Exeter - eDoctor | Patient Centred Medical Blog by Online .... Neck Resection Full exposure of both...
20
Exeter ™ total hip system Primary V40 ™ Surgical Protocol
Transcript of Exeter - eDoctor | Patient Centred Medical Blog by Online .... Neck Resection Full exposure of both...

Exeter™
total hip system
Primary V40™
Surgical Protocol

2. Neck ResectionFull exposure of both the acetabulum and theproximal femur is necessary to prepare,cement and implant the components. As theExeter™ stem has no collar, the level andorientation of neck resection are not critical.
1. Pre-operative Planning:Pre-operative templating is important to select the correctimplant sizes, their positions and the minimum cementmantle thickness required. Any surgical approach can beused, and where appropriate, it is important that the patientis firmly and accurately supported in the lateral decubitusposition.
6. Femoral PreparationThe femur is prepared by using the tapered reamers,Capener long-handled gouge and the appropriate raspselected during the pre-op templating. It is important toopen the femur laterally in order to achieve neutralalignment of the stem. The rasp creates a cavity which willhold the stem with a complete cement mantle of at least2mm around it. Usually a smaller rasp is used initiallyfinishing with the rasp corresponding to the templateconsidered appropriate for the femur. It is a seriousmistake to over-rasp the canal and remove too muchcancellous bone.
7. Trial ReductionThe appropriate head trial is positioned onto therasp. A trial reduction will verify the correct stemsize, offset and position. A metal spigot protectormay be applied onto the rasp and the stemintroducer attached. A diathermy mark or short Kwire can then be used to indicate the correct lengthaccording to the leg length device.
SURGICAL PROTOCOL HIGHLIGHTSV40™
CementIt is important to note thatdifferent types of bone cementset at various timescales andthe temperature of theoperating theatre also effectsthe setting time.
Acetabular CementingTypically using Simplex®bone cement with a theatretemperature of 21°C, cementinjection and pressurationshould take place 6–8 minutesafter commencement ofmixing.
Femoral CementingTypically using Simplex®bone cement and with atheatre temperature of 21°C,the cement should beinserted into the cavity at21⁄2–3 minutes aftercommencement of mixing.The stem is typically insertedapproximately 6 minutesafter the start of mixing.
1
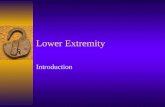
Head diameter�mm222628303236
44mm

3. Acetabular PreparationThe acetabulum is reamed to reveal bleedingsubchondral bone (trabecular bone whereverpossible). After removing any osteophytes,fixation pits are made with multiple drill holes.The sucker-aspirator may be used in the domeof the ilium.Trial cups are inserted to select the cup whichwill give a minimum of 2mm of cement mantle.After lavage, the bone should be dried toprovide a sound key for the cement.
4. Acetabular CementingCement is introduced into the acetabulumand pushed firmly into the fixation pits.The acetabular pressuriser is placed overthe cement and inflated to create a seal. Itis pushed onto the cement to counter thebleeding pressure and to force cement intothe bone. Please see cement panel for typicalsetting times. Typically Simplex® bonecement will be pressurised for 6 to 7minutes before the cup is introduced.
5. Cup InsertionThe acetabular cup is placed on the introducer. The shaft is heldso that the long alignment rod is vertical and the short onehorizontal and perpendicular to the patient’s long axis. Rotatingthe handle of the introducer will place the skirt in the desiredposition.
The cup is implanted about 3 minutes before the cementpolymerises, and is held in place with the cup pusher until thecement is completely set.
8. Plug IntroductionThe correct intramedullary plugsize is selected by using theExeter™ plug trials. Thecorresponding sized plug isimplanted to provide a firm sealfor pressurising the cement. Thefemur is then cleaned with lavageand dried to provide a clean drysurface prior to cement injection.
9. Femoral CementingAfter retrograde filling with cement, the spout of thegun is cut off at the seal, and the seal is then forcedonto the end of the femur to form a closed cavityappropriate for pressurisation.The remainingcement is injected and the pressure maintained untilimmediately prior to stem insertion.
Typically, with Simplex® bone cement and a theatretemperature of 21 degrees centigrade the stem willbe introduced 5 to 6 minutes after commencementof mixing.
10. Stem IntroductionWith the centraliser in place, the stem is inserted in onecontinuous smooth movement down the centre of the femur.During insertion, pressure is maintained by the thumb placedmedially over the area of the calcar. The stem can be insertedthrough the stem seal to its final position, or the seal can bepositioned after the stem is inserted, and held in place until thecement polymerises.

3
1. Pre-operative Planning:
Pre-operative templating is important andwill usually allow the surgeon to select animplant of the appropriate size and offsetfor the hip to be reconstructed, and to planthe positions in which the componentsshould be placed (Fig. 1).
Allowance must be made for the need toobtain a complete mantle of cement forthe femoral component that is to be used.Alongside the stem profiles on thetemplates are marks that demonstrate theextent of cement mantles of varyingwidths. The first mark indicates theminimum mantle allowed. It may benecessary to template the opposite hip.
2. Surgical Exposure
The Exeter™ Hip can be implantedthrough the direct lateral or lateralapproaches or through the Southern orposterior approach. The Southern orposterior approach is featured in thistechnique manual. Whichever approach isused, a full exposure of both theacetabulum and the proximal femur isessential for effective preparation of thebony cavities, cementing, and implantinsertion.
Appropriate soft tissue releases shall beperformed to allow adequate exposure ofthe whole socket rim and mobilisation ofthe proximal femur.
The patient must be firmly and accuratelysupported in the lateral decubitus position(Fig. 2) to help ensure that the acetabularcomponent is orientated correctly. It isalso important not to flex the contralateralhip too much as this could reduce thelumbar lordosis, with subsequent risk ofretroversion of the cup.
S U R G I C A L P R O T O C O L
Figure 1
Figure 2
V40™
Head diameter�mm222628303236
44mm
Alignment points: �Proximal Stem seal
Neck resection level
20% oversize to allow�for X-Ray magnificationGraduated marker�indicating minimum�cement mantle 2mm
The stem centraliser will compress to a minimum of 10mm.�If the femoral canal is less than this the centraliser wings�should be removed.
EXETER“
total hip system
V40“
44mm No.2�0580-1-442

Either the femur or the acetabulum maybe prepared first.
3. Femoral Neck Resection
The level and orientation of neck resectionis not critical as the Exeter™ Hip Stem hasno collar or other features which will affectthe osteotomy line. The level of sectionusually runs from mid-way between theupper margin of the lesser trochanter andthe inferior aspect of the head, to theupper surface of the base of the neck(Fig. 3).
4. Femoral Preparation
The leg is positioned and held with afemoral elevator. A gluteus mediusretractor may be to fully expose theproximal femur (Fig. 4).
Figure 3
Figure 4

5
V40™
The opening in the cut surface of thefemoral neck is developed from within thecalcar toward the proximal aspect of thegreater trochanter as far as necessary toallow the Exeter™ stem to be passeddirectly down the femur in the long axis ofthe medullary canal.
The cavity is opened using the straightCapener type gouge or a box chisel, toundercut the base of the neck, and developthe slot into the trochanteric region(Fig. 5), if necessary using a rongeur toresect the bone of the neck afterundercutting. The taper pin reamer is usedto develop the slot to ensure that thefemoral stem can be inserted down themid-line of the femur.
The taper pin reamer should be positionedwithin the canal so that it aligns with thepopliteal space (Fig. 6), or with the patellaif the lateral approach is being used.
Trabecular bone is removed from withinthe calcar until a strong layer isencountered, usually this will leave2 - 3mm of strong trabecular bone.
This layer of trabecular bone provides afirm foundation for the micro-interlock ofcement within the bone.
Figure 5
Figure 6

A smaller rasp is used initially finishingwith the rasp corresponding to thetemplate considered appropriate for thefemur. It is a serious mistake to over-raspthe canal and remove too much cancellousbone.
If excess force is required to introduce arasp to this level then the canal should befurther developed with the taper pinreamer or gouge, without compromisingthe layer of strong trabecular bone.
Figure 7 - use of rasps
A
C
D
B

7
V40™
5. Acetabular Preparation
The true acetabular lip is identified,osteophytes are removed with anyredundant capsular folds, and thetransverse acetabular ligament is leftintact. The true floor of the socket isidentified.
Grater reamers are used to remove allremnants of articular cartilage and toshape the cavity with exposure of acancellous surface where feasible, excepton the medial wall. The curtain osteophyteis then removed. The cortical layer abovethe teardrop is never removed. The reamershaft should be orientated at 40° ofabduction and 10°-15° of anteversion(Fig. 8).
Care must be taken not to enlarge theantero-posterior diameter of theacetabulum, unduly thinning the anteriorand posterior walls.
A gouge may optionally be used to createfixation pits in the three main bones of thepelvis (Fig. 9A). Multiple drill holes arethen made in the ilium, pubis and ischiumfor fixation (Fig. 9B).
Supplementary 6mm drill holes shouldalso be used where appropriate, especiallyjust within the rim of the acetabulum.
Trial cups are inserted into the preparedacetabulum to confirm or change theselection of cup made on the basis of pre-operative templating. The selected trialcup must be completely surrounded bybone (Fig. 10A).
The pressuriser is tested against theacetabular rim to make certain that aperfect seal is obtained (Fig. 10B).Cancellous autograft chips taken duringthe preparation of the upper femur orduring the preparation of the acetabularpits should be packed under the transverseligament to ensure that the spaceunderneath is totally occluded. Any otherrim deficiencies should be made goodwith impacted cancellous chips, and it isusual to place a layer of cancellous bonechips on the cortical floor of theacetabulum just above the teardrop. Theseare held in place with the outer side of along spoon whilst the acetabulum iscleaned.
Figure 8

6. Acetabular Cementingand Pressurisation
The acetabulum is thoroughly cleanedusing lavage. It is irrigated withHartmann’s solution, and packed withswabs soaked in 10 vols. hydrogenperoxide whilst the Simplex® bone cementis being mixed. These swabs are heldfirmly in place using the cup pusher untilthe cement is ready to use.
A sucker-aspirator may be used to assistcement intrusion and prevent bloodaccumulating at the interface. The cementmass is placed into the socket, and cementis thumbed into the pits. The level ofcement in the acetabulum should beapproximately 5mm below the acetabularrim to ensure a good seal by thepressuriser (Fig. 10C).
Figure 9
Figure 10
A B
A
B
C

9
V40™
The cement is pressurised using theacetabular pressuriser. A piece of gauzeand a latex sheet are placed over thepressuriser balloon. The balloon isinflated, then applied to the socket rimand then pushed with considerable force.
Typically using Simplex® cement, andwith a theatre temperature of 21°C, thecement should be mixed for at least1minute, left to stand for at least 1 minuteand inserted into the cavity atapproximately 3 - 4 minutes.
Pressurisation should continue until theviscosity of the cement has risensufficiently to overcome the bleedingpressure of the bone.
A quantity of cement should be held in thesurgeon’s hands to help ascertain whencement reaches the stage when the cupshould be implanted. Normally this stagewill be reached at 6-8 minutes aftercommencement of mixing.
The pressuriser is removed by deflating theballoon, then breaking the seal by liftingthe gauze swab and peeling back the latexsheet.
Figure 11
Figure 12

7. Acetabular Implantation
The acetabular cup is then implanted. It ispositioned onto the introducer (Fig. 12),and pushed into the acetabulum.Considerable force should be necessary toovercome the viscosity of the cement, butthe cup should not be allowed to bottomout. The initial force applied is medial andthen superiorly.
The cup is correctly positioned when theface of the cup is at an angle of40° of abduction and 10°-15° ofanteversion (Fig. 13). The guide rods onthe introducer will place the cup in thisorientation if they are correctly used andprovided the patient has been accuratelyplaced and stabilised in the lateraldecubitus position (as detailed previouslyin Fig. 2). If the direct lateral or lateralapproach has been used the cup may beplaced in a more neutral position. Duringinsertion the cup should be rotated so thatthe apex of the skirt should lie postero-laterally either at 10 o’clock or 2 o'clockaccording to the side.
The long alignment rod should be vertical,and the short pin horizontal and at 90º tothe patient's long axis. There should be anadequate thickness of cement between thecranial surface of the cup and theacetabular bone of no less than 3 - 4mm.This layer will of course be appreciablythicker in the region of the fixation pits.
Once the cup has been properlypositioned, it is held in place with lightpressure using the universal cup pusher,with the appropriately sized trial femoralhead, so that there is no tendency for thecup to be moved within the cement mantlewhilst the cement is polymerising(Fig. 14). Avoid using a damaged trial headwhich may lock in the cup and cause it tomove.
After cement polymerisation the fixationis checked by rocking the cup andwatching for evidence of ‘pumping’ ofblood at the cement-bone junction.Evidence of this indicates inadequatefixation, and immediate revision shouldbe considered.
Significant osteophytes should be removedto prevent premature impingement of thefemoral component or femur on theacetabular rim at the extremes ofmovement. If during trial reduction theneck of the prosthesis impinges on theskirt then that part of the skirt should beresected.
Figure 14
Figure 13
90°

11
V40™
8. Trial reduction
The proximal femur is re-exposed and theappropriate head trial is positioned ontothe rasp. A trial femoral head is placedover the spigot and the hip is reduced.Head trials are colour coded; blue is for aminus (-) neck length, black for neutraland green for a plus (+) neck length.
Correct restoration of leg length may beassessed by comparing the relativepositions of the femoral condyles.If the leg has been shortened this can becompensated for by implanting the stemto a higher level. Leg lengthening can becompensated by impacting the raspfurther into the femur and repeating thetrial reduction. A smaller rasp may berequired.
When the correct leg length has beenachieved, the trial femoral head is removedand a metal spigot protector is positionedover the neck trial. The stem introducer ismounted onto the metal spigot protectorensuring that it is aligned with the rasp.The femur can be marked with diathermyand methylene blue dye at the levelindicated by the leg length gauge(Fig. 15). Alternatively a K wire may beused. The spigot protector and neck trialsare then removed. The rasp handle isreattached and the rasp removed.
Figure 15
15

The correct intramedullary plug size isselected by using Exeter™ plug trials. Theappropriate size of intramedullary plug ismounted on the introducer (Fig. 16A),and driven in 17-18cm distal to the tip ofthe greater trochanter (Fig. 16B).
A tight fit for the plug is essential.
The proximal femoral seal and backingplate are positioned onto the cement gunnozzle. These are placed over the proximalend of the femur to ensure a good fit(Fig. 17). If a good fit cannot be achieved,the other size of seal should be tried, or thefemoral slot altered to ensure a tight seal. Ifa tight fit cannot be obtained after any ofthese measures, the use of the gun shouldbe abandoned and the ‘suck-down’technique should be used with doughycement and vigorous finger packing.
The canal is thoroughly cleaned usinglavage. A catheter is placed in the distalend of the canal and connected to suction.
Ribbon gauze soaked in 10 vols. hydrogenperoxide is packed into the femur tomaintain haemostasis in the canal and toprovide a clean dry surface into which thecement can key. The ribbon gauze andsuction catheter are removed immediatelybefore cement injection starts.
Figure 16A & B, 17
16B
17
16A
9. Further Femoral Preparation

13
V40™
Figure 18A & B
18A
10. Femoral Cementing
Using Simplex® bone cement, the cementshould be mixed in a mixing bowl for 1minute and then poured into the cementbarrel, which should be left to stand for 30seconds. Three mixes may be necessary forlarge femora. The nozzle is fixed to thebarrel, the femoral seal and backing platepositioned, and the cement gun is primed.
Cement is introduced in a retrograde (ie.from distal to proximal) fashion(Fig. 18A). Typically, using Simplex® bonecement and with a theatre temperature of21°C, this is usually 21⁄2 to 3 minutes aftercommencement of mixing. As the cementreaches the upper part of the canal, thenozzle of the gun is cut off distal to thefemoral seal.
The femoral seal is then impacted forciblyonto the upper end of the femur, and theremaining cement is slowly pumped intothe femur (Fig. 18B). This action willmaintain a steady pressure to overcomethe bleeding pressure inside the femur.
When pressurisation is correctlyperformed, a steady extrusion of fatthrough the walls of the upper femur maybe seen.
Cement injection and pressurisation iscontinued until the viscosity of the cementstarts rising. Typically, using Simplex bonecement and with a theatre temperature of21°C, this is seldom less than 6 minutesfrom commencement of mixing, judgedby a small sample held in the hand. Thefemoral stem is then inserted.
The aim should be to delay stem insertionas long as possible remembering thatduring stem insertion interface pressuresin the canal are directly related to theviscosity of the cement.
18B

11. Stem Implantation
The hollow centraliser must be used withthe Exeter™ stem. Each Exeter™ V40™stem is supplied with a winged and awingless centraliser. If an intramedullaryplug of less than 10mm is used it may bepreferable to use a wingless centraliser.The use of the hollow centraliser prevents‘end-bearing’ of the stem, and ensures thatthe proximal, expanded taper of the stemwill engage properly in the cement mantle.
The selected stem is mounted on theintroducer. It is important to note that thehandle of the introducer is exactly in themid-line of the stem and so the introducerand the stem can be lined up with themedullary canal of the femur. The stemintroducer can be used with one hand, andhas a smooth trigger action which releasesthe introducer pin from the dimple in thelateral shoulder of the stem implant.
The stem is introduced through theproximal femoral opening closer to theposterior femoral cortex than the anterior,and aiming at the middle of the poplitealfossa if the Southern or posteriorapproach is used, or the patella if the directlateral or lateral approach is used(Fig. 19A).
The stem can be driven into the canalthrough the stem seal and its backing platewhich should be held firmly in position onthe cut surface of the femoral neck.
Otherwise the stem is driven into placewith the surgeon’s thumb occluding themedial exit from the upper end of thefemur between the stem and the calcar, tofurther pressurise the cement into thecancellous bone (Fig. 19B). During steminsertion, there should be furtherextrusion of fat through the walls of thefemur.
19A
19B
19C
Figure 19A, B & C

15
V40™
Figure 20A, B, C & D
20A
20B
20C
20D
The insertion should be brisk until thestem reaches a position approximately1cm. above its final position. Insertionthereafter should be slower, graduallybringing the stem to its finalpredetermined position as judged by theleg length gauge (Fig. 19C). The femur canbe marked with diathermy and methyleneblue dye at the level indicated by thegauge.
When the final position has been reachedand the introducer removed, the stem sealand backing plate are positioned and firm
pressure maintained on the top of thecement until it polymerises (Fig. 20A, B &C). Ensure that the stem does not back outduring cement polymerisation. Thesurgeon may wish to use the stem sealpusher to apply firm pressure onto thestem seal until the cement polymerises(Fig. 20D).
The surgeon should remove all cementfrom the cut surface of the cortical calcar.

12. Reduction
The spigot protector is then removed andthe spigot thoroughly cleaned.
A further trial reduction may be carriedout using the appropriate trial heads onthe V40™ spigot. Checks are then madeagain for correct leg length and stability.Reduced and increased neck lengths areavailable. The appropriate size of femoralhead is removed from its packaging andplaced over the stem spigot. It is secured inplace by firm blows with the palm of thehand. Alternatively, the head may bepushed on by hand & rotated 10º. Neitherexcess force, impaction nor hardinstruments should be used as this maydamage the fine polished surface(Fig. 21).
Figure 21A, B and C
21A 21B 21C

17
P O S T- O P E R A T I V E M A N A G E M E N T
DAY OF OPERATION
Encourage breathing exercises. Check thatfoot, ankle and quadriceps exercises arecarried out hourly by the patient.
FIRST POST-OPERATIVEDAY
Supervise breathing and foot, ankle andquadriceps exercises. Begin resistedexercises for the un-operated leg andassisted active exercises for the operatedleg, including external rotation and activehip abduction with the weight of the legbeing taken by the physiotherapist. Thepatient is encouraged to do themovements with assistance from thephysiotherapist. Avoid internal rotation,sitting erect or the use of too manypillows. Younger patients may stand onthe first post-operative day.
SECOND POST-OPERATIVE DAY
Continue with breathing exercises, foot,ankle, quads and gluteal exercises. Removethe drains. The physiotherapist shouldhelp the patient to get out of bed, afterensuring that the bed is at the correctheight. The patient should wear shoes.
Knee flexion is encouraged with thepatient sitting sideways on the edge of thebed. In getting into a standing position thepatient should take as much weight aspossible on the non-operated leg withsupport from the physiotherapist whoshould stand on the same side as theaffected hip with a stick in the patient'sopposite hand or another helper on thatside if necessary.
In the standing position the patientshould be shown how to stand and walk.The patient should be encouraged to takenormal steps, although the first walkshould be kept within the patient'stolerance. Touch weight bearing isadvisable except in the elderly.
The patient must be taught to turn aroundwithout straining the hip in a rotatoryposition, and be taught how to sit andstand correctly from a chair.
The physiotherapist should teach thepatient how to get back into, and out ofbed, and assist them to do so, preventinginternal rotation and adduction of the hipduring these manoeuvres.
THIRD POST-OPERATIVEDAY
All static exercises and breathing exercisesare supervised. The patient may be taughtto turn prone and is encouraged to lieprone for two periods of twenty minutesdaily.
FOURTH POST-OPERATIVE DAY
Continue supervision of static exercisesand breathing exercises. The physio-therapist should continue to supervisecorrect walking and the patient canincrease the number and duration of thewalks. The patient is instructed in gettinginto a sitting position on the toilet. Thephysiotherapist should start to teach thepatient to lift the leg on to the bottom stepof the stairs flexing the hip and knee whilstavoiding internal rotation.
FIFTH POST-OPERATIVEDAY
Continue supervision of static exercises.The patient should be able to walk to thetoilet alone. The physiotherapist shouldstart the patient walking up and downsteps and generally increase walking. Apost-operative X-ray is taken. The patientshould be independent upon dischargeand allowed home with suitable walkingaids supplied by the occupationaltherapist. The patient should avoidexcessive flexing of and internally rotatingthe hip.
V40™

The first post-operative follow-up visit isusually two to three months after surgery.X-rays at this stage are only taken if bonegrafting was performed. If the patient'scondition is satisfactory at three months,the next appointment should be one yearfrom the time of operation. X-rays shouldbe taken. If these are satisfactory, furtherfollow-up visits are not needed, unless thepatient develops symptoms suggesting anyproblem with the arthroplasty. However,arrangements should be made for thearthroplasty to be viewed by X-ray twoyears from the time of the operation.Provided these films are satisfactory, nofurther films need be taken for seven toeight years, unless the patient developssymptoms suggesting problems with thearthroplasty. From eight years on, filmsshould again be taken at two yearlyintervals.

This document is intended solely for the use of healthcare professionals.
The information presented in this brochure is intended to demonstrate the breadth of Stryker productofferings. Always refer to the package insert, product label and/or user instructions before using any Strykerproduct. Products may not be available in all markets. Product availability is subject to the regulatory ormedical practices that govern individual markets. Please contact your Stryker representative if you havequestions about the availability of Stryker products in your area.
Products referenced with ™ designation are trademarks of Stryker.Products referenced with ® designation are registered trademarks of Stryker.
Literature Number: EXEOT01E02MTX/GS 10/06Copyright © 2006 Stryker
1 Presentation, European Hip Society, June 2004.
Excellent Long Term Results
• From the original 433 Exeter Hips, withrevision for aseptic stem loosening as theend-point, survivorship into the 33rdyear of follow-up is 91.46%1.
Stryker SACité-CentreGrand-Rue 901820 MontreuxSwitzerland
t : +41 21 966 12 01f : +41 21 966 12 00
www.europe.stryker.com