HIMSS CCDA Story BSWH_HSP Roundtable_Jan 2016
32
C-CDA Direct Messaging: Are We There Yet? Baylor Scott and White Health
-
Upload
oscar-glorioso -
Category
Documents
-
view
186 -
download
0
Transcript of HIMSS CCDA Story BSWH_HSP Roundtable_Jan 2016

C-CDA Direct Messaging: Are We There Yet?
Baylor Scott and White Health

PresentersCherie Price, RN, CTT+, IQCIBaylor Scott & White Healthcare at GrapevineRN Care Manager and Care Management Informatics
Cindy Sunderman Neese, MSN, RN-BC, CPHIMSBaylor Scott & White HealthcareNurse Informaticist, Manager — eQuality MeasuresStrategy and Operations, STEEEP Analytics
Oscar Glorioso, RN, MSNBaylor Scott & White Healthcare Clinical Application Specialist IIAllscripts EHR — Clinical Documentation Team
Abeezar Shipchandler, MD, FACPInternal Medicine/HospitalistBaylor Regional Medical Center at PlanoClinical Assistant Professor Texas A&M HSC COM, Dept. of Internal MedicinePhysician Clinical Informatics Leader, Baylor Scott & White Health

Special Thanks
Joseph H. Schneider, MD, MBA, FAAP
David Nickel, PMO
Linda Hodges, PMO

Introduction



Learning Objectives
• Identify pre-implementation considerations and potential challenges to implementing inbound/outbound direct messaging of C-CDA visit summaries
• Discover methods of C-CDA data exchange for outbound direct messaging of C-CDA documents
• Learn about the benefits of implementing inbound/outbound direct messaging of C-CDA documents

The Road Ahead
Baylor Scott & White decided to implement C-CDA not only to avoid steep penalties from Medicare, but also as part of our goal to achieve strong transitions from the inpatient setting to the next level of care.

The Journey
• Resource planning
• Development
– Technical configuration
• C-CDA document data mapping and configuration
• HISP configuration
• MU2 dashboard development
– Workflow development
• Implementation
• Monitoring and Meaningful Use attestation

Resource Planning

C-CDA Document Configuration
• Patient Information• Reason for Referral• Reason for Visit• Functional Status• Treatment Plans• Instructions• Discharge Diet• Hospital Discharge
Instructions

C-CDA Document Configuration
• Vital Signs• Medications• Problems• Hospital Admission
Diagnosis• Hospital Discharge
Diagnosis• Allergies• Results• Procedures• Immunization• Social History

C-CDA Document Configuration
• Encounters• Health Care Provider• Patient Contacts

Data MappingCXD_Functional_Status
Extremity Movement
298331001^Normal motor response to command (finding)^SNOMED CT
MAE on command, no obvious deficits noted
225606002^Abnormal movement (finding)^SNOMED CT
MAE on command, no obvious deficits noted except
225606002^Abnormal movement (finding)^SNOMED CT RUE
225606002^Abnormal movement (finding)^SNOMED CT LUE
225606002^Abnormal movement (finding)^SNOMED CT Bilateral UE
225606002^Abnormal movement (finding)^SNOMED CT RLE
225606002^Abnormal movement (finding)^SNOMED CT LLE
3915700^Flaccid paralysis (finding)^SNOMED CT
Flaccid
26544005^Muscle weakness (finding)^SNOMED CT Weakness
163605002^On examination - quadriplegia (disorder)^SNOMED CT Quadriplegic
163604003^On examination - paraplegia (disorder)^SNOMED CT Paraplegic
163660009^On examination - flexion contracture
(disorder)^SNOMED CTContractures
6077001^Foot-drop (finding)^SNOMED CT Foot drop
298222004^Active range of joint movement reduced
(finding)^SNOMED CT Limited ROM
• Allergies = UNI code• Problems= CPT, ICD 10 and
SNOMED CT• Functional status= SNOMED
CT• Social History = SNOMED
CT

HISP Configuration
• Primarily done by vendor engineer– URL– Direct address
• Smoke testing in non-production environment

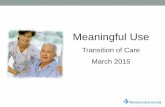
Workflow DevelopmentOutbound
Care Coordination use report to
identify patient
Disclosure Note saved on account and
triggers C-CDA Visit Summary
transmission via Direct Messaging
Vendor Cloud
HISP Receiving EHR
Average 80 outbound transmissions/day

Workflow DevelopmentBSWH
partners and other Referring Practices sends C-
CDA
Sender’sHISP
Receiving HISP
Vendor Cloud
InboxCorporate
HIM matches C-CDA to patient
(Name, DOB, Address)
C-CDA saved to patient’s
chart
Clinicians views C-
CDA under the
documents tab or viewer
Inbound
Average 100 matches/day

Implementation
3-4-14 C-CDA Discharge Summary Document (Inpatient) Go Live
4-29-14 C-CDA Summary of Care Document (Outpatient) Go Live
9-16-14 C-CDA-Visit Summary Document Go Live
1-23-15 Inbound Messaging Go Live
6-2-15Sending C-CDA Visit Summary via
Direct Messaging Go Live (Outbound)

Monitoring and Meaningful Use Attestation

Monitoring and Meaningful Use Attestation

Monitoring and Meaningful Use Attestation

Monitoring and Meaningful Use Attestation

• Galvanized focus workgroup– Identified providers/groups who were high admitters
at each facility– Involved Clinical Informatics at each facility– Pursued addition of post-acute care facilities via
vendor portal– Daily monitoring, weekly update meetings
Monitoring and Meaningful Use Attestation

Monitoring and Meaningful Use Attestation

The Bumps Along The Way• People
– HIPAA Privacy office and/or Health Information Management department was engaged late in the planning
• New requirements were added to align with Legal/ Compliance
• Direct Messaging was added on existing HIM workflow
– Leadership changes slowed decision making and escalation of issues
• Logistics– Several hospitals would not meet the MU threshold with only
sending C-CDAs to the one physician group
– Other primary physician groups maintains a one to one Direct Messaging address versus practice Direct Address

The Bumps (cont.)

The Bumps (cont.)
Technical: Outbound
Occasional C-CDA transmission failures
• 10MB limit (includes document data as well as message information)
• Cloud and/or network failures
• Misspelled Direct Addresses
Functional Status 80% captured
• Discrete vs free text• More Nursing and Allied Health
data than Physician dataMedication Dictionary • Brand vs Generic1
Problem Management • Discharge Dx• Historic vs Current2

The Bumps (cont.)
Technical: Inbound
Matching C-CDA documentation to patients
• limited demographic
Extra document being sent besides C-CDADifferent C-CDA naming convention for every organization

The Destination
• No direct benefit for inpatient physician, the C-CDA provides outpatient providers a snapshot of key information and assume care without combing through hundreds of pages of records
• Next providers of care were able to quickly identify patients in need of additional intervention to prevent readmissions and other issues
– Decrease in readmission rates since July 2015

Lessons Learned
• Conduct an analysis early on in the project to estimate reach for proposed solutions
• Regular meetings, clear communication and detailed documentation are essential to success
• Teamwork is critical
• Development of a report to quickly identify targeted patients is critical to time management
• HIM needs to be at the table• Automation of the process is ideal, but still requires additional
technical work to avoid release of PHI to inappropriate resources

Looking Forward
• Logistics– Facility/hospital ownership of
outbound Direct Messaging workflow (decentralization)
– Leveraging Direct Messaging to build partnership across the country
– Integrate Direct Messaging with other IT initiative
• NSQIP• Breeze
– Measure Direct Messaging patient care outcome
• Workflow– PAMI data reconciliation
(Meaningful Use Stage 3)– Problem list management
• Meaningful Use– 50% threshold for Stage 3
(2018)• Vendor Enhancement
– Show Brand and Generic Drugs

Contact Information
Cherie Price, RN, CTT+, [email protected]
Cindy Sunderman Neese, MSN, RN-BC, [email protected]
Oscar Glorioso, RN, [email protected]
Abeezar Shipchandler, MD, [email protected]