Endometrial Polyps1
4
Endometrial Polyps Endometrial polyps are small, soft growths on the lining of the uterus (the endometrium). Also known as uterine polyps, endometrial polyps can irritate the surrounding tissue and cause spotting or vaginal bleeding. The polyps can occur alone or in groups. Most uterine polyps are noncancerous (benign). What causes endometrial polyps? While the exact cause of endometrial polyps isn't known, they form when there is an overgrowth of tissue in the lining of the uterus. What are the symptoms of endometrial polyps? Endometrial polyps often cause no symptoms. If signs or symptoms do occur, they may include: Irregular menstrual bleeding Bleeding between menstrual periods Excessively heavy menstrual periods Vaginal bleeding after menopause Infertility What are the risk factors for endometrial polyps? Factors that may increase your risk of developing endometrial polyps include: Obesity Use of tamoxifen, a drug therapy for breast cancer High blood pressure (hypertension) Cervical polyps How are endometrial polyps diagnosed? Tests that may be run to determine the presence of polyps include: Pelvic exam (in some cases endometrial polyps may be seen if they are protruding through the cervix) Pap smear Ultrasound Hysterosalpingogram (HSG). Uses an x-ray and contrast dye injected into the uterus to detect polyps. Dilatation and curettage (D&C). Scraping the walls of the uterus to obtain a tissue sample. Hysteroscopy. Minimally invasive approach that uses a tiny telescope (hysteroscope) to examine the uterine lining for polyps. How are endometrial polyps treated? Treatment options for endometrial polyps include:
-
Upload
luke-obusan -
Category
Documents
-
view
5 -
download
2
description
about polyps in the uterus
Transcript of Endometrial Polyps1
Endometrial PolypsEndometrial polyps are small, soft growths on the lining of the uterus (the endometrium). Also known as uterine polyps, endometrial polyps can irritate the surrounding tissue and cause spotting or vaginal bleeding. The polyps can occur alone or in groups. Most uterine polyps are noncancerous (benign).What causes endometrial polyps?While the exact cause of endometrial polyps isn't known, they form when there is an overgrowth of tissue in the lining of the uterus.What are the symptoms of endometrial polyps?Endometrial polyps often cause no symptoms. If signs or symptoms do occur, they may include: Irregular menstrual bleeding Bleeding between menstrual periods Excessively heavy menstrual periods Vaginal bleeding after menopause InfertilityWhat are the risk factors for endometrial polyps?Factors that may increase your risk of developing endometrial polyps include: Obesity Use of tamoxifen, a drug therapy for breast cancer High blood pressure (hypertension) Cervical polypsHow are endometrial polyps diagnosed?Tests that may be run to determine the presence of polyps include: Pelvic exam (in some cases endometrial polyps may be seen if they are protruding through the cervix) Pap smear Ultrasound Hysterosalpingogram (HSG). Uses an x-ray and contrast dye injected into the uterus to detect polyps. Dilatation and curettage (D&C). Scraping the walls of the uterus to obtain a tissue sample. Hysteroscopy. Minimally invasive approach that uses a tiny telescope (hysteroscope) to examine the uterine lining for polyps.How are endometrial polyps treated?Treatment options for endometrial polyps include:Watch and wait approach.If the polyps are small and not causing symptoms, they may be left alone and watched to see if they go away on their own.Medication.Certain medications may shrink the polyps and lessen symptoms, however the symptoms typically recur once the medication is stopped.Surgical removal.Endometrial polyps can be removed duringhysteroscopy, a procedure that uses a tiny telescope (hysteroscope) and thin surgical instruments to view and treat areas inside the uterus. A curettage may also be performed - scraping of the uterus to remove the polyps - guided by a hysteroscope.Hysterectomy.In rare cases ahysterectomy(surgery to remove the uterus) may be recommended to remove cancerous cells or numerous polyps. Uterine polyps can recur, requiring additional treatment.endometrial polyporuterine polypis amassin the inner lining of the uterus.[1]They may have a large flat base (sessile) or be attached to the uterus by an elongatedpedicle(pedunculated).[1][2]Pedunculated polyps are more common than sessile ones.[3]They range in size from a few millimeters to several centimeters.[2]If pedunculated, they can protrude through thecervixinto thevagina.[1][4]Small blood vessels may be present, particularly in large polyps.[1]Contents[hide] 1Cause and symptoms 2Diagnosis 3Treatment 4Prognosis and complications 5Risk factors and epidemiology 6Structure 7See also 8ReferencesCause and symptoms[edit]No definitive cause of endometrial polyps is known, but they appear to be affected by hormone levels and grow in response to circulatingestrogen.[2]They often cause no symptoms.[3]Where they occur, symptoms include irregular menstrual bleeding, bleeding between menstrual periods, excessively heavy menstrual bleeding (menorrhagia), and vaginal bleeding aftermenopause.[2][5]Bleeding from the blood vessels of the polyp contributes to an increase of blood loss during menstruation and blood "spotting" between menstrual periods, or after menopause.[6]If the polyp protrudes through the cervix into the vagina, pain (dysmenorrhea) may result.[4]Diagnosis[edit]
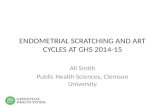
Micrographof an endometrial polyp.H&E stain.Endometrial polyps can be detected byvaginalultrasound(sonohysterography),hysteroscopyanddilation and curettage.[2]Detection by ultrasonography can be difficult, particularly when there isendometrial hyperplasia(excessive thickening of the endometrium).[1]Larger polyps may be missed by curettage.[7]Treatment[edit]Polyps can be surgically removed usingcurettagewith or without hysteroscopy.[8]When curettage is performed without hysteroscopy, polyps may be missed. To reduce this risk, the uterus can be first explored using graspingforcepsat the beginning of the curettage procedure.[6]Hysteroscopy involves visualising the endometrium (inner lining of the uterus) and polyp with a camera inserted through thecervix. If it is a large polyp, it can be cut into sections before each section is removed.[6]Ifcancerouscells are discovered, ahysterectomy(surgical removal of the uterus) may be performed.[2]A hysterectomy would usually not be considered if cancer has been ruled out.[6]Whichever method is used, polyps are usually treated undergeneral anesthetic.[7]It is unclear if removing polyps affects fertility as it has not been studied.[9]Prognosis and complications[edit]Endometrial polyps are usuallybenignalthough some may beprecancerousorcancerous.[2]About 0.5% of endometrial polyps containadenocarcinomacells.[10]Polyps can increase the risk ofmiscarriagein women undergoingIVFtreatment.[2]If they develop near thefallopian tubes, they may lead to difficulty in becoming pregnant.[2]Although treatments such as hysteroscopy usually cure the polyp concerned, recurrence of endometrial polyps is frequent.[6]Untreated, small polyps may regress on their own.[11]Risk factors and epidemiology[edit]Endometrial polyps usually occur in women in their 40s and 50s.[2]Risk factors includeobesity,high blood pressureand a history ofcervical polyps.[2]Takingtamoxifenorhormone replacement therapycan also increase the risk of uterine polyps.[2][12]The use of anIntraUterine Systemcontaininglevonorgestrelin women taking Tamoxifen may reduce the incidence of polyps.[13]Endometrial polyps occur in up to 10% of women.[1]It is estimated that they are present in 25% of women with abnormal vaginal bleeding.[12]Structure[edit]Endometrial polyps can be solitary or occur with others.[14]They are round or oval and measure between a few millimeters and several centimeters in diameter.[6][14]They are usually the same red/brown color of the surrounding endometrium although large ones can appear to be a darker red.[6]The polyps consist of dense, fibrous tissue (stroma), blood vessels and glandlike spaces lined with endometrialepithelium.[6]If they are pedunculated, they are attached by a thin stalk (pedicle). If they are sessile, they are connected by a flat base to the uterine wall.[14]Pedunculated polyps are more common than sessile ones.[3]