Gregory Burns, MMS, PA-C Past President-Florida Academy of Physician Assistants (FAPA) Assistant...
68
Update in Hypertension Management Gregory Burns, MMS, PA-C Past President-Florida Academy of Physician Assistants (FAPA) Assistant Professor of Barry University PA Program- St. Petersburg
-
Upload
madyson-casson -
Category
Documents
-
view
223 -
download
1
Transcript of Gregory Burns, MMS, PA-C Past President-Florida Academy of Physician Assistants (FAPA) Assistant...

Update in Hypertension Management
Gregory Burns, MMS, PA-CPast President-Florida Academy of Physician Assistants (FAPA)
Assistant Professor of Barry University PA Program-St. Petersburg

Define the different types of HTN Compare old JNC Guidelines to new JNC-8
Guidelines Know the screening of HTN Know the correct ways of BP measurements Know how to evaluate a patient with HTN Know the Goals of Therapy Examine different Trials of HTN Examine different classes of Therapy Examine the 9 Recommendations of JNC-8
Objectives

The treatment of hypertension is the most common reason for office visits of non-pregnant adults to physicians in the United States and for use of prescription drugs.
The National Health and Nutrition Examination Survey (NHANES) conducted from 2005 through 2008 estimated that approximately 29 to 31 percent of adults in the United States have hypertension.
This means up to 65 Million US Adult Hypertensives!
Facts


1977: JNC-1 First Report of JNCno specific recommendation on treating SBP;
Identified DHTN at 105; consider treatment 90-105
2003: JNC-7 =Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure
http://www.nhlbi.nih.gov/guidelines/hypertension/jncintro.htm
December 2013: JNC-8= Eight Report is finally out now!
HTN Guidelines


Blood Pressure Classification
Normal <120 and <80
Prehypertension 120–139 or 80–89
Stage 1 Hypertension 140–159 or 90–99
Stage 2 Hypertension >160 or >100
BP Classification SBP mmHg DBP mmHg

The pathogenesis of primary, or essential, hypertension is poorly understood.
Factors that may implicate include:1. Increased sympathetic neural activity, with
enhanced beta-adrenergic responsiveness2. Increased angiotensin II activity and
mineralocorticoid excess3. Genetic factors account for approximately
30 percent of the variation in blood pressure in various populations
ESSENTIAL (PRIMARY) HYPERTENSION

Secondary or Identifiable Causes of Hypertension
Pheochromocytoma Coarctation of the aorta Thyroid or parathyroid
disease *Oral contraceptives
Sleep apnea Drug-induced or related
causes Chronic kidney disease Primary aldosteronism Renovascular disease Chronic steroid therapy
and Cushing’s syndrome

Isolated systolic hypertension: blood pressure of ≥140/<90 mmHg
Isolated diastolic hypertension: blood pressure <140/≥90 mmHg
Malignant hypertension: severe hypertension with retinal hemorrhages, exudates, or papilledema, with or without hypertensive encephalopathy
Hypertensive urgency: severe hypertension (diastolic pressure >120 mmHg) in asymptomatic patients
Other Types

Resistant hypertension is defined in the 2008 American Heart Association (AHA) scientific statement as blood pressure that remains above goal in spite of concurrent use of three antihypertensive agents of different classes
Thus, patients whose blood pressure is controlled with four or more medications should be considered to have resistant hypertension
Resistant Hypertension

All patients with resistant hypertension should be evaluated for the possible presence of primary aldosteronism, renal artery stenosis, chronic kidney disease, and obstructive sleep apnea (Most Common Cause).
Less common identifiable causes of resistant hypertension include pheochromocytoma, Cushing's syndrome, and aortic coarctation.
Resistant Hypertension

Resistant Hypertension that cannot be controlled (up to 10% of this population) is called Refractory Hypertension.
Neurologic mechanisms (eg, sympathetic overactivity) may be the culprit of Refractory Hypertension.
Potentially reversible factors that contribute to resistant hypertension include suboptimal therapy, lifestyle and diet, medications and herbal preparations that can raise the blood pressure, and secondary causes of hypertension
Resistant Hypertension

The 2007 United States Preventive Services Task Force (USPSTF) guidelines on screening for high blood pressure recommend screening every two years for persons with systolic and diastolic pressures below 120 mmHg and 80 mmHg, respectively (normal BP in JNC 7), and yearly for persons with a systolic pressure of 120 to 139 mmHg or a diastolic pressure of 80 to 89 mmHg (prehypertension in JNC 7)
Same for JNC 8!
Screening for HTN

BP Measurement Techniques
Method Brief Description
In-office Two readings, 5 minutes apart, sitting in chair. Confirm elevated reading in contralateral arm.
Ambulatory BP monitoring Indicated for evaluation of “white-coat” HTN. Absence of 10–20% BP decrease during sleep may indicate increased CVD risk.
Self-measurement Provides information on response to therapy. May help improve adherence to therapy and evaluate “white-coat” HTN.

Office BP Measurement
Use auscultatory method with a properly calibrated and validated instrument.
Patient should be seated quietly for 5 minutes in a chair (not on an exam table), feet on the floor, and arm supported at heart level.
Appropriate-sized cuff should be used to ensure accuracy.
At least two measurements should be made.
Clinicians should provide to patients, verbally and in writing, specific BP numbers and BP goals.

Self-Measurement of BP
Provides information on:1. Response to antihypertensive therapy2. Improving adherence with therapy 3. Evaluating white-coat HTN
Home measurement of >135/85 mmHg is generally considered to be hypertensive.
Home measurement devices should be checked regularly.

Suspected episodic hypertension (eg, pheochromocytoma)
Hypertension resistant to increasing medication
Hypotensive symptoms while taking antihypertensive medications
Autonomic dysfunction
Ambulatory Measurement

The Dublin Outcome Study in 2005Results: Ambulatory measurement of blood
pressure is superior to clinic measurement in predicting cardiovascular mortality, and nighttime blood pressure is the most potent predictor of outcome
Ambulatory Measurement

Patient Evaluation
Evaluation of patients with documented HTN has three objectives:
1. Assess lifestyle and identify other CV risk factors or concomitant disorders that affects prognosis and guides treatment.
2. Reveal identifiable causes of high BP.
3. Assess the presence or absence of target organ damage and CVD.

CVD Risk
The BP relationship to risk of CVD is continuous, consistent, and independent of other risk factors.
Each increment of 20/10 mmHg doubles the risk of CVD across the entire BP range starting from 115/75 mmHg.
Prehypertension signals the need for increased education to reduce BP in order to prevent hypertension.

CVD Risk Factors
Hypertension* Cigarette smoking Obesity* (BMI >30 kg/m2) Physical inactivity Dyslipidemia* Diabetes mellitus* Microalbuminuria or estimated GFR <60 ml/min Age (older than 55 for men, 65 for women) Family history of premature CVD
(men under age 55 or women under age 65)
*Components of the metabolic syndrome.

Target Organ Damage
Heart• Left ventricular hypertrophy• Angina or prior myocardial infarction• Prior coronary revascularization• Heart failure
Brain• Stroke or transient ischemic attack
Chronic kidney disease
Peripheral arterial disease Retinopathy Reduce CVD and renal morbidity and mortality.

Benefits of Lowering BP
In stage 1 HTN and additional CVD risk factors, achieving a sustained 12 mmHg reduction in SBP over 10 years will
prevent 1 death for every 11 patients treated.

Lifestyle Modification
Modification Approximate SBP reduction(range)
Weight reduction 5–20 mmHg/10 kg weight loss
Adopt DASH eating plan 8–14 mmHg
Dietary sodium reduction 2–8 mmHg
Physical activity 4–9 mmHg
Moderation of alcohol consumption
2–4 mmHg
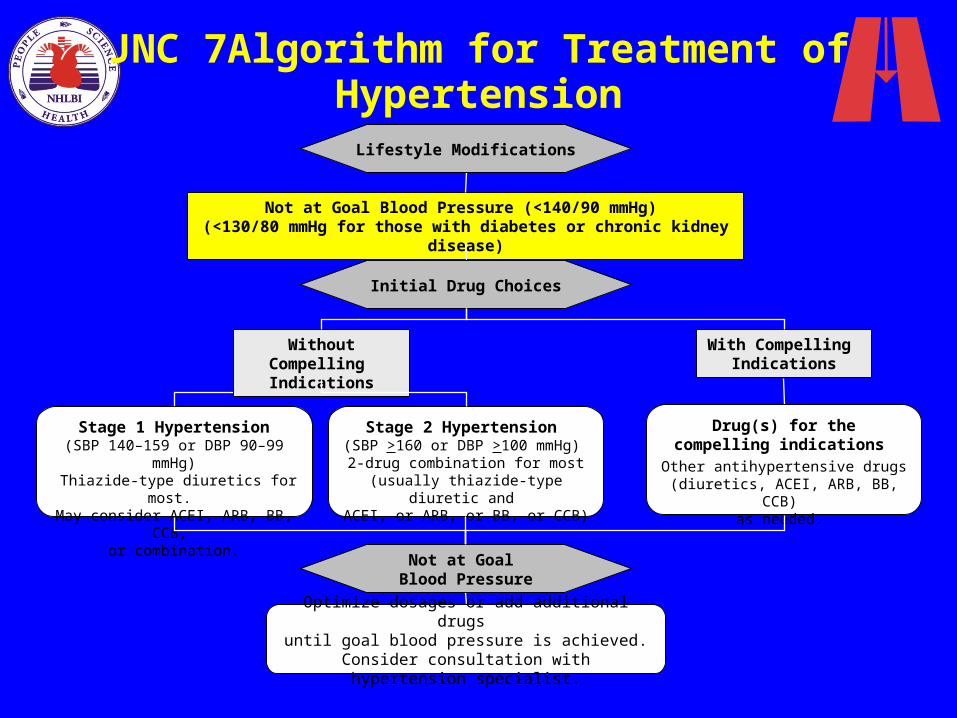
JNC 7Algorithm for Treatment of Hypertension
Not at Goal Blood Pressure (<140/90 mmHg) (<130/80 mmHg for those with diabetes or chronic kidney disease)
Initial Drug Choices
Drug(s) for the compelling indications
Other antihypertensive drugs (diuretics, ACEI, ARB, BB, CCB)
as needed.
With Compelling Indications
Lifestyle Modifications
Stage 2 Hypertension (SBP >160 or DBP >100 mmHg)
2-drug combination for most (usually thiazide-type diuretic and
ACEI, or ARB, or BB, or CCB)
Stage 1 Hypertension(SBP 140–159 or DBP 90–99 mmHg)
Thiazide-type diuretics for most. May consider ACEI, ARB, BB, CCB,
or combination.
Without Compelling Indications
Not at Goal Blood Pressure
Optimize dosages or add additional drugs until goal blood pressure is achieved.
Consider consultation with hypertension specialist.

Followup and Monitoring
Patients should return for followup and adjustment of medications until the BP goal is reached.
More frequent visits for stage 2 HTN or with complicating comorbid conditions.
Serum potassium and creatinine monitored 1–2 times per year.

Followup and Monitoring(continued)
After BP at goal and stable, followup visits at 3- to 6-month intervals.
Comorbidities, such as heart failure, associated diseases, such as diabetes, and the need for laboratory tests influence the frequency of visits.

The Antihypertensive and Lipid Lowering Treatment to Prevent Heart Attack Trial
Trial from 1994 thru 2002 involving over 42,000 patients.
Results: The principal finding of ALLHAT is that chlorthalidone, amlodipine, and lisinopril provided similar protection from coronary heart disease death and nonfatal myocardial infarction among patients with hypertension and risk factors for cardiovascular disease.
ALLHAT Trial


Chlorthalidone at the same dose is approximately 1.5 to 2.0 times as potent as HCTZ. Thus, 12.5 mg/day of chlorthalidone is equivalent to 19 to 25 mg/day of HCTZ.
Longer duration of action of chlorthalidone (24 to 72 hours versus 6 to 12 hours with HCTZ)
Chlorthalidone may be a better choice for nighttime coverage than HCTZ. Watch out for Hypokalemia. No difference-HCTZ.
Chlorthalidone versus hydrochlorothiazide (HCTZ)

Avoiding Cardiovascular Events in Combination Therapy in Patients Living with Systolic Hypertension Trial
In the ACCOMPLISH trial, amlodipine plus benazepril was associated with a 20 percent lower rate of cardiovascular events compared to hydrochlorothiazide plus benazepril, despite slightly higher 24-hour blood pressures in the amlodipine arm.
ACCOMPLISH Trial-Combination Trial

Hypertension in OlderPersons
More than two-thirds of people over 65 have HTN.
This population has the lowest rates of BP control.
Treatment, including those who with isolated systolic HTN, should follow same principles outlined for general care of HTN.
Lower initial drug doses may be indicated to avoid symptoms; standard doses and multiple drugs will be needed to reach BP targets.

Postural Hypotension
Decrease in standing SBP >10 mmHg, when associated with dizziness/fainting, more frequent in older SBP patients with diabetes, taking diuretics, venodilators, and some psychotropic drugs.
BP in these individuals should be monitored in the upright position.
Avoid volume depletion and excessively rapid dose titration of drugs.

Hypertension in Women
Oral contraceptives may increase BP, and BP should be checked regularly. In contrast, HRT does not raise BP.
Development of HTN—consider other forms of contraception.
Pregnant women with HTN should be followed carefully. Methyldopa, BBs, and vasodilators, preferred for the safety of the fetus. ACEI and ARBs contraindicated in pregnancy.


Hypertensive Urgencies and Emergencies
Patients with marked BP elevations and acute target organ dysfunction (TOD) (e.g., encephalopathy, myocardial infarction, unstable angina, pulmonary edema, eclampsia, stroke, head trauma, life-threatening arterial bleeding, or aortic dissection) require hospitalization and parenteral drug therapy.
Patients with markedly elevated BP but without acute TOD usually do not require hospitalization, but should receive immediate combination oral antihypertensive therapy.

Additional Considerations in Antihypertensive Drug Choices
Potential favorable effects
Thiazide-type diuretics useful in slowing demineralization in osteoporosis.
BBs useful in the treatment of atrial tachyarrhythmias/fibrillation, migraine, thyrotoxicosis (short-term), essential tremor, or perioperative HTN.
CCBs useful in Raynaud’s syndrome and certain arrhythmias.
Alpha-blockers useful in prostatism such as BPH.

Additional Considerations in Antihypertensive Drug Choices
Potential unfavorable effects
Thiazide diuretics should be used cautiously in gout or a history of significant hyponatremia.
BBs should be generally avoided in patients with asthma, reactive airways disease, or second- or third-degree heart block.
ACEIs and ARBs are contraindicated in pregnant women or those likely to become pregnant.
ACEIs should not be used in individuals with a history of angioedema.
Aldosterone antagonists and potassium-sparing diuretics can cause hyperkalemia.


Brand name is Tekturna Direct Renin Inhibitor Became available March 2007 Black box warning-fetus/pregnancy AVOID Trial: this med combined with
losartan showed 20% greater reduction in proteinuria than losartan alone but no real clinical effect.
ALTITUDE Trial: Patients with DM2 and kidney disease were randomly assigned to this med or placebo. Trial stopped early due to futility or increase in non-stroke, hypotension and hyperkalemia.
Aliskiren

Clonidine and Methyldopa: Alpha2-Adrenergic Agonists
--Stimulates the Alpha2 receptors in the brain decreasing cardiac output and peripheral vascular resistance.
Hydralazine and Nitroprusside: Vasodilators
Other Meds


Date of download: 2/9/2014Copyright © 2014 American Medical Association.
All rights reserved.
From: 2014 Evidence-Based Guideline for the Management of High Blood Pressure in Adults: Report From the Panel Members Appointed to the Eighth Joint National Committee (JNC 8)
JAMA. 2014;311(5):507-520. doi:10.1001/jama.2013.284427
Comparison of Current Recommendations With JNC 7 Guidelines
Figure Legend:

Date of download: 2/9/2014Copyright © 2014 American Medical Association.
All rights reserved.
From: 2014 Evidence-Based Guideline for the Management of High Blood Pressure in Adults: Report From the Panel Members Appointed to the Eighth Joint National Committee (JNC 8)
JAMA. 2014;311(5):507-520. doi:10.1001/jama.2013.284427
2014 Hypertension Guideline Management AlgorithmSBP indicates systolic blood pressure; DBP, diastolic blood pressure; ACEI, angiotensin-converting enzyme; ARB, angiotensin receptor blocker; and CCB, calcium channel blocker.aACEIs and ARBs should not be used in combination.bIf blood pressure fails to be maintained at goal, reenter the algorithm where appropriate based on the current individual therapeutic plan.
Figure Legend:

There 9 Recommendations proposed from JNC 8!
Nine Recommendations from JNC 8

The main objective of hypertension treatment is to attain and maintain goal BP.
If goal BP is not reached within a month of treatment, increase the dose of the initial drug or add a second drug from one of the classes in recommendation 6 (thiazide-type diuretic, CCB, ACEI, or ARB).
The clinician should continue to assess BP and adjust the treatment regimen until goal BP is reached.
#1 Recommendation from JNC 8

If goal BP cannot be reached with 2 drugs, add and titrate a third drug from the list provided.
Do not use an ACEI and an ARB together in the same patient.
If goal BP cannot be reached using only the drugs in recommendation 7 because of a contraindication or the need to use more than 3 drugs to reach goal BP, antihypertensive drugs from other classes can be used. Referral to a hypertension specialist may be indicated for patients in whom goal BP cannot be attained using the above strategy or for the management of complicated patients for whom additional clinical consultation is needed.
#1 Recommendation from JNC 8

In the general population aged ≥60 years, initiate pharmacologic treatment to lower blood pressure (BP) at systolic blood pressure (SBP) ≥150 mm Hg or diastolic blood pressure (DBP) ≥90 mm Hg and treat to a goal SBP <150 mm Hg and goal DBP <90 mm Hg.
(Strong Recommendation – Grade A)
#2 Recommendation from JNC 8

In the general population <60 years, initiate pharmacologic treatment to lower BP at DBP ≥90 mm Hg and treat to a goal DBP <90 mm Hg.
(For ages 30-59 years, Strong Recommendation – Grade A; For ages 18-29 years, Expert Opinion – Grade E)
#3 Recommendation from JNC 8

In the general population <60 years, initiate pharmacologic treatment to lower BP at SBP ≥140 mm Hg and treat to a goal SBP <140 mm Hg.
(Expert Opinion – Grade E)
#4 Recommendation from JNC 8

The change to a more lenient systolic blood pressure goal may be confusing to many patients who are accustomed to the lower goals of JNC 7, including the <140/90 mm Hg goal for most patients and <130/80 mm Hg goal for patients with hypertension and major comorbidities.
Why Recommendations #2, 3, and 4?

The guidelines were informed by results of 5 key trials: the Hypertension Detection and Follow-up Program (HDFP), the Hypertension-Stroke Cooperative, the Medical Research Council (MRC) trial, the Australian National Blood Pressure (ANBP) trial, and the Veterans’ Administration (VA) Cooperative.
In these trials, patients between the ages of 30 and 69 years received medication to lower DBP to a level <90 mm Hg. Results showed a reduction in cerebrovascular events, heart failure, and overall mortality in patients treated to the DBP target level.
JNC 8 Changes due to 5 Key Trials

In the population aged ≥18 years with chronic kidney disease (CKD), initiate pharmacologic treatment to lower BP at SBP ≥140 mm Hg or DBP ≥90 mm Hg and treat to goal SBP <140 mm Hg and goal DBP <90 mm Hg.
(Expert Opinion – Grade E)
#5 Recommendation from JNC 8

In the population aged ≥18 years with diabetes, initiate pharmacologic treatment to lower BP at SBP ≥140 mm Hg or DBP ≥90 mm Hg and treat to a goal SBP <140 mm Hg and goal DBP <90 mm Hg.
(Expert Opinion – Grade E)
#6 Recommendation from JNC 8

In the general nonblack population, including those with diabetes, initial antihypertensive treatment should include a thiazide-type diuretic, calcium channel blocker (CCB), angiotensin-converting enzyme inhibitor (ACEI), or angiotensin receptor blocker (ARB).
(Moderate Recommendation – Grade B)
#7 Recommendation from JNC 8

In the general black population, including those with diabetes, initial antihypertensive treatment should include a thiazide-type diuretic or CCB.
(For general black population: Moderate Recommendation – Grade B; for black patients with diabetes: Weak Recommendation – Grade C)
#8 Recommendation from JNC 8

In ALLHAT Study, mentioned before, a thiazide-type diuretic was shown to be more effective in improving cerebrovascular, heart failure, and combined cardiovascular outcomes compared to an ACEI in the black patient subgroup, which included large numbers of diabetic and nondiabetic participants
ALLHAT Study Again! (added)

In the population aged ≥18 years with CKD, initial (or add-on) antihypertensive treatment should include an ACEI or ARB to improve kidney outcomes. This applies to all CKD patients with hypertension regardless of race or diabetes status.
(Moderate Recommendation – Grade B)
#9 Recommendation from JNC 8

First-line and later-line treatments should now be limited to 4 classes of medications: thiazide-type diuretics, calcium channel blockers (CCBs), ACE inhibitors, and ARBs.
Second- and third-line alternatives included
higher doses or combinations of ACE inhibitors, ARBs, thiazide-type diuretics, and CCBs.
Other JNC 8 Changes

Date of download: 2/9/2014Copyright © 2014 American Medical Association.
All rights reserved.
From: 2014 Evidence-Based Guideline for the Management of High Blood Pressure in Adults: Report From the Panel Members Appointed to the Eighth Joint National Committee (JNC 8)
JAMA. 2014;311(5):507-520. doi:10.1001/jama.2013.284427
Evidence-Based Dosing for Antihypertensive Drugs
Figure Legend:

Several medications are now designated as later-line alternatives, including the following: beta-blockers, alpha-blockers, alpha1/beta-blockers (eg, carvedilol), vasodilating beta-blockers (eg, nebivolol), central alpha2/-adrenergic agonists (eg, clonidine), direct vasodilators (eg, hydralazine), loop diuretics (eg, furosemide), aldosterone antagoinsts (eg, spironolactone), and peripherally acting adrenergic antagonists (eg, reserpine).•
Other JNC 8 Changes

CCBs and thiazide-type diuretics should be used instead of ACE inhibitors and ARBs in patients over the age of 75 years with impaired kidney function due to the risk of hyperkalemia, increased creatinine, and further renal impairment.
Other JNC 8 Changes

Date of download: 2/9/2014Copyright © 2014 American Medical Association.
All rights reserved.
From: 2014 Evidence-Based Guideline for the Management of High Blood Pressure in Adults: Report From the Panel Members Appointed to the Eighth Joint National Committee (JNC 8)
JAMA. 2014;311(5):507-520. doi:10.1001/jama.2013.284427
Guideline Comparisons of Goal BP and Initial Drug Therapy for Adults With Hypertension
Figure Legend:

Date of download: 2/9/2014Copyright © 2014 American Medical Association.
All rights reserved.
From: 2014 Evidence-Based Guideline for the Management of High Blood Pressure in Adults: Report From the Panel Members Appointed to the Eighth Joint National Committee (JNC 8)
JAMA. 2014;311(5):507-520. doi:10.1001/jama.2013.284427
Strategies to Dose Antihypertensive Drugsa
Figure Legend:

JNC 7 is posted on NHLBI website. Most of these slides are from their program,
with starred ones from: Kaplan NM, Domino FJ. 2012 UptoDate Topic
3852 Version 18.0 J Am Coll Cardiol, 2011; 57:2037-2114,
doi:10.1016/j.jacc.2011.01.008 (Published online 25 April 2011).
http://guidance.nice.org.uk/CG127/NICEGuidance/doc
http://jama.jamanetwork.com/article.aspx?articleid=1791497
References

http://www.nhlbi.nih.gov/guidelines/cvd_adult/background.htm
http://www.nejm.org/doi/full/10.1056/NEJMoa0806182
Up-to-date.com Medscape.com
References
Thank you for your attention!
Questions???