
Giulia Veronesi Division of Thoracic Surgery European Institute of Oncology CERIGNOLA 7 MAGGIO 2011...
76
Giulia Veronesi Giulia Veronesi Division of Thoracic Surgery European Division of Thoracic Surgery European Institute of Oncology Institute of Oncology CERIGNOLA 7 MAGGIO 2011 CERIGNOLA 7 MAGGIO 2011 NUOVE PROSPETTIVE NUOVE PROSPETTIVE NELLA PREVENZIONE E NELLA PREVENZIONE E CURA DEI TUMORI CURA DEI TUMORI POLMONARI POLMONARI
-
Upload
clifford-barton -
Category
Documents
-
view
214 -
download
0
Transcript of Giulia Veronesi Division of Thoracic Surgery European Institute of Oncology CERIGNOLA 7 MAGGIO 2011...
Giulia VeronesiGiulia VeronesiDivision of Thoracic Surgery European Institute of OncologyDivision of Thoracic Surgery European Institute of Oncology
CERIGNOLA 7 MAGGIO 2011CERIGNOLA 7 MAGGIO 2011
NUOVE PROSPETTIVE NUOVE PROSPETTIVE NELLA PREVENZIONE E NELLA PREVENZIONE E CURA DEI TUMORI CURA DEI TUMORI POLMONARIPOLMONARI

1) PREVENTION2) ROBOTIC SURGERY
3) TARGET THERAPY

5.4 PREMATURE DEATHS IN 2000
TOBACCO USE REMAINS THE LEADINGPREVENTABLE CAUSE OF DEATH IN THE
WORLD
US Dept of Health and Human Services. Women and Smoking: A Report of the Surgeon General. Public Health Service, Office of the Surgeon General. 2001Ezzati M. Estimates of global mortality attributable to smoking in 2000. Lancet. 2003
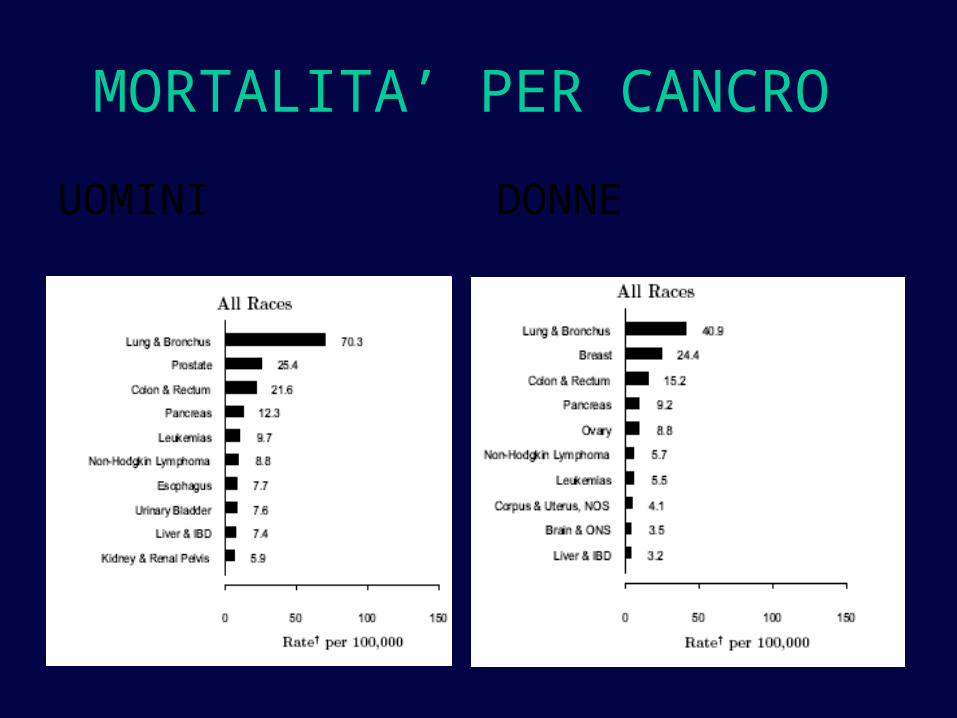
MORTALITA’ PER CANCRO
UOMINI DONNE

THE WORLD HEALTH ORGANIZATION
In 2030Tobacco-attributable deaths:• 3 millions western countries• 7 milions in developing countries

Richard Doll
LUNG CANCER FIRST CAUSE OF CANCER DEATH

ANTI SMOKING CAMPAIGN
LIMITS1) High lung cancer risk in former smokers2) Women and young people 3) Smoking in deveoping countries
Early detection

diametro< 1 cm
SOPRAVVIVENZA A 5 ANNI80-90%
Continous Observation of SMoking Subjects
COSMOS
LD-CT
• Scientific world divided in two groups– Pro RCT > Mortality issue – Contra RCT > Ethical issue
-mortality analysis with historical controls
-proof of principle “early detection is the cornerstone of any effective treatment”

LCST (Lung Cancer Screening Trial)
2002-2010
Nodules > 4mmFurther exams early treatment
53.000 subjects
55 years, 30 packs-year
R3 annual LD TC 3 annual Chest x ray
FUP x 5 years
20% lung cancer specific
mortality reduction
6.9% reduction of overall mortality

CRITERIA FOR IMPLEMENTATION OF CT SCREENING
• False positive cases
• Best target population
• Overdiagnosis
• Best screen interval
• Cost effectiveness analysis
• Radiation exposureNO NEED OF RCT
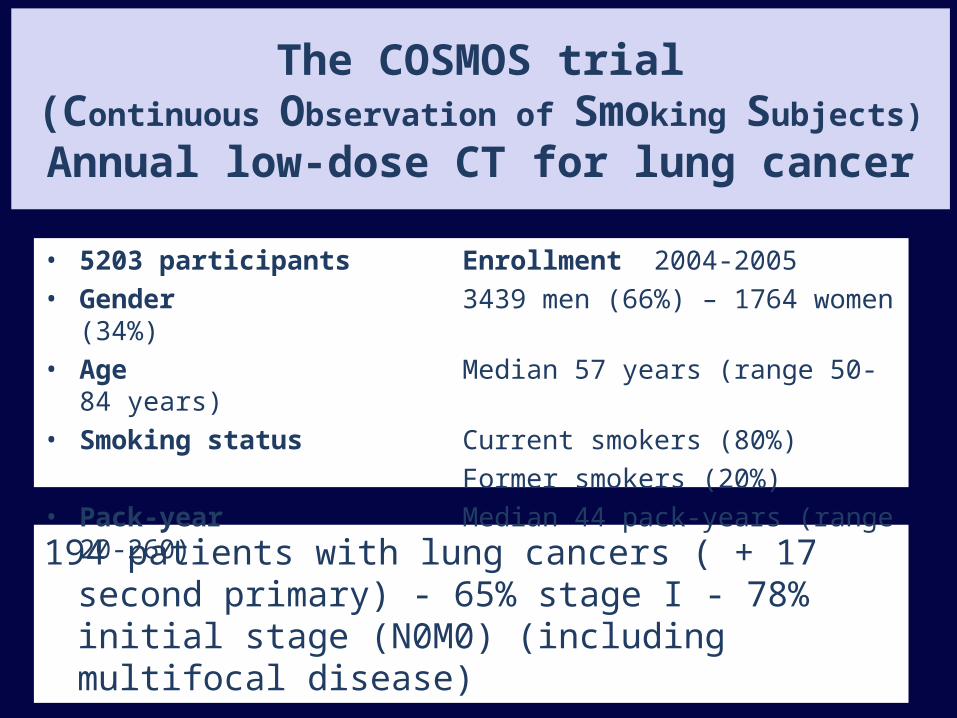
194 patients with lung cancers ( + 17 second primary) - 65% stage I - 78% initial stage (N0M0) (including multifocal disease)
The COSMOS trial(Continuous Observation of Smoking Subjects)
Annual low-dose CT for lung cancer
• 5203 participants Enrollment 2004-2005• Gender 3439 men (66%) – 1764 women
(34%)• Age Median 57 years (range 50-84
years)• Smoking status Current smokers (80%)
Former smokers (20%) • Pack-year Median 44 pack-years (range 20-
260)
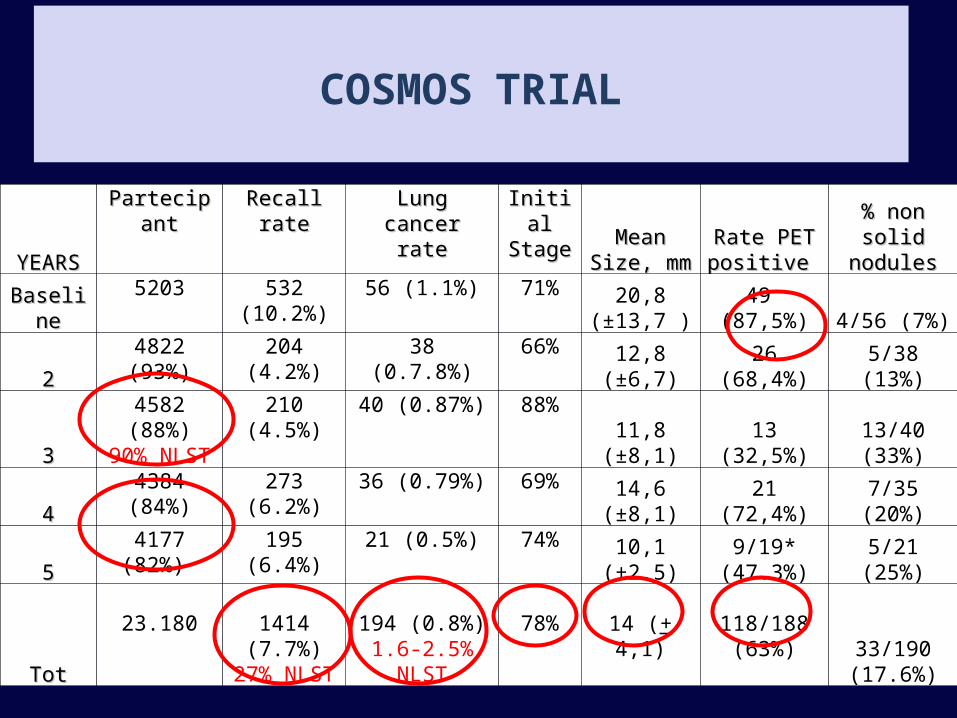
YEARSYEARS
PartecipantPartecipant Recall rateRecall rate Lung cancer Lung cancer raterate
Initial Initial StageStage
Mean Mean Size, mmSize, mm
Rate PET Rate PET positive positive
% non solid % non solid nodulesnodules
BaselineBaseline
5203 532 (10.2%)
56 (1.1%) 71% 20,8 (±13,7 ) 49 (87,5%) 4/56 (7%)
22
4822 (93%) 204 (4.2%) 38 (0.7.8%) 66%
12,8 (±6,7) 26 (68,4%) 5/38 (13%)
33
4582 (88%)90% NLST
210 (4.5%) 40 (0.87%) 88%
11,8 (±8,1) 13 (32,5%) 13/40 (33%)
44
4384 (84%) 273 (6.2%) 36 (0.79%) 69%
14,6 (±8,1) 21 (72,4%) 7/35 (20%)
55
4177 (82%) 195 (6.4%) 21 (0.5%) 74%
10,1 (±2.5)9/19*
(47.3%) 5/21 (25%)
TotTot
23.180 1414 (7.7%)
27% NLST
194 (0.8%)1.6-2.5%
NLST
78%14 (+ 4,1)
118/188 (63%) 33/190
(17.6%)
COSMOS TRIAL

STAGESTAGE
Cosmos study
Stage I65%
Stage II13%
Stage III17%
Stage IV5%
SEER
Screen cancers stage I-II: 78% Non screen cancers stage I-II: 17%

SURGERY
Pneumonectomy 2% versus 10% in the routine Postop morbidity 23.7%, 90 days mortality 0.5%

35 DEATHS after a median follow-up of 64 months
Overall survival (95% CI)
1-year 91% (86-95%) 2-year 85% (80-91%) 3-year 82% (76-88%) 4-year 79% (72-88%) 5-year 72% (63-82%) (60% LCST)
Patients at risk
194 149 119 87 56 16
Years
Lung cancer mortality
1.3/1000-year
SURVIVAL OF SCREENING-DETECTED* LUNG CANCER
* including 6 interval cancers

OVERALL MORTALITY
116 deaths
37 Other primary cancer34 Cardiovascular31 Lung Cancer
9 Other cause5 Unknown cause
5-year survival = 97%
(NSLT Trial 96%)

CRITERIA FOR IMPLEMENTATION OF CT SCREENING
• False positive
• Best target population
• Overdiagnosis
• Cost effectiveness analysis
• Best screen interval
• Radiation exposure

DIAGNOSTIC PERFORMANCE OF COSMOS PROTOCOL
Observed
Negative Lung cancer
Predicted Negative 4976 25
Lung cancer 34 168
Invasive procedure for benign disease =34/5203 in 5 years = 1.3 per thousand every year
FP
NELSON trial NEJM 2009

BENIGN NODULES False positive
False positive cases 15% of all positive cases less than those observed in the routine clincial practice (22%)

Sensitivity of protocol: 168/194 = 87.0%Specificity of protocol: 4976/5001 = 99.5%
PPV: 168/202 = 83.2%NPV: 4976/5001 = 99.5%
Sensitivity of protocol: 168/194 = 87.0%Specificity of protocol: 4976/5001 = 99.5%
PPV: 168/202 = 83.2%NPV: 4976/5001 = 99.5%
DIAGNOSTIC PERFORMANCE OF COSMOS PROTOCOL

CRITERIA FOR IMPLEMENTATION OF CT SCREENING
• False positive
• Best target population
• Best screen interval
• Overdiagnosis
• Cost effectiveness analysis
• Radiation exposure

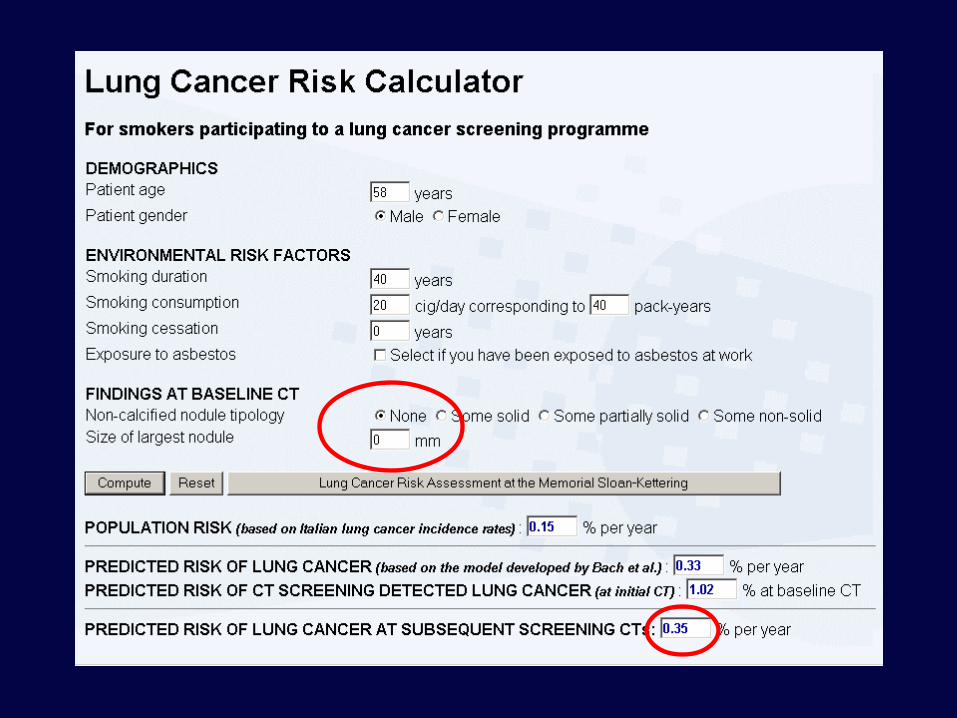
A risk model based on clinical and radiological variables extrapolated by the data of the Cosmos study identifies subgroups of subjects at different risk of cancer
Results
• quantify the risk of an asymptomatic smoker to be identified with lung cancer by LD-CT screening
• optimize the timing of low dose CT • target chemopreventive trials
Low risk group (40% of cosmos population) can safely perform CT screening every 2-3 years
LUNG CANCER RISK SCORE
Submitted




CRITERIA FOR IMPLEMENTATION OF CT SCREENING
• False positive
• Best target population
• Best screen interval
• Overdiagnosis
• Cost effectiveness analysis
• Radiation exposure

Classification according to VDT
• Fast-growing: <400 days
• Slow growing: 400 - 600 days
• Indolent : >600 days
ASSESSMENT OF DOUBLING TIME IN CT SCREENING FOR LUNG CANCER
ASSESSMENT OF DOUBLING TIME IN CT SCREENING FOR LUNG CANCER
DISTRIBUTION OF VOLUME DOUBLING-TIME
ResultsIndolent and slow growing lung cancer represent 12% and 9% of screened detected cases The other 79% screen detected lung cancers are fast growingPrognosis in patients with indolent and slow growing tumors is excellent (100% stage I)A sublobar resection can be appropriate surgical approach for slow growing tumors to avoid overtreatment
VDT 95 days
0,0
200,0
400,0
600,0
800,0
1000,0
1200,0
1400,0
1600,0
1800,0
2000,0
2200,0
2400,0
2600,0
1 11 21 31 41 51 61 71 81 91 101 111

Median follow-up 24 months

GENOMIC ANALYSIS IN EARLY STAGE LUNG CANCER
Analised 100
Metafasis no 28% Metafasis yes 72%
Normal 30%
Aneuployd 70%
1) The majority of screening detected tumors presented aneuploidy and advanced genomic abnormalities despite very initial stage
2) Genomic scanning was able to detect regions of chromosomal alterations in early lung cancer patients.
3) Three common regions of copy number variations were identified: two large scale events (5p amplification and 8p deletion) and one focal 1Mb amplification at 8p11.
4) INDO-INDOL1 involved in the tryptophan catabolism and immune tolerance against tumors One region contains the Gene INDO involved in immuno
Oncogene 2010
CRITERIA FOR IMPLEMENTATION OF CT SCREENING
• False positive
• Best target population
• Best screen interval
• Overdiagnosis
• Cost effectiveness analysis
• Radiation exposure
COSTS/RADIATIONS
• It has been estimated that annual low-dose screening CT from age 50 to 75 incurs a lifetime lung cancer risk of 0.23% in men and 0.85% women
• Costs analysis report range 10-50.000 dollars per year life- saved (lower than raccomandation values and not different from breast screening)
Berrington de González J Med Screen 2008Chirikos CHEST 2008

OTHER QUESTIONS
• Best Treatment For Small Screen Detected Cancers
• Long Term Outcome Of Screening And Optimal Duration Of Screening
• Role Of Serum Markers In Screening • Prevention Of Cardiovascular Disease

We analysed a consecutive series of clinical N0 screening detected lung malignancy to identify predictive criteria of nodal involvement.
Journal of Thoracic Oncology 2011
Screening-detected lung cancers: is systematic nodal dissection always essential?
c-Stage T1N0M0
lung cancer
c-Stage T1N0M0
lung cancer< 3 cm Ø< 3 cm Ø Anatomical resection
+ lymphadenectomy Anatomical resection+ lymphadenectomy
no prior treatment no prior
treatment Preoperative
PET scanPreoperative
PET scan
SCREENING CLINIC pN0 pN+ pN0 pN+ ≤10mm / SUV <2 25 0 14 0 ≤10mm / SUV ≥ 2 23 0 9 0 >10mm / SUV < 2 14 0 20 1 (4.8%) >10mm / SUV ≥ 2 29 6 (17.1%) 116 33 (22.2%)
In either very small (less than 1 cm) or PET negative tumors, hilar and mediastinal lymph node dissection is nonessential with very limited risk of nodal involvement (0-2.3%)
In either very small (less than 1 cm) or PET negative tumors, hilar and mediastinal lymph node dissection is nonessential with very limited risk of nodal involvement (0-2.3%)

ROBOTIC SURGERY AND SUBLOBAR RESECTIONS
PosterolateralThoracotomy
Lateral Muscle Sparing Thoracotomy
Minimally invasive Robotic Approach

S39 LUNG CANCER DETECTION RATE % PER YEAR S39 RATE OF STAGE IA
Mean 0.8% /year Mean 66%

MICRO RNAs
• Short non-coding fragments of RNAs• Function as modulators of gene
expression • Involved in the regulation of cellular
differentiation, proliferation, and apoptosis
• Expression often deregulated in human cancers in a tissue- and cancer-specific manner
• Present in human plasma in a remarkably stable form (they are protected from endogenous RNAse activity)
We investigated the role of circulating miRNAs as a non-invasive diagnostic tool for the detection of lung cancer

• High detection of stage I tumors with limited rate of
recalls
• Mainly non invasive diagnostic protocol
• High resectability rate with low p.o. morbidity and
mortality
• Good overall survival (72% at 5-years)
• Mortality reduction demontrated in the largest
randomised trial
These data support CT screening of lung cancer
CONCLUSIONS

• Increase effectiveness of screening by application of COSMOS risk models reducing radiation exposure and costs
• Validate serological markers and develop genomic analysis
• Control concomitant causes of death such as cardiovascular disease (i.e. calcium score analisys)
• Implement smoking cessation clinics
• Reduce invasiveness of treatment by implementing limited resections in slow growing and subcentimetric tumors (roll), robotics and non surgical treatments (stereotactic radiotherapy)
• Develop chemoprevention and WOP trials
FUTURE STUDIES

ROBOTIC SURGERY


VATS LOBECTOMY- Introduction of the minimally invasive
approach marks one of the great advances in surgery and the advantages of VATS lobectomy are well accepted
- Shortcomings: - limited visual information
- limited freedom of movement
- poor ergonomics- Significant learning curve to develop and
maintain advanced skills
The majority of advanced thoracoscopic cases are performed by a small number of surgeons

ROBOTIC SYSTEM
Robotic system has made advanced thoracoscopic surgery accessible to surgeons who do not have advanced videoendoscopic training
Advantages: natural movements of the surgeon’s hands are traslated into precise instrument movements inside the patient with tremor filtration. Three dimensional view offers a visual magnification even better than that available in open surgery

ROBOT vs. CONVENTIONAL VIDEOSURGERY INSTRUMENTS: ADVANTAGES AND DISADVANTAGES
ADVANTAGES
1. Intuitive movements2. Tremor filtration3. Increased degrees of freedom4. Motion scaling5. Stereoscopic vision6. Stable camera platform7. Equivalence between the
dominant and non-dominant hands
8. Motion analysis9. Eye-hand-target alignment10. Possibly shorter learning curve
DISADVANTAGES
1. Costs2. Loss of tactile feedback3. Limited instrumentation
available4. Significant system set-up time 5. Need of at least one
experienced assistant 6. Possible delayed response by
the surgeon in case of catastrophic event
As every evolving technology, robotic has many limitations, but its advantages were already proven and seem to overcome the disadvantages

ROBOTIC LOBECTOMIES: CASE SERIES
Study n
Median (*)/ mean (**)
operative time (min.)
Median (*)/ mean (**) length of
stay (days)
Median (*)/ mean (**) chest tube duration
(days)
Convertion rate (%)
Mortality (%)
Park et al, USA, 2006
34 218 (155-350) * 4.5 (2-14) * 3 (2-12) * 14 0
Melfi et al, Italy, 2008
107 220 (130-250) * 5 (?-?)** 3 (2-28) ** 9.4 0.9
Gharagozloo et al,
USA, 2009100 216 (173-369) ** 4 (3-42) * Non specified 1 3
Augustin et al, Austria,
201026 228 (162-375) * 11 (7-53) * 7 (3-15) * 19.2 0
Veronesi et al, Italy,
2010
54 213 (85-411) * 4.5 (3-38)* 3.5 (2-30) 12 0

ROBOTIC LOBECTOMIES: TECHNIQUE
Number of arms: 3 versus 4
Insufflation C02
Timing of utility incision
Site of utility incision and other ports

IEO SURGICAL TECHNIQUE
• Lateral position• Robot at the head
posteriorly • Four incisions including
a small utility incision• Camera arm: VII space
mid axillary line• No rib spreading • Individual ligation of
hilar elements

PATIENTS AND ROBOT POSITIONING

RIGH UPPER LOBECTOMY
Isolation of RULpulmonary artery
Isolation of RULpulmonary VEIN

RIGH UPPER LOBECTOMY
Section of the fissure
Isolation of RULbronchus

Left superior segmentectomy: Left superior segmentectomy: bronchusbronchus

Acceptable learning curve?
Adequate oncological radicality?
ROBOTIC LOBECTOMIES

CASE CONTROL STUDY
Objective:
To evaluate learning curve and surgical radicality of robotic lobectomies in early stage NSCLC patients
Method:
54 cases were performed by a single surgeon, using the da 4 arms Vinci system
We used the propensity score matching, a statistical method that mimics randomization
Control group (n=54) patients with the same characteristics submitted to open lobectomy
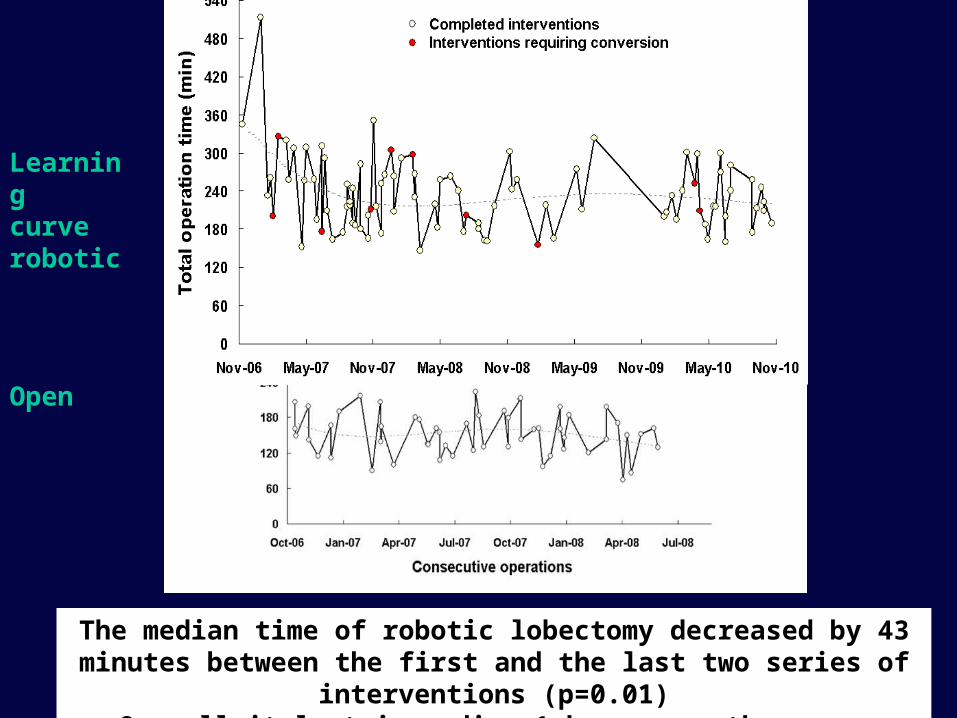
The median time of robotic lobectomy decreased by 43 minutes between the first and the last two series of interventions (p=0.01)
Overall it last in median 1 hour more than open surgery.
Learning curve robotic
Open

LEARNING CURVE - SAFETY - RADICALITY
ROBOT (54) OPEN (54) p value p value
I II III I vs II+III II+III vs Open
------------------------------------------------------------------------------------------------------------------------------------------------
Complications 33% 22% 6% 19% 0.04 0.77
Operative time 260 213 235 154 0.02 <0.0001
Postop days 6 days 5 days 4 days 6 days 0.002 0.002
Median N° LN 15 17 17 18 0.24 0.72
------------------------------------------------------------------------------------------------------------------------------------------------
1) Complications, postoperative days and operative time declines across the 3 robotic tertiles 2) Postoperative stay was SHORTEN after robotic than open procedures3) Complications and N° lymph nodes removed were comparable in open and robotic lobectomies
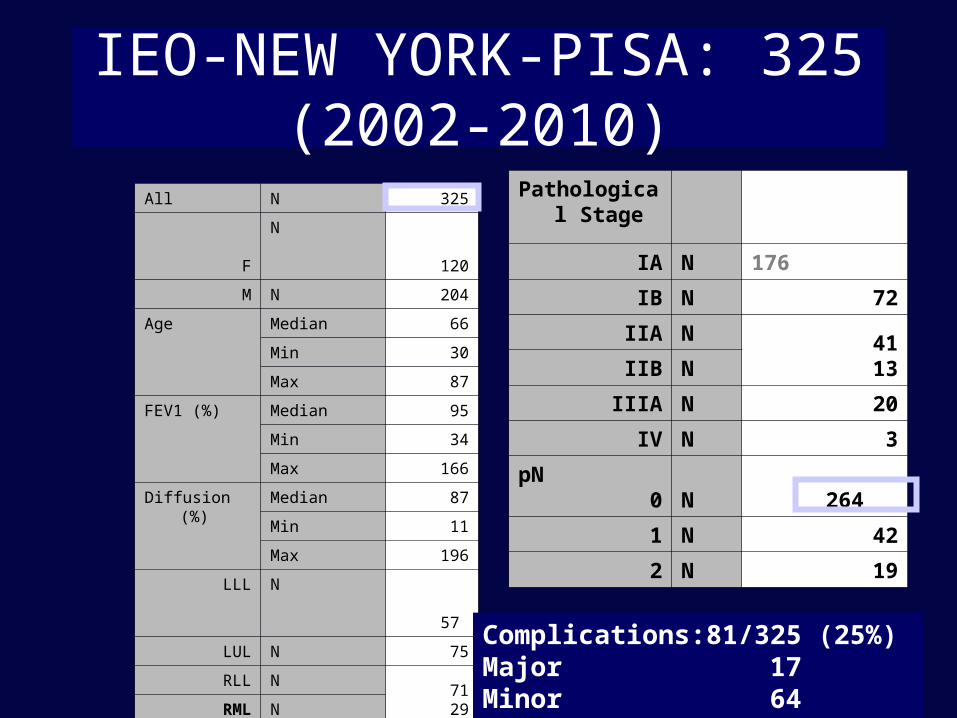
IEO-NEW YORK-PISA: 325 (2002-2010)
All N 325
F N 120
M N 204
Age Median 66
Min 30
Max 87
FEV1 (%) Median 95
Min 34
Max 166
Diffusion (%) Median 87
Min 11
Max 196
LLL N 57
LUL N 75
RLL N7129RML N
RUL N 92
RUL/ML N 1
Pathological Stage
IA N 176
IB N 72
IIA N 4113IIB N
IIIA N 20
IV N 3
pN0 N 264
1 N 42
2 N 19
Complications:81/325 (25%) Major 17Minor 64
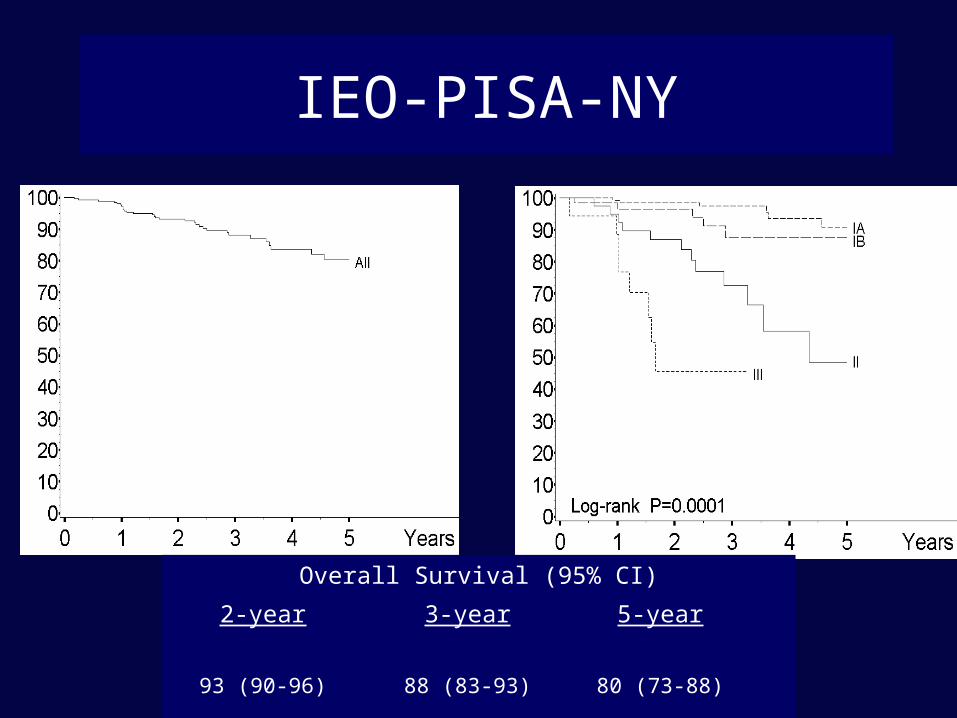
IEO-PISA-NY
Overall Survival (95% CI)
2-year 3-year 5-year
93 (90-96) 88 (83-93) 80 (73-88)

LIMITED RESECTION
• Multicenter RCT (800 cases) to demonstrate that sublobar resection may have the same oncological result than lobectomy plus lymph node dissection for stage Ia lung tumors less than 2 cm
CONCLUSIONSModern medicine and diffusion of screening programs require less
invasive treatment for very early stage lung cancers
Robotic systems have made advanced thoracoscopic surgery accessible to surgeons who do not have advanced videoendoscopic training
The learning curve for robotic lobectomy includes less than 18 cases for surgeons with no experience in vats lobectomies
Robotic lobectomy with lymph node dissection is safe and associated with significantly shorter postoperative hospitalization than open surgery
The number of lymph nodes removed suggests that the procedure is oncologically correct
Most disadvantages of the robotics will be overcome when technological advances improves instrumentation and extended use of robotics reduces costs

LETS THINK TO WHAT ROBOTICS WILL BE AND NOT TO WHAT
ROBOTICS IS !
ROBOTIC STAPLERS
ROBOTIC SUCTION
DUAL CONSOLE (TANDEM SURGERY – TRAINING)
DISTANCE TELESURGERY
DISTANCE PROCTORING

TARGET THERAPY

ISEL
Hirsch JCO 2006

DuyKhanh Pham , JCO 2005DuyKhanh Pham , JCO 2005

Iackman JCO 2007Iackman JCO 2007RP: 10%RP: 10%
TTP: 3,5 mosTTP: 3,5 mos2 yrs OS: 19%2 yrs OS: 19%
The presence of an EGFR mutation was strongly The presence of an EGFR mutation was strongly correlated with disease control, prolonged TTP, and correlated with disease control, prolonged TTP, and
survivalsurvival
First line treatment in selected First line treatment in selected patients: evidence from patients: evidence from
randomized trialrandomized trial
Mok et al NEJM 2009Mok et al NEJM 2009
Carboplatin–Paclitaxel in Carboplatin–Paclitaxel in Pulmonary AdenocarcinomaPulmonary Adenocarcinoma
patients in East Asia who had advanced pulmonary adenocarcinoma and who were
nonsmokers or former light smokers

Mok et al NEJM 2009Mok et al NEJM 2009
Carboplatin–Paclitaxel in Carboplatin–Paclitaxel in Pulmonary AdenocarcinomaPulmonary Adenocarcinoma
1217 pts
mPFS: 5.7 mos (gefitinib) and 5.8 mos (CT)
12-month rates of PFS: 24.9% (gefitinib) and 6.7% (CT)

Mok et al NEJM 2009Mok et al NEJM 2009
Carboplatin–Paclitaxel in Carboplatin–Paclitaxel in Pulmonary AdenocarcinomaPulmonary Adenocarcinoma
261 pts EGFR mutation positive
progression-free survival was significantly longer among those who
received gefitinib
hazard ratio for progression or death, 0.48; 95% CI, 0.36 to
0.64; P<0.001
176 pts EGFR mutation negative
progression-free survival was
significantly longer among those who
received CT
hazard ratio for progression or death with gefitinib, 2.85; 95% CI, 2.05 to 3.98;
P<0.001

Mok et al NEJM 2009Mok et al NEJM 2009

EGFR MUTATIONEGFR MUTATION
How often?How often?

Rosell et al
NEJM 2009
EGFR mutations were found in 350 of 2105 patients
(16.6%).
Screening for Epidermal Growth Factor Receptor Mutations in Lung
Cancer

EGFR MUTATIONEGFR MUTATION
What else?What else?

Target designed trial in Advanced settingI line II line Beyond II line
EGFR Trigger (II)
ALK Crizotinib (III) Crizotinib (II)LDK378 (I)
MET SAR125844 (I)
PI3K BKM120 (Ib/II) BKM120 (Ib/II)
MUC 1 TG4010 (IIb/III)
MEK GSK 1120212 GSK 1120212
Treatment option at IEO according to molecular/antigen profile
Target designed trial in Adjuvant settingMAGE-A3 MAGRIT (III)
Prame Prame (Ib)


EML4-ALK mutation
(A)Fuorescent in situ hybridization (FISH) reveals a split of red and green probes that flank the ALK translocation site in an EML4-ALK–positive tumor (arrows)
(B) ALK immunohistochemistry reveals cytoplasmic ALK staining.
(C) Hematoxylin and eosin staining of the same tumor. Arrows in (B) and (C) indicate signet ring cells, which are commonly found in EML4-ALK–positive tumors.
Shaw et al, JCO 2009

KWAK NEJM 2010


















