First: Notes to the ECRN Changes have/are taking place this fall Advocate Condell became a Level I...
112
First: Notes to the ECRN Changes have/are taking place this fall Advocate Condell became a Level I trauma center eff October 1, 2009 Grayslake Emergency Center will begin to take BLS ambulance patients effective November 1, 2009 This is the Lake Forest Hospital facility in Grayslake All nurses need to be advised of these changes
-
Upload
ilene-gray -
Category
Documents
-
view
216 -
download
1
Transcript of First: Notes to the ECRN Changes have/are taking place this fall Advocate Condell became a Level I...

First: Notes to the ECRN
Changes have/are taking place this fall Advocate Condell became a Level I
trauma center eff October 1, 2009 Grayslake Emergency Center will begin
to take BLS ambulance patients effective November 1, 2009
This is the Lake Forest Hospital facility in Grayslake
All nurses need to be advised of these changes

Condell as Level I Trauma Center
Condell ECRN will be receiving calls from farther out departments
Region IX and Region X (Lake County’s Region) have similar criteria for Category I trauma
If a department or helicopter service is calling Condell, they have already decided we are the best destination for the patient Take report, get an ETA, activate the
Trauma Alert

Category I Trauma Patient
Any unstable patient and those meeting criteria as a Category I level trauma must be transported to the highest level Trauma Center within 25 minutes
Patients may be by-passing facilities to get to a higher level trauma center

Notes to the ECRN
Grayslake Emergency Center Formerly referred to as the Lake Forest
Acute Care Center Just west of the intersection of Routes
45 and 120 EMS may transport non-emergent
patients being treated with BLS procedures
Will NOT transport patients with IV, cardiac monitors, in labor, and others with anticipation of the need for admission

Notes to the ECRN Grayslake Emergency Center transport
EMS to call their respective Resource Hospital
Condell is the Resource Hospital for:CountrysideGrayslakeLake Forest FireLibertyvilleMundeleinRound Lake WaucondaMurphy

Note to the ECRN
EMS will alert Grayslake Emergency Center to monitor 400
Resource Hospital will take report on 400 and give orders, if needed, including approval for the transport destination requested
Report does not need to be called to the Grayslake Emergency Center Grayslake Emergency Center will be
monitoring the call

Notes to ECRN If EMS was unable to contact
Grayslake Emergency Center, they will advise the Resource Hospital
At that point in time, can determine who will call Grayslake Emergency Center with report The Resource Hospital will forward
report OR EMS will repeat the report
Just be clear who is forwarding report so it does get done

Note to the ECRN
Your function is as a liaison between the field personnel and the ED
Always think, “what is best for the patient?”
Obtain and record report received Ask for clarification, if necessary Obtain ETA

ECRN Responsibilities EMS has an SOP to follow EMS may still be calling Medical Control
for guidance (not all inclusive list) Minors with no parents available Emancipated minor
The girl under 18 that is pregnant is emancipated and after delivery, if she remains a parent, she remains emancipated
The person with alcohol on board Questionable release situations Psychiatric calls

Radio Etiquette Listen attentively Fill in the radio log as completely as possible Ask pertinent questions
Do you really need to know which leg is injured?
Respect field limitations Limited manpower Limited space to work in Driver needs to be focused on driving and is
not being used to communicate on the radio
This policy is now being followed by most departments

The ECRN and Medical Control
The ECRN can only give orders from the SOP’s
If orders above and beyond the SOP’s are necessary, the ED MD must order them
Before leaving the radio to ask the MD for orders, tell EMS to “stand-by” EMS may think you are not copying
their transmission if you do not acknowledge them

Clarifications for Specific Calls Blood glucose levels
EMS is required to obtain glucose levels in the following populations:
Known diabetic with diabetic related problem
Not appropriate for the hospital to order a glucose level just because the patient is a diabetic
Unconscious unknown reasons Any altered level of consciousness
Not all patients require a blood glucose level

Clarifications for Specific Calls
IV access Is it really necessary in the field? Consider the less than ideal environment
in the field for invasive maneuvers Indications IO access
Shock, arrest, or impending arrest Unconscious/unresponsive to verbal
stimuli 2 unsuccessful IV attempts or 90 second
duration

The Patient with Dyspnea
ECRN CE Packet Module II 2009Site Code: 107200-E-1209
Prepared by: Lt. William Hoover, Wauconda FireReviewed/revised by: Sharon Hopkins, RN, BSN, EMT-P

Objectives
Upon successful completion of this module, the ECRN will be able to:
Identify the anatomy and physiology of the respiratory system including
The upper airway The lower airway
Identify clues which will assist in determining the severity of a patient’s respiratory distress.
Identify the components of the assessment of patients with dyspnea.

Objectives
Identify history and physical assessment to be obtained for patients with dyspnea.
Initial assessment SAMPLE history OPQRST Physical Assessment Auscultation of Lung Sounds 12 Lead EKG

Objectives Identify abnormal respiratory
patterns and adventitious breath sounds.
Cheyne-Stokes Kussmaul’s Agonal respirations Crackles Wheezes Rhonchi Snoring

Objectives
Identify the main causes of dyspnea: Upper airway obstruction Respiratory disease processes Cardiovascular diseases Neuromuscular diseases Other causes Psychogenic hyperventilation

Objectives
Identify treatment options for the main causes of dyspnea
Upper airway obstruction Respiratory disease processes Cardiovascular diseases Neuromuscular diseases Other causes Psychogenic hyperventilation
Identify complications of different treatments and procedures associated with dyspnea

Objectives
Identify the following medications and their EMS field use for patients with dyspnea
Albuterol Benadryl Benzocaine Epinephrine 1:1000 Lasix Versed
List assessment post intubation in both the adult and pediatric populations
Identify components of the regular Albuterol kit and EMS in-line procedure

Anatomy & Physiology of Upper Airway
Assists in heating, purifying, & moistening inhaled airNasal cavityOral cavityTongueUvulaEpiglottis – protects trachea
during swallowingVocal cords

Anatomy and Physiology Lower Airway
Trachea Right and left mainstem bronchi Bronchial tree Lungs Lobes Alveoli – the functional unit of the
respiratory system where gas exchange occurs

Upper Airway
Larynx joinsupper andlower airways

Lower Airway
Alveoli arethe functionalunits of therespiratorysystem and iswhere gasexchange takesplace

Difference With the Pediatric Airway
Fundamentally the same as an adult Size and positioning differences
Jaw smaller, tongue relatively larger
Epiglottis floppier and rounderLarynx more superior and anterior
(higher and more forward) in children

Pediatric Considerations
Anatomical differences between adults & children dictate the following: Oral airways slid in without turning
them – tongues are larger than adults Preferable to use straight blade due to
floppy pediatric tongue Before age 10, cricoid cartilage is the
narrowest part of the airway ETT are uncuffed

Determining the Severity of Respiratory Distress
Posture: Sitting up, leaning on arms (Tripod)
Unable to speak in complete sentences without pausing to catch breath
Breathlessness when at rest Imminent respiratory failure or arrest
indicated by bradycardia, bradypnea, agonal respirations or apnea

Tripod position – helps lungs expand

Pediatric Respiratory Distress
Patient exhibits increased work of breathing and the patient is using all resources to compensate for self Child alert, irritable, anxious, restless Increased respiratory effort Use of accessory muscles
Intercostal retractionsSeesaw respirations (abdominal
breathing)Strained neck muscles

Pediatric Respiratory Failure
Energy reserves exhausted Patient cannot maintain adequate
oxygenation and ventilation (breathing)Sleepy, less than alertIntermittently combative or agitatedBradycardic heart rate indicates
hypoxiaImmediate attention to airway and
ventilation rate to fix the bradycardia

Assessing Patients with Dyspnea
Primary Assessment (ABC’s) SAMPLE history OPQRST Physical Assessment Lung Sounds Minimally cardiac monitor; possibly 12
Lead EKG Pulse oximetry
Acceptable normal 95 – 99% Mild hypoxia 91 – 94% Severe hypoxia <91%

All Those Initials!!! ABC’s
Airway, breathing, circulation SAMPLE history
Signs and symptoms, allergies, meds, pertinent past history, last oral intake of fluids or solids, events leading to the incident
OPQRST of assessment Onset – what was pt doing at the time;
provocation/palliation; quality; radiation; severity on 0 – 10 scale; time of onset

Abnormal Respiratory Patterns Cheyne-Stokes
Indicates brainstem injury Progressively deeper, faster breathing
alternating with shallow, slower breathing
Kussmaul’s Commonly found in diabetic
ketoacidosis and can be seen in Aspirin (acetylsalicylic acid) overdose
Deep, slow, or rapid & gasping

Abnormal Patterns cont’d
Agonal Indicates brain anoxiaShallow, slow, or infrequent
breathing

Auscultating Lung Sounds Warm your stethoscope, have the
patient cough to clear their airway and then you’re ready to auscultate
The patient should take deep but easy breaths breathing in and out through their mouth

Auscultating Anterior Lung Sounds

Auscultating Posterior Lung Sounds Start at the top and
move your stethoscope from the right to the left comparing the sides as you walk your stethoscope methodically downward
Sounds are heard better when auscultated in the posterior fields directly over the skin

Abnormal Lung Sounds Crackles (rales)
Fine, bubbling sound heard on inspiration; indicates fluid in smaller airways
Wheezes Musical, squeaking, whistling sound heard
usually on inspiration & expiration; indicates bronchial constriction
Rhonchi Coarse, rattling noise on inspiration,
indicates inflammation, mucous, or fluid in bronchioles
Snoring Indicates partial upper airway obstruction

The patient with dyspnea:Causes Signs and SymptomsEMS Field Treatment Options

Upper Airway Obstruction Foreign body
Airway blocked; food most common culprit Infections – causes airway swelling
Croup – viral infection Epiglottitis – bacterial infection
Anaphylaxis – severe reaction to allergen Sudden onset after exposure (eating or injection
common) Laryngospasm – closure of glottic opening
May be triggered by infection or irritants Blood thinners (Coumadin, Plavix)
Spontaneous hematomas in soft tissue of neck

Foreign Body Obstruction
Esophageal foreign bodies can also present an airway challenge especially if the foreign body moves
Toe ring

Signs & Symptoms of Impaired Airway
Foreign body (FB) Sensation of a FB after eating
(food is the #1 cause of airway obstruction)
Stridor or wheezing respirations Infection (epiglottitis, croup)
Gradual onset Pain on swallowing, drooling Difficulty opening mouth Fever, cough, seal bark cough

Treatment Airway Obstruction Foreign body
Remove the object If patient can cough on own or rescuer needs to
apply the Heimlich or abdominal thrusts (back slaps and chest thrusts for infants)
May need to use blade and handle and retrieve object while using the magill forceps
Secure the airway if unable to relieve the blockage (Quick Trach)
Infections – Croup or epiglottits Prehospital supportive care Supplemental oxygen 6 ml normal saline in nebulizer kit Albuterol if patient is wheezing with croup

Signs & Symptoms of Impaired Airway Related to Anaphylaxis
Anaphylaxis Hives Rash that itches Wheezing Hypotension – unique to anaphylaxis Nausea Abdominal cramps Inability to urinate
Is quickly life-threatening

EMS Adult Anaphylaxis SOP
Anaphylaxis – patient unstable Altered mental status & B/P <100 systolic Support airway; intubate as necessary IV wide open (1000 ml normal saline) Epi: 1:1000 IM 0.5 mg Benadryl 50 mg IVP slowly over 2 min or IM If wheezing, Albuterol 2.5mg/3ml
May repeat If worsening, medical control contacted
Medical Control may order Epi 1:10,000 IV/IO

EMS Pediatric Anaphylaxis SOP
Anaphylaxis – patient unstable Altered mental status Epi 1:1000 IM 0.01 mg/kg (max 0.3 mg or 0.3 ml per
dose) May repeat every 15 minutes Benadryl 1mg/kg slow IVP; max 50 mg IV fluid challenge 20ml/kg
May repeat as needed to max of 60 ml/kg Albuterol 2.5mg/3ml
May repeat Albuterol treatment If worsening, medical control contacted
To consider Epinephrine 1:10,000 at 0.01 mg/kg IV/IO

Respiratory Diseases - Asthma
Bronchoconstriction Stimulants cause inflammatory
response Stimulants can include:
Allergens Weather changes Exercise Respiratory infections Foods/medications

Signs & Symptoms of Asthma
Cough Wheezes
Heard first at the end of exhalation Absent breath sounds = deadly implications Shortness of breath Chest tightness (not to be confused with chest
pain) Use of accessory muscles in severe cases Ask if the patient has ever needed intubation
These patients tend to deteriorate faster and need careful and close monitoring

EMS Asthma SOP
Attempt pulse oximetry reading before administration of oxygen
Assess & record VS, breath sounds, pulse oximetry before/during/after treatment
Oxygen by most appropriate route Albuterol 2.5 mg/3ml (O2 flow at 6 L)
Severe cases, treat while transporting

EMS Treatment of Severe Asthma
Patients with inadequate ventilations or oxygenation are at risk of not being able to continue to ventilate themselves and will need intubation
In-line Albuterol therapy provided to deliver medications to the lungs Albuterol can be delivered via BVM in-line
while preparing to intubate the patient Once intubation is accomplished, continue
to deliver Albuterol via the in-line method

Respiratory Diseases - COPD
Blanket term for diseases that impede the functioning of the lungs
Chronic Bronchitis Increased mucous production in the
bronchial tree Decreased gas exchange in the alveoli Irreversible airway obstruction
Emphysema Destruction of alveolar walls Loss of capacity for lungs to recoil Irreversible airway obstruction

COPD
Most COPD patients have elements of both chronic bronchitis and emphysema
Abnormal ventilation is a common feature Often the cilia lining the respiratory tract are
destroyed Common findings
Bronchospasm Some elements are reversible, some not
Inflammation of respiratory passages Air trapping distal to the obstruction
Desensitization to a chronic state of hypoxia Patients susceptible to repeat respiratory
infection

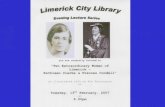
COPD vs. Healthy Lungs

Signs & Symptoms of COPD Chronic bronchitis
Chronic productive cough Tend to be obese with low blood oxygen levels
(referred to as blue bloaters) Wheezing, crackles, or rhonchi can all be
auscultated Rising carbon dioxide blood levels
Emphysema Typically thinner build with barrel chests Hyperventilating to maintain blood oxygen levels Color usually good (referred to as “pink puffers”) Lungs sounds seem very distant Use pursed lip breathing when exhaling

EMS Treatment of COPD with Wheezing
Albuterol treatment2.5 mg / 3 mlO2 flow rate at 6 l/min
Need to generate a mist to inhale and absorb the medication
May repeat albuterol as needed EMS may contact Medical Control to
obtain an order for CPAP in the symptomatic patient

Respiratory Diseases - Pneumonia Infection of lower respiratory tract Primarily a ventilation problem Can be bacterial or non-bacterial
Mycoplasma Chlamydia Viral Tuberculosis
Fluid and inflammatory cells collect in the alveoli
5th leading overall cause of death in the USA

Pneumonia

Signs & Symptoms of Pneumonia
Patients generally appearing ill and feel ill Shaking chills Fever Generalized weakness with gradual onset Pleuritic chest pain Shortness of breath with tachypnea Tachycardia Productive cough – yellow to brown
sputum Crackles in involved lung segment
May also hear wheezes and rhonchi

EMS Treatment of Pneumonia
Supportive care Supplemental oxygen Patient usually dehydrated and fluid
therapy is supportive Need to be accurate on diagnosis
Pneumonia needs fluid therapy CHF/Pulmonary edema needs fluid
restriction CPAP may help patient in severe cases

Aspiration – A Deadly Complication

Protection Against Aspiration
- Positioning – patient on their side if not contraindicated
- Suctioning turned on and ready to be used
- Cricoid pressure used during intubation attempts
- Intubate the patient that is unable to protect their own airway

Respiratory Disorders
Pneumothorax Abnormal collection of air in the pleural
space Spontaneous or traumatic
Pulmonary embolism Arterial blockage to pulmonary circulation Venous clots Embolism can also be from fat, bone
marrow, tumor fragments, amniotic fluid, or air bubbles
Toxic inhalation

Pneumothorax

Signs & Symptoms of Spontaneous Pneumothorax
Sudden sharp, pleuritic chest pain or shoulder pain
May occur after coughing Diminished lung sounds
May be difficult to distinguish in smaller sized lung collapse (<20%)
Young individuals with tall, thin body types are most susceptible
Tachypnea Diaphoresis Possible subcutaneous emphysema

EMS Treatment of Spontaneous Pneumothorax
Majority of spontaneous pneumothorax are not detected in the field – breath sounds not appreciated to be diminished
Care is supportive O2 via NRB mask Assist patient in sitting upright Monitor for change to tension
pneumothorax Tension pneumothorax needs needle
decompression

Pulmonary Embolism – Blood Flow Blocked

Signs and Symptoms of Pulmonary Embolism
Symptoms can be non-specific and vary depending on the site and size of obstruction
Sudden onset severe & unexplained dyspnea
Pleuritic chest pain may be present Cough, usually non-productive but
occasionally blood tinged Tachycardia & tachypnea In severe cases, confusion, hypoxia,
cyanosis, hypotension, death

EMS Treatment of Pulmonary Embolism
Supportive care Rapid transport High flow oxygen; possible
intubation Rapidly fatal once patient arrests Hospital treatment may include
anticoagulation or surgery to remove clot

Cardiovascular Diseases
CHF with acute pulmonary edema
Impaired pumping ability of the heart
Acute Myocardial Infarction Death of heart muscle

Signs & Symptoms of CHF/Acute Pulmonary Edema
Dyspnea at rest Unable to lie flat Crackles in lungs – heard initially in the bases Dependent edema – pedal edema in the
mobile patient JVD especially in the upright position Acute MI (AMI)
Dyspnea may be the initial symptom At times difficult to determine which came
first – AMI affecting function of the heart or hypoxia leading to AMI

CHF with Pulmonary Edema

EMS SOP Stable Pulmonary Edema B/P >100 mmHg
All therapies cause vasodilation and may drop the B/P – monitor B/P carefully
Nitroglycerin 0.4 mg SL (max 3 doses) Consider CPAP Lasix 40 mg IVP (80 mg if on Lasix at
home) Morphine 2 mg slow IVP; may repeat
every 2 minutes to max of 10 mg) If wheezing, Medical Control contacted
for Albuterol order

EMS Interventions For Pulmonary Edema
Nitroglycerin Used for its venodilation effects to pool blood away
from the heart CPAP
Prevents collapse of the alveoli; also lowers B/P Lasix –
Diuretic effect will take approximately 20 minutes but venodilation effect evident in the field to pool blood
Morphine Reduces anxiety level Also a venodilator and will pool blood away from the
heart

EMS SOP For Cardiac Complaints
At minimum consider EKG monitoring EMS to consider early 12 Lead EKG
Take 12 lead as soon as possible STEMI – ST elevation in 2 or more
contiguous leads (I, aVL, V5, V6; II, III, aVF; V1 – V6)
Cardiac Alert ED contacted early to decrease door to
balloon time Transmit 12 lead EKG to hospital
Abnormal rhythms treated

Neuromuscular Diseases
Muscular dystrophy Wasting disease of the muscles
Amyotrophic lateral sclerosis (ALS) Lou Gehrig’s disease Muscular dystrophy caused by
degeneration of motor neurons of the spinal cord
Guillain-Barre syndrome Myasthenia gravis

Guillain-Barre Syndrome

Signs & Symptoms of Neuromuscular Diseases
Amyotrophic Lateral Sclerosis (ALS) Chronic progressive wasting of muscles Difficulty swallowing and speaking Mental functions remain lucid
Guillian-Barre syndrome Weakness starting distally (hands/feet) moving
upward - “ascending” paralysis ending in temporary paralysis
Sensory loss or decreased reflexes Myasthenia Gravis
Weakness that improves with rest, worsens with activity
Crisis level can affect respiratory muscles

Treatment of Neuromuscular Disorders
Conscious sedation intubation if necessary If lung muscles do not work, we have to do
it for them Supportive care
May have to assist patient with BVM In chronic cases, these patients fatigue
easily These patients are prone to chronic
infection

Other Causes of Dyspnea
Anemia Inadequate hemoglobin in the
blood Unable to supply body’s oxygen
demands Hyperthyroid disease – increased
rate of metabolism Metabolic acidosis Psychogenic hyperventilation
Psychological causes

Treatment of Hyperventilation
Determine treatment based on situation Could be deadly to assume these
patients are hyperventilating and a “psych” patient
Do not have people “blow into a bag” Inappropriate to place an O2 mask on
patient and not connect it to oxygen!!! Use verbal counseling on patient to slow
their breathing down if possible

Additional EMS Field Treatment Options

Procedure for Adult Intubation Patient must be pre-oxygenated (100% O2) Equipment checked
Blade and handleStraight blade preferred for pediatric
patients due to floppy epiglottis and large sized tongue
Light is bright and tight ET tube and one back-up tube Stylet – adult or pediatric Syringe for adult ET tube cuff inflation Mechanism to secure tube in place (ie: tape,
commercial tube holder device)

Confirming ET Tube Placement
Max of 30 seconds for intubation attempt time Immediately after intubation, remove the style
to prevent delay in initiating ventilations As ventilations are begun, perform 5 point
auscultation Auscultate 1st over the epigastrium Then auscultate 4 points over the lungs
Observe bilateral rise & fall of the chest Ventilate 1 breath every 6 – 8 seconds
Inflate the adult cuff until no air leak heard Observe yellow coloring on ETCO2 device

Procedure for Pediatric Intubation
Steps nearly identical to the adult Straight blade preferable due to floppy
epiglottis and large sized tongue The pediatric ET tube up to and including
size 6 is uncuffedThe pediatric patient somewhat has
their own cuff effect anatomically due to the natural narrowing of the airway at the cricoid cartilage
Always watch for gentle chest rise and fall to dictate the amount of volume to use with the BVM

Respiratory Rates
BVM support to patient with a heart beat – rescue breathing Adults ventilate once every 5 - 6 sec Infant & child ventilate once every 3 - 5
seconds Once patient intubated, all patients
are ventilated once every 6 – 8 seconds

EMS SOP Conscious Sedation Intubation
Indications Failure to maintain adequate airway or for
risk of aspiration Actual or impending respiratory failure GCS <8 due to head injury Inability to ventilate/oxygenate patient
after insertion of airway and/or BVM Anticipated deterioration

EMS SOP Conscious Sedation Intubation
Contraindication Age less than 16
Need permission from Medical Control B/P < 100mmHg Known hypersensitivity or allergy to the
medication Consider risk vs benefit if the patient is
pregnant

EMS SOP Conscious Sedation Medications
Lidocaine 1.5 mg/kg IVP one time only If head injury/insult, used prophylactically to
decrease risk of cough reflex Coughing raises intrathoracic pressures which will
increase intracranial pressures Versed 5 mg IVP – relaxes/sedates patient
2 mg repeated every minute to relax and sedate patient (1 mg every 5 minutes post procedure to maintain sedation)
Total dose used is 15 mg including post-procedure Versed does not take away any painful stimulus

EMS SOP Conscious Sedation Medications
Morphine 2 mg IVP slow over 2 minutes – relaxes pt Repeated every 3 minutes to a max of
10 mg Benzocaine spray – eliminates gag reflex
Limited to 1-2 short sprays to posterior pharynx
Can stroke the eyelashes to determine presence of a gag reflex
The blink reflex disappears at the same time as the gag reflex

In-line Albuterol Kit
Albuterol can be delivered via BVM or through ET tube to be delivered into lungs
Kit prepared as usual but mouthpiece taken off
BVM placed where mouthpiece was Adaptor added to distal end of corrugated
tube in preparation to connect the adaptor to ET tube
Need to confirm ET tube placement in the usual manner
Can start to bag patient delivering Albuterol prior to ET tube placement

In-line Albuterol Kit
Mouthpiece taken off and replaced with BVM
Adaptor added to end of blue corrugated tubing and attached to mask (or ET tube)
Can begin to ventilate patient before intubation

CPAP Device for Pulmonary Edema
Oxygen started via non-rebreather mask while equipment being set up
Medications are administered simultaneously with CPAP
Medications used and CPAP can all cause a drop in blood pressure; monitor B/P carefully
CPAP will give time fort he medications to take effect
ED will usually call respiratory therapy when expecting a patient on CPAP Resp therapy to set up equipment for patient

CPAP Device
In under 5 minutes patients will feel better
Patients need psychological support to get over the suffocating feeling from the tight fitting mask

Advanced Airway Alternative - Combitube
Indications Arrested patient, unresponsive medical or
trauma patient with no gag reflex and ET tube placement cannot be achieved
Contraindications Age less than 16
This tube is a one size fits all so limited use in pediatric patients and short adults (less than 5 feet)
Gag reflex presentKnown esophageal disorder/caustic
ingestion

Combitube
Patient hyperventilated prior to insertion Equipment checked and prepared and
distal tip lubricated Device is inserted mid-line and to depth
of printed ring level with teeth Pharyngeal cuff inflated with 100 ml of air Distal cuff inflated with 15 ml of air

Combitube
Placement shown is in the esophagus
Proximal and distal balloons both get inflated

Combitube cont’d
Ventilations begin via tube #1 Placement confirmed
Observe gentle rise and fall of the chest wall Perform 5 point auscultation over the
epigastrium and bilaterally over the lungs If unable to confirm tube placement,
then attach BVM to tube #2 and ventilate Repeat confirmation steps
Secure device

Combitube in the ED
If patient arrives with combitube in place Use this advanced airway device until
adequate staffing and competence to change to an ETT
When ready to intubate the patient with ETT, deflate the combitube cuffs
Cuff balloons are marked with amount of air
Blue cuff balloon – 100 mlWhite cuff balloon – 15 ml

Case Scenario Review
Read the cases Treatment is based on the EMS
SOP’s Determine what your response
would be on the radio call Check your own answers with the
power point slides

Case Scenario #1
911 was called to the scene for a 72 year-old obese male with complaints of increased shortness of breath today and with fever
VS: B/P 152/94; P – 104; R – 26; SpO2 92%
Meds: Ventolin, Prednisone, Glucophage, Verapamil, Isordil, Hydrochlorathiazide
Observation: Patient’s color is dusky, slightly diaphoretic, cannot talk in complete sentences, productive cough

Case Scenario #1
What else needs to be done during the assessment phase?
History – is this problem old or new? What are the lung sounds? EKG monitor – possibly obtain a 12 lead
based on assessment findings Sputum is dark brown

Case Scenario #1 Patient found to have exacerbation of signs
and symptoms of COPD with wheezing; possibly a secondary lung infection
EMS Field treatment: Oxygen starting at 2-6 L/minute per nasal
cannula IV TKO – for access if necessary
Carefully monitor flow rate not to over hydrate Albuterol 2.5 mg/3ml attached to O2 at 6L flow
Reassess frequently watching for deterioration and hoping for improvement

Case Scenario #2
EMS arrived at the scene of a local fast food chain for a 3 year-old choking victim
Upon EMS arrival they noted a conscious patient who appears exhausted and is clutching at their throat, color is pale, and they had a weak cough
As EMS approached, the child looks at them with wide eyes and is trying to cough but was no longer making any sound
What is your assessment & what action plan should be started?

Case Scenario #2
Impression – partially obstructed airway that is now a completely obstructed airway If the patient can speak or cough, you are
to allow them to try to relieve the obstruction with coughing
In a conscious child, you perform the Heimlich maneuver (abdominal thrusts) until the patient is unconscious or the obstruction is relieved
Equipment to prepare and have on stand-by Intubation equipmentChild BVMMagill forceps

Case Scenario #2
If the patient has a history of asthma and is wheezing, short of breath, and has an increased respiratory rate, how do you tell the difference between an asthma attack and an obstructed airway?
Don’t let patient history steer you wrong
Assess the patient Asthma – bilateral wheezing, usually
identifiable trigger evident FB – wheezing on obstructed side, patient
usually eating or child playing with small objects at onset of incident

Case Scenario #3
EMS is called to the scene of 32 year-old female having an asthma attack
The episode started approximately 3 hours ago and the patient has used her inhaler with no success
Appearance: Anxious, pale, dry oral mucous membranes (mouth), unable to talk in complete sentences, appears exhausted, using accessory muscles
What is your impression? What else should be assessed? What treatment by EMS is appropriate?

Case Scenario #3
Initial impression – acute asthma attack Assessment to obtain
Lung sounds, pulse oximetry List of medications Verification of allergies EKG monitor to check rhythm
Treatment Set up the Albuterol kit Need to coach patient in her ear to talk her
through slowing down her breathing, then taking deeper breaths, and finally holding the deeper breath to get the medication into the lungs

Case Scenario #3
The patient is so exhausted, their level of consciousness is deteriorating and SpO2 is falling
EMS will prepare for in-line Albuterol administration and intubation
Upon ED arrival, continue administration of Albuterol until the dose is completedThe chamber will be empty of liquid

Case Scenario #4
911 was called to the scene for a 68 year-old male with sudden onset of difficulty breathing
Patient is sitting upright on a chair, leaning forward resting their arms on their thighs (tripod position)
Appearance Rapid respirations with noisy ventilations Cyanotic finger tips and pale, diaphoretic face Using accessory muscles
Your impression? Further assessment? EMS intervention?

Case Scenario #4 Further assessment to be obtained
History Allergies & medications Lung sounds
Bilateral crackles and wheezing Vital signs and SpO2 reading
B/P 180/110; P – 110; R- 32; SpO2 89% EKG monitor and 12 lead EKG
Atrial fibrillation; no ST elevation Impression
Acute pulmonary edema

Case Scenario #4
EMS interventions Is patient stable or unstable?
Stable – B/P 180/110 Medications to be given:
Nitroglycerin 0.4 mg slVasodilator
Lasix 40 mg IVP (80 mg if used at home)Morphine 2 mg IVP If wheezing, Albuterol needs to be requested
from Medical Control Device
CPAP – keep alveoli open

Bibliography
Campbell, J. Basic Trauma Life Support, 5th Edition, Brady. 2004
Dalton, Limmer, Mistovich, Werman. Advance Medical Life Support, 3rd Edition. Brady. 2007.
Region X Standard Operating Procedures, March 2007 Amended version May 1, 2008
Conscious Sedation (Page 7) Acute Pulmonary Edema (Page 19) Airway Obstruction (Page 22) Adult Allergic reaction/Anaphylactic Shock (Page 23) Asthma/COPD (Page 25) Pediatric Respiratory Failure (Page 53) Pediatric Acute Asthma (Page 55) Pediatric Airway Obstruction (Page 56) Croup/Epiglottitis (Page 64) Pediatric Allergic Reaction/Anaphylaxis (Page 70)
www.WebMD.com