FIREFISH: Safety, survival and ... - Roche Medically Home
2
Presented at the 2nd International Scientific & Clinical Congress on SMA, Evry Genocentre, Paris, France 5th–7th February 2020 Acknowledgments We would like to thank the infants and their families for participation in this study, as well as the investigators and trial staff involved in the FIREFISH study. We would also like to thank our collaborators at PTC Therapeutics and the SMA Foundation. The study was funded by F. Hoffmann-La Roche AG, Basel, Switzerland. Writing and editorial assistance was provided by Lindsey Weedon, of MediTech Media, UK, in accordance with Good Publication Practice (GPP3) guidelines (http://www.ismpp.org/gpp3). Abbreviations AE, adverse event; BiPAP , bilevel positive airway pressure; CHOP-INTEND, Children’s Hospital of Philadelphia Infant Test of Neuromuscular Disorders; ECG, electrocardiogram; HINE-2, Hammersmith Infant Neurological Examination Module 2; IQR, interquartile range; PD, pharmacodynamics; PK, pharmacokinetics; SAE, serious adverse event; SMA, spinal muscular atrophy; SMN, survival of motor neuron. References 1. Mercuri E, et al. Lancet Neurol. 2012; 11:443–452; 2. Lefebvre S, et al. Cell. 1995; 80:155–165; 3. Lorson CL, et al. PNAS. 1999; 96:6307–631; 4. De Sanctis R, et al. Neuromuscul Disord. 2016; 26:754–759; 5. Finkel R, et al. Neurology. 2014; 83:810–818; 6. Hamilton G and Gillingwater TH. Trends Mol Med. 2013; 19:40–50; 7. Poirier A, et al. Pharmacol Res Perspect. 2018; 6:e00447; 8. Clinicaltrials.gov: NCT02913482 (Accessed January 2020). FIREFISH: Safety, survival and motor function in infants with Type 1 spinal muscular atrophy (SMA) receiving risdiplam (RG7916) R Masson, 1 G Baranello, 1,2 B Darras, 3 JW Day, 4 N Deconinck, 5,6 A Klein, 7,8 M Mazurkiewicz-Bełdzińska, 9 E Mercuri, 10 K Rose, 11 H Xiong, 12 D Vlodavets, 13 E Zanoteli, 14 M El-Khairi, 15 S Fuerst-Recktenwald, 16 M Gerber, 17 K Gorni, 18 H Kletzl, 17 RS Scalco, 16 L Servais 19,20 on behalf of the FIREFISH Study Group 1 Fondazione IRCCS Istituto Neurologico Besta, Developmental Neurology Unit, Milan, Italy; 2 The Dubowitz Neuromuscular Centre, UCL Great Ormond Street Institute of Child Health, London, UK; 3 Boston Children’s Hospital, Harvard Medical School, Boston, MA, USA; 4 Department of Neurology, Stanford University, Palo Alto, CA, USA; 5 Neuromuscular Reference Center, UZ Gent, Ghent, Belgium; 6 Queen Fabiola Children’s University Hospital, ULB, Brussels, Belgium; 7 University Children’s Hospital Basel, Basel, Switzerland; 8 Inselspital, Bern, Switzerland; 9 Department of Developmental Neurology Medical University of Gdańsk, Gdańsk, Poland; 10 Paediatric Neurology and Nemo Center, Catholic University and Policlinico Gemelli, Rome, Italy; 11 Paediatric Gait Analysis Service of New South Wales, The Children’s Hospital at Westmead Sydney, Australia; 12 Department of Pediatrics, Peking University First Hospital, Beijing, China; 13 Russian Children Neuromuscular Center, Veltischev Clinical Pediatric Research Institute of Pirogov Russian National Research Medical University, Moscow, Russia; 14 Hospital das Clinicas, São Paulo, Brazil; 15 Roche Products Ltd, Welwyn Garden City, UK; 16 Pharma Development Neurology, F. Hoffmann-La Roche Ltd, Basel, Switzerland; 17 Pharma Development, Safety, F. Hoffmann-La Roche Ltd, Basel, Switzerland; 18 PDMA Neuroscience and Rare Disease, F. Hoffmann-La Roche Ltd, Basel, Switzerland; 19 Reference Center for Neuromuscular Disease, Centre Hospitalier Régional de La Citadelle, Liège, Belgium; 20 MDUK Neuromuscular Centre, Department of Paediatrics, University of Oxford, UK. Background • Spinal muscular atrophy (SMA) is caused by reduced levels of the survival of motor neuron (SMN) protein due to deletions and/or mutations of the SMN1 gene. 1,2 — A second SMN gene, SMN2, produces low levels of functional SMN protein, but is unable to compensate for the loss of SMN1. 3 • Untreated infants with Type 1 SMA fail to achieve major developmental milestones such as rolling over, or sitting independently, 4 and typically die or require permanent ventilation before 2 years of age (median [IQR] age at death or permanent ventilation is 13.5 [8.1–22.0] months). 5 • Increasing preclinical evidence indicates that SMA is a multisystem disease. 6 — Therapies that increase SMN protein levels systemically may have broader therapeutic benefit than those targeting motor neurons alone. • Risdiplam (RG7916) is a centrally and peripherally distributed oral SMN2 pre-mRNA splicing modifier that increases the levels of functional SMN protein. 7 • FIREFISH (NCT02913482) is an open-label, multicenter clinical study assessing the safety, tolerability, PK, PD and efficacy of risdiplam in infants with Type 1 SMA. 8 — Part 1: Dose-finding period followed by open-label extension. — Part 2: Efficacy and safety at the dose selected in Part 1. • Open-label risdiplam treatment for 24 months. CHOP-INTEND HINE-2 Safety 82% (14/17) of Cohort B (high dose) had a CHOP-INTEND score ≥40 after receiving risdiplam for 16 months After 16 months of treatment, 12% (2/17) of infants from Cohort B (high dose) achieved bouncing, the first milestone on the HINE-2 walking assessment No infant has required tracheostomy or reached permanent ventilation 86% (18/21) of all infants were event free* after receiving risdiplam for 16 months FIREFISH Part 2 is underway and will further assess the efficacy and safety of risdiplam Denotes an infant from Cohort B who was uncooperative during CHOP-INTEND assessment Denotes the age at which infants from Cohort A were switched to the high dose Treatment cohort Cohort A: Low dose Cohort B: High dose Median change from baseline in CHOP-INTEND score at Month 16 Cohort A (n=3) Cohort B (n=14) All infants (n=17) 9.0 20.5 19.0 CHOP-INTEND total score: Individual infant plots showed continuous improvement from baseline after receiving treatment with risdiplam for 16 months Each line represents an individual infant. Intent-to-treat infants from FIREFISH Part 1 (N=21). Cohort A: Low-dose cohort. Cohort B: Dose adjusted per protocol. The three surviving infants from Cohort A were subsequently dose adjusted at ages 24.4, 20.6, and 20.8 months, respectively for each infant. A score of 0 was given for missed items in the CHOP-INTEND assessment. Data cut-off: 02 July 2019. CHOP-INTEND score Maximum score Age (Months) 6 12 18 24 30 36 0 0 10 20 30 40 50 60 64 * * Motor milestones achieved in infants treated with risdiplam for 16 months, as assessed by HINE-2 Each circle represents an individual infant. Cohort A: Low-dose cohort. Cohort B: Dose adjusted per protocol. Intent-to-treat infants from FIREFISH Part 1 (N=21); ‘cannot test’ results are not included. Between baseline and Month 12, two infants died; one from Cohort A and one from Cohort B. One infant in Cohort B died between Month 12 and Month 16 and one infant discontinued from treatment after Month 16, but did not perform the HINE-2 at Month 16. Data cut-off: 02 July 2019. Cohort B (high dose) Indicates the highest motor milestone achieved by infants at Month 16 Cohort A (low dose) Bouncing Cruising Walking independently Walking Baseline (N=21) Month 12 (n=19) Month 16 (n=17) Does not support weight Supports weight Stand with support Stands unaided Standing At the data cut-off (02 July 2019): - 48% (10/21) of infants were able to maintain upright head control - 10% (2/21) of infants were able to roll from supine to prone - 33% (7/21) of infants were sitting independently - 5% (1/21) of infants were able to stand supporting their weight - 10% (2/21) of infants were able to bounce. Baseline (N=21) Month 12 (n=19) Month 16 (n=17) HINE-2 motor milestones HINE-2 motor milestones Unable to maintain upright Wobbles Maintain upright Head control Baseline (N=21) Month 12 (n=19) Month 16 (n=17) No rolling Roll to side Prone to supine Supine to prone Rolling Baseline (N=21) Month 12 (n=19) Month 16 (n=17) Cannot sit Sits with support at hips Props Stable sit Sitting Baseline (N=21) Month 12 (n=19) Month 16 (n=17) Data cut-off: 02 July 2019. *Reported in ≥20% of infants; † Fatal events were reported in four infants: (1) Viral respiratory tract infection in female infant aged 7 months at enrollment. First symptoms started on Day 5 with fatal event on study Day 21. The event was complicated by bilateral atelectasis. (2) Fatal cardiac arrest and respiratory failure on study Day 236 in female infant aged 7 months at enrollment on concurrent night ventilation (BiPAP for less than 16 hours per day) in the context of suspected aspiration; (3) Respiratory tract infection with onset on study Day 386 in female infant aged 5 months and 3 weeks at enrollment. In the absence of fever and due to moderate symptomatology (nasal congestion and labored breathing) which seemed to improve the infant was not hospitalized and died 1 day after onset of respiratory tract infection; (4) Cardiac arrest and hypoxia in the context of pneumonia in a male infant, aged 3 months and 3 weeks at enrollment, who discontinued treatment with risdiplam on Day 585 due to parental request and experienced the fatal event approximately 3.5 months after discontinuing treatment. • 235 AEs were reported in 21 infants. • The most common SAEs were pneumonia (reported in 4 infants) and respiratory tract infection, respiratory tract infection (viral), acute respiratory failure and respiratory distress (each reported in 2 infants). • Three infants died during the trial. One additional infant died 3.5 months after discontinuing treatment with risdiplam. † • Preclinical safety findings were not observed in any infant: - ophthalmologic monitoring has not shown any evidence in humans of the retinal findings seen in preclinical monkey studies - hematological parameters have remained stable over time and no drug-induced skin findings have been observed. • No adverse trends have been reported after a review of all available safety laboratory results, vital signs and ECG data. Infants with at least one AE, n (%) Infants with at least one SAE, n (%) Most common AEs,* number of infants (%) Pyrexia Upper respiratory tract infection Diarrhea Vomiting Cough Infants with a grade 3–5 AE, n (%) Discontinuations due to drug-related AEs, n Total (N = 21) 21 (100) 12 (57) 12 (57) 10 (48) 6 (29) 6 (29) 5 (24) 9 (43) 0 Please scan using your QR reader application to access the graphs and data presented in this poster. NB: there may be associated costs for downloading data. These costs may be high if you are using your smartphone abroad. Please check your mobile data tariff or contact your service provider for more details. Alternatively this can be accessed at: https://bit.ly/39KkSnY *Event free in FIREFISH is defined as alive with no permanent ventilation (i.e. no tracheostomy or BiPAP ≥16 hours per day continuously for >3 weeks or continuous intubation >3 weeks, in the absence of, or following the resolution of, an acute reversible event). Data cut-off: 02 July 2019. *Comments related to the same infant. Caregiver comments on infants in FIREFISH Part 1 within the 16-month treatment period. Data cut-off: 02 July 2019. Conclusions “Increased talking, says numbers, colors and single word commands”* “Sits unsupported for one hour at a time. Rolls faster”* “Stand(s) with support and with orthosis at ankle” Caregiver comments on infants in FIREFISH Part 1
Transcript of FIREFISH: Safety, survival and ... - Roche Medically Home

Presented at the 2nd International Scientific & Clinical Congress on SMA, Evry Genocentre, Paris, France 5th–7th February 2020
AcknowledgmentsWe would like to thank the infants and their families for participation in this study, as well as the investigators and trial staff involved in the FIREFISH study. We would also like to thank our collaborators at PTC Therapeutics and the SMA Foundation. The study was funded by F. Hoffmann-La Roche AG, Basel, Switzerland. Writing and editorial assistance was provided by Lindsey Weedon, of MediTech Media, UK, in accordance with Good Publication Practice (GPP3) guidelines (http://www.ismpp.org/gpp3).
AbbreviationsAE, adverse event; BiPAP, bilevel positive airway pressure; CHOP-INTEND, Children’s Hospital of Philadelphia Infant Test of Neuromuscular Disorders; ECG, electrocardiogram; HINE-2, Hammersmith Infant Neurological Examination Module 2; IQR, interquartile range; PD, pharmacodynamics; PK, pharmacokinetics; SAE, serious adverse event; SMA, spinal muscular atrophy; SMN, survival of motor neuron.
References1. Mercuri E, et al. Lancet Neurol. 2012; 11:443–452;2. Lefebvre S, et al. Cell. 1995; 80:155–165;3. Lorson CL, et al. PNAS. 1999; 96:6307–631;4. De Sanctis R, et al. Neuromuscul Disord. 2016; 26:754–759;
5. Finkel R, et al. Neurology. 2014; 83:810–818;6. Hamilton G and Gillingwater TH. Trends Mol Med. 2013; 19:40–50;7. Poirier A, et al. Pharmacol Res Perspect. 2018; 6:e00447;8. Clinicaltrials.gov: NCT02913482 (Accessed January 2020).
FIREFISH: Safety, survival and motor function in infants with Type 1 spinal muscular atrophy (SMA) receiving risdiplam (RG7916)R Masson,1 G Baranello,1,2 B Darras,3 JW Day,4 N Deconinck,5,6 A Klein,7,8 M Mazurkiewicz-Bełdzińska,9 E Mercuri,10 K Rose,11 H Xiong,12 D Vlodavets,13 E Zanoteli,14 M El-Khairi,15 S Fuerst-Recktenwald,16 M Gerber,17 K Gorni,18 H Kletzl,17 RS Scalco,16 L Servais19,20 on behalf of the FIREFISH Study Group1Fondazione IRCCS Istituto Neurologico Besta, Developmental Neurology Unit, Milan, Italy; 2The Dubowitz Neuromuscular Centre, UCL Great Ormond Street Institute of Child Health, London, UK; 3Boston Children’s Hospital, Harvard Medical School, Boston, MA, USA; 4Department of Neurology, Stanford University, Palo Alto, CA, USA; 5Neuromuscular Reference Center, UZ Gent, Ghent, Belgium; 6Queen Fabiola Children’s University Hospital, ULB, Brussels, Belgium; 7University Children’s Hospital Basel, Basel, Switzerland; 8Inselspital, Bern, Switzerland; 9Department of Developmental Neurology Medical University of Gdańsk, Gdańsk, Poland; 10Paediatric Neurology and Nemo Center, Catholic University and Policlinico Gemelli, Rome, Italy; 11Paediatric Gait Analysis Service of New South Wales, The Children’s Hospital at Westmead Sydney, Australia; 12Department of Pediatrics, Peking University First Hospital, Beijing, China; 13Russian Children Neuromuscular Center, Veltischev Clinical Pediatric Research Institute of Pirogov Russian National Research Medical University, Moscow, Russia; 14Hospital das Clinicas, São Paulo, Brazil; 15Roche Products Ltd, Welwyn Garden City, UK; 16Pharma Development Neurology, F. Hoffmann-La Roche Ltd, Basel, Switzerland; 17Pharma Development, Safety, F. Hoffmann-La Roche Ltd, Basel, Switzerland; 18PDMA Neuroscience and Rare Disease, F. Hoffmann-La Roche Ltd, Basel, Switzerland; 19Reference Center for Neuromuscular Disease, Centre Hospitalier Régional de La Citadelle, Liège, Belgium; 20MDUK Neuromuscular Centre, Department of Paediatrics, University of Oxford, UK.
Background• Spinal muscular atrophy (SMA) is caused by reduced levels of the survival of motor neuron (SMN) protein due to deletions and/or
mutations of the SMN1 gene.1,2
— A second SMN gene, SMN2, produces low levels of functional SMN protein, but is unable to compensate for the loss of SMN1.3
• Untreated infants with Type 1 SMA fail to achieve major developmental milestones such as rolling over, or sitting independently,4 and typically die or require permanent ventilation before 2 years of age (median [IQR] age at death or permanent ventilation is 13.5 [8.1–22.0] months).5
• Increasing preclinical evidence indicates that SMA is a multisystem disease.6
— Therapies that increase SMN protein levels systemically may have broader therapeutic benefit than those targeting motor neurons alone.• Risdiplam (RG7916) is a centrally and peripherally distributed oral SMN2 pre-mRNA splicing modifier that increases the levels of functional
SMN protein.7
• FIREFISH (NCT02913482) is an open-label, multicenter clinical study assessing the safety, tolerability, PK, PD and efficacy of risdiplam in infants with Type 1 SMA.8
— Part 1: Dose-finding period followed by open-label extension. — Part 2: Efficacy and safety at the dose selected in Part 1. • Open-label risdiplam treatment for 24 months.
CH
OP-
INTE
ND
HIN
E-2
Safe
ty
82% (14/17) of Cohort B (high dose) had a CHOP-INTEND score ≥40 after receiving
risdiplam for 16 months
After 16 months of treatment,
12% (2/17) of infants from Cohort B
(high dose) achieved bouncing, the first milestone on the HINE-2 walking
assessment
No infant has required
tracheostomy or reached permanent
ventilation
86% (18/21) of all infants were event free* after receiving
risdiplam for 16 months
FIREFISH Part 2 is underway and will further assess the
efficacy and safety of risdiplam
Denotes an infant from Cohort Bwho was uncooperative during CHOP-INTEND assessmentDenotes the age at which infants from Cohort A were switched to the high dose
Treatment cohortCohort A: Low doseCohort B: High dose
Median change from baseline in CHOP-INTEND score at Month 16
Cohort A(n=3)
Cohort B(n=14)
All infants(n=17)
9.0 20.5 19.0
CHOP-INTEND total score: Individual infant plots showed continuous improvement from baseline after receiving treatment with risdiplam for 16 months
Each line represents an individual infant. Intent-to-treat infants from FIREFISH Part 1 (N=21). Cohort A: Low-dose cohort. Cohort B: Dose adjusted per protocol. The three surviving infants from Cohort A were subsequently dose adjusted at ages 24.4, 20.6, and 20.8 months, respectively for each infant. A score of 0 was given for missed items in the CHOP-INTEND assessment.Data cut-off: 02 July 2019.
CH
OP
-IN
TEN
D s
core
Maximum score
Age (Months)6 12 18 24 30 360
0
10
20
30
40
50
6064
*
*
Motor milestones achieved in infants treated with risdiplam for 16 months, as assessed by HINE-2
Each circle represents an individual infant. Cohort A: Low-dose cohort. Cohort B: Dose adjusted per protocol. Intent-to-treat infants from FIREFISH Part 1 (N=21); ‘cannot test’ results are not included. Between baseline and Month 12, two infants died; one from Cohort A and one from Cohort B. One infant in Cohort B died between Month 12 and Month 16 and one infant discontinued from treatment after Month 16, but did not perform the HINE-2 at Month 16. Data cut-off: 02 July 2019.
Cohort B (high dose) Indicates the highest motor milestone achieved by infants at Month 16Cohort A (low dose)
Bouncing Cruising Walking independently
Walking Baseline (N=21)
Month 12 (n=19)
Month 16 (n=17)
Does not support weight Supports weight Stand with support Stands unaided
Standing
At the data cut-off (02 July 2019):- 48% (10/21) of infants were able to maintain upright head control- 10% (2/21) of infants were able to roll from supine to prone - 33% (7/21) of infants were sitting independently - 5% (1/21) of infants were able to stand supporting their weight- 10% (2/21) of infants were able to bounce.
Baseline (N=21)
Month 12 (n=19)
Month 16 (n=17)
HINE-2 motor milestones HINE-2 motor milestones
Unable to maintain upright Wobbles Maintain upright
Head control
Baseline (N=21)
Month 12 (n=19)
Month 16 (n=17)
No rolling Roll to side Prone to supine Supine to prone
Rolling Baseline (N=21)
Month 12 (n=19)
Month 16 (n=17)
Cannot sit Sits with support at hips Props Stable sit
Sitting Baseline (N=21)
Month 12 (n=19)
Month 16 (n=17)
Data cut-off: 02 July 2019. *Reported in ≥20% of infants; †Fatal events were reported in four infants: (1) Viral respiratory tract infection in female infant aged 7 months at enrollment. First symptoms started on Day 5 with fatal event on study Day 21. The event was complicated by bilateral atelectasis. (2) Fatal cardiac arrest and respiratory failure on study Day 236 in female infant aged 7 months at enrollment on concurrent night ventilation (BiPAP for less than 16 hours per day) in the context of suspected aspiration; (3) Respiratory tract infection with onset on study Day 386 in female infant aged 5 months and 3 weeks at enrollment. In the absence of fever and due to moderate symptomatology (nasal congestion and labored breathing) which seemed to improve the infant was not hospitalized and died 1 day after onset of respiratory tract infection; (4) Cardiac arrest and hypoxia in the context of pneumonia in a male infant, aged 3 months and 3 weeks at enrollment, who discontinued treatment with risdiplam on Day 585 due to parental request and experienced the fatal event approximately 3.5 months after discontinuing treatment.
• 235 AEs were reported in 21 infants.
• The most common SAEs were pneumonia (reported in 4 infants) and respiratory tract infection, respiratory tract infection (viral), acute respiratory failure and respiratory distress (each reported in 2 infants).
• Three infants died during the trial. One additional infant died 3.5 months after discontinuing treatment with risdiplam.†
• Preclinical safety findings were not observed in any infant:
- ophthalmologic monitoring has not shown any evidence in humans of the retinal findings seen in preclinical monkey studies
- hematological parameters have remained stable over time and no drug-induced skin findings have been observed.
• No adverse trends have been reported after a review of all available safety laboratory results, vital signs and ECG data.
Infants with at least one AE, n (%)
Infants with at least one SAE, n (%)
Most common AEs,*number of infants (%)
Pyrexia
Upper respiratory tract infection
Diarrhea
Vomiting
Cough
Infants with a grade 3–5 AE, n (%)
Discontinuations due to drug-related AEs, n
Total(N = 21)
21 (100)
12 (57)
12 (57)
10 (48)
6 (29)
6 (29)
5 (24)
9 (43)
0
Please scan using your QR reader application to access the graphs and data presented in this poster. NB: there may be associated costs for downloading data. These costs may be high if you are using your smartphone abroad. Please check your mobile data tariff or contact your service provider for more details. Alternatively this can be accessed at: https://bit.ly/39KkSnY
*Event free in FIREFISH is defined as alive with no permanent ventilation (i.e. no tracheostomy or BiPAP ≥16 hours per day continuously for >3 weeks or continuous intubation >3 weeks, in the absence of, or following the resolution of, an acute reversible event). Data cut-off: 02 July 2019.
*Comments related to the same infant. Caregiver comments on infants in FIREFISH Part 1 within the 16-month treatment period. Data cut-off: 02 July 2019.
Conclusions
“Increased talking, says numbers, colors and single
word commands”*“Sits unsupported for one hour
at a time. Rolls faster”*“Stand(s) with support and with
orthosis at ankle”
Caregiver comments on infants in FIREFISH Part 1
AbbreviationsCHOP-INTEND, Children’s Hospital of Philadelphia Infant Test of Neuromuscular Disorders; HINE-2, Hammersmith Infant Neurological Examination Module 2.
Supplementary page(This page provides additional online content and will not be available at the poster stand. Attendees will be able to view and download this page by scanning the QR code on the main poster)
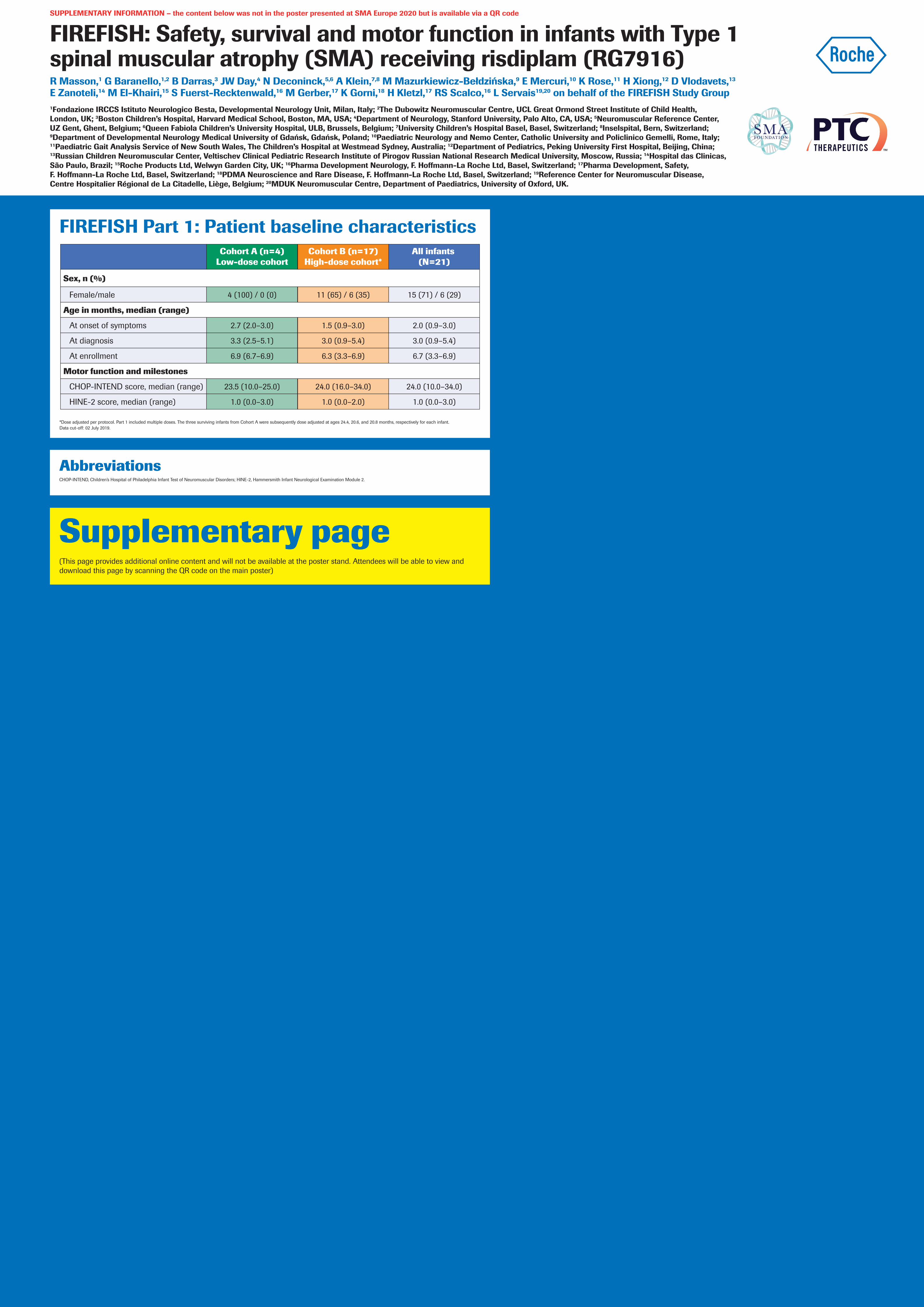
FIREFISH Part 1: Patient baseline characteristics
*Dose adjusted per protocol. Part 1 included multiple doses. The three surviving infants from Cohort A were subsequently dose adjusted at ages 24.4, 20.6, and 20.8 months, respectively for each infant. Data cut-off: 02 July 2019.
Sex, n (%)
Female/male
Age in months, median (range)
At onset of symptoms
At diagnosis
At enrollment
Motor function and milestones
CHOP-INTEND score, median (range)
HINE-2 score, median (range)
Cohort A (n=4)Low-dose cohort
4 (100) / 0 (0)
2.7 (2.0–3.0)
3.3 (2.5–5.1)
6.9 (6.7–6.9)
1.0 (0.0–3.0)
23.5 (10.0–25.0)
Cohort B (n=17)High-dose cohort*
11 (65) / 6 (35)
1.5 (0.9–3.0)
3.0 (0.9–5.4)
6.3 (3.3–6.9)
1.0 (0.0–2.0)
24.0 (16.0–34.0)
All infants (N=21)
15 (71) / 6 (29)
2.0 (0.9–3.0)
3.0 (0.9–5.4)
6.7 (3.3–6.9)
1.0 (0.0–3.0)
24.0 (10.0–34.0)
SUPPLEMENTARY INFORMATION – the content below was not in the poster presented at SMA Europe 2020 but is available via a QR code
FIREFISH: Safety, survival and motor function in infants with Type 1 spinal muscular atrophy (SMA) receiving risdiplam (RG7916)R Masson,1 G Baranello,1,2 B Darras,3 JW Day,4 N Deconinck,5,6 A Klein,7,8 M Mazurkiewicz-Bełdzińska,9 E Mercuri,10 K Rose,11 H Xiong,12 D Vlodavets,13 E Zanoteli,14 M El-Khairi,15 S Fuerst-Recktenwald,16 M Gerber,17 K Gorni,18 H Kletzl,17 RS Scalco,16 L Servais19,20 on behalf of the FIREFISH Study Group1Fondazione IRCCS Istituto Neurologico Besta, Developmental Neurology Unit, Milan, Italy; 2The Dubowitz Neuromuscular Centre, UCL Great Ormond Street Institute of Child Health, London, UK; 3Boston Children’s Hospital, Harvard Medical School, Boston, MA, USA; 4Department of Neurology, Stanford University, Palo Alto, CA, USA; 5Neuromuscular Reference Center, UZ Gent, Ghent, Belgium; 6Queen Fabiola Children’s University Hospital, ULB, Brussels, Belgium; 7University Children’s Hospital Basel, Basel, Switzerland; 8Inselspital, Bern, Switzerland; 9Department of Developmental Neurology Medical University of Gdańsk, Gdańsk, Poland; 10Paediatric Neurology and Nemo Center, Catholic University and Policlinico Gemelli, Rome, Italy; 11Paediatric Gait Analysis Service of New South Wales, The Children’s Hospital at Westmead Sydney, Australia; 12Department of Pediatrics, Peking University First Hospital, Beijing, China; 13Russian Children Neuromuscular Center, Veltischev Clinical Pediatric Research Institute of Pirogov Russian National Research Medical University, Moscow, Russia; 14Hospital das Clinicas, São Paulo, Brazil; 15Roche Products Ltd, Welwyn Garden City, UK; 16Pharma Development Neurology, F. Hoffmann-La Roche Ltd, Basel, Switzerland; 17Pharma Development, Safety, F. Hoffmann-La Roche Ltd, Basel, Switzerland; 18PDMA Neuroscience and Rare Disease, F. Hoffmann-La Roche Ltd, Basel, Switzerland; 19Reference Center for Neuromuscular Disease, Centre Hospitalier Régional de La Citadelle, Liège, Belgium; 20MDUK Neuromuscular Centre, Department of Paediatrics, University of Oxford, UK.