
GLOBAL gf forum
121
GLOBAL INFORM ADVISE REACH EDUCATE GOING DIGITAL IN 2013 sneak peak in December gf g f GLOBAL forum OCTOBER 2012 =63 0::<, IN THIS ISSUE PAYERS AND REIMBURSEMENT - PART 2 - PAGE 10 NEW SECTION: WOMEN IN HEALTHCARE PAGE 107 DIA 2013 CHAIR ANNOUNCED PAGE 116
Transcript of GLOBAL gf forum

GLOBALINFORM ADVISE REACH EDUCATE
GOING DIGITAL IN 2013 s n e a k p e a k in December
gfgfGLOBALforumOCTOBER 2012
IN THIS ISSUEPAYERS AND
REIMBURSEMENT - PART 2 -PAGE 10
NEW SECTION: WOMEN IN
HEALTHCAREPAGE 107
DIA 2013 CHAIR ANNOUNCED
PAGE 116

Couldn’t Attend DIA 2012?Now You Can See and Hear Everything You Missed!If you missed out on this year’s DIA 2012 Annual Meeting, you can now purchase content that was delivered at this year’s program! DIA wants you to continue to benefit from opportunities to learn and grow professionally, year-round.
View available presentations captured in digital audio with synchronized slides.
Download available offerings in MP3 format to your mobile device for portable listening.
01 Clinical Operations02 Project/Portfolio Management and Strategic Planning03 Innovative Partnering Models and Outsourcing Strategies04 Non Clinical and Translational Development/ Early Phase Clinical Development05 Product Advertising and Marketing06 Medical Writing and Medical Communications07 Processes and Technologies for Clinical Research08 Regulatory Affairs and Submissions 09 Medical Diagnostics and Devices 10 Public Policy/HealthCare Compliance/Regulatory Law11 Compliance to Good Clinical Practice (GCP), Good Laboratory Practice (GLP), and Quality Assurance (QA)
12 Pharmaceutical Quality 13 Health Economics and Outcomes (HEO)/ Comparative Effectiveness Research (CER)/Health Technology Assessment (HTA)14 Clinical Safety and Pharmacovigilance15 Statistical Science and Quantitative Thinking16 Professional Development17 Global Regulatory18 Rare/Neglected Diseases19 SIAC Showcase21 Late Breaker22 White Paper Showcase
This year’s tracks include:
Note: Continuing education credits are NOT available for archived content accessed through the Live Learning Center.Content available for 18 months and will expire on December 28, 2013.
Visit www.diahome.org/dia2012 for more information.
Entire Meeting Package: $799.99

1
INFORM10
ADVISE24
REACH38
EDUCATE92
CONTENTSCONTENTS
Open Forum 4Andrze j Czarnecki
President’s Message 6Ling Su
Executive Director’s Message 8Paul Pomerantz
INFORM 10Pricing and Reimbursements of Medicines: Who Wil l Pay for Innovation? (Part 2) 11 A lberto Gr ignolo, PhD The Payer/Reimbursement Environment in China: Current and Future 12 Kather ine WangNew Times For Health Technology Assessment In Brazi l ’s Public Healthcare System 14
Ivan V ie joPharmaceutical Reimbursement Environment in Korea: Current and Future 17 Soo MiThe Payer/Reimbursement Environment in Canada: Current and Future 21 Judi th Glennie
ADVISE 24What To Do if You Expect
Joseph McMi l l ian Kimber ly BrownThe Cloud Teleconference Summary 30 R. L. Chamber la in Pamela Campbel lElectronic Credential ing and Quality Management 36 Matt Haddad
REACH 38
NORTH AMERICADIA 2012: Cal l to Meta-Collaborate 39DIA 2012: Securing the Supply Chain 42DIA 2012: Orphan Drug Development 44 K innar i Pate lDIA & NORD Team for Rare Disease/Orphan Product Conference 46
STUDENTS REFLECT ON DIA 2012Students’ Focus on DIA 2012 Collage 48
Ashlyn JoseSession Report:
Natal ie MelamedSession Report:Prescription Drug Marketing
E l isa L. Pr iestSession Report:
Slanix Paul T. A lexSession Report:Patient Advocacy in Product
Ashlyn JoseCanadian Annual Meeting:
Role of Cl inical Pharmacology in Successful IND and NDA Submissions using Principles of Pharmacokinetics
Dr. Puni t Marathe Dr. Mehul MehtaUpcoming Events: North America 62
gfgf

GLOBAL FORUM gfgf
P U B L I S H I N G I N F O R M AT I O N
VO
L 4
ISS
UE
5
2
Paul Pomerantz
Andrzej Czarnecki
Global Forum Staff
Mission
Global
Forum
Publishing and Subscription:
Contact Information for Advertising:
Global Forum
Global Forum
Postmaster:
Design:
DIA is a neutral organization that does not advocate for or against any issue. The views expressed by the individual authors or interviewees in the Global Forum are theirs and do not necessarily represent the views of the Drug Information Association.

3
JAPANJapan’s Efforts to Keep Innovative Research on Japanese Soil 63 Meg Egan AudersetSpeaking Up in Japan 66 Meg Egan AudersetThe First DIA CMC Forum in Japan 68 Haruhi ro Okuda
LATIN AMERICAQuestions and Answers with Dr. Eduardo Johnson 70DIA and the Brazi l ian Society of Pharmaceutical Medicine Form Strategic Partnership 72 A le jandro H. Bermudez-Del V i l larExpanding Horizons in the Region: Successful Risk Management DIA Tutorial in Bogota, Colombia 73
CHINAPatent Draft ing Strategies:
EUROPEHow the EU Regulatory Environment is Changing for Drug/Device Combinations and Companion Diagnostics 79 Shayesteh Fürst-Ladani
EuroMeeting in Amsterdam 81DIA Conference on European
Upcoming Events: Europe 86
INDIATamil Nadu Student Chapter Regulatory Workshop 87 Annabel le Rajaseharan
Mumbai Student Chapter Hosts “Leaders of Tomorrow” 89
EDUCATE 92Affordable Care Act: What Happens Next? 93
REGULATORY ROUNDUPDIA 2012: CDER, CBER & CDRH
Report from DIA 2012 CDER Town Hall 97Regulatory Consideration forCombination Products 99 Carol H. Danie lson
ACPE Credit Request Update 102NIH Director Highl ights Innovation Forum 103 Francis Col l ins
WOMEN IN HEALTHCARE DIA & HBA Collaborate to Address Challenges in Women’s Leadership 107Kickoff Meeting of the HBA/DIA Women’s Leadership Collaborative Effort. 110
IN EVERY ISSUE
ASSOCIATION NEWSBoard of Director President Ling Su Visits DIA Headquarters 112 New SIAC for Translational Medicine 113 Online Community Content
Dr. Sandra Mil l igan Named DIA 2013 Program Chair 116
CONTENTSCONTENTS

GLOBAL FORUM V
OL
4
IS
SU
E 5
4
gfgf
O P E NF O RU M
The Global Forum INFORM section is dedicated to provide useful information on many aspects of our everyday work and we do hope that our readers benefit well from the content of these sections, which, over the last period, covered many topics, e.g. biosimilars, ICH, orphan drugs and rare diseases, transparency and social media and others. We plan many more, which in our view are very interesting. However, the Editorial Board would be very interested to hear from our readers what they would like to see as topics to be addressed by Global Forum in the future. Our publication, just as our organisation, is based on volunteers who wish to contribute, deliver and in that way provide support for our readers.
The Global Forum, which is in your hands today, provides a compilation of information worth keeping in your library at least for some time. The Pricing and Reimbursement (P&R) articles from several countries outside of the ICH regions (these were
ANDRZEJCZ ARNECKI
presented in the August issue) certainly qualify to be a part of our collection. They should be read by many people on all sides of the debate on P&R but, specifically by those involved in arguments on making the drugs available for patients. Potential inclusion of reimbursement/economic debates into the drug licensing process started more than 20 years ago and used to be called the 4th hurdle at the time when budgets became stretched and pharmacoeconomics was gaining ground. The answer to what extent P&R became the 4th hurdle in today’s environment, I leave to those reading our series of articles on these topics in the August and October issues, and those directly involved in licensing in many countries where a very close association between the regulatory process and the P&R exists. The EU, EMA Roadmap 2015, released early last year, refers to a need to collect data on efficacy and effectiveness at the same time to collect relevant data during the regulatory process, which could be used for the subsequent P&R review. It may be worth giving a thought what will be the impact on drug availability created by coexistence
Global Forum Library
of these two processes. I would like to thank Alberto Grignolo for his excellent guidance and contribution to this section, which will become a part of our Global Forum library.
In several previous issues the reference to innovation has been made in different areas, not only in the pharmaceutical field. One of the driving engines for successful progress in our lifetime is the fast development of ‘computing technology’. It has an impact on all areas of progress, including a big change in our personal/interpersonal and overall communication, which arrived with the extensive use of social media (see April issue). In the ADVISE section of this issue one can find the article entitled ‘The Cloud’. It is a well-written summary report from a teleconference that took place about 15 months ago. It is clear from the discussion that cloud computing and its further developments enter our life now and will change the way we work and use our computer hardware and computer technology to communicate and progress to our future goals. It may become one of the turning points, which as many times in the past, have managed to change entirely our lives.
Frequently, living through a change we do not realize what happens and do not appreciate it. We got used to technological progress so much that 43 years after the first landing of men on the Moon, supported by the use of technology less powerful than today’s home use laptop, a huge
technological step forward related to the landing on Mars of an extremely sophisticated vehicle was quickly overshadowed by everyday news.
The above example illustrates well the enormous progress in science and technology, which allows for everyday use of fantastic equipment that drives the next generation into the future in every area. What more is needed, however, is to combine forces to facilitate the open mindedness allowing creative people to use technology and knowledge in combination with their brain power to move science, remove barriers, and provide economy to support development of new technologies and medicines. One can appreciate now how the Moon landing technology coming into our houses pushed society ahead; proving usefulness of innovations that at first may not be apparent but become phenomenally useful in the future.
Pricing and reimbursement are the concepts that have arisen from constrained budgets attempting to control spending. This is a very noble idea in provision of health care to wider societies. What must be remembered, however, is that any breakthrough development requires investment of concept (brain), technology and economy. The Moon and Mars landings happened thanks to such commitments; so did medical innovations. Let’s keep it that way despite all obstacles.
Global ForumEditorial Board
Andrzej Czarnecki, MD, PhD, DSc
Richard Chamberlain, PhDECS, Inc.
Ronald D. Fitzmartin, PhD, MBAManaging Partner
Decision Analytics, LLC
Alberto Grignolo, PhDPAREXEL
Justina A. Molzon, MS Pharm, JD Associate Director for International Programs
CDER, FDA
Sarah PowellTh omson Reuters
Nancy D. Smith, PhDPotomac, MD
Jean H. Soul-Lawton, DPhilGlaxoSmithKline
Veronica TodaroParkinson’s Disease Foundation
J. Rick Turner, PhDQuintiles
Qingshan Zheng, PhDShanghai University of
Chinese Medicine, China

GLOBAL FORUM V
OL
4
IS
SU
E 5
6
gfgf
P R E S I D E N T ’ S M E S S A G E
This Global Forum continues the focus on pricing and reimbursement for pharmaceutical and related healthcare products that we began to explore in our August issue. Having previously examined the current and future pricing and reimbursement climates for these products in the US, Europe and the European Union, and Japan, this issue examines these topics as they manifest in China, India and Latin America. I am grateful to Dr. Alberto Grignolo for the exemplary creativity and stewardship he has demonstrated by serving as editor for these special sections on such a timely and important subject.
DIA has a strong tradition of providing education and training in drug development. But no matter how carefully they are designed,
developed, tested, marketed or monitored, pharmaceutical therapies are only useful to the degree they can be accessed by the patients for whom they are intended. As a result, regulatory approval and marketing authorization are no longer the “finish line” for our products. Pricing and reimbursement strategies and frameworks are critical not only to the sponsors who make such significant investments in developing and manufacturing these products, but to the patients whose well-being these products will improve.
This is just one of many examples of how DIA strives to center our work on the patient. For another, I invite you to read in this issue about our upcoming second annual US Conference on Rare Diseases & Orphan Product: Shaping the Future Now, presented this month in partnership with the National Organization for Rare Disorders, which will bring patients and patient advocates together with
Pricing, Patients and Program Participation
LINGSU

7
industry experts, senior leadership from the FDA and National Institutes of Health to discuss innovative ways to develop, regulate, market and pay for orphan products to treat patients with rare diseases. DIA Europe presents an annual rare disease/orphan product conference in partnership with EURORDIS (“The Voice of Rare Disease Patients in Europe”) each spring, to complement this DIA-NORD conference each fall.
At the same time, other upcoming opportunities demonstrate our drive to meet the needs of our patient, industry, regulator and other stakeholders in a modern world that seems to grow more globally interconnected each day. Our regional staff and volunteer leadership in Europe have teamed to present our 6th Annual Clinical Forum in Europe: The Empowered Patient at the Hague in the Netherlands, our first Clinical Forum to offer patient, student and young professional fellowships. We’ve just concluded our annual Latin American Regulatory Conference in Mexico City (Mexico), thanks to the efforts of our volunteer leadership, regional staff, and program committee composed of clinical, regulatory and industry leaders from throughout the Americas. Soon we will come together for our 2012 Canadian Annual Meeting, our 9th DIA Japan Annual Meeting, and our 7th Annual Conference in India: Discovery through
Commercialization: Innovative Strategies for Individualized Healthcare which, again, puts the individual patient at the center of its agenda.
DIA is a worldwide professional network of members voluntarily serving our global healthcare community. I sincerely thank our volunteer program committees for the time and expertise they’ve shared to develop these important opportunities; through your efforts, our global and multidisciplinary association will work and learn together. If you’re not yet a DIA member or volunteer, please accept this invitation to join us. Amidst all these educational and networking forums, among all these topics and locations, there is surely room for your contribution too.
GLOBAL FORUM V
OL
4
IS
SU
E 5
8
gfgf GLOBAL FORUM
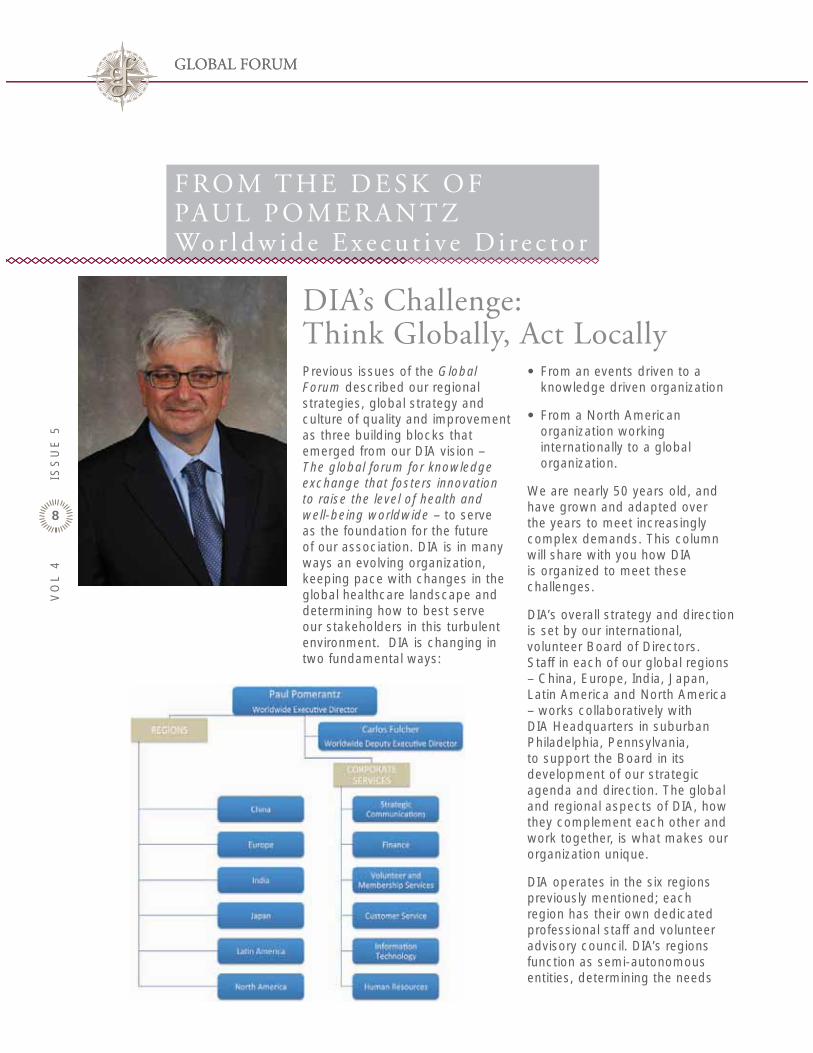
F RO M T H E D E S K O FPAU L P O M E R A N T ZWo r l d w i d e E x e c u t i v e D i r e c t o r
Previous issues of the Global Forum described our regional strategies, global strategy and culture of quality and improvement as three building blocks that emerged from our DIA vision – The global forum for knowledge exchange that fosters innovation to raise the level of health and well-being worldwide – to serve as the foundation for the future of our association. DIA is in many ways an evolving organization, keeping pace with changes in the global healthcare landscape and determining how to best serve our stakeholders in this turbulent environment. DIA is changing in two fundamental ways:
From an events driven to a knowledge driven organization
From a North American organization working internationally to a global organization.
We are nearly 50 years old, and have grown and adapted over the years to meet increasingly complex demands. This column will share with you how DIA is organized to meet these challenges.
DIA’s overall strategy and direction is set by our international, volunteer Board of Directors. Staff in each of our global regions – China, Europe, India, Japan, Latin America and North America – works collaboratively with DIA Headquarters in suburban Philadelphia, Pennsylvania, to support the Board in its development of our strategic agenda and direction. The global and regional aspects of DIA, how they complement each other and work together, is what makes our organization unique.
DIA operates in the six regions previously mentioned; each region has their own dedicated professional staff and volunteer advisory council. DIA’s regions function as semi-autonomous entities, determining the needs
DIA’s Challenge: Think Globally, Act Locally
ffffffffffffffffffffggggggggggggffffffffffffffffggggggggggggggggggggggggggggggggggggffffffffffffffffffggggggggggggggggggggggggggffffffffffffffffffffffffffggfffffffgggfgggggggggggggggggfggggggggggggggggggggggggggggggggggggggggggggffffggggfffffggggggggfffggggggggggggggfgggggggggggggggggggggggggggggggggggggggggggggggggggggggggggggggggggggggffffffffffffggggggggggggggggfffffffffffffggggggggggggggfffffffffffffggggggggggggfffffffffffffgggggggggggggggggggggggggggggggggggggggggggggggggggggggggggggggggggggggggggggggggggggggggggggggfggggggggggggggggggggggggggggggggggggggggggggggggggggfggggggggggggggggggggggfgggggggfffffgggggggggggggggggggggggggggggggggggggggggggggggggggffffffggggggggggggggggggggggggggggggggggggggggggggggggggggggggggggggggggggggggffgggggggggggggggggggfgfgf

9
of the region and implementing programs to address them. Moreover, each advisory council is representative and maintains close ties with each of our four stakeholder communities—regulatory, patient, industry and academia.
DIA simultaneously operates on a global level. Our Corporate Services team, based at worldwide headquarters, provides finance and accounting, human resources, customer service, information technology services and support, to every DIA region (see accompanying graphic). Our publications, the Drug Information Journal (to be relaunched in January 2013 as Therapeutic Innovation & Regulatory Science and already attracting global attention) and our membership magazine, your Global Forum, also fall under Corporate Services. As Worldwide Executive Director, I am directly accountable to the Board of Directors for the successful implementation of the DIA Strategic Plan, the identification of opportunities and potential partnerships to enable the association’s growth, and to nurture and develop in all our regions the best practices that will enhance their maturity and our stakeholders’ DIA experience.
DIA is constantly challenged by the familiar expression: “Think globally, act locally.” To create an effective global community, we must identify and work with the different types of regional relationships, including those between industry, regulators, and other organizations like DIA. An opportunity in China, for example, needs to be addressed in a completely different way than an equivalent one in India:
The culture and stakeholders are different and the way they communicate about and with each other is different.
DIA Europe provides a most fascinating case in a very complex environment: To develop effective programs for our members and volunteers in their region, DIA Europe often works with the European Union and its 27 different Member States, plus non-Member States, and the European Medicines Agency (EMA) as well as the national regulatory authority for each Member and non-Member State. DIA Europe must operate judiciously to successfully navigate this complex system.
For a more global perspective, let’s turn to an international corporation like McDonalds®. No matter where you are, from New York to Paris to Tokyo, you’re generally going to be served the same product, and your customer experience will have pretty much the same look and feel, regardless of location. A “brand” describes an organization’s reputation and the expectations of its customers or constituents. While not as dispersed or well-known as McDonalds, DIA nonetheless has a consistent global brand that transcends and encompasses all our regions. The training and tools provided by DIA volunteers to improve the quality and safety of medical products have credibility all over the world.
We also must balance certain geopolitical realities. DIA is very active in both Japan and China, our most rapidly growing region. While western and central European nations have helped develop and lead activities in DIA
Europe, nations in eastern and southern European countries would like to become more involved in advancing these agendas. How does a worldwide organization responsibly address these issues, effectively balancing local countries’ needs with the global good? How do we recognize and measure such opportunities, not only from the business and organizational perspective, but also from a socially responsible point of view?
Two recent initiatives that successfully navigated this global/local challenge are the designation of North America (NA) as a standalone region and the development of the new SIAC Leadership Council. By divesting DIA NA from global headquarters’ operations, DIA has evolved from a North American-centric organization with offices in other countries into a truly global organization in which all six regions are equally recognized and supported. The new volunteer SIAC Leadership Council now has a place on the Member & Volunteer Engagement Committee of our Board, elevating the SIACs to global stature.
As DIA broadens our services from a historically events-driven organization to a knowledge provider dedicated to helping improve the global quality of and access to healthcare products, we can feel this transformation taking place. DIA stands at the inflection point of becoming a new kind of organization. Join us on our journey.
INFORMINFORM gfgfPayers and
Reimbursement

11
Pricing and Reimbursements of Medicines: Who Will Pay for Innovation? (Part 2)
In Part 1 of this Special Section (Global Forum, August 2012) we surveyed the frameworks for the pricing and reimbursement of medicines in the United States, the European Union and Japan. Thanks to the respective authors’ expert illustrations, we saw how heterogeneous and complex these frameworks are, and how fluid they remain.
In this issue of Global Forum we turn our attention to four additional markets of importance – Brazil, Canada, China and Korea. And once again we see heterogeneity and complexity, as well as continuously evolving national thinking in the face of economic pressures on health care budgets. In the context of economic evaluation, will we soon see a “Brazilian NICE?” Will the Canadian Evidence Building Program (EBP) for oncology products yield the desired clinical- and cost-effectiveness data and satisfy the information needs of payers? Will China succeed in supplementing the Basic Medical Insurance (BMI) scheme with commercial healthcare insurance, and how should pharmaceutical innovators conduct themselves to ensure future reimbursement in this evolving environment? Is the Korean HIRA (Health Insurance Review and Assessment) service and its focus on therapeutic and economic aspects for benefit coverage a model for others in the Asia Pacific region or elsewhere?
It seems rather clear that a convergence of regulatory, clinical and commercial strategies from the earliest stages of drug development is now a sine qua non to help ensure patient access and commercial success in a “dynamic” global pricing and reimbursement environment for medicines. In industry, this will require R&D and Commercial colleagues to be less arm’s length from each other than has often been the case, and to start speaking the same language from Day 1 of drug development, in effect conducting drug development with reimbursement in mind.
ALBERTO
GRIGNOLO
PhD
Specia l Sect ion Edi tor
Read Your Global Forum
on the
GO

GLOBAL FORUM | V
OL
4
IS
SU
E 5
12
gfgf
OVERVIEW OF BASIC MEDICAL INSURANCE PROGRAMS
Healthcare represents a large and rapidly growing market in China. The Chinese government has been the main payer in the market, offering a social security net comprised mainly of three types of health insurance: Basic Medical Insurance (BMI) for Urban Employees, BMI for Urban Residents1, and Rural Cooperative Medical Scheme2. Private insurance offers optional add-on coverage but this segment remains very small.
The BMI for Urban Employees, contributed by both employers and employees, was initiated in 1999 and is mandatory for urban employees. Fundamental policies and rules are made by the central government agencies for the coverage of the BMI for Urban Employees and to be implemented by provinces with authorized variations. The BMI for Urban Residents, piloted since 2007, is voluntary for urban residents not eligible for the BMI for Urban Employees, e.g. unemployed, seniors, children, students and disabled and covers serious diseases and hospitalization. Rural Cooperative Medical Scheme, established
in 2003, is voluntary for rural population and covers serious diseases and hospitalization. Those who cannot afford any of these three health insurances and suffered from serious diseases may be qualified for public medical aid for the poor. By the end of 2011, approximately 95% of the total population was covered by one of the three types of basic medical insurance.3
Drugs reimbursed by the BMI for urban population are defined in the Reimbursable Drug List (RDL). The Ministry of Human Resources and Social Security (MOHRSS) is in charge of defining the National RDL, which is expected to be updated every 2 years but such frequency is not mandatory. Historically, the inclusion of drugs in the National RDL lacked a consistent process and allowed little transparency into the evaluation criteria. The opinions from key opinion leaders in the relevant therapeutic areas of clinical practice played a dominant role. The latest National RDL was issued in November 2009 and comprised 1,140 chemical/biological medicines and 987 traditional Chinese medicines. Along with the publication of the National RDL, MOHRSS also announced a more comprehensive approach for future RDL listing process. In addition to opinions from key medical practitioners, MOHRSS will consider evidence-based data as well as pharmaco-economic information.4
KATHERINE
WANG
Th e Payer/Reimbursement Environment in China:
Current and Future

13
price. The growth potential from BMI reimbursement appears limited; future growth may arise from the private insurance segment. One of the initiatives indicated in the recent five-year plan for healthcare reform is to further promote the growth of commercial healthcare insurance as a supplement to BMI. Pharmaceutical companies are encouraged to adopt a combination of strategies to better adapt to the changing reimbursement paradigm.
References/citations from this article are available upon request.
Bureau of Medical Insurance to set an annual cap for hospital expenditure. Hospitals which did not exceed the annual BMI spending can keep budget savings; those exceeding the annual BMI spending will need to self-fund excess spending and face delayed BMI payment in the subsequent cycle as well as delayed funding for infrastructure expansion. The per patient payment scheme aims to cap BMI spending based on the forecast of total patients receiving outpatient services during the BMI payment cycle (typically one year), with an objective to reimburse fees for basic medical diagnostic tests, basic treatment and Class A National RDL drugs. The per disease payment scheme focuses on diseases with a clear clinical pathway and stable treatment costs and aims to cap BMI spending for a particular disease for the entire treatment cycle.
Additional policy initiatives were introduced to change the hospital financing structure. Drug sales have historically been the main income source for Chinese hospitals. The Ministry of Health (MOH) and the National Development and Reform Commission (NDRC) would like to adjust prices for healthcare services through an increase in fees for physician services and regular diagnostic tests and a decrease in fees for new and high-end diagnostics. The agencies also piloted a program to remove hospital mark-ups on drug sales. Some local bureaus of health use drug income containment as a key performance indicator for hospitals and hospital directors and results would be linked to financial incentives.
OUTLOOK
The Chinese government is clearly determined to broaden the BMI coverage at an affordable
The provincial Bureaus of Human Resources and Social Securities (BOHRSS) are responsible for defining the Provincial RDLs applicable to each province. Drugs in the National RDL are grouped into two Classes with different reimbursement ratios and flexibilities for local adjustment by provincial BOHRSS. Class A of National RDL includes drugs which are necessary and widely used in clinical treatment with good efficacy and lower prices and cannot be adjusted by provincial governments. All drugs listed in Class A of National RDL are fully reimbursable. Class B of National RDL include drugs which are available for clinical treatment with good efficacy and higher prices than a comparable Class A drug. Local governments can adjust the types of drugs listed in Class B of National RDL based on local state of economic development, medical needs and prescription pattern. Drugs listed in Class B of National RDL are only partially reimbursable and provincial governments may impose prescription restrictions by indication and/or hospital size on certain drugs with higher likelihood of abuse or greater toxicity and side effects.
NOTABLE POLICY LEVERS TO CONTROL HEALTHCARE SPENDING
While the coverage of basic medical insurance is expanding, the overall healthcare expenditure paid by the BMI fund is growing rapidly. In order to effectively control BMI costs, MOHRSS issued an opinion5 in May 2011 to introduce a few policy levers, notably BMI budget control, per patient payment for outpatient costs and per disease payment for costs associated with hospitalization and outpatient treatment for severe diseases. Over 40 cities in China, including Beijing and Shanghai, have been selected to pilot BMI budget control, which requires the local
KATHERINE WANG is a Counsel for Sidley Austin LLP’s Global Life Sciences Practice in Shanghai. She participates in providing risk analyses on life sciences com-panies’ operations and business strategies in China. Ms. Wang assists pharmaceutical, biotech-nology, and medical device com-panies on a wide range of corpo-rate, commercial, and regulatory matters, including product regis-tration, pricing, reimbursement, clinical studies, GMP compliance, promotional practices, patient disputes caused by adverse drug events, FCPA/anti-bribery, and general IP issues. She also as-sisted institutional investors and corporate clients in structuring transactions and conducting reg-ulatory due diligence (e.g. GMP and pharmacovigilance) of their investment targets in China. Ms. Wang has been recognized as a leading lawyer in life sciences by Chambers Asia since 2011.
Ms. Wang received her LL.M. de-grees from Harvard Law School and National Taiwan University. She is admitted to the New York Bar. She is a native Chinese speaker and is fluent in English.

GLOBAL FORUM | V
OL
4
IS
SU
E 5
14
gfgf
INTRODUCTION
Brazil’s public healthcare system – SUS (Sistema Único de Saúde) – aims to deliver healthcare coverage to the whole population. Despite this objective, from 1998 to 2008 only 58.6% of interventions (on average) in SUS were fully covered by public funding1, while the remaining were funded by patients through either private health schemes or out-of-pocket payments.
People are provided healthcare through the government and it is funded through salary-based compulsory contributions by employers and employees; general taxation through federal, state, and municipal budgets; and other sources. Besides this coverage, 24% of the population has some level of private healthcare coverage2.
In Brazil, although the Ministry of Health is the main responsible party for management of healthcare policies and services through the national health service (SUS), it is the States and Municipalities who are provisioning and delivering healthcare to their respective populations.
In order to coordinate the actions of these three layers of geographical coverage, together with the Ministry of Health there
are two other main bodies: CONASS3 (Conselho nacional de secretaries de saúde)- National Council of Health Secretaries, composed of the health secretaries of the 26 states; and CONASEMS4 (Conselho nacional de secretarias municipais de saúde) - National Council of Municipal Secretaries of Health, which coordinates health policies and actions across Brazilian municipalities.
In addition to these bodies, there is one national agency that supervises and regulates the activity of private health plans in Brazil, the so-called ANS5 (Agência Nacional de Saúde Suplementar) - National Agency for Supplemental Health. This agency is directly under control of the Ministry of Health.
Despite the widespread coverage of the public health system, it only represents a small percentage of total drug expenditure in Brazil, while private expenditure accounts for 79%6.
PRICING AND REIMBURSEMENT OF PHARMACEUTICALS
Once regulatory approval is granted by ANVISA (Agência Nacional de Vigilância Sanitária), pricing is generally agreed within 1-2 months at a national level (maximum price to consumer).
IVAN VIEJO
New Times For Health Technology Assessment
In Brazil’s Public Healthcare System

15
CONITEC (Comissão Nacional de Incorporação de Tecnologias no SUS) - National Committee for the Incorporation of Technologies in SUS.
The mission of CONITEC is to advise the Ministry of Health for the incorporation, alteration or exclusion from SUS of new health technologies, new medicines, products and procedures and to elaborate and modify clinical protocols and therapeutic guidelines. CONITEC will evaluate, on manufacturer’s request, new medicines, products and technologies/procedures, and after a public consultation period, will publish its recommendations on whether a new technology should be incorporated in SUS and under what conditions. From the moment of application until final recommendation there is a period of 270 days. Experimental procedures and medicines, products or new technologies not registered at ANVISA (Agência Nacional de Vigilância Sanitária) - National Agency for Health Surveillance - are not entitled to apply for incorporation into SUS.
CONITEC is also responsible for updating of RENAME (Relação Nacional de Medicamentos Essenciais), the National Formulary for Essential Medicines.
ECONOMIC EVALUATION
Decree 7.646 establishes that one of the criteria for evaluation of new products and technologies is the economic evaluation of the product compared to current ones used at SUS. In addition to this, for a new drug the manufacturer must present the price given by CMed.
To add more complexity to the pricing system, every Brazilian State applies a different taxation level to medicines. This tax can be as high as 19%.
For pharmaceutical purchases (municipal, state, and federal) within the public system a price reduction factor (CAP) is applied. The CAP is uniformly applied to the ex-factory price of new products, which is established by an international reference price system. Calculation of the price reduction factor takes into account Brazil’s per capita GDP and the equivalent in the reference countries.
There is no kind of reimbursement system in place for a prescription generated outside the public Hospital/Clinic environment in Brazil.
INCREASING IMPORTANCE OF HTA (HEALTH TECHNOLOGY ASSESSMENT)
On the 28th April 2011 a new law (Lei 12.401-sobre a assistência terapêutica e a incorporação de tecnologia em saúde no âmbito do SUS) defined new criteria and process for the incorporation of new health technologies within SUS. This includes drugs, medical devices and procedures. Lei 12.401 defines criteria for evaluation of new drugs/products/technologies and, in addition to the “classical” criteria of efficacy and safety, it specifically mentions economic evaluation.
On December 21, 2011, Decree 7.646 (Decreto 7.646 sobre a CONITEC e sobre o proceso administrativo para a incorporação, exclusão e alteração de tecnologías no SUS) established a new committee,
Prices of pharmaceuticals in Brazil have been regulated by CMed (Câmara de Regulação do Mercado de Medicamentos) - National Chamber for Regulation of Medicines Market - since 2003. CMed has preserved a pre-existing limit on pharmacy profit levels of 30%, as well as adopted strict criteria for setting a ceiling for retail drug prices. The framework bases its estimates on an ‘adequate price coefficient’ of each drug in a basket of nine Western countries - Australia, Canada, Spain, the US, France, Greece, Italy, New Zealand and Portugal - and the product’s country of origin.
The system establishes that the manufacturer’s price for a new, patented product (class I) may not be lower than the lowest equivalent price in any of the countries in the basket. If the drug is classified as non-innovative (Class II) then the proposed price for the drug cannot be higher than the existing alternatives in the market.
CMed also conducts annual price reviews of branded and generic drugs to adapt its prices to the consumer price index evolution (5.81% year-to-year rate on December 20117). In March 2012 CMed authorized an increase of 5.85% for those drugs with a generic market share, within the same therapeutic class, equal or superior to 20% of sales; and an increase of 2.8% for those drugs with a generic market share, within the same therapeutic class, between 15%-19% of sales8. CMed has also the power to exclude registered products from the pricing regime, chiefly to the benefit of inexpensive, essential medicines.

GLOBAL FORUM | V
OL
4
IS
SU
E 5
16
gfgf
it is still unclear how binding its recommendations would be and what could be the real extent of its influence. A wait-and-see approach could be a wise strategy.
If the law and decree on CONITEC and its role are fully implemented, we could be seeing a “Brazilian NICE” (the U.K.’s National Institute for Health and Clinical Excellence) for the public health system in Brazil in the near future, and manufacturers will have to develop “Brazil-tailored” strong economic evidence for their products and technologies.
References/citations from this article are available upon request.
In this new context, where economic evaluation will play a central role for the incorporation of new technologies and products into SUS and RENAME, manufacturers would have to evaluate carefully whether it is worthwhile to invest in developing economic evidence to support their case or not.
They would need to study thoroughly what are the current alternatives used by SUS and, in the case of drugs, if they could successfully develop economic evidence based on price levels given by CMed. This last scenario may have time implications as some manufacturers may opt for delaying the development of this evidence until a price is formally assigned.
Even a positive recommendation from CONITEC would not guarantee that States and municipalities will adopt new technologies and products, since resources within the public system are limited. On top of that, the strongly de-centralized model for provision of healthcare in Brazil makes interaction with payers more complex, as the numbers of key stakeholders increase with each layer of administrative control (national, regional and local).
An initial strategy for new products for creating advocacy in the public system could be approaching some big hospitals that work as mixed economy societies and have a certain independence regarding introduction and use of new products not covered by SUS.
Because CONITEC has been very recently created and has just conducted a few evaluations
Decree 7.646 does not provide that much information about what kind of economic analysis would give a more favourable recommendation for the incorporation of new products and, in the case of new drugs, it is expected that the price used for any potential health economic analysis or model would be the one approved by CMed.
By May 8, 2012, CONITEC had already received 44 applications for evaluation of products. Five of those applications were for medical devices and 39 for drugs9. Twenty-four applications were rejected because of incomplete documentation. On June 19th there were 8 final recommendations published by CONITEC and 6 still open for public consultation10.
Once CONITEC publishes a positive recommendation on the use/incorporation of a new technology or product, SUS will have 180 days to make it available for use.
Financial responsibility for funding of new technologies and products in SUS will be agreed on by the Tri-party commission, where national government, federal states and municipalities are represented.
KEY CONSIDERATIONS FOR GETTING INTO THE PUBLIC SYSTEM: TOWARDS A BRAZILIAN NICE?
While public pharmaceutical expenditure represents only a small part of the Brazilian market, private healthcare and out-of-pocket payments from patients make up almost 80% of the pharmaceutical market.
IVAN VIEJO
Ivan has more than 4 years of experience in market access and price and reimbursement of drugs and medical devices. He has assisted multinational pharmaceutical/biotechnol-ogy companies in developing strategies for the launch and commercialization of new prod-ucts, from clinical trial design to global pricing and launch strategies in the EU, US, BRIC and Latin America markets. He has worked in Market Access and P&R positions at GSK and Simon-Kucher and Partners.
Ivan holds an MPharm and an MBA in pharmaceutical indus-try, from the University of Alcala de Henares in Madrid, Spain.

17
NATIONAL HEALTH INSURANCE PROGRAM IN KOREA
The healthcare system in Korea has two components: National Health Insurance and Medical Aid. The national health insurance system provides coverage to all citizens and it is managed comprehensively in the form of social insurance. It is funded by beneficiary’s contributions. Medical aid component provides support to lower income groups and is funded by general revenue. The medical insurance act was legislated in 1963. But
compulsory medical insurance program was started from company units in 1977 and Universal coverage was achieved in 1989. The Ministry of Health and Welfare (MOHW) oversees the national health insurance system. The National Health Insurance Corporation (NHIC) serves as the insurer and the Health Insurance Review & Assessment service (HIRA) conducts reviews and assessment of medical fees (Figure 1). The review process starts with the health institution submitting claims for medical fees to HIRA. After the HIRA reviews and determines the amount to be reimbursed to the provider, the results are notified to the NHIC and health institution for payment. (HIRA homepage www.hira.or.kr)
SOO MI
Pharmaceutical Reimbursement Environment in Korea:
Current and Future

GLOBAL FORUM | V
OL
4
IS
SU
E 5
18
gfgf
DRUG REIMBURSEMENT SYSTEM IN KOREA
The introduction of positive listing system
The pharmaceutical reimbursement system in Korea has been changed several times. The major change from negative listing system to positive listing system was done in the end of 2006. In the negative listing system, almost all the drugs that were approved by the Korean Food & Drug Administration (KFDA) were automatically listed for reimbursement. However, in the positive listing system, the MOHW grants benefits selectively to pharmaceuticals with cost-effectiveness. The background of introduction of positive listing system was related to the concerns of cost containment and the efficient usage within the limited healthcare resources. The number of listed drugs was over 20,000 in 2007 (Table 1). Also the annual growth and relative increase rate of pharmaceutical expenditure were the reasons of this change (Figure 2). The main purpose of the new system was to select drugs that are effective in both therapeutic and economic aspects for benefit coverage. And another aspect is the separation of reimbursement assessment and pricing decision process. In the negative listing system, the HIRA was responsible for reimbursement as well as the price decision. However, the reimbursement assessment and pricing decision were separated in order to ensure the mutual checks and balance since the introduction of positive listing system (Table 2).
Table 1. Th e number of listed drugs
Figure 1. National Health Insurance Program
Year ’07.1.1 ’08.1.1 ’09.1.1 ’10.1.1 ’11.1.1 ’12.1.1
Figure 2. Pharmaceutical expenditure in Korea

19
the pharmaceutical company is trying to list the drugs with higher price than that of comparators, economic evaluations to prove cost-effectiveness of it should be submitted for the decision-making. Meanwhile, if the drug is satisfied with the following criteria: if the new drug has no alternative treatment; it is used for life-threatening disease; it is used for a minority of patients who have rare disease and also is capable of proving clinically meaningful and substantial improvement such as extended survival, the
negotiation within 60 days. Finally, the MOHW publishes the price to the public after the Health Insurance Policy Council reviews the results within 30 days (Figure 4).
ASSESSMENT FOR DRUG REIMBURSEMENT
For the reimbursement of new drugs, pharmaceutical companies need to prove the clinical usefulness and cost-effectiveness of new drugs through comparison with alternatives. Especially, if
The reform of pricing system (price reduction of patent-expired drugs)
Since January 2012, generic pricing methods have been changed. The same pricing policy in the case of same drugs (same substance, strength, forms) was introduced. Before the implementation of this pricing reform, the price of first generics was 68% of the original’s price while the originals’ price was adjusted to 80% of the previous listing price. However, in the new system, the price of first generics is 59.5% of the original drug price while the original’s price is lowered to 70% of the listed price before patent expiry for the first year when the first generic was listed. After 12 months, the prices of all drugs (original and generics) are lowered to 53.55% of the original product’s price (Figure 3).
DRUG PRICING AND REIMBURSEMENT DECISION-MAKING PROCEDURE
Korea Food & Drug Administration (KFDA) is in responsible for the approval of drugs through evaluation of efficacy and safety. However, for the reimbursement of pharmaceuticals, the pharmaceutical companies should submit the applications to the HIRA on a voluntary basis. Afterwards the Drug Benefit Coverage Assessment Committee (DBCAC) in the HIRA assesses the appropriateness of the reimbursement of new drugs within 150 days and the National Health Insurance Corporation (NHIC) determines the upper limit price of new drugs through
Table 2. Comparison of drug pricing scheme before and after positive listing system
Before 2007 After 2007
Figure 3. Th e reform of drug pricing system from 2012

GLOBAL FORUM | V
OL
4
IS
SU
E 5
20
gfgf
the manufacturers (or importers) that they can request pre-submission consulting services regarding evaluation methods and process prior to submitting their assessment application.
ACHIEVEMENTS AND CURRENT ISSUES
Since 2007, the recommendation rate of new drugs by the HIRA is about 73%. The rejection was mainly due to the obscure/unacceptable cost effectiveness. The HIRA is delisting the drugs which are neither produced nor claimed for 2 years from the drug reimbursement list. Through various kinds of efforts, the number of listed drugs has been decreased from 20,775 in 2007 to 13,814 in 2012. Our organization, the HIRA, has been making an effort for the settlement of the positive listing system. For instance, the HIRA has developed assessment and submission guidelines for cost-effectiveness, indirect comparison and provided disclosure of the drug assessment results in our homepage (www.hira.or.kr). However, there are several issues that we need to work on in the future. That is value-based pricing which is addressed by the pharmaceutical companies, especially in the case of a new drug having difficulties in conducting economic analysis. Nowadays, new policies such as a refund system or risk sharing agreement are being reviewed but deliberate approach to that strategy is needed for the balance between accessibility of drugs for patients and sustainability of reimbursement system.
References/citations from this article are available upon request.
financial impacts, reimbursement status and pricing in foreign countries for the determination of the pharmaceutical reimbursement (Figure 5). For the harmonious communication with pharmaceutical company, HIRA gives the opportunity to
NHIC can conduct the negotiation process with the company without data proving cost-effectiveness. In most cases, the HIRA considers clinical usefulness, cost-effectiveness, disease severity,
Figure 4. Drug Listing Procedure
Figure 5. Pharmaceutical evaluation process
21
A BRIEF HISTORY OF TIME
From a reimbursement perspective, Canada has long been seen as one of the more challenging environments in which to achieve product funding. As an “early HTA” country, economic evaluations became part of the decision making framework for government funded drug programs in the early 1990’s along with other countries like Australia. This explicit approach to assessing a product’s value is the foundation upon which recent developments have occurred in the area of reimbursement.
RECENT DEVELOPMENTS
1) Risk Sharing Agreements1,2
Also known as managed entry agreements, product listing agreements, or performance- or value-based reimbursement
schemes, all are intended as tools for managing the uncertainty (i.e., clinical, economic, health-related quality of life) associated with funding of new products. In the Canadian context financial agreements have predominated in many parts of the country, with little to no attention being paid to the clinical/health outcome side of the equation. From both a public policy and an industry perspective, this focus on financials is short-sighted. It does not address the fundamental question of whether a product really performed or brought value to the health care system as anticipated. In addition, it shifts the discussion away from the core principles of data-driven decision making and, thus, undermines the value of future innovative products.
JUDITH
GLENNIE
Pres ident of J.L. G lenn ie Consu l t ing Inc. and a former DIA Board member (2001-2003, 2008-2011). She can be reached by emai l at jud i th_g lenn [email protected] ibn.com or by phone at 905-726-5846.
Th e Payer/Reimbursement Environment in Canada:
Current and Future

GLOBAL FORUM | V
OL
4
IS
SU
E 5
22
gfgf
procedures that were a first for the Canadian environment. Under pCODR the intent is to make public the vast majority of information provided by stakeholders (with some caveats), as part of their commitment to transparency of the evidence evaluation process. This is aligned to the approach of some major regulators (i.e., FDA, EMA) and HTA bodies (NICE). It is, however, a major adjustment for Canadian industry and it will be important to monitor progress to ensure that there are no unintended impacts.
IMPLICATIONS FOR DRUG DEVELOPMENT
The need for understanding payer-related data needs as a cornerstone of drug development has never been clearer. International efforts are underway to create means of communicating these needs, with some being driven by those in HTA (e.g., HTAi Green Park Collaborative)11 while others have evolved from regulatory-industry discussions (e.g., European Healthcare Innovation Leadership Network)12. In the Canadian context, the challenge is in obtaining “real” payer input, as opposed to that of intermediaries (i.e., CADTH, pCODR), who do not have the same accountabilities and/or priorities. Ultimately, evolution in the approaches to both early and late-stage development (i.e., Phase IV and CED-type approaches) will be necessary - to address payer needs to ensure that funded products provide good value to the system, and to ensure value from a patient perspective.
References/citations from this article are available upon request.
While all 3 input processes underwent program evaluation in 2011, results have yet to be made public.
3) pCODR
Last year (2011) saw the introduction of a national oncology drug review process, separate from the CDR process whose focus is non-oncology pharmaceuticals.9 As with the CDR, the pan-Canadian Oncology Drug Review (pCODR)10 is intended to bring consistency and clarity to the clinical and cost-effectiveness evidence review process, to provide individual jurisdictions and agencies with an analysis that facilitates their final drug funding decisions.
The creation of a separate agency for oncology sets an important precedent, with de facto recognition of a need for different approaches to evaluate evidence for oncology products. Clinical expertise is front and centre in the pCODR process, proving that it is possible to work around issues of perceived conflict in order to get clinical expert engagement.
As with the agencies noted above, pCODR has also introduced a patient input process. Theirs stands out, however, in that patient input is sought both at the front end (to inform the process) as well in response to the initial recommendation. In addition, how patient input has been incorporated into the review recommendations is much clearer. These reflect the distinctively constructive and collaborative approach that has been taken throughout the launch of pCODR.
With the introduction of pCODR came a distinct shift in disclosure
One exception to this was the introduction of the Evidence Building Program (EBP)3 for oncology products in Ontario, a program founded in the principles of coverage with evidence development.4 The EBP is a pilot program which seeks to resolve uncertainty around clinical- and cost-effectiveness data related to the expansion of cancer-drug coverage. Funding is provided for a fixed period to allow the collection of real-world data about a product’s clinical and cost-effectiveness, to help inform a final funding decision. While concerns of complexity and expertise are very real, good policy would dictate that payers should push for performance-based agreements when relevant to addressing the data issues that form the foundation of their decision-making frameworks.
2) Patient Input Processes
In contrast to the EU and UK, the move towards patient engagement in various aspects of pharmaceutical policy in Canada has been slow. In 2010, the Canadian Agency for Drugs and Technology and Health (CADTH) introduced a patient group input process for drugs being evaluated under the Common Drug Review (CDR) process.5 The provinces of Ontario6 and British Columbia7 followed suit in the same year. The level of patient engagement in the design, execution and evaluation of these processes has paled in comparison to the very comprehensive and inclusive approach taken by the Patient-Centered Outcomes Research Institute (PCORI)8 in the US. Patient groups have expressed particular concern related to how their input is being used as part of the evidence evaluation process.

23
Headquarters Hosts First DIA Residents’ DayTh irteen Residents from the University of the Sciences, Philadelphia (PA), and fi ve Residents from Janssen Biotech in Horsham (PA), attended the fi rst “DIA Residents Day” with a visit to DIA Worldwide Headquarters on August 20, 2012. Susan Cantrell, Director DIA North America, presented an Overview of Careers in the Pharmaceutical Industry, while other sessions provided Residents with information about DIA’s history, meetings, trainings, publications and future opportunities to participate.

ADVISEADVISE gfgf
25
What To Do if You Expect to Be Audited
There are few things that create greater consternation than learning that you are going to be audited, yet it’s a common occurrence. Common because the ethical pharmaceutical industry has the responsibility to design, manufacture and market its products according to the highest standards. Unfortunately, those standards all too often remain unmet. We routinely read in the news about pharmaceutical companies being fined for non-compliance1.
BACKGROUND
Companies can minimize, if not avoid, compliance problems by developing clearly defined processes and compliance standards for its R&D, manufacturing and promotional processes. These ‘defined processes and standards’
include national and international regulations, industry codes, and company policies. However, simply establishing compliance policies, processes, and standards isn’t enough. We have the responsibility to monitor and evaluate these processes and internal controls to ensure that requirements are being met and that controls are adequate to mitigate potential risks. Enter the audit.
There are three types of audit that you may undergo: internal audits, audits by regulatory authorities, and/ or audits by an industry association. The differences:
An internal audit is primarily used to confirm adherence to company policies. These policies should incorporate regulatory and industry requirements.
JOSEPH
MCMILLIAN
KIMBERLY
BROWN

GLOBAL FORUM | V
OL
4
IS
SU
E 5
26
gfgf
When you learn of an impending audit, you should review your policies and procedures to see if they agree with current practice. Often SOPs are written in accordance with policy and distributed. As time passes, changes are implemented to improve the process – without changing the corresponding policies and/or SOPs and providing sufficient communication about the changes to appropriate personnel. The first thing an auditor will do is check the date of the document(s) last review and then compare your SOPs to actual practice. If she/he sees any variance, it becomes a prompt to look deeper into procedures and documentation to see what other requirements are not being met. It is okay to initiate SOP updates following this review, but be cautious of making fast, sweeping changes to your process in anticipation of the audit. It can lead to confusion and muddled documentation at a time when you least want it. Follow normal change control procedures. The auditor will adapt to the changes.
When scheduling the audit the auditor should give sufficient advance notice and should be reasonably flexible in scheduling times that cause the least amount of disruption to your business processes.
When planning for the audit, you should be prepared to provide the following to the auditor:
An overview of your area of the business.
An organization chart for your site and related job descriptions.
The site’s office hours and dress code. It is reasonable to expect
A clearly defined process and documented procedures for the pharmaceutical process in question3. These SOPs become the template for site personnel to follow. Be sure that the SOPs are readily available to everyone involved with the process, and that employees are trained on the requirements and evidence of that training is readily available for review. Training alone is not assurance that employees understand the defined process. The last part of the preceding sentence isn’t as silly as it sounds. All too often personnel misunderstand or misinterpret information they were given in training, which could result in compliance failures increasing risk to the business.
There should be an established process for regular document review, updating and communication of any changes. Each policy or SOP should have a clear owner and be version controlled.
Sufficient personnel to execute requirements within time frames defined by corporate policy and required by local regulatory agencies. This often becomes problematic in times of budgetary constraints, however the business is still accountable to provide a quality product within a highly regulated industry. Internal controls cannot be compromised. Shortcuts in process and procedures increases risk to the business and the consumer.
Organized archive files with sufficient documentation (evidence) to prove that corporate policy, local SOPs and regulatory requirements are being met.
Regulatory agency audits are intended to ensure that the company is meeting regulatory requirements in the country in which the product will be used. These requirements should be reflected within local Standard Operating Procedures (SOPs).
Industry requirements can be rigorous. In some countries, trade associations2 issue codes of conduct to member companies, and may, if conditions warrant, conduct audits to see if the company is following the code. These requirements should also be reflected within local SOPs or work guidance documents which provide additional information to supplement SOPs.
Standards for audits generally fall into one of four categories:
Regulatory requirements for the country in which the product is studied, manufactured, or used.
The Company’s policies.
Company-wide standards and/or SOPs [not all companies have these].
Local SOPs and, in some locations, work guidance documents.
PREPARING FOR AN AUDIT
Now that we’ve discussed the reasons for an audit, the types of audit you may undergo, and the criteria that an auditor will likely use, let’s discuss how to prepare.
Regardless of whether or not you expect to be audited, there are several things that you should already have in place:

27
As noted above, standards generally fall into four categories: regulatory requirements, the company’s policies, company-wide global standards/SOPs (if applicable), and/or local SOPs. Two of these, regulatory requirements and SOPs, provide the primary audit standards used by the auditor.
Depending on the type of audit, the auditor will examine the information you provide in:
Websites (usually for labeling and advertising and promotional audits), comparing the product marketing authorizations to promotional claims and disclaimers.
Review and approval evidence specific to the process under review to verify the process is in accordance with related policies or procedures.
Appropriate and timely submissions to the relevant regulatory agencies. Local approved labeling (for labeling and pharmacovigilance audits), comparing at least the Contraindications, Warnings, Precautions, and Adverse Reactions and Interactions sections to the marketing authorization and the company’s core reference document.
Local advertising/promotional materials (for audits of marketing and sales programs), comparing the materials to locally approved product labeling / marketing authorizations.
Toxicology and clinical study records, comparing the records to study protocols and pre-clinical and clinical regulations in the countries in which the drug
THE AUDIT
During the audit the auditor will, hopefully, use objective/established standards to assess your processes. We say ‘hopefully’ because an inexperienced auditor will often base assessments on personal opinion. Even though this is a bad approach, they often get away with it because people are reluctant to disagree with an auditor. This approach undermines the credibility of the auditor and the audit. When formulating recommendations during an audit, the auditor’s assessment of whether or not controls are effective and working as intended should be based upon objective, clearly defined standards.
If you feel the standards aren’t objective, you should raise the issue for discussion with the auditor before the audit is finalized and the report issued. If you disagree with the auditor on an audit assessment, raise the issue with the auditor. As the auditee you have an obligation to ensure the findings are factual and the obligation to take remedial actions. One of the worst things that can happen is for you to agree to a finding or to agree to take an action, just to get rid of the auditor. This type of response will back fire when the audit is followed up and will reflect poorly on you for not completing the actions, or for later admitting you really didn’t agree. Either way, once the audit is completed and findings and related corrective actions are agreed to, you have an obligation to take action. If resolution isn’t reached, you should notify your management that you feel the assessment is inaccurate. Again, you should do so at the earliest opportunity and certainly before the audit report is finalized.
the auditor to conduct the audit within your normal working hours and specific dress code.
Someone to act as a liaison with the auditor, and if necessary, to provide translation assistance. In some instances, an outsourced partner will accompany the audit team to provide the translation service.
A summary of legal requirements in your country, or geographic areas of responsibility.
A space to work. It needn’t be extensive, but should be relatively private to accommodate conference calls and sufficient space to arrange documents, procedures, other work related materials, and access to the internet.
Your policies and SOP(s) for the process(es) being audited.
The associated training documentation.
Associated process documentation and any other document requests identified in the audit notification.
If an internal auditor, copies of previous internal and external audits. If an external auditor (usually a regulatory agency), you should only provide copies of previous audits by the inspecting agency if requested. The external auditor may ask for internal audit reports but will usually respect the confidentiality of internal audits. If they insist, it’s time to consider contacting your legal department for guidance.
Documentation that issues identified during previous audits have been corrected.

GLOBAL FORUM | V
OL
4
IS
SU
E 5
28
gfgf
so years of auditing experience, fewer than 5% of the initial audits that we conducted were without recommendations. However, the personnel who diligently followed up on recommended actions had few, if any, corrective actions in follow-up audits.
Second, take corrective actions where indicated. Unidentified issues of non-compliance are a problem. If they have been identified and not corrected, they are a bigger problem. Most of the significant regulatory actions and regulatory fines we have seen involved audit findings that were discussed and agreed to with the auditee, established corrective action plan(s) and then the auditee failed to complete the corrective action. Once issues have been identified, they need to be corrected in a timely manner. The definition of ‘timely’ can be contentious, so be prepared to defend the length of time you take to correct each of the identified issues. At the same time, propose a reasonable length of time to secure an appropriate (and successfully implemented) corrective action. If you are not able to implement the corrective action within the agreed upon timeframe, be proactive and formally request an extension.
Finally, notify the auditor and those members of management who were copied on the audit report when all corrective actions have been completed. Any time you say that corrective actions are complete, be prepared to provide details including the person or persons who facilitated the corrective action, what was done, and when completed. Only when all corrective actions for open findings have been completed will the audit be considered “closed.”
General governance processes (Operations, Information Systems) that would include risk identification and mitigation processes.
At the conclusion of the audit, it’s usual for the auditor to provide a summary of audit findings, typically in an audit close meeting. This is an opportunity to be sure that you understand each of his/her assessments and provide comments to correct any misunderstandings– before the audit report is issued. It’s also an opportunity to clarify any misconceptions about your processes or procedures as reflected in the text of the finding. But any requested changes should be based on factual accuracy.
AFTER THE AUDIT
Follow up actions to an audit are surprisingly simple.
First, look at the results of the audit as an opportunity to improve your processes. That’s the purpose of an audit. In the 30 or
is studied, and the countries of intended use.
Supplementary marketing programs (including sales training, product sales details to health care professionals, drug sampling, hospitality/entertainment, conventions, grants, donations, publications, digital and web-based initiatives and educational support), comparing these activities to local regulations and industry codes governing these activities. Other elements that could be considered within this review would include third party agreements, master services agreements, Statement of Work documents, financial controls, financial reporting and privacy laws.
Package inserts / SmPC4 documents (for manufacturing audits), comparing these materials to locally approved labeling, and the requirements for current marketing authorizations.
Read Your Global Forum
on the GO

29
References/citations from this article are available upon request.
COMPANY FINE DATE
Total $11.6436 Billion
Above are the details for the summary of promotional fi nes given in the page one footnote. Source: a Google search.
Joseph McMillian, BS, MA, has extensive expe-rience in the pharmaceutical industry. McMillian spent 9 years with American Hospital Supply in sales and sales management and 21 years with Aventis Pharma in sales, professional educa-tion, scientific communications, and regulatory compliance. Since 1989, he has been heavily involved in international auditing of adverse event reporting, labeling, advertising and promotion, and privacy. In 2000, he joined Wyeth Pharma-ceuticals to develop a labeling, advertising/pro-motion, pharmacovigilance, and privacy compli-ance function.
In May 2008, he retired from Wyeth as Assistant Vice President, Global Business Compliance, Global Compliance Auditing Division. Since then he has been mostly retired, with occasional con-sulting projects.
Kimberly A. Brown, BS, MSM, has over 26 years experience within the pharmaceutical industry. Brown spent over 24 years with Wyeth Pharmaceuticals working in different capacities within the Medical Affairs, Legal, Marketing and Sales Operations departments with her last 5 years of tenure as an Audit Manager in Global Compliance Auditing. Since 2010, she has been an Audit Leader at AstraZeneca within Group Internal Audit providing independent assurance to the Board and the Audit Committee.
Robert Quinty, BS, MBA, was a co-author on the article that appeared in the August issue entitled,”An Auditor’s View of SOPs” and his name was omitted from the author bylines. He has had extensive pharmaceutical industry expe-rience during his career with Wyeth Pharmaceu-ticals as an analytical medicinal chemist, a re-search supervisor and then in Regulatory Affairs and the Global Compliance Auditing Division. His areas of expertise include the global and local processes and activities for pharmacovigilance, labeling, marketing/promotional programs, and employee/clinical trial privacy. Since January 2012, Quinty has been working as a private con-sultant in the pharmaceutical industry.

GLOBAL FORUM | V
OL
4
IS
SU
E 5
30
gfgf
Following is a summary of the DIA Cloud Computing Teleconference sponsored jointly by the Validation and IT SIACs on July 7, 2011. It was felt that even though it was one year ago that the teleconference was held, this summary is useful, and the information still current.
After the Future of Cloud Computing, is a suggested list of “Next Steps” to be addressed with future meetings, teleconferences, publications, or training sessions.
WHAT IS CLOUD COMPUTING?
Two extremes
1. Dumb Terminal accessing a computing facility.
2. PC accessing a Computing facility but only for communications.
Assume you have a laptop or desktop PC and you are accessing your corporate computer facility. Some computing operations will be performed on your laptop and others will be executed on the corporate facility.
For example, you would do word processing on Microsoft Word where Word is stored on your laptop. If you had a system for entering data from a clinical trial, each site in the trial might have a
R. L.
CHAMBERLAIN
PhD, Chair Val idat ion SIAC
PAMELA
CAMPBELL
MBA,Chair IT SIAC
THE CLOUDTeleconference Summary

31
copy of the software on their local computer where they enter the data as they see patients and then periodically, perhaps daily, the data is transferred to a database to be joined with data from other patients.
An alternative might be to have Word on one (or more) of the servers in the corporate facility and then each user has a program on their laptop that makes the server think they are logged directly into the server. In this example, the software on the PC would be operating as a “Browser.”
In the case where the clinical trial data is being entered, there could be just one copy of the entry system on the corporate facility and then all of the sites would access that version and the data would go directly into one database.
The corporate facility in this case might be considered a private “cloud.”
The idea is to setup the computer resource “as a service.” That is, you are buying a computer “service” instead of buying hardware, software, and hiring a staff to run the hardware and software. This also potentially means you can buy only what you use or need.
If you have access to a cloud, one of the things you will have to do is make a decision as to how your applications are distributed between your own computer and the cloud. That is, do you keep the software on your laptop but put all of the data on the cloud?
Do you put all of the application on the cloud so you can access your application from any
computer that has the appropriate browser? Or, presumably, some combination of the two.
This introduces the notion of using the cloud “as a service.” There are three versions of this:
Software as a service – Everything is on the cloud
Platform as a service – Applications are placed on the cloud using some cloud software
Infrastructure as a service – The cloud is just used as a utility
Access to the cloud could also be controlled. This leads to different ways to make the cloud available. There are four ways to do this; through a Private Cloud, Community Cloud, Public Cloud, or Hybrid Cloud.
THE FOLLOWING ARE DEFINITIONS OF THESE TERMS FROM THE NATIONAL INSTITUTE OF STANDARDS AND TECHNOLOGY(NIST)
Cloud Software as a Service (SaaS). The capability provided to the consumer is to use the provider’s applications running on a cloud infrastructure. The applications are accessible from various client devices through a thin client interface such as a web browser (e.g., web-based email). The consumer does not manage or control the underlying cloud infrastructure including network, servers, operating systems, storage, or even individual application capabilities, with the possible exception of limited user-specific application configuration settings.
Cloud Platform as a Service (PaaS). The capability provided to the consumer is to deploy onto the cloud infrastructure consumer-
created or acquired applications created using programming languages and tools supported by the provider. The consumer does not manage or control the underlying cloud infrastructure including network, servers, operating systems, or storage, but has control over the deployed applications and possibly application hosting environment configurations.
Cloud Infrastructure as a Service (IaaS). The capability provided to the consumer is to provision processing, storage, networks, and other fundamental computing resources where the consumer is able to deploy and run arbitrary software, which can include operating systems and applications. The consumer does not manage or control the underlying cloud infrastructure but has control over operating systems, storage, deployed applications, and possibly limited control of select networking components (e.g., host firewalls).
DEPLOYMENT MODELS
Private cloud. The cloud infrastructure is operated solely for an organization. It may be managed by the organization or a third party and may exist on premise or off premise.
Community cloud. The cloud infrastructure is shared by several organizations and supports a specific community that has shared concerns (e.g., mission, security requirements, policy, and compliance considerations). It may be managed by the organizations or a third party and may exist on premise or off premise.
Public cloud. The cloud infrastructure is made available to the general public or a large

GLOBAL FORUM | V
OL
4
IS
SU
E 5
32
gfgf
provider?
How will e-record time stamping be handled?
More Compliance Issues
Validation/Part 11 criteria for the cloud environment
Validation/Part 11 criteria for client applications hosted in the cloud
Maintenance of validation for the provider’s cloud and the client’s application
Security/access controls for provider’s cloud and client’s applications
THE FUTURE OF CLOUD COMPUTING
We have discussed cloud computing in four different forms when in fact it is more like a continuum. The different forms of cloud will merge as our technology advances. The line between “system” software and “application” software is already often subject to interpretation. More and more our computing technology will appear to do more complex tasks “automatically.” All of those electrons emitting slight amounts of energy as they perform their tasks will continue to operate at the speed of light to do more complex tasks “automatically.”
With the cloud all of our computing technology is “connected.” This is from our own brain, next to our “hand-held” to the largest computer facility anywhere on the world. With Internet and telephone communications it is all connected.
The Service Level Agreement (client/provider contract) will need to be very detailed regarding:
Exactly, what is the intended (regulated) use of the cloud
Exactly, what responsibilities are associated with the intended use of the cloud
Exactly, which party, client or provider, will support each of the defined responsibilities
What is your intended (regulated) use?
Host Record/Data Collection Application
Host Record/Data Manipulation/Modification Application
Records Archival service (special GLP considerations)
Record Back-up service
What are the Compliance Issues?
If hosting an application, how will computerized system validation be handled?
How will the Installation Qualification be handled? Documentation of the Baseline Configuration?
Who will act as the system administrator? Client or Service Provider…or both?
How will change control be handled? Client SOP or Provider SOP….or both?
How will Disaster Recovery be handled? Client SOP or Provider SOP….or both?
In the event of down-time, how will business continuity be handled…by the client…by the
industry group and is owned by an organization selling cloud services.
Hybrid cloud. The cloud infrastructure is a composition of two or more clouds (private, community, or public) that remain unique entities but are bound together by standardized or proprietary technology that enables data and application portability (e.g., cloud bursting for load balancing between clouds).
Of course, regardless of the type of service or deployment model, we still have “Compliance” issues to address. The requirements of Quality, Integrity, Reliability, and Security, all still apply and are the responsibility of the consumer.
THINGS TO CONSIDER WHEN DEALING WITH THE “CLOUD”
Public Clouds are generally shared services, usually grouping multiple clients together on the same physical servers.
Since a client is renting access to a virtual machine, placement of the machine is done to optimize the service provider’s costs.
While some hypervisor may provide for resource capping, others will let a user consume as much as they like if others are not using it – this can give excellent performance, but introduces variability.
Isolation from other users – or even from one’s own instances (anti-collocation) – can increase resiliency, but at a higher cost.

33
A lot of people believe that life is an energy form. There are a lot of different energy forms in our world. We know of light, gravity, heat, and others. The energy forms are invisible and can only be observed when they exert some force on matter. Without matter we would not know energy existed.
The first law of thermodynamics stipulates that energy can neither be created nor destroyed, it simply changes states.
When two humans produce a child, their life energies change the state of some of their energies to produce another life energy. It has taken hundreds of millions of years to have this process evolve into human life.
All of our computer technologies are full of energies. They contain electrical energy as well as light energy. Beside these they are also influenced by gravitational energy, heat energy, and the user’s life energy. With the fairly recent introduction of PDAs, iPods, iPads, call phones, and other hand held tools, these energies are all coming in contact with one another.
Since I (Dick Chamberlain) got my new computer last fall with Windows 7 I have been frustrated by the way it tries to organize my files. I set up my own organization and I use that. About 4 months ago I signed up for the Microsoft Cloud. I have only really used it a couple of times. Well, over the last two months there have been what appear to be 5 random occasions where, when I stored a file, it actually stored it in my structure and not the Windows 7 organization.
TRADITIONAL DATA CENTER PUBLIC CLOUD
Data on dedicated platforms Platform shared with other customers
Location(s) known at all times and relatively static
Location may migrate across geographic boundaries
Hard to scale up or down quickly Scaling up or down in minutes
Expensive Disaster Recovery Cost effective Disaster Recovery
Information Protection through strong boundary protection
Information Protection requires boundary protection PLUS data at rest protection
BENEFITS CHALLENGES
Operational vs. Capital expense Trust and privacy (security) SAS 70 or SSAN16, Encryption
“Pay as you grow” – no, low startup costs
Availability, reliability and scalability
Can store and manage large scale data
Relatively new technology: limited production use, lack of standard
Scale and agility on demand Regulatory and legal issues
Commoditized services handled by 3rd party
How do you deal with multiple clouds?
You can focus on core areas of expertise (application/use)
CLOUD SUMMARY
Service Level Agreements (SLAs)
Access Control
Attention to Data Security
Business Continuity / Recoverability
Provider Financial Stability
Regulatory Compliance
SOME APPROACHES

GLOBAL FORUM | V
OL
4
IS
SU
E 5
34
gfgf
will come alive. This will probably happen over the next few years. It appears that it has already started. Will it evolve into one life form or millions of life forms all maturing at a very fast rate, all because of the cloud?
It might be good for us. Those life forms that are involved with Wii doing exercises will decide that we should all be doing exercises. Our computers will not work if we have not done our exercises.
References/citations from this article are available upon request.
Obviously, a new life form has been generated by changing the state of some of the other energies available.
During this period I was also able to figure out how to add the number of pages to a “footer” in a Word 2010 document. I spent three months of looking at Help, calling friends, and searching the Internet to try and figure out how to do this. Then one day, I repeated a search for “number of pages in a footer” and the message said to insert “Quick Parts,” “Fields,” and “NumPages.”
Now who would think the number of pages in a document is a “Quick Part.” It had to be a new life form evolving. If it matures in thinking like Windows 7, what is the future of civilization in for?
This raises the question of how long will it take this life form to “evolve.” How long will it take other energy forms to change their states into similar life forms on other computers or will they even form on the computers? They may just be in the cloud – or why not both?
Other life forms have taken hundreds of millions of years to evolve, but that is because it took years for them to reproduce which is when they would change states. However, if we look at similar things happening in our electronic world where information and the interaction between various energy forms is happening at the speed of light, what was taking hundreds of millions of years to evolve will take hundreds of days to evolve.
In other words, the cloud will provide the basis for a new life form. Our information technology
The four speakers at the te le-conference were:
Brian Snitzer – IBM
Glenn Watts – MediData Solut ions
Gary Palgon – L ia ison Sys-tems
Harry Huss – Brandywine Compl iance Consul t ing
The ent i re te leconference can be found on the DIA websi te by going to the ConneX page and choosing the Val idat ion SIAC. Both an audio of the ta lks and copies of a l l s l ides are there.
On February 20, 2012 a fo l low-up te leconference was held. The presentat ion inc lud-ed a case study on “Contract-ing Regulated Technology Serv ices in the Cloud.” The s l ides for th is presentat ion are a lso avai lable on ConneX.

35
CLOUD – NEXT STEPS
New England IRB is the premier, AAHRPP-accredited,central IRB, providing quality study review servicesacross North America.
� Single Point of Contact� FastTrack™ Web Portal for secure document exchange
and updates� One-week Protocol Review Turnaround� 24 – 48 Hour Site Review Turnaround
Contact us to discuss your next study.
Your needs are unique.Choose the IRB with the
flexibility to fit your needs,with ethics and integrity.
Learn more
85 Wells Ave | Newton, MA 02459www.neirb.com | [email protected]

GLOBAL FORUM | V
OL
4
IS
SU
E 5
36
gfgf
Each day, millions of patients place their lives in the hands of the nation’s five million healthcare professionals, with the hope that they will receive quality medical care. However, most patients know little more about their doctor’s qualifications than what they may see hanging from an office wall. It is in that most vulnerable of situations—putting their family’s health in another’s hands—that patients typically have to go on faith that their healthcare provider has the professional qualifications and expertise to treat their conditions.
Patient care begins and ends with clinicians. Who these providers are and what skills they possess directly determine the quality of patient care. Medical credentialing is the one procedure that allows patients to confidently place their trust in their healthcare providers’ qualifications. Unfortunately, due to high costs and overwhelming administrative burdens associated with typical paper-based, manual credentialing processes, many healthcare organizations collect and verify provider credentials only once every 2-3 years in order to decide affiliation status. Once affiliation is approved, years may pass before re-examination, during which time that provider may lose his license, fail to renew her malpractice liability insurance,
or experience disciplinary actions. This inefficiency and inaccuracy is directly related to the heavily manual nature of current standard credentialing processes and adversely impacts patient safety and risk to the healthcare organization.
THE CURRENT STATE OF AFFAIRS: A MANUAL CREDENTIALING PROCESS
Generally, the credentials process starts with the attempt to acquire provider information, typically through various paper applications. Initial information is then checked for completeness, often requiring manual follow-up with the provider to complete the application. The information must then be verified against approved “primary” sources, a step which typically lasts several months and requires a flurry of letter writing, faxing and manual web searching to find and record verification results. The length of time it takes to manually verify these elements also often results in the expirations of other verified credentials, requiring duplicate efforts to re-collect and verify renewed credentials.
Once verification is complete, collected information is manually entered into available database systems and compiled into printed verified profiles for committee review. To further complicate the issue, most organizations have
MATT
HADDAD
i s pres ident and CEO of Medversant. As a heal th-care industry consul tant , Mr. Haddad has arranged f inancing and prov ided in-ter im manage-ment to acute care fac i l i t ies, sk i l led nurs ing fac i l i t ies, psy-chiatr ic care fac i l i t ies and ass isted l iv ing centers. He is a lso a pat-ent holder of Medversant’s AutoVer i f i™ technology.
Electronic Credentialing and Quality Management

37
of avoiding audit issues. How much could be accomplished if such information were not only efficiently collected and processed but easily available? Quality care is found at the crossroad between clinical care data and provider information – only a move toward comprehensive integration of real-time provider credentials will ensure the industry-wide safety of true provider quality.
THE FUTURE: THE END OF MANUAL CREDENTIALING SILOS
Centralized electronic credentialing will become the dominant credentialing process within the healthcare industry, ultimately replacing credentials processing activities by individual healthcare organizations. The truth is that single healthcare organizations simply do not have the ability to invest and maintain sophisticated electronic credentialing platforms. While today, the vast majority of healthcare organizations perform credentialing on their own, in the future this process will be handled by centralized service bureaus utilizing electronic credentialing methods. Moreover, credentials will be checked continuously and results captured and reported on in real time. This paradigm shift will mean healthcare providers will spend a fraction of the time on credentialing, healthcare organizations will be proactively alerted to issues before they become liabilities, and patients will be empowered with real-time knowledge that results in a better quality of care.
References/citations from this article are available upon request.
information, (2) a centralized provider data repository, (3) automated electronic verification of provider information, and (4) integration of provider information to upstream and downstream systems. Additionally, not only does electronic credentialing improve efficiency and eliminate error, it lays the foundation for expanding the scope of what can be collected and processed efficiently such as quality information necessary for pay-for-performance programs, ongoing practice evaluation and other required skills assessments for the industry’s changing needs.
THE NEED FOR CHANGE
With an understanding of the capabilities and opportunities inherent to electronic credentialing, the question remains: why are these paper-based, manual processes still the norm? Part of the reason is that for years, healthcare organizations were advised to remain ignorant of their providers’ backgrounds by legal counsel seeking to protect their clients from respondeat superior liability. However, in most jurisdictions it has now been firmly established that healthcare organizations have a legally enforceable duty to know the exact quality and background of their providers.
In addition, it seems to be a general truth that the healthcare industry has not yet realized the importance of provider information in the efficient management of patient care. While other industries recognize “intellectual capital” as one of the most important assets of a business, the US healthcare industry places virtually no value on the personnel information it collects other than for the purpose
separate database systems for credentialing, billing, HR, etc., often leading to duplicative efforts and the creation of multiple discrepant provider records. During this entire process, which can last as long as six months, the provider receives no information about their application status. To make matters worse, this process is repeated by every healthcare organization with which the provider is affiliated. Suddenly, the burden of these inefficient processes becomes nearly unbearable.
While current credentialing methods may seem merely insufficient today, they are completely unequipped to handle the much larger crisis that is looming. In coming years, a wave of new providers may be needed to accommodate a patient pool that is expected to swell with 30 million more newly insured Americans1 should healthcare reform be implemented. Healthcare organizations will be unable to keep pace with the increased numbers of providers coupled with the need to ensure quality care. To meet these challenges head-on, healthcare organizations must move away from current credentialing models and embrace new tools that allow real-time data collection and verification which meet the need for constant quality assurance today and in the future. The answer is electronic credentialing.
WHAT IS ELECTRONIC CREDENTIALING?
Electronic credentialing involves several features which change the paradigm for how credentialing has been performed. These features include (1) a provider portal allowing real-time electronic submission of provider

REACHREACH
REACH
gfgf

39
DIA 2012: Call to Meta-Collaborate
NORTH AMERICA
One of several DIA 2012 sessions that centered on the 48th Annual Meeting program theme “Collaborate to Innovate,” Meta-Collaborations: A Call to Action (Session 208) convened a panel discussion across the medical and healthcare spectrums to discuss different types of collaborations, and the challenges and benefits they present to patients and industry. This panel was moderated by Freda Lewis-Hall, MD, and introduced by Annual Meeting Program Chair Craig H. Lipset (both from Pfizer, Inc.).
Few would argue that collaboration is not valuable, Craig said. But how do we get more out of collaboration? Do we need more collaboration, or bigger ones, or smaller, or…? “This particular session is near and dear to this theme,” he noted.
Dr. Lewis-Hall began the discussion by recounting her recent conversation with a cab driver who engaged her in talk en route and, upon learning her vocation, asked why people like her kept medicines away from people like him. “Despite the fact that we are bringing cures forward, we’re not bringing
“Th e DIA panel that I participated in was the best session I have ever been a part of.”
GLOBAL FORUM | V
OL
4
IS
SU
E 5
40
gfgf
(NIH), provides a great example of successful collaboration between industry, patient and regulatory stakeholders, she explained. Dr. Lewis-Hall then introduced and invited the panelists to share their thoughts on the fruits of, and barriers to, successful collaboration.
Peter C. Adamson, MD (Children’s Hospital of Philadelphia), introduced the Hospital’s Children’s Oncology Group (COG), which has grown to
encompass more than 200 clinical sites around the world and which he serves as chair, as another example of successful meta-collaboration. The COG and predecessor organizations have helped power an increased number of children’s oncology treatments. What has their experience taught them?
The pace of discovery is much more rapid now, he explained – so rapid that it’s challenging existing scientific, clinical and regulatory models. These discoveries are showing us that childhood cancer is really a patchwork of
enough of them and we’re not bringing them fast enough,” she said. “What can we do to ensure that we meet the medical needs of the most enormous ‘age wave’ of our time?”
The moderator presented her own definition of meta-collaboration: “All hands on deck, with a specific notion and a plan.” Repurposing (“rescuing”) dormant compounds from industry storehouses for clinical evaluation as potential orphan products, championed by the National Institutes of Health
Session Chair Dr. Freda Lewis-Hall
Dr. Peter C. Adamson
“Meta-Collaborations: Call to Action” Discussion Panel

41
different diseases that create even smaller pediatric subset populations. He also noted that the push for cancer therapeutics had previously been driven by the National Cancer Institute and related organizations, but is now being driven by economically-incentivized industry. “Some of the keys to success are when people recognize that the total is greater than the sum of its parts,” Dr. Adamson concluded. “So, meta-collaborations have to be structured so that people can see the short-term and long-term value of these collaborations.”
“People are kind of expecting that collaboration will reap immediate benefits,” cautioned Margaret Anderson, MS, who spoke on behalf of FasterCures, which works to “speed up the time it takes to get important new medicines from discovery to patients.” But, she asked, where are the collaborations to help us face the patent cliff, shrinking budgets and other global medical challenges?
Margaret cited the Cystic Fibrosis Foundation’s collaboration with Vertex on the first oral treatment for cystic fibrosis, plus similar efforts by the Michael J. Fox Foundation for Parkinson’s disease patients, as specific examples of venture philanthropy as collaboration. “These groups
have become the ‘new darling’ of big pharma,” she explained. “These groups bring what we call ‘passion capital’ to the table.”
Kathy L. Hudson, PhD (NIH) introduced the NIH National Center for Advancing Translational Sciences: “Our goal is to foster collaboration so that the whole is greater than the sum of its parts.” Dr. Hudson referred back to “rescuing” dormant compounds plus the innovative “tissue on a chip” as examples of NIH’s successful collaborative endeavors. “There have been collaborations since the dawn of man,” she reminded everyone. “Basically, every single thing we do is a collaboration.”
“I’m here because the FDA thinks this is critically important,” began Susan McCune, MD (Office of Translational Sciences, CDER), whose presentation summarized ongoing CDER collaborations that have improved the Center’s ability to predict, measure and even improve efficacy: New endpoints for clinical trials in pneumonia and skin infections collaboratively developed with the Biomarkers Consortium, innovative clinical trial designs, and patient-reported outcomes and natural history studies (especially for rare diseases). CDER also participates in private-public partnerships with the Cardiac Safety Research Consortium, the Clinical Trials Transformation Initiative, the International Series Adverse Events Consortium and similar groups.
After their presentations, Dr. Lewis-Hall asked the panel to suggest their single biggest – the most “wicked” – barrier to successful collaboration. “We spend a lot of time and energy on issues that are no value added,” suggested Dr. Adamson. “Let’s lower the barriers to clinical trials that have nothing to do with science.”
Margaret stressed the importance of communication: “You’ve got to be clear on what you want to get done and get everyone to agree to that language.”
“I really do think that intellectual property is the most ‘wicked’ barrier,” offered Dr. Hudson.
DIA/FDA: Revitalizing Pro-ductivity in Drug Develop-ment (#12028),
“Reaching crucial industry leadership, creating new business relationships, and tapping some of the brightest minds in the fi eld are all major attractions to the DIA (Annual Meeting) and are why I will keep coming back.”

GLOBAL FORUM | V
OL
4
IS
SU
E 5
42
gfgf
Turning to shortages, Dr. Wirthumer-Hoche suggested that some businesses may be unable or unwilling to comply with the increased number and complexity of regulatory requirements and simply walk away from manufacturing essential products. Dir 2001/83/EC Art 81, issued in November 2001, protects public health in such circumstances: “The Marketing Authorization Holder for a medicinal product and the distributors of the said medicinal product…shall, within the limits of their responsibilities, ensure appropriate and continuous supplies of that medicinal product…”
In addition, some Member States – Cyprus, for example – present markets so small that some companies don’t bother to apply for marketing authorizations there. Dir 2001/83/EC Art 126a (“the Cyprus clause”) says that if a product is authorized in another Member State, “a Member State may for justified public health reasons authorize the placing on the market of the said medicinal product.”
Dr. Wirthumer-Hoche concluded by summarizing two lessons that regulators in Europe have learned: Regulators must balance the risk of product shortages against the risk of non-compliant products when there are no alternative treatments; and regulatory frameworks must be flexible enough to update marketing authorizations to introduce additional manufacturing sites that will alleviate a potential shortage.
S. Leigh Verbois, PhD (ODSIR, CDER) overviewed current Threats & Vulnerabilities to Supply Chain Security. Dr. Verbois explained
Presented in an industry and regulatory context that continues to grow more global, DIA’s 48th Annual Meeting session Risks to & Securing of Global Supply Chain (Session 324) provided a forum for leadership from Europe and North America to share industry and regulatory efforts that ensure product quality and availability, and combat counterfeit (or falsified) drugs and drug shortages.
“As regulators, we are challenged with what is now, for us, a global supply chain,” noted Session Chair Connie T. Jung, PhD (Office of Compliance/Office of Drug Security, Integrity & Recalls, CDER).
Christa Wirthumer-Hoche, PhD (Austrian Medicinal & Medical Device Agency) delivered the viewpoint from the Compliance
& Inspection Sector in Europe. “Not all products are produced in the EU. That’s totally clear,” she began. While manufacturing globalization introduces new points of vulnerability, importing active substances or finished products from a constantly changing set of global suppliers simultaneously increases the complexity of the supply chain. Counterfeit drugs are one unintended outcome of this complexity. “This is a topic which is worldwide,” Dr. Wirthumer-Hoche allowed. “Unfortunately, it has grown tremendously.”
In response, the EU Directive on Falsified Medicines (Dir 2011/62/EU) directs the creation of a EudraGDP database in which compliant traders, wholesalers or distributors would register; it further directs purchasers to audit their suppliers, and provides more explicit definitions of a trader, wholesaler and distributor. The Directive came into force in July 2011; EU Member States must start applying its measures in January 2013.
DIA 2012: Securing the Supply Chain
43
that FDA currently regulates products that come through more than 130,000 importers and 300,000 foreign facilities in more than 150 countries, and that about 40% of finished drug products are imported. “Today, globalization at the FDA means a number of things,” said Dr. Verbois. “What this really means is that there’s no distinction between foreign and domestic products any longer.”
Dr. Verbois then summarized four components of the FDA’s special report on its “Pathway to Global Product Safety & Quality” released in December 2011: Build global coalitions with foreign regulatory counterparts; build global data-information systems that proactively share data; extend risk analytics and intelligence gathering; and leverage the combined interests and efforts of governments, industry and other third parties. This was supplemented by a special FDA report on “Global Engagement” in which FDA Commissioner Dr. Margaret Hamburg wrote: “Today we recognize that to successfully protect US public health, we must think, act and engage globally. Our interests must be broader than simply those within our borders.”
Dr. Verbois concluded by summarizing the basic responsibilities and organization of the FDA Office of Drug Security, Integrity & Recalls, which builds integrity into the supply chain through surveillance/monitoring and other regulatory and enforcement tools, and its collaborative efforts with the Customs Border Protection, Drug Enforcement Agency, Department
of State, Federal Bureau of Investigation and Immigration & Customs Enforcement. One such collaboration was 2011’s Operation Pangea IV, an INTERPOL-led global operation that targeted internet websites supplying illegal or counterfeit drugs, in which more than 80 countries participated. More than 2.4 million counterfeit pills were confiscated, and more than 13,500 websites were shut down, as a result of this operation.
“It’s not only prescription drug products that are being counterfeited,” Dr. Verbois concluded. “Every type of product is vulnerable.”
Special Agent Greg Goneconto from the Office of Criminal Investigations (OCI) discussed Targeting Counterfeit Drugs. Why are we seeing so much increased counterfeit, diversionary, and other criminal activity surrounding medicinal products? “On a gram per gram basis, many drugs are now more expensive than gold,” he explained.
Greg explained that the OCI has about 170 criminal investigators who investigate and enforce drug diversion and counterfeiting issues such as product substitution and tampering, new drug application or clinical investigator fraud, illegal importation, and off-label promotion of drugs and devices. Consumers who continue to buy drugs outside of the legitimate supply chain are also part – a big
part – of these problems. “It was interesting listening to Krista talk because the issues that they’re having in Austria, we’re also having here,” he said.
Greg also referred to 2011’s Operation Pangea and further explained other OCI collaborations with the National Intellectual Property Rights Coordination Center and the Permanent Forum on International Pharmaceutical Crime to help combat drug diversion and counterfeiting.
“What can we do to protect patients from counterfeit drugs? Where can we make the most impact with our limited resources?” he asked. “Without a strong FDA presence, diversion will thrive.”
“We can’t begin to understand the scope of this problem until we understand the supply chain,” Greg concluded.
Read Your Global Forum
on the
GO

GLOBAL FORUM | V
OL
4
IS
SU
E 5
44
gfgf
Dr. Haffner first summarized the “rarity paradigm”: Rare disease patients have an illness which is poorly understood, is often diagnosed late, and are geographically dispersed because their population is so small. “They don’t all live in North America,” she explained. “They don’t all live in the United States. Rare diseases know no borders.”
Dr. Haffner suggested that sponsors interested in developing an orphan drug first check the Office of Orphan Products Development (OOPD) website to see if other products for the same disease are already in development, and also directed attendees to an online FDA “tip sheet” for developing orphan products and submitting your orphan designation application. “You need to clearly define what the disease is,” she explained. “What is this drug and why does it treat only this rare disease?”
Dr. Haffner’s other suggestions for sponsors included involving the OOPD and your review division early in your application process, collaborating with NORD and patient advocacy groups, and ensuring that you understand the patients’ true therapeutic needs. “You will almost always be asked to conduct multi-center if not multi-national trials,” she explained. While clinical trials are simply unfeasible for certain conditions, data from registry or natural history studies can sometimes be submitted in these circumstances.
Rare diseases are a highly diverse collection of disorders, Dr. Haffner concluded, and clinical development programs for products to treat them must
The urgent need for developing orphan drugs, challenges to global orphan drug development, strategies to overcome these challenges, and the pending impact of PDUFA V, were critically
examined at DIA 2012 through Orphan Drug Development: Global Regulatory Challenges & Initiatives (Session 359). “The experts here really know the orphan space and regulations,” enthused Session Chair Kinnari Patel, PharmD, RPh (Bristol-Myers Squibb Company).
She established context for this session by reviewing the FDA’s statement of purpose for
the 1983 Orphan Drug Act: “To stimulate innovation in developing treatments for patients with rare diseases and conditions and to foster the prompt availability of therapeutically superior drugs.” The act primarily provides financial incentives, such as waiving application fees, to accomplish this purpose. For further context, she reminded attendees of the FDA’s definition of a rare (“orphan”) disease – it affects less than 200,000 people in the US – and that there are more than 7,000 rare diseases known to affect more than 25 million Americans. In 2011, 323 requests for orphan drug designation were filed with the FDA, and 192 designations were granted.
Marlene Haffner, MD, MPH (Haffner Associates, LLC) overviewed Current Challenges in the Designation & Development of Orphan Products, while Regulatory Challenges & Initiatives: Strategies for Success was presented by Jonca C. Bull, MD (Novartis Pharmaceuticals Corporation).
DIA 2012: Orphan Drug Development
KINNARI
PATEL
PharmD, RPh,Chair
“Keynote Speaker Dean Kamen was awesome and deeply inspiring!”

45
reflect the disease and population being studied, and the sponsor’s understanding of the proposed intervention and its expected impact on the disease. One size will NOT fit all.
“First and most importantly, there remains a tremendous unmet need,” began Dr. Bull. Over 80% of rare diseases seem genetic in origin – research has defined the genetic basis of more than 2,000 rare diseases – which means they can potentially be identified and impacted in their pediatric stages.
Dr. Bull noted that PDUFA V authorizes hiring more CDER and CBER resources to facilitate communication to sponsors during drug development. “You put some dollars behind the research. That’s always important,” he said.
Dr. Bull turned to development and clinical trial programs for orphan drugs. How can your enterprise translate innovative science into therapies that meet regulatory requirements for marketing? “I think we can all agree that the overall process of drug development is too costly and too long,” Dr. Bull continued. “The other thing that has a huge impact is that things are so much more complex.”
“The principle of orphan drug development is not different: You still need to demonstrate safety and efficacy,” said Dr. Bull. “The process is different.” Dr. Bull noted the importance of the patient and advocacy community in drug development, citing the cystic fibrosis drug developed by Vertex as an example of
successful patient community involvement. “Patients are going to have a much greater voice in benefit/risk,” he suggested.
Dr. Bull concluded with a sobering reality check: What is the capacity of the US health care system to pay for novel therapies that benefit a relatively small population? “Where is the greater public health need served?” he asked.
Timothy R. Coté, MD, MPH (Coté Orphan Consulting; Keck Graduate Institute) delivered Good Words from the Orphanage: Risks, Metrics & PDUFA V. Dr. Coté itemized three kinds of risk in drug development – scientific, management and execution, and regulatory – and focused primarily on its regulatory aspects. Getting the orphan designation is not easy, he allowed. Regulatory hierarchy and its companion statutes, regulations, policies and practices are not always transparent. FDA likes to approve orphan drugs but still requires substantial evidence of safety and effectiveness. “This business of demonstrating substantial evidence of effectiveness is no joke,” he said.
Take advantage of your pre-IND meeting to establish a collaborative relationship with those who, by definition, are always right. “Your pre-IND meeting is your opportunity to take advantage of that invitation – ‘let’s talk,’” he stressed.
Turning to metrics, Dr. Coté cited data that compared the number of trials, the number of patients in trials, and other statistics for orphan and non-orphan products, and then compared clinical development times for orphan and non-orphan products and found they did not significantly differ: The median time in the clinic for both orphan and non-orphan products was 69 months, and the median FDA review time for both orphan and non-orphan products was 14 months.
“PDUFA is the watchword of this conference,” Dr. Coté reminded attendees. “What does PDUFA mean for orphans?” He described PDUFA as the “legislative vehicle” that brings together numerous important, timely initiatives into “a must-pass piece of legislation.” He concluded with a summary review of the new “Breakthrough Therapy” provision of Title VIII, “Drug Regulatory Improvement,” and other Titles of the legislation.

GLOBAL FORUM | V
OL
4
IS
SU
E 5
46
gfgf
crossing over from one theme into another:
Research & Regulation includes trial designs and statistical considerations, endpoint development, natural history studies and working with the FDA
Policy includes the impact of the July 2012 FDA Safety & Innovation Act (FDASIA) on orphan product development, comparative effectiveness research and health technology assessments (CER/HTA), and the role of academic health centers in orphan product development
Special Challenges in Rare Diseases includes access and reimbursement, the internationalization of the rare disease patient community, and new relationships between
DIA will present the second annual US Conference on Rare Diseases & Orphan Products: Shaping the Future Now in partnership with the National Organization for Rare Disorders (NORD) from October 22-24 at the Capitol Hilton in Washington, DC. Patient advocates and industry experts will convene with senior leadership from the FDA and NIH to discuss how to comply with NIH grant and FDA regulatory requirements for investigational new drugs and marketing applications for orphan products to treat rare diseases.
Attendees will be welcomed by NORD President & CEO Peter L. Saltonstall and Dr. Anne R. Pariser (Associate Director for Rare Diseases, Office of New Drugs, CDER, FDA). The conference will explore these topics through sessions organized into three themes, with several sessions
DIA & NORD Team for Rare Disease/Orphan Product Conference

47
patients, industry, FDA and the National Institutes of Health (NIH).
Each day’s plenary sessions will tie back to one of these themes. The closing plenary, What the Future Looks Like for the Rare Disease Patient, is scheduled to feature remarks by Peter Saltonstall, Dr. Janet Woodcock (Director, CDER FDA), Jonathan S. Leff, MBA (Warburg Pincus) and other speakers. In addition, the conference will feature a poster session and tabletop exhibits.
DIA Europe presents an annual rare disease/orphan product conference in partnership with EURORDIS (“The Voice of Rare Disease Patients in Europe”) each spring, to complement this annual DIA-NORD offering each fall.
“It turns out that our ability to break down the human genome helps us to better diagnose conditions, and the more we learn, the more we discover that rare diseases affect a tremendous number of people. Now, we have a better opportunity to understand and treat these diseases.” explains Paul Pomerantz, DIA Worldwide Executive Director. “The ability to address rare diseases has a major impact on the quality of healthcare.”
“The other thing that’s exciting about this meeting is that it really opens up the innovative process to patients as essential stakeholders. In the rare disease realm, patients and patient groups now play an incredibly important role in helping to better understand the science, the types of studies we need, benefit/risk and related issues,” Paul continues. “This meeting is important from a humanitarian
point of view. It’s important from a business point of view, because many companies have identified orphan products as a critical path for their business future. In addition, this meeting helps further the engagement of patients and other stakeholders in the rare disease treatment area.”
This US Conference on Rare Diseases & Orphan Products is also presented in collaboration
with the US FDA, NIH, EURORDIS and the Duke Department of Pediatrics (Duke University School of Medicine).
US Conference on Rare Diseases & Orphan Products
Travel Once, Learn About Rare Diseases Twice and
Save $200!
Register for both events and Save $200!
DIA/NORD’s US Conference on Rare Diseases & Orphan Products: Shaping the Future Now October 22-24 | Washington, DC
Clinical Trial Endpoints: Methods and Practice in Developing Measurements October 25 | Washington, DC

GLOBAL FORUM | V
OL
4
IS
SU
E 5
48
Students' Focus on DIA 2012gfgf

49

GLOBAL FORUM | V
OL
4
IS
SU
E 5
50
gfgf
Rewind to the fall of 2007, when I was a college freshman excited to begin my quest to obtain my Doctor of Pharmacy degree. In my mind, pharmacy was a career path that was expanding but still mainly restricted to
retail, laboratory and hospital settings. As I progressed through school and introductory hands-on experiences in retail and hospital settings, I began to realize that my skill set and interests could paint a much bigger picture. I had the ambition to understand the pathway a product travels from the time of creation to the time it was given to the patient. My expertise in medications could not only affect the surrounding community but affect millions worldwide. And while speaking to numerous established
professionals for career advice, all pointed to the DIA Annual Meeting as an invaluable learning experience and stepping stone to a bright career in pharma.
As the Annual Meeting approached, my St. John’s classmates and I prepared using the technology and literature DIA provided; we found these to be extremely helpful, especially for “first-timers” not knowing what to expect. The communication between DIA and students should be commended for its accuracy and promptness.
Our three-day experience began with the Student Forum, where we not only learned networking techniques but also practiced among ourselves. It was great to see other students who shared similar goals for their own careers. Throughout the next few days we attended sessions that we felt were pertinent to our future careers. I personally found that some material was overwhelming, which is understandable considering I have little experience with the terminology or work environment. However, it was very impressive that the speakers
answered all questions with the same time and respect no matter who asked. In one session, I found myself asking a question directly after the DIA President, and my question received the same respect and response time as his.
Networking is a skill that cannot be perfected without practice, but students do not have many opportunities to practice networking in a professional setting. At DIA 2012, I did more than just practice: I was able to observe people using proper networking techniques throughout the sessions. This was the first time that I had to use business cards, and I now understand how crucial they are for a smooth conversation with a new colleague. I also found the speed networking/orientation session to be very useful in meeting many people as well as a good crash course on how to approach someone. Another small yet extremely useful meeting attribute was the SIAC-specific ribbons. I personally have a goal to become a Medical Science Liaison and the specific green ribbon for the Medical Science Liaison SIAC helped me to identify and ask advice from professionals in this field.
Overview: DIA 2012
STUDENTS REFLECT ON DIA 2012
ASHLYN JOSE
i s a PharmD Candidate at St . John Univers i ty ’s School of Pharmacy & Al l ied Heal th Profess ions.

51
The exhibit hall was a sort of spectacle for a student who has never attended any convention such as this. Although the exhibitors were not particularly looking for students and were more geared to selling their products or services, many of them were willing to help explain what their companies did and potential future opportunities in their company for PharmD professionals such as myself. The number of companies far exceeded my expectations and truly broadened my view beyond the “big name” companies that are always on the news. The SIAC luncheon and ongoing SIAC online communities are also quite valuable to both students and professionals. I look forward to interacting with professionals in my SIAC community to help establish my chosen career path.
The DIA Annual Meeting is something I would highly recommend to anyone even remotely considering a career path in pharma, and I look forward to learning and networking even more in the years to come.
Session Report:DIA 2012 Regulatory
Summit What regulatory collaboration will look like as we go further into the 21st century was a primary focus at the DIA 2012 Annual Meeting, especially throughout Regulatory Collaboration/ 21st Century Innovation: Views of the Heads of Health Canada, the European
Medicines Agency, and the US FDA (Session 139). This panel discussion addressed some upcoming challenges and steps in regulatory cooperation as well various approaches the agencies employ to meet their domestically-focused mission in our increasingly global environment.
In April 2011, Health Canada updated user fees for its human drugs and medical devices
in 14 years, explained Paul Glover, MBA (Assistant Deputy Minister, Health Products & Food Branch, Health Canada). Previous funding
numerous backlogs. Parliament, while approving this new fee structure, made it very clear that this structure came with the companion expectation that Health Canada would do a better job.
Health Canada’s new operating environment is based on three basic priorities: Remain true to the evidence as a science-based regulatory Agency, and invest in
abreast (if not ahead) of an industry that grows increasingly global and complicated; deliver operational excellence; and embrace regulatory modernization in Health Canada’s transformation into an Agency that simultaneously
the interconnected global industry it regulates.
NATALIE
MELAMED
i s a Master’s Candidate in the Cl in ica l Tr ia l Sciences (Regulatory Affa i rs ) pro-gram at the Univers i ty of Medic ine & Dent ist ry of New Jersey.

GLOBAL FORUM | V
OL
4
IS
SU
E 5
52
gfgf
Executive Director of the European Medicines Agency, Dr. Guido Rasi spoke about facing some of these very same challenges such as clinical trials, supply shortages, personalized medicine, counterfeit medicine, and so on. Dr. Rasi used two key words to summarize the future of regulatory cooperation in our increasingly global environment: Trust and Role.
We must trust in each other as regulators, and even more trust is required when dealing with the results of clinical trials conducted in another country. It is clear that trust in regulators and industry have seriously declined. To overcome this decline will require new and improved ways of communication, transparency and even greater levels of industry-regulatory collaboration. Dr. Rasi also referenced the alarming and growing number of people who use unregulated substances because they trust what their neighbors tell them or what they read on the internet more than they trust regulatory or industry expertise. It is paramount that we all work together to restore the trust between consumers, industry and regulators, and thereby truly protect public health and safety.
role in our collaborative future, Dr.
found in answers to such questions as: Are we the gatekeeper or are we the enabler? What is the regulators’ role in comparative effectiveness? Is industry ready to challenge us with other tools to assess their efforts to produce innovation? Addressing these basic principles of trust and role, assured Dr. Rasi, will help move global regulatory collaboration forward.
FDA Commissioner Dr. Margaret Hamburg added another word to Dr. Rasi’s critical terms: Partnership. We live in a world where science is advancing rapidly in an increasingly globalized world. The FDA regulates products that come in whole or in part from more than 300,000 facilities in over 150 countries. At the same time, it is critically important that science remains the single most important tool in our regulatory processes. All these factors combine to demand that regulators are adequately positioned to address the challenges of today, tomorrow and the future.
important part of the foundation we need to introduce the changes that regulatory agencies need to accomplish their mission.
Over the past decade, numerous regulatory authorities have formed partnerships to share information through bilateral and multilateral agreements. They have also worked toward harmonization of standards as well as converging upon ways to approach problems with different international organizations. Even so, we cannot continue to do global work through this patchwork of formal and informal relationships.
the demands of globalization, Dr. Hamburg explained.
Industry, patients, consumers, healthcare providers, media, lawmakers and other critical stakeholders must all work together to advance new ways of thinking
challenges, the panel concluded. These new ways of thinking will
be regulating products that meet
and quality.
Paul Glover of Health Canada, Margaret Hamburg of FDA, and Guido Rasi of EMA discuss regulatory collaboration at DIA 2012.
Read Your Global Forum
on the
GO

53The first in a series of advertising and promotional sessions that spanned Wednesday June 27 at DIA 2012: Collaborate to Innovate, the Prescription Drug Marketing Regulatory Primer (Session 308) introduced the environmental forces and agencies impacting the regulation of prescription drug promotion, applied these advertising and promotional regulations to advertising/marketing materials, and explained the importance of FDA guidances, warning letters and other communications pertinent to these regulatory decisions.
An introductory session on any pharmaceutical or regulatory topic could be a dry listing of rules and regulations, but these presenters took an entirely different approach. Janet “Lucy” Rose, MBA (Lucy Rose and Associates, LLP), energetically encouraged the early morning audience to speak
out and ask questions while she roamed the workshop to share her knowledge and occasionally quiz the audience. This added to the workshop atmosphere. Lucy’s presentation summarized basic definitions which provided foundational knowledge for less experienced participants, and a thorough review for those more experienced in prescription drug advertising and promotion. She included basic information on the organization and structure of government oversight agencies such as the Department of Health & Human Services to the FDA’s individual regulatory review divisions.
Lucy began by discussing regulations in the context of a changing environment. FDA expects that prescription drug promotions be accurate, balance risk and benefit information, be consistent with the prescribing information approved by the FDA, and only include information that is supported by strong evidence from clinical studies, she explained. At the same time, the rapidly evolving world of social media will continue to influence the drug promotion landscape. Social media was a hot topic throughout DIA 2012 and was highlighted in many other sessions.
Next, the discussion turned to focus on the major challenges to determining what is false or misleading in a prescription drug promotion. Two major themes that repeated throughout this and other related sessions were the evaluation of the content and the context of the promotion. Lucy concluded her presentation by offering this advice: The most important thing that participants
Session Report: Prescription Drug Marketing
Regulatory Primer
ELISA L.
PRIEST
just completed her DrPH in Epidemiology at the Univer-s i ty of North Texas School of Publ ic Heal th and is the Manager of Cl in ica l Tr i -a ls at Baylor Heal th Care System in Dal-las, Texas.

GLOBAL FORUM | V
OL
4
IS
SU
E 5
54
gfgf
could do when they returned to their workplaces was to thoroughly read FDA guidance documents and enforcement letters in great detail, because they provide insight into the FDA’s current points of view.
Michael A. Sauers from the FDA Office of Prescription Drug Promotion followed with an excellent presentation that provided additional regulatory details and demonstrated how to apply the concepts from Lucy’s presentation to the real business and regulatory world. He showed examples of print and television advertisements – plus other marketing materials such as websites and patient and physician testimonials – that had resulted in enforcement letters from the FDA.
He gave the audience time to review each example and to identify why the FDA found the promotion in violation. These examples helped to explain to a novice in this field why drug promotions that appear in magazines are often several pages long, and demonstrated the complex nature of drug promotions and the challenges the FDA faces in enforcement. When examining the presentation of risk for a drug, for example, factors including the location, font, spacing, and ordering of the text are important; so are other subtle details, such as the appearance of the models or actors used in the promotion – persons used in promotions must be representative of the target population for the drug. Similarly, patient testimonials or imagery used in a promotion must be consistent with the average experience of the patients for whom the drug is indicated.
Finally, Mr. Sauers discussed the challenges that face the FDA in the review of drug advertising and promotion. Because of the high demand for review of promotional materials, the FDA takes a risk-based approach based on several factors – including the severity of the disease, the newest approved drugs, drug warnings, and intended audience of the promotion – to their review.
This workshop brought the audience together with industry and regulatory experts in the advertising and promotion field, allowing for direct interaction with the FDA. Those attending this morning workshop received a solid introductory foundation in prescription drug advertising and promotion.
As a DIA first-timer and student interested in the pharmaceutical industry, I had expected to attend a session on professional development at some point during the DIA 2012 Annual Meeting. However, little did I know that I would attend a session as a “foreign species” not because I was
a clueless first-timer student but because I am a man. What possessed me to choose My Big Break: Women at the Top in the Biotechnology Sector (Session 147) of all available sessions, since it was obviously geared
towards another audience? Ironically, the lessons and insight I gained from this seminar were ultimately much more profound and impactful than those from other sessions. The topics covered in this session were universal, applicable to both sexes, and reinforced the idea that the trials and tribulations one goes through in the path of professional development are generally the same for men and women.
This session was chaired by C. Latham Mitchel, MD (Erudita Biotechnological, LLC), and featured panelists Leslie Williams, MBA, RN (ImmusanT); Carole Sable, MD (Merck & Co. Inc.); and Yvonne Greenstreet, MD (Pfizer Inc).
The first question asked the panelists what their “big break” was. When I heard this question, I sat up in full attention. You can imagine my curiosity, as a student eagerly waiting for how I might expedite my own “big break.” While I heard commonly
Session Report: “My Big Break”
SLANIX PAUL
T. ALEX
i s a PharmD Candidate at St . John’s Uni-vers i ty Col lege of Pharmacy & Heal th Sci-ences
55
used phrases – always strive for excellence and growth, and never give up – what particularly caught my attention was when one of the panelists simply said that you can work extremely hard and strive for excellence and growth, but at the end of the day luck always plays an immense role. This refreshing, realistic outlook put a whole new perspective on professional development. She advised us that sometimes things don’t go your way, no matter how hard you work; be a smart player in the career game, with a diversified playbook, and learn that you must sometimes move onto another strategy to push forward.
Another piece of particularly profound advice was that everyone’s first “big break” happens when a person discovers their passion and uncompromisingly strives toward it. This involves many things, including going out of your comfort zone to see your passion come to life. While I definitely believe this is true, I also think that one must tie passion to practicality, which goes back to the earlier statement that sometimes things just don’t work out – you may be passionate about something, but you also have to accept failure when it comes and learn to move on. Truly successful people have all failed at some point. It’s how they rose up from that failure that defined them. In this sense, failure may have been their “big break.”
The second topic was the importance of mentorship in career development. What struck me about this conversation was how these women came to realize later which mentors they benefitted from the most.
Every panelist echoed the same sentiment: It wasn’t the person they identified with or opened up to, but rather the person who was critical and expected a lot, who gave them more responsibility than they themselves thought they could handle and took a risk on them. These mentors subtly guide you in the right direction by asking the right questions and letting you make a few mistakes to learn from along the way. The key point was that proper direction from their mentors stretched each panelist beyond their comfort zone; they were forced to adjust and learn on the go, a valuable trait in the pharmaceutical industry.
The session’s final topic centered on the role and importance of gender, especially to women, in the pharmaceutical industry. This topic has particularly fascinated and at the same time confounded me. While much progress has been made in this realm, there is still room for improvement. I think we can all agree that women are just as intelligent and equally qualified. Does this disparity come from something much deeper? Is it cultural or societal? I think of my personal family experiences: I have had conversations with female family members about their career paths, and why they chose to do what they do. Not one decided to go down a scientific or technical path; all chose teaching
or other healthcare fields instead. Is this because women are raised with an imbedded mindset that certain jobs are not feminine? If so, is this mindset based on certain biological and psycho-social perceived norms? It pains me to think that the answers to these questions are yes, since I know many women with brilliant scientific minds who would thrive in the pharmaceutical industry. My only hope is that we can overcome these perceived norms and perhaps even redefine what is feminine.
Overall, this session truly opened my eyes to the struggles that all people, not just women, face as they work to lift themselves to the top of the biotechnology industry. My only hope is that, as we progress into this modern age, the struggles that we face are not based on gender, and we can provide everyone with the same level playing field on which they can draw up their own personal game plans.

GLOBAL FORUM | V
OL
4
IS
SU
E 5
56
gfgf
“The customer is always right” is a common expression followed by many top businesses. The customer has always been seen in the business world as the driving force and ultimate power behind decisions made and policies implemented. However,
in health care – particularly in medical product development – the “customer” has just recently gained a voice in the crucial steps a product takes through the rigorous paths and channels of the FDA. The DIA 2012 Annual Meeting offering Patient Advocacy in Medical Product Development: The Evolving Relationship Between FDA & Its Patient Stakeholders (Session 312) analyzed the steps the FDA is taking to ensure that the patient is an integral aspect of this whole process.
Session chair James E. Valentine, MHS (Office of Special Health Issues, Office of the Commissioner, FDA) began by presenting the background and evolution of connecting the patient to the medical product development process. The OSHI was originally created in the late 1980’s when HIV/AIDS patient protesters shut down the FDA for an entire day with protests so large that no one could move in or out of the building. These patients knew that HIV/AIDS medications were in the process of being reviewed for approval, but had no idea about the regulatory review process or how soon they might receive these medications. There was imminent demand for process transparency and for patients to play a role in making decisions about the drugs they would receive as therapy.
This started the FDA’s patient representative program, which is still around today: The FDA recruits patients and patient advisors to serve on their review committees and has made the patient a key voice in their committee decisions. This patient program has amassed
Session Report: Patient Advocacy in Product
Development
ASHLYN JOSE
i s a PharmD Candidate at St . John Univers i ty ’s School of Pharmacy & Al l ied Heal th Profess ions.
tremendous results, such as the accelerated approval pathway in which patient advocates can voice their opinions and concerns.
As President and CEO of the International Cancer Advocacy Network, Marcia K. Horn has repeatedly worked with patient advocates and regulators. Her presentation continuously commended the FDA for their efforts to put patients first. As researchers come closer each day to finding a product to help cancer patients desperate for a cure, the voice of this patient population is more important than ever. The Agency has even implemented more easy to use paperwork such as single patient NDAs. All future plans point to an Agency that will continue to put patients first.
Patrick Frey (Office of Planning & Analysis, CDER) spoke mainly on the new benefit/risk assessment framework implemented by PDUFA V. This framework was initially developed by assessing previous cases that were labeled as difficult. The responsible review team was asked to identify and categorize how they determined an attribute was a risk or a benefit, and to write short benefit/risk summaries that specifically addressed benefit/risk trade-offs that were made. This benefit/risk analysis framework tells the story of the specific problem, other current potential interventions, the benefit of the proposed intervention and specific concerns to monitor. A major policy change will allow patient information to be assessed earlier in the product development and review/approval paths.
The FDA takes patient advocacy very seriously and will publish a

57
and Paul Litowitz (Therapeutic Products Directorate, Health Canada), our DIA Canadian Annual Meeting is presented in collaboration with BIOTECanada, Canada’s Research-Based Pharmaceutical Companies, the Canadian Association of Professional Regulatory Affairs, and the Clinical Research Association of Canada.
The opening plenary session on November 6 will explore The Big Risks of Today; Forecasts for Tomorrow, and will set the stage for more detailed conversations in subsequent meeting sessions. This plenary will feature Robert Cushman, MD, FRCPC (Director General, Biologics & Genetic Therapies Directorate, Health
DIA’s focus on benefit/risk and its crucial role in drug development and lifecycle management will be discussed at our DIA Canadian Annual Meeting: Evolutions in Risk Thinking in Ottawa, Ontario. The meeting will open on November 5 with tutorials on How to Prepare a New Drug Submission and How to Prepare for a Pharmacovigilance Regulatory Inspection, then proceed through plenary sessions and three meeting tracks – drug development, pharmacovigilance and information technology/communications – that will more comprehensively examine benefit/risk topics on November 6-7.
Co-chaired by Neerja Goyal (GlaxoSmithKline, Inc., Canada)
Canadian Annual Meeting: Evolutions in Risk Th inking
five-year plan to make their review and approval processes more transparent. This plan will include public workshops on twenty disease states open for public comment, one each quarter for five years, which will be invaluable in pinpointing unaddressed aspects of these diseases.
Mr. Marc Boutin, JD (COO of the National Health Council), provided insight regarding the changes that the government has taken to make drug development more patient-oriented. Mr. Boutin defined a “consumer” as an individual who uses the health care system for acute care, and a “patient” as an individual who will use the health care system regularly to manage their quality of life. This difference is crucial because what patients and consumers see as important in the benefit/risk relationship may not be the same. “Ten years from now, everyone will look back on PDUFA V and point to this as the most important part: That no other country has a qualitative framework for benefit versus risk,” Mr. Boutin said. The passing of this legislation, along with its supporting policy changes and actions, will surely be significant for patients, healthcare professionals and regulators. These and other changes have created patient expectations that all government agencies will treat all disease states with equal importance.
As patients become more educated about the drug development process, FDA will continue to transform its culture to a state where the patient is just as important to new therapies as the scientist behind the molecules. As the Agency moves forward, a new
FDA Patient Network program will include a newsletter about recent and upcoming approval decisions, an annual meeting to address patient concerns, and a new
website that will serve patients looking to learn more about their illness plus patients who are more interested in advocacy.

GLOBAL FORUM | V
OL
4
IS
SU
E 5
58
gfgf
Canada); Christine Janus (Canadian Skin Patient Alliance); Neil Maresky, MD (AstraZeneca Canada, Inc.); and Jeffrey Turnbull, CM, MD, MER, FRCPC (Chief of Staff, Ottawa Hospital; President, Canadian Medical Association).
Any discussion of benefit/risk assumes a patient who will either benefit from or be at risk from a proposed therapy, Paul and Neerja suggest, and since patient benefit and safety is at the forefront of healthcare product development, use, regulation and marketing, patient benefit and safety is at the forefront of these three meeting tracks. For example, presenters in the Rare Disease/Orphan Drug session from the drug development track will include Durhane Wong-Reiger, President of the Canadian Organization for Rare Disorders. The IT/communication track includes a session that evaluates the effectiveness of risk communications to patients and their professional caregivers, as well as a session on developing aids to help patients make better benefit/risk decisions about their therapies.
The closing plenary session on November 7 will overview case studies and best practices for Managing Drug Shortages, which Neerja will co-chair with Alice Hui (Therapeutic Products Directorate, Health Canada). Alice and Neerja served as co-Chairs for DIA’s 2011 Canadian Annual Meeting.
In between, Neerja and Paul will co-chair the plenary What Keeps Your Members/Organizations Up at Night? This session will focus on practical ways to compare and
contrast actual and perceived risks, and approaches to overcome key risks that industry and Health Canada currently face. This plenary will feature Ron Boch, PhD (BIOTECanada); Kenneth Hughes, PhD (Canada’s Research Based Pharmaceutical Companies, Rx&D); Barbara J. Sabourin (Director General, Therapeutic Products Directorate, Health Canada); and Julie Tam (Canadian Generic Pharmaceutical Association).
This session came about from program committee discussions about whether the different types of pharmaceutical companies face the same key risks, Neerja and Paul explain. While the pharmaceutical industry is often viewed as one collective entity, it is composed of different types of organizations (biotechs, generics, large pharma, etc.) who face different types of risks; this plenary will lead to greater awareness about the similarities and differences in the risks these different organizations face.
DIA Cana-dian Annual Meeting

59
Clinical pharmacology is a scientific discipline that contributes substantially to the creation and execution of a clinical plan to move compounds from discovery to marketing and beyond. In early phase development, the role of clinical pharmacology is to facilitate the advancement of new molecular entities through proof of confidence. In late phase development, the same discipline is responsible for providing the capability to profile the compound and identify the appropriate patient population for treatment at the right dose, right schedule and right time.
In the early stages of drug development, the role of a clinical pharmacologist is to work with key stakeholders from various disciplines (metabolism and pharmacokinetics, drug safety, pharmaceutics, regulatory,
translational physicians, clinical biomarkers) and create a clinical plan. The plan has to take into account the fundamental properties of the drug molecule such as physicochemical properties, absorption, distribution, metabolism, excretion and toxicology. In early development (Phase 1-2a trials), the main objectives are to select a dose based on preclinical safety and efficacy data; characterize safety, pharmacokinetics (PK) and pharmacodynamics (PD) of the new drug entity and help selection of doses for Phase 2b studies based on integrated data analysis and modeling approaches.
At the forefront of pharmacokinetic characterization of a new drug entity is a validated bioanalytical assay. Pharmacokinetic data is of limited utility if not generated using validated methodology. Several regulatory documents provide guidance for developing a validated method in different matrices, accuracy and precision criteria, single vs. multi-component analysis etc. Similarly, pharmacodynamic characterization requires optimized assays for biomarker development.
The biopharmaceutic properties of a new drug entity govern development of an optimal dosage form and its behavior in vivo. Biopharmaceutic principles provide mechanistic understanding of drug absorption and can aid in understanding the relationship between the physicochemical properties of the drug and release characteristics of the dosage form to in vivo performance. These properties also govern specifications for dissolution conditions,
Role of Clinical Pharmacology in Successful IND and NDA Submissions using Principles
of Pharmacokinetics and Pharmacodynamics
DR. PUNIT
MARATHE
DR. MEHUL
MEHTA

GLOBAL FORUM | V
OL
4
IS
SU
E 5
60
gfgf
requirements for immediate release vs. modified release product and food effect and pH effect on oral exposure. Key dosage forms utilized during drug development need to be bridged to the one that will be marketed with respect to relative bioavailability and bioequivalence. Inter- and intra-subject variability in pharmacokinetics and dosage form performance can make the study design of bioequivalence studies quite complex.
Understanding disposition of the drug candidate in terms of distribution, metabolism and excretion is a major aspect of clinical pharmacology studies. It is also important to characterize the potential of drug candidates to inhibit or induce key enzymes and transporters involved in drug disposition. These studies form the basis of how the drug candidate will behave in the presence of concomitantly administered drugs. Knowledge of enzymes and transporters involved in the disposition of drugs is fundamental for designing clinical pharmacology studies in later phases of drug development. Investigating clinical drug-drug interactions, to characterize the potential of an investigational drug to affect the disposition of a co-administered drug (perpetrator) or vice versa (victim) is also an integral part of drug development and regulatory review. Which drug-drug interaction studies should be included in a clinical pharmacology program is an important aspect of the overall clinical plan. The decision is made based on target effects of the drug candidate (activity on cytokines, steroids etc.), routes of human metabolism and excretion and the need for concomitant
medications. Pharmacokinetic and pharmacodynamic characterization in special populations is crucial from the point of view of appropriate dosing recommendations in the subgroup of patients that may have altered metabolism and excretion pathways. Intrinsic factors such as age, gender, renal vs. hepatic impairment, ethnicity and pregnancy have to be studied for appropriate labeling recommendations in dedicated studies or by applying population pharmacokinetic approaches.
Pharmacogenomics is a new area that holds promise towards rational drug therapy and personalized medicine. It is a study of variations of DNA and RNA characteristics as related to drug response. Pharmacogenetics is a subset of pharmacogenomics and focuses on more targeted analysis of DNA sequence as related to drug response. Phase 1 studies may be designed by the clinical pharmacologist to collect information on pharmacogenomics (with respect to drug metabolism/transport and drug target) as secondary endpoints to enable patient selection and stratification for better drug response with reduced liability due to drug-related adverse events. Pharmacogenomic data is valuable in identifying the basis for PK outliers and inter-subject variability in clinical response; prioritizing drug-drug interaction studies; elucidating the basis of lack of efficacy or adverse reactions and designing trials to test or enrich subgroup effects.
A key component of rational drug development is application of pharmacometric principles. Pharmacometrics is defined as
the science that quantifies drug, disease and trial information to aid efficient drug development, regulatory decisions and rational drug treatment in patients. Pharmacometric analysis allows integration of data from multiple sources and can play a crucial role in biomarker evaluation for early PK-PD readout, demonstration of efficacy and proper assessment of risk vs. benefit.
Assessment of cardiac safety of a new drug has become another standard feature of drug development. The study is conducted in a randomized, blinded, placebo-controlled and active-controlled manner with inclusion of a therapeutic and supra-therapeutic dose. The timing of a thorough QT study and its impact on subsequent drug development are important considerations in the overall clinical pharmacology plan.
Pharmaceutical industry is expanding the scope of drug development from traditional small molecules to more targeted biologics or protein drug candidates. Biologics offer unique challenges based on their PK and PD properties. Some of these challenges include requirement for specialized bioanalytical methods, target-mediated disposition, impact of immunogenicity on PK and PD and requirement of minimal anticipated biologically effective level (MABEL).
In summary, the role of clinical pharmacology is to enable identification of the right dose for the right patient at the right time. It leverages and facilitates integration of knowledge and expertise in multiple functional areas to deliver a package for IND

61
and NDA regulatory submissions. Clinical pharmacology enables drug development through pharmacodynamics, pharmacokinetics, biomarkers and pharmacogenomics; characterizes the in vivo performance of formulations; ensures the cardiac conduction safety of new drugs; informs the need for dose adjustment in specific populations; defines key exposure-response relationships and informs the need for dose adjustment due to co-administration of other medicines. “Using Pharmacokinetic and Pharmacodynamic Principles to Enable IND and NDA Submissions” is a course dedicated towards these concepts and practices.
Mehul Mehta, PhD is the Director, Division of Clinical Pharmacology I (DCP I), Of-f ice of Cl inical Pharmacology, OTS, CDER (Center for Drug Evaluation and Research), FDA. His division is respon-sible for reviewing the cl inical pharmacology (CP) and bio-pharmaceutics (B) aspects of the Cardio-Renal, Neurophar-macological and Psychiatr ic drug products. He received his BSc and MSc in Chem-istry and Synthetic Organic Chemistry from the University of Bombay in 1976 and 1979, MS in Medicinal Chemistry from the University of Houston in 1981 and PhD in Pharma-cokinetics from the University of Pittsburgh in 1986.
Dr. Mehta joined the Divi-sion of Biopharmaceutics, FDA in 1986 as a reviewer, was promoted to the Section Head, Oncology and Pulmo-nary Drug Products, in 1992, to the Deputy Director, DCP I in 1995, and to the Director, DCP I in 1999. In addit ion to his review oversight, admin-istrative, and management responsibi l i t ies, he currently co-chairs the CDER wide BCS (Biopharmaceutics Classif i-cation System) Committee, is member of the FIP BCS SIG, is the Chair of the OCP Working Group for revising the CDER ‘PK in Hepatic Impair-ment’ guidance issued in 2003, and is a member of the CDER 21st Century Review Init iat ive Subcommittee.
Punit Marathe, PhD is a Group Director in the Metabolism and Pharmacokinetics Depart-ment at Bristol-Myers Squibb in Princeton, New Jersey. She has extensive experience in all areas of Drug Metabolism and Pharmacokinetics including drug discovery, lead optimization, preclinical and clinical phar-macokinetic studies leading to product registration and life-cycle management.
Dr. Marathe received her PhD degree in Pharmacokinetics from the Department of Pharmaceu-tics at the University of Wash-ington followed by a postdoctor-al fellowship in the Department of Medicinal Chemistry at the University of Washington. Her current responsibil it ies include collaborating with drug discov-ery for selection, optimization and characterization of lead candidates for development. She is also responsible for an in vivo animal group that con-ducts pharmacokinetic and metabolism studies in support of discovery and development.
Dr. Marathe has worked to establish a greater scientif ic (PK-PD-ADME) presence in India and has been involved in the co-organization of various research-oriented meetings that have fostered partnerships with India-based faculty at different research institutions. She has played a critical leadership role in the optimization of nonclini-cal PK study cycle times and implementation of global sourc-ing in support of nonclinical PK screening. Dr. Marathe has published over 75 publications and external presentations. Her research interests include understanding pharmacokinetic-pharmacodynamic relationships in nonclinical animal models, translation to humans and prediction of human efficacious doses.

GLOBAL FORUM | V
OL
4
IS
SU
E 5
62
gfgf
UPCOMINGEVENTSNORTH AMERICA
“Using Pharmacokinetic and Pharmacodynamic Principles to Enable IND and NDA Submissions” is a course dedicated towards the concepts and practices presented in this article. To learn more, register for this course which is being offered on November 29-30, in Washington, DC.
OTHER COURSES OF INTEREST IN DIA’S REGULATORY CURRICULUM:
Preparing for a US FDA Advisory Committee MeetingOctober 18, 2012 (#12437)Horsham, PA
DIA/FDA Industry PDUFA VOctober 18-19, 2012 (#12013)Washington, DC
European Regulatory Affairs October 22-23, 2012 (#12410)San Diego, CA
Regulatory Affairs for Biologics: The IND and BLA Phases October 22-25, 2012 (#12432)San Diego, CA
Annual Canadian Meeting: Evolutions in Risk ThinkingNovember 6-7, 2012 (#12019)Ottawa, Canada
Regulatory Considerations for Drug/Device Combinations and Companion DiagnosticsNovember 7-8, 2012 (#12016)Washington, DC
Global Considerations for Regulatory Strategy DevelopmentNovember 8-9, 2012 (#12439)Horsham, PA
Regulatory Affairs Part 1: The IND Phase and Part II: The NDA PhaseNovember 12-15, 2012Philadelphia, PA (#12428)
For more information about these courses or to register, please visit the DIA website at www.diahome.org, select Meetings and Training from top menu bar, Find Meetings and Training, and enter the five-digit number as the key word.
Upcoming DIA Exhibit Opportunities EDM and ERS/eCTDOct 8-10 | Baltimore, MD
Global Benefit-Risk Management Oct 9-10 | Silver Spring, MD
Global Labeling 2012Oct 11-12 | Silver Spring, MD
US Conference on Rare Diseases & Orphan ProductsOct 22-24 | Washington, DC
DIA’s Annual Canadian MeetingNov 6-7 | Ottawa, ON
Regulatory Considerations for Drug/Device Combinations and Companion DiagnosticsNov 7-8 | Washington, DC
DIA 2013 49th Annual MeetingJun 24-26, 2013 | Boston, MA
Visit www.diahome.org/exhibit for more details.

63
JAPAN
Japan’s Eff orts to Keep Innovative Research on
Japanese SoilMeasures by Japan’s Pharmaceuticals and Medical Devices Agency (PMDA) to strengthen pharmaceutical research and development received repeated mention at a PMDA “town hall meeting” at the annual DIA conference. Speakers from the agency described a variety of activities, including strategic consultations on research and development with product sponsors and academic researchers, initiatives to strengthen clinical trials, and efforts to advance collaborations with academia. Presenters
uniformly expressed optimism for the future of Japanese pharmaceutical development and innovation.
As Japan’s regulatory agency, the PMDA describes its purpose as comprising a “safety triangle” of 3 key areas, including initial reviews of proposed drugs and medical devices for marketing authorization. (Japan’s Ministry of Health, Labor and Welfare performs subsequent reviews and is ultimately responsible for
MEG EGAN
AUDERSET
Medical/Regu-latory Wr i ter, Thomson Reuters,margaret [email protected]

GLOBAL FORUM | V
OL
4
IS
SU
E 5
64
gfgf
approvals.) Post-market safety efforts are overseen by the PMDA, including data collection and analysis, research to develop safety standards for drugs and devices, consultations with consumers about safe use, and advice to sponsors to enhance product safety. And the agency provides relief services to patients who have experienced adverse health effects due to approved products, including compensation for severe illness and disabilities.
The following summarizes several of the key PMDA programs highlighted at the DIA town hall.
PHARMACEUTICAL AFFAIRS CONSULTATIONS ON R&D STRATEGIES
The PMDA has noted a gap in product development, with too many of the drugs and devices that originate in Japan being taken elsewhere for development and clinical testing. To help remedy that disconnect, in 2011 the PMDA introduced a “strategic consultation service” to assist with pharmaceutical research and development. The agency is particularly interested in consulting with academics “because most researchers in academia don’t understand the exact process for pharmaceutical regulations and so on,” explained Hideo Utsumi, PhD, PMDA Executive Director and Director General of the Agency’s Office of Review Innovation. Researchers might seek guidance on endpoints and sample sizes for early clinical trials, for example, or on toxicity studies to develop biologics and cell-and-tissue-based products
The PMDA service provides 3 levels of consultations. The first two, introductory consultations
and pre-consultations, are free of charge and considered non-binding. They are intended to help applicants prepare for the “real consultation”: a 2-hour, recorded meeting that takes place face-to-face, Utsumi said. Applicants pay a fee for face-to-face consultations; outcomes are binding, so it is important to be familiar with relevant regulations and prepare data appropriately.
Between July 1, 2011 and March 31, 2012, the PMDA provided 120 introductory consultations, 166 pre-consultations, and 36 face-to-face consultations, according to Utsumi’s data. Most (56%) concerned anti-neoplastic drugs; another 21% concerned cardiovascular drugs. Fees charged to commercial entities are considerably higher than those levied to academics. For pharmaceutical products, a face-to-face consultation costs about $19,000 US for companies, while academics pay about 10% of that (approximately $1,900 US). Similarly, a company would pay about $11,000 US to consult about a medical device; academics would pay about $1,100 US.
SCIENCE BOARD TO THE PMDA
Speakers at the town hall touted a variety of recent PMDA achievements, including organizational changes that have helped reduce review times for new drugs. In FY2007, an average standard product review took approximately 20.7 months (12.9 months for regulatory review, 7.9 months for the applicant); by FY2011 a standard review took about 11.5 months (6.30 for regulatory review, 5.1 for the applicant), according to

65
data presented by PMDA Chief Executive Tatsuya Kondo, MD, PhD. This exceeded the PMDA FY2011 target of 12 months for a standard review (9 months for the regulators, 3 for the applicant). Priority reviews in FY2011 took about 6.5 months total, down from 12.3 months in FY2007. Japan has also greatly reduced its “drug lag”: the delay in time between a drug’s release in the US and its release in Japan. The drug lag in FY2007 totaled 3.4 years, according to Kondo; in FY2010, it was down to 1.1 years.
While the PMDA takes pride in those accomplishments, it continues to set new goals and is particularly driven to embrace advanced technologies and promote Japanese innovation, Utsumi said. Drawing on experts from a variety of Japanese universities, in May 2012 the PMDA established a Science Board to advise the agency’s Office of Review and Office of Safety on technological advancements relevant to each stage of product development. The 17-member board tasks include helping to develop and review guidelines and policies for innovative products, and to improve scientific aspects of the review process. Subcommittees will focus on specific areas: pharmaceuticals, medical devices, biologics, and cell-and-tissue-based products. Utsumi stressed that the Science Board will not be directly involved in the review of individual products.
IMPROVING INFRASTRUCTURE FOR CLINICAL TRIALS
Japan’s Ministry of Health, Labor and Welfare (MHLW) has initiated
several programs to strengthen the clinical trial infrastructure, with efforts aimed at promoting early-stage and exploratory clinical trials, according to Kenichi Tamiya, Deputy Director for MHLW’s Research and Development division. A 2010 review of the MHLW’s five-year “clinical trial activation plan” (FY2007-2011) showed that late-stage clinical trials were “greatly improved” in Japan, Tamiya said, but that early-stage and exploratory trials lagged behind those in the US and EU. Furthermore, too many drug candidates discovered in Japan were being shipped to other countries for the research and trials that determine practical applications.
“One of the main reasons is that in Japan there are few hospitals that are able to conduct first-in-human studies of drug candidates, especially of first-in-class,” Tamiya explained at the session. “That’s because of the lack of infrastructure in terms of human resources and facilities. So even the innovative drug candidates of [Japanese] origin are tested in humans first in other countries [that have the] infrastructure for early stage clinical trials. We regard this [as] one of the main reasons for drug lag and it should be overcome to bridge the gap between the promising reserves of basic research and clinical application.”
Tamiya described a five-year (FY2011-2015) MHLW program that has designated five early-stage and exploratory clinical trial centers to focus on pharmaceutical and device development for cancer
indications, cerebrovascular and cardiovascular diseases, intractable immune diseases, and neurologic and psychiatric indications. The ministry designated approximately $6.38 million US to develop the infrastructure needed to support first-in-human and proof-of-concept trials (e.g., to retain experienced investigator and clinical review coordinators, or to acquire necessary diagnostic equipment). A research grant of about $1.88 million US is supporting investigator-initiated clinical trials (e.g., to fund the production of study drugs, draft protocols, or pay for PMDA consultations).
In March 2012, the MHLW initiated its five-year clinical trial “vitalization plan,” which aims to improve medical standards in Japan and “spread Japanese innovation throughout the world,” Tamiya said. The new MHLW plan builds on existing initiatives, including a focus on improving clinical trial infrastructure. Among other measures, the MHLW has designated five “clinical trials core hospitals” that will be developed for high-quality investigator-initiated clinical trials, with the aim of raising trial data in Japan. Each hospital will receive an annual infrastructure subsidy of approximately $6.38 million US; annual research grants total approximately $1.25 million US per hospital. The ministry plans to request another 5 clinical trials core hospitals in the FY2013 budget.
GLOBAL FORUM | V
OL
4
IS
SU
E 5
66
gfgf
The Japanese stereotype depicts a hard-working survivor who can cope with devastating typhoons and tsunamis, a traditionalist with a centuries-old respect for authority. But demographics have changed dramatically in Japan over the last 25 years, and the old stereotype needs an upgrade, according to presenters at the DIA 2012 Annual Meeting. While modern Japanese maintain the survivor image, that unquestioning respect for authority has eroded, said speakers at a session on the “emerging role of the patient voice” in Japan. Japanese patients want to be heard and, gradually, they are finding arenas to inform and voice their opinions.
A 2011 report on social security in Japan, published by the National Institute of Population and Social Security Research (NIPSSR), calls demographic shifts the “most prominent” social change in Japan since the end of World
War II. A decreasing birth rate has led to fewer young people: NIPSSR population estimates project that by 2055 only 8.4% of the population will be 14 years or younger, in comparison to 24.3% in 1975. An estimated 51.1% Japanese will be aged 15-64 years in 2055, compared to 67.7% in 1975. And by 2055, approximately 40.5% will be aged 65 and older, as compared to 7.9% in 1975.
As demographics have changed so have disease patterns, according to Tatsuo Kurokawa, a professor of pharmacy at Keio University who spoke at the DIA session. Patients live much longer now, shifting the healthcare focus from acute disease to chronic “lifestyle” diseases. “Very many people became serious about their health,” he said. The internet offers the public constant, easy access to health-related information, and today’s patients want to explore and discuss treatment options with their physicians. Many now approach physicians and the government with increased scrutiny, Kurokawa said, questioning the long-held
MEG EGAN
AUDERSET
Medical/Regu-latory Wr i ter, Thomson Reuters.margaret [email protected]
Speaking Up in Japan
tsiepassscu
eiroa
hww a
ernn
govK
theutiny scrhening t
esc
retayto
de atio
Mas a
reasues
oachnt
anm
, Kurolong-held
oanm
Khel
tant,ela
y’s p
ns wny
sedtion
nt,ed
s padis
wiy n
td
on
onstanelat
ay’nd
nsan
nse
ststio
anynd ted
aynd disw
nstaated
h thappro
nmentwaok
ld
ppnme
dokaw
pproment
kawa

67
belief that those in charge have the best interests of the general public in mind.
A series of high-profile healthcare events in recent decades have fed the public desire for medical information, according to Kurokawa, including a lengthy lawsuit against drug companies and the Japanese government by hemophiliacs infected with HIV from tainted blood products. The first of the hemophiliac plaintiffs filed suit in 1989; more than 400 accepted a settlement from the government and five pharmaceutical companies in 1996. In 2008, after determining that thousands of Japanese had contracted hepatitis C from tainted blood products administered during the 1970s to early 1990s, the government passed a law enabling some of those affected to pursue compensation. The prime minister also publicly accepted government responsibility for the hep C infections.
Such exposure and widespread publicizing of treatment-related adverse events has compounded public skepticism about the government’s intention to do “the right thing at the right time,” Kurokawa said. Japan’s Ministry of Health, Labor and Welfare (MHLW) responded by inviting more input from patients and patient groups, beginning with drug-safety issues in the 1990s, according to Kurokawa. (The MHLW oversees the country’s social security systems, including healthcare.) Since then, the MHLW has invited patient representatives to attend advisory committee meetings with increasing frequency, although their involvement has occurred in “case-by-case situations” and
does not constitute “systematic recruitment,” Kurokawa said. As an example, he described the 2011 establishment of a “special committee” to the MHLW Health Sciences Council, which was tasked with reviewing potential amendments to Japan’s Pharmaceutical Affairs Law (PAL). The amendments were intended to promote drug and device safety and effectiveness. The 16-member committee included scientists, physicians, patient representatives from cancer groups, and representatives of people who had contracted hepatitis C from tainted blood products.
Conference presenters spoke about the growing strength of the patient voice in Japanese drug development and the healthcare arena—but they noted room for progress. Patient participation in MHLW councils is limited to patients appointed by council members, for example, and most appointees are men, according to Hiromi Matsumoto of Nattoku-shite Iryou wo Erabu-Kai, a medical consumer group that liaises between patients and medical providers. While Matsumoto described patient representation on disease-specific councils as “well-balanced,” representing 25-35% of total membership, patient representation on the “permanent” councils is far lower, she said.
The 20-member Cancer Control Promotion Council includes five patients, for example, and seven of the 20-member Council on Promotion of Hepatitis Measures are patients, according to data presented by Matsumoto. (The cancer council also includes 12 medical experts; the hepatitis council includes seven. The
remaining members represent “other” fields, such as journalism, labor unions, and the law.) In contrast, the permanent councils typically host no more than one patient member, if any. A 22-member council devoted to pharmaceutical safety includes just one patient representative, Matsumoto said; 20 are experts. A 21-member council devoted to blood and blood products includes two patient representatives and 16 experts, while a council for non-prescription drugs includes no patient representatives among its 16 members.
“We don’t understand why,” Matsumoto said. “It’s not experts but general people who buy and use these products.”
Matsumoto’s organization advocates for an even distribution of patients, experts, and “others” on the MLHW councils, and for equal numbers of male and female members. Nattoku-shite Iryou wo Erabu-Kai also supports term limits for council members; Matsumoto noted that some have served on the same councils for as many as 10 years. She asserted the importance of including the patient perspective in MHLW considerations, but described several factors that inhibit patient participation. Some experts believe patient participation slows proceedings, she said, because patients are unfamiliar with technical information and do not share experts’ “common sense.”
There are roughly 1,500 patient groups in Japan, although group size and history vary greatly, according to Keiko Ebihara, Director for Regulatory and
Kut
oe
ysS
oute
ncms,
e te
nhen
nt these
comta
mmitfre
eeequencyment as
ase situa
b gu s t
w (Ts cdi h
M LWi s
et
Sinpatienadvisoinc
y sing f
involvem“case-by-ca
eso
ngain
casase-
issueuro
ntry’snc
MHtati
, a oc
Kurokuntr
nclhe
ntaeecy,
s at
ssuesawa
y’s udin
MHtiv
ma
con
is esrokawa
unt scludi
he Mativee m
y, a
atio
y c
trepr
visorinc asi
r in“c
repsory
increathe
ory ep
reasheir i
in “c

GLOBAL FORUM | V
OL
4
IS
SU
E 5
68
gfgf
Vaccine Policy, Health Policy and Access at MSD K.K. Of the 300 “main” patient groups, 70 have existed for more than 30 years and 100 for fewer than 10, she told DIA attendees; 100 groups have fewer than 100 members, and 7 have more than 10,000. Early patient groups formed in response to “unethical medical practices” and focused primarily on curing disease and improving conditions for convalescent care, according to Ebihara.
Groups focused on patient networking began forming in the 1960s, and “have been continuously established up to the present time,” Ebihara said. “In recent years in particular more and more patient groups which focus on peer support have been established with the primary goal of aggressively expanding advocacy-related activities.” Peer support remains the main focus of Japanese patient groups.
Ebihara noted several ways in which patient groups differ in Japan when compared to those in the US and European Union (EU). Groups in the US and EU tend to be much larger and more structured with a variety of funding sources, both private and public; most typically a central office with a dedicated staff and board of directors. Only a few Japanese patient groups perform advocacy and very few support research for new treatments, she said.
Speakers stated repeatedly that patients and patient groups in the US and EU have more influence than their Japanese counterparts on drug development and policy. While US regulations mandate that each FDA advisory committee meeting devote at least an hour for an open public hearing, for example, and each advisory committee includes at least one patient representative with a vote equal to that of experts on the committee, the Japanese do
not have a guaranteed platform. Interactions and cooperation between Japanese patient groups, the government, and the pharmaceutical industry occur only on a case-by-case basis, according to Ebihara. “The regulation and infrastructure does not exist to involve the patient voice into drug development in Japan,” she said.
Recently, the First DIA CMC Forum in Japan was held at the Nakano Sunplaza, Tokyo. DIA Japan has traditionally dealt with mainly
pharmaceutical issues related to safety and clinical development, not issues related to product quality, and so this forum focused on issues related to CMC for the first time. When I was first approached to act as Program Chairperson for the forum, I was concerned as to whether we could create a program that would generate interest, as there are already many product quality-related symposiums and forums in Japan. However, I was attracted by the forum’s
unique characteristic of enabling in-depth discussion between industry, government agencies, and universities by using the DIA’s global network, and so I agreed to serve as Program Chairperson.
A condition for holding the forum was that the program’s main theme be a global one. Recent issues in Japan related to product quality are the notable increase in raw materials for drug formulations from China, India, and other countries and the fact that these raw materials are used frequently in not only generic drugs but also new pharmaceuticals. It was therefore decided that the forum should focus on active pharmaceutical ingredients (API) and examine efforts to maintain and improve API product quality in emerging Asian regions.
Dr. Ping Wang of the Chinese Pharmacopoeia Commission (SFDA presented the keynote speech. In addition, experts
Th e First DIA CMC Forum in Japan
HARUHIRO
OKUDAPhD
Nat ional Inst i -tute of Heal th Sciences, Japan

69
from Chinese pharmaceutical manufacturing, as well as the United States and India spoke; officers responsible for product quality and other representatives from the Japan Generic Medicines Association, the Japan Pharmaceutical Traders’ Association, the Pharmaceuticals and Medical Devices Agency (PMDA), and Mega Pharma also gave presentations.
Dr. Wang described the current situation regarding pharmaceutical regulations in China and future efforts in his keynote speech entitled, “Challenge of Quality Improvement in China.” Following the keynote speech, presentations took place in three sessions—“Current Pharmaceutical Manufacturing Status and Challenge of Quality Improvement in Asia,” “PIC/S Accession and Next Challenge from Quality Inspection,” and “Dealing with Regulatory Differences”—and the forum concluded with a panel discussion with all of the speakers and featured a lively debate mixed with answers to questions from the audience.
Due to space limitations, it is difficult to describe the individual presentations in detail, but in line with the aim of the program, the forum enabled participants to hear directly about other countries’ issues that would be difficult for other forums or symposiums to examine. These include a description of the problems encountered by a US FDA inspector when conducting on-
site inspections of manufacturers located within China and points that new pharmaceutical manufacturers consider when subcontracting manufacturing, such as in China and India, and procuring raw materials for drug formulations. The forum enabled participants to obtain far more useful information than they can read or hear, and in addition, the content was very useful for considering quality assurance of pharmaceutical products in Japan in the future.
As mentioned earlier in this article, this forum was the first held by DIA Japan focusing on product quality, and it drew around 100 participants. The overwhelming enthusiasm of the meeting exceeded the number of participants, and the content was worth sharing with many others.
A meeting to review the symposium’s success was held and, as a result, it was decided that DIA Japan will hold a second CMC forum in late spring 2013. It has been agreed in principle that this forum will again examine issues related to pharmaceutical product quality, focusing especially on China and India, and
may also examine in detail issues related to auditing. I, therefore, encourage many people in relevant fields to participate in the forum to gain useful information for their own work.
Lastly, I would like to mention that a networking meeting was held after the symposium, which included both speakers and program committee members, to exchange opinions with Dr. Ping Wang of China’s SFDA and many others. This was another unique and valuable characteristic of this forum as advances the mission of the DIA to act as a global knowledge resource to advance health and well-being worldwide.
annandnd
Read Your Global Forum
on the
GO

GLOBAL FORUM | V
OL
4
IS
SU
E 5
70
gfgf
attendee in both regional and international meetings— the former will allow for sharing regional experiences, while the latter will help creating awareness on our activities in Latin America.
What are your personal aspirations that could be enhanced by service on pACLA?
My personal aspirations have expanded as part of pACLA— I aim to help improve coordination with other Latin American countries in the area of regulations, in the field of bioequivalence and clinical trials in general.
What inspired you to apply for a pACLA voluntary board member position?
My main interest to join, as a member of the volunteer board of pACLA, is being able to collaborate in planning activities that would potentially improve regulatory and training issues in the pharmaceutical area in both my country and in Latin America.
What aspects of your new role are you particularly looking forward to?
In my new role, I’m looking forward to continuing my participation as speaker or
EDUARDO
JOHNSON
LATIN AMERICA
A&Q
Questions and Answers with Dr. Eduardo Johnson

71
What is one goal you have set for yourself as a member of pACLA to advance the mission in this area?
Establishing coordination between DIA and educational institutions and Chilean regulatory agencies of which I am a part, in order to carry out joint training activities.
What would be the most pressing issues to be addressed in Chile?
In my country it is of paramount importance to carry out training courses on clinical trials, both in terms of ethics—by improving the composition and operation of scientific ethics committees—and by addressing the inspection area of clinical trials.
How do you see the industry evolving in Chile in the next 5 years?
In the next 5 years our domestic industry will undergo a major change in terms of safety and efficacy of manufactured generics, because new regulations demand compliance with good manufacturing practices, mainly in the validation of their processes, and checking Bioequivalence standards.
In your view, what should be the priorities for DIA to address in the Latin American region?
In my view, DIA in Latin America should permanently serve as liaison and coordinator among regional countries with the aim to foster better collaboration within the fully neutral and transparent realm that has always characterized DIA.
What are the unique challenges faced by the Latin American market that differentiate it from the other global regions?
There are three aspects that I think Latin American markets differ from other global economies: one is entry barriers for products, both in regard to duties and requirements for marketing authorization (Sanitary registration). Another one is the issue of pharmaceutical patents— whose regulation is different for each one country. The third is the insufficient research on new products in our countries. Today we depend entirely on the major producing countries.
What is the current role of the Industry in Latin America and how do you see it positioning itself in the global market?
The pharmaceutical industry requires uniform sanitary regulations among the various Latin American countries where they market their products. Although there are currently several initiatives for the harmonization of sanitary regulations between Latin American countries, sponsored by international organizations, the results, so far, have been insufficient.
What would you advise to other industry leaders looking into applying for a DIA pACLA position in the future?
My advice would be that industry leaders and regulatory authorities should participate actively in Latin America. This collaboration should aim at improving quality and access to better drugs and medical devices in our countries.
The latter could be worked through by becoming members of DIA, which allows for a great environment to achieve these objectives.
Eduardo Johnson holds a Masters in Publ ic Heal th Epidemiology Ment ion and a Dip loma in Bioeth ics f rom the Univers i ty of Chi le. Cur-rent ly, he is a Candidate for Master of Cl in ica l Bioeth ics at the Univers i ty of Chi le. He serves as an Associate Pro-fessor of Heal th Law at the Cathol ic Univers i ty of Chi le, a Profess ional eva luator for the author izat ion of c l in ica l t r ia ls in Chi le in the Nat ional Drug Inst i tute of Publ ic Heal th of Chi le and is an evaluator of veter inary b io logica l products at the Nat ional Drug Agency of the Publ ic Heal th Inst i tute of Chi le. Eduardo is a lso a Corresponding Member of the Academy of Sciences of Chi le and has held the fo l lowing posi t ions prev iously: Di rec-tor, Department of Vaccine Product ion Inst i tute of Publ ic Heal th of Chi le; Di rector, Na-t ional Drug Agency at the Pub-l ic Heal th Inst i tute of Chi le; Temporary Advisor of the Pan Amer ican Heal th Organiza-t ion severa l t imes in the area of immunology and c l in ica l essays ( t r ia ls ) ; Consul tant in pediatr ic medic ines regulat ion in the Wor ld Heal th Organiza-t ion; as Pres ident of the Phar-macists Col lege of Chi le and as a Member of the Research Eth ics in the East Metropol i tan Heal th Serv ice of Chi le.

GLOBAL FORUM | V
OL
4
IS
SU
E 5
72
gfgf
DIA’s Worldwide Executive Director Paul Pomerantz and the Brazilian Society of Pharmaceutical Medicine (SBMF) President João Massud Filho recently signed a Dual Membership Agreement in Philadelphia under the auspices of DIA’s Annual Meeting.
In line with the recommendations and guidelines established by the DIA Board of Directors during its June 2012 Retreat, the partnership between DIA and SBMF allows for members of the latter to become DIA members by covering the corresponding regional fee. Approximately one hundred SBMF professionals have became DIA members since the agreement was signed. The agreement covers only membership-related operations; however, it opens the doors for more formal collaboration
knowledge transfer, cross-promotional activities, volunteer engagement and networking and discussion forums.
The Dual Membership agreement
DIA to expand its presence, focus and reach into Latin America. The recent regional growth has created unmet demands for pharmaceutical and medical device products for basic consumer goods and better access to healthcare. Brazil, Mexico and Argentina are the largest markets; Brazil’s market alone was valued at US $34.8 billion in 2011.
As in other regions of the globe, DIA is equally committed in Latin America to the broad dissemination of information, with continuously improved professional practice as
ALEJANDRO
H. BERMUDEZ-
DEL VILLAR
MA/IBDD, DIA’s Latin America & Global Program Development Coordinator. Alejandro works in the Washington
can be reached at +1.215.293.5825, [email protected].
DIA and the Brazilian Society of Pharmaceutical Medicine Form Strategic Partnership
DIA’s Worldwide Executive Director Paul Pomerantz and the Brazilian Society of Pharmaceutical Medicine (SBMF) President João Massud Filho sign the MOU in Philadelphia.

73
the goal. DIA’s neutral, impartial environment is highly valued in this region, since it is the only global organization that operates
any one organization or authority.
and its mission is the promotion of
knowledge and skills for those who work with pharmaceutical medicine
information for healthcare products
society.
The signing of the Agreement is
strong interest of DIA to enhance cooperation and collaboration with all stakeholders from Latin
”Creating regional strategic partnerships enhances DIA’s goal to operate globally and act locally,” stated Paul during the signing ceremony in Philadelphia.
Expanding Horizons in the Region: Successful Risk Management DIA
Tutorial in Bogota, Colombia DIA’s efforts to invest in the Latin American region are yielding results on various fronts. The most recent example is a successful DIA tutorial on Risk Management that took place in Bogota, Colombia on August 9, 2012. The Tutorial was carried out jointly with the nonprofit professional Colombian association called AVANZAR (devoted to the advancement and development of Clinical Research in the country); and framed by its 6th Clinical Research Conference.
The Tutorial, officially entitled “Managing Risk and Opportunity in Clinical Trial Projects” was provided by DIA’s professor Douglas Call and accounted for
46 attendees from pharmaceutical companies, CROs, Investigative Sites and the Colombian Regulatory Agency, INVIMA. The interactivity and dynamism of DIA’s program quickly engaged the attendees, who participated actively during the entire educational experience.
Dr. Diana Valencia, DIA’s Regional Advisory Council Member and AVANZAR President, expressed that the tutorial was extremely helpful for the Colombian Industry attendees: “The wealth and breadth of knowledge provided as content, as well as the practical examples given by Dr. Call reinforced and enriched the program in a great fashion.” Dr.
Attendees during one of the Tutorial activities Dr. Diana Valencia, DIA’s Regional Advisory Council Member and AVANZAR President, interacting with an attendee.
DIA’s Professor Douglas Call's dynamic exercises.

GLOBAL FORUM | V
OL
4
IS
SU
E 5
74
gfgf
Valencia actually attended and volunteered to co-facilitate the group activities which enhanced the experience as the group broke the ice at a faster pace. The Post Conference Survey yielded great results as 95% of attendees rated the Tutorial as “Excelente” (excellent) and 5% rated it “Buena” (good).
The design and crystallization of this project is intrinsically connected to DIA’s efforts to increase its presence in Latin America as well as to explore new possibilities for initiatives in the region. Back in March 2012, DIA’s Regional Advisory Council
for Latin America held a face to face meeting in Bogota, and provided two introductory free workshops for the industry. The success of those activities greatly enhanced plans and expedited the partnership negotiations with AVANZAR for this August Risk Management Tutorial.
AVANZAR (Asociación Para El Avance De La Investigación Clínica En Colombia) is devoted to promoting an adequate environment for the development of Clinical Research in Colombia; and works to ensure continued education process for its affiliates, keeps scientific methodology
standards in clinical trials and facilitates Good Clinical Practice knowledge through the research community across the country.
The DIA “Managing Risk and Opportunity in Clinical Trial Projects” tutorial in Colombia was a success on different fronts, including the expanded presence locally and the strengthening of links between the DIA, its local members and the different Colombian stakeholders. DIA Latin America renews its commitment to assist in advancing the pharmaceutical and medical devices industries in the region.
Here with a helping hand. ClinForce is a national provider of resource
solutions providing talented professionals or project teams to accomplish
client goals. With over 30 years of experience, companies seeking clinical
research staffi ng services as well as clinical trials outsourcing services have
come to rely on our expertise and our innovation. To learn more, call us at
800-964-2877 or email us at [email protected]

75
CHINA
Patent Drafting Strategies: Get it Right the First Time
With the booming of the Chinese market, obtaining and enforcing patents has become a crucial way to protect commercial interests there. However, patent applicants outside China often overlook certain requirements unique to the country when drafting patent applications, which means that good inventions may not be granted patent rights, or that the patents granted become unenforceable.
Applicants may enhance their chance of obtaining a globally acceptable patent by understanding the requirements and adopting proper patent drafting strategies that take into account preventable pitfalls, as
shown in our relevant practice and related provisions, including the newly amended Chinese Patent Law, Implementing Regulations of the Patent Law (the Implementing Regulations), Guidelines for Examination and the Interpretation of the Supreme People’s Court.
AMENDING APPLICATION DOCUMENTS
China’s restrictions on amending documents after filing the application are stricter than those in other countries.
Article 33 of the Chinese Patent Law (2008) provides that: “the amendment to the application for a patent for invention or utility

GLOBAL FORUM | V
OL
4
IS
SU
E 5
76
gfgf
model may not go beyond the scope of disclosure contained in the initial description and claims.” In accordance with the Guidelines for Examination, the word “disclosure” is construed as content that could be “determined directly and unambiguously” from the specification as originally filed. This is a stringent criterion that requires the original application documents to be of high quality.
Moreover, Chinese Patent Law has no provision for a post-grant amendment procedure. If a patent owner finds an error in a granted patent, there is almost nothing that can be done to remedy the error. Furthermore, in the invalidation process, a technical feature which is merely disclosed in the description is not allowed to be incorporated into the claims to make the amended claims patentable. Permitted amendments are generally limited to deleting or combining claims or removing alternative technical solutions. This means that if an independent claim has a defect related to novelty or a support issue because the claimed scope of protection is too broad, the case will be difficult in the invalidation procedure if there are no appropriate dependent claims which can serve as backup.
Patent applicants are advised to conduct a sufficient search before drafting patent specifications to get a clear grasp of the technological landscape, and seek a reasonable scope of protection in the initial claims; by refraining from an overly broad protection scope, they may avoid extensive amendments in the examination stage.
Applicants should also draft their dependent claims carefully and try to include technical features in
the dependent claims if they could be useful to the claims in the invalidation stage for purposes of novelty, inventive step or support of claims. They will otherwise have no opportunity to do so once the invalidation process starts.
If the claims relate to multiple groups of subject matters, such as compound, composition, use and manufacturing method, a later independent claim to cite all the preceding claims of the relevant group is best. For instance, where a first group of claims refers to a series of active compounds, the second group of claims claiming the uses of the compounds may be drafted in the manner of: “uses of the compound of any of claims 1-10 in the manufacture of a medicament for the treatment of cardiovascular diseases,” to avoid limiting the reference to claim 1 or only a few claims, and allowing more room for flexible deployment in the invalidation stage.
Finally, applicants should ensure that a commercially important product is covered by at least one dependent claim, even if the scope might be narrow. Especially for pharmaceutical patents, the active compound finally selected should be written into a dependent claim. Compared with independent claims with broad protection scope, dependent claims that cover only one or several particular compounds are sometimes more enforceable, as they are not only more stable when facing a validity challenge because of the narrow scope, but also permit more direct judgment of infringement in litigation.
FUNCTIONAL LANGUAGE
Article 4 of the Supreme People’s Court’s Interpretation of Several
Issues Concerning Application of Law to Trial of Cases of Dispute Arising from Infringement of Patent Rights promulgated by the Supreme People’s Court in 2009 (the Patent Infringement Interpretation) explains the technical features represented by functional language in the claims. The Article stipulates that: “for a technical feature in a claim represented by function or effect, the courts shall determine the content of such technical feature by reference to the specific embodiment and its equivalent embodiment(s) of the function or effect as depicted in the description and the appended drawings.”
When representation in terms of structural features fails, defining the technical features in the claims by functional language is necessary in some cases. However, given the fact that representation by functional language tends to be too general literally, such representation, on top of the functional depiction, should be accompanied by embodiments and equivalent embodiments for defining protection scopes.
In the construction of functional features, Article 4 of the Patent Infringement Interpretation and the Guidelines for Examination are not in line with each other. The relevant provision in the Guidelines for Examination as stated in Section 3.2.1 in Chapter 2 of Part II reads: “technical feature defined by function in a claim shall be construed as embracing all the means which are capable of performing the function.” In accordance with this, the scope of examination by the examiner should “embrace all the means which are capable of performing

77
the function.” This stipulation has actually tightened the criteria of patent granting for novelty, inventive step and claims support. In infringement litigation, however, the scope of protection that can be asserted covers merely the specific means of carrying out the technical feature in the description and the drawings and its equivalent embodiment. This means that undergoing more stringent examination for patent grants only leaves the right-holder with a narrower scope of protection, which is obviously unfair. Unfortunately, consensus on the issue is not likely to be reached between the Supreme People’s Court and the Patent Office for at least the next couple of years.
As long as consensus on the issue is yet to be reached, functional definitions should be used in a discreet manner. If the use of functional language is necessary, as many embodiments as possible should be included in the description so that the coverage of a broader protection scope can be secured for future exploitation of the patent rights.
LACK OF CLARITY
Rule 20.1 of the Implementing Regulations of the Chinese Patent Law, now Article 26.4 of the Patent Law following revision of the law in 2008, provides that: “the claims shall be supported by the description and shall define the extent of the patent protection sought for in a clear and concise manner.” This provision has been one of the most frequently cited provisions in examination opinions, especially in the chemistry field.
In practice, most lack of clarity defects in the claims can be
overcome by amending the application documents or explaining in the observations. However, some of these are defects incapable of being overcome or remedied such that patent applications are rejected or protection scopes are narrowed down substantially.
An example is a reexamination case concerning a patent application with a claim directed to a coated food product containing syrup, where the dry material of the syrup has DP4 of 0.7-1.5% by weight. In the application, DP4 is the main feature distinguishing the invention from the prior art, and the fact that DP4 appears only as an abbreviation with no definition nor its full name spelt out throughout the description led the examiner to object to the application in the reexamination process. The examiner cited various documents to prove that the term has more than one meaning. As such, the term was considered unclear, and the patent application was ultimately rejected due to this lack of clarity.
Many serious non-clarity defects are caused by unclearness in the meaning of technical terms. Worse still, correcting these problems once the application documents are filed is not easy. For this reason, this issue should be avoided from the start when new applications are drafted.
Patent applicants should double-check the technical terms in the claims against the description as soon as an initial draft is ready to ensure that the core terms in the claims or potentially controversial terms are clearly defined in the description. More detailed definitions can be introduced by expressions such as “for instance”
or “preferably” to cover varied senses of the terms.
Abbreviations should be used discreetly and if necessary, providing their full names or relevant references in the description is better. Finally, technical terms should be defined carefully to ensure precise and accurate definitions.
EXPERIMENTAL DATA
In China, experimental data disclosed in patent applications are important, in particular those in pharmaceuticals and chemistry. Such experimental data are relevant for factors such as sufficient disclosure, claims support and inventive step, which contribute to determining whether to grant a patent and the protection scope obtained. Compared with many other countries, China’s patent law imposes tougher requirements on experimental data in this context.
Applicants have limited opportunity to overcome defects through filing supplementary data during the examination process, despite the harsh statutory requirements. Generally, filing experimental data after the filing date of an application to overcome insufficient disclosure or prove claims support is not accepted. Even worse, to overcome the lack of inventive step rejection, supplementary data for an unexpected technical effect may not be considered by the examiner, unless the experimental data furnished are comparative data and the data concern a technical effect already recited expressly in the original application documents with corresponding data. This means that if the initial description contains no experimental data

GLOBAL FORUM | V
OL
4
IS
SU
E 5
78
gfgf
to support the technical effect caused by the invention to some extent, the experimental data furnished by the applicant to prove a technical effect after the filing date or in the responses to office actions will normally not be accepted, even if there is a conclusive statement about the technical effect in the description.
Data for technical effects should be prepared carefully when drafting the application documents. For inventions related to active compounds, pharmaceutical compounds, secondary pharmaceutical uses, and biotechnology, referring to Sections 3 and 9.2 in Chapter 10 of Part II of the Examination Guidelines issued by the State Intellectual Property Office could help avoid the lack of experimental data. Furthermore, for subsequent applications filed within one year of the date of filing an application, there is an option to add subsequently obtained experimental data to the text of the application documents.
THE ESTOPPEL DOCTRINE
Article 6 of the Patent Infringement Interpretation touches on the doctrine of estoppel in patent infringement proceedings as a limitation against the doctrine of equivalents. This is the first ever provision stipulated by the Supreme People’s Court that introduces this doctrine.
The provision stipulates that where a patent applicant or a patent owner surrenders a technical solution by amending the application documents or a written statement in the observations during the examination or invalidation procedures, the applicant or patent owner will not
be allowed to reassert his rights in patent infringement proceedings. The Article does not mention the motivation behind the amendment or statement, whether there is any causal link between this amendment or statement and patent grant, nor whether they are accepted by the examiners. This means that the doctrine of estoppel will be applicable no matter whether the amendment is made for the purpose of obtaining patentability or not.
China’s patent examination is characterised by a rigid requirement on amendments to the specification. As generalisation after filing is not permitted in the Chinese system, applicants often need to overcome such substantive defects as lack of inventive step or support in the independent claims by limiting the original broad scope of protection to a narrower one recited in the description, which in many cases is the scope of a specific example. This stipulation is restrictive as the limiting amendment to the claims or statement in the observations made by the applicants in the examination process often unfavourably influences the enforceability of a patent eventually granted.
For this reason, writing a broad scope of protection for the claims when drafting an application is not necessarily a good idea. If an overly broad protection scope asserted in the initial claims is limited to a narrower scope of protection to overcome problems of novelty or claims support, the right-holder will be banned from asserting infringement under the doctrine of equivalents for any technical solution in the surrendered scope from the initial claim. However, if a reasonable
scope of protection is written in the initial claim, the right-holder may still assert equivalent infringement for the aforesaid surrendered scope through the doctrine of equivalents. The reality is that an initial claim with a narrower protection scope may turn out to achieve a broader scope of protection in infringement litigation.
Sufficient and diligent searches before drafting a patent application to get a full picture of the technological landscape, and writing a reasonable scope of protection in the initial claims to avoid multiple amendments in the examination stage are advised. This further shows the importance of search in drafting patent applications.
In addition, adequate room should be left for amendments, such as outlining a series of technical solutions with protection scopes narrowing down by various degrees between the broad scope of the main claim and the narrow one of the embodiments in the description or the dependent claims. By doing this, when the broad protection scope is not granted, there is still the option to retreat to technical solutions with narrower protection scopes, which will minimise the risk of narrowing down the protection scope to that of a specific embodiment.
Given the relatively complicated statutory requirements governing patent applications in China, drafting patent applications is a challenging job. Applicants need to prepare well before drafting new applications with informed knowledge of issues that arise in subsequent procedures, so as to effectively exploit their patent rights and protect their interests.

79
EUROPE
DIA’s latest meeting on the regulation of combination products entitled ‘Anticipating the New Regulatory Landscape for Drug/Device Combinations and Companion Diagnostics: an Overview of the Current and Likely Future EU rules’ provided delegates with a critical and timely insight into the changing regulatory landscape for these often complex and unique products.
The event, held last month in Basel, Switzerland, focused on the current requirements as well as the nature of the shifts that are likely to impact all manufacturers
of products such as drug/device combinations and companion diagnostics.
Speakers from various regulatory authorities, as well as from industry, spoke about the current challenges that they face in regulating drug/device combinations and companion diagnostics according to the existing medtech regulations. In the EU, these products are currently mainly regulated by the Medical Device Directives, rather than the Pharma Directives.
Any manufacturer active in this area – many of those coming
How the EU Regulatory Environment is Changing for
Drug/Device Combinations and Companion Diagnostics
SHAYESTEH
FÜRST-LADANI
A report on DIA Europe’s Combina-tion Products Workshop the by Programme Co-chair Shayesteh Fürst-Ladani, Managing Director, SFL Regulatory Af-fairs & Scien-tific Commu-nication Ltd, Switzerland.

GLOBAL FORUM | V
OL
4
IS
SU
E 5
80
gfgf
from a pharma background – must therefore ensure that they are well acquainted with the Medical Device Directives and culture, as well as the ongoing changes. Speakers shared their experience and lessons learned when developing drug and device combination products and companion diagnostics.
This is a complex area where competent authorities, under the present legislative framework, are not always in agreement about the classification of a combination or borderline product, and where manufacturers would do well to get clarification at an early stage of product development about from the authorities. Leaving questions to be sorted out by national or EU courts is not a good option – being described by one speaker as “Russian roulette.”
But views were also expressed that regulation should not be so tight or detailed that they straightjacket regulators and industry alike and block innovation and creative solutions to complex problems for the benefit of patients.
Attendees heard that there is pressure for urgent measures to tighten the medtech regulations that will affect all manufacturers in the area.
Much of the pressure originates from the European Commission following the uncoordinated response among Competent Authorities to the PIP breast implant scandal, and means imminent changes ahead. It is likely that the Commission’s new measures will be implemented already in 2013 and should lead to more co-ordinated vigilance and closer monitoring of the Notified Bodies by the authorities,
as well as closer monitoring of manufacturers by the Notified Bodies.
As part of the urgent new measures, Notified Bodies will need to be much more vigilant and proactive in monitoring manufacturers and companies who could find themselves subject to un-announced visits. Also, analysis of post-market reporting is intended to be more centralised and co-ordinated to enable the authorities to pick out trends and potential risks of medical devices at an early stage.
Attendees heard that the revision process of the current Medical Device Directives will take several years, but will offer a new context to manage the influx of new and innovative products over the next 20 years or so.
The Commission’s first draft proposals are due to be published soon.
The current EU medtech rules are enshrined in Directives. As a result, they had to be transposed into the national laws of the Member States when they were introduced a couple of decades ago. According to the national legislative cultures and backgrounds, this transposition resulted in different interpretation and challenges in co-ordination for all stakeholders, including industry and regulators. The revisions are now being introduced as Regulations – which means they will apply directly and uniformly in the laws of each and every EU Member State. This already represents a significant regulatory shift.
It is anticipated that the new medtech Regulations, once adopted, could become effective
from 2015-2016 and that there will be some form of transition period for products already on the market.
The meeting stressed the need under future rules for greater clarity over reporting adverse incidents with combination and borderline products, and some connection between the Eudravigiliance (pharma) and Eudamed (medical device) vigilance databases, with gaps in reporting to be identified and plugged.
A desire was also expressed for a common vocabulary between the two sectors, so that there can be better communication in this area.
The regulatory environment for some combination products, particularly where the drug plays an ancillary role to the device, is likely to be considerably tighter under the new regime. At present, such products are considered high risk and are regulated as Class III medical devices. This is expected to continue. However, there is now pressure from the European Parliament to have pre-market authorisation of Class III devices by the authorities which would also include drug/device combinations. This approach is opposed by the European Commission, which proposes a process where a new Committee at the European Commission, known as the Medical Device Co-ordination Group, will have an opportunity to review applications of such combination products to Notified Bodies before the Notified Bodies make their final decision.
There is also a question about the future regulation of integral non-reusable drug/device combination products classified as drugs. According to the

81
Medical Devices Directive 93/42/EEC (MDD), these products are governed by the pharmaceutical requirements, Directive 2001/83/EC, whereas “the relevant Essential Requirements of Annex I to this Directive (ie MDD) shall apply to device component as far as safety and performance-related features are concerned.” The MDD fails, however, to explain how this should be done, and to spell out who has responsibility for verifying this.
Considerable lobbying for clarity has been carried out by industry in this area, and it is expected that under new EU rules the manufacturer will need to supply evidence (such as an EU declaration of conformity or a certificate issued by a notified body) concerning the device element.
For first time, new rules governing companion diagnostics are also anticipated and will impact the pharma industry too. At present, companion diagnostics are regulated as general in vitro diagnostics (IVDs) and not subject to Notified Body involvement. However, the expected new framework sees these tests under Notified Body scrutiny for the first time. In addition, the risk categories of most IVDs are likely to change upwards. This will not only mean that companion diagnostics will need auditing by Notified Bodies, but also that their conformity assessment procedures will need to change. As a result, companies will have a big, expensive and time-consuming job ahead in changing their technical documentation to meet the new requirements.
There were calls for simplicity in the combination area, and to learn lessons from the US example
where the Office of Combination Products plays a decision-making and co-ordinating role, and helps manage the uncertainty about classification and regulatory responsibilities.
There were also questions raised during discussions in the breaks about the role of notified bodies in making submissions themselves on behalf of their clients to the pharma agencies and the EMA regarding the drug element of a device/drug combination, and a proposal that they should be cut
out as the middle man for this particular role. In conclusion, manufacturers of drug/device combination products and companion diagnostics will be impacted by an increasingly strict regulatory environment in Europe. Changes will occur in two timeframes – imminently and in three years’ plus time.
It is essential that all stakeholders in this sector keep abreast of the changes, to ensure they remain legally compliant, ready to lobby where necessary and at the forefront of industry.
will afford participants the opportunity to network with professional colleagues from around the world. With an appealing range of topics set in 17 themes the co-Chairs, Beatriz Vicén Banzo and Peter Bachman, anticipate fruitful and engaging discussions that will serve to improve further healthcare systems everywhere.
Amsterdam is the ultimate “small big city” and combines all the advantages of a cosmopolitan capital with a compact, easy-to-navigate size which translates in
DIA’s 2013 Annual EuroMeeting, to be held 4-6 March in the Amsterdam RAI, is global in scope and will attract more than 3,000 medicines development professionals from around the world. It will bring together experts from the biopharmaceutical industry, contract research and service organisations, academic research centres, regulatory agencies and health ministries as well as delegates from patient organisations. This convergence
DIA Celebrates 25th Annual EuroMeeting in Amsterdam

GLOBAL FORUM | V
OL
4
IS
SU
E 5
82
gfgf
less time spent in commuting and more time enjoying what the city has to offer. The city has a rich cultural heritage and 2013 is a year to celebrate important events there. Besides the 400-year anniversary of the Canal Ring, Amsterdam will be celebrating the re-opening of the fully renovated Rijksmuseum, the 125th anniversary of the Concertgebouw (concert hall) and the Royal Concertgebouw Orchestra, the 225th anniversary of Felix Meritis conference and event centre, and the 175th anniversary of Artis Royal Zoo. 2013 also marks the 50th anniversary of the host country’s Medicines Evaluation Board. The Amsterdam EuroMeeting will feature a theme on Regulatory Science organised by the MEB.
With a focus on better public health protection, greater transparency of the processes and the rational use of medicinal products, the proposed areas for discussion for this, the 25th Annual EuroMeeting, are classified into general disciplines including Pharmacovigilance and Regulatory Affairs for medicinal products and medical devices, R&D and Clinical Trials.
The scope of the presentations will cover the experience gathered after the implementation of the new Pharmacovigilance legislative framework, as well as from the patients’ and Health Technology Assessment (HTA) perspective. Experts and authorities in the fields will be presenting their considerations for debate.
By 2013, the new Pharmacovigilance Directive will have been in place for almost a
year; knowing what still needs to be done - or improved, and most importantly: are we getting what was initially expected? These are some of the key areas that the professionals attending the meeting will be able to learn about and debate.
Other important topics to be covered include the Falsified Medicines Directive, the Information to Patients - what is the status? - the role played by scientific societies as experts, and considerations over an ageing population and the potential impact on hospitalisations.
OPENING PLENARY DEBATE – LACK OF MEDICINAL PRODUCTS
The globally recognised shortage of medicinal products could be due to a number of factors such overregulation, reduced R&D or an overall decrease in investment – among others. Whatever the reasons, a panel of thought leaders from industry, regulatory authorities and patient organisations will debate the hot issues around this thought provoking subject. The discussion will be moderated by a journalist with an in-depth knowledge of medicines development.
The annual DIA Awards Ceremony will take place during the opening plenary.
EUROMEETING 2013 PROGRAMME OVERVIEW
The themes for the EuroMeeting 2013 include the professional disciplines of regulatory affairs, safety and efficacy for human medicines, diagnostics and devices. Much innovation will be fostered by interaction between disciplines and jointly between the stakeholders of healthcare innovation such as industry professionals, academia, regulatory competent authorities, patient representatives, and the general public. The themes and their theme leaders are as follows:
Health Technology Assessment (HTA)/Sustainability of Health Systems in Europe. Luca De Nigro, Coordinator, Drugs Monitoring Registers Unit, Italian Medicines Agency, Italy and Lidia Retkowska-Mika, Head Legal Unit, Office for Registration of Medicinal Products, Poland.
HIGHLIGHTS OF THE 2013 EUROMEETING INCLUDE:
Speakers from the European Medicines Agency, the European Commission, the FDA and other regulatory agencies from European countries and other regions of the world
Unparalleled multi-disciplinary networking opportunities
Student and professional poster sessions
Active involvement of patient organisations
Pre-conference tutorials led by expert faculty
Hot topic sessions
More than 200 exhibitors on one of the largest exhibition floors in Europe

83
Development of Medicinal Products for Paediatric, Elderly and other Special Populations. Gesine Bejeuhr, Senior Manager Regulatory Affairs/Quality, vfa Research-Based Pharm Companies, Germany and Markus Pasterk, COO and VP of Science, International Prevention Research Institute, France.
Legal/Transparency/Risk & Litigation. Burkhard Sträter, Lawyer, Kanzlei Sträter, Germany.
Pharmacovigilance. Vicki Edwards, Senior Director, European Pharmacovigilance, Abbott, UK, Jan Petracek, CEO, Director of Pharmacovigilance Services, Pharminvent, Czech Republic.
Clinical Research and Development. Andrei Kravchenko, Head of Office, Harrison Clinical Research, Ukraine and Nermeen Varawalla, Founder and CEO, ECCRO, UK.
Quality (including Falsified Medicines). Susanne Keitel, Director, European Directorate for the Quality of Medicines and Healthcare (EDQM), Council of Europe, EU and John Kerridge,
Quality Leader, EU QA External Relations, Lilly, France.
Devices & In Vitro Diagnostics and Combination Products. Shayesteh Fürst-Ladani, Managing Director, SFL Regulatory Affairs and Scientific Communication, Switzerland and Sinisa Tomic, Counsellor for European Affairs, Agency for Medicinal Products and Medical Devices, Croatia.
eHealth. Rob Middel, Head of Operations, Director, Quality Management Center of Excellence, Global Development Organisation, Janssen Biologics, Netherlands and Hans van Bruggen, Director, Electronic Common Technical Document (eCTD) Consultancy, Netherlands.
Involvement of Patients and Academia as Experts in the Drug Approval Process. Gonzalo Calvo Rojas, President of the European Association for Clinical Pharmacology and Therapeutics (EACPT), Spain and Judith Creba, Head EU Liaison & Policy, Novartis, Switzerland.
Known Active Substances Marta Marcelino. Member CMDh, Medicines Evaluation Department, National Authority of Medicines and Health Products (INFARMED), Portugal and Maren von Fritschen, Director Regulatory Affairs, PharmaLex, Germany.

GLOBAL FORUM | V
OL
4
IS
SU
E 5
84
gfgf
Anti-Infective Treatments. Norbert Clemens, Managing Director, Head of Clinical Development, CRS Mannheim, Germany and Marc Sprenger, Director, European Centre for Disease Prevention and Control (ECDC), Sweden.
Effectiveness and Efficiency of the EU Regulatory system - Does new legislation enable innovation and facilitate co-operation? Melek Bostanci Önol, Head of Regulatory Affairs & Quality Assurance, Boehringer Ingelheim, Turkey and Isabelle Stöckert, Head Global Regulatory Affairs EU/CAN, Bayer Pharma, Germany.
Globalisation. Christer Backman, Member CMDh, EU Coordinator and Senior Expert, Medical Products Agency, Sweden and Ning Xu, Executive Director, Head of CDS, Covance Pharmaceutical R & D, China.
Regulatory Science. Christine Gispen-De Wied, Clinical Coordinator; Member of SAWP, Medicines Evaluation Board (MEB), Netherlands and Hubert Leufkens, Chairman, Medicines Evaluation Board (MEB), Netherlands.
Growing Demand for Quantitative Approaches in Drug Development. Jürgen Kübler, Global Head, Clinical
Sciences, CSL Behring, Germany and Steven Teerenstra, Statistical Evaluator, Medicines Evaluation Board, Biostatistics Working Party (BSWP), Netherlands.
Non-Clinical. Jan Willem van der Laan, Senior Pharmacological Toxicological Assessor, Medicines Evaluation Board (MEB), Netherlands.
The IMI Public-Private Partnership in Medicines Research Education and Training - for Professionals and for Patients. Fritz Bühler, IMI Pharmatrain, European Center of Pharmaceutical Medicine, ECPM Executive Office, University of Basel, Switzerland and Hans Lindén, Leader European Projects , European Federation for Pharmaceutical Sciences (EUFEPS), Sweden.
PATIENTS, STUDENTS & YOUNG PROFESSIONALS
The DIA Patient Fellowship, now in its seventh year, is a programme to promote the participation of representatives of patient organisations at the EuroMeeting. DIA fully supports 22 patient representatives covering their
complete travel and accommodation costs plus complimentary admission to the EuroMeeting, and provides 25 additional patient representatives complimentary registration for the Meeting.
DIA keeps students up to date on the latest industry
information through programmes and events that help them gain a real-world understanding of how education can be applied directly to their professional careers.
In addition to discounted student registration fees to attend the full conference, the EuroMeeting features special programmes for students to network and get valuable feedback and insight from professionals in the pharmaceutical sector.
DIA Europe promotes the participation of students in the annual EuroMeeting by offering up to 15 complimentary registrations for full-time under graduate students. DIA Europe also promotes the participation of young professionals in the annual EuroMeeting by offering up to 15 complimentary registrations for professionals under the age of 30.
FOR MORE INFORMATION ABOUT THE 25TH ANNUAL EUROMEETING CONTACT [email protected]
And for more information about how to enjoy Amsterdam please visit www.iamsterdam.com.
fal
of 30.

85
Now in its 13th year, the catching line for this milestone event taking place in Munich 28-30 November is “keep discovering.” Discovery is a central part of our jobs and our lives. Discovery of new pharmaceuticals, of course, but also discovery of better ways of working; new technologies, new requirements. For many years the main focus of Electronic Document Management (EDM)
was to create, assemble and deliver registration dossiers to regulatory agencies.
Thanks to relentless efforts, we have now reached a point where this part is well understood and controlled. Now our focus is shifting to other parts of the EDRM universe: management of clinical documents (eTMF), dossier lifecycle management, new ways of creating content (XML, component-based authoring), and new business models (service-
DIA Conference on European Electronic Document
Management
Munich, venue for DIA’s Conference on European Electronic Document Management

GLOBAL FORUM | V
OL
4
IS
SU
E 5
86
gfgf
based EDRM, cloud computing). At the 13th DIA Conference on European Electronic Document Management we are, and will always be, at the forefront, discovering ever new ways of making technology serve a changing business environment.
In the past, DIA’s EDM Conference has attracted wide interest from across the document management world, including academic researchers, agency representatives (e. g. inspectors and reviewers), clinical operations representatives, CMC regulatory compliance specialists, CROs, CMOs and service providers. Also, document and records managers, IT and support personnel, medical and technical writers, pharmacovigilance professionals, quality assurance and compliance professionals, regulatory affairs/operations representatives.
Our conference gets off to a flying start with two pre-Conference full-day Tutorials on Wednesday, 28 November 2012 with Tutorial 1, Electronic Trial Master File(eTMF) – Migrating From Paper Trial Master Files To Electronic, Tutorial 2, Effective Document Migration Strategies: Understanding Bear-Traps and Honey Pots and Tutorial 3, EVMPD.
Programme Co-Chairs Anita Paul, Head of Corporate Records Management, F. Hoffmann La-Roche AG, Switzerland and Hans van Bruggen, Senior Regulatory Affairs Consultant, eCTDconsultancy, the Netherlands then lead a busy and stimulating programme covering New EDM Opportunities, EVMPD/IDMP, Cloud Legal Aspects and risk management, TMFs – Electronic and Paper Lifecycle Management,
Submission Planning, Registration Tracking, eCTD Lifecycle, Module 3 Lifecycle and Templates, eTMF Reference Model/eTMF implementation, RPS, EDM Integration, Long-Term Preservation, Data Migration, Inspection — experience, expectations, and Regional Regulatory Requirements. There will be panel discussions as well as a “Meet the Regulators” session featuring invited guests from the FDA, MEB, BfaRM and more.
The Programme Committee for the conference consists of Thomas Altenwerth, Consultant, Germany, Joris Kampmeijer, Head of Information Processing, Medicines Evaluation Board, the Netherlands, Dimitri Stamatiadis, Director Management Processes, Merck Serono, Switzerland and Bran van den Brink, Global Heads Records Operation Center, Regulatory Operations, Abbott Healthcare Products B. V, the Netherlands.
UPCOMINGEVENTSEUROPE
Joint BfArM/DIA Statistics Workshop17-19 October 2012Bonn, Germany
Workshop on Local Tolerance Testing for Topical Products: From science to regulations29-30 October 2012Berlin, Germany
GCP Forum14 NovemberLondon, United Kingdom
Clinical Trial Registries Conference15-16 November 2012London, United Kingdom
Impact of the New Pharmacovigilance Legislation on Regulatory Affairs20-21 November 2012 London, United Kingdom
Quality Risk Management Conference26-27 November 2012London, United Kingdom
13th Conference on European Electronic Document Management (eDM) and Exhibition28-30 November 2012Munich, Germany
87
INDIA
The Tamil Nadu Chapter, founded in February 2009 as DIA’s first Chapter in India for students and young professionals, is unique because it encompasses not only university students but research students from government and private educational institutions as well. On August 18, this Chapter presented a Regulatory Affairs workshop at the National Institute of Research for Tuberculosis (NIRT) in Chennai. Dr. Annabelle Rajaseharan served as Chair.
Students and academics from twelve medical/pharmacy colleges plus young professionals from pharmaceutical companies, CROs
and other organizations came from Chennai, Chidambaram, Coimbatore, Madurai and Pondicherry to listen with great enthusiasm to leading regulators from the US FDA, the Central Drugs Standard Control Organization (CDSCO) and the Directorate of Drug Control, and industry leaders.
The workshop was opened by Mr. R. Poornalingam, IAS, Former Secretary to the Government of India; during his tenure as Health Secretary to the Government of Tamil Nadu, he set up the Tamil Nadu Medical Services Corporation to ensure the availability of quality medicines,
Tamil Nadu Student Chapter Regulatory Workshop
ANNABELLE
RAJASE-
HARAN
MD, MBAHead, Tamil Nadu Student Chapter

GLOBAL FORUM | V
OL
4
IS
SU
E 5
88
gfgf
at a competitive cost, to the poor being cared for in government hospitals. He spoke about quality and safety in the drugs
available to the people of India, especially the poor. Greetings were also offered by Dr. S. Soumya, Director of NIRT, and by Dr. Mohanasundaram, Dean, Melmaruvathur Adhiparasakthi Institute of Medical Sciences & Research (MAPIMS).
Keynote Speaker Dr. Albinus D’sa, Deputy Country Director of US FDA’s India Office, spoke of the growing challenges faced by the US FDA. Globalization has poured pharmaceutical products through US through ports, and annual imports through airports have shot up to two trillion dollars. Today’s boundaries are no longer barriers and products can no longer be inspected only at your borders. This has led to the global presence of the FDA, such as FDA’s New Delhi office in India, he said.
Because the FDA has focused on building its regulatory science and capacity, Dr. D’sa noted, he was very happy to note that this Workshop was well attended by Tamil Nadu’s drug
inspectors (regulators). Through several broad initiatives across its offices all over the world, FDA obtains better and more robust
information to help officials in their Centers and at US borders make better decisions about the products that are being developed for the US market, being reviewed for US marketing authorization, are being presented for entry into
the US, and are already on the US market. Dr. D’sa subsequently explained that regulators must be vigilant, strategic, quick and visible in order to be strong and effective.
Mr. P.B.N. Prasad, Deputy Drug Controller of India for South Zone, described the regulatory structure in India and administrative
measures the CDSCO has taken to improve regulatory efficiency and transparency. Mrs. Vijayalakshmi, Assistant Drug Controller of Tamil Nadu, explained proactive measures taken by the Directorate of Drug Control of Tamil Nadu, including the recent banning of certain drugs.
Regulating and assessing the efficacy and safety of drugs, their manufacturing quality, and their distribution and accessibility, is complex and differs from country to country. Regulations from Latin America, the Middle East, the Far East, other ASEAN countries, Korea and Africa, were discussed in a very practical way by Dr R. Ezhil Arasan (Chairman of Winlands; Chairman of Dr.VRE Research Laboratories).
Post-lunch sessions were presented by Dr. S. Gunasakaran (Head of Clinical Research
& Medical Affairs, Azidus Laboratories), who delivered an Overview of INDs & NDAs; and by Dr. Arun Kumar (Chettinad Hospitals and Research Institute), whose Overview of CTDs & eCTDs addressed the nuances of data submission through the lifecycle of a drug.

89
Dr. C. Suthakaran of MAPIMS delivered a fitting finale on Audits & Inspections. Medicines are not ordinary consumer products, he explained, and consumers in most instances are not in a position to make informed decisions about when to use drugs, which drugs
to use, how to use them, and how to weigh potential benefits against risks.
The Tamil Nadu Student Chapter reaches out to all students to augment their understanding of issues facing today’s healthcare
professionals, and has presented seminars and workshops on medical ethics, legal issues concerning medicines, biosimilars and documentation in drug research with the help of international, national and local facilitators.
On August 25, DIA’s Student Chapter in Mumbai organized their first seminar, Leaders of Tomorrow, at the Bombay College of Pharmacy. The event was a great success due to participation from 61 pharmacy students representing five pharmacy colleges in Mumbai. Manoj Trivedi of DIA India staff opened the event by introducing the Chapter’s coordinator, Mayur Fariya (a post- graduate College of Pharmacy student) and Kaushik Desai, Director of DIA India.
Mr. Desai delivered an introductory talk about DIA’s activities both in India and on a global level. He emphasized how students would benefit from joining an international association to learn what is happening in drug research, clinical research, regulatory affairs and other developments in the pharma sector around the globe, which will help shape their careers.
Nidhi Saxena (Chairman and CEO of Karmic Life Sciences) described The Leadership Prerogative: Vision, Innovation & Execution. She focused on how to identify the leader in ourselves and how to be dedicated to one’s duties. Leaders, she said, have
three important qualities: Vision, innovation and execution. More importantly, she emphasized, the greatest virtue of a leader is that they are a most humble human being.
Dr. Raja Smarta (Interlink Marketing Consultancy Pvt. Ltd.), a very experienced professional with more than 28 years of service in the marketing field, spoke about Innovations. He explained and illustrated principles of innovation with the help of a video about Mr. Mistry, an Indian innovator who invented “sixth sense” technology – a wearable device consisting of a projector, mirror, and camera, all connected to a computer small enough to fit in your pocket, operated by hand gestures. This video really inspired participants to “think outside of the box.” The event concluded with the Vote of Thanks from Elvis A. Martis, another post-graduate College of Pharmacy student.
In their feedback, participants requested future activities oriented toward the professional “soft skills” that they do not study in their pharmacy curriculum.
Mumbai Student Chapter Hosts “Leaders of Tomorrow”

GLOBAL FORUM | V
OL
4
IS
SU
E 5
90
gfgf
Discover a World of Differencewith DIA Meetings
Join global professionals involved in the discovery, development, and life cycle management of pharmaceuticals, biotechnology and related medical products
9th Annual Meeting Japan 2012Importance of Development Strategies for Life Cycle
Management of Safe and Effective Medical Products
Toshi Center Hotel, Tokyo, JapanNovember 19-20 2012
DIA JAPANNisso 22 Building 7F
1-11-10 Azabudai Minato-ku Tokyo 106-0041 Japan
Tel. +81.3.5575.2130 | Fax +81.3.3583.1200 [email protected]
Asia Regulatory Conference 2013Regulatory Convergence and Cooperation to Improve Access and Quality
Raffles Convention Centre, SingaporeJanuary 28-30, 2013
DIA NORTH AMERICA800 Enterprise Road, Suite 200 Horsham, PA, USA 19044-3595
Tel. +1.215.442.6100 | Fax [email protected]
Canada Annual MeetingEvolutions in Risk Thinking
Ottawa, Ontario, CanadaNovember 6-7 2012
DIA NORTH AMERICA800 Enterprise Road, Suite 200 Horsham, PA, USA 19044-3595
Tel. +1.215.442.6100 | Fax [email protected]
DIA WORLDWIDE HEADQUARTERS 800 Enterprise Road, Suite 200 Horsham, PA 19044, USA Tel. +1.215.442.6100 | Fax +1.215.442.6199www.diahome.org

91
EDUCATEEDUCATE gfgf

93
Aff ordable Care Act: What Happens Next?
On July 26, nearly one month to the day since the US Supreme Court upheld the Affordable Care Act, DIA presented the webinar Will the PhRMA Deal Stand & What Happens Next? What the BioPharm Industry Needs to Know in the Wake of the Supreme Court Decision Upholding the Affordable Care Act (#12227). Three veteran health law and policy experts, in discussions moderated by John F. Kamp (Coalition for Healthcare Communication), explained what might happen next as reforms from the Affordable Care Act (ACA) continue to evolve.
In his Legal Overview of Decision, former FDA Associate Chief Council Arnold I. Friede (Arnold I. Friede & Associates) discussed how and what the Supreme Court decided about the mandate that requires individuals to either purchase health insurance or pay a tax penalty. The Court evaluated this mandate under the Commerce clause, which gives Congress the authority to regulate commerce, and under the Tax clause, which gives Congress the authority to tax. The Court ruled that this mandate is not valid under the Commerce clause, he explained, because it compels people to engage in an activity that Congress has no authority to compel (commonly referred to as “the broccoli analogy”: Though its health benefits are well-known,

GLOBAL FORUM | V
OL
4
IS
SU
E 5
94
gfgf
for bringing these innovative biologics to the market? Who defines “innovative,” and how? What does “biosimilarity” mean? Is it the same or different from “interchangability?” What’s the difference between “exclusivity” and “patent protection?” Legislators, industry, and regulators need these answers to understand and implement this policy.
The “essential drug list” is another important aspect that seems currrently overlooked, he continued. Does the federal government own and define it, or the state exchanges? Similarly, while we will soon see the formative stages of these state insurance exchanges, no one seems to know what they will look like. “States really are the laboratory of reform,” Mr. Pitts said. “A ‘model state exchange’ developed in the Washington Beltway will be a ‘best practice’ for nobody.”
The panelists and moderator agreed that we’re still in the first few chapters of what’s going to most likely be a very long book. They further agreed that we’ll probably see some reform of the reform, now that the ACA has been upheld, and shared their hope that this political process will center around what’s best for patient care.
Dr. Manning concluded by presenting statistics about the prescription landscape in which the ACA will be implemented. The total number of prescriptions filled by Americans age 65 or older declined by more than 3% in 2011 (after declining by nearly 3% in 2010), but the number of prescriptions filled in 2011 by patients between the ages of 19 and 25 increased by 2%. “The bottom line, for me, is that there are bound to be winners and losers as a result of the Act, and I think it will be, in aggregate, essentially ‘a wash,’” Dr. Manning concluded. “This doesn’t provide a windfall for the industry in any sense.”
Former FDA Associate Commissioner Peter J. Pitts (Center for Medicine in the Public Interest) delivered the webinar’s final presentation, Moving from Healthcare Reform to Healthcare Evolution – Because One Size Cannot Fit All. Now that the ACA has been upheld, he asked, how will bringing approximately 20 million new people into the insurance market actually work? Young people entering the insurance market for the first time, and senior citizens who utilize Medicare Part D, have very different perspectives on the value of health insurance, and very different needs, he explained.
Another important question which nothing seems to definitively answer, is how does FDA create its regulatory pathway
Congress cannot compel citizens to buy and eat broccoli, no matter how good it may be for them). But this mandate was upheld under the Tax clause because it imposes a tax penalty on citizens who do not have health insurance, and Congress has authority to impose a tax.
The second important aspect of this decision, Mr. Friede explained, was the ACA’s requirement that state Medicaid programs cover everyone whose income is below 133% of poverty level, and if they refused, the state would forfeit funds already received through the current Medicaid structure. The Court ruled that Congress cannot take away previously awarded funds.
Richard Manning, PhD (Bates White Economic Consulting) reviewed its Implications for the Pharmaceutical Industry. “What’s it going to do to our particular issues in our business?” he asked. Industry will primarily benefit from an expanded insured population – which will grow through the expansion of Medicaid and insurance purchased through state exchanges by citizens who don’t want to pay the tax penalty – from closing the Medicare Part D “donut hole” and from twelve years of data exclusivity for innovative biologics. Of course, he continued, few benefits come without attendant risks: Industry will most likely be expected to subsidize closing that “donut hole” and will be subject to potential payment reviews and restrictions by the new Independent Payment Advisory Board created by the ACA.

95
As CDER, CBER and CDRH work toward all-electronic environments that facilitate the review of applications and submissions, the perennial Annual Meeting highlight The State of Electronic Submissions at CDER, CBER & CDRH (Session 394) provided an overview of review center goals and practical advice to sponsors. “We have a unique offering for you: An opportunity to hear from all three FDA Centers and where they are with electronic submissions and other related initiatives,” said Gary M. Gensinger, MBA (Office of Business Informatics, CDER), who served as chair.
Before the Centers’ updates, Hilmar Hamann, PhD (Office of Business Informatics, CDER) delivered an overview of Electronic Submissions: The Final Frontier. He noted that standardized electronic submissions have grown
many times over since 2007, at a relatively steady pace of about 6000 new entity registrations per year. Dr. Hamann then explained that PDUFA V and related Biosimilar and Generic Drug User Fee Acts (the “UFAs”) provide the legislative mandate for electronic submissions, implemented through legally binding guidance that will initially focus on eCTD 3.2.2. Electronic submission of NDAs/ANDAs will be mandatory by December 31, 2015; electronic submission of commercial INDs will be mandatory by December 31, 2016. “They all have standards for electronic submissions to drive efficiencies and streamline the submissions process,” he said.
The Center for Devices & Radiological Health (CDRH) Update presented by Terrie Reed, MLS, MS, overviewed specific initiatives that will improve the data management and governance
REGULATORY ROUNDUPDIA 2012: CDER, CBER & CDRH
Electronic Submissions
“Th e DIA Annual Meeting off ers not only a wealth of knowledge, but a great network of fabulous connections!””

GLOBAL FORUM | V
OL
4
IS
SU
E 5
96
gfgf
and analyze your sample eCTD; the eData team helps validate, load and troubleshoot data sets, and helps with legacy data submissions. Current workloads promise to keep both teams busy: The number of eCTD submissions received in 2011 was more than twice the number received in 2008. She overviewed the tools and systems that the Center is currently using, and the file types accepted, for submissions. “We’ve said time and again that we prefer the ESG,” she reminded attendees.
Next, Ginny explained the difference between a “rejected” eSubmission and a “refuse to file”: “Rejection” generally happens for a technical reason that prevents the Center from loading, reading, or archiving your submission; “refuse to file” indicates a gross error or omission in your submission. Approximately 1% of submissions are rejected; 50% of rejections are duplicate submittals.
Ginny concluded with an overview of pertinent CDER projects, such as:
An update of eCTD Module 1 that allows applying one submission to multiple applications (bundling) and allows the CDER Office of Prescription Drug Promotion (OPDP, formerly the DDMAC) to accept eCTD submissions.
New validation codes and software updates, including Global Submit 2010, currently planned for January 2013 implementation.
Automated validation, loading and versioning of study data.
(ESG) that industry will use to submit that work, and the backend systems behind the Center’s receipt of that work. These include:
Developing an eSubmitter program that delivers Individual Case Safety Reports directly to the CBER Electronic Document Room (EDR). This was completed just a few weeks before this session, with pilot testing by “the big four” vaccine corporations scheduled for July and August. “This is what I call a classic example of working in cooperation with our regulated industry,” Michael said.
Finalizing guidance for electronic Lot Distribution Data (eLDD) in an XML-based Structured Product Labeling (SPL) format so that eLDD SPL submissions can be automatically processed via the ESG. “The result of proceeding in this manner is that it will be easier for the Agency to determine if there is a pharmacovigilance issue and to identify that issue with a product because the SPL presentation is user friendly and that presentation lends itself to data mining,” Michael explained.
Updating FDA fillable Form 356h and fillable Form 1571 to facilitate their electronic submission (an announcement that received spontaneous and hearty audience applause).
The Center for Drugs Evaluation & Research (CDER) Update presented by Virginia Hussong began by illustrating a recent reorganization that created two teams for electronic data and document solutions: The eSub team provides general help with electronic submissions, and will even review
aspects of eSubmissions in the pre- and post-market environments:
for future paperless eSubmissions that better meet internal and external business requirements.
for complete, clean and consistent definitions for core data, and CDRH-specific data vocabularies, identification systems and formats.
Participating in the
, and working through a Device Subgroup to include device requirements in CDISC.
Terrie turned to review another current and important initiative: In 2007, Congress passed legislation directing FDA to establish a unique device identification system for medical devices which is consistent, unambiguous, standardized, unique at all packaging levels, and internationally harmonized. Different from, and more specific than, the device lot number or even serial number, the Unique Device Identifier (UDI) will not only aid in recalls but will improve signal detection for adverse event reports, and make registries more effective because they will collect more complete and accurate information. “We can improve the timeliness and effectiveness of recalls because we can identify the device,” Terrie explained. “When something’s being recalled in the device world, it’s very difficult to find out where that device is.”
The Center for Biologics Evaluation & Research (CBER) Update presented by Michael B. Fauntleroy overviewed initiatives that affect how industry will work, the Electronic Submissions Gateway

97
The final day of the DIA Annual Meeting has traditionally featured the two-part CDER Town Hall, where attendees have the opportunity to ask questions and receive immediate feedback from CDER leadership. The DIA 2012 Annual Meeting CDER Town Hall (Sessions 413 & 425) provided nearly three hours of give and take on critical regulatory topics between these regulators and the constituents they regulate: Tom Abrams: Director, Office of Prescription Drug Promotion; Dr. Gerald Dal Pan: Acting Director, Office of Surveillance & Epidemiology; Dr. John Jenkins: Director, Office of New Drugs; Captain Justina Molzon: Associate Center Director for International Programs; Dr. Robert Temple: Deputy Center Director for Clinical Science; and Julie Zawisza: Director, Office of Communications. Gary Gensinger (Deputy Director, Office of Business Informatics, CDER) also joined the panel to address questions about electronic submissions. Dr. Nancy Smith, ORISE Fellow at FDA and Program Chair of DIA’s 45th Annual Meeting in San Diego (2009), served as moderator. “This is your session,” Dr. Smith reminded attendees. “Our objective is to learn about hot topics, but you’re going to tell us what those hot topics are.”
In response to a question, Dr. Dal Pan expanded upon the background and purpose of
the April 2012 draft guidance for industry, “E2C(R2) Periodic Benefit-Risk Evaluation Report,” which updates and combines two ICH guidances, “E2C Clinical Safety Data Management: Periodic Safety Update Reports for Marketed Drugs” (E2C guidance) and “Addendum to E2C Clinical Safety Data Management: Periodic Safety Update Reports for Marketed Drugs” (addendum to the E2C guidance). This draft guidance describes the format, content, and timing of a periodic benefit-risk evaluation report (PBRER) for an approved drug or biologic; the harmonized PBRER is intended to promote a consistent approach to periodic postmarket safety reporting among the ICH regions and to enhance efficiency by reducing the number of reports generated for regulatory submission.
Dr. Temple and Capt. Molzon teamed to answer a question about multi-regional clinical trials: When different countries request country-specific changes to a multi-regional clinical trial protocol, how do you reflect that in the IND? CDER knows that country-specific changes to protocols can create statistical issues, explained Capt. Molzon from her international perspective, and continues to work to resolve these issues.
What changes or new activities can we expect to see from CDER
REGULATORY ROUNDUPReport from DIA 2012
CDER Town Hall
Dr. John Jenkins, Director, Offi ce of New Drugs
Dr. Nancy Smith moderates DIA 2012 CDER Town Hall
Dr. Robert Temple, Deputy Center Director for Clinical Science, CDER

GLOBAL FORUM | V
OL
4
IS
SU
E 5
98
gfgf
A number of guidances called for in PDUFA IV aren’t finished yet, said Dr. Temple, and finishing those will be an important priority. Tom explained that his office will continue to focus on developing policy for communication of risk information, and for use of social media in product promotion.
“The first one is ‘The Program’ for NMEs and BLAs that comes into effect October 1,” said Dr. Jenkins. “That’s a major cultural change.”
“Basically, just to continue to work toward regulatory cooperation,” said Capt. Molzon, “because regulatory authorities have been blessed with much work to do.”
“Our work doesn’t stop and our knowledge doesn’t stop when the drug is on the market,” Julie continued. “How do we balance the need to get information out urgently and responsibly without causing a panic?”
“It’s very much a priority for us and I appreciate that question,” she concluded.
The Town Hall concluded with each presenter summarizing their organization’s most important short- and long-term goals. Julie said that implementation of PDUFA V will require a lot of public communication about drug safety and other programs. “We’re also working very hard to improve our own website,” she concluded.
after the re-authorization of PDUFA (PDUFA V), particularly in the areas of the patient perspective on benefit/risk, and SENTINEL and other post-marketing adverse event initiatives? “We have agreed that we’re going to conduct twenty public meetings to request public input on twenty different disease areas,” explained Dr. Jenkins (one meeting per quarter for all five years covered by PDUFA V).
“We’ve been working for a while now on a structured benefit/risk approach for products,” he continued. “The framework is a qualitative document, not a quantitative one. It does not intend to reduce benefit/risk to an equation.”
“We’ve been talking a lot about risk-based monitoring,” Dr. Temple added.
The ICH E5 Guideline for Ethnic Factors is now fourteen years old, and while the US and Europe don’t seem to care much, this remains a hot topic in Asia, said another attendee. Why don’t countries like the US worry about ethnic factors in Asia? Most multinational clinical trials, explained Dr. Temple, have shown that it’s very rare that a drug works in one region but not in another. Capt. Molzon further explained that China, Japan and Korea had formed a tripartite commission to explore this specific issue.
What is the FDA doing to communicate their position on benefit/risk analysis and uncertainty? “It goes without saying that the Agency has to communicate in a timely and relevant way,” Julie began. We know what patients really want to know: “Is it okay for me to take this drug or not? Is it okay for me to give this to my child or not?”
Understand the Regulatory Frameworks for Drug/Device Combinations and Drug/Diagnostic Pairs
DIA WORKSHOP:Regulatory Considerations for Drug/Device Combinations and Companion DiagnosticsNovember 7-8 | Washington DC
Register by October 17 at www.diahome.org/combo and SAVE!
99Combination products are defined by FDA in 21 CFR 3.2 (e) and can be categorized as (1) products that are chemically, physically or otherwise combined as a single entity (e.g. drug eluting stents, transdermal patches), (2) products that are packaged together (e.g. drug with a delivery device), (3) drugs, devices, or biologics packaged separately but labeled for use together and where both are needed to achieve the intended purpose, where approval of the combination will require labeling changes (e.g. photosensitizing drug and activating laser), (4) investigational drugs, devices, or biologic products packaged separately but labeled for use together and where both are needed to achieve the intended purpose.
Fixed dose drug combinations consisting of 2 or more combined drugs are not technically combination products in the US in that they do not meet the definition in 21 CFR 3.2 (e). Fixed drugs combinations are regulated under 21 CFR 300.50 and FDA has provided separate guidance. Likewise drug and cosmetic combinations and drug and dietary supplement combinations are not “combination products” under 21 CFR part 3.2 (e); these products are regulated as drugs in FDA’s Center for Drug Evaluation and Research (CDER). Human Tissue and Cellular Products (HTC/Ps) that are more than minimally manipulated are regulated as medical devices or biologics depending on how these products are combined and used.
President,Regulatory Advantage, LLC
Combination products are therapeutic and diagnostic products that combine drugs, biologics, and medical devices in one of 4 possible combinations: drug/device, drug/biologic, biologic/device and drug/biologic/device.
REGULATORY ROUNDUPRegulatory Consideration for
Combination Products

GLOBAL FORUM | V
OL
4
IS
SU
E 5
100
gfgf
REGULATORY STRATEGY
Generally only one application is required by FDA for marketing approval of a combination product. Clinical studies will be conducted under an IND or IDE and the combination product will be reviewed and approved as an NDA by CDER, a BLA by CBER or CDER (for well-characterized biotechnology products) or a PMA or 510(k) by CDRH or CBER (for certain blood-related medical devices). The lead agency assignment has a significant impact on the regulatory pathway, time to approval, postmarketing requirements, and cost. Development and strategy efforts involve different approaches to preclinical, clinical studies, CMC and compliance, adverse event reporting, advertising and promotion, and postmarketing activities. For combination products, intercenter collaboration and consultations are standard and the safety requirements of each individual component, as well as the combination must be demonstrated to FDA’s satisfaction. Although many administrative and application requirements for drugs and biologics have been harmonized, the requirements and expectations for drugs and biologics compared to medical devices can be significant. For example, medical device applicants with an approved product intending to add a biologic component such as a stem cell to a next generation product, may find the combination assigned to CBER rather than CDRH with an array of new and unanticipated expectations.
Product Classification Issues and Interpretation of the Term “Chemical Action” in the Definition of Device under Section 201(h) of the Federal Food, Drug, and Cosmetic Act. Assignment of lead agency is based on Primary Mode of Action (PMOD) of the combination product. Data to support the proposed jurisdictional assignment are submitted and sponsors typically present their best case for assignment to a preferred review center. OCP will determine within 5 days if the RFD is reviewable and is mandated to issue a jurisdictional decision within 60 days. The graph below (modified to combine years) shows data from FDA’s website with the number of RFDs filed per month for fiscal years 2011 and 2012 through May 2012. In Fiscal year 2011 OCP filed 43 RFD requests and for fiscal year 2012 through May, OCP filed 28 RFD requests.
JURISDICTIONAL DECISIONS
The Office of Combination Products (OCP) within FDA’s Office of the Commissioner was established as mandated by the Medical Device User Fee and Modernization Act of 2002 (MDUFMA I) to facilitate jurisdictional decisions for assignments of combination products to a lead center, CDER, CBER, or CDRH. Sponsors of combination products can submit a formal Request for Designation (RFD) under 21 CFR 3.7. OCP issued a guidance, How to write a Request for Designation in April 2011. OCP also issued 2 guidances in June 2011 to assist applicants in the RFD process: Classification of Products as Drugs and Devices & Additional

101
device combinations historically reviewed under CDRH may be looked at more closely by CBER in future applications.
Global development of combination products presents unique challenges due to differences in definition of a combination product and regulatory pathways for medical devices. For example, in the EU a device intended to deliver a medicinal product is regulated as a device and the medicinal product in the device is regulated as a medicinal product. If the device and medicinal product form a single integrated product for single use (e.g. asthma inhalers, transdermal patches), the product is regulated as a medicinal product but certain requirements of the Medical Device Directive (MDD) must be met. If the combination product contain a cellular or tissue component it is regulated as an Advanced Therapeutic Product regardless of the contribution on the medical device. Due to these regulatory complexities, harmonization of combination product requirements is unlikely for the near future.
expedited reporting and 7-day written reports for blood related fatalities associated with collection or transfusion. FDA issued a proposed rule for postmarketing safety reporting for combination products that appeared in the Federal Register in October 2009 and has proposed regulations for postmarketing requirements for combination products to be codified as 21 CFR part 4 as subpart B. To date neither the cGMP nor Postmarketing Safety Reporting proposed rules have been finalized.
FUTURE FOR COMBINATION PRODUCTS
FDA expects to see a continuing increase in combination products in the upcoming years. Technological advances have provided new ways to deliver existing products through innovative delivery systems, improvement in outcomes have been shown using therapeutic combinations and an increased number of companion diagnostics are being developed for personalized medicine and to assure the safety of patients.
Industry may see some reclassification of existing combination product types based on FDA’s reassessment of mode of action or regulatory classification. For example more scrutiny and reevaluation are being given to certain components previously regulated as medical devices but now being assessed as drugs. Likewise stem cells and
GUIDANCE FOR COMBINATIONS
The greatest challenge for companies developing combination products is meeting the scientific and quality requirements to support the safety and efficacy of each component, as well as the final combination product. The agency has provided guidance for combination product sponsors/applicants to meet requirements for cGMPs in its 2004 draft guidance, Current Good Manufacturing Practice for Combination Products. The guidance on when drug and device GMPs are to be followed and provides guidance on incorporating Quality Systems requirements with pharmaceutical GMPs for products combined as one entity or packaged together. FDA issued a proposed rule in the Federal Register in September 2009 that clarifies and supplements the guidance and is intended by FDA to eventually be codified in 21 CRF part 4 subpart A.
One area where requirements for drugs and biologics differ significantly from the requirements for medical devices is in safety reporting. Although in general drugs and biologics have been largely harmonized for some time, there are some specific requirements for blood-related products and medical device reporting frameworks that differ from those of drugs and biologics. Product type specific reporting requirements include: 5-day safety reports and 30-day malfunction report for devices, 15-day postmarketing alert reports for drugs and biologics, 3-day field alert reports for drugs, and

The Accreditation Council for Pharmacy Education (ACPE) and the National Association of Boards of Pharmacy (NABP) have collaborated on the CPE Monitor, an electronic system for pharmacists and pharmacy technicians to track their completed continuing pharmacy education (CPE) credits. The CPE Monitor offers boards of pharmacy the opportunity to electronically authenticate the CPE units completed, rather than requiring pharmacists and pharmacy technicians to submit their proof of completion statements (i.e. statements of credit) upon request or for random audits.
To use the CPE Monitor, pharmacists and pharmacy technicians need to obtain an e-Profile ID through the NABP website at net. DIA has enhanced its credit request system, My Transcript, to record this e-Profile ID, as well as the learner’s date of birth (MMDD), when receiving continuing pharmacy education credit requests.
You might be asking yourself, how will this affect me as a pharmacist? This new change will mean that a pharmacist must submit his/her credit request through DIA’s My Transcript within 45 days after participation in an ACPE-certified CE activity.
Once DIA has received a pharmacist and/or pharmacy technician’s NABP e-Profile ID and date of birth (MMDD), this information will be stored within the DIA user’s profile for future reference. The NABP e-Profile ID and date of birth will be populated in all future CE credit requests with DIA.
DIA has begun submitting data of the 2012 pharmacists requested CEUs through the CPE Monitor. If you have not previously submitted your CPE credit request for your participation in a 2012 activity, please be sure to submit your request through DIA’s My Transcript. My Transcript is available on DIA’s homepage at
, “Login to My DIA,” and click on “My Transcript” on the left side toolbar. Please be sure to submit your credit requests promptly so that you will not be excluded in the data transmission reports to ACPE and NABP.
If you have any questions regarding the credit request process or how to obtain your NABP e-Profile ID, please email Karen Wetzel at [email protected].
ACPE Credit Request Update
VO
L 4
ISS
UE
5
102
GLOBAL FORUM | gfgf

103
Panelists included Marc M. Boutin, JD (Executive Vice President & Chief Operating Officer, National Health Council), CDER Director Dr. Janet Woodcock, and Margaret Anderson (Executive Director, Faster Cures/The Center for Accelerating Medical Solutions), and were live streamed in audio and video on the Post’s website.
In the Forum’s closing session, Mary Jordan interviewed Francis Collins, MD, PhD, Director of the (US) National Institutes of Health. Dr. Collins is a recipient of the Presidential Medal of Freedom
(2007) and the National Medal of Science (2008); in 2009, his nomination to serve as Director of the National Institutes of Health (NIH) was unanimously approved.
In this interview, Dr. Collins enthusiastically described the scientific momentum of discoveries that seem to pour out of laboratories each day, and the challenge of translating these scientific discoveries into safe and effective therapies. “While science is an intellectually satisfying experience, it’s not really rewarding for those of us in
NIH Director Highlights Innovation Forum
On September 13, The Washington Post hosted an Forum at the Ronald Reagan Building in Washington, DC. Moderated by Post Editors Mary Jordan and Frances Sellers, this Forum comprised panel discussions on scientific literacy, job growth and other issues related to medical innovation.
Francis Collins, MD, PhD, Director of the (US) National Institutes of Health

GLOBAL FORUM | V
OL
4
IS
SU
E 5
104
gfgf
makes everything tougher, let’s be clear about that,” he allowed.
“I have the greatest confidence that the trajectory we’re on scientifically will lead to the breakthroughs that we’re all looking for,” Dr. Collins concluded. “We will find the ways to treat, prevent and cure diseases. We can do that. We can do that together.”
Technology & Innovation Foundation (ITIF) titled Leadership in Decline: Assessing US International Competitiveness in Biomedical Research, Dr. Collins noted that budgets /resources are the only limitation to research and innovation at present – there is no shortage of ideas, or of scientific talent interested and qualified to pursue those ideas. “Recession
medical research until that benefit comes forward, and we want to speed that up,” he said.
He cited some examples of therapeutic progress driven by advancing science: Over the past fifty years, infant mortality has decreased by 40%, deaths from heart attack by more than 50%, and deaths from strokes by more than 70%, while someone diagnosed today with HIV at age 21 now has a life expectancy of more than 70 years. He further described how advancements in the field of genetics have improved patient care by, for example, identifying genetic frameworks in which certain drugs have proven to be more effective than others; and described a computerized chip that can be inserted under a diabetic’s skin to continually monitor their blood sugar and other biomarkers (and which someday might be replaced by an artificial pancreas). “We are poised to take those advances to the next level because of our ability to learn new things,” said Dr. Collins.
What future medical innovation is Dr. Collins most excited about?
“Cancer is at an amazing junction. Because of this ability to read the letters of DNA, we’ve learned how to look at a cancer cell and tell you every single reason why that cell went bad,” he said. “This generation of targeted therapies for cancer is starting to look pretty exciting. These are not the ‘carpet-bombing’ kind of drugs. These are the ‘smart bombs.’”
“No more ‘one size fits all,’” he continued. “That is truly dramatic, and it’s coming very fast.”
Referring to a May 2012 report issued by the Information
Two Superb Events at the Same Location!
Discuss the Challenges, Best Practices, and Emerging Role of DMCs.
Data Monitoring Committees: Best Practices and Future Directions Register at www.diahome.org/DMCS
Gain Answers for Solutions to Barriers You Will Face!
DIA Adaptive Designs in Clinical Trials: Overcoming Persistent BarriersRegister at www.diahome.org/Adaptive Designs
November 29-30 Hyatt Regency Washington | Washington, DC
Register by November 8 to Save!
Featuring
Joint
Sessions

105
I believe that effective science-based, public health-focused, drug regulation involves a dialogue amongst stakeholders. Through a variety of venues - advisory committee meetings, open public hearings, public workshops, scientific conferences and regulatory conferences, FDA interacts with its stakeholders. The DIA Annual Meeting is a productive and efficient forum to discuss timely regulatory matters, while the smaller meetings that occur throughout the year provide a venue to discuss specific scientific-regulatory topics.
I think that DIA very effectively brings together industry and regulators, and by doing so fosters an environment that allows for productive discussion of regulatory topics. My experience is that topics that are largely
P RO F I L E
I started in 2004, when I was a division director in the former Office of Drug Safety. I had participated in the CIOMS VI effort, which discussed safety data collection in clinical trials. Fellow CIOMS VI participants and I presented an overview of our work at the DIA Annual Meeting. In a separate session at that meeting, I participated in a panel discussion on Medication Guides. Interest in patient-focused communications was increasing at that time, and the DIA Annual Meeting was a good forum for an industry-regulator dialogue.
Dr. Gerald Dal Pan
On June 12, 2012, the US FDA announced the promotion of Gerald Dal Pan, MD, to the position of permanent Director of FDA’s Office of Surveillance and Epidemiology (OSE), where he had been serving as Acting Director. OSE had recently undergone a reorganization that transformed it from a relatively minor office within the Center for Drug Evaluation and Research into a so-called “super office.” Dr. Dal Pan has served as the head of OSE since 2005, and was made Acting Director of the new office when it was reorganized in June 2011.
A&Q

GLOBAL FORUM | V
OL
4
IS
SU
E 5
106
gfgf
enjoyed the review of IND and NDA submissions. To be able to do more epidemiology, I moved to the Office of Drug Safety (now the current Office of Surveillance and Epidemiology [OSE]) in late 2003, and became its director about two years later. It’s been a somewhat circuitous path from being an academic neurologist to becoming the director of OSE, but the journey has been, and continues to be, wonderful.
Science is the foundation of everything we do at FDA. Advances in biomedical sciences, informatics, and other areas impact the scientific evolution of medicines. Regulatory scientists have to be part of this.
I strongly believe that the education of healthcare professionals has to include formal training on how to use medicines safely and how to manage the risks of medicines. Ideally, this would include an overview of the basic regulations that form the basis of FDA’s oversight of medicines.
Organization. Thus, I interact with people who work within highly developed drug regulatory systems and with people who work within developing drug regulatory systems. What is absolutely clear from this experience is how much we all have in common in terms of our goals and challenges. Everyone want medicines that are safe and effective, and everyone wants better postmarketing safety data.
I really love my job, and yes, I would certainly do it again. But I’m not really sure that I ever “took” this path; rather, I think I followed a trail that led me here. I am trained as an internist and a neurologist, and I always thought I would have a career in academic neurology, mainly in clinical research. To pursue that path, I obtained a master’s degree in clinical epidemiology, an experience that made me realize two things. First, I came to appreciate the extraordinary role that public health plays in improving the lives of large numbers of people. Second, I very much enjoyed the quantitative methods of epidemiology. My early academic work involved both observational epidemiology (cohort studies) and clinical trials of new treatments for nervous system disorders. The latter work peaked my interests in drug development, which led to my moving to a small pharmaceutical company for a few years. I learned lots about drug development in industry, but my interest in broader public health issues kept tugging at me. I joined FDA in July 2000 as a premarket medical reviewer in the Office of New Drugs, and
regulatory in nature tend to have less academic involvement. In contrast, meetings of scientific organizations tend to have very little regulatory discussion. I think that there needs to be a forum for topics that require both academic and regulatory issues. DIA does some of this with its meetings on scientific-regulatory topics. Attracting more academics to such meetings could be helpful.
My undergraduate major was biochemistry, though I pursued a broad liberal arts course of study. After medical school, I trained in internal medicine and neurology. I also have a master’s degree in clinical epidemiology.
The biggest change that I have seen in the last ten years is the increased emphasis on transparency. As society becomes more engaged in health-related issues, healthcare professionals and the public at large are more interested in information on medicines than ever before. As part of our commitment to transparency at FDA, we have developed an active program on drug safety communications. Communicating to the public is an important part of our public health mission at FDA.
I work with international regulators and industry through ICH and through the World Health

107
To address these factors, DIA and the Healthcare Businesswomen’s Association (HBA) have teamed up on a multi-year initiative to accelerate the growth of women’s leadership skills and increase their impact on the changing business and regulatory environments. This exciting initiative, called the DIA/HBA Leadership Project, was launched in June during the DIA 2012 Annual Meeting in Philadelphia.
The DIA/HBA Leadership Project is led by co-chairs Minnie Baylor-Henry, Vice President of Worldwide Regulatory Affairs at Johnson & Johnson Medical Devices and Diagnostics and DIA President-elect, and Ilyssa Levins, President of the Center for Communication Compliance (CCC) and an HBA Corporate Board Director This initiative grew out of friendship and a grassroots movement through shared contacts.
WOMEN IN HEALTHCAREDIA and HBA Collaborate to Address
Challenges in Women’s Leadership
It is well known that women in regulatory, medical, legal, and compliance roles can enhance their organizations’ reputation, value, and diversity while stimulating innovation and maximizing effectiveness of clinical operations. Yet, research shows that a number of factors inhibit the ability of women in these roles to ascend to higher levels of leadership in their organizations.
Founders Ilyssa Levins (CCC) and Minnie Baylor-Henry (J&J and DIA) are joined by Susan Cantrell, Director, North America (DIA) and Laurie Cooke, CEO (HBA) at the DIA/HBA Leadership Project kick-off meeting in June.

GLOBAL FORUM | V
OL
4
IS
SU
E 5
108
gfgf
this number could easily triple,” Baylor-Henry remarks.
Guided by a steering committee of women in senior positions in government, industry, and consultancy organizations, the initiative seeks to achieve its goals by building a community of like-minded professionals who will share insights on how to nurture and inspire leadership, creating and implementing a skill-building roadmap for success, and shaping the direction of women’s initiatives currently underway, or being developed, to support the non-commercial functions. The initial program committee meeting and kick-off event were so successful that the expectation is that it won’t be the last. “We clearly tapped into an unmet need. Company programs have opportunities to network but they are primarily with women in your company; DIA/HBA have a unique opportunity to network with women in similar jobs in other companies” and women became convinced that if we spread the word, this meeting’s numbers could have tripled.
According to Baylor-Henry, “This initiative will build portable and visible skills that go beyond mere technical expertise. It will also establish women in regulatory, medical, legal and compliance as strategic business partners within an organization. Both are practical goals designed to benefit current and future leaders.”
“Our plan is to accelerate leadership development and spotlight the impact these four functions have on our changing business and regulatory environments,” adds Levins.
The hope to foster these types of conversation continued to be fueled recently by the article entitled, “Why Women Still Can’t Have it All,” by Anne-Marie Slaughter that appeared in The Atlantic earlier this year. It became a rallying call for women who wanted to talk to other women about networking, career paths, and what it takes to reach the c-suite, if that is what your goal is.
“Women in these areas don’t tend to end up being the CEO of a company because that is not the pathway in these careers. This is fine for some women; but for others who chose to be senior leaders, a path forward is not as clear if you are in a non-commercial role,” Minnie says. Baylor-Henry and Levins got to work, opening their contact lists and spreading a wide net to see what, if any, interest was out there for this type of mentoring alliance. The response they received was surprising. “We easily and quickly had 150 women who wanted to come and we were convinced if we opened it up even further,
Ilyssa and Minnie have known each other for years and have often spoken about the complementary natures of HBA, whose members are primarily in commercial marketing and DIA, whose membership is largely non-commercial professionals. DIA is a global community focused on advancing the discovery, development, and lifecycle management of pharmaceuticals and other medical products and HBA is the premier catalyst for leadership development of women in healthcare worldwide. When evaluating each organization’s strengths, missions, and services, there is commonality but little overlap, creating an ideal opportunity for synergy in this area. DIA and HBA plan to combine their unique capabilities to carry out this project. Baylor-Henry and Levins conceptualized the initiative after attending an HBA event last fall where the two discussed the needs and challenges of women in regulatory, medical, legal and compliance roles to raise to senior leadership roles.
HBA/DIA RECOMMENDED READING“Letters to My Younger Self” -Ellyn Spragins
What I Know Now About Success: Letters from Extraordinary Women to Th eir Younger Selves

109
make sure that women get and stay engaged. The planning group is working hard to ensure that by developing a clear program to show that the dialog can continue and that members can come together as a community of women interested in being successful- both in their career and in life. “We want to provide an opportunity for women leaders to network with other women in their jobs at different companies, to lift up their heads from their work and share their stories.” After all, every one of us does have a story and we all eventually do get to our destination- in our own way and on our own time. The key is to make sure you are controlling your destiny, deciding where you want to be and setting a path for how to get there.
More than 125 women attended the inaugural event at the DIA Annual Meeting to hear a panel of female leaders share their thoughts on the state of women’s leadership today and to learn more about the project’s vision and to discuss what “having it all” really looks like. The panel discussion was facilitated by Baylor-Henry and panelists included Dr. Freda Lewis-Hall, Executive Vice President and Chief Medical Officer at Pfizer and the 2011 HBA Woman of the Year; RADM Sandra Kweder, MD, Deputy Director of the Office of New Drugs at the U.S. Food and Drug Administration (FDA) and DIA board member; and Tracy Rockney, JD, divisional Vice President of Regulatory Affairs at Abbott Pharmaceutical Products Division. Hailing from a variety of backgrounds, each of these women has become a leader in her field and provided an overview of her personal “roadmap” to where she is in her career. Taking divergent paths, the common bond between them is that they all wound up where they wanted to be. “Our initiative is not only to encourage c-suiters,” says Minnie, “but also for junior level leaders and newly minted professionals who want to understand what a solid development pathway looks like.” Women want to talk about the challenges they are facing at their current levels and how to advance and balance that dream career with their family life. “We all want to be successful,” Minnie continues, “but when you look at some of the sacrifices that are being asked to get to that level, some women decide it is not their pathway.” The challenge for the DIA/HBA Leadership Project is to
Th e conversation continues...
HBA Leadership ConferenceNovember 7-9, 2012, Orlando
DIA 2013June 23-27, 2013, Boston
Look for info on….
A series of white papers on critical issues and challenges facing women in leadership roles
Executive women’s breakfast
Fall get together
JOIN HBA
Visit https://www.hbanet.org/join-hba for details

GLOBAL FORUM | V
OL
4
IS
SU
E 5
110
gfgf
Kickoff meeting of the HBA/DIA Women’s Leadership
collaborative eff ort.

111

GLOBAL FORUM V
OL
4
IS
SU
E 5
112
gfgf
A S S O C I AT I O N N E W SBoard of Director President Ling Su Visits DIA Headquarters
Current DIA Board President Dr. Ling Su addressed the DIA HQ staff recently for the first time since his election in June of this year. After a warm welcome from Worldwide Executive Director Paul Pomerantz, Dr. Su provided an overview of his background and experience over two decades in international pharmaceutical companies and regulatory organizations.
Dr. Su outlined three objectives for his DIA presidency. First was the support of DIA’s growing presence in China. As DIA’s first Asian President, he believes there are “vast opportunities” for DIA as an organization to provide assistance in developing content and training relevant to the China market by extending our services and getting to know our customers in that area and what it is they want and need from us.
He also spoke enthusiastically about the Board’s vision for DIA and efforts over the past year to reposition the organization from a meeting-centric group to a knowledge resource for all our stakeholders. This will be accomplished by the completion of our Digital Initiative, the
globalization of our content and the development of new markets. In addition, Dr. Su briefly spoke about the scenario planning activities of the board as a way to be proactive and prepared for anticipated changes in the healthcare landscape during the next decade.
While speaking to the importance of DIA’s status as an impartial nonprofit in garnering support and involvement from regulators and industry leaders, Dr. Su shared with the staff that his first interaction with DIA was as a student poster presenter at the 1999 Annual Meeting in Montreal. The value he found in that experience kept him involved in DIA and led him from the classroom to the board room.
Lastly, Dr. Su expressed his excitement about the upcoming DIA Board Meeting in Beijing, emphasizing how important he believes it is for the directors to see the country, interact with the major players there, visit the SFDA and experience a high tech and incubator park.“Strategic planning in an open forum of brainstorming with a change of venue,” he concluded, is often a way to stimulate new thinking.
DIA Board President Ling Su (left) accepts an award from Worldwide Executive Director Paul Pomerantz during Dr. Su’s recent visit to DIA Headquarters in Horsham.

113
AAMIR
SHAHZAD
A S S O C I AT I O N N E W S
To help consolidate our members’ knowledge base and understanding of translational medicine, DIA announces the formation of a new Translational Medicine Special Interest Area Community (SIAC). Dr. Aamir Shahzad will serve as Chair.
“The goal of translational medicine is to expedite the development of newly identified compounds to enhance the patient’s quality of life. Translational medicine is the synergy between epidemiology, basic research and clinical trials,” explains Prof. Shahzad. “It results from collaborations between clinics, research hospitals, governments, academic centers and industry, when diseases are identified and candidate therapeutics optimized and tested in cell cultures, humanized small animal models and clinical trials. And yet, despite its importance,
New SIAC for Translational Medicine
there is no single universal definition. Various institutions have tailored their own definitions according to the needs of their field. One of the things our SIAC will work toward is consensus for a universal definition of translational medicine.”
“Translational medicine has become important because of its promise of accelerating pharma and biotech product R&D. Translational medicine (TM) has the potential to guide rapid and effective product development in all clinical phases,” he continues. “However, the general scientific community is not fully aware of translational medicine concepts and objectives. To realize its full promise, there is a need for an international platform to keep industry and academia updated and to provide expertise in this field.”
As economic and humanitarian considerations keep driving science and industry to develop new ways to develop new drug treatments more quickly and efficiently, translational medicine has emerged as a promising field. In January 2012, for example, the US National Institutes of Health launched a new National Center for Advancing Translational Sciences, with the mission of catalyzing the generation of innovative methods and technologies that will enhance the development, testing and implementation of diagnostics and therapeutics across a wide range of human diseases and conditions.

GLOBAL FORUM V
OL
4
IS
SU
E 5
114
gfgf
Annual Meeting, EuroMeeting and other international symposia. We also hope to develop a comprehensive website for the interdisciplinary exchange of current TM knowledge and concepts and to keep members updated with latest developments, educational opportunities and other topics of interest, and a global database of TM experts from the pharma, biotech and medical device industries and academic centers, for potential collaboration opportunities.”
Look for Translational Medicine to soon appear on the list of “Special Interest Area Communities” under “Networking & Communities” on www.diahome.org.
WHAT MESSAGE WOULD THE CHAIR LIKE TO DELIVER ABOUT THIS NEW SIAC?
“This SIAC aims to provide a comprehensive platform on translational medicine and to familiarize our members with the latest TM approaches and tools to enable and accelerate the R&D process in the pharma, biotech and medical device industries. These industries are increasingly aware of the benefits that can be gained, and desire to understand TM approaches and tools to overcome hurdles in R&D is growing,” says Prof. Shahzad.
“We look forward to helping to develop TM education and training under DIA auspices at the DIA
Currently based in Vienna, Austria, Professor Aamir Shahzad is one of the pioneers in the translational medicine fi eld. Prof. Shahzad cur-rently serves as Director of Admin-istration and Secretary General for the International Society for Trans-lational Medicine; he also serves as editor-in-chief for the journals Molecular Medicine & Th erapeutics and Translational Biomedicine. He is Professor of Microbiology (V) and Professor of Medicine (V) at Harbin Medical University (China), and has participated in establishing transla-tional medicine infrastructures for several organizations.
DIA Patient InitiativeAnnual Meeting Patient Fellowship ProgramPatient Advocate Fellowship Alumni ProgramEuroMeeting Patient Fellowship ProgramPhilanthropy Grant ProgramLinkedIn for Patient OrganizationsDIA and PCORIDIA and NORD
Contact [email protected] for more information about these programs and other opportunities for patient organizations.
Customized In-company Training Solutions
Expert training from professionals in the pharmaceutical, biotechnology, and related industriesQuality content and delivery—all at your company locationCourses tailored to meet your specific training objectivesContinuing education credits
Contact [email protected] or visit www.diahome.org/incompany and submit a consultation request.

115
A S S O C I AT I O N N E W S
While DIA’s Digital Initiative reached a major milestone upon the rollout of our new www.diahome.org website in April 2012, website refinements and enhancements continue. Two recent upgrades have made online networking and collaboration more accessible and convenient.
The audio portion of every Showcase that was presented by a DIA Special Interest Area Community (SIAC) at our recent DIA 2012 Annual Meeting was recorded. These audio files and the corresponding slides are now available on the main page for each SIAC so that you can experience, with no login required, a presentation on a topic of essential importance to that specific professional discipline. Please visit “Special Interest Area Communities” under “Networking & Communities” to learn more. Our homepage also features one SIAC Showcase each week, on a rotating basis, to further increase the visibility and accessibility of these online communities.
In addition, “News & Publications” has recently been updated to include archived meetings of DIA’s
Online Community Content Growing
Virtual Journal Club. Presented by the Statistics SIAC, this Club regularly invites the author of a recent Drug Information Journal article to deliver a teleconference presentation, generally an hour, which examines the article topic in more depth. Author slides that reiterate and expand upon the article are distributed in advance for Club members to follow while listening to the call. The recorded teleconference and accompanying slides from Club meetings in March and June 2012 are currently available through the new “Virtual Journal Club” under “Publications & Research.”
Read Your Global Forum
on the
GO
A S S O C I AT I O N N E W S
Dr. Milligan previously served on the Annual Meeting Program Committee for 2010, 2011 and 2012. In 2009, she delivered a presentation for the Annual Meeting session Labeling Risk: Practical Approaches After Wyeth v. Levine, and in 2011 and 2012 chaired a very popular mock trial session/workshop, Mock Trial on Pharmaceutical Company Fraud and Abuse Settlements: Having Conviction to Avoid Conviction/Marketing Practices
SANDRA
MILLIGAN
Dr. Sandra Milligan Named DIA 2013 Program Chair
on Trial. Dr. Milligan also served on the Program Committee for the 2011 Marketing of Pharmaceuticals meeting.
Prior to Genentech, Dr. Milligan served for nearly a decade in various roles for Amgen, including Global Regulatory Therapeutic Area Head for the Bone Franchise, as Head of Regulatory Communications Strategy & Operations, and as Senior Counsel for the Development, Regulatory & Compliance Law Group, where she provided strategy for development, regulatory and safety groups.
Sandra Milligan, MD, JD, a member of the DIA Board of Directors and Vice President Global Regulatory Therapeutic Area Head for Inflammation, Virology and Ophthalmology for Genentech, will serve as Program Chair for DIA’s 2013 Annual Meeting: Advancing Therapeutic Innovation & Regulatory Science, June 23-27, 2013 in Boston, MA.
GLOBAL FORUM gfgfV
OL
4
IS
SU
E 5
116

49th Annual MeetingAdvancing Therapeutic Innovation and Regulatory Science
June 23-27, 2013Boston Convention and Exhibition CenterBoston, MA
DIA 2013Registration Will Open
October 2012
Join more than 7,000 professionalsinvolved in the discovery, development, and life cycle management of pharmaceuticals, biotechnology, medical devices, and related products to unlock the innovation needed to expand global access to effective and affordable patient care.
Program Chair
Sandra A. Milligan, JD, MDGlobal Regulatory Therapeutic Area Head Genentech, Inc.
Reaching crucial industry leadership, creating new business relationships, and tapping some of the brightest minds in the field are all major attractions to the DIA Annual Meeting and are why I will keep coming back.
The
‘must attend’is aDIA meeting
Likely the
on the planet!of its kindbest meeting
Visit www.diahome.org/DIA2013 for more details.

Translation | Back Translation | Desktop Publishing| Independent Review | Editing | Proofreading
When translating documents for FDA submission such as dossiers, CRFs, labeling, adverse event reports, and product information, Corporate Translations understands the critical need for accuracy Our rigorous translation process includes multiple quality inspections, guaranteeing the most accurate translations quickly and cost-effectively. We stand by
with each document. Partnering with Corporate Translations allows you
Translations is the preferred supplier of ISO 9001 translation and
www.corptransinc.com1-855-727-6003
Your FDA submission documents are serious. So are their translations.
dossiers, CRFs, ion, Corporate y Our rigorous s, guaranteeing ly. We stand by
ions allows you
translation and
Your FDA submission documents are serious. So are their translations.
www.corptransinc.com1-855-727-6003
When translating documents for FDA submission such as dossiers, CRFs, labeling, adverse event reports, and product information, Corporate Translations understands the critical need for accuracy Our rigorous translation process includes multiple quality inspections, guaranteeing the most accurate translations quickly and cost-effectively. We stand by
with each document. Partnering with Corporate Translations allows you
Translations is the preferred supplier of ISO 9001 translation and
Translation | Back Translation | Desktop Publishing| Independent Review | Editing | Proofreading

GL
OB
AL
FO
RU
M A
gfgf












![GF Forum 2009 Report en[2]](https://static.fdocuments.us/doc/165x107/577d35c81a28ab3a6b916494/gf-forum-2009-report-en2.jpg)





