EMERGENCY EVALUATION - Greenville Health System Evaluation of the Acute...EMS Stroke Screening EMS...
16
EMERGENCY EVALUATION OF THE ACUTE STROKE PATIENT Angel Rochester, MD Associate Director of Critical Care & Trauma Associate Director of Chest Pain
Transcript of EMERGENCY EVALUATION - Greenville Health System Evaluation of the Acute...EMS Stroke Screening EMS...
EMERGENCY EVALUATION OF THE
ACUTE STROKE PATIENT
Angel Rochester, MD Associate Director of Critical Care &
Trauma Associate Director of Chest Pain
Greenville County EMS
800 Square Miles in Greenville County Busiest EMS organization in South
Carolina 62,000 Annual Responses Over 500 Stroke transports per year Strong relationship with County Hospitals Involvement in Hospital meetings
EMS Stroke Screening
EMS Dispatchers perform a pre-arrival stroke screen over the phone
EMS Providers conduct a Cincinnati Stroke Scale upon arrival
NIH Stroke Scale Pre-hospital Stroke Thrombolytic Check
List
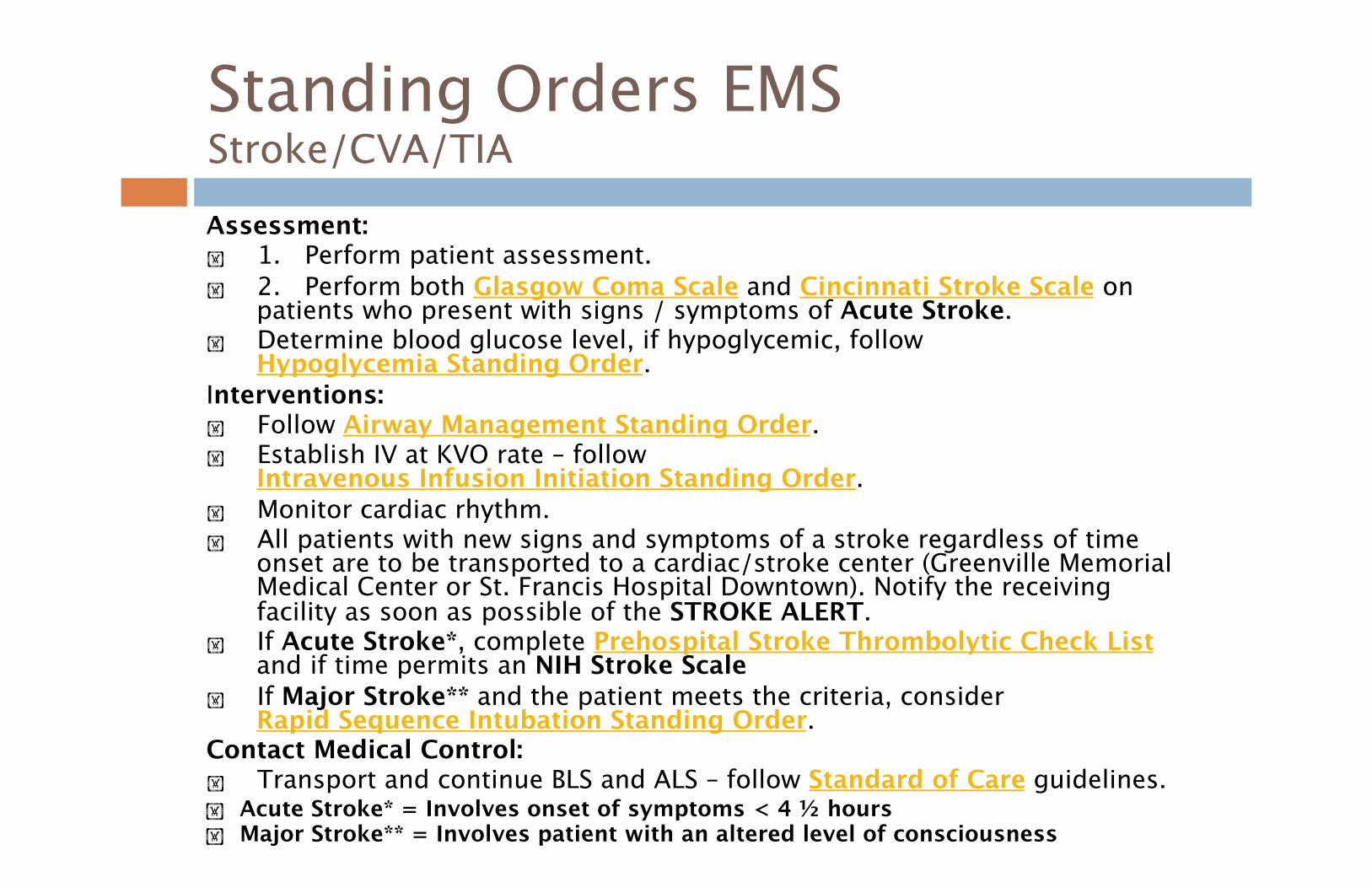
Standing Orders EMSStroke/CVA/TIA Assessment: 1. Perform patient assessment. 2. Perform both Glasgow Coma Scale and Cincinnati Stroke Scale on
patients who present with signs / symptoms of Acute Stroke. Determine blood glucose level, if hypoglycemic, follow
Hypoglycemia Standing Order. Interventions: Follow Airway Management Standing Order. Establish IV at KVO rate – follow
Intravenous Infusion Initiation Standing Order. Monitor cardiac rhythm. All patients with new signs and symptoms of a stroke regardless of time
onset are to be transported to a cardiac/stroke center (Greenville Memorial Medical Center or St. Francis Hospital Downtown). Notify the receiving facility as soon as possible of the STROKE ALERT.
If Acute Stroke*, complete Prehospital Stroke Thrombolytic Check List and if time permits an NIH Stroke Scale
If Major Stroke** and the patient meets the criteria, consider Rapid Sequence Intubation Standing Order.
Contact Medical Control: Transport and continue BLS and ALS – follow Standard of Care guidelines. Acute Stroke* = Involves onset of symptoms < 4 ½ hours Major Stroke** = Involves patient with an altered level of consciousness
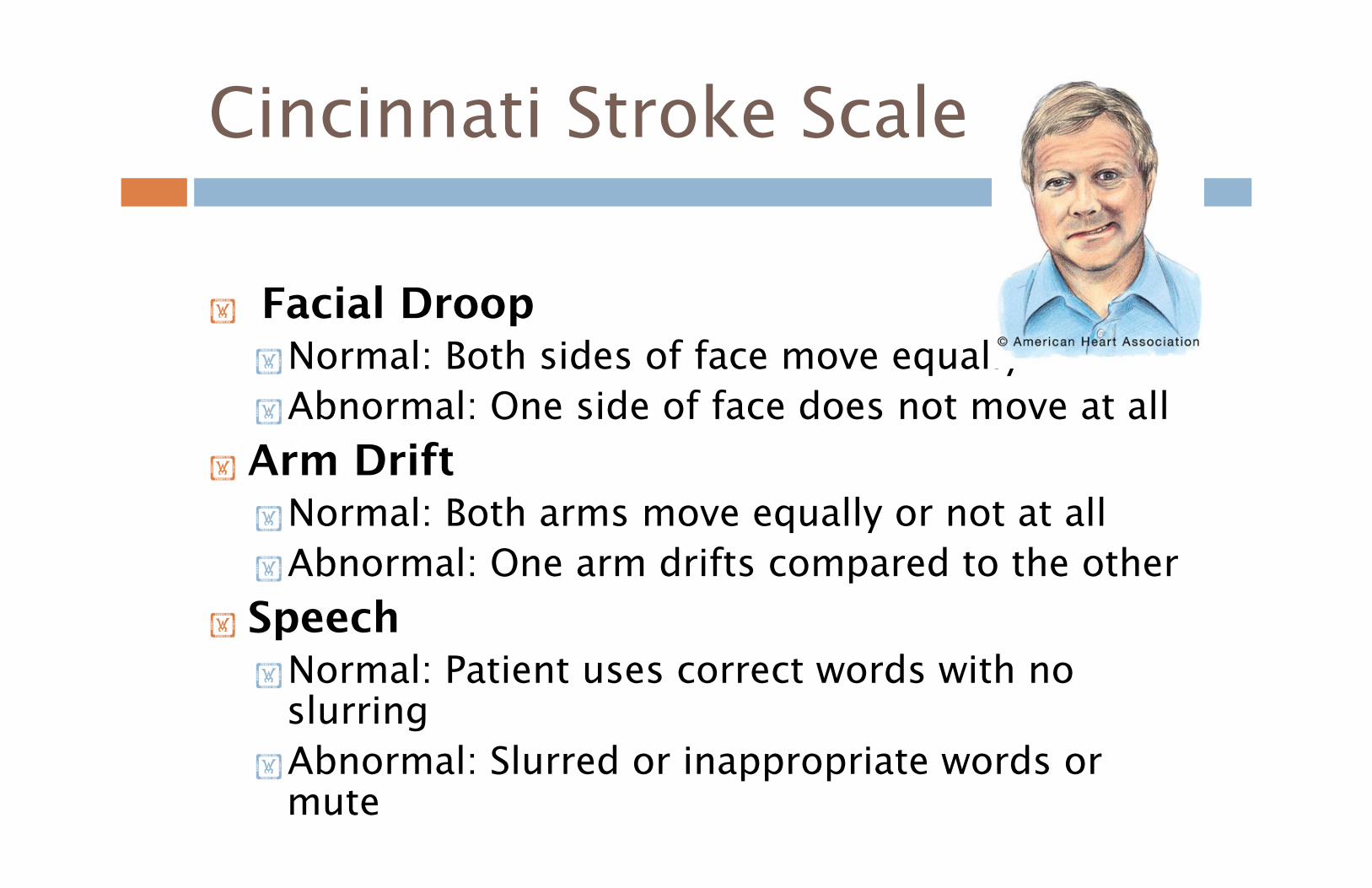
Cincinnati Stroke Scale
Facial Droop Normal: Both sides of face move equally Abnormal: One side of face does not move at all
Arm Drift Normal: Both arms move equally or not at all Abnormal: One arm drifts compared to the other
Speech Normal: Patient uses correct words with no
slurring Abnormal: Slurred or inappropriate words or
mute
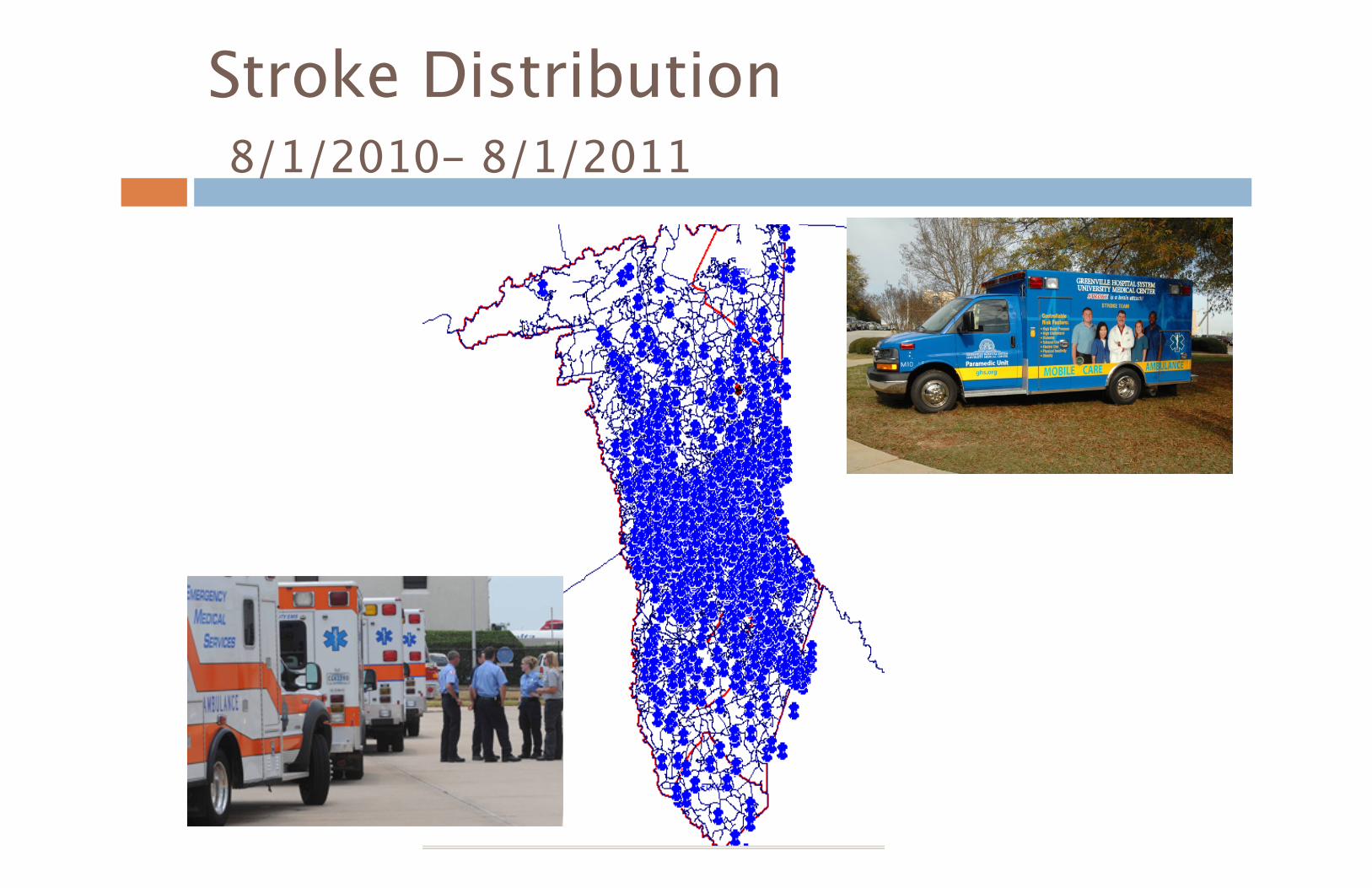
Stroke Distribution 8/1/2010- 8/1/2011
GHS Referral Line Transfers
GHS Satellites have a dedicated onsite STEMI/Stroke stretcher and Activation Line
GCEMS has an ambulance stationed at Hillcrest and Greer
Mobile Care Reach® Access to surrounding counties
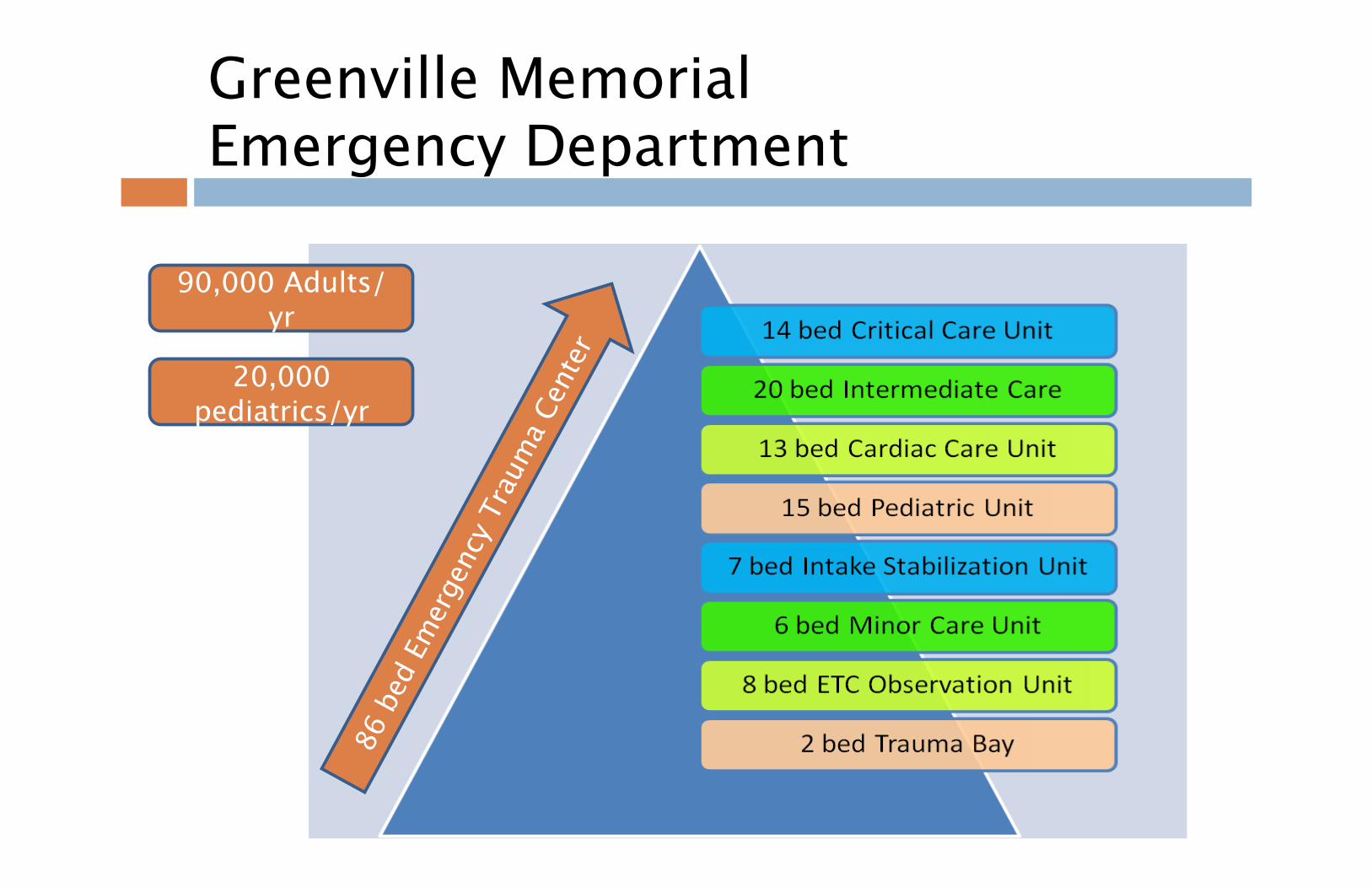
Greenville MemorialEmergency Department
90,000 Adults/yr
20,000 pediatrics/yr
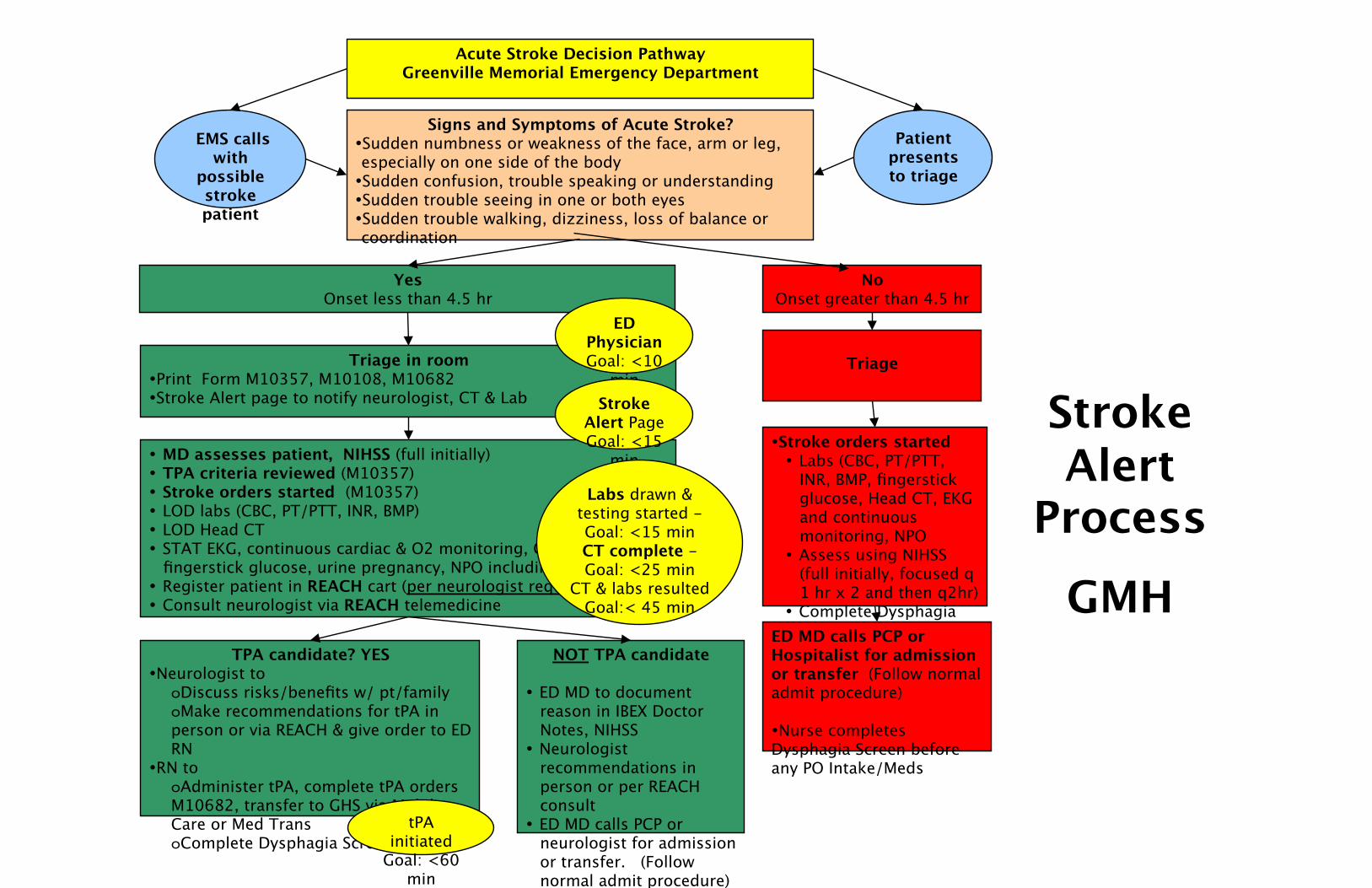
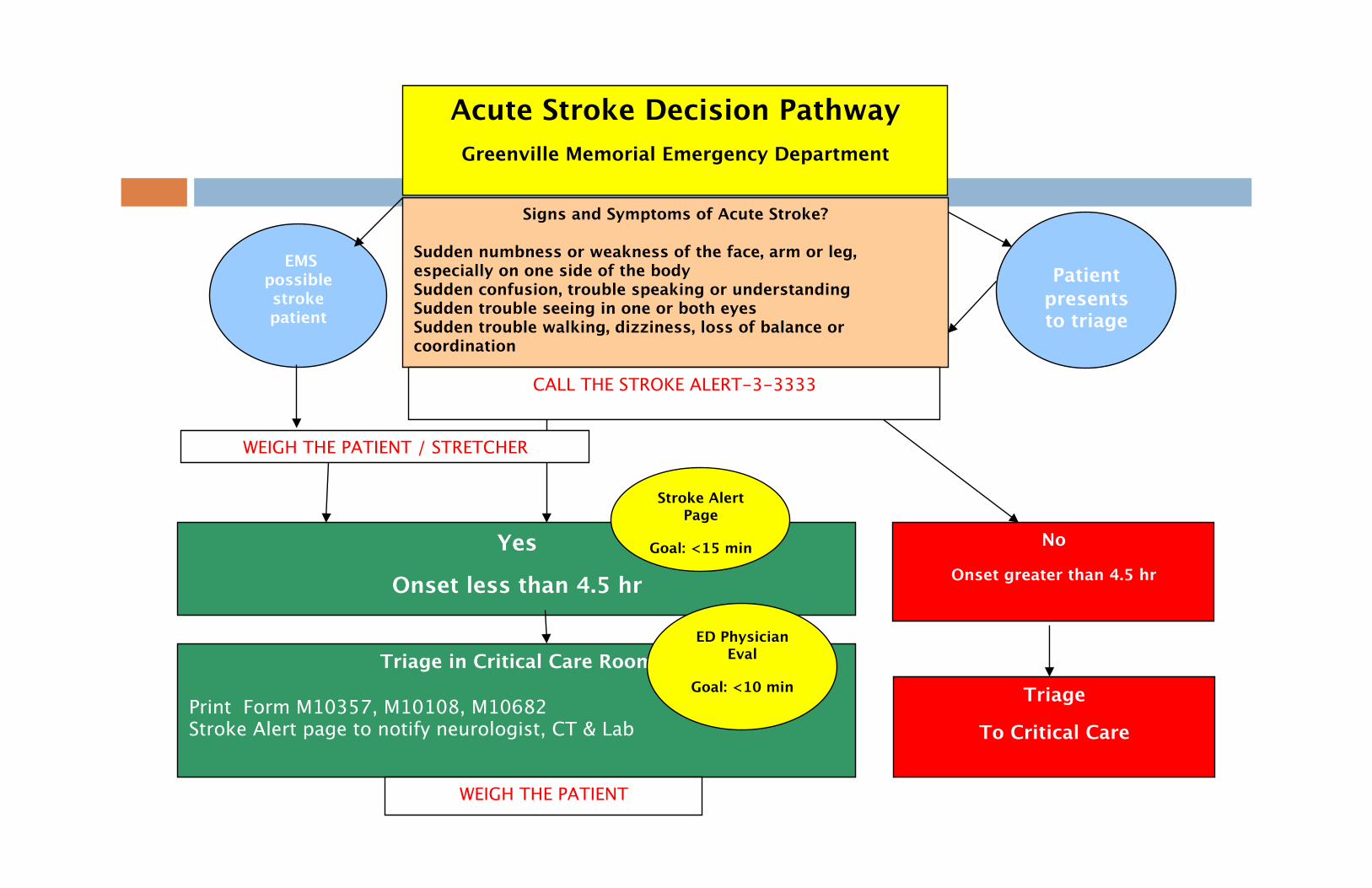
Acute Stroke Decision Pathway Greenville Memorial Emergency Department
Signs and Symptoms of Acute Stroke? • Sudden numbness or weakness of the face, arm or leg, especially on one side of the body • Sudden confusion, trouble speaking or understanding • Sudden trouble seeing in one or both eyes • Sudden trouble walking, dizziness, loss of balance or coordination
Yes Onset less than 4.5 hr
Triage in room • Print Form M10357, M10108, M10682 • Stroke Alert page to notify neurologist, CT & Lab
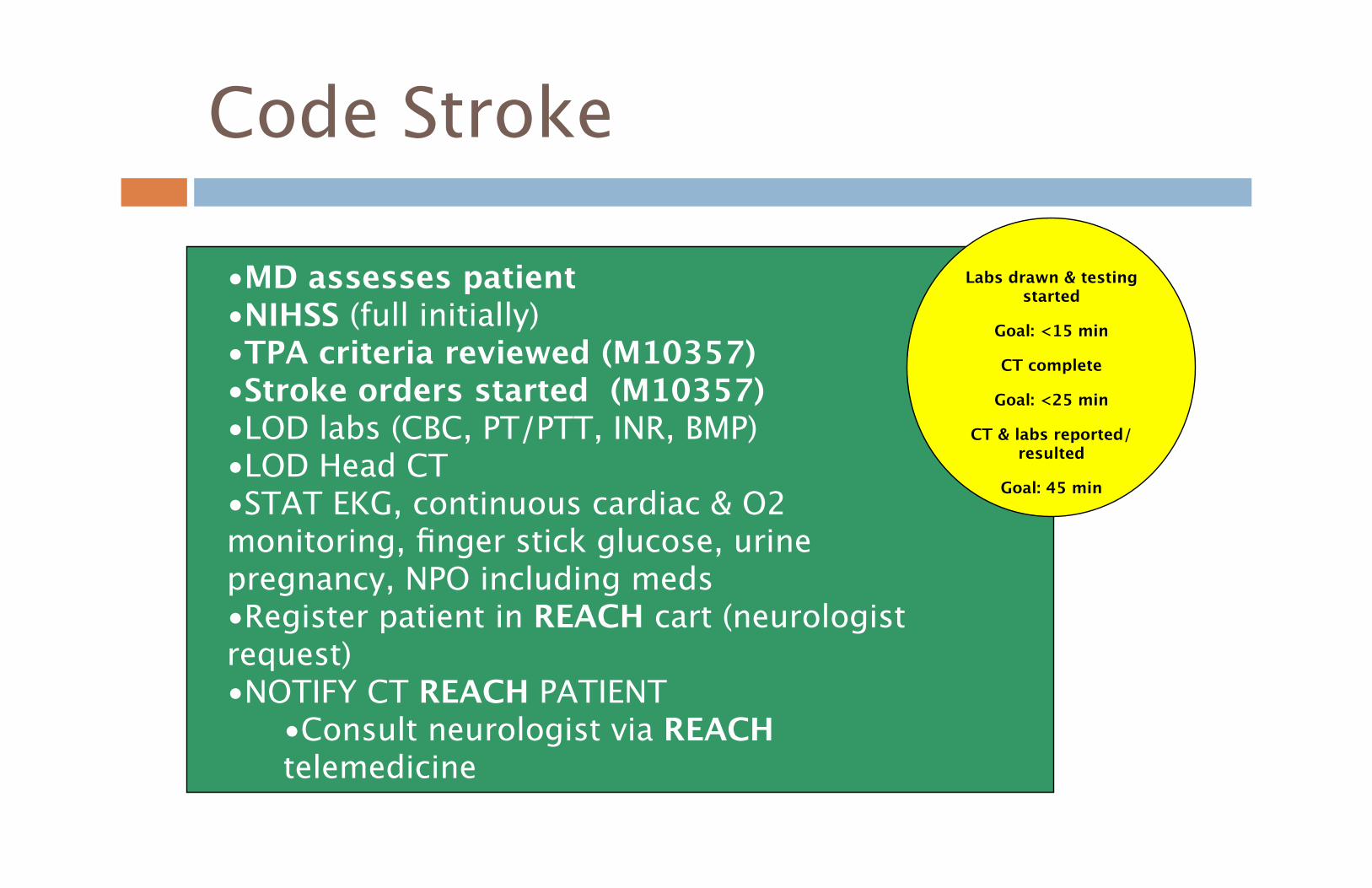
• MD assesses patient, NIHSS (full initially) • TPA criteria reviewed (M10357) • Stroke orders started (M10357) • LOD labs (CBC, PT/PTT, INR, BMP) • LOD Head CT • STAT EKG, continuous cardiac & O2 monitoring, CXR,
fingerstick glucose, urine pregnancy, NPO including meds • Register patient in REACH cart (per neurologist request) • Consult neurologist via REACH telemedicine
TPA candidate? YES • Neurologist to
o Discuss risks/benefits w/ pt/family o Make recommendations for tPA in person or via REACH & give order to ED RN
• RN to o Administer tPA, complete tPA orders M10682, transfer to GHS via Mobile Care or Med Trans o Complete Dysphagia Screening
NOT TPA candidate
• ED MD to document reason in IBEX Doctor Notes, NIHSS
• Neurologist recommendations in person or per REACH consult
• ED MD calls PCP or neurologist for admission or transfer. (Follow normal admit procedure)
No Onset greater than 4.5 hr
Triage
• Stroke orders started • Labs (CBC, PT/PTT,
INR, BMP, fingerstick glucose, Head CT, EKG and continuous monitoring, NPO
• Assess using NIHSS (full initially, focused q 1 hr x 2 and then q2hr)
• Complete Dysphagia Screen ED MD calls PCP or
Hospitalist for admission or transfer (Follow normal admit procedure)
• Nurse completes Dysphagia Screen before any PO Intake/Meds
Patient presents to triage
EMS calls with
possible stroke patient
ED Physician Goal: <10
min Stroke
Alert Page Goal: <15
min
Labs drawn & testing started - Goal: <15 min CT complete - Goal: <25 min
CT & labs resulted Goal:< 45 min
tPA initiated
Goal: <60 min
Stroke Alert
Process GMH
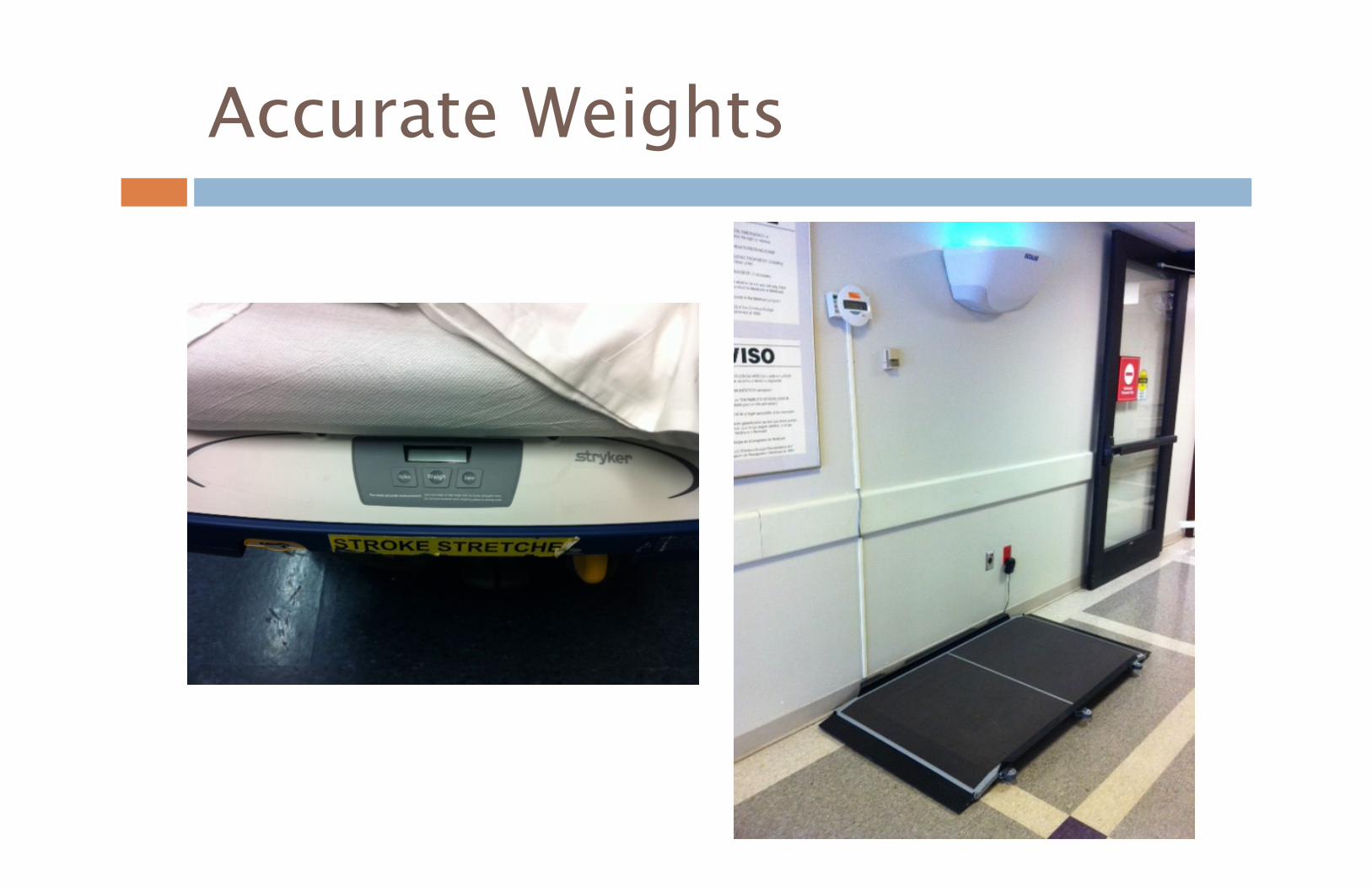
Accurate Weights
Acute Stroke Decision Pathway Greenville Memorial Emergency Department
Signs and Symptoms of Acute Stroke?
Sudden numbness or weakness of the face, arm or leg, especially on one side of the body Sudden confusion, trouble speaking or understanding Sudden trouble seeing in one or both eyes Sudden trouble walking, dizziness, loss of balance or coordination
Patient presents to triage
EMS possible stroke patient
Yes
Onset less than 4.5 hr
No
Onset greater than 4.5 hr
Triage in Critical Care Room
Print Form M10357, M10108, M10682 Stroke Alert page to notify neurologist, CT & Lab
ED Physician Eval
Goal: <10 min Triage
To Critical Care
Stroke Alert Page
Goal: <15 min
WEIGH THE PATIENT
CALL THE STROKE ALERT-3-3333
WEIGH THE PATIENT / STRETCHER
Labs drawn & testing started
Goal: <15 min
CT complete
Goal: <25 min
CT & labs reported/resulted
Goal: 45 min
• MD assesses patient • NIHSS (full initially) • TPA criteria reviewed (M10357) • Stroke orders started (M10357) • LOD labs (CBC, PT/PTT, INR, BMP) • LOD Head CT • STAT EKG, continuous cardiac & O2 monitoring, finger stick glucose, urine pregnancy, NPO including meds • Register patient in REACH cart (neurologist request) • NOTIFY CT REACH PATIENT
• Consult neurologist via REACH telemedicine
Code Stroke
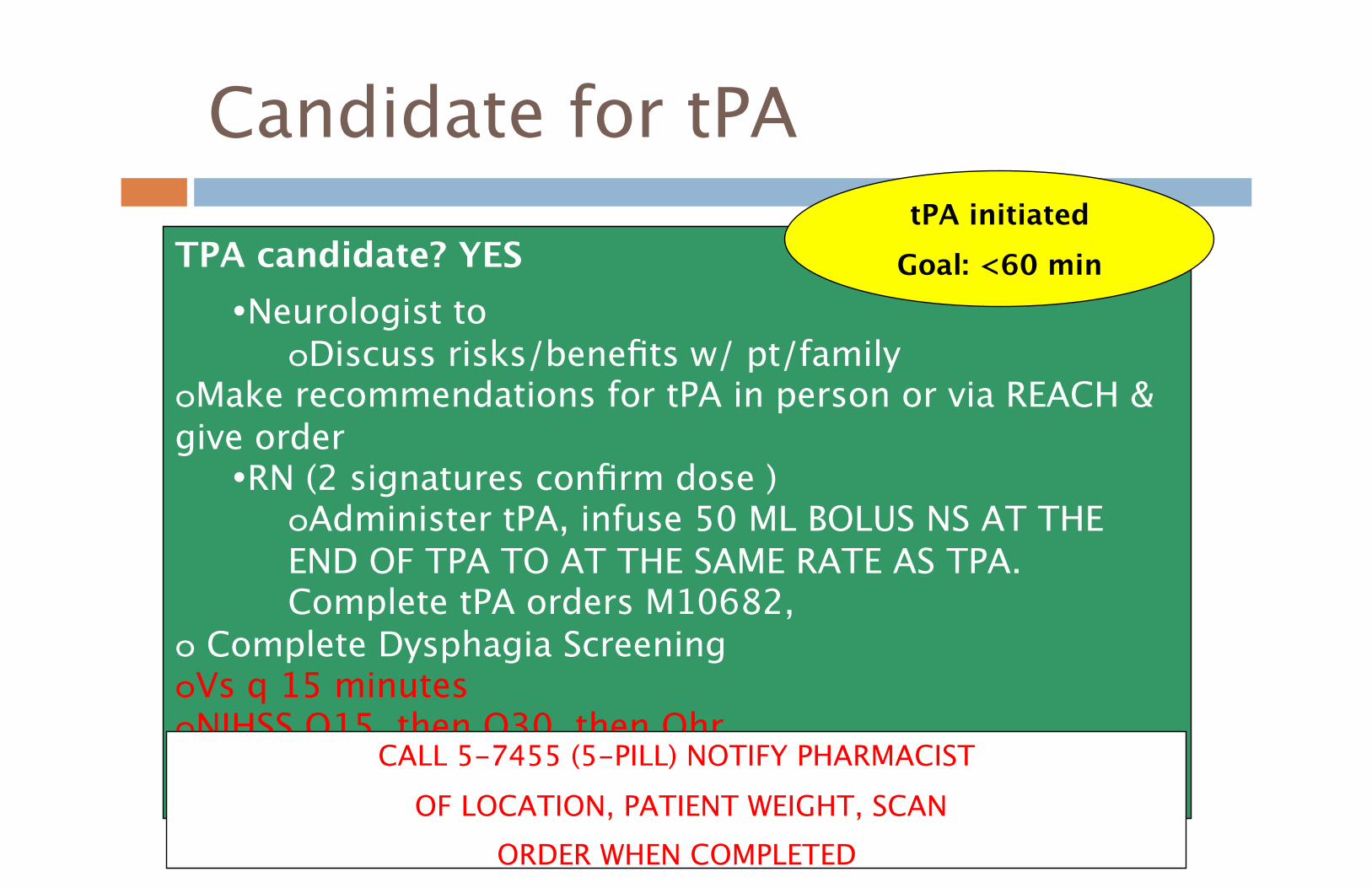
Candidate for tPA
TPA candidate? YES • Neurologist to
o Discuss risks/benefits w/ pt/family o Make recommendations for tPA in person or via REACH & give order
• RN (2 signatures confirm dose ) o Administer tPA, infuse 50 ML BOLUS NS AT THE END OF TPA TO AT THE SAME RATE AS TPA. Complete tPA orders M10682,
o Complete Dysphagia Screening o Vs q 15 minutes o NIHSS Q15, then Q30, then Qhr
tPA initiated Goal: <60 min
CALL 5-7455 (5-PILL) NOTIFY PHARMACIST OF LOCATION, PATIENT WEIGHT, SCAN
ORDER WHEN COMPLETED
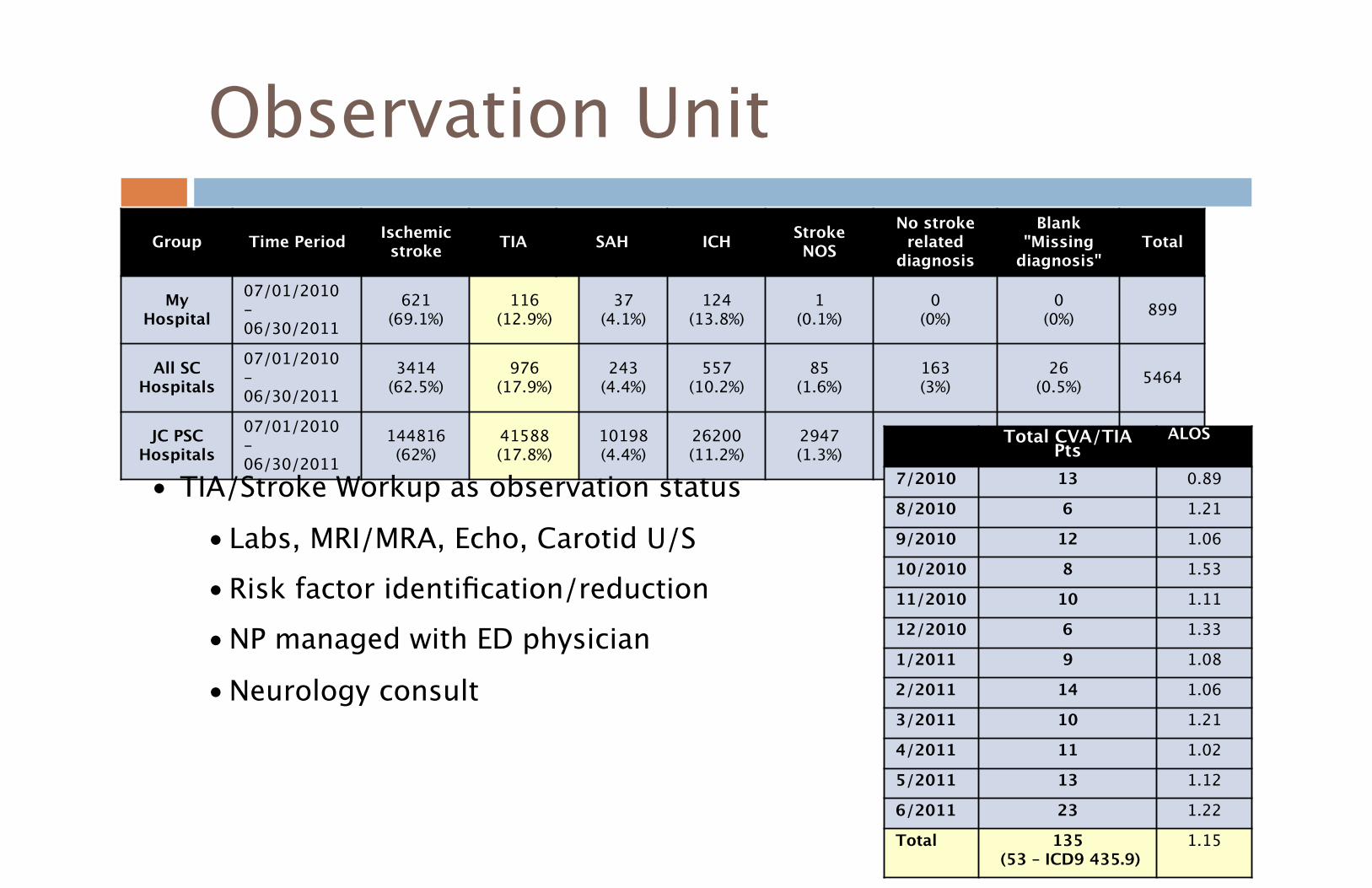
Observation Unit Group Time Period Ischemic
stroke TIA SAH ICH Stroke NOS
No stroke related
diagnosis
Blank "Missing
diagnosis" Total
My Hospital
07/01/2010 - 06/30/2011
621 (69.1%)
116 (12.9%)
37 (4.1%)
124 (13.8%)
1 (0.1%)
0 (0%)
0 (0%) 899
All SC Hospitals
07/01/2010 - 06/30/2011
3414 (62.5%)
976 (17.9%)
243 (4.4%)
557 (10.2%)
85 (1.6%)
163 (3%)
26 (0.5%) 5464
JC PSC Hospitals
07/01/2010 - 06/30/2011
144816 (62%)
41588 (17.8%)
10198 (4.4%)
26200 (11.2%)
2947 (1.3%)
5159 (2.2%)
2770 (1.2%) 233678 Total CVA/TIA
Pts ALOS
7/2010 13 0.89 8/2010 6 1.21 9/2010 12 1.06 10/2010 8 1.53 11/2010 10 1.11 12/2010 6 1.33 1/2011 9 1.08 2/2011 14 1.06 3/2011 10 1.21 4/2011 11 1.02 5/2011 13 1.12 6/2011 23 1.22 Total 135
(53 – ICD9 435.9) 1.15
• TIA/Stroke Workup as observation status • Labs, MRI/MRA, Echo, Carotid U/S • Risk factor identification/reduction • NP managed with ED physician
• Neurology consult
Observation Unit
• TIA/Stroke Workup as observation status • Labs, MRI/MRA, Echo, Carotid U/S • Risk factor identification/reduction • Neurology Consult • NP managed with EM Physician • Work up completed in 24-48 hours, 365 days
Questions?
Thank You