Functional Anatomy of the Diabetic Foot Cavanagh …...AdAndersen H. Al dAccelerated atrophhy off...
129
Huub J.L. van der Heide MD PhD, Leiden, the Netherlands. Peter R Cavanagh PhD, Seattle, USA FUNCTIONAL ANATOMY OF THE DIABETIC FOOT
Transcript of Functional Anatomy of the Diabetic Foot Cavanagh …...AdAndersen H. Al dAccelerated atrophhy off...

Huub J.L. van der Heide MD PhD, Leiden, the Netherlands. , ,Peter R Cavanagh PhD, Seattle, USA
FUNCTIONAL ANATOMY OF THE DIABETIC FOOT

Sign‐up for a download of Sign up for a download of the presentation
Write your Email on the sheet being passed daround
or Email Peter Cavanagh:

OutlineOutline
Neuropathic syndromeseu opat c sy d o es Comparison with the foot in Hereditary Motor and Sensory Neuropathy (HSMN)
Evidence for Musculoskeletal Changes MRI Studies of extrinsics
S d f MRI Studies of intrinsics Structural and Functional Characteristics
Cl t Ski Claw toes Skin Tissue Stiffness Joint Mobility Gait Posture Gait Posture

EvidenceEvidence
Wh ibl ill f id i Where possible, we will refer to evidence in the literature.
f ll b h d l d bl References will be on the downloadable handout

Changes in the Extrinsic Changes in the Extrinsic Muscles of the Leg

Approach to StudyApproach to Study

Changes in the Extrinsic Changes in the Extrinsic MusclesKey paper
Andersen H, Gadeberg PC, Brock B, Jakobsen J.Muscular atrophy in diabetic neuropathy: a Muscular atrophy in diabetic neuropathy: a stereological magnetic resonance imaging study. Diabetologia. 1997 Sep;40(9):1062‐9.g p

Note the fatty infiltration
Neuropathic Non‐neuropathic

Volume of Ankle dorsiflexorsand plantar flexors was and plantar flexors was reduced by 32% compared to y 3 pnon‐neuropathic patients

Loss progressed proximal to distaldistal
3% ‐3% ‐43% 43
‐65%

What are the functional What are the functional consequences?

Changes in the Extrinsic Changes in the Extrinsic MusclesKey paper
Andersen, Nielsen, Mogensen & JakobsenMuscle Strength in Type 2 Diabetes Diabetes June Muscle Strength in Type 2 Diabetes Diabetes .June 2004 vol. 53 no. 6 1543‐1548

What are the functional What are the functional consequences?
d % d i f 17 and 14% reduction of strength of ankle flexors (P < 0.02) and ankle extensors (P < 0.03),
At the knee strength of At the knee, strength of extensors and flexors was reduced by 7% (NS) and 14% (P ) ti l< 0.05), respectively.
Wrist and elbow Strength were preserved
Andersen et al. 2004 Muscle strength in type 2 diabetes. Diabetes. 2004 Jun;53(6):1543‐8.

Prospective follow‐up of Prospective follow up of Changes in the Extrinsic M lMuscles
Key paperAndreassenCS, Jakobsen J, Ringgaard S, Ejskjaer N, Andersen H. Accelerated atrophy of lower leg and foot muscles: a follow‐up study of long‐term diabetic
l th i ti i i polyneuropathy using magnetic resonance imaging (MRI). Diabetologia. 2009 Jun;52(6):1182‐91.

Studied 26 type 1 diabetic patients x2: 9‐12 years apartyears apart
Neuropathic
Baseline Follow upBaseline Follow‐up
Control

Annual Volume Loss of 4‐5%Annual Volume Loss of 4 5%
Plantar Flexors Dorsiflexors

Changes were Correlated with Changes were Correlated with Severity of Neuropathy
Plantar Flexors Dorsiflexors

Changes in the Intrinsic Changes in the Intrinsic Muscles of the Foot

K PKey Paper:Bus SA, Yang QX, Wang JH, Smith MB,
d l h C h lWunderlich R, Cavanagh PR. Intrinsic muscle atrophy and toe deformity in the diabetic
thi f t ti neuropathic foot: a magnetic resonance imaging study. Diabetes Care. 2002 Aug;25(8):1444 50Aug;25(8):1444‐50.

20
Age Matched Control Neuropathic

50 year old Neuropathic 53 year old non‐Neuropathic PatientControl
21

Prospective follow‐up of Prospective follow up of Changes in the Intrinsic M lMuscles
Key paperAndreassenCS, Jakobsen J, Ringgaard S, Ejskjaer N, A d H A l d h f l l d Andersen H. Accelerated atrophy of lower leg and foot muscles: a follow‐up study of long‐term diabetic polyneuropathy using magnetic resonance imaging polyneuropathy using magnetic resonance imaging (MRI). Diabetologia. 2009 Jun;52(6):1182‐91.

9‐12 year follow up9 12 year follow up
Neuropathic
Baseline Follow upBaseline Follow‐up
Control

Quantitative DataQuantitative Data
3% per year loss related to neuropathy severity

Claw Toe DeformityClaw Toe Deformity
Key Paper:
Bus SA, Maas M, Cavanagh PR, Michels RP, Levi M. Plantar fat‐pad displacement in neuropathic diabetic patients with toe deformity: a magnetic resonance imaging study. Diabetes Care. 2004 Oct;27(10):2376‐81.

Measurement of fat pad displacement
Thickness under MTHThickness Ratio =
Thickness under MTHThickness under Phalanx

Thickness RatioThickness Ratio
0.6
0.7
0.8
0.3
0.4
0.5
0
0.1
0.2
3
Claw Toe Control
Indicating anterior displacement of fat pad

Claw Toe Deformity and Claw Toe Deformity and Plantar Pressure
Key Paper:
Bus SA, Maas M, de Lange A, Michels RP, Levi M. El d l i hi Elevated plantar pressures in neuropathic diabetic patients with claw/hammer toe deformit J Biomech 200 Sep 38(9) 9 8 2deformity. J Biomech. 2005 Sep;38(9):1918‐25.


600
700
400
500
600
Claw Toe
100
200
300Claw ToeNormal Toes
0
100
MTH P
Toe PressurePressure

Claw Toe DeformityClaw Toe Deformity
Key Paper:Bus SA, Maas M, Michels RP, Levi M. Role of intrinsic muscle atrophy in the etiology of claw toe deformity in diabetic neuropathy may not b i h f d id l b li dbe as straightforward as widely believed.Diabetes Care. 2009 Jun;32(6):1063‐7.
.

Claw Toes Do Not Necessarily yAccompany Intrinsic Muscle Atrophy
2002 Paper
32
2002 Paper

Assessed muscle ImbalanceAssessed muscle Imbalance


Quantitative ResultsQuantitative Results
Muscle atrophy (r =0.18) and muscle p y ( )imbalance (r=0.14) were not well related to toe deformityrelated to toe deformity

Changes in Skin Changes in Skin

Skin Glycosylation has been Skin Glycosylation has been widely documented
Smit AJ, Gerrits EG. Skin autofluorescence as a measure of advanced glycation endproduct deposition: a novel risk marker in chronic kidney glycation endproduct deposition: a novel risk marker in chronic kidney disease. Curr Opin Nephrol Hypertens. 2010 Nov;19(6):527‐33.

Skin GlycosylationSkin Glycosylation
B i h f b d k f h But it has often been used as a marker for other complications, e.g.
chronic kidney disease glycemic variability

Direct Effects on Foot HealthDirect Effects on Foot Health
Pageon H. Reaction of glycation and human skin The human skin: The effects on the skin and its components, reconstructed skin as a model Pathologie BiologieBiologieVolume 58, Issue 3, June 2010, 226‐23

K Key paper: Reihsner et al. Alterations of biochemical and
d l b h l ftwo‐dimensional biomechanical properties of human skin in diabetes mellitus as compared to ff t f i it ti l ti effects of in vitro non‐enzymatic glycation.
Clinical Biomechanics 15 (2000) 379‐386

DMDiabetic Ti i
ESS
Tissue is more
STRE
Control
more than 2x
ff S Controlstiffer than than control
STRAIN

Limited Joint MobilityLimited Joint Mobility
K Key paper:
Glasoe et al. Dorsal mobility and first ray stiffness in patients with diabetes mellitus. Foot Ankle Int. 2004 Aug;25(8):550‐5.

Patients with a i i ipositive prayer sign
had significant first iff ( 0 )ray stiffness (p <.05)
43

Limited Joint MobilityLimited Joint Mobility
K Key paper:
Abate M, Schiavone C, Pelotti P, Salini V.Limited joint mobility in diabetes and ageing: recent advances in pathogenesis and therapy.Int J Immunopathol Pharmacol. 2010 Oct‐Dec;23(4):997‐1003.

Passive ROM reduced Passive ROM reduced (35% AJC/40% MTPJ1)
50
)
AJC Passive
MPJ P i
30
40
tion (d
eg) MPJ1 Passive
20
nge of M
ot
0
10
Ran
DM Ulcer Control

ROM during Gait ReducedROM during Gait Reduced(19% AJC/24% MTPJ1)
30
20
25
10
15 AJC Gait
MPJ1 Gait
0
5
DM Ulcer Control

Plantar Tissue StiffnessPlantar Tissue Stiffness
Key paper: Key paper: Hsu et al. Diabetic effects on microchambersand macrochambers tissue properties in human and macrochambers tissue properties in human heel pads Clinical Biomechanics 24 (8) October 2009, Pages 682‐6862009, Pages 682 686

Macrochambers
Microchambers

Quantitative ResultsQuantitative Results
32% stiffer in DM
66% l66% lessstiff in DM

Ex vivo StudyEx vivo Study
Pai S, Ledoux WR.,The compressive mechanical properties of diabetic and non‐diabetic plantar soft tissue.pJ Biomech. 2010 Jun 18;43(9):1754‐60.

Quantitative DataQuantitative Data
Diabetic plantar tissue Diabetic plantar tissue 93% stiffer over all locations locations (1147 kPa vs. 593 kPa)

K Key paper:Turner DE, Helliwell PS, Burton AK, Woodburn J.The relationship between passive range of motion and range of motion during gait and plantar pressure measurements. Diabet Med. 2007 Nov;24(11):1240‐6.

POSTURE
Valbo (1979)
53
Valbo (1979)Stephens and Choo (1996) Penfold (1950)
There may be 60‐90 mechanoreceptors per cm2

We generally focus on the loss of touch and pressure sensation but…..
54
Muscle Spindles (Sense of Position and Velocity)

55
Gogi Tendon Organs (Force Control)

Postural StabilityPostural Stability
Tracking Movement of a passive target using VICON
F1
F2
Center ofF1 Center of Pressure migration using a Force Platform
56
Quantifying Postural Sway

10 mm
15‐20 mm
Total path length is summed
Center of Pressure migration in 30 seconds

60
70
40
50
60(c
m)
SWAY
10
20
30
CoP
( S
NormalDM C t l
Eyes open0
10
ControlDMDM Control
NeuropathicSimoneau et al. 1994
DMControl DM
Neuropathic
58Eyes open

60
70
30
40
50oP
(cm
)SW
AY
Eyes closed10
20
30
Co S
NormalDM Control
Neuropathic
Eyes open
Eyes closed0
ControlDM Neuropathic
Simoneau et al. 1994
DMControl DM
Neuropathic
59
Eyes open

GaitGait
Key Paper:Allet et al. Gait characteristics of diabetic patients: a systematic review. Diabetes Metab Res Rev. 2008 Mar‐Apr;24(3):173‐912008 Mar‐Apr;24(3):173‐91.

There is agreement that There is agreement that diabetic patients:
• walk slower • with greater step variability• and higher plantar pressure
than age matched non‐DM controls
61
Allet et al. Gait characteristics of diabetic patients: a systematic review. Diabetes Metab Res Rev. 2008 Mar‐Apr;24(3):173‐91.

Reduced Toe Clearance during Reduced Toe Clearance during Swing
Liu MW, Hsu WC, Lu TW Chen HL Liu HC 250
ControlTW, Chen HL, Liu HC. Patients with type II diabetes mellitus di l d d t
200
(mm)
Control
DM
display reduced toe‐obstacle clearance with altered gait
100
150
learan
ce (
patterns during obstacle‐crossing.Gait Posture 2010
0
50Cl
Gait Posture. 2010 Jan;31(1):93‐9.
Low Medium High

Injuries from Falls
The neuropathic group had:
Injuries from Falls
The neuropathic group had:
• Odds ratios of 15.0 for reported injuries during gait relative to the control group
Si ifi tl l (l f• Significantly lower scores (less safe, p = 0.004) than the control group on perceived safety in unusual conditionsperceived safety in unusual conditions
Cavanagh et al. Problems with gait and posture in neuropathic patients with insulin‐dependent diabetes mellitus. Diabet Med. 1992 Jun;9(5):469‐74.

SummarySummary
• Many changes in structure and function in DM echo those in HMSN
• Muscle atrophy of the intrinsics and extrinsics is notable and progressivenotable and progressive
• The relationship between muscle atrophy/imbalance and claw toe deformity is unclearunclear
• Range of motion at key joints is markedly reduced• Diabetic skin is stiffer than control• Diabetic plantar tissue is stiffer than control• Postural stability is degraded by neuropathy• Gait is slower, more, variable, an obstacle clearance Gait is slower, more, variable, an obstacle clearance
is less.

Functional anatomy For the diabetic foot.
Huub van der Heide, consultant orthopaedic surgeon Leiden University Medical Center ISDF May 2011

“The” diabetic foot


“The” neuropathic foot
• Diabetes • Alcohol • HMSN • Other neurological
disorders

What do I want to discuss?
• pathofysiology
• prevention
• treatment
Of the deformity!

How large is the problem? • About 500.000 diabetes
patients in the Netherlands (total 16 M)
• 15% ‘ll develop an ulcer (75.000)!!
• 15-25% of these will be amputated (10-15.000)



5%
• After 6 weeks (!!) you’ll remember < 5% of this presentation.
• Muscle imbalance
• Deformity
• Compensation

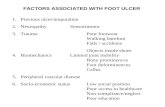
neuropathy
• Those who suffer from having no pain
• Alterred autonomous regulation
– no vasodilatation
– Dry skin
• Alterred motor function
– Secondary foot deformity

causes
• Pressure
• Pressure
• Pressure
• Poor healing



Basic patterns

• Equinus
• Varus
• Cavus (high arch)





Normal anatomy and function
• We start at the back
• Move to distal
• Focus on movement
• Recruitment and deformity

• Plantar flexion – Triceps surae
– Long Peroneal
• Dorsal flexion – AnteriorTibial
muscle
– Long toe extensors
• Eversion – Peronei
– Toe extensors
• Inversion – Anterior Tibial
muscle
– Posterior Tibial Muscle

force
• Triceps > anterior tibial
– So recruitment and/or equinus
• Posterior tibial > peroneal muscle
– Varus deformity
• And the peroneals

• Short peroneal (and tertius) attach to fifth MT
• The long peroneal attaches to
• Plantar side of MT 1!
• Plantar flexion of the first ray:
• Pronation of the forefoot

• The foot is “fixed”to the floor….
• Pronation of the forefoot
– Plantar flexed first ray
• This (hyper) pronation of the forefoot will result in a hindfoot V

• The foot is “fixed”to the floor….
• Pronation of the forefoot
– Plantar flexed first ray
• This (hyper) pronation of the forefoot will result in a hindfoot Varus

Difficult!
• This is the essential part
• When you understand this you can go to the beach

Normal Tarso-metatarsal twist
• pronation hindfoot > supination forefoot
• supination hindfoot > pronation forefoot
‘eversion twist’

Tarso-metatarsal twist

Supination and pronation
• Combined movements
• Supination = inversion+ endorotation + adduction
• Pronation = eversion + exorotation + abduction

• The most important thing is to distinguish a hindfoot varus from a compensatory hindfoot varus due to a plantar flexed first ray!



Treatment
• Custom made shoe with pronation of the foot (allow first ray to plantar flex).
• Maybe surgery??






When we would do an operation..
• Comprehensive approach
• Peroneus longus to brevis transfer
• Tib. Post. to anterior transfer
• Dorsal flexion wedge osteotomy of first ray
• Achilles tendon lenghtening
• Sometimes calcaneus osteotomy
• Sometimes release plantar fascia
• And the toes





Typical neuropatic foot (HMSN)

forefoot
• Long toe extensors recruited to dorsiflex
• Weakness of the intrinsics:
– Extension in MPJ
– Flexion in PIPJ













Release toe extensors




So: a “full-house”
• Posterior tibial transfer 4 incisions
• Peroneal transfer 1 incision
• Achilles tendon 3 incisions
• Osteotomy MT1 1 incision
• Calcaneus osteotomy 1 incision
• 4 claw toes 4 incisions
• IP fusion hallux ( + Jones) 1 incision
• Total 15 incisions

5 %
• Pressure reduction
• Long peroneal and tib.post
• (compensatory??) varus
• Coleman block test
• Deformity is predictive but also predictable!

References
1. Abate M, Schiavone C, Pelotti P, Salini V. Limited joint mobility in diabetes and ageing: recent advances in pathogenesis and therapy. Int J Immunopathol Pharmacol. 2010 Oct-Dec;23(4):997-1003.
2. Allet et al. Gait characteristics of diabetic patients: a systematic review. Diabetes Metab Res Rev. 2008 Mar-Apr;24(3):173-91.
3. Andersen H, Gadeberg PC, Brock B, Jakobsen J. Muscular atrophy in diabetic neuropathy: a stereological magnetic resonance imaging study. Diabetologia. 1997 Sep;40(9):1062-9.
4. Andersen, Nielsen, Mogensen & Jakobsen. Muscle Strength in Type 2 Diabetes Diabetes. June 2004 vol. 53 no. 6 1543-1548
5. Andreassen CS, Jakobsen J, Ringgaard S, Ejskjaer N, Andersen H. Accelerated atrophy of lower leg and foot muscles: a follow-up study of long-term diabetic polyneuropathy using magnetic resonance imaging (MRI). Diabetologia. 2009 Jun;52(6):1182-91.
6. Bus SA, Yang QX, Wang JH, Smith MB, Wunderlich R, Cavanagh PR. Intrinsic muscle atrophy and toe deformity in the diabetic neuropathic foot: a magnetic resonance imaging study. Diabetes Care. 2002 Aug;25(8):1444-50.
7. Bus SA, Maas M, Cavanagh PR, Michels RP, Levi M. Plantar fat-pad displacement in neuropathic diabetic patients with toe deformity: a magnetic resonance imaging study. Diabetes Care. 2004 Oct;27(10):2376-81.
8. Bus SA, Maas M, de Lange A, Michels RP, Levi M. Elevated plantar pressures in neuropathic diabetic patients with claw/hammer toe deformity. J Biomech. 2005 Sep;38(9):1918-25.
9. Bus SA, Maas M, Michels RP, Levi M. Role of intrinsic muscle atrophy in the etiology of claw toe deformity in diabetic neuropathy may not be as straightforward as widely believed. Diabetes Care. 2009 Jun;32(6):1063-7.
10. Cavanagh et al. Problems with gait and posture in neuropathic patients with insulin-dependent diabetes mellitus. Diabet Med. 1992 Jun;9(5):469-74.
11. Glasoe et al. Dorsal mobility and first ray stiffness in patients with diabetes mellitus. Foot Ankle Int. 2004 Aug;25(8):550-5.
12. Hsu et al. Diabetic effects on microchambers and macrochambers tissue properties in human heel pads Clinical Biomechanics 24 (8) October 2009, Pages 682-686
13. Liu MW, Hsu WC, Lu TW, Chen HL, Liu HC. Patients with type II diabetes mellitus display reduced toe-obstacle clearance with altered gait patterns during obstacle-crossing. Gait Posture. 2010 Jan;31(1):93-9.
14. Pageon H. Reaction of glycation and human skin: The effects on the skin and its components, reconstructed skin as a model Pathologie Biologie Volume 58, Issue 3, June 2010, 226-23
15. Pai S, Ledoux WR. The compressive mechanical properties of diabetic and non-diabetic plantar soft tissue. J Biomech. 2010 Jun 18;43(9):1754-60.
16. Reihsner et al. Alterations of biochemical and two-dimensional biomechanical properties of human skin in diabetes mellitus as compared to effects of in vitro non-enzymatic glycation. Clinical Biomechanics 15 (2000) 379-386
17. Smit AJ, Gerrits EG. Skin autofluorescence as a measure of advanced glycation endproduct deposition: a novel risk marker in chronic kidney disease. Curr Opin Nephrol Hypertens. 2010 Nov;19(6):527-33.
18. Turner DE, Helliwell PS, Burton AK, Woodburn J. The relationship between passive range of motion and range of motion during gait and plantar pressure measurements. Diabet Med. 2007 Nov;24(11):1240-6.