Diabetic Foot 2006
77
VASCULAR SURGERY VASCULAR SURGERY DIVISION OF DEPARTMENT OF SURGERY DIVISION OF DEPARTMENT OF SURGERY
Transcript of Diabetic Foot 2006

VASCULAR SURGERYVASCULAR SURGERYDIVISION OF DEPARTMENT OF SURGERYDIVISION OF DEPARTMENT OF SURGERY

PERIPHERAL VASCULAR DISEASESPERIPHERAL VASCULAR DISEASES
Complication Of Diabetes MellitusComplication Of Diabetes MellitusDIABETIC FOOT DIABETIC FOOT

The ProblemsThe Problems The rising incidence and prevalence of DMThe rising incidence and prevalence of DM
an even greater increase in prevalence an even greater increase in prevalence complicationscomplications
foot ulceration is one of the most foot ulceration is one of the most common ( common ( ± 20% )± 20% )
Despite advances in management Despite advances in management foot foot problems continue to be the most common problems continue to be the most common reason for hospitalizationreason for hospitalization

Diabetes MellitusDiabetes Mellitus the single strongest risk factor for limb lossthe single strongest risk factor for limb loss ± 40 x for leg amputation at normal (trauma)± 40 x for leg amputation at normal (trauma) 50% will undergo a second leg amputation 50% will undergo a second leg amputation within 5 yearswithin 5 years
Annual health care cost (exceeds 1 billion Annual health care cost (exceeds 1 billion dollars) dollars)
NutrientsNutrients RehabilitationsRehabilitations

Months 2001 2002 2003 2004
January 1 3 4 3
February 0 1 4 0
March 3 3 6 7
April 0 0 5 8
May 0 1 1 2
June 0 1 3 5
July 1 1 1 2
Augusts 0 5 1 2
September 2 3 1 5
October 1 4 4 3
November 0 4 4 1
December 1 1 3 5
Total / year 9 27 37 43
Total 116
Amputated Diabetes Mellitus Patient during 2001 – 2004 in Amputated Diabetes Mellitus Patient during 2001 – 2004 in Cipto Mangunkusumo Hospital - JakartaCipto Mangunkusumo Hospital - Jakarta

Amputated Trauma Patient during 2001 – 2004 in Amputated Trauma Patient during 2001 – 2004 in Cipto Mangunkusumo Hospital - JakartaCipto Mangunkusumo Hospital - Jakarta
Months 2001 2002 2003 2004
January 0 1 0 2
February 2 0 2 2
March 1 1 1 3
April 1 2 1 3
May 0 0 1 3
June 0 2 0 6
July 0 0 0 1
Augusts 0 1 2 0
September 0 0 3 2
October 2 0 5 2
November 0 0 1 0
December 0 0 6 3
Total / year 6 7 22 27
Total 62

• Diabetes Mellitus Patient• 116/178 patient x 100 % = 65 %
• Traumatic Patient • 62/178 Patient x 100 % = 35 %

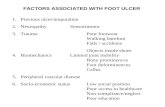
Ischemia (vascular systems)Ischemia (vascular systems) NeuropathyNeuropathy InfectionsInfections
tissue ulcerationtissue ulceration
necrosisnecrosis
gangrenegangrene
The pathogenic mechanismsThe pathogenic mechanisms

Two distinct types of vascular disease are :Two distinct types of vascular disease are : microvascular (microcirculatory)microvascular (microcirculatory)
RetinopathyRetinopathyNephropathyNephropathyNeuropathyNeuropathy
MacroangiopathyMacroangiopathy coronary arterialcoronary arterialperipheral arterialperipheral arterial carotid arterialcarotid arterial
IschemiaIschemia

MacroangiopathyMacroangiopathy
Peripheral arterialPeripheral arterial
- - the non diabetic patient is pattern and the non diabetic patient is pattern and locations of the occlusive / locations of the occlusive /
atherosclerosis above popliteal atherosclerosis above popliteal segmentsegment
- - the diabetic patient the diabetic patient below popliteal below popliteal (intragemiculate)(intragemiculate)


PatophysiologyPatophysiology : :
NeuropathyNeuropathy The pathogeneses of diabetic neuropathy The pathogeneses of diabetic neuropathy
is not fully understood, possible is not fully understood, possible explanations for the development these explanations for the development these disorders (on theories) disorders (on theories)
changed in nerve supplying blood vessel changed in nerve supplying blood vessel (vasa nervorum) or abnormalities in (vasa nervorum) or abnormalities in metabolism metabolism

- Peripheral neuropathy : 60% of all patientsPeripheral neuropathy : 60% of all patients
as focal, diffuse as focal, diffuse
include both the autonomic neuropathy include both the autonomic neuropathy chronic sensory motor polyneuropathieschronic sensory motor polyneuropathies
foot ulcerationfoot ulceration
- Sensoryneuropathy : Sensoryneuropathy :
the distal lower extremities, centrally and the distal lower extremities, centrally and tends to be symmetricaltends to be symmetrical

Sensory nerve fiber loss of the protective Sensory nerve fiber loss of the protective sensation of pain motor nerve fiber losssensation of pain motor nerve fiber loss
small muscle atrophy in the footsmall muscle atrophy in the foot
flexion of the metatarsalflexion of the metatarsal
prominence of the metatarsal headprominence of the metatarsal head
clawing of the toesclawing of the toes in turn results in the development of abnormal in turn results in the development of abnormal
pressure pointpressure point lack protective sensations culminating In lack protective sensations culminating In
ulcerationulceration

Loss of intrinsic muscle function (motor Loss of intrinsic muscle function (motor neuropathy)neuropathy)
- Digit contractures- Digit contractures- Hammer toe- Hammer toe- clawed toe- clawed toe- pes cavus- pes cavus
UlcerationUlcerationCan also involve the ankle joint (equinus Can also involve the ankle joint (equinus
deformity)deformity)



2. Autonomic denervation leads to loss of 2. Autonomic denervation leads to loss of sympathetic tone and increase AV sympathetic tone and increase AV shuntingshunting
nutrient flownutrient flow
impaired regulations of the sweat impaired regulations of the sweat glands (anhidrosis and cracking of dry glands (anhidrosis and cracking of dry skin)skin)
predisposition to skin breakdown and predisposition to skin breakdown and ulcerationulceration

(sympathetic innervation) (sympathetic innervation)
osteoarthropathy associatedosteoarthropathy associated
Charcot’s foot (sensorymotor and Charcot’s foot (sensorymotor and autonomic neuropathies)autonomic neuropathies)

- Diabetic foot infection may result from :Diabetic foot infection may result from :
- a simple puncture wound- a simple puncture wound
- a neuropathic ulcer- a neuropathic ulcer
- the nail plate- the nail plate
- from the interdigital web space- from the interdigital web space

Infections :Infections :
- Most infections progress within the plantar Most infections progress within the plantar aspect of the foot consisting of three aspect of the foot consisting of three compartments :compartments :
- MedialMedial
- central central
- laterallateral

The intrinsic muscle of each digit The intrinsic muscle of each digit the the respective plantar compartment respective plantar compartment may may progress to a plantar abscess ( impairing progress to a plantar abscess ( impairing capillary blood flow ) capillary blood flow ) tissue ischemic-necrosis tissue ischemic-necrosis
To bacterial spread form one compartment to To bacterial spread form one compartment to another through direct perforation of the medial another through direct perforation of the medial or lateral intermuscular septumor lateral intermuscular septum

How to manage Diabetic Foot ?How to manage Diabetic Foot ?


The HistoryThe History
Directed to previous foot and limb Directed to previous foot and limb problemsproblems
1.1. Infection Infection as to the potential for healing as to the potential for healing2.2. NeuropathyNeuropathy3.3. Arterial occlusive disease Arterial occlusive disease arterial arterial
insufficiencyinsufficiency To need for treatment ?To need for treatment ?

Physical examinationPhysical examination
General :General : - vital sign- vital sign- eye :- eye : - visual- visual
- retinopathy- retinopathy The status of the vascular (should be The status of the vascular (should be
contralateral to the examination)contralateral to the examination) Upper-lower extremityUpper-lower extremity
pulse examinationspulse examinations signs of ischemiasigns of ischemia

Inspection :
-Skin : hair, pale
-Muscle : disused atrophy

PALPATION :PALPATION :
* warm / cold* warm / cold
* pulse : + / - * pulse : + / - weakweak
* capillary refill test* capillary refill test

Vascular form :Vascular form :PalpationPalpation

The carotid artery

Auscultation of the carotid arteries

The subclavian artery

The axillary artery

The femoral pulse

The popliteal pulse

The dorsalis pedis pulse

The posterior tibial pulse

ANKLE BRACHIAL INDEX (ABI)
The Ratio of the ankle systolic pressure to the brachial systolic pressure
Indication : all disorders of the lower extremities
Procedures :






ABI valueABI value
▪ ▪ ≥ ≥ 1 1 : : normalnormal
▪ ▪ < 1 – 0,7 < 1 – 0,7 : intermittent claudication: intermittent claudication
▪ ▪ < 0,3 < 0,3 : rest pain : rest pain stenosis stenosis

Neuropathy : - sensation Neuropathy : - sensation vibration vibration
pin-prickpin-prick
thermalthermal
- loss at the ankle reflex- loss at the ankle reflex
- dry and cracked - dry and cracked (autonomic) (autonomic)
- paresthesia- paresthesia

Laboratorium examinationLaboratorium examination
Basic blood test :Basic blood test : - hemoglobin- hemoglobin- leucocyte- leucocyte- thrombocyte - thrombocyte (APTT, thrombocyte (APTT, thrombocyte aggregation) aggregation)- blood sugar- blood sugar
Liver function : albumin, globulin ratioLiver function : albumin, globulin ratio Renal function : ureum, creatinineRenal function : ureum, creatinine

Non Invasive (arterial) evaluationNon Invasive (arterial) evaluation
Ankle Brachial Index (ABI)Ankle Brachial Index (ABI) Radiographic :Radiographic : - calcified vessels- calcified vessels
- bone deforrmity (charcot’s)- bone deforrmity (charcot’s)- osteomyelitis- osteomyelitis
PlethysmographPlethysmograph USG DopplerUSG Doppler Laser fluxemetre Laser fluxemetre
regional transcutaneus oximetry (TcPO2)regional transcutaneus oximetry (TcPO2)


CT Scan multiple slices angiographyCT Scan multiple slices angiography





ArteriographyArteriography

Digital Substraction AngiographyDigital Substraction Angiography

The assessment of infections The assessment of infections (treatment plan should consider the(treatment plan should consider the following)following) : :
- Choice of antibiotic (microbiology)Choice of antibiotic (microbiology)- The need for drainage (incisions)The need for drainage (incisions)- The need for “debridement”The need for “debridement”- RevascularizationsRevascularizations- Medical conditionsMedical conditions- The need for amputationsThe need for amputations

Limb threatening infections require urgent:Limb threatening infections require urgent:
- hospitalizations- hospitalizations
- bed rest- bed rest
- surgical debridement- surgical debridement
- broad spectrum antibiotics- broad spectrum antibiotics

The treatment of ischemia in the diabetic The treatment of ischemia in the diabetic foot is aimed at restoring maximal foot is aimed at restoring maximal perfusions to the foot perfusions to the foot ideally a palpable ideally a palpable foot pulsefoot pulse
Approaches include :Approaches include :by pass grafting (autogenous-prosthetic by pass grafting (autogenous-prosthetic
graft) graft)endovascular (angioplasty-stunting)endovascular (angioplasty-stunting)combinationscombinations


Non Surgical :Non Surgical :
Medical :Medical :
- anti DM- anti DM
- anti coagulant- anti coagulant
- antibiotic- antibiotic

Surgical :Surgical :
• Incision :Incision :
- drainage- drainage - simple- simple - multiple- multiple

Necrotomy – DebridementNecrotomy – Debridement

Vascular ReconstructionVascular Reconstruction

The choice of dressing remains controversial due to The choice of dressing remains controversial due to the lack of large well-controlled comparative studiesthe lack of large well-controlled comparative studies- slough is resent - slough is resent disloughing agents (saline disloughing agents (saline moisturized gauze as a standard treatment)moisturized gauze as a standard treatment)- clean - clean hydrocolloid dressing hydrocolloid dressing- silver containing dressing (antibacterial)- silver containing dressing (antibacterial)- becaplermin (platelet derived growth factor)- becaplermin (platelet derived growth factor)- living dermal (neonal fobroblast)- living dermal (neonal fobroblast)- graft skin- graft skin

EDUCATION :EDUCATION : DietDiet
Exercise (Obesity)Exercise (Obesity)

The FootThe Foot
Hygiene of the footHygiene of the foot The entire foot :The entire foot :
Web spacesWeb spacesNail bedsNail bedsInterdigital “kissing” ulcerInterdigital “kissing” ulcerCallusCallus
Search for infections :Search for infections : - cellulitis- cellulitis
- ulcers- ulcers

- Smoking- Smoking
- Hypertension- Hypertension
- Hyperlipidemia- Hyperlipidemia
- Family history- Family history
Risk factors areRisk factors are


▪▪ Ascending infectionAscending infection - Incision (wide)- Incision (wide) - Amputation- Amputation
T/Supportive/AlternativeT/Supportive/Alternative - Hyperbaric- Hyperbaric - Ozone (oxygen therapy) - Ozone (oxygen therapy)
Emergency caseEmergency case

ConclusionConclusion
1. 1. The management of the diabetic foot The management of the diabetic foot is is challenging and requires a challenging and requires a multidisciplinary approachmultidisciplinary approach
2. 2. Identification of high risk patients Identification of high risk patients requires screening (regular)requires screening (regular)
3. 3. Patient education should be part of Patient education should be part of this this processprocess
4. 4. Once ulceration Once ulceration aggressive aggressive management management