of Chartered Surveyors; 1996.
134. Davis, A. Submission to the Inquiry into Inequalities in Health. Input paper: transport and pollution. 1998.
135. Acheson, D., Barker, D. et al. Independent inquiry into inequalities in health: report. pp.1-164. 1998. London, The Stationery Office.
136. Egan, M. and Petticrew, M. New roads and human health: a systematic review. American Journal of Public Health, in press, 2003
137. Andersson, P. K., Lund, B. L. C. et al. Omfartsveje: den trafiksikkerhedsmæssige effekt. 2002. Copenhagen, Danmarks TransportForskning.
138. Amundsen, A. H. and Elvik, R. Amundsen AH, Elvik R. Effects on road safety of new urban arterial roads. [draft manuscript]. 2001. Oslo.
139. Appleyard, D. Liveable streets. Berkeley, University of California Press. 1981.
140. Rogers, R. and Power, A. Cities for a small country. London, Faber and Faber Limited. 2000.
141. Watkiss, P., Brand, C. et al. Informing traffic health impact assessment in London. pp.1-141. 2000. London, AEA Technology and NHS Executive London.
142. Roberts, I., Li, L. et al. Trends in intentional injury deaths in children and teenagers (1980-1995). Journal of Public Health Medicine, 20 (4) pp.463-466, 1998
143. Roberts, I., Ashton, T. et al. Preventing child pedestrian injury: pedestrian education or traffic calming? Australian Journal of Public Health, 18 (2) pp.209-212, 1994
144. DiGuiseppi, C., Roberts, I. et al. Influence of changing travel patterns on child death rates from injury: trend analysis. British Medical Journal, 314 pp.710, 1997
145. ITE Task Force. ITE Pedestrian and bike task force survey results summary. ITE Journal. 2001.
146. Wazana, A., Krueger, P. et al. A review of risk factors for child pedestrian injuries: are they modifiable? Injury Prevention, 3 (4) pp.295-304, 1997
147. Roberts, I. Adult accompaniment and the risk of pedestrian injury on the school-home journey. Injury Prevention, 1 (4) pp.242-244, 1995
148. Harborview Injury Prevention and Research Center. Child pedestrian injury interventions. 2002. Available at http://depts.washington.edu/hiprc/childinjury/
149. Jarvis, S., Towner, E. et al. "Accidents" in The health of our children ed. Botting, B. London, Office of Population Censuses and Surveys, HMSO. 1995.
150. McCarthy, M. "Transport and health" in Social determinants of health eds. Marmot, M. and Wilkinson, R. G. Oxford, Oxford University Press. 1999: pp.132-154.
151. Hillman, M., Adams, J. et al. One false move: a study of children's independent mobility. London, Policy Studies Institute. 1990.
152. Carlin, J. B., Stevenson, M. R. et al. Walking to school and traffic exposure in Australian children. Australian and New Zealand Journal of Public Health, 21 (3) pp.286-292, 1997
153. Christie, N., Dale, M. et al. Child safety in rural areas: a critical review of the literature and commentary. Road Safety Research Report No. 32. 2003. London, Department for Transport. Available at http://www.roads.dft.gov.uk/roadsafety/roadresearch/rural/pdf/01.pdf
Page 122

References
154. Barker, J., Farmer, S. et al. Injury accidents on rural single-carriageway roads, 1994-95 - an analysis of STATS 19 data. TRL Report 304. 1998. Crowthorne, Berkshire, Transport Research Laboratory.
155. Glaister, S., Graham, D. et al. COMPEAD statement on transport and health in London. 1999. Committee on the Medical Effects of Air Pollutants, Department of Health.
156. Contributors to the Cochrane Collaboration and the Campbell Collaboration. Evidence from systematic reviews of research relevant to implementing the "wider public health" agenda. 2000. NHS Centre for Reviews and Dissemination. available at http://www.york.ac.uk/inst/crd/wph.htm
157. COMEAP. The health effects of air pollutants. COMEAP advice. 2000. Committee on the Medical Effects of Air Pollutants. Available at http://www.doh.gov.uk/comeap/statementsreports/healtheffects.htm
158. Department of the Environment Transport and the Regions. Health effect noise assessment methods: a review and feasibility study. 1997. A review by the National Physical Laboratory and the Institute of Sound and Vibration Research for the Noise and Nuisance Policy Unit.
159. Öhrström, E. and Rylander, R. Sleep disturbance effects of traffic noise - a laboratory study on after effects. Journal of Sound and Vibration, 84 pp.87-103, 1990
160. Stansfeld, S. A., Haines, M. et al. Rapid review on noise and health for London. A review to support the development of the Mayor of London's Ambient Noise Strategy. 2001. Department of Psychiatry, Department of Geography, St Bartholomew's and the Royal London School of Medicine and Dentistry, Queen Mary, University of London.
161. Kageyama, T., Kabuto, M. et al. A population study on risk factors for insomnia among adult Japanese women: a possible effect of road traffic volume. Sleep, 20 (11) pp.963-971, 1997
162. Tarnopolsky, A. and Morton–Williams, J. Aircraft noise and prevalence of psychiatric disorders: research report. 1980. London, Social and Community Planning Research.
163. Halpern, D. Mental health and the built environment: more than bricks and mortar. London, Taylor and Francis. 1995.
164. Babisch, W. Traffic noise and cardiovascular disease: epidemiology review and synthesis. Noise and Health, 8 pp.9-32, 2000
165. Babisch, W., Ising.H. et al. Traffic noise and cardiovascular risk: the Caerphilly study, first phase. Outdoor noise levels and risk factors. Archives of Environmental Health, 43 pp.407-414, 1998
166. Babisch, W., Ising.H. et al. Traffic noise and cardiovascular risk: the Caerphilly and speedwell studies, third phase. 10 years follow up. Archives of Environmental Health, 54 pp.210-216, 1999 77. Social Exclusion Unit. Making the connections. final report on transport and social exclusion. 2003. London. available at http://www.socialexclusionunit.gov.uk
167. OECD. The wealth of nations: the role of human and social capital. 2001.
168. Coleman, J. Social capital in the creation of human capital. American Journal of Sociology, 94 pp.S95-S120, 1988
169. Wolfe, B. and Haveman, R. "Accounting for the social and non-market benefits of education" in The contribution of human and social capital to sustained economic growth and well-being: International Symposium Report ed. Helliwell, J. F. Human Resources Development Canada and OECD. 2001.
170. Kenkel, D. Health behaviour, health knowledge, and schooling. Journal of Political Economy, 99 (2) pp.287-305, 1991
171. Whitty, G., Aggleton, P. et al. "Education and health inequalities" in Inequalities in health: the evidence presented to the Independent Inquiry into Inequalities in Health, chaired by Sir Donald Acheson eds. Gordon, D., Shaw, M. et al. Bristol, The Policy Press. 1999: pp.138-147.
172. Sampson, R. J. "Family management and child development: insights from social disorganization theory" in Facts, frameworks and forecasts: advances in criminological theory ed. McCord, J. New Brunswick, NJ, Transaction Publishers. 1992: pp.63-93.
Page 123

References
173. McCulloch, A. and Joshi, H. E. Neighbourhood and family influences on the cognitive ability of children in the British National Child Development Study. Soc.Sci.Med., 53 pp.579-591, 2001
174. Morrow, V. M. Conceptualising social capital in relation to the well-being of children and young people: a critical review. Sociological Review, 47 pp.744-765, 1999
175. Paluska, S. A. and Schwenk, T. L. Physical activity and mental health - current concepts. Sports Medicine, 29 (3) pp.167-180, 2000
176. Rowland, T. W. and Freedson, P. S. Physical activity, fitness and health in children: a closer look. Pediatrics, 93 pp.669-672, 1994
177. Seymour, J., Jefferis, B. et al. Rapid review of housing and the built environment. Rapid reviews of public health for London. 2001. London School of Hygiene & Tropical Medicine for the NHS Executive, London. Available at http://www.doh.gov.uk/london/hatbe.htm
178. Lurigo, A. J. Are all victims alike? The adverse, generalized and differential impact of crime. Crime and Delinquency, 33 pp.452-467, 1987
179. Crime Concern. Review to support the development of the health strategy for London: crime and disorder. ed. Cane, R. 1999. London, A report prepared for the London Regional Office of the NHS Executive. Available at http://www.doh.gov.uk/london/hsrapid.htm
180. Michie, C. and de Rozarieux, D. The health impacts of green spaces: a rapid review to support the Mayor of London's Biodiversity Strategy. 2001. London, Ealing Hospital NHS Trust.
181. Cattell, V. Poor people, poor places, and poor health: the mediating role of social networks and social capital. Soc.Sci.Med., 52 pp.1501-1516, 2001
182. Stevenson, D. Regeneration. Presentation at the conference The State of London's Health. 2001. London, King's Fund.
183. Graetz, B. Health consequences of employment and unemployment: longitudinal evidence for young men and women. Soc.Sci.Med., 36 (6) pp.715-724, 1993
184. Shortt, S. E. D. Is unemployment pathogenic? A review of current concepts with lessons for policy planners. International Journal of Health Services, 26 (3) pp.569-589, 1996
185. Campbell, M., Sanderson, I. et al. Local responses to long term unemployment. York, YPS for the Joseph Rowntree Foundation. 1998.
186. Performance and Innovation Unit. Improving labour market achievements for ethnic minorities in British society. 2001. London, Cabinet Office. Available at http://www.cabinet-office.gov.uk/innovation
187. Crime reduction toolkits: rural crime. 2003. Available at http://www.crimereduction.gov.uk/toolkits/rc0101.htm
188. McCabe, A. and Raine, J. Framing the debate: the impact of crime on public health. 1997. Birmingham, Public Health Alliance.
189. Robinson F and J, K. The impacts of crime on health and health services: a literature review. Health, Risk and Society, 2 (3) pp.253-266, 2000
190. Pain R H. Gender, race, age and fear in the city. Urban Studies, 38 (5/6) pp.899-913, 2001
191. Farrington D. Understanding and preventing youth crime. 1996. York, Joseph Rowntree Foundation. Available at http://www.jrf.org.uk
192. Crutchfield R, Geerken M et al. Crime rates and social integration: The impact of metropolitan mobility. Criminology, 20 pp.467-478, 1982
193. Sampson R J. Neighbourhood and crime: The structural determinants of personal victimisation. Journal of Research in Crime and Delinquency, 22 pp.7-40, 1985
Page 124

References
194. Clarke R V. Situational Crime Prevention: Successful Case Studies. New York, Harrow and Heston. 1992.
195. Koskela H and R., P. Revisiting fear and place: women's fear of attack and the built environment. Geoforum, 31 pp.269-280, 2000
196. Walklate S. Victimology. London, Unwin Hyman. 1995.
197. Pease, K. "A review of street lighting evaluations: crime reduction effects" in Surveillance of public space: CCTV, street lighting and crime prevention eds. Painter, K. and Tilley, N. Monsey, NY, Criminal Justice Press. 1999: pp.47-76.
198. Phillips, C. "A review of CCTV evaluations: crime reduction effects and attitudes towards its use" in Surveillance of public space: CCTV, street lighting and crime prevention eds. Painter, K. and Tilley, N. Monsey, NY, Criminal Justice Press. 1999: pp.123-156.
199. Ditton J. Crime and the City: Public attitudes towards open-street CCTV in Glasgow. British Journal of Criminology, 40 (692-709), 2000
200. LaGrange R L, Ferraro K F et al. Perceived risk and fear of crime: Role of social and physical incivilities. Journal of Research in Crime and Delinquency, 29 (3) pp.311-334, 1992
201. Henrik Andershed, Margaret Kerr et al. Bullying in School and Violence on the Streets: Are the Same People Involved? Journal of Scandinavian Studies in Criminology and Crime Prevention, 2 (1) pp.31-49, 2001
202. Office of the Deputy Prime Minister. Planning for the communities of the future. 1998. Available at http://www.planning.odpm.gov.uk/future/
203. Office of the Deputy Prime Minister. Planning Policy Guidance (PPG) 3: housing. 2002. Available at http://www.planning.odpm.gov.uk/ppg/ppg3/index.htm
204. Office of the Deputy Prime Minister. PPG7 The countryside: environmental quality and economic and social development. 1997. Available at http://www.planning.odpm.gov.uk/ppg/ppg7/index.htm
205. Office of the Deputy Prime Minister. Planning Policy Guidance (PPG) 10: planning and waste management. 1999. Available at http://www.planning.odpm.gov.uk/ppg10/
206. Office of the Deputy Prime Minister. PPG13: Transport. 1994. Available at http://www.planning.odpm.gov.uk/ppg/ppg13/index.htm
207. Office of the Deputy Prime Minister. Planning Policy Guidance (PPG) 17: planning for open space, sport and recreation. 2002. HMSO. Available at http://www.planning.odpm.gov.uk/ppg/ppg17/index.htm
208. Office of the Deputy Prime Minister. Planning Policy Guidance (PPG) 24: planning and noise. 2002. HMSO. Available at http://www.planning.odpm.gov.uk/ppg/ppg24/
209. Department of Environment, Food and Rural Affairs. Our Countryside: The Future – A Fair Deal for Rural England. HMS0. 2003. Available at http://www.defra.gov.uk/rural/ruralwp/whitepaper/chapter1.htm
210. Department of Environment. Circular 5/94 Planning Out Crime. HMSO. 1994. Available at http://www.iowcrime-disorder.org/design1.html#planningout
211. Office of the Deputy Prime Minister. Local Government Act. 2000. London, HMSO. 27-1-2003. Available at http://www.local-regions.odpm.gov.uk/lgbill99
212. Office of the Deputy Prime Minister. Local Government Act factsheet: community well being. 2002. HMSO. Available at http://www.local-regions.odpm.gov.uk/lgbill99/factsheets/wbeing.htm
213. Suffolk County Council. Suffolk Structure Plan. 2001. Available at http://www.suffolkcc.gov.uk/e-and-t/structure_changes/adopted_structure_plan/
214. Babergh District Council. Babergh Local Plan (2003) Second Deposit Draft. Alteration No. 2. Available at http://www.babergh-south-suffolk.gov.uk/planplcy/blp2dep/text.htm
Page 125

References
215. Central Suffolk Primary Care Trust. Local Health Delivery Plan. July 2003. Available at http://www.centralsuffolk-pct.nhs.uk/scripts/default.asp?site_id=8&id=5182
216. Suffolk County Council. Suffolk Health Strategy. 2001. Available at http://www.suffolkcc.gov.uk/policy/beacon/01-2nd1.pdf
217. Wanless D. HM Treasury. Securing Our Future Health: Taking the Long Term View. 2002. Available at http://www.hm-treasury.gov.uk/consultations_and_legislation/wanless/consult_wanless_final.cfm
218. Wanless D. HM Treasury. Securing Good Health for the Whole Population. 2004. Available at http://www.hm-treasury.gov.uk/consultations_and_legislation/wanless/consult_wanless04_final.cfm
219. Social Exclusion Unit. A new commitment to neighbourhood renewal: national strategy action plan. 2001. Crown Copyright.
220. Department of Health. The NHS Plan: a plan for investment – a plan for reform. Cm 4818-I. 2000. Available at http://www.doh.gov.uk/nhsplan/nhsplan.htm
221. Department of Health. Shifting the balance of power: the next steps. 2001. London, Crown Copyright. Available at www.doh.gov.uk/shiftingthebalance
222. Department of Health. Tackling health inequalities: cross-cutting review. 2002. London. Available at http://www.doh.gov.uk/healthinequalities/ccsrfinal.pdf
223. Shotley Parish Council. 1996. Shotley: What We Think. Community Consultation.
224. GSCC. 2001. The Future Development of the former HMS Ganges Site Shotley. Community Consultation.
Page 126