Epiglottitis and torsade de pointes tachycardia · Epiglottitis andtorsade depointestachycardia...
4
Br Heartj 1994;72:205-208 CASE REPORT Epiglottitis and torsade de pointes tachycardia Carl-Magnus Pripp, Per Blomstrom Abstract Severe throat infection is not usually associated with a higher risk of paroxys- mal attacks of torsade de pointes tachy- cardia. A patient is reported in whom epiglottitis was associated with the sud- den development of cardiac syncope caused by an acquired adrenergic- dependent long QT syndrome and the development of ventricular arrhythmias. (Br Heart Y 1994;72:205-208) Case report A 70 year old man with a history of essential hypertension was admitted to the emergency ward with fever, dyspnoea, and severe throat pain. He had been treated with propranolol (80 mg daily), polythiazide (1 mg daily), and hydralazine (50 mg three times a day), during which time his electrocardiogram was normal (fig 1). Epiglottitis was diagnosed. In view of his severe respiratory distress, endotracheal intubation was performed and the patient was treated with mechanical ventilation for 10 days. A parapharyngeal abscess developed on aVL VI a ,1 i, III the right side of his neck. Computed tomo- graphy localised the abscess, surrounded by a severe inflammatory reaction, near the carotid artery and the sympathetic nerves on this side (fig 2). On the third day the abscess was drained through an incision along the sterno- cloidomastoid muscle, beneath the omohyoid muscle, and medial to the vessels. A digital dissection towards the abscess was per- formed. The patient was discharged from hospital after four weeks. Seven weeks later he was readmitted because of repeated transient sudden attacks of unconsciousness. During these attacks he had no signs of tonic or clonic movements or faecal or urinary incontinence. After each episode he felt exhausted and found it diffi- cult to get up off the floor. No abnormalities were found on physical examination. Routine laboratory tests were normal with serum digoxin concentration of 1-9 nmol/l. A consultant neurologist found no signs of neurological deficits or neurological disease. Apart from a slightly enlarged heart, the chest x ray showed no other changes. Treatment with digitalis and propranolol was stopped. Department of Cardiology, University Hospital of Lund, S-221 85 Lund C-M Pripp P Blomstrom Correspondence to: Dr Carl-Magnus Pripp, Department of Cardiology, University Hospital of Lund, S-221 85 Lund, Sweden. Is 50mm/s -- 1 s 25 mm/s Figure 1 Electrocardiogram recorded before the epiglottitis developed (paper speed 50 mmis, rhythm strip 25 mmls). 205 on May 14, 2021 by guest. Protected by copyright. http://heart.bmj.com/ Br Heart J: first published as 10.1136/hrt.72.2.205 on 1 August 1994. Downloaded from
Transcript of Epiglottitis and torsade de pointes tachycardia · Epiglottitis andtorsade depointestachycardia...

Br Heartj 1994;72:205-208
CASE REPORT
Epiglottitis and torsade de pointes tachycardia
Carl-Magnus Pripp, Per Blomstrom
AbstractSevere throat infection is not usuallyassociated with a higher risk of paroxys-mal attacks of torsade de pointes tachy-cardia. A patient is reported in whomepiglottitis was associated with the sud-den development of cardiac syncopecaused by an acquired adrenergic-dependent long QT syndrome and thedevelopment ofventricular arrhythmias.
(Br Heart Y 1994;72:205-208)
Case reportA 70 year old man with a history of essentialhypertension was admitted to the emergencyward with fever, dyspnoea, and severe throatpain. He had been treated with propranolol(80 mg daily), polythiazide (1 mg daily), andhydralazine (50 mg three times a day), duringwhich time his electrocardiogram was normal(fig 1). Epiglottitis was diagnosed. In view ofhis severe respiratory distress, endotrachealintubation was performed and the patient wastreated with mechanical ventilation for 10days. A parapharyngeal abscess developed on
aVL VIa ,1 i,
III
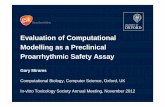
the right side of his neck. Computed tomo-graphy localised the abscess, surrounded by asevere inflammatory reaction, near the carotidartery and the sympathetic nerves on this side(fig 2). On the third day the abscess wasdrained through an incision along the sterno-cloidomastoid muscle, beneath the omohyoidmuscle, and medial to the vessels. A digitaldissection towards the abscess was per-formed. The patient was discharged fromhospital after four weeks.
Seven weeks later he was readmittedbecause of repeated transient sudden attacksof unconsciousness. During these attacks hehad no signs of tonic or clonic movements orfaecal or urinary incontinence. After eachepisode he felt exhausted and found it diffi-cult to get up off the floor.No abnormalities were found on physical
examination. Routine laboratory tests werenormal with serum digoxin concentration of1-9 nmol/l. A consultant neurologist found nosigns of neurological deficits or neurologicaldisease. Apart from a slightly enlarged heart,the chest x ray showed no other changes.Treatment with digitalis and propranolol wasstopped.
Department ofCardiology,University Hospital ofLund, S-221 85 LundC-M PrippP BlomstromCorrespondence to:Dr Carl-Magnus Pripp,Department of Cardiology,University Hospital of Lund,S-221 85 Lund, Sweden.
Is 50mm/s
-- 1 s 25 mm/s
Figure 1 Electrocardiogram recorded before the epiglottitis developed (paper speed 50 mmis, rhythm strip 25 mmls).
205 on M
ay 14, 2021 by guest. Protected by copyright.
http://heart.bmj.com
/B
r Heart J: first published as 10.1136/hrt.72.2.205 on 1 A
ugust 1994. Dow
nloaded from

Pripp, Blomstr6m
Figure 2 Computed tomograminflammatory reaction surround(car), absc, abscess; car, carotic
A resting electrocardiogram showed sinusbradycardia with a ventricular rate of 45 beatsper minute, a normal corrected QT interval(QTc), and a prominent U wave (fig 3).Twenty four hour Holter monitoring showedan unusually stable sinus rhythm with a fre-quency varying between 45-85 beats perminute and single supraventricular and ven-tricular extrasystoles. Furthermore, duringthe daytime there were two episodes of tran-sient ventricular tachycardia (fig 4) when thepatient felt dizzy. The ventricular rates duringthe attacks were 170 beats per minute and200 per minute, and the attacks lasted sevenand nine seconds respectively. The ventricu-lar tachycardias were of the torsade depointes type and were preceded by an episodeof sinus bradycardia and ventricular extra sys-toles (fig 4). An exercise test, up to 95 W,showed no signs of coronary artery disease;
_; ; &.iSi :-L Xatib4i the corrected QT interval was slightly pro-longed (0-47 s) during rest and increased to amaximum of 0-49 s during work. No arrhyth-mias were seen. A cold pressor test showe(no QT prolongation compared with the rest-ing state. Intravenous injection of a bolusdose of isoprenaline (isoproterenol) (2 ug',produced prolongation of QTc from 0-47 s t(o
_ _ ~~~~~~~~~~~~0-50sWe attributed the patient's episodes of
unconsciousness to attacks of torsade depomtes tachycardia caused by an acquiredadrenergic-dependent long QT syndrome,because there was no family history of syn-cope, sudden death or long QT syndrome,nor was the patient taking drugs known to
showing a parapharyngeal abscess (absc, arrow), and the cause torsade de pointes tachycardia. Becauseling it, affecting the vessels at the right side of the neck the attacks of ventricular tachycardia werei artery; dx, right; sin, left. preceded by episodes of sinus bradycardia
aVL VI 7
V2 T U
-aVR V3 I
a:: A V4
V5
III
V6
_______________ is 50 mm/s
25 mm/s i-I Is
Figure 3 Electrocardiogram recorded after an attack of unconciousness showing a normal corrected QT interval but largeT waves (T) and U waves (U) (paper speed 50 mmls, rhythm strip 25 mmIs).
206
on May 14, 2021 by guest. P
rotected by copyright.http://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.72.2.205 on 1 August 1994. D
ownloaded from

Epiglouitis and torsade de pointes tachycardia
Figure 4 Holtermonitoring showingunusualy constant RRintvals and episodes oftorsade de pointestachycardia, preceded byan episode ofsinusbradycardia with singleventncular extrasystoles.
AALAAAIIkAA
A k I~~~1.1A I A A A I
0 10 S
and we wished to treat the adrenergic-dependent long QT syndrome with fl block-ade, the patient was given an atrial demandrate-adaptive (AAI-R) system.Two years later he still had a prolonged
QT interval but he had not had any moreattacks of syncope. Several Holter recordingsdid not show any ventricular arrhythmias.
DiscussionAccording to Jackman et al the long QT syn-drome can be classified into three maingroups: pause-dependent long QT syn-dromes, adrenergic-dependent long QT syn-dromes, and an intermediate group withcharacteristics of both.' The first group is alsocalled acquired long QT syndrome.The tachycardia associated with the pause-
dependent long QT syndrome is usually pre-ceded by a long cycle (which enhances thesubsequent U wave). After the pause there isa normal QRS complex of sinus origin fol-lowed by the first impulse of the torsade depointes tachycardia. This sequence is in turnpreceded by an abnormal impulse, which caneither be the last beat of a ventricular tachy-cardia or a ventricular extra systole. Thus theinitiating cycle is short-long-short.2
Drugs are the most frequent cause ofpause-dependent or acquired long QT syn-dromes.13 Anorexia nervosa, starvation,electrolyte disturbances, and severe brady-arrhythmias are other known causes of pause-dependent or acquired long QT syndromes.'Rare cases of classic pause-dependent torsadede pointes without any recognised cause areusually referred to as idiopathic.'The adrenergic-dependent or congenital
long QT syndromes are typified by anenhanced adrenergic responsiveness.' 4 Thedevelopment of episodes of torsade depointes tachycardia is often associated with
an increase in catecholamines.4 The congeni-tal long QT syndromes are classified intothree syndromes: the Jervell-Lange-Nielsensyndrome,5 the Romano-Ward syndrome,67and a nonfamilial form with normal hearing.Episodes of ventricular tachycardias, oftentorsade de pointes, are more typically seen inchildren or young adults. The arrhythmiasusually appear as a result of physical exercise,pain, fright, sudden startling, or other intenseemotional states associated with increasedsympathetic activity. Atypical forms of adren-ergic-dependent long QT syndromes are seenin patients with intracranial disease, mitralvalve prolapse, and after radical neck dissec-tion and carotid endarterectomy.'
Patients with classic adrenergic-dependentlong QT syndromes show QTU interval pro-longations, abnormal TU waves, a lower thannormal heart rate and T wave alternans in theelectrocardiogram during sinus rhythm, butthese abnormalities may vary in size fromtime to time. These changes may be elicitedby manoeuvres that increase sympathetic tonefor example, exercise, the cold pressor test, orthe Valsalva manoeuvre.89
Catecholamine infusion with adrenalineisoprenaline, or phenylephrine has been usedto distinguish between the two groups."10 Inthe pause-dependent long QT syndromes,catecholamine infusion increases the heartrate, shortens the QTU interval, decreasesthe U wave amplitude, and suppresses ven-tricular arrhythmias. On the other hand, inthe adrenergic-dependent long QT syn-dromes, catecholamines lengthen the QTUinterval and may instigate torsade de pointestachycardia in susceptible individuals.'
It has been suggested that an abnormality ofunequal sympathetic tone, with overactivityin the left-sided cardiac efferent nervesaccompanied by malfunction of the right-sided cardiac efferents that causes a sympa-
207 on M
ay 14, 2021 by guest. Protected by copyright.
http://heart.bmj.com
/B
r Heart J: first published as 10.1136/hrt.72.2.205 on 1 A
ugust 1994. Dow
nloaded from

208riWpp, Blomstrdm
thetic imbalance and left sympathetic domi-nance, may cause a disparity in the ventricu-lar recovery process and thus prolong thevulnerable phase.4 Another possible causeunderlying the adrenergic-dependent longQT syndromes is an intrinsic myocardialabnormality of repolarisation, perhaps anabnormal ion channel protein, that leadsto early afterdepolarisations and triggeredactivity." 12
Yanowitz et al showed that in anaesthetiseddogs the QT interval is prolonged after right-sided stellectomy or by left stellate ganglionstimulation.'3 This accords with clinicalobservations of accentuation of abnormalitiesafter right stellate block or a reduction inabnormalities by right stellate stimulation andleft stellate block. Moss and McDonald firstshowed that left stellectomy is a highly effec-tive treatment for ventricular arrhythmias inthe adrenergic-dependent long QT syndromeand that it significantly reduces mortality.'4Otteni et al studied 60 patients undergoingradical neck dissection."' Right radical neckdissection resulted in a large, statistically sig-nificant increase in QT interval; the sameprocedure on the left side of the neck did notalter the QT interval. Ventricular tachycardiaof the torsade de pointes type, which causedcirculatory arrest, was seen in three patientsundergoing right radical neck dissection.Otteni et al suggest that the alteration (surgi-cal trauma) of right sympathetic outflow tothe heart by neck dissection probablyaccounts for QT interval prolongation andthe arrhythmias. This is supported by experi-mental data."3 Behne et al studied 40 patientsafter radical neck dissection. 16 This studyshowed significantly more frequent and largerQT prolongation in patients undergoingsurgery on the right side of the neck than inthose operated on the left side. However,none of the patients experienced any severearrhythmias. These observations also suggestthat sympathetic imbalance with decreasedright-sided activity was the pathogeneticmechanism. Pfeiffer et al described a case ofintermittent long QT syndrome in a 21 yearold woman in whom postmortem examina-tion showed active inflammation of stellateganglia."7Our patient had no family history of synco-
pal attacks or long QT syndrome, nor was hetaking any drugs known to cause QT prolon-gation or torsade de pointes tachycardia.Therefore we postulate that the parapharyn-geal abscess itself or the surgery on the right
side of the neck destroyed, damaged or dis-turbed conduction in the sympathetic fibreson the right side of the neck, leading to QTprolongation and an adrenergic-dependentlong QT syndrome.The recommended treatment for adrener-
gic-dependent long QT syndrome with ven-tricular arrhythmia is fi blockade.418 Toprotect against bradycardia, which may trig-ger the onset of torsade de pointes tachycar-dia during such treatment, our patient wasgiven an atrial demand rate adaptive pace-maker (AAI-R system)."9
1 Jackman WM, Friday KJ, Anderson JL, Aliot EM, ClarkM, Lazzara R. The long QT syndromes: a criticalreview, new clinical observations and a unifying hypo-thesis. Prog Cardiovasc Dis 1988;31:115-72.
2 Cranefield PF, Aronson RS. Torsade de pointes and otherpause-induced ventricular tachycardias: the short-long-short sequence and early afterdepolarizations. PACE1988;11:670-8.
3 Stratmann HG, Kennedy HL. Torsade de pointes associ-ated with drugs and toxins: Recognition and manage-ment. Am Hearty 1987;113:1470-82.
4 Schwartz PJ. Idiopathic long QT-syndrome: progress andquestions. Am HeartJ 1985;109:399-411.
5 Jervell A, Lange-Nielsen F. Congenital deaf-mutism,functional heart disease with prolongation of the Q-T-interval and sudden death. Am HeartJ 1957;54:59.
6 Romano C, Gemme G, Pongiglione R. Aritmie cardiacherare delleta pediatrica. La Clinica Pediatrica 1963;45:656.
7 Ward OC. New familial cardiac syndrome in children. J IrMedAssoc 1964;54: 103.
8 Curtiss EI, Hiebel RH, Shaver JA. Autonomic maneuversin hereditary Q-T interval prolongation (Romano-Wardsyndrome). Am HeartJ 1978;95:420-7.
9 Vincent MG, Jaiswal D, Timothy KW. Effects of exerciseon heart rate, QT, QTc and QT/QS2 in the Romano-Ward inherited long QT syndrome. Am J Cardiol 1991;68:498-503.
10 Wataru S, Tohru 0, Takashi K, Katsuro S. Differentialresponse ofQTU interval to exercise, isoproterenol, andatrial pacing in patients with congenital long QT syn-drome. PACE 1991;14:1966-70.
11 Zipes DP. The long QT interval syndrome, a rosetta stonefor sympathetic related ventricular tachyarrhythmias.Circulation 1991;84: 1414-9.
12 Shimizu W, Ohe T, Kurita T, et al. Early afterdepolarisa-tions induced by isoproterenol in patients with congeni-tal long QT syndrome. Circulation 1991;84:1915-23.
13 Yanowitz F, Preston JB, Abildskov JA. FunctionalDistribution of Right and Left Stellate Innervation tothe Ventricles. Circulation Res 1966;18:416-28.
14 Moss AJ, McDonald J. Unilateral cervicothoracic sympa-thetic ganglionectomy for the treatment of long Q-Tinterval syndrome. N EnglJ Med 197 1;285:903.
15 Otteni JC, Pottecher T, Bronner G, Flesch H, Diebolt JR.Prolongation of the Q-T interval and sudden cardiacarrest following right radical neck dissection.Anesthesiology 1983;59:358-61.
16 Behne M, Hermann R, Lischke V, L6rz M. Unter-suchungen zur Verlangerung der QT-Zeit im EKG nachOperationen am Hals (Neck dissection). HNO 1989:12:449-53.
17 Pfeiffer D, Fiehring H, Henkel HG, Rostock KJ, RathgenK. Long QT syndrome associated with inflammatorydegeneration of the stellate ganglia. Clin Cardiol 1989;12:222-4.
18 Crawford MH, Karliner JS, O'Rourke RA, Friedman WF.Prolonged Q-T interval syndrome: successful treatmentwith combined ventricular pacing and propanolol. Chest1975;68:369-71.
19 Eldar M, Griffin JC, Abbott JA, et al. Permanent cardiacpacing in patients with the long QT syndrome. . AmColl Cardiol 1987;10:600-7.
208 on M
ay 14, 2021 by guest. Protected by copyright.
http://heart.bmj.com
/B
r Heart J: first published as 10.1136/hrt.72.2.205 on 1 A
ugust 1994. Dow
nloaded from




![Torsade de Pointes Induced by Hypokalemia from Imipenem ...downloads.hindawi.com/journals/cric/2017/4565182.pdf · 4 CaseReportsinCardiology [8] R. Passman and A. Kadish, “Polymorphic](https://static.fdocuments.us/doc/165x107/5d54163388c993de068b4c64/torsade-de-pointes-induced-by-hypokalemia-from-imipenem-4-casereportsincardiology.jpg)