Endometrial CA
74
ENDOMETRIAL CARCINOMA
-
Upload
mohamad-zekry-zuhairy -
Category
Documents
-
view
237 -
download
2
description
EndoCa
Transcript of Endometrial CA
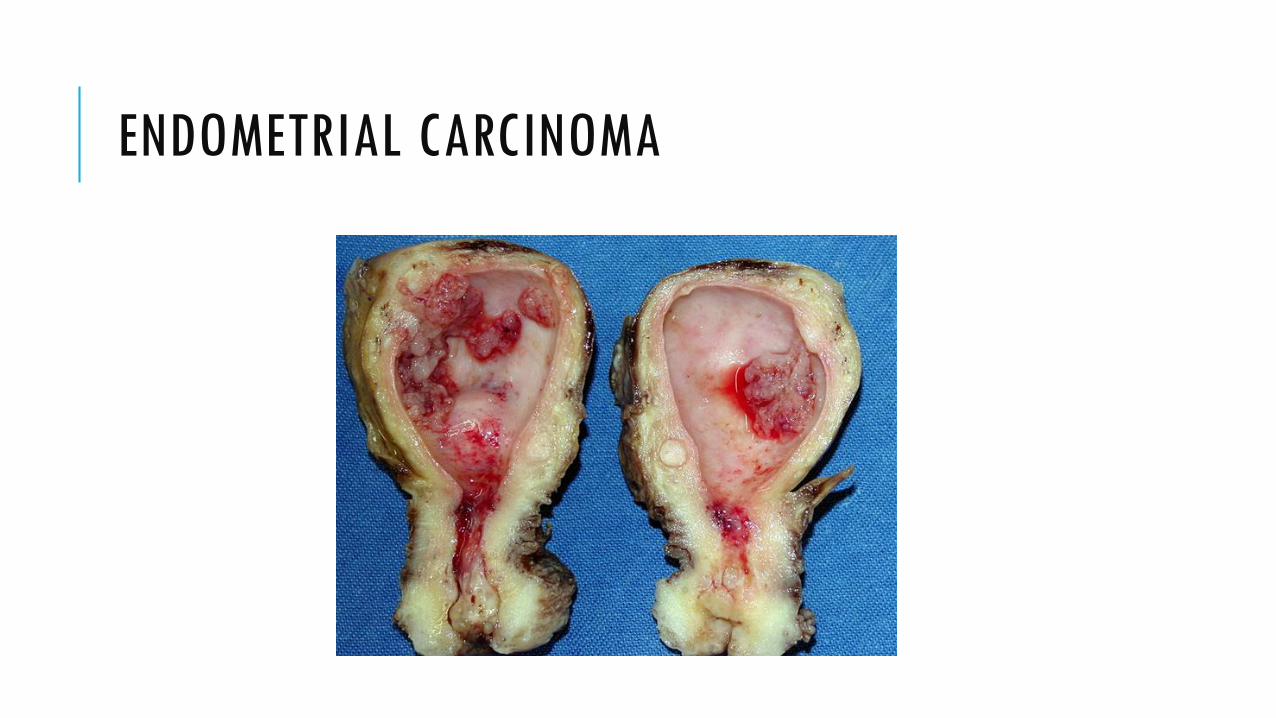
ENDOMETRIAL CARCINOMA
TRIGGER:
55 years old, nulliparous lady come to clinic for bleeding per vaginal for 2 weeks. She was menopause for 3 years duration. She had diabetes and hypertension and was on treatment for 2 year.
DEFINITION –POSTMENOPAUSAL BLEEDING
Any vaginal bleeding that occurs after 12-months period of amenorrhea that has occur due to menopause.
In Malaysia, average menopausal age are
51.7 years old
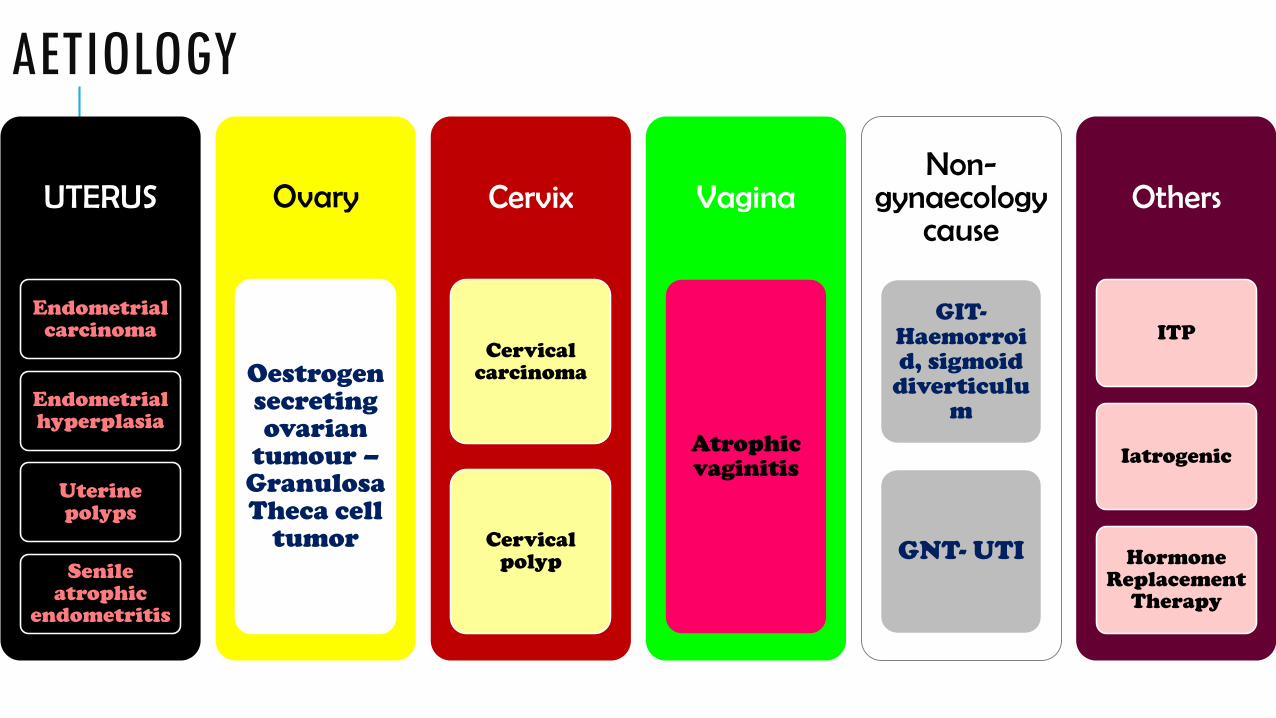
AETIOLOGY
UTERUS
Endometrial carcinoma
Endometrial hyperplasia
Uterine polyps
Senile atrophic
endometritis
Ovary
Oestrogensecreting ovarian
tumour –Granulosa Theca cell
tumor
Cervix
Cervical carcinoma
Cervical polyp
Vagina
Atrophic vaginitis
Non-gynaecology
cause
GIT-Haemorroid, sigmoid
diverticulum
GNT- UTI
Others
ITP
Iatrogenic
Hormone Replacement
Therapy
ENDOMETRIAL CARCINOMA
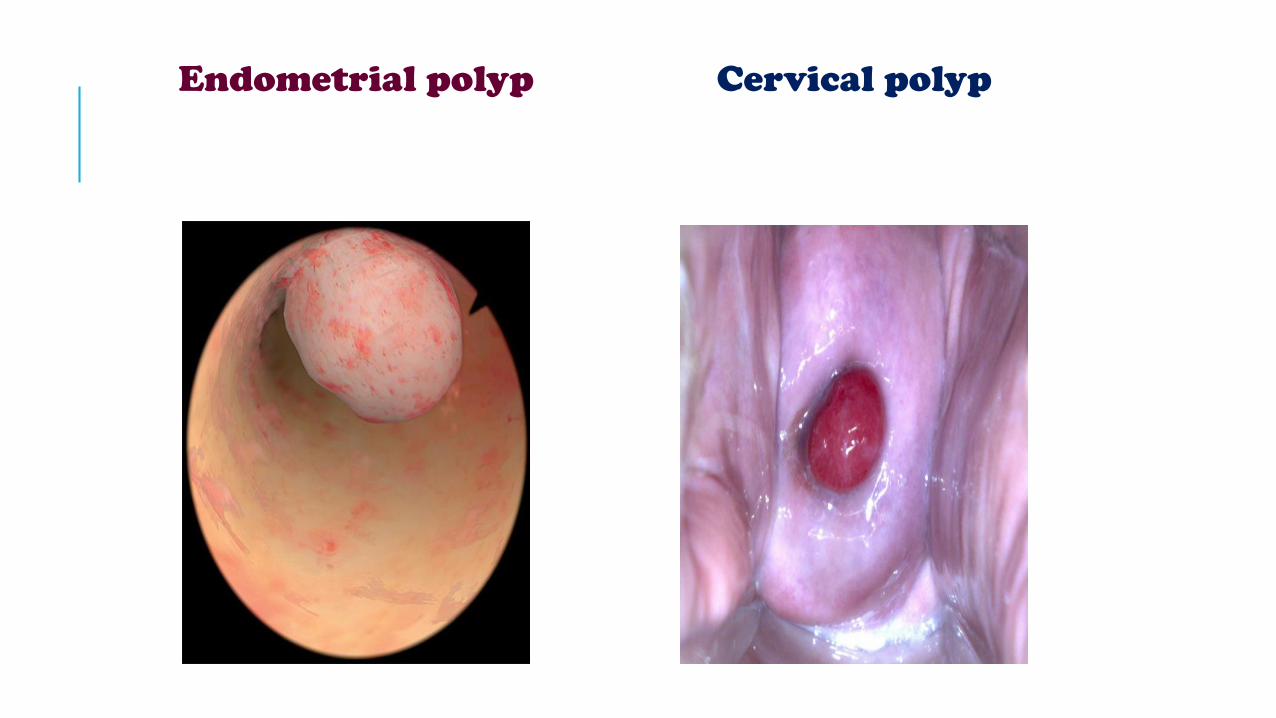
Endometrial polyp Cervical polyp
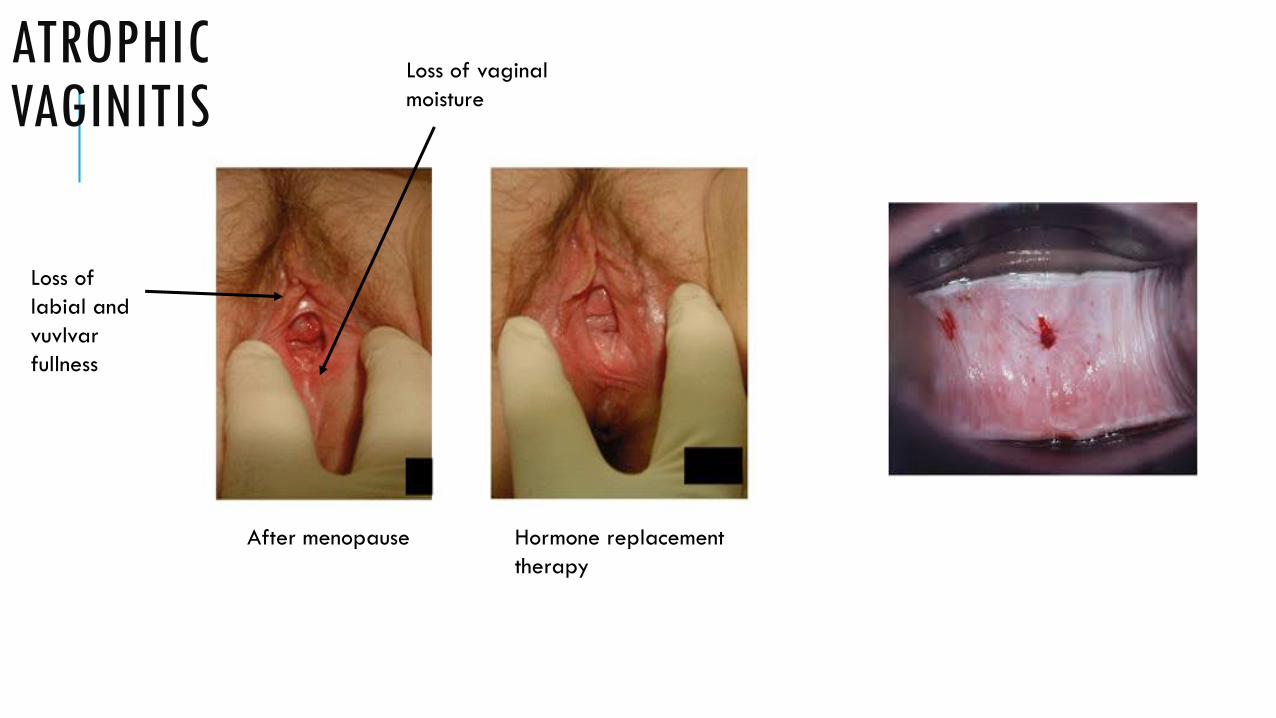
ATROPHIC VAGINITIS
After menopause Hormone replacement
therapy
Loss of vaginal
moisture
Loss of
labial and
vuvlvar
fullness
DEFINITION –ENDOMETRIAL CARCINOMA
Endometrial carcinoma is types of malignancy that arise from endometrium or lining of uterus. Encyclopedia of Cancer, Volume 1
Cancer that forms in tissues of the uterus (the small, hollow, pear-shaped organ in a woman's pelvis in which a fetus develops). National Cancer Institute
RISK FACTORS:
Hypertension
Nulliparous
Gender
Age
Diabetes
RISK FACTOR
Obesity Early Menarche
Late Menopause >52 years
Polycystic Ovarian Syndrome
Functioning Ovarian Tumour
Chronic Anovulatory Genetic
Family History
Hormone Replacement Therapy
Tamoxifen
ESTROGEN
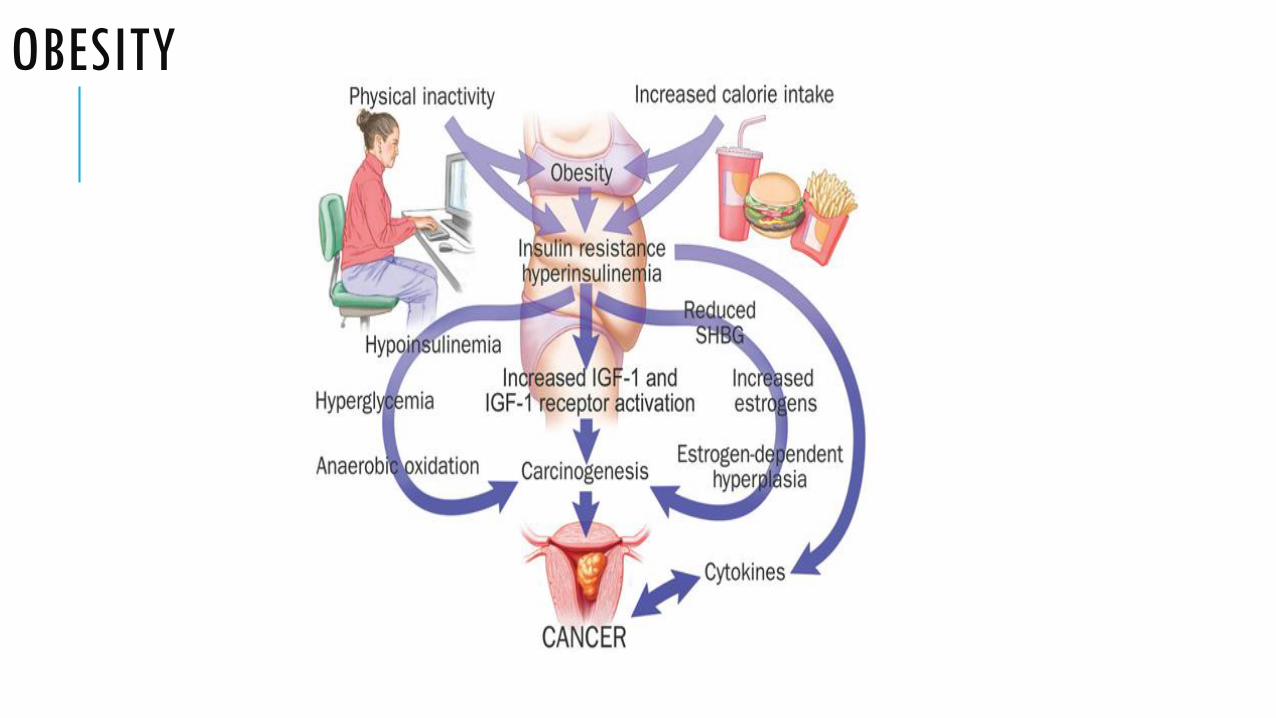
OBESITY
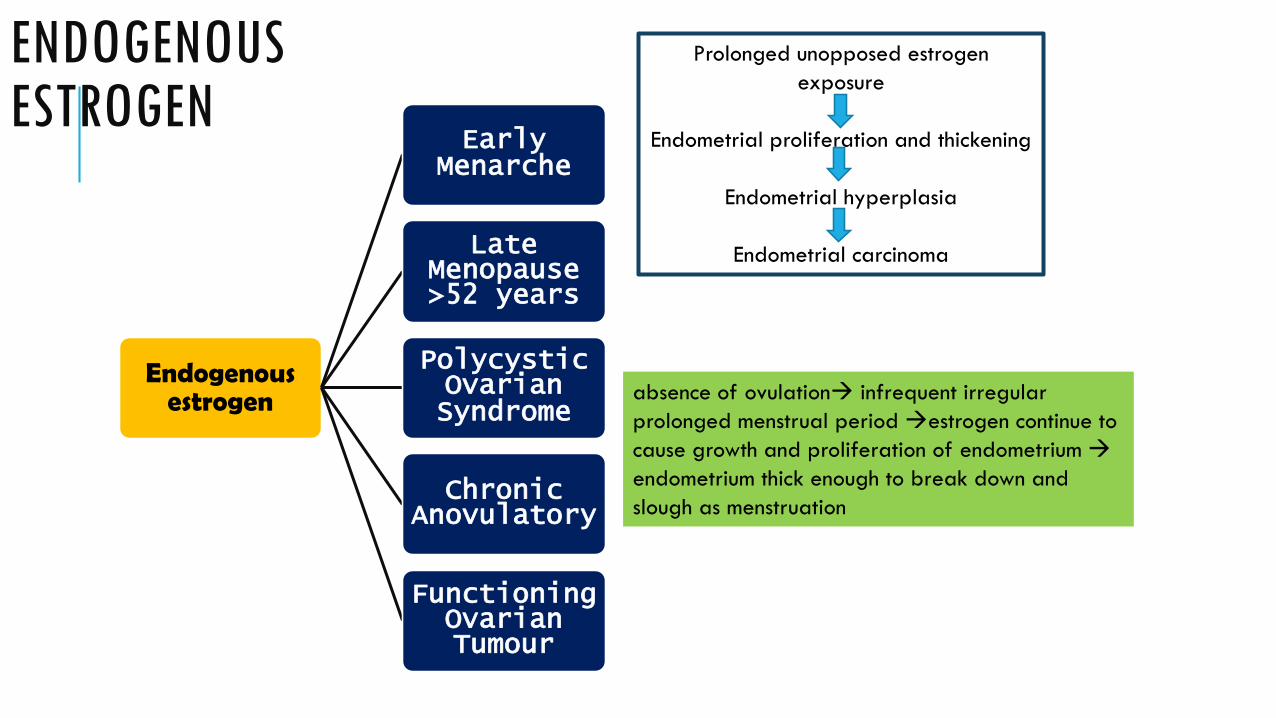
ENDOGENOUS ESTROGEN
Endogenous estrogen
Early Menarche
Late Menopause >52 years
Polycystic Ovarian Syndrome
Chronic Anovulatory
Functioning Ovarian Tumour
absence of ovulation infrequent irregular
prolonged menstrual period estrogen continue to
cause growth and proliferation of endometrium
endometrium thick enough to break down and
slough as menstruation
Prolonged unopposed estrogen
exposure
Endometrial proliferation and thickening
Endometrial hyperplasia
Endometrial carcinoma
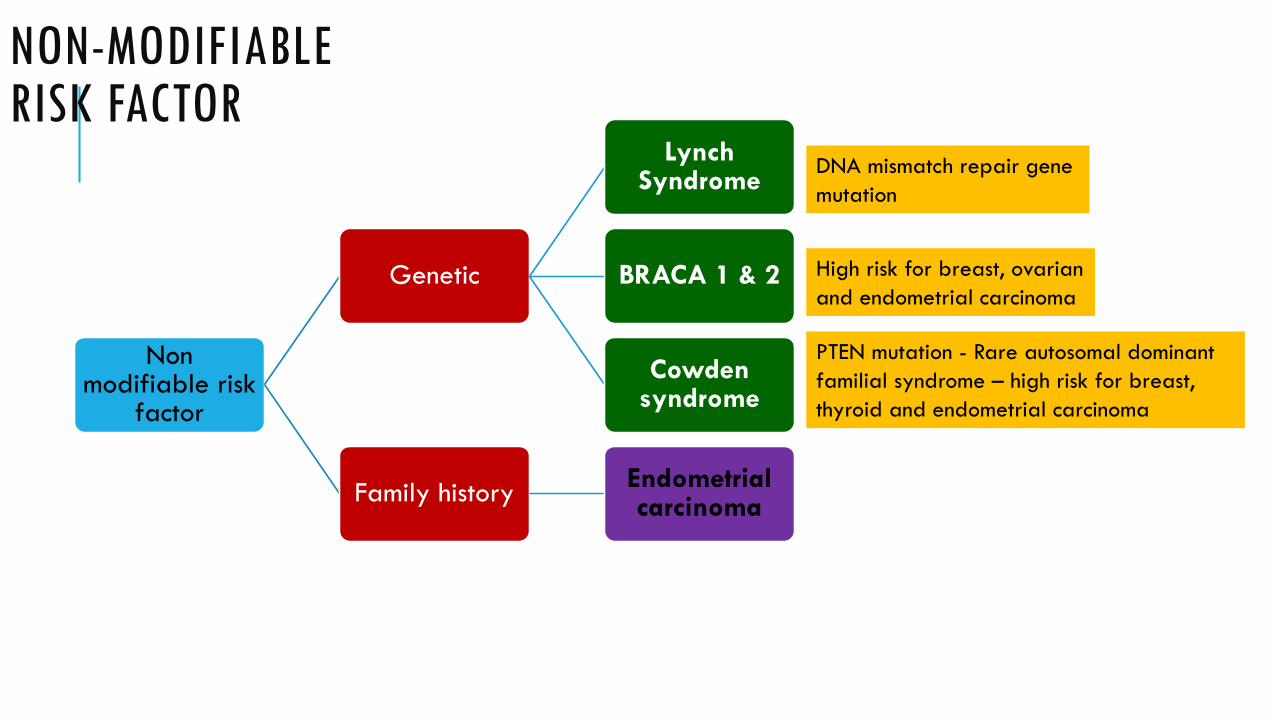
NON-MODIFIABLE RISK FACTOR
Non modifiable risk
factor
Genetic
Lynch Syndrome
BRACA 1 & 2
Cowden syndrome
Family historyEndometrial carcinoma
DNA mismatch repair gene
mutation
PTEN mutation - Rare autosomal dominant
familial syndrome – high risk for breast,
thyroid and endometrial carcinoma
High risk for breast, ovarian
and endometrial carcinoma
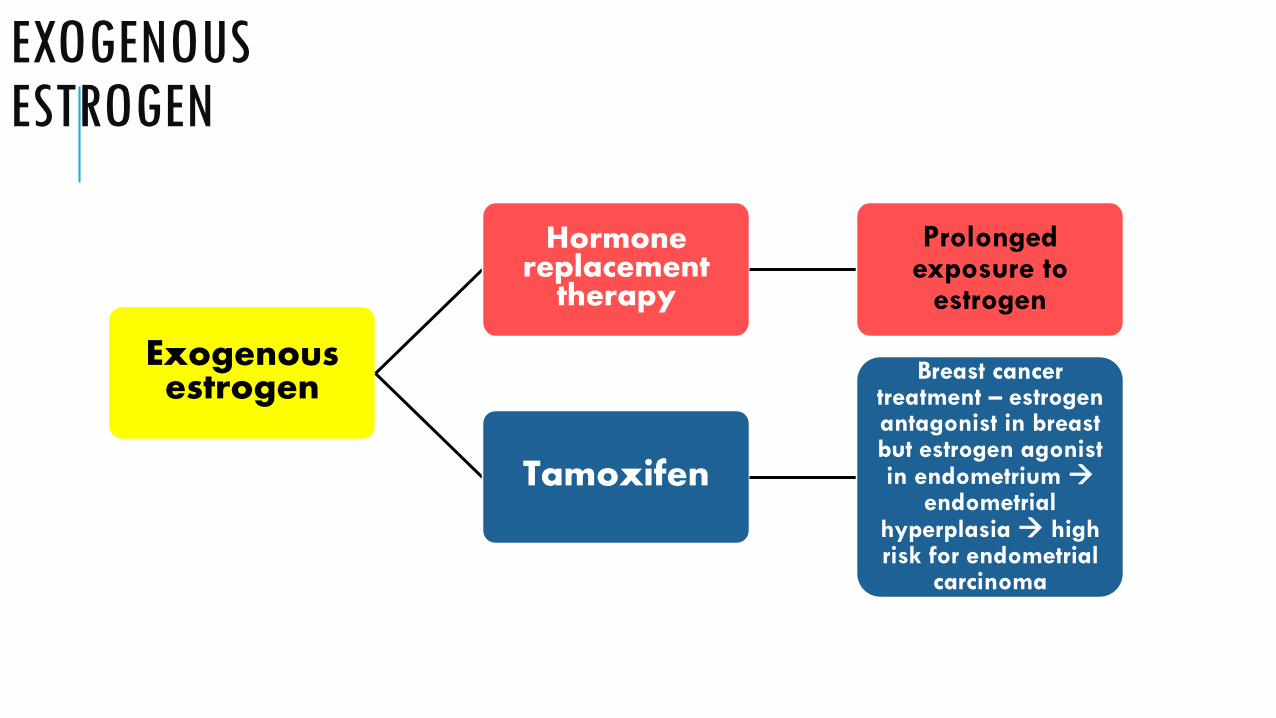
EXOGENOUS ESTROGEN
Exogenous estrogen
Hormone replacement
therapy
Prolonged exposure to
estrogen
Tamoxifen
Breast cancer treatment – estrogen antagonist in breast but estrogen agonist in endometrium
endometrial hyperplasia high risk for endometrial
carcinoma

His
tory
ta
kin
g
age
LMP
Bleeding
Vaginal discharge
Constitutional symptoms
Obstetric hx
Gynaecology hx
Drug hx15
History Taking
16
• Last menstrual period?
• Age?
• Bleeding:
Amount & duration of bleeding?
Is it associated with intercourse?
Any associated symptom?
Any similar previous episodes?
• Any vaginal discharge:
Any features suggestive of infection?
• Any constitutional symptom (LOW, LOA)?
• Obstetric history:
Nulliparity associated with endometrial carcinoma or ovarian
carcinoma
• Gynaecology history:
Result of pap smear test
• Drug history:
Usage of HRT?
On Tamoxifen therapy?
17
History Taking

18
Physical Examination
• General appearance
Pallor
Cachexia
Lymphadenopathy
Establish BMI
• Abdominal examination
Uterus with normal size
Enlargement of uterus in late cases
• Vaginal examination with speculum
Endometrial carcinoma
• 30% of all gynaecological malignancies
• Mean age diagnosis is 54
• Seen in post menopausal age group, but
may still be seen in peri-menopausal women
19

Aetiology of endometrial carcinoma
• Unknown exact cause
• Clear association with high levels of
circulating oestrogen in body.
20
Pathology of endometrium carcinoma
• Clinicopathologic studies and molecular
analyses support the classification of
endometrial carcinoma into type I and type II.
• Type I: Endometrioid adenocarcinoma
(commonest, 90%)
• Type II: Serous papillary carcinoma
21
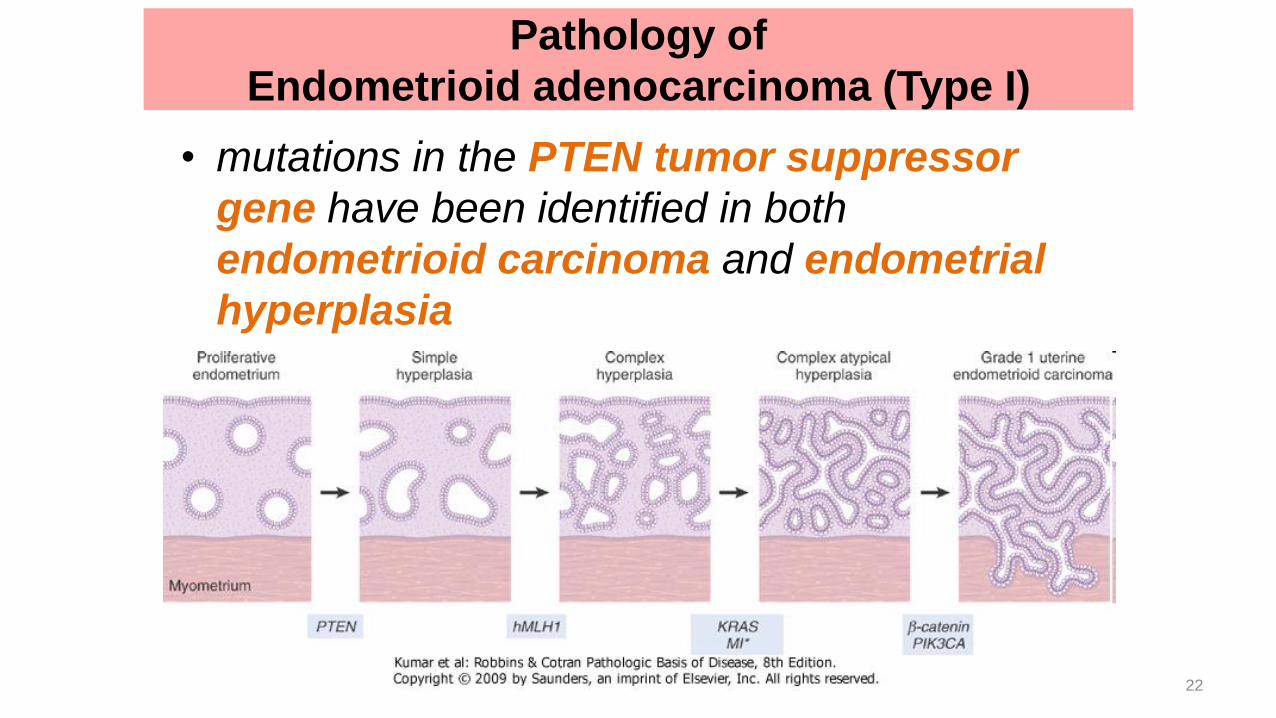
• mutations in the PTEN tumor suppressor
gene have been identified in both
endometrioid carcinoma and endometrial
hyperplasia
Pathology of
Endometrioid adenocarcinoma (Type I)
22
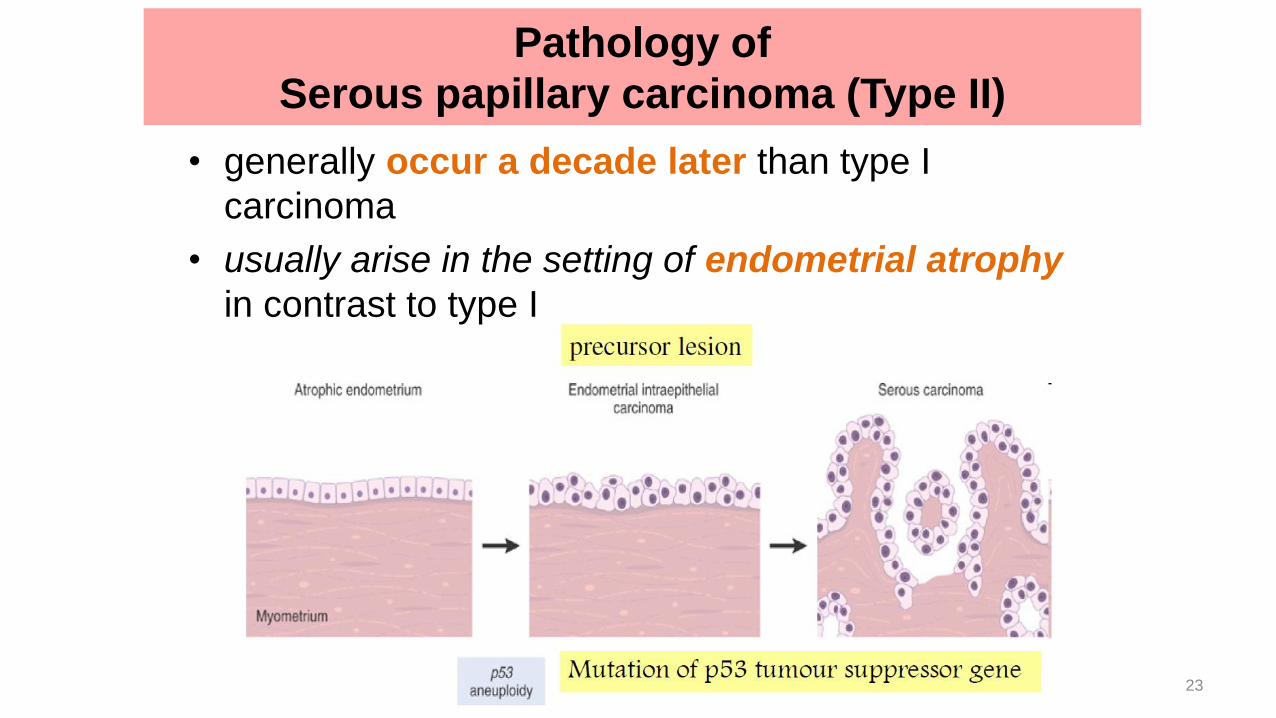
• generally occur a decade later than type I
carcinoma
• usually arise in the setting of endometrial atrophy
in contrast to type I
Pathology of
Serous papillary carcinoma (Type II)
23
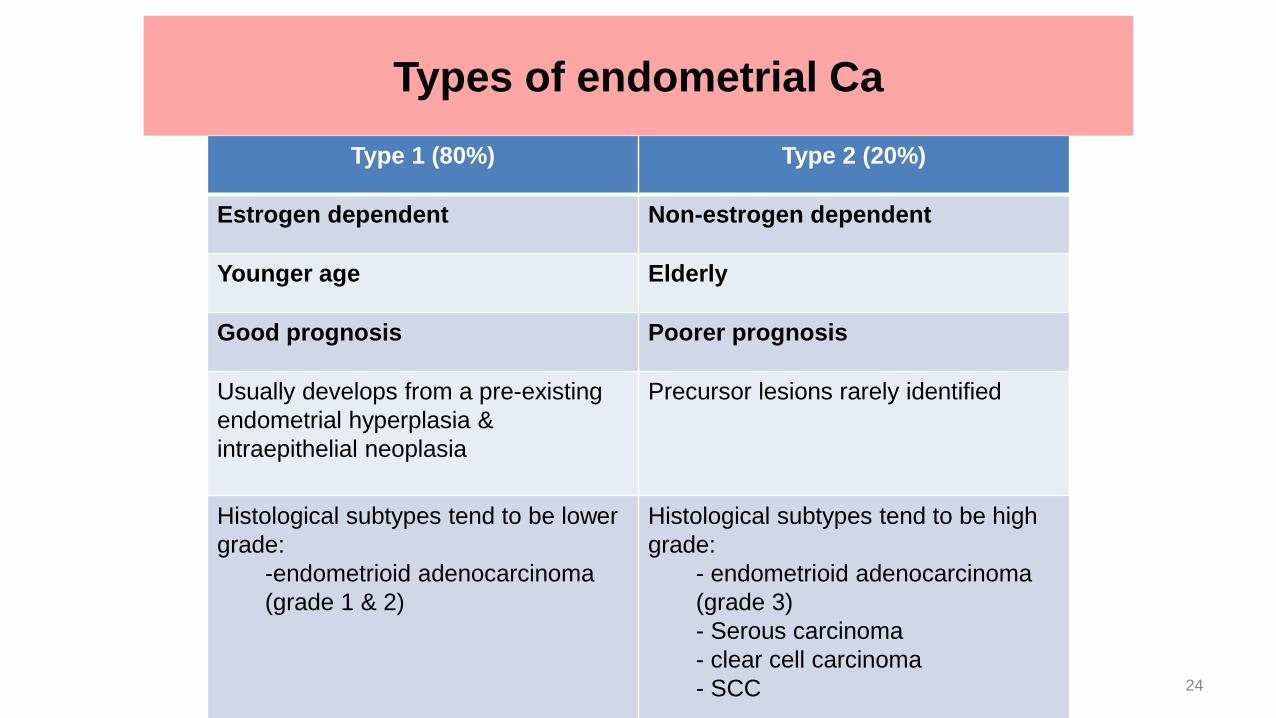
Type 1 (80%) Type 2 (20%)
Estrogen dependent Non-estrogen dependent
Younger age Elderly
Good prognosis Poorer prognosis
Usually develops from a pre-existing
endometrial hyperplasia &
intraepithelial neoplasia
Precursor lesions rarely identified
Histological subtypes tend to be lower
grade:
-endometrioid adenocarcinoma
(grade 1 & 2)
Histological subtypes tend to be high
grade:
- endometrioid adenocarcinoma
(grade 3)
- Serous carcinoma
- clear cell carcinoma
- SCC 24
Types of endometrial Ca
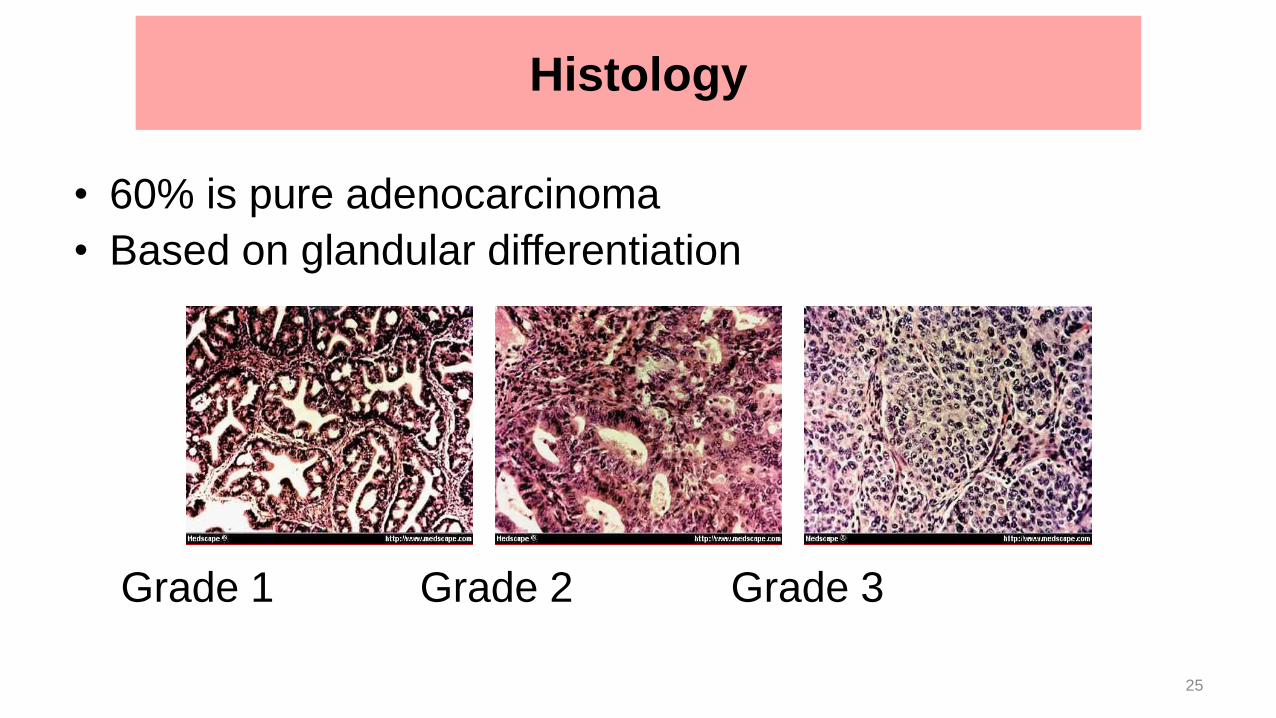
• 60% is pure adenocarcinoma
• Based on glandular differentiation
Grade 1 Grade 2 Grade 3
Histology
25
• Adeno-squamoid. Divided into 2:
Grade 1 Adeno-acanthoma. Squamous cell well-
differentiated
Grade 2 adeno-squamous. Poorly differentiated
squamous cell
Histology
26
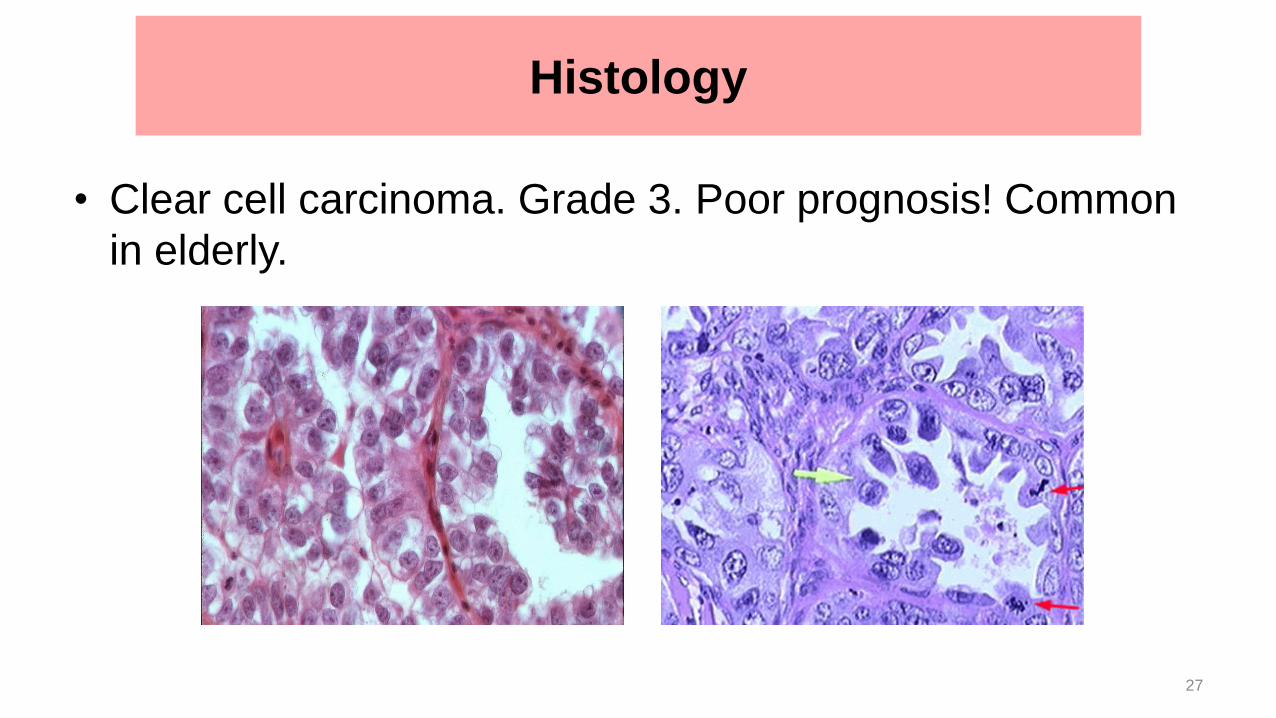
• Clear cell carcinoma. Grade 3. Poor prognosis! Common
in elderly.
Histology
27

• abnormal vaginal bleeding.- post-menopausal or
irregular-90% cases
• Postmenopausal woman >> postmenopausal bleed
(slight and intermittent at first, then become
continuous and heavy) and watery vaginal discharge
which later become offensive.
• Premenopausal woman >> intermenstrual bleeding,
blood-stained vaginal discharge, heavy menstrual
bleeding, lower abdominal pain, & dyspareunia.
Clinical Features
• Loss of appetite, Loss of weight
• Compression symptoms
• Pap smear result showed abnormal glandular
cytology
• advance cancer, these symptoms may be seen:
– Evidence of fistula (uterus to bladder / rectum)
– Bony metastases
– Altered liver functions
– Respiratory symptoms
Clinical Features
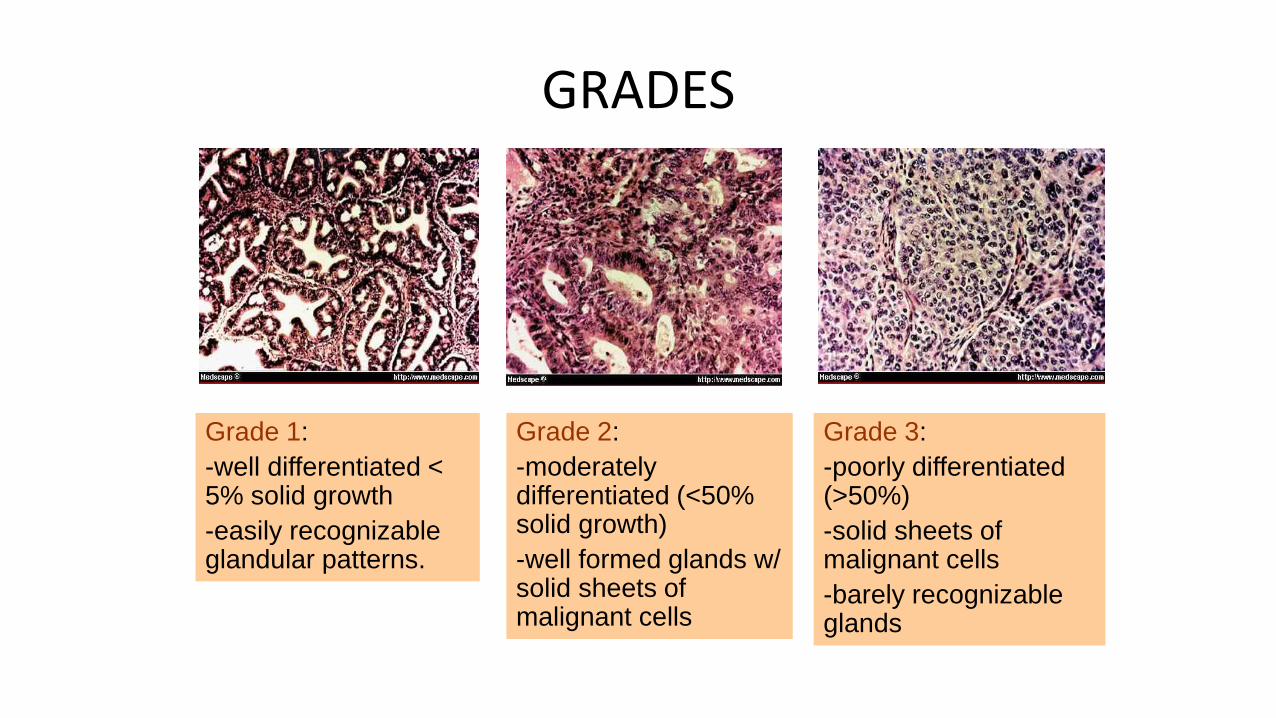
GRADES
Grade 1:
-well differentiated < 5% solid growth
-easily recognizable glandular patterns.
Grade 2:
-moderately differentiated (<50% solid growth)
-well formed glands w/ solid sheets of malignant cells
Grade 3:
-poorly differentiated (>50%)
-solid sheets of malignant cells
-barely recognizable glands
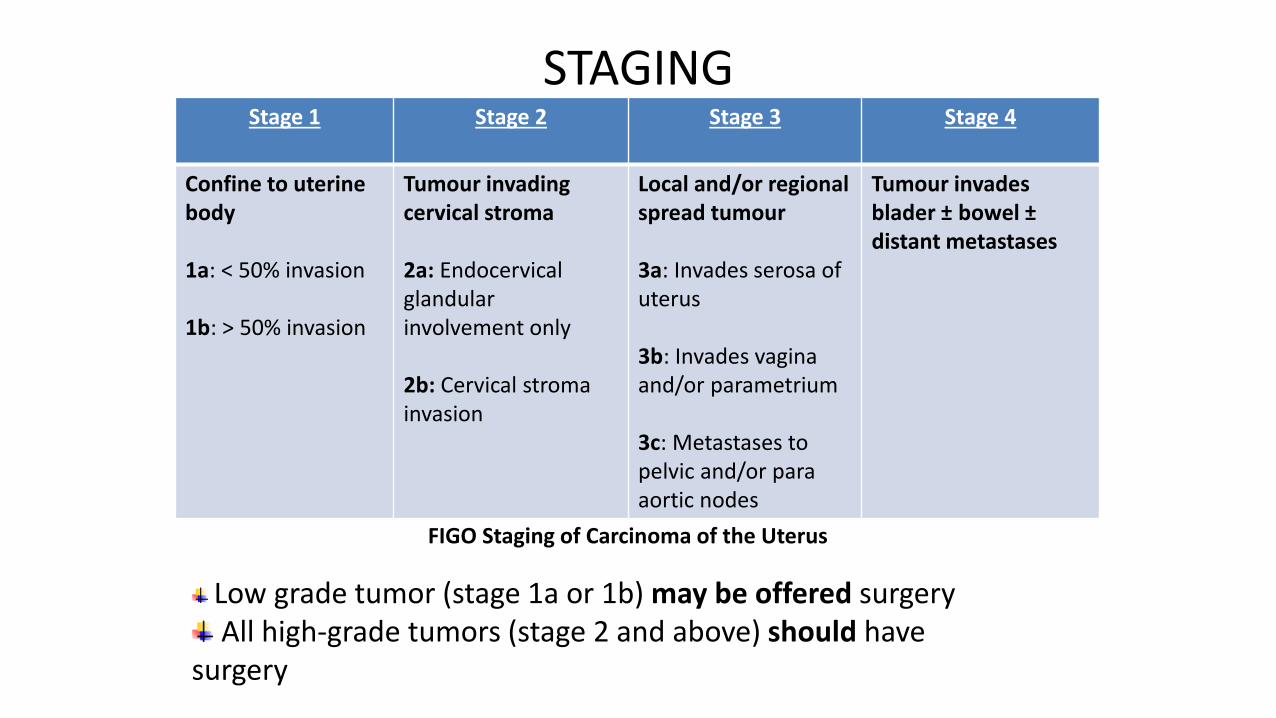
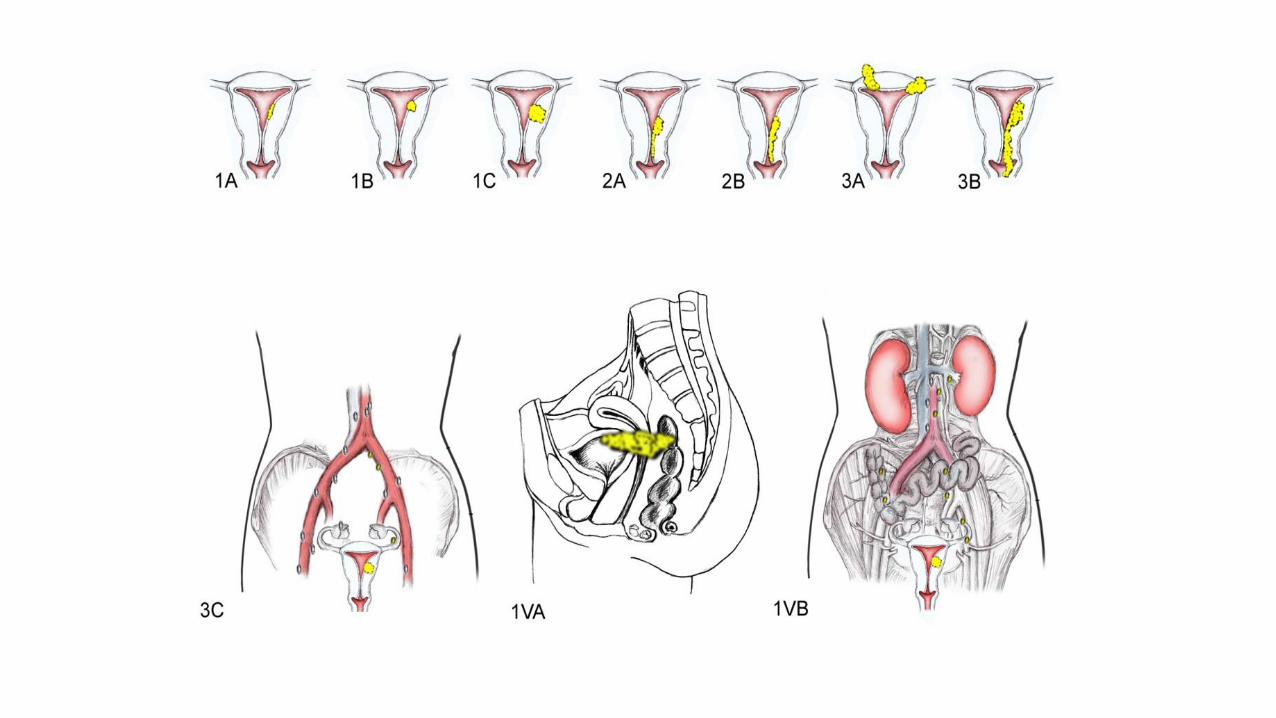
STAGINGStage 1 Stage 2 Stage 3 Stage 4
Confine to uterine body
1a: < 50% invasion
1b: > 50% invasion
Tumour invading cervical stroma
2a: Endocervicalglandular involvement only
2b: Cervical stromainvasion
Local and/or regional spread tumour
3a: Invades serosa of uterus
3b: Invades vagina and/or parametrium
3c: Metastases to pelvic and/or para aortic nodes
Tumour invades blader ± bowel ±distant metastases
FIGO Staging of Carcinoma of the Uterus
Low grade tumor (stage 1a or 1b) may be offered surgeryAll high-grade tumors (stage 2 and above) should have
surgery
METASTASIS
• Slow to spread – endometrium lack of lymphatics
• Most metastases occur in adjacent structure and peritoneum
• Advance cases – distant metastases occur, most commonly in lung, occasionally in liver, vertebrae or other bones and in supraclavicular lymph nodes
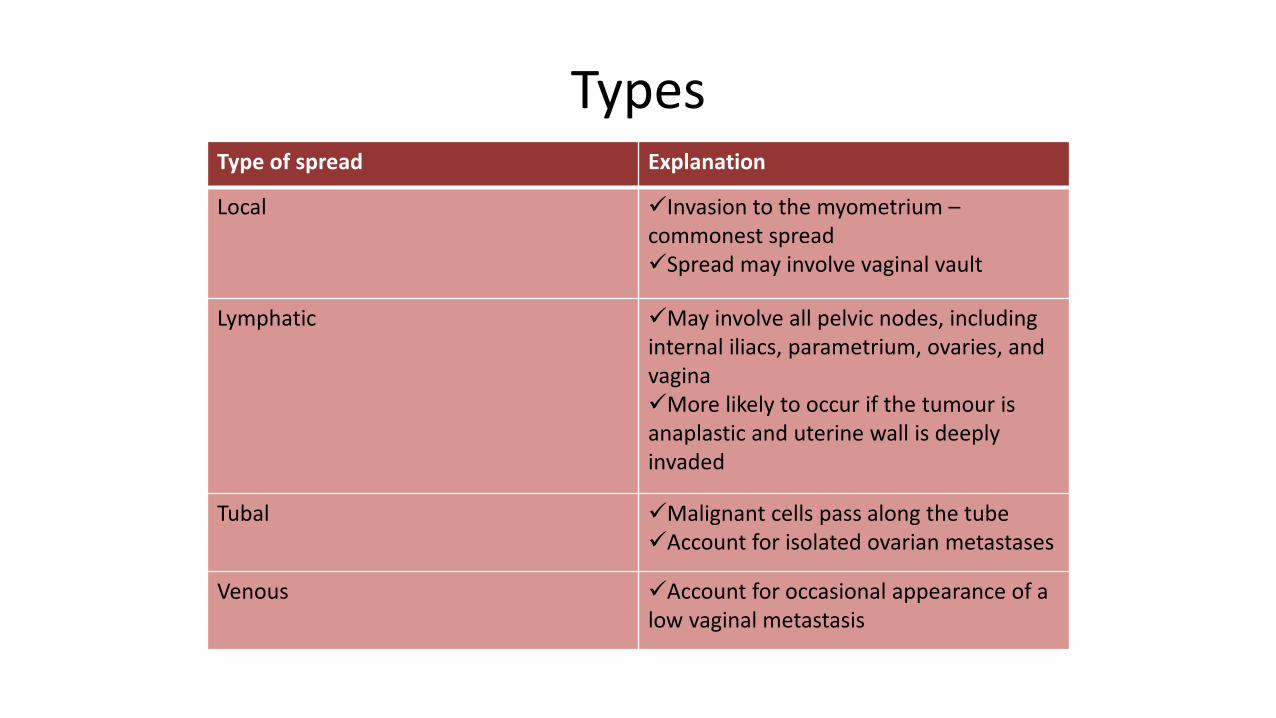
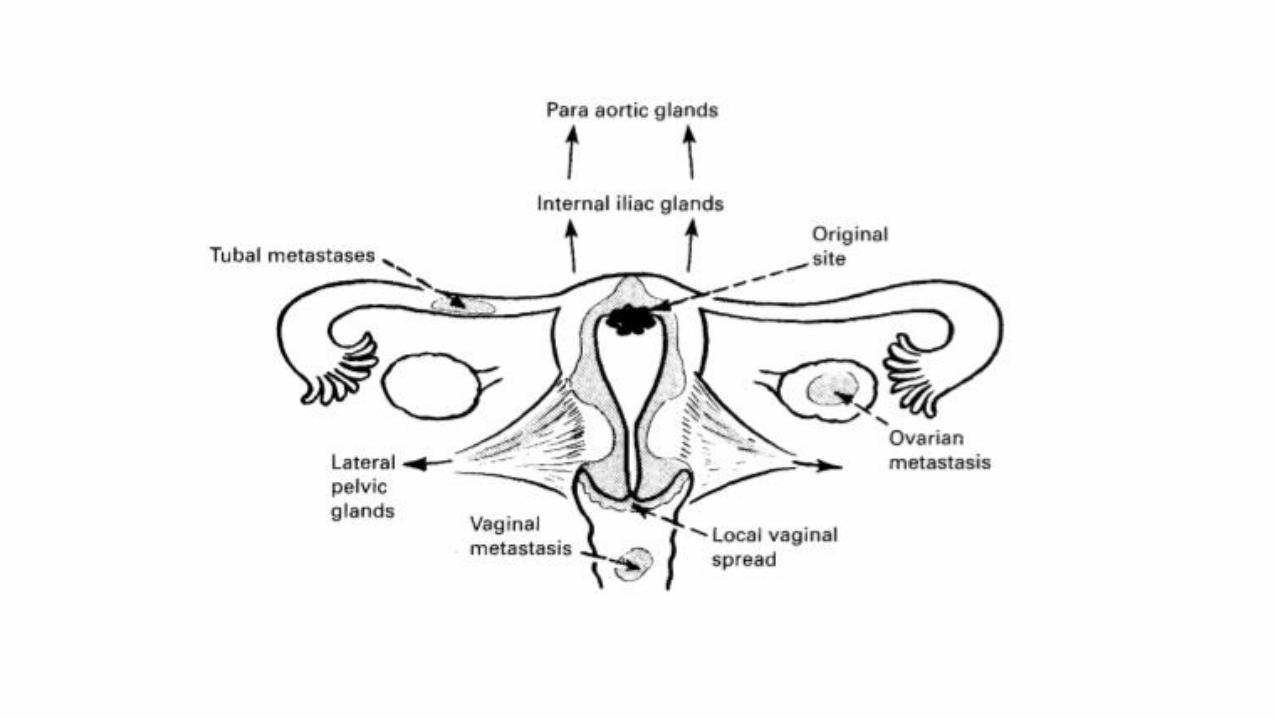
TypesType of spread Explanation
Local Invasion to the myometrium –commonest spreadSpread may involve vaginal vault
Lymphatic May involve all pelvic nodes, including internal iliacs, parametrium, ovaries, and vaginaMore likely to occur if the tumour is anaplastic and uterine wall is deeply invaded
Tubal Malignant cells pass along the tubeAccount for isolated ovarian metastases
Venous Account for occasional appearance of a low vaginal metastasis

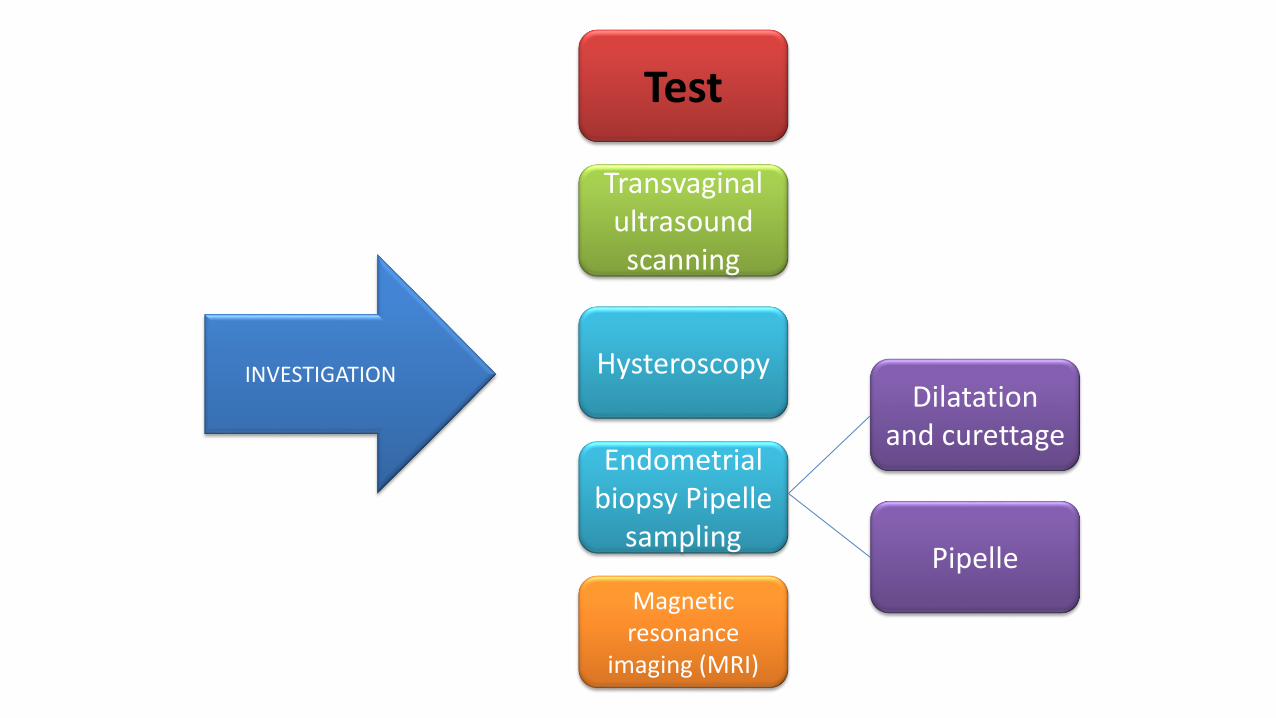
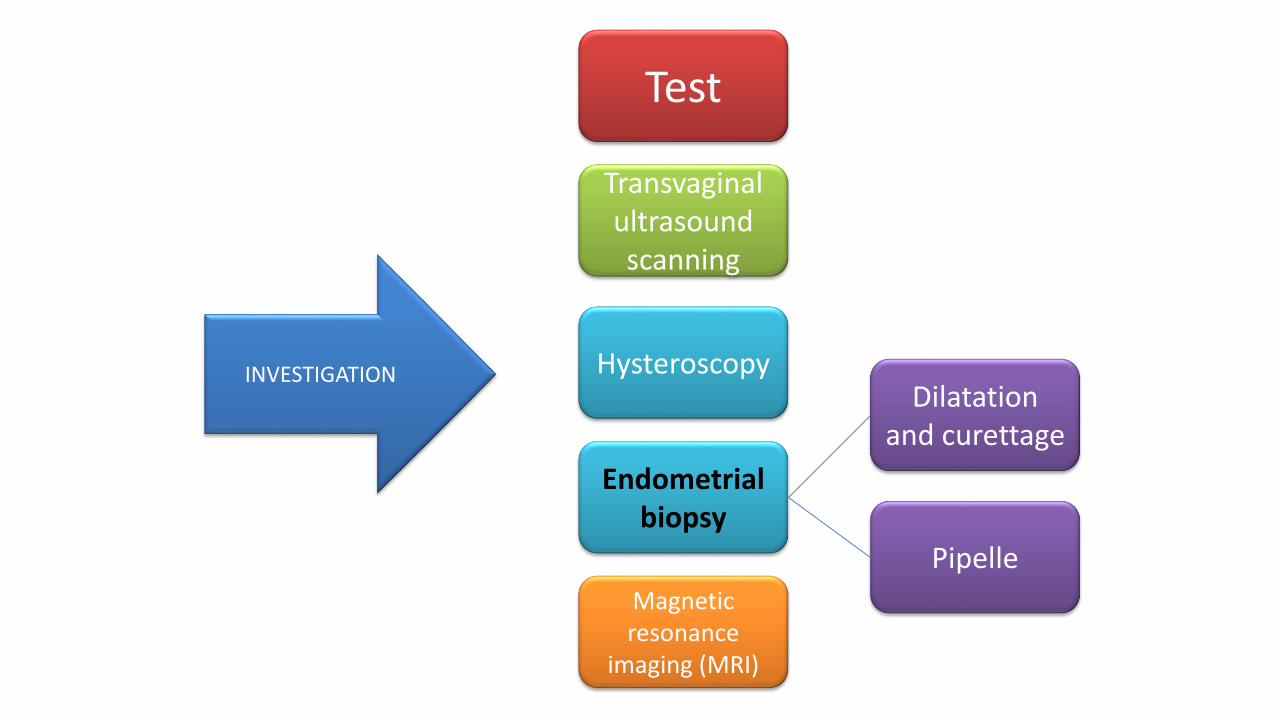
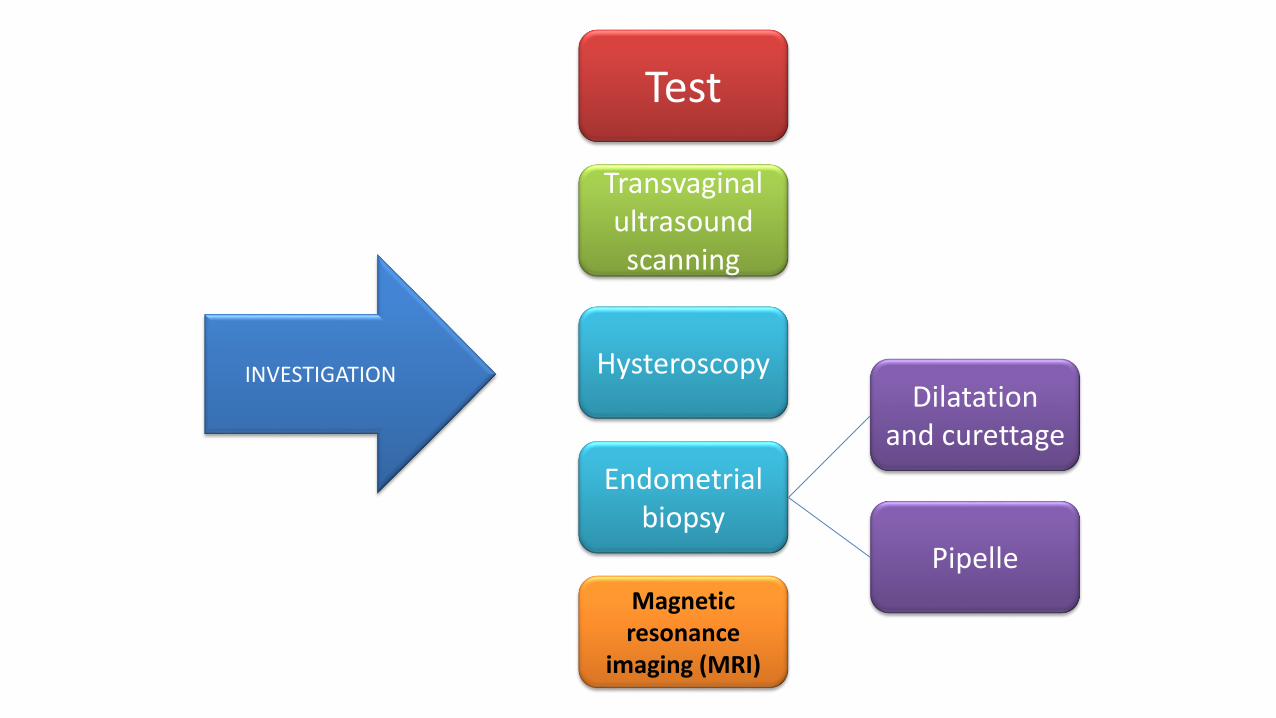
INVESTIGATIONS
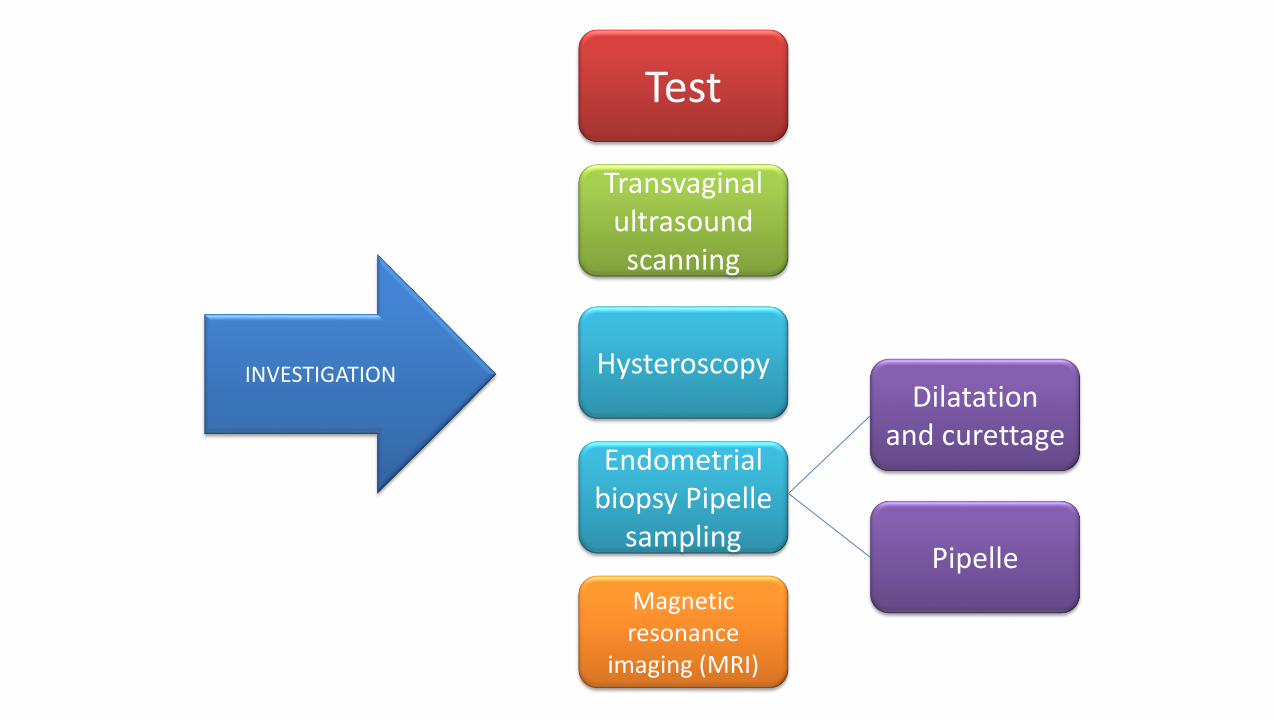
INVESTIGATION
Test
Transvaginalultrasound scanning
Dilatation and curettage
Hysteroscopy
Magnetic resonance
imaging (MRI)
Endometrial biopsy Pipelle
samplingPipelle
INVESTIGATION
Test
Transvaginalultrasound scanning
Dilatation and curettage
Hysteroscopy
Magnetic resonance
imaging (MRI)
Endometrial biopsy Pipelle
samplingPipelle
a) Liver function test - evidence of metastasis
b) Renal profile - ureteric obstruction / evidence
of metastasis
c) CA-125 tumour marker (advanced
endometrial cancer)
d) Chest X-ray – look for lung metastasize

INVESTIGATION
Test
Transvaginalultrasound scanning
Dilatation and
curettage
Hysteroscopy
Magnetic resonance
imaging (MRI)
Endometrial biopsy Pipelle
samplingPipelle
• Accurate assessment of endometrial thickness and of the ovaries
• Thickness of endometrium :< 4mm = cancer is very unlikely
> 4mm = require hysteroscopy and biopsy
• Women on tamoxifen (breast cancer) cannot be diagnosed by using TVUS due to thickened, irregular and cystic endometrium (distorted endometrial architecture)
prefer hysteroscopy and endometrial biopsy

INVESTIGATION
Test
Transvaginalultrasound scanning
Dilatation and curettage
Hysteroscopy
Magnetic resonance
imaging (MRI)
Endometrial biopsy Pipelle
samplingPipelle
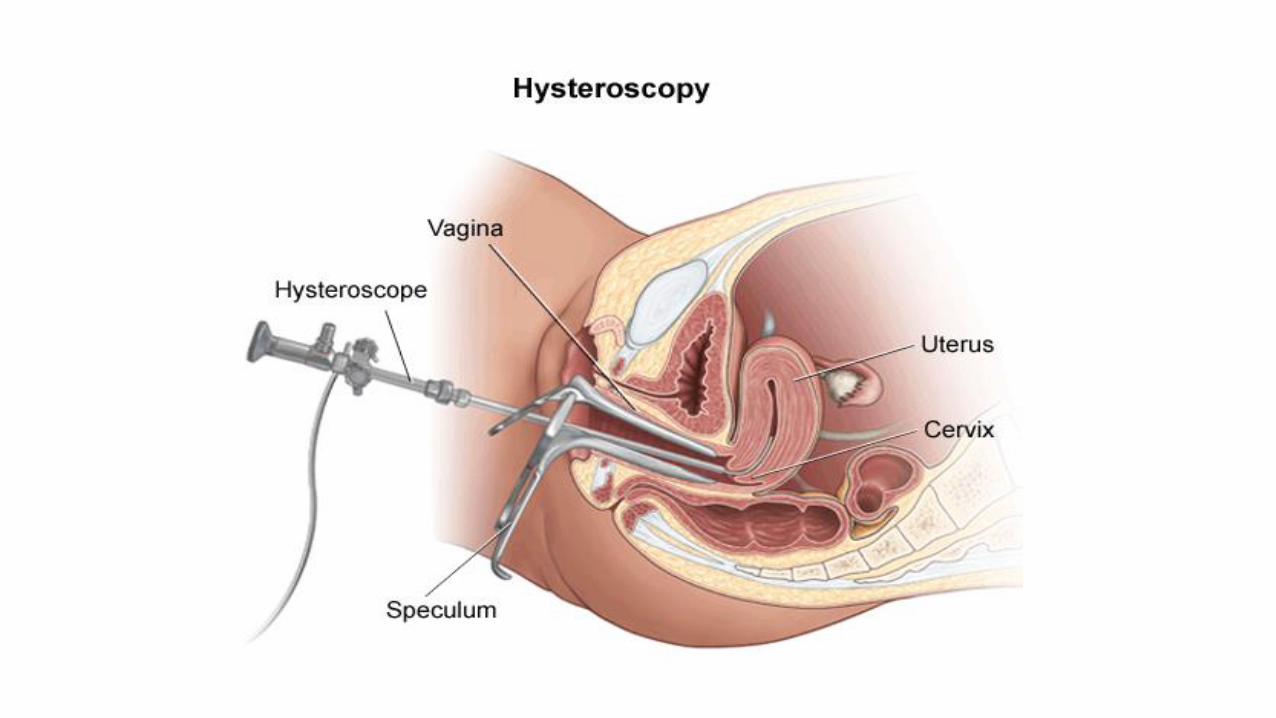
• Performed in the outpatient setting or inpatient under general anaesthetic
• Allow :Direct visualization of the whole endometriumDirected biopsy to be performed
• Indications: any abnormal bleeding from the uterus can be investigated
postmenopausal bleeding
irregular menstruation, intermenstrual bleeding, and postcoital bleeding
persistent menorrhagiapersistent discharge suspected uterine malformations suspected Asherman’s syndrom
INVESTIGATION
Test
Transvaginalultrasound scanning
Dilatation and curettage
Hysteroscopy
Magnetic resonance
imaging (MRI)
Endometrial biopsy
Pipelle
• Endometrial cancer can only be diagnosed by histological examination of a biopsy
• Done in women whose ultrasound scan reveals endometrial thickness of greater than 4 mm
• Performed using an endometrial sampler :
dilatation and curettage
Pipelle
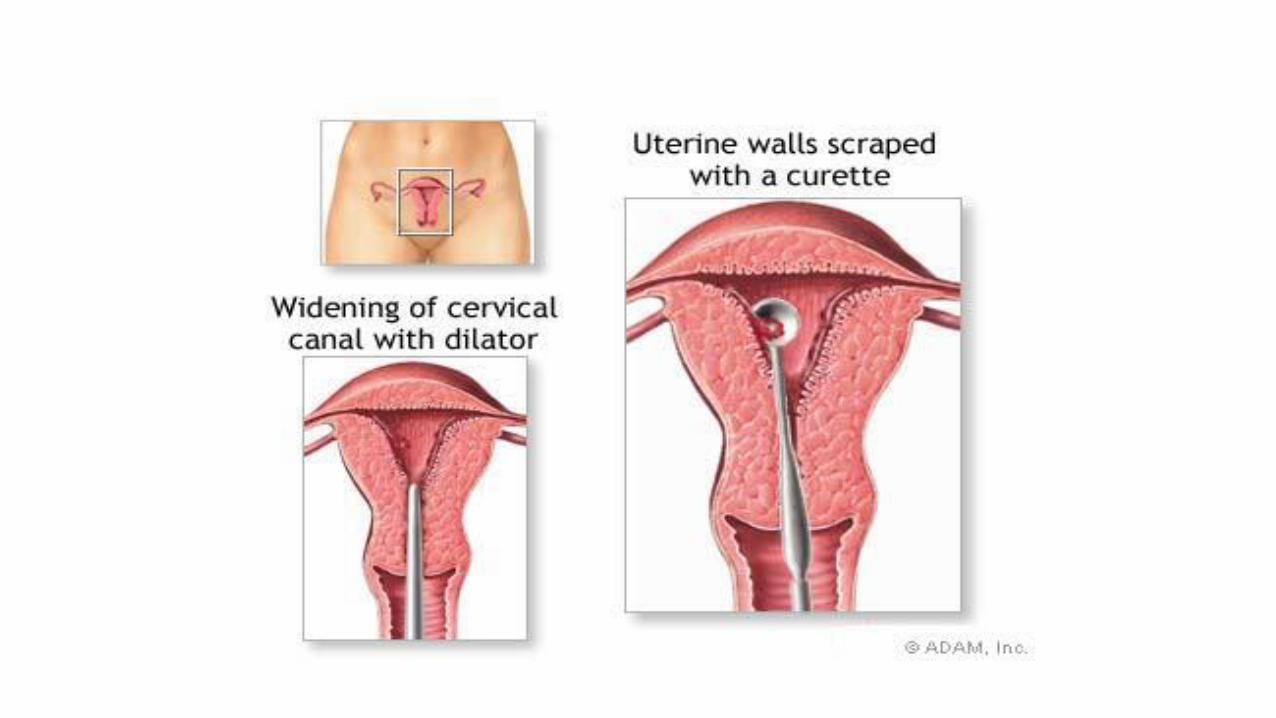
Dilatation and Curettage
• Can be done under general, spinal or local anesthesia
• May be done with hysteroscopy
• Risks include bleeding, perforation and infection and anesthesia complications.
• Perform a bimanual pelvic examination to assess the size and position of the uterus.
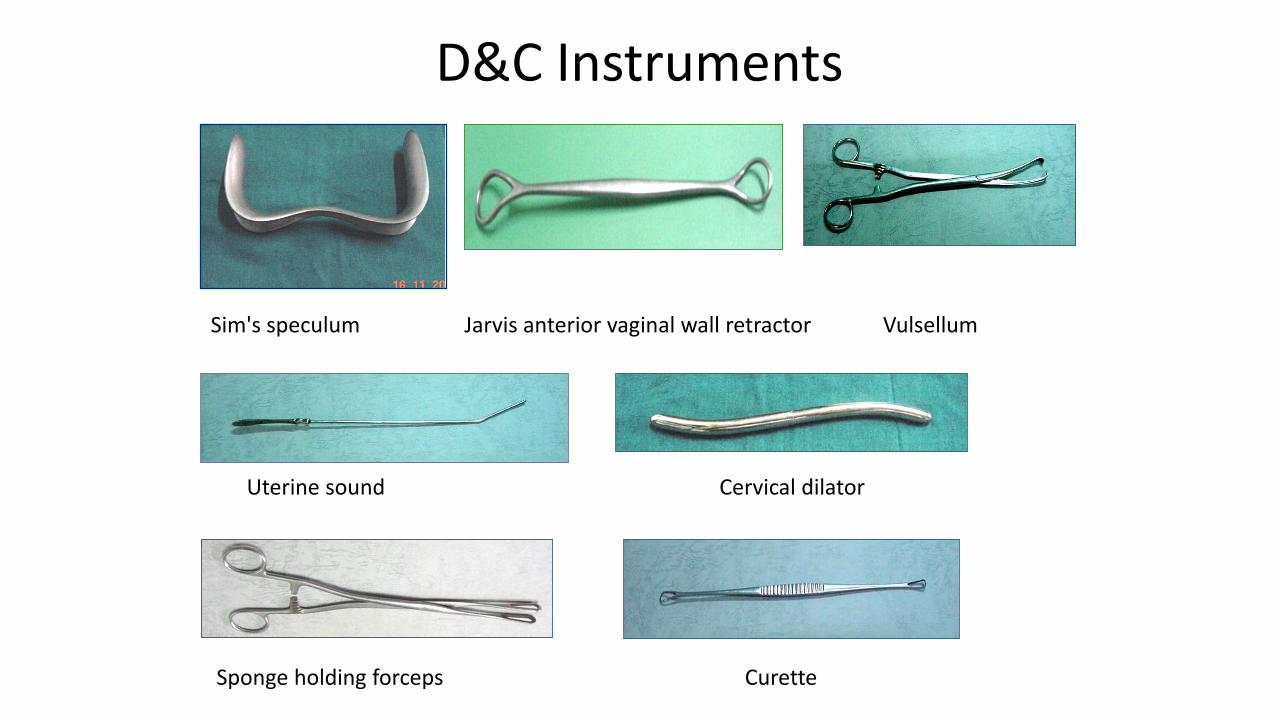
D&C Instruments
Sim's speculum Jarvis anterior vaginal wall retractor Vulsellum
Uterine sound Cervical dilator
Sponge holding forceps Curette
Dilatation and Curettage Procedure
• Explain the procedure to patient; benefits & complications
• Consent form
• Anaesthesia
• Lithotomy position
• Empty bladder & Sterile environment
Anterior vaginal wall is retracted with Jarvis anterior vaginalwall retractor
Gently grasp the anterior lip of the cervix with a vulsellum or single-toothed tenaculum
Gently pass a uterine sound through the cervix to assess the length
and direction of the uterus
Use graduated Hegar’s dilators. Begin with the smallest dilator
and end with the largest dilator that ensures adequate dilatation
(usually 10–12 mm)
Evacuate the contents of the uterus with a large curette. Scrape the
uterus until gritty sensation felt.
Send material for histopathological examination
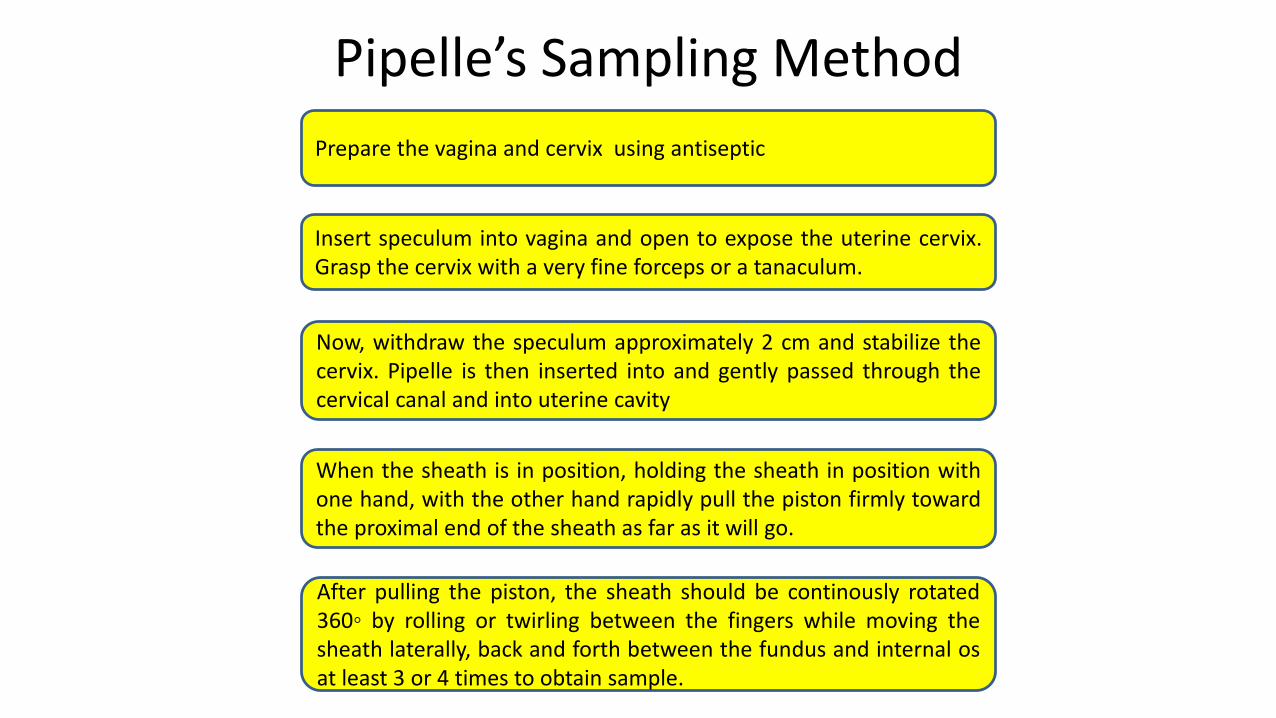
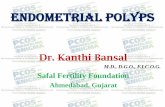
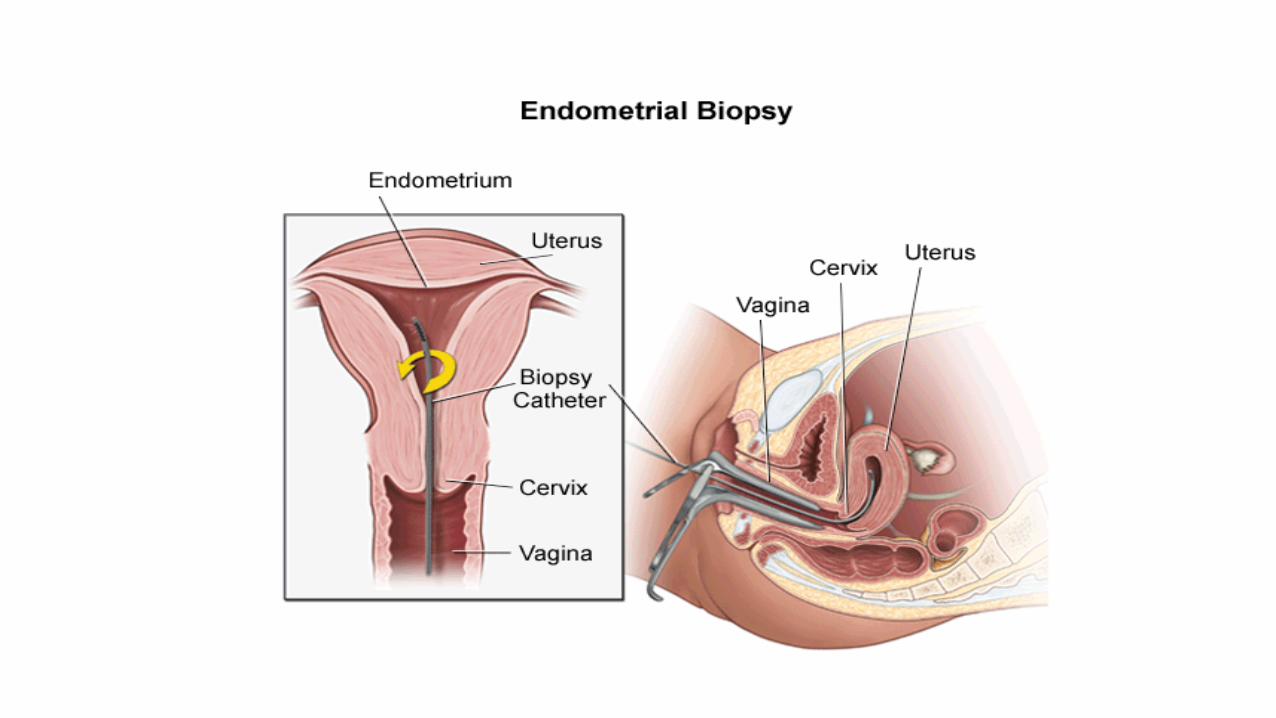
Pipelle’s Sampling Method
Prepare the vagina and cervix using antiseptic
Insert speculum into vagina and open to expose the uterine cervix.Grasp the cervix with a very fine forceps or a tanaculum.
Now, withdraw the speculum approximately 2 cm and stabilize thecervix. Pipelle is then inserted into and gently passed through thecervical canal and into uterine cavity
When the sheath is in position, holding the sheath in position withone hand, with the other hand rapidly pull the piston firmly towardthe proximal end of the sheath as far as it will go.
After pulling the piston, the sheath should be continously rotated360◦ by rolling or twirling between the fingers while moving thesheath laterally, back and forth between the fundus and internal osat least 3 or 4 times to obtain sample.
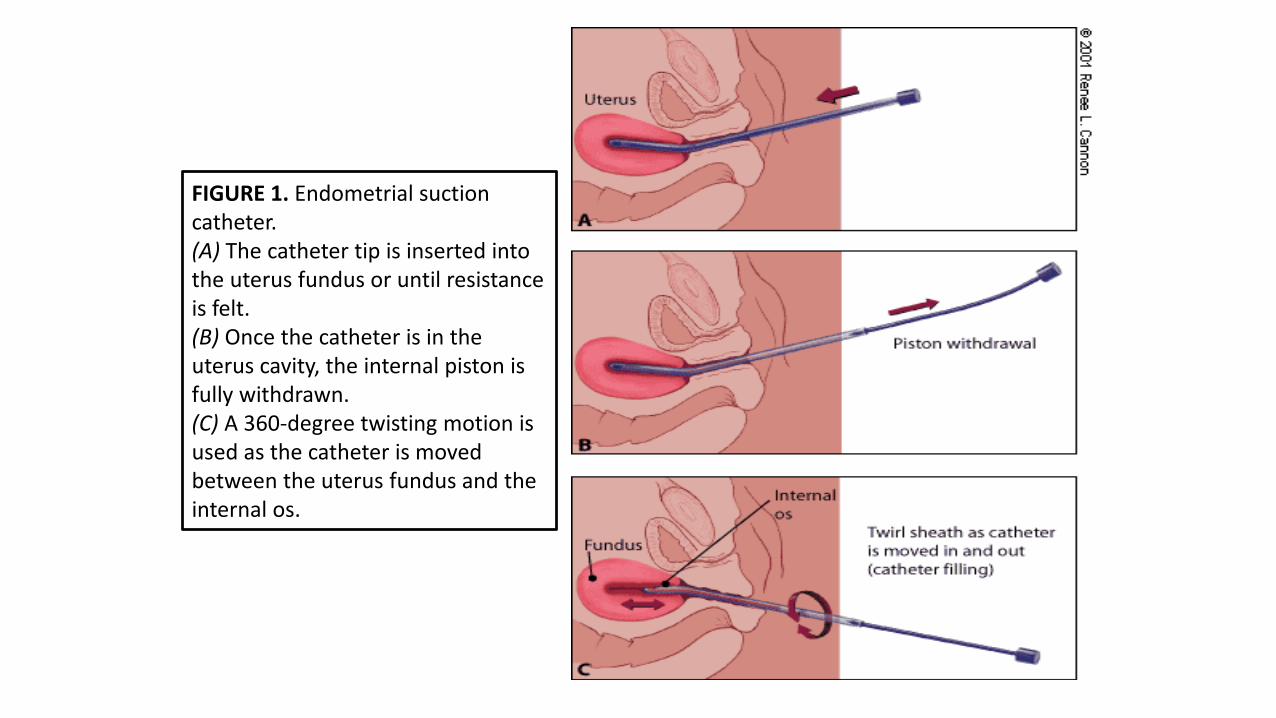
FIGURE 1. Endometrial suction catheter. (A) The catheter tip is inserted into the uterus fundus or until resistance is felt. (B) Once the catheter is in the uterus cavity, the internal piston is fully withdrawn. (C) A 360-degree twisting motion is used as the catheter is moved between the uterus fundus and the internal os.
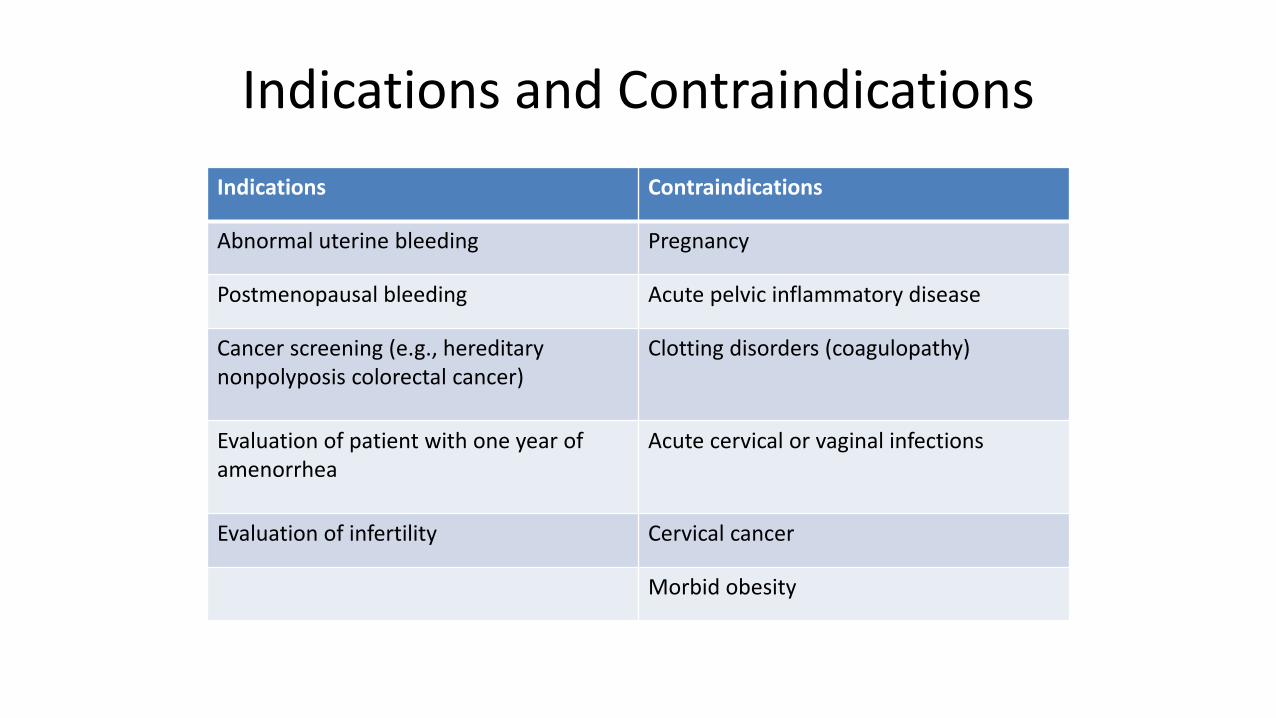
Indications and Contraindications
Indications Contraindications
Abnormal uterine bleeding Pregnancy
Postmenopausal bleeding Acute pelvic inflammatory disease
Cancer screening (e.g., hereditary nonpolyposis colorectal cancer)
Clotting disorders (coagulopathy)
Evaluation of patient with one year of amenorrhea
Acute cervical or vaginal infections
Evaluation of infertility Cervical cancer
Morbid obesity
Advantages
• Takes only a few minutes to perform
• Less bleeding
• Less pain
• Least expensive
• Not requiring hospitalisation, anaesthesia or cervical dilatation
• Low risk of perforation
• High degree of sensitivity and specificity for the detection of endometrial
Disadvantages
• Procedure being uncomfortable or even painful, especially in nulliparous women
• Miss focal lesions in the uterine cavity (polyp and sub mucous fibroid)
• Inadequate sampling may be obtained, particularly in post menopausal women
INVESTIGATION
Test
Transvaginalultrasound scanning
Dilatation and curettage
Hysteroscopy
Magnetic resonance
imaging (MRI)
Endometrial biopsy
Pipelle

• Function :
Give information regarding extent of disease (stage)
Decide on the type of surgical treatment offered to patient
Management
• Surgery
• Adjuvant treatment
Surgery
Extent of surgery depends on factors:Grade of disease
MRI stage
Patient’s comorbidities
Standard surgery:Total hysterectomy, bilateral sapingectomy
Performed abdominally OR laparoscopically
Pre-operative Evaluation1) Blood test
Full blood count
Postprandial sugar
Urea and electrolyte
Liver function test
Renal function test
2) Urine for protein,sugar and pus cells
3) ECG & Chest X-ray for cardiopulmonary assessement
4) Abdominal and pelvic ultrasonography for ascites, metastatic liver, para-aortic nodes
5) MRI/ CT imaging (optional)- to assess extrauterine spread of disease and degree of myometrium
Stage 1-confined to uterine body
Total abdominal hsyterectomy, bilateral salpingo-oopherectomy (TAHBSO)
Well differentiated/ Grade 1-2 tumour
Superficially invasive (Stage 1a)
Peritoneal saline washings for cytology
ADD Post-operative radiotherapy in:
Deeply invading tumour (Stage 1b)
Increase incidence of LN involvement
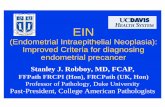
Stage 2-invade cervical stroma
Radical hysterectomy
Pelvic lymphadenoctomy + Para-aortic node sampling
Alternative: Local and external radiotherapy
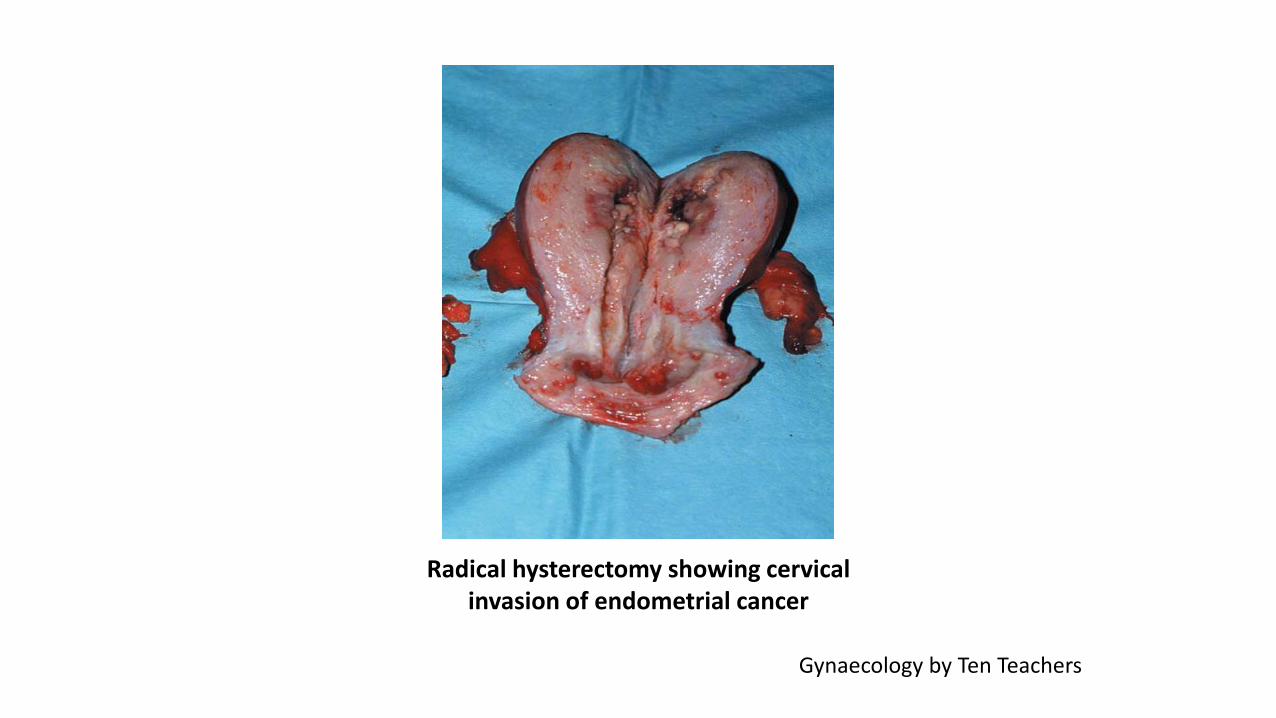
Radical hysterectomy showing cervical invasion of endometrial cancer
Gynaecology by Ten Teachers
Stage 3-Local and or regional spread of tumour
Radical hysterectomy
Pelvic lymphadenectomy
Para-aortic sampling
Omentectomy
Adjuvant Radiotherapy
Local radiotherapy to vaginal vault
high dose radiotherapy, HDR
External beam radiotherapy
Stage 4-Distant metastases
Debulking surgery
Adjuvant radiotherapy
Chemotherapy
Drugs commonly used: doxorubicin, cyclophosphamide, cisplatin
Others: adriamycin, carboplatin, 5-fluorouracil
Hormonal therapy
Adjuvant progestogen therapy
Adjuvant treatment
• Postoperative radiotherapy
Aim: to reduce local recurrence rate
• Chemotherapy
Aim: to combat risk of distant spread of cancer
• Indications for primary radiotherapy:
Women unfit for surgery
Women with significant medical comorbidities
Surgically inoperable disease
Those with higher risk recurrence
Patients with advanced disease for palliation therapy
• Containdications of radiotherapy:
Presence of pelvic mass
Pelvic abscessPrevious
laparotomy
Adhesions with bowel
Prior pelvic radiation

Prognosis
Overall 5 year survival rate: 80% depends on:
Age
Staging
Grading
Tumour type
Risk factor
Myometrium invasion
LN involvement
Prognosis
Adverse prognostic features for survival include:
Advanced age >70 years
High BMI
Grade 3 tumours
Papillary serous or clear cell histology
Lymphovascular space involvement
Nodal metastases
Distant metastases
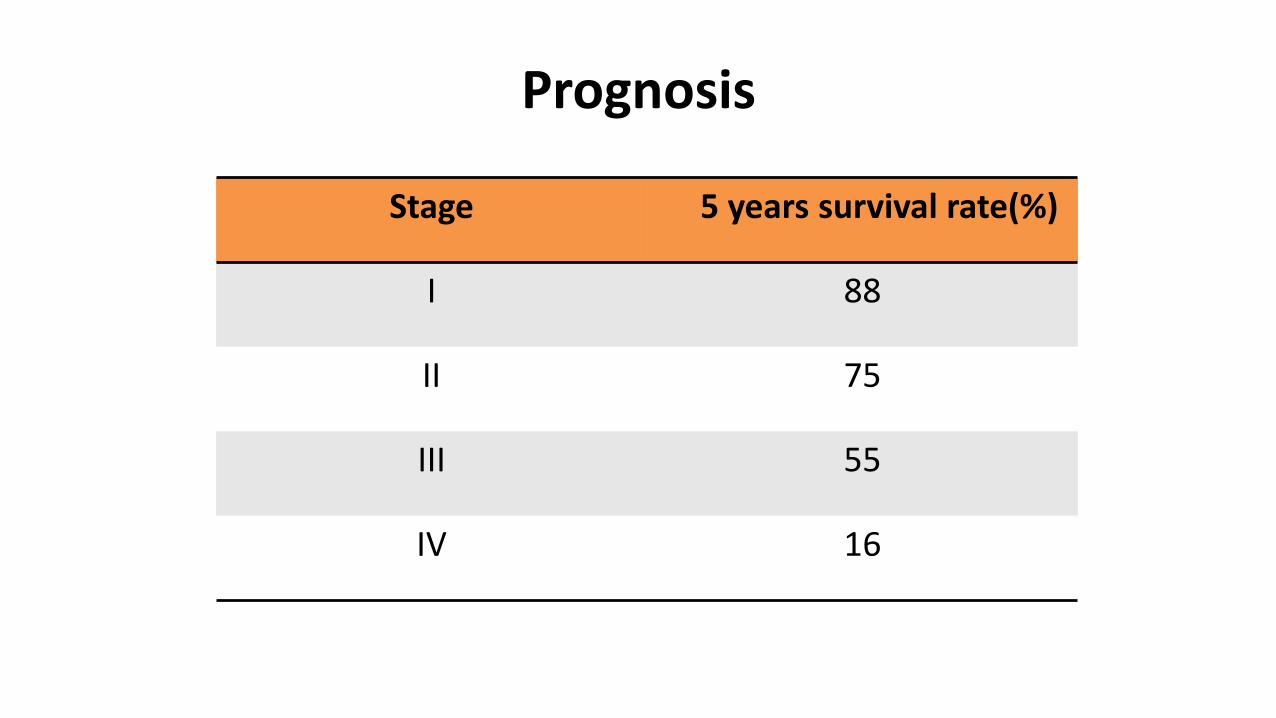
Prognosis
Stage 5 years survival rate(%)
I 88
II 75
III 55
IV 16