
Global Forum Presentation_Programme Mwana_Zambia
19
Adoption and Scale-up of an mHealth Initiative to enhance Early Infant Diagnosis (EID) of HIV in Zambia Presentation by: Kaluba K. Mataka mHealth Project Manager, Zambia Center for Applied Health Research and Development (ZCAHRD) December 10-11, 2014
-
Upload
kaluba-mataka -
Category
Documents
-
view
25 -
download
0
Transcript of Global Forum Presentation_Programme Mwana_Zambia
Adoption and Scale-up of an mHealth Initiative to enhance Early Infant
Diagnosis (EID) of HIV in Zambia Presentation by:
Kaluba K. Mataka
mHealth Project Manager,
Zambia Center for Applied Health Research and Development (ZCAHRD)
December 10-11, 2014
Background • The Human Immunodeficiency Virus (HIV) prevalence in
Zambia estimated at 14.3%
• 21% of HIV infections result from Mother-to-child
transmission (MTCT)
• Antiretroviral (ART) therapies are used to prevent MTCT
• However, EID is critical to support early initiation of ART
in infants when prevention of MTCT fails
• Dried blood spot (DBS) samples from infants are sent to a small number of regional
laboratories to be tested for HIV with polymerase chain reaction (PCR)
• Timely sample transportation and result delivery constitute a big challenges to
developing an effective EID service in low resource settings
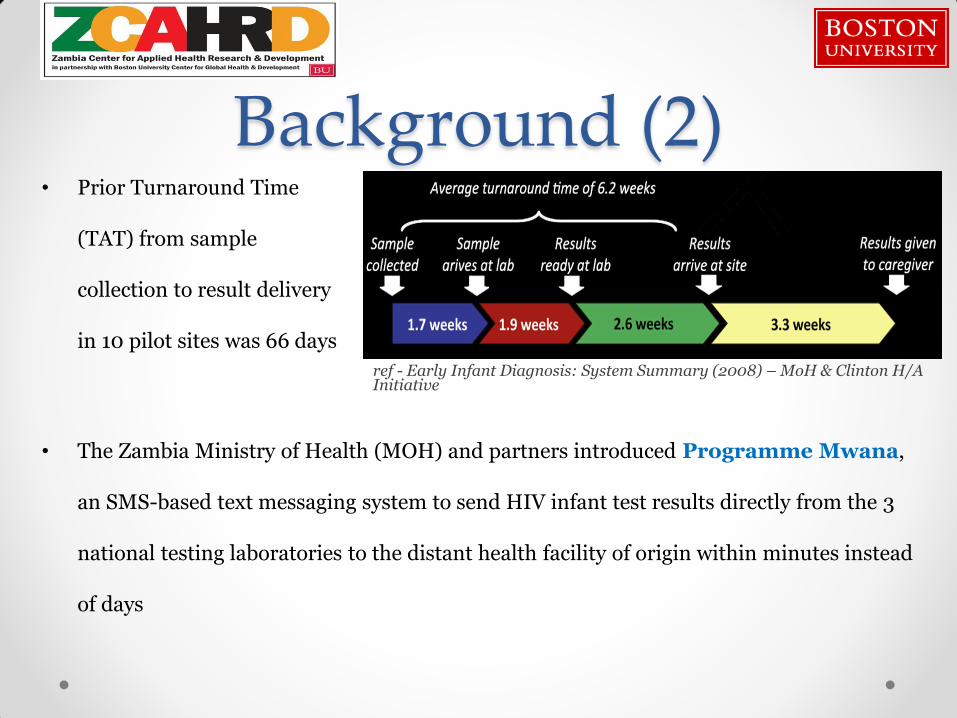
Background (2)
• The Zambia Ministry of Health (MOH) and partners introduced Programme Mwana,
an SMS-based text messaging system to send HIV infant test results directly from the 3
national testing laboratories to the distant health facility of origin within minutes instead
of days
• Prior Turnaround Time
(TAT) from sample
collection to result delivery
in 10 pilot sites was 66 days
ref - Early Infant Diagnosis: System Summary (2008) – MoH & Clinton H/A Initiative

• In 2008 CHAI, ZCAHRD and UNICEF began exploring measures to
reduce lengthy HIV testing turnaround times:
Meetings with MOH and identification of groups/persons at the
ministry to spearhead this process
Identify stakeholders in EID and implementers with expertise
• CHAI (Clinton Health Access Initiative)
• ZPCT II (Zambia Prevention Care and Treatment Partnership)
• ZCAHRD (Zambia Center for Applied Health Research and Development)
• UNICEF (United Nations Children’s fund)
• MOH (Zambia Ministry of Health)
Site and Facility selection for pilot phase based on partners
identified
Partners Identification

Partners: Aligned Interest
MOH
• Focus on EID program • Central control and support for mHealth intervention • Local ownership and direction
CHAI
• Conducted EID study in 2008
• Proposed usage of SMS printers
ZCAHRD
•PMTCT capacity for quick on-site implementation
•Ability to conduct research and evaluations
UNICEF
• RapidSMS experience + technical capacity
• Funding

Locations of Pilot Sites Luapula Province: • 11 Sites • Across 3 Districts • Implementer: UNICEF
Southern Province: • 10 sites • Across 2 Districts • Implementer: ZCAHRD
Central Province: • 3 Site • Across 3 Districts • Implementer: CHAI & ZPCTII
Copperbelt Province: • 3 Sites • Across 2 Districts • Implementer: CHAI & ZPCT II
Northern Province: • 2 Sites • Across 1 District • Implementer: CHAI & ZPCT II
North-Western Province: • 2 Sites • Across 2 Districts • Implementer: CHAI & ZPCT II
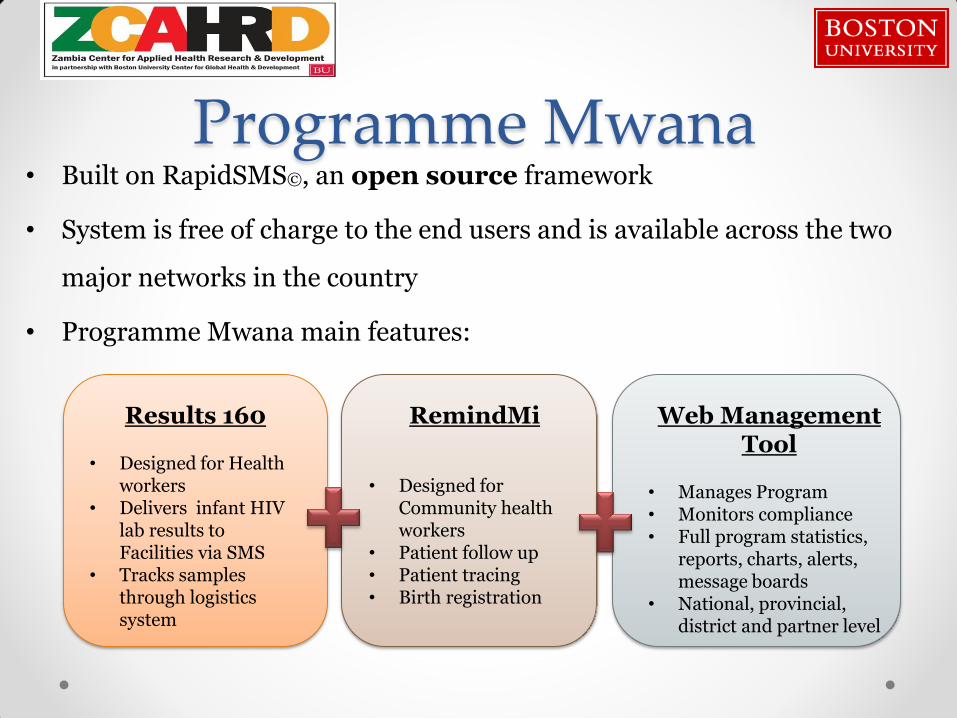
Programme Mwana • Built on RapidSMS©, an open source framework
• System is free of charge to the end users and is available across the two
major networks in the country
• Programme Mwana main features:
Results 160
• Designed for Health workers
• Delivers infant HIV lab results to Facilities via SMS
• Tracks samples through logistics system
RemindMi
• Designed for Community health workers
• Patient follow up • Patient tracing • Birth registration
Web Management Tool
• Manages Program • Monitors compliance • Full program statistics,
reports, charts, alerts, message boards
• National, provincial, district and partner level



From Pilot to scale MOH approved Pilot Proposal
Onsite system development supported by UNICEF
Launch of the Pilot phase (8
Months)
Publication of pilot
evaluation (WHO bul.)
Evaluation & Dissemination meeting with
MoH and Partners
Recommendation to scale and
National Launch
2009 – 10 Jul ‘10 – Feb ‘11
May‘11 Nov ‘11 Mar ‘12
* National Scale-up activities for Programme Mwana commenced in 2012 beginning with 200 sites
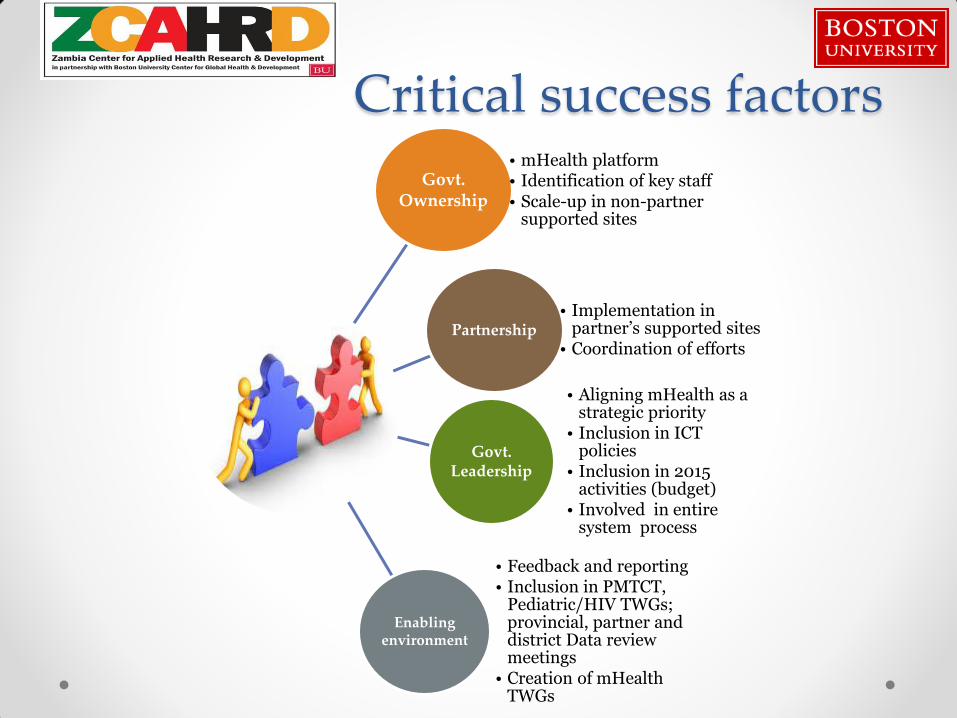
Govt. Ownership
• mHealth platform • Identification of key staff • Scale-up in non-partner
supported sites
Partnership • Implementation in
partner’s supported sites • Coordination of efforts
Govt. Leadership
• Aligning mHealth as a strategic priority
• Inclusion in ICT policies
• Inclusion in 2015 activities (budget)
• Involved in entire system process
Enabling environment
• Feedback and reporting • Inclusion in PMTCT,
Pediatric/HIV TWGs; provincial, partner and district Data review meetings
• Creation of mHealth TWGs
Critical success factors

Coordination • Provided through leadership of MOH & UNICEF
• Use of both international and local software developers Collaboration of
development teams
• Provision of system on two major networks Collaboration with mobile
service providers
• To coordinate and oversee all mHealth activities Creation of the mHealth
TWG
• Based on lessons learnt from pilot and scale-up phases Refinement of system
• Creation of national training materials based on lessons learnt
Standardization of training materials
• At partner and provincial level Training of national
master trainers
• Creation of national scale-up through mHealth TWG Coordination of scale-up
process

System Integration • System fit into already existing PMTCT and EID programs • Translated into the 7 major languages • Standardization of registers used • Inclusion of mHealth in National eHealth strategy
Adaptability
• Reports generated by system included in national review meetings • Users receive monthly aggregated reports • Use of data to inform the management and direction of the program
System data
• Use of local developers • Access databases located in DNA PCR testing labs • System server based at MOH • Ease and duration of trainings
System
• No cost to end users • Simplicity of messages • Use of personal phones
Usability

• MOH endorsed national scale up to all PMTCT/EID sites in the country
o Partners involved in the scale-up strategy development and
adoption
• MOH established the national mHealth TWG chaired by the ministry to
oversee, manage and report back on the scale up process
• Master trainers formed at provincial and district levels to cascade localized
training and support
• Scale up activities commenced in 2012 with 200 facilities targeted
o Currently operating in > 730 facilities (52% coverage) across 10 provinces
Sustainability

System Impact
Scale-up activities conducted in
facilities with and without mobile network access
Availability of program data for implementers via
the Mwana web tool at National, provincial,
district and partner level
Increase in DBS testing numbers
from 4829 samples in 2010
to 11076 in 2012*
Effective usage of the blast
messaging feature for other health related issues
(+7790 messages sent out)
Transparency of data: https://mwana.moh.gov.zm
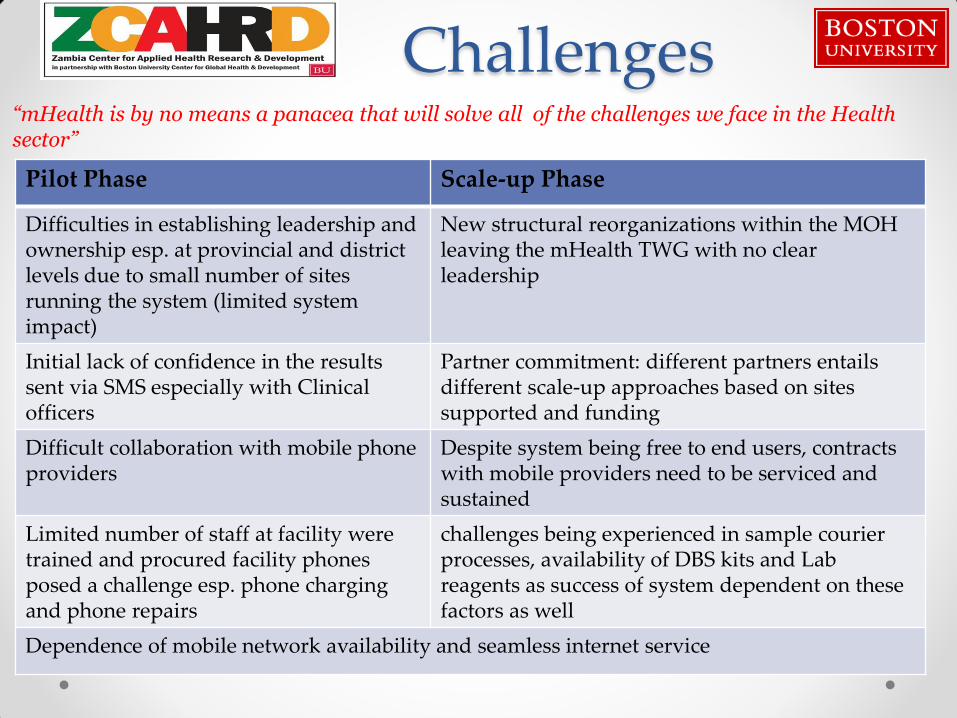
Challenges “mHealth is by no means a panacea that will solve all of the challenges we face in the Health sector”
Pilot Phase Scale-up Phase
Difficulties in establishing leadership and ownership esp. at provincial and district levels due to small number of sites running the system (limited system impact)
New structural reorganizations within the MOH leaving the mHealth TWG with no clear leadership
Initial lack of confidence in the results sent via SMS especially with Clinical officers
Partner commitment: different partners entails different scale-up approaches based on sites supported and funding
Difficult collaboration with mobile phone providers
Despite system being free to end users, contracts with mobile providers need to be serviced and sustained
Limited number of staff at facility were trained and procured facility phones posed a challenge esp. phone charging and phone repairs
challenges being experienced in sample courier processes, availability of DBS kits and Lab reagents as success of system dependent on these factors as well
Dependence of mobile network availability and seamless internet service

Next steps with mHealth in Zambia
• MCDMCH (Ministry of Community Development Mother and Child Health) is scaling up Option B+ in Zambia and this offers up new creative and innovative way to use Mwana: o Adherence
o Mentorship
o Community
o Patient follow up
• Other possible system modules for inclusion o Disease Surveillance module
o Stock module to address issues related to stock management
• Working closely with the ministries to further enhance partnerships with the mobile providers o Bring on board 3rd mobile provider
Thank You Contributors: Judith Nguimfack, Corrie Haley, Jill Berkowitz, Kebby Musokotwane & Donald Thea
Funders: CDC, Bill & Melinda Gates Foundation, Johnson & Johnson, USAID, Global Fund
Government through: MOH & MCDMCH
Partners: UNICEF, CHAI, CHAZ, CIDRZ, ZCAHRD & ZPCTII



















