Gastrointestinal Disorders Road Map to …ccn.aacnjournals.org/content/31/4/69.full.pdfabsorb...
19
regarding location of the cancer, cell type, predisposing factors, and sur- gery type will help focus the patient’s treatment and influence the quality of care. Throughout the management of patients with esophageal cancer, the primary focus of all nurses involved remains the provision of education and emotional support for both patients and patients’ fami- lies. Most patients undergo surgery soon after cancer has been diag- nosed. Information relayed in pre- operative teaching may not be well received or remembered because of increased anxiety levels or reduced retention levels at that time. Fear and anxiety levels often remain high as patients have little time to absorb information and develop realistic expectations. This anxiety is often intensified by the fact that a reliable prognosis can be given only after surgical resection, when pathol- ogy results are available. This situa- tion and the fact that individual progress can be very unpredictable makes keeping patients and their families informed of daily progress very important. Nursing goals revolve around improving the patient’s tolerance of treatments, maintaining stability, and realizing recovery in an effort Barbara Logue, RN, BSN, BA, CCRN Scott Griffin, RN, BSN, CCRN, CSC Road Map to Esophagectomy for Nurses Gastrointestinal Disorders were reported. 1 Esophageal cancer ranks seventh among all cancers in mortality among men. 2 The lifetime risk of having esophageal cancer diagnosed in the United States is now 1 in 200 people. 1 The incidence of esophageal cancer is 4 times higher in men than in women and the dis- ease predominantly affects older persons (mean age, 60-70 years). 1,2 Treatment continues to advance, with care now managed by multi- disciplinary teams as multimodal therapy is provided. Nursing care now necessitates advanced clinical judgment to provide safe and effec- tive care to obtain optimal outcomes throughout the patient’s course of treatment. Nursing knowledge E sophageal cancer remains one of the deadliest forms of cancer today. It is a disease with an insidious onset and poor prognosis. The mortality rate remains high, with a 5-year survival rate of 10% to 35% regardless of treatment man- agement. 1-5 Although esophageal cancer is considered uncommon in the United States when compared with other cancers, its occurrence has increased steadily. In 2009, 16 470 new cases of esophageal cancer were diagnosed and 14530 deaths due to esophageal cancer ©2011 American Association of Critical- Care Nurses doi: 10.4037/ccn2011426 www.ccnonline.org CriticalCareNurse Vol 31, No. 4, AUGUST 2011 69 Esophageal cancer, although considered uncommon in the United States, con- tinues to exhibit increased incidence. Esophageal cancer now ranks seventh among cancers in mortality for men in the United States. Even as treatment continues to advance, the mortality rate remains high, with a 5-year survival rate less than 35%. Esophageal cancer typically is discovered in advanced stages, which reduces the treatment options. When disease is locally advanced, esophagectomy remains the standard for treatment. Surgery remains challenging and complicated. Multiple surgical approaches are available, with the choice determined by tumor location and stage of disease. Recovery is often fraught with complications—both physical and emotional. Nursing care revolves around complex care managing multiple body systems and providing effective education and emotional support for both patients and patients’ families. Even after recovery, local recurrence and distant metastases are common. Early diagnosis, surgical advancement, and improvements in post- operative care continue to improve outcomes. (Critical Care Nurse. 2011;31[4]:69-86) by AACN on June 18, 2018 http://ccn.aacnjournals.org/ Downloaded from
Transcript of Gastrointestinal Disorders Road Map to …ccn.aacnjournals.org/content/31/4/69.full.pdfabsorb...

regarding location of the cancer, celltype, predisposing factors, and sur-gery type will help focus the patient’streatment and influence the qualityof care. Throughout the managementof patients with esophageal cancer,the primary focus of all nursesinvolved remains the provision ofeducation and emotional supportfor both patients and patients’ fami-lies. Most patients undergo surgerysoon after cancer has been diag-nosed. Information relayed in pre-operative teaching may not be wellreceived or remembered because ofincreased anxiety levels or reducedretention levels at that time. Fearand anxiety levels often remainhigh as patients have little time toabsorb information and developrealistic expectations. This anxietyis often intensified by the fact that areliable prognosis can be given onlyafter surgical resection, when pathol-ogy results are available. This situa-tion and the fact that individualprogress can be very unpredictablemakes keeping patients and theirfamilies informed of daily progressvery important.
Nursing goals revolve aroundimproving the patient’s tolerance oftreatments, maintaining stability,and realizing recovery in an effort
Barbara Logue, RN, BSN, BA, CCRNScott Griffin, RN, BSN, CCRN, CSC
Road Map to Esophagectomyfor Nurses
Gastrointestinal Disorders
were reported.1 Esophageal cancerranks seventh among all cancers inmortality among men.2 The lifetimerisk of having esophageal cancerdiagnosed in the United States is now1 in 200 people.1 The incidence ofesopha geal cancer is 4 times higherin men than in women and the dis-ease predominantly affects olderpersons (mean age, 60-70 years).1,2
Treatment continues to advance,with care now managed by multi-disciplinary teams as multimodaltherapy is provided. Nursing carenow necessitates advanced clinicaljudgment to provide safe and effec-tive care to obtain optimal outcomesthroughout the patient’s course oftreatment. Nursing knowledge
Esophageal cancer remainsone of the deadliest formsof cancer today. It is adisease with an insidiousonset and poor prognosis.
The mortality rate remains high,with a 5-year survival rate of 10% to35% regardless of treatment man-agement.1-5 Although esophagealcancer is considered uncommon inthe United States when comparedwith other cancers, its occurrencehas increased steadily. In 2009,16 470 new cases of esophagealcancer were diagnosed and 14530deaths due to esophageal cancer
©2011 American Association of Critical-Care Nurses doi: 10.4037/ccn2011426
www.ccnonline.org CriticalCareNurse Vol 31, No. 4, AUGUST 2011 69
Esophageal cancer, although considered uncommon in the United States, con-tinues to exhibit increased incidence. Esophageal cancer now ranks seventh amongcancers in mortality for men in the United States. Even as treatment continues toadvance, the mortality rate remains high, with a 5-year survival rate less than 35%.Esophageal cancer typically is discovered in advanced stages, which reduces thetreatment options. When disease is locally advanced, esophagectomy remains thestandard for treatment. Surgery remains challenging and complicated. Multiplesurgical approaches are available, with the choice determined by tumor location andstage of disease. Recovery is often fraught with complications—both physical andemotional. Nursing care revolves around complex care managing multiple bodysystems and providing effective education and emotional support for both patientsand patients’ families. Even after recovery, local recurrence and distant metastasesare common. Early diagnosis, surgical advancement, and improvements in post -operative care continue to improve outcomes. (Critical Care Nurse. 2011;31[4]:69-86)
by AACN on June 18, 2018http://ccn.aacnjournals.org/Downloaded from

to help the patient attain an optimalquality of life.
Anatomy and PhysiologyThe esophagus is a muscular
tube that connects the pharynx tothe stomach and is used as a pas-sageway for food. It has no digestive,absorptive, or secretory function.The esophagus bridges 3 anatomiccompartments: the neck, the thorax,and the abdomen. The esophagealwall has a rich lymphatic networkand a dense microvascular bloodsupply. Esophageal cancer growthstarts from the external wall andpenetrates inward, often obstruct-ing the lumen of the esophagus asit grows.
The esophagus is the only partof the gastrointestinal system thatlacks a protective serosal outer layer.The absence of that protective layerallows esopha geal tissue to expandeasily to accommodate food bolusespropelled by peristalsis. The elastic-ity of the esophagus often delaysidentification of the most commonpresenting signs and symptoms ofesophageal cancer: progressive dys-phagia and weight loss. Sixty per-cent of the circumference of theesophagus may be invaded by tumorbefore patients experience symp-toms severe enough to seek medicalattention.6 Luminal obstruction by
tumor invasion often causes a grad-ual change in diet, as it becomesmore difficult to swallow solid foods;nutritional deficiencies and weightloss often follow. People often com-pensate for these symptoms bychanging dietary habits (eatingmore soft foods, soaking solid foodsin liquids, or transitioning to a liq-uid diet) and delay seeking medicalevaluation.7
Lacking a protective serosal mem-brane, the esophagus is more vulner-able to the invasive nature of cancercells. Also, the extensive network oflymphatic vessels nearby meansthat tumors can advance quickly.By the time the patient seeks med-ical help, esophageal cancer is oftenlocally advanced, with cancer invad-ing deep into the esophageal wall,spreading to nearby lymph nodesand often advancing into adjacentstructures.8-12 Of these patients, 50%will have unresectable metastaticdisease.2,6,13,14
HistologyMost esophageal cancers can be
classified as adenocarcinoma orsquamous cell carcinoma. Until the1970s, most esophageal cancers inthe United States were squamous cellcarcinomas.3,7,15-18 Today esophagealcancer has seen a significant change,with a substantial increase in the
prevalence of adenocarcinoma.Increasing more than 350% in thepast 30 years, adenocarcinoma hasbecome the most common form ofesophageal cancer.13 Today squamouscell carcinoma accounts for around40% of esophageal cancers diagnosedin the United States.2 Typicallysquamous cell carcinoma occurs inthe cells that line the upper to mid-dle parts of the esophagus. Adeno-carcinoma is found in the distalpart of the esophagus or the gastro -esophageal junction in the cells thatmake and release mucus and othersecretions. Today, around 60% ofdiagnosed esophageal cancers areadenocarcinomas.2
Causes and Risk FactorsThe causes of esophageal cancer
have never been clearly identified,but evidence shows a strong link toenvironmental carcinogens.19 Theprincipal precursor lesion in squa-mous cell carcinoma is thought to beepithelial dysplasia.19 It is hypothe-sized that esophageal cancer devel-ops from dysplasia to carcinoma toneoplasm. The precursor lesion inadenocarcinoma exhibits as colum-nar epithelium originating from thecondition called Barrett esophagus.These cells replace the squamouscells found in the lower part of theesophagus. It is hypothesized thatthe progression of metaplasia to low-grade dysplasia to high-grade dys-plasia leads to adenocarcinoma.19
Chronic irritation of the esopha-gus has long been considered a majorpredisposing factor for both typesof esophageal cancer. Chronic expo-sure to the environmental carcino-gens associated with excessive alcoholconsumption and long-time cigarettesmoking have been more closely
Barbara Logue is a staff nurse in the cardiothoracic intensive care unit at Barnes JewishHospital in St Louis who also serves as charge nurse and a member of the unit practicecommittee.
Scott Griffin is a staff nurse in the cardiothoracic intensive care unit at Barnes Jewish Hos-pital in St Louis who also trains and mentors new staff and provides educational support.
Authors
Corresponding author: Scott Griffin, RN, BSN, CCRN, CSC, 1726 Baxston Ct, Swansea, IL 62226 (e-mail: [email protected]).
To purchase electronic or print reprints, contact The InnoVision Group, 101 Columbia, Aliso Viejo, CA 92656.Phone, (800) 899-1712 or (949) 362-2050 (ext 532); fax, (949) 362-2049; e-mail, [email protected].
70 CriticalCareNurse Vol 31, No. 4, AUGUST 2011 www.ccnonline.org
by AACN on June 18, 2018http://ccn.aacnjournals.org/Downloaded from

metastases.7,18 Information gatheredfrom these specialized tests can becombined to determine the clinicaldisease stage of the cancer and todevelop a treatment plan.2,15,19
Staging is a standardizedapproach developed by the Ameri-can Joint Committee on Cancerusing the tumor (T), node (N),metastasis (M), TNM classificationto establish clinical state of the dis-ease8 (Table 2). The rationale forthis system is the recognition thatcancer can spread in 3 distinctways, through the surrounding tis-sue, through lymphatic fluid, orthrough the blood. TNM informa-tion is used to substantiate theadvanced state and spread of apatient’s current disease.19
• T refers to the primary tumorand identifies how deep thetumor has grown into the 4layers of esophageal tissue.
• N refers to spread to regionallymph nodes that are close tothe primary tumor.
• M refers to metastases shownby spread to a distant lymphnode or other organs.
The first step is to categorizewhere the tumor is present in thebody. The second step combinesthis information with possible
study used to distinguish tumorfrom a stricture. This study providesanalysis of dysphagia, motility, andemptying and is used to evaluateesophageal form and function in rela-tion to other mediastinal structures.Findings may include mucosal irregu-larities and narrowing of the lumen.19
Once tumor has been identified,endoscopy can be done to determinetumor size and to enable removalof tissue samples and cells for cyto-logic examination and biopsy.Endoscopy is useful for the diagno-sis of cervical lymph node involve-ment and can be used to distinguishinvolvement of the esophageal wall.5
Computed tomography (CT) isused to begin pretreatment stagingby identifying involvement ofregional lymph nodes and the pres-ence of distant metastases. A CTscan should include the chest,abdomen, and pelvis.5,17
Endoscopic ultrasonography isused for better evaluation of involve-ment of local lymph nodes anddetermination of tumor penetration.Ultrasonography may be combinedwith fine-needle aspiration of lymphnodes for pathologic confirmationof involvement.3
Positron emission tomographyis performed to assess for distant
related to development of squamouscell cancer.7,20-22 The longer the useand the higher the intake of alcoholand cigarettes, the greater the risk ofesophageal cancer developing. Com-bined use of smoking and drinkingalso expands the risk. A diet low infruits and vegetables may increasethe risk of esophageal cancer devel-oping, probably because of the lossof vitamins and minerals. Drinkinghot liquids or consuming foods highin nitrates, achalasia, and irradiationof the upper part of the abdomen orthe chest have also been identifiedas risk factors more closely relatedto squamous cell carcinoma.13,14,22,23
Changes in lifestyle patterns (diet,activity level, obesity) are consideredcontributing factors to the increasedincidence of gastroesophageal refluxdisease and Barrett esophagus (pre-malignant cells of the distal part ofthe esophagus) in the United States.13,23
These diseases may create suscepti-bility significant to the increaseddevelopment of adenocarcinoma ofthe esophagus.3,15,16 If reflux of stom-ach acid into the lower part of theesophagus continues for a long time,the lining of the esophagus can bedamaged. Normal cells are replacedwith glandular cells that may even-tually develop into dysplasia or Bar-rett esophagus.7,18,20 Barrett esophagusis regarded as a premalignant lesionfor adenocarcinoma13 (Table 1).
DiagnosisEstablishing the diagnosis and
evaluating esophageal cancer isaccomplished by means of multiplelaboratory and diagnostic tests.Radiographic tests are used to estab-lish location and extent of esopha gealinvolvement. A timed-barium swal-low study is often the first imaging
Table 1 Risk factors for esophageal cancer
Squamous cell carcinoma
Chronic tobacco use Heavy alcohol use History of head or neck cancer History of radiation therapy Chronic esophagitisChronic stricture or achalasiaDietary/nutritional deficiencyLow intake of fruits/vegetables High intake of red meat or nitrate-containing foodsConsumption of scalding hot beverages
Adenocarcinoma
Cigarette smokingObesityAlcohol consumptionGastroesophageal reflux diseaseBarrett esophagus
www.ccnonline.org CriticalCareNurse Vol 31, No. 4, AUGUST 2011 71
by AACN on June 18, 2018http://ccn.aacnjournals.org/Downloaded from

neoadjuvanttherapy. Thistime frame is toallow patientsto recoverbefore surgery,as both chemo -therapy andradiation thera-pies have well-known adverseeffects of nau-sea, vomiting,and inflamma-tion. Patientsare often nutri-tionally com-promised at thetime of diagno-
sis, so a jejunostomy tube (J tube)may be placed before neoadjuvanttherapy to provide nutritional sup-port.11,12 Optimal treatment willfocus on multimodality care involv-ing nurses, oncologists, gastroen-terologists, and nutritionists, alongwith an experienced surgical team.
EsophagectomyEsophagectomy remains the
primary treatment for esophagealcancer.19 The surgery is highly com-plex and technically demanding,involving multiple incisions andmultiple body systems. It involvesremoval of the esophagus and theupper portion of the stomach. Theremainder of the stomach, approx-imately the same length as theesophagus, is most commonly usedfor replacement. Before removal ofthe esophagus starts, the stomachis reshaped. Once the esophagushas been removed, the newlyshaped stomach is then relocatedto the esophageal area posterior tothe mediastinum.
undetected micrometastases notfound at the time of diagnosis.5,9-11,16,17
The chemotherapy used inesophageal cancer often consists of adual-medication approach such as useof cisplatin and 5-fluorouracil.19 Thedrugs are generally given through atunneled central venous catheter or aperipherally inserted central venouscatheter. A cycle of treatment gener-ally consists of 3 doses a week for 2 or3 weeks. The purpose of chemother-apy is to kill the cancerous cells thatare responsible for metastatic spread.Although the 5-year survival rate hasnot improved substantially with pre-operative use of chemotherapy, the2-year survival rate has improved.10
The radiation therapy used inesophageal cancer is generallygiven twice daily for 3 weeks. Thepurpose of the radiation therapy isto shrink the tumor to a moreresectable size and remove micro-scopic persistent disease remainingafter chemotherapy.19
It is recommended that sur-gery occur within 6 weeks after
involvement of nearby and remotestructures to determine clinicalstage (0-IV). This knowledge isessential for making informed rec-ommendations and appropriatetreatment plans.4,15,17
Presurgical TreatmentThe standard of care for locally
advanced esophageal cancer has beenthe surgical procedure esophagec-tomy. It is the only treatment offeredthat provides a curative outcome.19
Continued developments in surgicaland diagnostic techniques havebeen unsuccessful in improving the5-year life expectancy, whichremains less than 20%.1,2,4,5,16,17 Theaddition of neoadjuvant therapycombining chemotherapy and/orradiation before or after surgery hasbecome common in an attempt tocreate a survival advantage not pro-vided by surgery alone. Neoadjuvanttherapy could improve surgical out-comes by reducing tumor size, thusincreasing the feasibility of resec-tion, and addressing the issue of
Table 2 Standardized approach to staging cancersa
Stage
0
I
IIa
IIb
III
IVa
IVb
TNM
Tis, N0, M0
T1, N0, M0
T2 or 3N0, M0
T1 or 2, N1, M0
T3, N1, M0T4, N0 or N1, M0
Any T, any N, M1a
Any T, any N, and M1b
Description
Earliest stage, rarely seen: cancer cells are limitedto innermost layer or epithelium
Cancer cells have invaded the submucosa
Cancer cells have invaded the muscle layer of theesophagus and possibly the adventitia—theconnective outer layer
Cancer cells have invaded beyond epithelium buthave not reached the adventitia; cancer hasspread to nearby lymph nodes
Cancer cells have invaded the adventitia andspread to nearby lymph nodes, or nearbyorgans but not lymph nodes
Cancer cells have spread to nearby lymph nodes
Cancer cells have spread to distant lymph nodesand other organs (not surgical candidates)
5-Year survival rate, %
90
50-80
30
20-25
13-18
5-10
0
a Information obtained from the American Cancer Society and National Cancer Institute Surveillance Epidemiology and End Results (2008).
72 CriticalCareNurse Vol 31, No. 4, AUGUST 2011 www.ccnonline.org
by AACN on June 18, 2018http://ccn.aacnjournals.org/Downloaded from

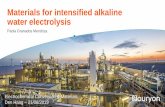
Transthoracic (Ivor-Lewis)Approach. The transthoracicapproach is also known as theIvor-Lewis procedure. This approachinvolves 2 incisions, a midlineabdominal incision (Figure 1) anda right thoracotomy incision (Fig-ure 2). The thoracotomy providesgreater exposure of the esophagus,allowing direct visualization as theesophagus is freed from mediastinalattachments. This approach alsoallows thoracic en bloc esophagec-tomy (radical excision of regionalmediastinal lymph nodes, sur-rounding tissue, and upper stom-ach) to be performed.24 The en blocresection may provide the bestchance of identifying and removingpotentially involved lymph nodes.25
An incision is made in the mid-line abdomen from the umbilicusup to the sternal border. Throughthis incision, the stomach is mobi-lized (freed from its attachments);this procedure alone can take up to1 hour to perform. Mobilization of
and its placement is verified bybronchoscopy before the patient isprepared and draped. The dual-lumenendotracheal tube allows 1 lung tobe deflated during surgery to improvevisibility in the operative field andto reduce potential lung trauma.The other lung is kept in active ven-tilation. The main disadvantage ofthe dual-lumen endotracheal tubeis that it must be removed andreplaced with a standard single-lumen tube before the patient leavesthe operating room.
Surgical ApproachesUnderstanding the surgical
technique used can help the nursetailor the nursing care to eachpatient. This knowledge can alsooptimize the patient’s postopera-tive course. Surgical approachdepends on the location of the pre-senting tumor, potential involve-ment of surrounding structures,the patient’s current stability, andthe surgeon’s preference.
During this procedure, the car-diovascular, pulmonary, lymphatic,and nervous systems are all affected.A dedicated thoracic team performsthe surgery, and the patient is typi-cally admitted to a cardiothoracicintensive care unit (ICU) for postop-erative care. Esophagectomypatients may have very atypical carerequirements compared with thesurgical patients usually admitted tocardiothoracic ICUs. The nurse mustprovide care that is often unlike thetraditional hemodynamic manage-ment of a cardiac patient or manage-ment of the pulmonary needs ofthoracic patients. Esophagectomypatients may have specific carerequirements related to the surgicalapproach, the amount of the esoph-agus removed, or preoperative pres-entation. The remainder of this articlecovers preoperative considerations,surgical approaches that may be used,tubes that may be placed, complica-tions that may arise, and postopera-tive management.
Preoperative ConsiderationsSeveral preoperative procedures
are common in all esophagectomypatients. Arterial and central cathetersare placed, an endotracheal tube isplaced under general anesthesia, anasogastric tube is placed, bladdercatheterization is performed, andthe patient is placed supine on theoperating table. Preoperative imag-ing is again reviewed to verify tumorlocation. Before surgical incision, 8to 12 mL of fluid per kilogram of thepatient’s body weight is infused tocompensate for insensible fluid loss.19
Antibiotics are also given to preventinfection just before incisions aremade. In certain approaches, a dual-lumen endotracheal tube is placed
Figure 1 Midline abdominal incision (open). A, Retrograde nasogastric tube; B,jejunostomy tube; C, abdominal incision closed in multiple layers.
www.ccnonline.org CriticalCareNurse Vol 31, No. 4, AUGUST 2011 73
by AACN on June 18, 2018http://ccn.aacnjournals.org/Downloaded from

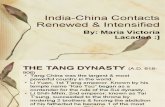
the stomach involves removing lymphtissue and fashioning the stomachinto a tube (from its S-shape as astomach). Four main arteries supplyblood flow to the stomach (Figures3A and 3B). Three of these 4 arteriesare clipped. The right gastroepiploicartery is prepared for mobilization
with the stomach. This single artery,the right gastroepiploic artery, nowsupplies blood flow to the stomach.The reduced blood flow compro-mises graft perfusion, which makesthe use of vasopressor support notwell tolerated in these patients. Thestomach conduit must have a 5-cm
tumor-free margin to be considereddisease free.19
After the stomach is mobilized,gastric tubes are placed. At thisinstitution (Barnes Jewish Hospital),placement of a retrograde gastrictube has been used as an alternativeto traditional placement of a naso-gastric tube, with good results. Theretrograde gastric tube is toleratedwell by postoperative patients,causing less discomfort than the tra-ditional nasogastric tube. The retro-grade gastric tube is placed into thesmall intestine above the ligamentof Treitz (Figure 4) and then fed intothe newly shaped (stomach) esopha-gus. Through a separate stab inci-sion, the retrograde gastric tube isbrought out through the abdominalwall (Figure 5). A J tube is thenplaced into the small intestine belowthe ligament of Treitz (Figure 4). TheJ tube is then brought out through aseparate stab incision and secured tothe wall of the abdomen with sutures(Figure 5). After occult bleeding is
Figure 2 Thoracotomy incision (open) is about an inch and a half wide at this point.
Figure 3 A, Drawing of the 4 arteries of the stomach and the anastomosis site; B, Photograph of the stomach as it is preparedto be mobilized.
A B
Left gastroepiploic artery
Right gastroepiploic artery
Left gastric artery
Right gastric artery
Anastomotic site
74 CriticalCareNurse Vol 31, No. 4, AUGUST 2011 www.ccnonline.org
by AACN on June 18, 2018http://ccn.aacnjournals.org/Downloaded from

achieved. The fifth rib will be shin-gled or purposely fractured to gainaccess, thereby allowing a ribspreader to be placed (Figure 8).The esophagus is then mobilizedand the stomach is brought upthrough the esophageal hiatus andpositioned into place (Figure 9).The margins on the esophagus andstomach are then clipped with a sta-pling device, which fastens and cutsin one action. The esophagus withtumor-free margins and a portionof the stomach are removed. Thisen-bloc specimen is then dissectedand prepared for testing. Thepathologist performs a frozen sec-tion analysis, which takes approxi-mately 20 minutes to complete. Ifthe margins are not clear, moreresection is needed.26,27
The upper part of the esophagusis now attached to the fundus of thestomach by using a stapler or handsuturing. This process restores con-tinuity between the oral cavity andthe stomach. Two chest tubes arethen brought through separate stabincisions and the chest is closed(Figures 10 and 11). One chest tubeis placed near the anastomosis andthe other in the dependent area ofthe pleural space of the right lung.With chest closure, the right lung isreinflated and the patient is placedsupine. Then, a third chest tube isplaced in the dependent area of thepleural space in the left lung. Allchest tubes will function to drainaway extra fluid that accumulates.19
An endoscopy is performed to assessthe anastomosis and tube placement.A bronchoscopy is then performedand the dual-lumen tube is replacedwith a single-lumen tube. The entireprocedure usually takes about 5 to6 hours in the operating room.3,4
intercostal space (Figure 2), and theright lung is deflated with the previ-ously placed dual-lumen endotrachealtube. A dual-lumen endotrachealtube allows the right lung to bedeflated while the left lung remainsinvolved in ventilation (Figure 7).With the right lung collapsed, goodexposure of the esophagus is
ruled out and after all sponge countsare completed, the abdominal inci-sion is closed (Figure 6).
The patient is then repositionedin the lateral position with the leftside down and the right side of thechest prepared and draped. A skinincision (thoracotomy) is madebetween the fifth or sixth rib’s
Figure 4 Abdominal tube placement. The jejunostomy tube and the retrogradenasogastric tube are both secured to the abdominal wall and the intestine.
Jejunostomy tube
Retrograde nasogastric tube
Figure 5 Abdominal tubes secured.
www.ccnonline.org CriticalCareNurse Vol 31, No. 4, AUGUST 2011 75
by AACN on June 18, 2018http://ccn.aacnjournals.org/Downloaded from

the transthoracic approach and aleft cervical incision (Figure 12).This approach is thought to be bothpain sparing and more suitable fora patient with marginal respiratorystatus because of the absence of athoracotomy.5,19 The type ofabdominal incision and the proce-dure for stomach mobilization arethe same as described for thetransthoracic approach.
After mobilization, the esopha-gus is bluntly dissected by usingthe fingers to pass up into the medi-astinum via the hiatus. Bleeding isgenerally minimal because of smallvessel spasms, which reduce bloodflow. A stapling device is used todivide and shape the stomach forreplacement of the esophagus. Thena cervical neck incision is made inthe left side of the sternomastoidmuscle. Through this, access to theupper part of the esophagus isgained. Again blunt dissection isperformed around the esophagusto meet the previous lower bluntdissection. The esophagus andupper stomach are then pulled upthrough the esophageal hiatus (Fig-ure 9 shows how this would look,but on top of the chest an actualpull-up would be difficult to dis-play in a photograph). This pull-upcan be performed in a number ofways, such as using the hand topush the stomach superiorly.19 Afterthe stomach is brought up throughthe neck incision, an anastomosissimilar to the Ivor-Lewis can beperformed and the abdominal andcervical incisions are closed (Figure13). Once again an endoscopy isperformed for anastomosis andtube assessment, and bilateral pleu-ral chest tubes are placed to drainany pleural fluid.
apart) allowed the stomach to bepositioned to achieve a cervicalanastomosis.19 This approach alsoinvolves 2 incisions, the same mid-line abdominal incision as used in
Transhiatal Approach. Use of thetranshiatal approach has increasedin the past 20 years. Use of a bluntdissection immobilization technique(no cutting, just pushing tissues
Figure 6 Abdominal incision closed.
Jejunostomy tube Retention suture
Head
Retrograde nasogastric tube
Figure 7 Dual-lumen endotracheal tube (carina). The left bronchus is to the left andthe right bronchus is to the right of the carina.
Carina
76 CriticalCareNurse Vol 31, No. 4, AUGUST 2011 www.ccnonline.org
by AACN on June 18, 2018http://ccn.aacnjournals.org/Downloaded from

Additional Surgical Approaches.Other surgical approaches combinethe techniques used in transhiatalor transthoracic esophagectomy.Use of a 3-hole or 3-field approachcombines aspects of the Ivor-Lewisapproach (abdominal incision andright thoracotomy) with the neckincision from the transhiatal
approach. This combinationapproach allows increased expo-sure for removal of a tumor in theupper part of the esophagus withthe needed 5 cm of margin.19
A left-sided approach may beused for tumors at the esopha-gogastric junction.5 A large leftthoraco ab dom inal incision or a
left thora cotomy are combinedwith a midline abdominal incision.This approach may be indicatedwhen the patient has had a previ-ous right thoracotomy. The difficul-ties with the left-sided approachinvolve working around the aortabecause it lies in front of the esoph-agus. The patient is positionedlying with right side down. Thesteps involved in this approach aresimilar to those used in the Ivor-Lewis approach. The difference isthat the left side is up, which bringsthe aorta into the surgical field.Also a left cervical incision (transhi-atal) might be necessary if a highanastomosis is needed.3,24,28 Manytimes the surgical approach isdriven by the surgeon’s personalpreference or dictated by the sizeand location of the tumor (Table 3).
Surgically Placed Tubes The gastric tube used can be
either a nasogastric tube or a retro-grade gastric tube. This tube willbe placed to low intermittent wallsuction. The purpose of this tubeis not to remove high volumes ofgastric residuals but to keep thestomach decompressed so that dis-tention and tension on suture linesare reduced while healing.19
The J tube is placed to gravitydrainage for the first 24 to 48hours. The J tube will be used forfeedings and for administration ofmedications.
Pleural and/or mediastinal chesttubes are placed regardless of surgi-cal approach, although surgicalapproach may dictate specific siteplacement. Chest tubes are placedto -20 cm of suction, and outputstarts bloody but should change toa serosanguineous color.
Figure 8 Thoracotomy incision has been completely opened (previous 11⁄2 in [3.81cm]) at almost 3 in (7.62 cm) or more. The pink area in the center is the right lung.
Figure 9 The newly shaped stomach/esophagus that will be pulled up is tested forlength and freedom from kinks before final placement.
www.ccnonline.org CriticalCareNurse Vol 31, No. 4, AUGUST 2011 77
by AACN on June 18, 2018http://ccn.aacnjournals.org/Downloaded from

ComplicationsEsophagectomy patients are at
risk for any number of different com-plications ranging from self-limitingproblems to life-threatening situa-tions. Despite advances in surgicaltechniques, preoperative assess-ment, and improved postoperative
management,esophagectomypatients have ahigh frequencyof postopera-tive complica-tions that affectrecovery.19 Themost commonmedical com-plication ispulmonaryrelated.3,24,26,29
Three of themost serioussurgical com-plications areanastomosisleak, chyle
leak, and gastric necrosis.3,4,24-26,29-31
Pulmonary Complications. Post-operative pulmonary complicationsoccur in 5% to 30% of patients and area major source of morbidity.3,4,24-26,29,30
Pneumonia is the most commonmedical complication and aloneincreased the incidence of mortality
by 20%.3 Many preoperative andsurgical factors may contribute tothe development of the most com-mon pulmonary complications ofpneumonia and respiratory insuffi-ciency (Table 4).
In a large retrospective studythat used the Department of VeteranAffairs medical database, researchersanalyzed the surgical outcomes of1777 esophagectomy patients in a10-year period, focusing on variablesthat lead to morbidity and mortal-ity. Eight hundred eighty patients(49.5% of all esophagectomy patients)had a significant complication post-operatively. The most commoncomplication was pulmonary related;specifically, 21% of the patients hadpneumonia, 16% had respiratoryfailure, and 22% required ventilatorsupport for longer than 48 hours.The patients in this study had a sig-nificant incidence of preexistingfactors such as active smoking,chronic obstructive pulmonary dis-ease, chronic steroid use, and dysp-nea at rest or with minimal exertion.31
Anastomosis Leak. Anastomosisleak or failure of an anastomosis toheal properly is not uncommon,with reported incidences from 1%to 30%.3,5,26,32,33 The esophageal tissueis more vulnerable to poor healingbecause of its lack of a protectiveserosal covering. Tension at anasto-mosis sites, reduced vascularity, andlong surgical ischemic time alongwith poor nutritional status and his-tory of chemoradiation are contrib-utory.19 Anastomotic leak was themost common surgical complication.3
Anastomosis breakdown allowsnonsterile secretions to drain intothe mediastinum, often resulting inmediastinitis. Patients who had aleak identified experienced an
Figure 10 Thoracotomy incision closed with liquid skin adhesive.
Figure 11 The cervical incision is open and the red gauze bandage is brought upfrom the chest through the opening.
78 CriticalCareNurse Vol 31, No. 4, AUGUST 2011 www.ccnonline.org
by AACN on June 18, 2018http://ccn.aacnjournals.org/Downloaded from

increased mortality rate of 37%.33
The cervical anastomosis has a higherincidence of developing a leak, inabout 10% of all cases. In contrast,mediastinal anastomosis leaks arerare, with about a 5% occurrencerate. The cervical anastomosis iseasier to drain and repair than isthe mediastinal anastomosis.19
Anastomosis leaks are graded on ascale of I to IV. A thoracic grade IVleak has a 90% mortality and agrade III leak has a 60% mortality.19
These leaks are verified by a contrast-enhanced swallowing study.30-37
Chyle Leak. A chyle (fluid fromthe lymphatic vasculature) leak isnoted as milky fluid draining fromthe chest tube and results frominjury of the thoracic duct, whichlies behind the esophagus anddrains from the midsternal area.The lymph system is a low-pressuresystem, which makes detection of aleak difficult. A chyle leak may benoted from a chest tube or incisionwhen the patient is fed by tube ororally. Chyle is defined as intestinallymphatic fluid that is enriched withfat, which is absorbed in the intes-tinal lumen and drained away bythe lymphatic system.34,35 The intro-duction of enteral nutrition increasesfat levels, which turn the chyle intoa visible white fluid. If the chest tubeoutput is white, testing is completedto rule out a chyle leak. Testing mayinclude measurement of triglyceridelevel of the fluid draining from thechest tube while the patient isreceiving feedings. A triglyceridelevel greater than 1.2 mmol/L isconsidered diagnostically positivefor a chyle leak.34,35
Incidence of a chyle leak afteresophagectomy is between 2% and4%.3,4,32 The chyle leak is often very
Figure 12 Cervical incision is closed with a Penrose drain coming out of the distalend of the incision.
Figure 13 Surgically placed abdominal tubes.
Jejunostomyfeeding tube
Main gastric port Keep to drainage orsuction as ordered
Second gastric portKeep open to air;
never clamp or cap!
Table 3 Transhiatal vs transthoracic esophagectomy
Transhiatal
Used for adenocarcinoma/barium enemaDecreased surgical timeDecreased blood lossLess painfulDecreased reflux developmentNeck anastomosis leakage easier to
control/repair
Transthoracic
More established, in use longerAccommodates larger tumorMore painfulIncreased direct visualizationAllows for en bloc nodal excisionCommon use of squamous cell cancerAnastomosis leakage hard to repair Increased incidence of pulmonary
complications
www.ccnonline.org CriticalCareNurse Vol 31, No. 4, AUGUST 2011 79
by AACN on June 18, 2018http://ccn.aacnjournals.org/Downloaded from

difficult to repair surgically or ligate.There are 2 types of chyle leaks: lowoutput and high output. Low output(<10 mL/kg per day) commonlyresolves without further surgical treat-ment.34 High output (>10 mL/kg perday) requires surgical interventionto ligate the thoracic duct.34 A chyleleak may cause the patient to havehigh volumes of fluid loss and mal-nutrition along with possible immunecompromise.35 It is this loss of chylefluid that puts the patient at increasedrisk for sepsis.34,35
Gastric Necrosis. One of the mostformidable complications ofesophagectomy is gastric necrosis,which is seen in 2% to 3% of patientsrecovering from esophagectomy.3,4,32,37
With this complication, the necroticgraft must be disconnected from thestomach. The necrosis can occur fora number of reasons, such as poorblood flow or poor surgical tech-nique. Stomach tissue that is viablewill be oversewn and left discon-nected, preventing drainage of gas-tric contents. The viable tissue inthe upper part of the esophaguswill be brought out through a cervi-cal incision (either existing or newlymade). The term cervical esophagos-tomy or spit-fistula refers to a com-plete disconnection between themouth and the newly fashionedesophagus. Spit (saliva) from themouth is allowed to drain away
through a surgically made fistulainto a bag or a dressing. This proce-dure prevents aspiration of drainageinto the lungs and allows time forthe compromised tissue to heal. Afterthe patient has recovered/healed, asecond surgery will be done to replacethe failed esophageal transplant(stomach). A colonic interpositionor even an ileoconduit could beused in place of the esophagus.33,36,37
Acute Postoperative Nursing Care
Postoperative patients oftenawaken in the ICU and can becomequickly overwhelmed by all of thecatheters, wires, tubes, and noisessurrounding them. No amount ofpreoperative teaching preparespatients for this first impression:multiple incisions often with bloodydressings, multiple tubes comingout of their body, and pain whenthey move or breathe. Nursing careof postoperative patients is often abalance to maintain needed hydra-tion while actively managing devel-oping pulmonary congestion,providing pain control, and offeringemotional support. Often thesepatients have a current smokingand/or drinking history that maycomplicate their stay as they experi-ence withdrawal.
Close observation and activemanagement by the ICU nurse are
vital to prevent or provide earlytreatment in the management ofpostoperative complications. Suchevents are more common within thefirst 3 days postoperatively whenintensive monitoring should be fol-lowed.19 Hydration, pain control,oxygenation, and tube managementand observation of tube drainageare of primary concern for esophagec-tomy patients.
HydrationIt cannot be overstated that
hydration is of primary importancein management of esophagectomypatients. Hydration ensures that thecirculating volume in the vascularsystem can adequately deliver neededoxygen and nutrients to promotehealing. Removal of the esophagus,multiple incisions, and long opera-tive time all combine to lead to highinsensible fluid loss. This situationmakes the patient prone to fluid lossfrom intravascular to extravascularspaces. Although the patient mayappear edematous and well per-fused, the created single-vessel graftis actually at risk for poor perfusion.
Four main arteries did supplyblood flow to the stomach (Figure 3).Three of these arteries have beenligated, leaving the right gastroepi-ploic artery as the sole artery sup-plying blood flow to the stomachsegment and distal anastomosis.The newly made esophagus anasto-mosis is located at the farthest pointaway from the right gastroepiploicartery. Proper hydration allowsgood blood flow to ensure healingof the surgical site. Vasopressor sup-port is poorly tolerated and avoidedif possible in these patients. Vaso-constriction further reduces bloodflow to anastomotic sites.
Table 4 Pulmonary complications
Preoperative factors
SmokingChronic obstructive pulmonary diseaseIncreased ageMalnutritionDecreased activity levelChemoradiation
Surgical factors
Length of surgeryExtent of lymph node dissectionReduced vascularization to
bronchopulmonary treeSurgical approach
80 CriticalCareNurse Vol 31, No. 4, AUGUST 2011 www.ccnonline.org
by AACN on June 18, 2018http://ccn.aacnjournals.org/Downloaded from

Hypovolemic shock can developeasily after surgery. One of the firstsigns of shock is cool clammy skin,which indicates that the skin is thefirst organ involved. The secondorgan would be the gut, shuntingblood to the core areas of the body.The reason esophagectomy patientsare at a high risk for shock relates tothe surgical environment. Long sur-gical times with tissues exposed tocooler temperatures allow increasedbleeding and fluid losses. The insen-sible losses during this surgery arehigh, with manipulation and removalof gastric segments, lymph tissues,cautery of tissue and bleeders allcontributing. Base intravenous fluidrates start out at 100 mL/h of lactatedRinger solution, but rates can be upto 250 mL/h. Multiple fluid bolusesmay be given, for example, 500 mLto 1000 mL of lactated Ringer solu-tion or normal saline. The goal ofgiving more fluid is to maintain fluidbalance while offsetting third spacing,which is common in these patients.
Esophagectomy patients havestrong indications for the use of acentral catheter. One advantage ofplacing a central catheter is to allowhigh infusion rates of fluids withoutrisk of infiltration. Measurement ofcentral venous oxygen saturationlevels is an important tool. Changesin central venous oxygen saturation(normal range, 60%-70%) are thefirst signs that the body is using moreoxygen than usual.38 Treating abnor-mal levels early helps avoid the devel-opment of lactic acidosis. Anotheradvantage is avoiding the use ofperipheral access for the first 24hours. These patients can be as muchas 6 L positive in fluid balance thefirst day after surgery. The resultingedema makes the risk of infiltration
high and gaining further peripheralaccess more difficult.
Pain ControlPain control in esophagectomy
patients is very difficult and chal-lenging to manage. The patientscannot have any oral medicationintake for at least a week. Thus onlyintravenous medication (intramus-cular and subcutaneous routes areunreliable in this population withswelling and fluid shifts) are avail-able for pain control, often with theunwanted adverse effects ofhypotension, apnea, itching, hallu-cinations, nausea, and altered sleeppatterns. The difficulty in control-ling pain relates to the multiplesites that are involved in this surgi-cal procedure. Pain located in theback, arm, chest, or abdomen, inci-sion pain, and pain with deep inspi-ration may all occur simultaneously.Multiple methods of relieving painare used, such as epidurals, patient-controlled analgesia (PCA) with basaland bolus rates, and routine andbreakthrough pain orders.
All patients have a thoracicepidural catheter placed in theoperating room. It is important forthe ICU nurse to ask if any medica-tions have been given through theepidural catheter, because medica-tions given by this route can haveprolonged effects. Some patientswill receive morphine injection viaepidural during the procedure. Aphysician can inject preservative-free morphine with a maximumdosage of 10 mg in a 24-hour period.Because the epidural route is used,no diffusion barrier is present andlower doses produce greater andlonger lasting effects. General dos-ing of preservative-free morphine
starts at 2 mg. Patients will comefrom the operating room with theepidural catheter capped. It is thebedside nurses’ responsibility toensure that the proper infusion isinitiated per epidural route. Theepidural infusion is generally bupi-vacaine started at a rate of 4 mL/hto a maximum rate of 12 mL/h.The doctor may push preservative-free lidocaine through the epiduralfor added pain relief.
PCA involves use of a pump thatcan be programmed to run a basalrate or the patient can use a buttonto receive programmed bolus doses.Usually both functions are used foresophagectomy patients. The PCAis commonly programmed with 1of 3 medications: morphine, dilau-did, or fentanyl.19,39 Morphine is themost widely used of the 3 medica-tions.19,39 A morphine bolus canrange from 1 to 10 mg; initial PCAsettings are often set at a 1-mg boluswith a repeat bolus in 10 minutes.This setting provides a maximumof 6 doses in a 1-hour time frame.The nurse must assess the patientand judge whether this dosing isappropriate.
When checking/reviewing thePCA program, attempts and deliv-eries are recorded. A good nonver-bal indicator that pain is notcontrolled would be more recordedattempts than deliveries, whichshould lead the nurse to assess thepatient for more pain medication.Interventions could include increas-ing the dose or frequency of med-ication. Frequent reassessment ofpain may be necessary. Dilaudid,another medication frequently usedin PCAs, is a synthetic version ofmorphine. Dilaudid is 4 times asstrong as morphine. This medication
www.ccnonline.org CriticalCareNurse Vol 31, No. 4, AUGUST 2011 81
by AACN on June 18, 2018http://ccn.aacnjournals.org/Downloaded from

is favored when the patient has renalinsufficiency due to the drugs clear-ance by the liver. The PCA would bestarted at a bolus of 0.25 mg every15 minutes and can be adjusted inthe same manner as morphine. Thefinal PCA medication is fentanyl, asynthetic derivative of morphinethat is 100 times more potent thanmorphine. The PCA would be startedat a bolus of 25 μg every 15 minutesand could also be adjusted in thesame manner as morphine.
Problems with the PCA andintravenous pain medications arethe peaks-and-valleys effect, wherebythe narcotic works quickly but alsowears off quickly, requiring escalat-ing doses.39 The PCA pump also hasa function called continuous rate orbasal rate. This basal rate is goodfor providing a continuous level ofpain control. This mode would bebeneficial to patients for its night-time dosing that allows patients tosleep and would thus help promoteappropriate sleep patterns. ThePCA can then be converted to bolusdosing during the day. Basal ratefunction is commonly used onpatients receiving mechanical venti-lation, whereas the basal rate maycause respiratory compromise inpatients who are not receivingmechanical ventilation.
With careful focused assess-ments, nurses can avoid compro-mise and ensure that adequatepain control is provided. Nursesshould also be aware of and famil-iar with the adjunctive medica-tions that could be used, such asdiphen hydra mine (for itching),ondansetron (nausea), promet-hazine (nausea), prochlorperazine(nausea), and naloxone (narcoticoverdose or itching).
OxygenationThe fraction of inspired oxygen
is initially decreased on the basis ofresults of arterial blood gas analysis,and then trends are monitored viapulse oximetry and capnography.Pulse oximetry and capnography,however, show only trends.
Major changes should be veri-fied by arterial blood gas analysis.One of the largest limiting factors inthe treatment of esophagectomypatients is how much fluid can betolerated in conjunction with properoxygenation.19 Esophagectomypatients’ fluid balance tends to be2 to 6 L positive. This positive fluidbalance coupled with a preexistingcondition such as chronic obstruc-tive pulmonary disease, emphysema,smoking history, obstructive sleepapnea, or morbid obesity can leadto increased difficulty in oxygendelivery. These patients are notplaced on continuous or bilevel pos-itive airway pressure to prevent thedevelopment of an anastomotic leakor dehiscence. If the patient cannotbe weaned from the ventilator, pro-longed use of an endotracheal tubeor early tracheotomy may be needed.
Early extubation is the goal foresophagectomy patients when allparameters permit extubation. Rein-tubation can be a very high-risk pro-cedure in such patients because ofthe increased edema; esophagealintubation could disrupt the surgicalanastomosis. The nasal cannula foroxygen delivery allows active pul-monary hygiene to be practiced bythe patient. The most common andeffective forms remain incentivespirometry along with turning,coughing, and deep breathing.Early ambulation is encouraged tohelp restore normal circulation and
body functions. All forms of pul-monary hygiene have the objectiveof reducing atelectasis and prevent-ing pneumonia.
Tube Management and Drainage Postoperative care also includes
the management and care of manytubes and drains. A nasogastrictube is placed during surgery, andnurses should be able to hear thesuction sound through the airlumen of the tube when suction isapplied (Figure 13). Listening forthat sound is important to ensurethat the suction does not cause thetube to become lodged against thewall of the stomach and cause anulcer. Repositioning of the nasogas-tric tube and use for medications orfeedings should be strictly avoided.Nasogastric tubes may be flushedwith saline to maintain patency.
All tube-administered medica-tions should be given via the J tubethat was placed during the initialsurgery. Fluids should be kept asthin as possible and flushed with 30to 45 mL of normal saline or waterto prevent tube clotting. It may beseveral days postoperatively beforeuse of the J tube is started.
Pleural and/or mediastinal chesttubes are placed around an anasto-mosis and must be assessed fordrainage (amount and color)changes. Outputs of 100 mL/h arecommon. These drains are moni-tored for changes in amount, color,and consistency of the drainagefluid. A Penrose drain from the cer-vical incision or a chest tube from athoracic incision can aid in detec-tion of an anastomotic or chyle leak and may provide an outlet for accumulated fluid near anasto-mosis sites.
82 CriticalCareNurse Vol 31, No. 4, AUGUST 2011 www.ccnonline.org
by AACN on June 18, 2018http://ccn.aacnjournals.org/Downloaded from

Generally, in the Ivor-Lewisapproach, a chest tube is placednear the midchest anastomosis. Inthe transhiatal approach, a Penrosedrain is placed at the high-neckanastomosis and brought out throughthe cervical neck incision. Drainplacement is especially importantafter enteral feedings have beenstarted and anastomotic leaks maybe more pronounced with the intro-duction of that additional fluid intake.Viewing bile from the chest tubeand or saliva from a cervical neckincision are signs of an anastomoticleak. Tube feedings and instillationof fluids in these tubes are promptlystopped and medical staff notified.19
Recovery Stage Nursing CarePatients are strongly encouraged
to be up in the chair as quickly aspossible to maximize coughing anddeep breathing exercises. Patientswho cannot sit up in the chair mustbe turned frequently. If more than24 hours in bed is necessary, thenurse may order a turning bed, whichhelps avoid hypotension. Turningbeds also improve oxygenation bypositioning each lung superiorly sev-eral times each hour. The advantageof turning is not in the angle of theturn but in the change of position ormotion such as a recurring 10-minuterotation. Turning helps to provide apulmonary toileting effect and pre-vent atelectasis.
Ambulation is a strong factor inhelping to promote fluid movementand preventing edema. The venoussystem involves a series of valves thatallow fluid to flow one way, and whenpatients are sedentary, the fluid poolsand causes swelling. With ambula-tion, fluid is pushed back to the heartand filtered out of the body by the
kidneys. Generally in esophagectomypatients, a fluid shift is seen at about72 hours after the surgery andautodiuresis begins. By ambulating,the patient is forced to take a deepbreath, thus preventing atelectasis.Another advantage of ambulation isthat the bowel function that isdecreased by all the pain medica-tion is improved because walkingpromotes bowel motility.
Recovery MilestonesRecovery from an esophagectomy
is often not easy or timely. Compli-cations may be many, can be severe,and prolong the postoperative course.The patient’s ICU stay may beextended to allow closer monitoringbefore transfer to a general surgicalunit. Because of this fact, it is oftendifficult to provide patients andtheir families with information onwhat to expect as far as the timingof the hospital stay. Nationwidestatistics from the Agency forHealthcare Research and Qualityindicate that the mean postopera-tive stay is 16.2 days for the entirehospital stay.40-43
Oral intake will be not allowedfor at least 1 week to ensure adequatetime for the anastomosis to heal.Medications and nutrition will beadministered either intravenouslyor through the J tube. After 5 to 7days, a barium swallow study willbe performed to evaluate for anasto-motic leaks. If the study is negative(no leaking noted), oral intake maybe started and the nasogastric andchest tubes may be removed ifdrainage is within normal limits. Ifthe swallow study shows a leak, theleak is considered a serious compli-cation that may require surgery orpossible draining, prolonging the
patient’s recovery and lengtheningthe hospital stay.
Providing nutritional support isoften a challenge to these patientswho often are malnourished andweakened because of the diseaseprocess before surgery. Somepatients may receive chemotherapyor radiation before surgery toshrink the tumor, which can causeloss of appetite and increase dys-phagia, further compromisingtheir nutritional status.
Tube feedings may be startedafter bowel sounds are noted andthe patient is passing flatus. Supple-mented enteral feedings may con-tinue for many months after surgerywhile the patient slowly makes thetransition to a normal diet. Postop-erative weight loss is common, asoral intake may be poorly toleratedat first. The newly fashionedesophagus no longer has the motil-ity properties of the original organ,and the remainder of the stomachno longer provides a large “holdingtank” for foods to be digested.Thus patients must eat smallermeals and possibly remain uprightfor a longer period to allow food tobe digested.
The patient with an uncompli-cated postoperative course willtypically be discharged from thehospital approximately 2 weeksafter the surgery. At that point, thepatient should be tolerating liquidsand tube feedings may be changedfrom continuous to cyclic (infusingat night) to help promote oralintake during the day. Education isrequired regarding wound care,pain control, and signs and symp-toms of infection. Patients willrequire frequent follow-up to evalu-ate their progress.
www.ccnonline.org CriticalCareNurse Vol 31, No. 4, AUGUST 2011 83
by AACN on June 18, 2018http://ccn.aacnjournals.org/Downloaded from

SummaryAlthough surgery remains the
best option for treating esophagealcancer, local recurrence and distantmetastases remain common. Con-cerns about the quality of life areserious because of the long recoverytime and poor survival rate. Majorand minor complications occur in40% of patients, with only a minor-ity symptom free after 5 years. Datashow a 50% morbidity rate and a10% mortality rate within 30 daysof surgery. The prognosis for recov-ery from an esophagectomy remainslow with the national average16%.3,4,40-43 Early diagnosis, surgicaladvancements, and improvement inpostoperative care continue to con-tribute to improved outcomes.40-44
Curative treatment has normallybeen measured by survival rates,but few studies have explored func-tional outcomes and quality-of-lifeissues. Often patients report a mini-mum of 6 to 12 months recoverybefore they have been able to returnto a somewhat normal daily pattern.Common symptoms that happenafter recovery are gastric reflux,dumping syndrome, and difficultyswallowing. Often patients have dif-ficulty dealing with the dietarychanges now required. Many patientsmay not tolerate an oral diet wellfor months after discharge. Becausepatients have to change dietaryhabits, a return to previous lifestyle
and activities is often hindered bothphysically and mentally.
As the patient progresses towarddischarge, nursing care changes tofocus on increasing functional lev-els, wound healing, nutritional sup-port, and patients’ emotional andeducational needs. Few patients willbe discharged from the hospitalwithout need for a healthcareprovider (often a family member) orassistance from a home-healthnurse to continue recovery. Regard-less of these developments, manyof these patients can function athome and return to work. CCN
Financial DisclosuresNone reported.
References1. Cancer Trends Progress Report—2007
Update, National Cancer Institute, NIH,DHHS, Bethesda, MD, December 2007.http://progressreport.cancer.gov/2007/.Accessed May 27, 2011.
2. National Cancer Institute. Surveillance Epi-demiology and End Results (SEER) Website. http://seer.cancer.gov/statfacts/html/esoph.html. Accessed May 27, 2011.
3. Tomaszek S, Cassivi SD. Esophagectomy forthe treatment of esophageal cancer. Gas-troenterol Clin North Am. 2009;38:169-181.
4. Enestved CK, Perry KA, Kim C, et al. Trendsin the management of esophageal carcinomabases on provider volume: treatment prac-tices of 618 esophageal surgeons. Dis Esoph-agus. 2010;23(2):136-144.
5. Boone J, Levestro DP, Elias Sjoerd G, et al.International survey on esophageal cancer:part I surgical techniques. Dis Esophagus.2009;22:195-202.
6. Kuo B, Urma D. Esophagus: anatomy anddevelopment. GI Motility Online 2006).Web site. http://www.nature.com/gimo/contents/pt1/full/gimo6.html. AccessedMay 27, 2011.
7. Tomizawa Y, Wang KK. Screening, surveil-lance, and prevention for esophageal cancer.Gastroenterol Clin North Am. 2009;38:59-73.
8. Esophagus. In: American Joint Committee onCancer: AJCC Cancer Staging Manual. 7thed. New York, NY: Springer; 2006:77-88.
9. Wang J, Liu F, Gao H, et al. The symptom-to-treatment delay and stage at the time oftreatment in cancer of esophagus. Jpn J ClinOncol. 2008;38:7-91.
10. Barbour AP, Jones M, Gonen M, et al.Refining esophageal cancer staging afterneoadjuvant therapy: importance of treat-ment response. Ann Surg Oncol. 2008;15(10):2894-2902.
11. Luu T, Gaur P, Force S, et al. Neoadjuvantchemoradiation versus chemotherapy forpatients undergoing esophagectomy foresophageal cancer. Ann Thorac Surg.2008;85:1217-1224.
12. Schneider B, Urba S. Preoperative chemora-diation for the treatment of locoregionalesophageal cancer: the standard of care.Semin Radiat Oncol. 2006;17:45-52.
13. Gibbs JF, Rajput A, Chadha KS, et al. Thechanging profile of esophageal cancer pres-entation and its implication for diagnosis.National Med Assoc. 2007;99:620-626.
14. Souza RF, Spechler S. Concepts in the pre-vention of adenocarcinoma of the distalesophagus and proximal stomach. Can JClin. 2005;55:334-351.
15. Scudiere JR, Montgomery EA. New treat-ments, new challenges: pathology’s perspec-tive on esophageal carcinoma. GastroenterolClin North Am. 2009;38:121-133.
16. Greenstein AJ, Wisnivesky JP, Litle VR.Effect of local therapy for the treatment ofsuperficial esophageal cancer in non-opera-tive candidates. Dis Esophagus. 2008;21:673-678.
17. Thompson SK, Ruszkiewicz AR, JamiesonG, et al. Improving the accuracy of TNMstaging in esophageal cancer: a pathologicalreview of resected specimens. Ann SurgOncol. 2008;15(12):3447-3458.
18. Ajani Jaffer A. Future developments onesophageal cancer research. GastroenterolClin North Am. 2009;38:183-188.
19. Patterson GA. Pearson’s Thoracic andEsophageal Surgery. Vol 2. 3rd ed. Philadel-phia, PA: Churchill Livingstone Elsevier, 2008.
20. Eslick G. Esophageal cancer: a historicalperspective. Gastroenterol Clin North Am.2009;38:1-15.
21. Rossine ARAL, Hashimoto CL, Iriya K, et al.Dietary habits, ethanol and tobacco con-sumption as predictive factors in the devel-opment of esophageal carcinoma in patientswith head and neck neoplasms. Dis Esopha-gus. 2008;21:316-321.
22. Kamangar F, Chow WH, Abnet CC, DawseySM. Environmental causes of esophagealcancer. Gastroenterol Clin North Am. 2009;38:27-57.
23. Falk G. Risk factors for esophageal cancerdevelopment. Surg Oncol Clin North Am.2009;18:469-485.
24. Dowson HMP, Strauss D, Ng R, et al. Theacute management and surgical reconstruc-tion following failed esophagectomy inmalignant disease of the esophagus. DisEsophagus. 2007;20:135-140.
25. Wolff CS, Castillo SF, Larson DR, et al. IvorLewis approach is superior to transhiatalapproach in retrieval of lymph nodes atesophagectomy. Dis Esophagus. 2009;22:328-333.
26. Boone J, Liverstro DP, Elias SG, et al. Inter-national survey on esophageal cancer: partII staging and neoadjuvant therapy. DisEsophagus. 2009;22:203-210.
27. Schroder W, Bollschweiler E, Kossow C, et al.Preoperative risk analysis—a reliable pre-dictor of postoperative outcome aftertransthoracic esophagectomy? LangenbecksArch Surg. 2006;391:455-460.
To learn more about gastrointestinal issues,read “Emergency Subtotal Colectomy in aJehovah’s Witness With Massive LowerGastrointestinal Bleeding: ChallengesEncountered and Lessons Learned” byRaman and colleagues in the American Journal of Critical Care, 2011;20:176-178.Available at www.ajcc online.org.
Now that you’ve read the article, create or contributeto an online discussion about this topic using eLetters.Just visit www.ccnonline.org and click “Submit aResponse” in either the full-text or PDF view of thearticle.
84 CriticalCareNurse Vol 31, No. 4, AUGUST 2011 www.ccnonline.org
by AACN on June 18, 2018http://ccn.aacnjournals.org/Downloaded from

www.ccnonline.org
28. Egberts J, Schniewind B, Bestmann B, et al.Impact of the site of anastomosis after onco-logic esophagectomy on quality of life: aprospective, longitudinal outcome study.Ann Surg Oncol. 2008;15(2):566-575.
29. Low D, Kunz S, Schembre D, et al.Esophagectomy: it’s not just about mortalityanymore: standardized perioperative clini-cal pathways improve outcomes in patientswith esophageal cancer. J Gastrointest Surg.2007;11:1395-1402.
30. Sarela A, Tolan DJ, Harris K. Anastomoticleakage after esophagectomy for cancer: amortality-free experience. J Am Coll Surg.2008;206(3):516-523.
31. Goan Y, Chang H, Hsu H, et al. An audit ofsurgical outcomes of esophageal squamouscell carcinoma. Eur J Cardiothorac Surg. 2007;31:536-544.
32. Bailey S, Bull D, Harpole D, et al. Outcomesafter esophagectomy: a ten-year prospectivecohort. Ann Thorac Surg. 2003;75:217-222.
33. Turkyilmaz A, Eroglu A, Aydin Y, et al. Themanagement of esophagogastric anastomoticleak after esophagectomy for esophagealcarcinoma. Dis Esophagus. 2008;22:119-126.
34. Lagarde S, Omloo MT, Jong K, et al. Inci-dence and management of chyle leakageafter esophagectomy. Ann Thorac Surg.2005;80:449-454.
35. Hayden JD, Sue-Ling HM, Sarela AI, et al.Minimally invasive management of chylousfistula after esophagectomy. Dis Esophagus.2007;20:251-255.
36. Michelet P, D’journo X, Roch A, et al. Peri-operative risk factors for anastomotic leak-age after esophagectomy. Chest. 2005;128:3461-3466.
37. Dowson H, Strauss D, Ng R, et al. The acutemanagement and surgical reconstructionfollowing failed esophagectomy in malignantdisease of the esophagus. Dis Esophagus.2007;20:135-140.
38. Collaborative Study Group on PerioperativeScv02 Monitoring. Multicenter study onperi- and postoperative central venous oxy-gen saturation in high-risk surgical patients.Crit Care. 2006;10:R158.
39. Klaus L. Recent developments in patient-controlled analgesia. J Pain Symptom Manage.2005;29(5):72-80.
40. Clifton JC, Finley RJ, Gelfand G, et al. Devel-opment and validation of a disease-specificquality of life questionnaire (EQOL) forpotentially curable patients with carcinomaof the esophagus. Dis Esophagus. 2007;20:191-201.
41. Lagarde SM, Franssen SJ, vanWerven JR, et al.Patient preferences for the disclosure ofprognosis after esophagectomy for cancerwith curative intent. Ann Surg Oncol.2008;15(11):3289-3298.
42. Parameswaran R, McNair A, Avery KNL, et al.A role of health-related quality of life out-comes in clinical decision making in surgeryfor esophageal cancer: a systematic review.Ann Surg Oncol. 2008;15(9): 2372-2379.
43. Chang LC, Oelschlager BK, Quiroga E, et al.Long-term outcome of esophagectomy forhigh-grade dysplasia or cancer found duringsurveillance for Barretts’s esophagus. J Gas-trointest Surg. 2006;10(3):341-346.
44. Avery K, Metcalfe C, Nicklin, J, et al. Satis-faction with care: an independent outcomemeasure in surgical oncology. Ann SurgOncol. 2006;13(6):817-822.
by AACN on June 18, 2018http://ccn.aacnjournals.org/Downloaded from

CCN Fast Facts CriticalCareNurseThe journal for high acuity, progressive, and critical care
Road Map to Esophagectomy for Nurses
treatment. Surgery remains challenging and complicated. Mul-tiple surgical approaches are available, with the choice deter-mined by tumor location and stage of disease.
Recovery is often fraught with complications—both physi-cal and emotional. Nursing care of postoperative patients isoften a balance to maintain needed hydration while activelymanaging developing pulmonary congestion, providing paincontrol, and offering emotional support. Often these patientshave a current smoking and/or drinking history that may com-plicate their stay as they experience withdrawal.
Close observation and active management by the intensivecare unit nurse are vital to prevent or provide early treatment inthe management of postoperative complications. Such eventsare more common within the first 3 days postoperatively whenintensive monitoring should be followed. Hydration, pain con-trol, oxygenation, and tube management and observation oftube drainage are of primary concern for esophagectomypatients.
Even after recovery, local recurrence and distant metastasesare common. Early diagnosis, surgical advancement, andimprovements in post operative care continue to improve out-comes.
FactsEsophageal cancer, although considered uncommon in the
United States, continues to exhibit increased incidence.Esophageal cancer now ranks seventh among cancers in mor-tality for men in the United States. Even as treatment continuesto advance, the mortality rate remains high, with a 5-year sur-vival rate less than 35%.
The causes of esophageal cancer have never been clearlyidentified, but evidence shows a strong link to environmentalcarcinogens. Chronic irritation of the esophagus has long beenconsidered a major predisposing factor for both types ofesophageal cancer. Chronic exposure to the environmental car-cinogens associated with excessive alcohol consumption andlong-time cigarette smoking have been more closely related todevelopment of squamous cell cancer. The longer the use andthe higher the intake of alcohol and cigarettes, the greater therisk of esophageal cancer developing. Combined use of smok-ing and drinking also expands the risk. All identified risk fac-tors for esophageal cancer are listed in the Table.
Esophageal cancer typically is discovered in advancedstages, which reduces the treatment options. When disease islocally advanced, esophagectomy remains the standard for
Logue B, Griffin S. Road map to esophagectomy for nurses. Crit Care Nurse. 2011;31(4):69-86.
Table Risk factors for esophageal cancer
Squamous cell carcinoma
Chronic tobacco use Heavy alcohol use History of head or neck cancer History of radiation therapy Chronic esophagitisChronic stricture or achalasiaDietary/nutritional deficiencyLow intake of fruits/vegetables High intake of red meat or nitrate-containing foodsConsumption of scalding hot beverages
Adenocarcinoma
Cigarette smokingObesityAlcohol consumptionGastroesophageal reflux diseaseBarrett esophagus
86 CriticalCareNurse Vol 31, No. 4, AUGUST 2011 www.ccnonline.org
by AACN on June 18, 2018http://ccn.aacnjournals.org/Downloaded from

Barbara Logue and Scott GriffinRoad Map to Esophagectomy for Nurses
http://ccn.aacnjournals.org/Published online ©2011 American Association of Critical-Care Nurses
10.4037/ccn2011426 69-86 31 2011;Crit Care Nurse
http://ccn.aacnjournals.org/cgi/external_ref?link_type=PERMISSIONDIRECTPersonal use only. For copyright permission information:
http://ccn.aacnjournals.org/subscriptions/Subscription Information
http://ccn.aacnjournals.org/misc/ifora.xhtmlInformation for authors
http://www.editorialmanager.com/ccn Submit a manuscript
http://ccn.aacnjournals.org/subscriptions/etoc.xhtmlEmail alerts
362-2049. Copyright ©2016 by AACN. All rights reserved. bimonthly by AACN, 101 Columbia, Aliso Viejo, CA 92656. Telephone: (800) 899-1712, (949) 362-2050, ext. 532. Fax: (949) Critical Care Nurse is an official peer-reviewed journal of the American Association of Critical-Care Nurses (AACN) published
by AACN on June 18, 2018http://ccn.aacnjournals.org/Downloaded from