
Getting an evidence based journal club into practice in a medium secure forensic setting. process...
17
‘Getting an evidence based journal club into practice in a medium secure forensic setting: process and changes to practice’ 9 th March 2012 Chris Honey, Nurse Therapist Clare Payne, Outreach Librarian
-
Upload
clare-payne -
Category
Healthcare
-
view
24 -
download
0
Transcript of Getting an evidence based journal club into practice in a medium secure forensic setting. process...
‘Getting an evidence based journal club into practice in a medium secure forensic setting: process and changes
to practice’
9th March 2012
Chris Honey, Nurse Therapist
Clare Payne, Outreach Librarian

Overview• Partnership• Drivers, evidence
base.
• New approach• Aims and early outcomes.
Origins
• PSI Course • Critical Thinking
– What happens in practice afterwards– Losing impetus
• Knowledge and Library Service– Induction– PICO, Critical Appraisal– View of library service
• Clinically integrated learning• Journal Club
• Research Practice Gap
• Barriers to integration of knowledge into practice
• Barriers can be countered by the use of journal clubs– (Seymour et al., 2003, McQueen et al., 2006, Rassool, 2005,
Thompson, 2006, Parkes et al., 2004 –Cochrane review)
• Specifically shown to:– Foster EBP skills – decision making process - apply research findings in practice. – Shape positive research attitudes. (Goodfellow 2004, and Owen et
al 2001, McQueen et al 2006). – increase the likelihood of implementation of research findings
into practice. (Rizzuto et al 1994, Thompson 1997)
• Clinically integrated teaching – changes in behaviour
The evidence for a Journal Club:
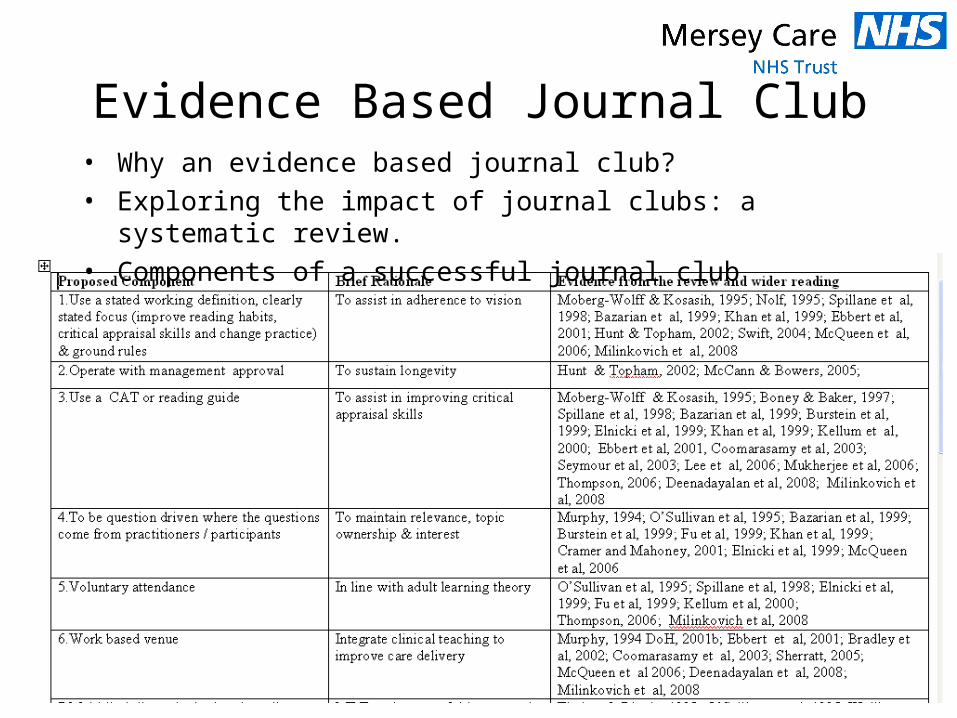
Evidence Based Journal Club• Why an evidence based journal club?• Exploring the impact of journal clubs: a systematic review.• Components of a successful journal club
Evidence Based Journal Club Principles• Ownership
– To be question driven where the questions come from practitioners / participants
– Themes of importance to staff – Articles chosen by participants
• Practice Based
• Voluntary attendance
• Multidisciplinary– Consultant Occupational Therapist & Clinical Director, Nurse
Consultant & Research Lead, Consultant Psychiatrist, Nurse Therapist, Outreach Librarian
• Work based venue
Putting the evidence into Practice: Ownership & Practice Based
• MDT meeting generated 36 questions
• Leave• What are the criteria used in the
decision making process that is adopted when initially granting / cancelling / reducing leave of absence (LOA) in a medium secure setting?
• How are decisions about the duration, location and frequency of leave, arrived at and what are the risk factors considered for increasing such parameters?
• Seclusion• How can the exit of seclusion within
a secure forensic setting, be best managed in terms of reducing the risk of harm to self or others?
• Activity and meaningful occupation of time
• What is the contribution of engagement, occupational activity or structure / routine to reducing stress levels in service users with mental illness and staff ?
• Fitness for Police Interview• What is the evidence base
involved in clinical decisions as to whether a person is fit to be interviewed by police?
• Treatment• How should the prescription of
anti-psychotic medication be affected by how heavily a person smokes tobacco?
Ownership: Choosing the articles
• Process – Partnership with facilitation team
• Shared expertise
• Finding articles that met our needs
• Shared decision making
• Insight
Validity, Reliability, ApplicabilityValidity, Reliability, Applicability
Key Sessions
• Seclusion / Management of Violence and Aggression– Patient restrictions: Are there ethical alternatives to seclusion and
restraint?– A clinical improvement project to develop and implement a decision
making framework for the use of seclusion.
– Prof. Richard Whittington, University of Liverpool
• Meaningful Activity– Q? How will increasing activity affect inpatient service user
presentation?• 'An occupational perspective of the recovery journey in mental
health' • Occupation, mental Illness and medium security: Exploring time use
in Forensic Regional Secure Units.
• Absconding while on leave
Results: Behavioural & attitudinal change
• Motivational• Improved reading habits• Critical & creative thinkers• Improved research awareness• I don’t need to get published to change practice• Raised awareness of KLS• Aims achieved!
Results: Practical outcomes to date• Multidisciplinary Working Groups
– Absconding• S17 Leave audit• S17 Decision making template
– Seclusion reduction• Improved relational security• Improved Patient Experience
– Meaningful activity audit• CQUIN – Improve current uptake
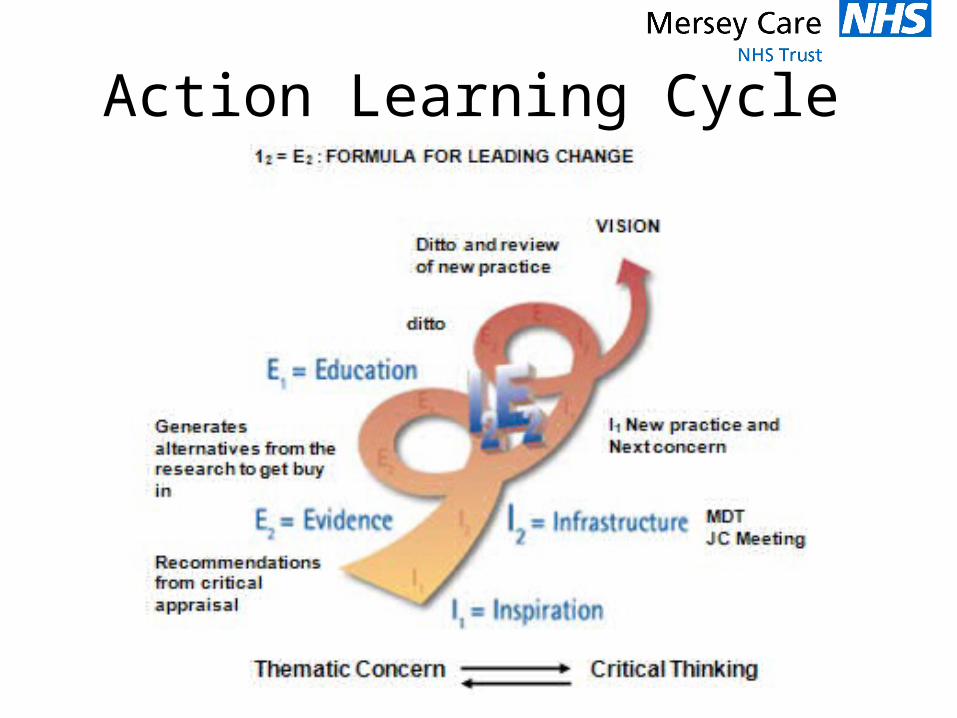
Action Learning Cycle
Next Steps• Current practice needs to remain informed
by the evidence base.
• Research champions
• Working groups to recommend amendments or new additions to practice.
• Evidence clinical impact – Quality Strategy
• Journal club series 2– Service user involvement
• Business case for a clinician in the KLS!!
Conclusion
• KLS + Clinicians = Vital partnership!
Thanks
• Everyone who attended and got involved
• The facilitation Team
• Professor Richard Whittington

Any Questions


















