EMS Stroke Conference Session Outline OHSU June … OHSU stroke...Common Hazards to Health Care...
10
1 Reproduced with permission from HumanFit, LLC © 2014. Reproduced with permission from HumanFit, LLC © 2014. EMS Stroke Conference OHSU June 2014 Safe Patient Mobilization Presented by Lynda Enos, RN, BSN, MS, COHN-S, CPE Ergonomics Consultant, HumanFit, LLC. Tel: 503-655-3308 Email: [email protected] Session Outline The Safe Patient Mobilization Program at OHSU Health Care Safety, Work Environment and Culture - Current perspective Why is Manual Patient Handling so Hazardous? Effective Safe Patient Mobilization/Handling Programs for EMS: Reducing the Risk for Musculoskeletal Disorders Low tech equipment demonstration during lunch 2 Equipment brand names, manufacturers or vendors seen in this webinar do not constitute endorsement of the device, equipment, product or service by HumanFit, LLC. Reproduced with permission from HumanFit, LLC © 2014. 3 Find Resources at www.hcergo.org www.orosha.org/grants/ff_ergo/index.html www.cdc.gov/niosh/topics/ems/pubsPatientHandling.html Reproduced with permission from HumanFit, LLC © 2014. 4 www. regonline.com/hcergo14 Reproduced with permission from HumanFit, LLC © 2014. 5 Late 1990s – 2009: A Lift Team approach was used to try and prevent back injuries to health care staff Pre Program Injury Data - Jan 2008-Dec 2011 45-60% of all cases appear to be related to patient lifting and moving activities. 65-80% of all lost time cases were related to patient mobilization cases Average days away from work (lost time) per patient mobilization claim = 3-16 days 65-85% of all workers’ compensation costs are attributed to patient mobilization activities OHSU Safe Patient Mobilization Program (SPM) Reproduced with permission from HumanFit, LLC © 2014. 6 The OHSU SPM Program ‘Create a Culture of Safe Patient Mobilization while Enhancing Health Care Provider and Patient Safety’ 2010 Interdisciplinary team formed including front line staff Business plan for the SPM program was written Staff trialed various patient handling and lift equipment 2011 2 pilot units implemented the SPM program: 10 K and & 7 Neuro ICU SPM Program Vision Statement
Transcript of EMS Stroke Conference Session Outline OHSU June … OHSU stroke...Common Hazards to Health Care...

1 Reproduced with permission from HumanFit, LLC © 2014.
Reproduced with permission from HumanFit, LLC © 2014.
EMS Stroke Conference
OHSU June 2014
Safe Patient Mobilization
Presented by Lynda Enos, RN, BSN, MS, COHN-S, CPE
Ergonomics Consultant, HumanFit, LLC.
Tel: 503-655-3308
Email: [email protected]
Reproduced with permission from HumanFit, LLC © 2014.
Session Outline
The Safe Patient Mobilization Program at OHSU
Health Care Safety, Work Environment and Culture -
Current perspective
Why is Manual Patient Handling so Hazardous?
Effective Safe Patient Mobilization/Handling Programs
for EMS: Reducing the Risk for Musculoskeletal
Disorders
Low tech equipment demonstration during lunch
2
Equipment brand names, manufacturers or vendors seen in this webinar do not constitute endorsement of the device, equipment, product or service by HumanFit, LLC.
Reproduced with permission from HumanFit, LLC © 2014.
3
Find Resources at
www.hcergo.org
www.orosha.org/grants/ff_ergo/index.html
www.cdc.gov/niosh/topics/ems/pubsPatientHandling.html
Reproduced with permission from HumanFit, LLC © 2014.
4
www. regonline.com/hcergo14
Reproduced with permission from HumanFit, LLC © 2014.
5
Late 1990s – 2009: A Lift Team approach was used to try and prevent back injuries to health care staff
Pre Program Injury Data - Jan 2008-Dec 2011
45-60% of all cases appear to be related to patient lifting and moving activities.
65-80% of all lost time cases were related to patient mobilization cases
Average days away from work (lost time) per patient mobilization claim = 3-16 days
65-85% of all workers’ compensation costs are attributed to patient mobilization activities
OHSU
Safe Patient Mobilization Program (SPM)
Reproduced with permission from HumanFit, LLC © 2014.
6
The OHSU SPM Program
‘Create a Culture of Safe Patient Mobilization
while Enhancing Health Care Provider and
Patient Safety’
2010
Interdisciplinary team formed including front line staff
Business plan for the SPM program was written
Staff trialed various patient handling and lift equipment
2011
2 pilot units implemented the SPM program: 10 K and
& 7 Neuro ICU
SPM Program Vision Statement
2 Reproduced with permission from HumanFit, LLC © 2014.
Reproduced with permission from HumanFit, LLC © 2014.
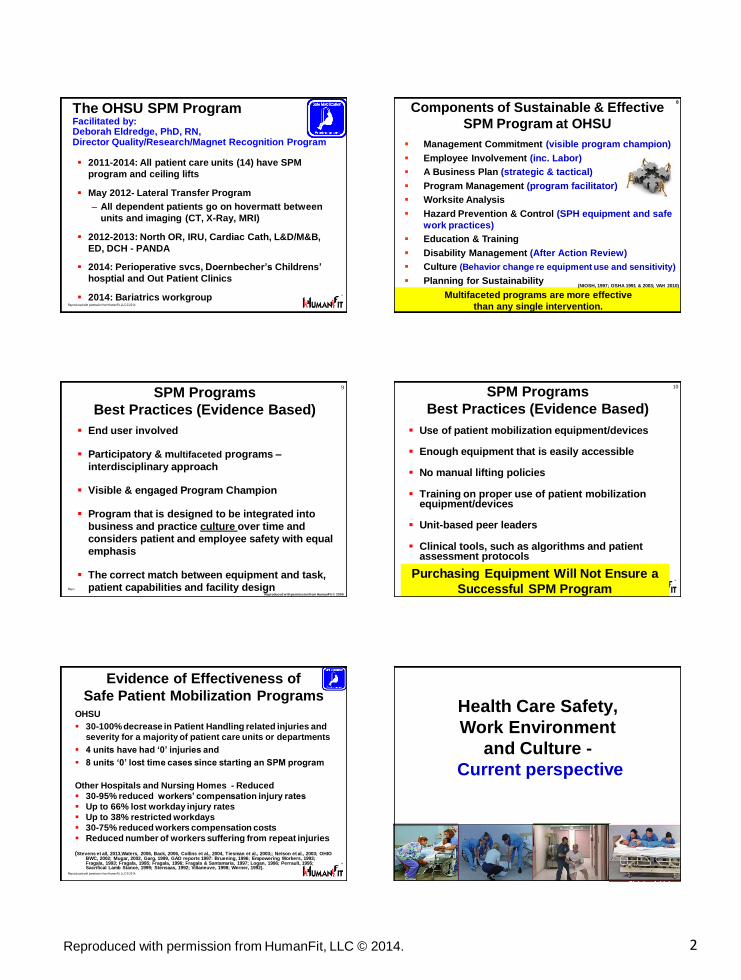
The OHSU SPM Program Facilitated by: Deborah Eldredge, PhD, RN, Director Quality/Research/Magnet Recognition Program
2011-2014: All patient care units (14) have SPM
program and ceiling lifts
May 2012- Lateral Transfer Program
– All dependent patients go on hovermatt between
units and imaging (CT, X-Ray, MRI)
2012-2013: North OR, IRU, Cardiac Cath, L&D/M&B,
ED, DCH - PANDA
2014: Perioperative svcs, Doernbecher’s Childrens’
hosptial and Out Patient Clinics
2014: Bariatrics workgroup
Reproduced with permission from HumanFit, LLC © 2014.
Management Commitment (visible program champion)
Employee Involvement (inc. Labor)
A Business Plan (strategic & tactical)
Program Management (program facilitator)
Worksite Analysis
Hazard Prevention & Control (SPH equipment and safe
work practices)
Education & Training
Disability Management (After Action Review)
Culture (Behavior change re equipment use and sensitivity)
Planning for Sustainability
Components of Sustainable & Effective
SPM Program at OHSU
Multifaceted programs are more effective
than any single intervention.
(NIOSH, 1997; OSHA 1991 & 2003; VAH 2010)
8
Reproduced with permission from HumanFit, LLC © 2014.
SPM Programs
Best Practices (Evidence Based)
End user involved
Participatory & multifaceted programs –
interdisciplinary approach
Visible & engaged Program Champion
Program that is designed to be integrated into
business and practice culture over time and
considers patient and employee safety with equal
emphasis
The correct match between equipment and task,
patient capabilities and facility design
9
Reproduced with permission from HumanFit © 2009
Reproduced with permission from HumanFit, LLC © 2014.
SPM Programs
Best Practices (Evidence Based)
Use of patient mobilization equipment/devices
Enough equipment that is easily accessible
No manual lifting policies
Training on proper use of patient mobilization equipment/devices
Unit-based peer leaders
Clinical tools, such as algorithms and patient assessment protocols
Nelson 2008
10
Purchasing Equipment Will Not Ensure a
Successful SPM Program
Reproduced with permission from HumanFit, LLC © 2014.
Evidence of Effectiveness of
Safe Patient Mobilization Programs OHSU
30-100% decrease in Patient Handling related injuries and
severity for a majority of patient care units or departments
4 units have had ‘0’ injuries and
8 units ‘0’ lost time cases since starting an SPM program
Other Hospitals and Nursing Homes - Reduced
30-95% reduced workers’ compensation injury rates
Up to 66% lost workday injury rates
Up to 38% restricted workdays
30-75% reduced workers compensation costs
Reduced number of workers suffering from repeat injuries
(Stevens et all, 2013,Waters, 2006, Back, 2006, Collins et al., 2004, Tiesman et al., 2003;; Nelson et al., 2003; OHIO BWC, 2002; Mugar, 2002, Garg, 1999, GAO reports 1997: Bruening, 1996; Empowering Workers, 1993; Fragala, 1993; Fragala, 1995; Fragala, 1996; Fragala & Santamaria, 1997; Logan, 1996; Perrault, 1995; Sacrifical Lamb Stance, 1999; Stensaas, 1992; Villaneuve, 1998; Werner, 1992).
11
Reproduced with permission from HumanFit, LLC © 2014.
12
Health Care Safety,
Work Environment
and Culture -
Current perspective

3 Reproduced with permission from HumanFit, LLC © 2014.
Reproduced with permission from HumanFit, LLC © 2014.
13
Ambulatory Surgical Centers
Home Health/Home Care & Hospice
Clinics/Rehabilitation
Emergency Services (EMS)
Nursing Homes
Residential Care & Assisted
Living Facilities
Adult Foster Care
The Health Care Continuum
Hospitals
Reproduced with permission from HumanFit, LLC © 2014.
14
Common Hazards to Health Care
Workers
Biological & Infectious Hazards
– Bloodborne pathogens
(Needlestick injuries, etc)
– Tuberculosis
Chemical Hazards – Latex
– Glutaraldehyde
– Ethylene Oxide
– Antineoplastics
– Volatile organic compounds (VOCs)
Physical Hazards
1. Musculoskeletal disorders
(MSDs) - patient &
materials handling; slips,
trips & falls
– Workplace violence
– Noise
– Radiation
– Motor Vehicle Accidents
Psychosocial Hazards
– Shift work, long hours,
and overtime; lateral
hostility
Reproduced with permission from HumanFit, LLC © 2014.
15 15 15
1. Emergency Medical Technicians and Paramedics
2. Nursing Assistants
3. Firefighters
4. Laborers and Freight, Stock, Material Movers
5. Light Truck Delivery Services
18. RNs
The Incidence of Musculoskeletal
Disorders due to Overexertion 2012 (Incidence rate per 10,000 full-time workers)
(United States Department of Labor [USDOL], 2013). Reproduced with permission from HumanFit, LLC © 2014.
16
Safety in Health Care: Why has it not Improved?
Organizational Culture
Patient Safety focus vs. employee safety
Focus on reimbursement, resource and ongoing
regulatory challenges (including health care reform)
etc.
Lack of systems approach to services provided (Silos)
Lack of resources to facilitate and sustain programs
long term
Problem Solving Approach = Blame the Worker
(Human Error)
Resident handling solutions in LTC = CALL EMS
Reproduced with permission from HumanFit, LLC © 2014.
17
– Patient comes first (self sacrificing mentality)
– A patient that is 120lbs is a ‘light weight’
– Proper body mechanics will prevent injuries
– The old ‘hoyer’ is difficult to use
– There’s no time to use equipment (hard to find, hard to
use, etc)
– I own a ranch – lift hay/round cattle and have never
been hurt
– Professional silos e.g. nursing vs. therapy
Is getting hurt on the job –
just ‘part’ of being a health care worker?
Safety in Health Care: Why has it not Improved?
Employee Culture
Reproduced with permission from HumanFit, LLC © 2014.
“Workforce safety is inextricably
linked to patient safety. Unless
caregivers are given the protection,
respect, and support they need, they
are more likely to make errors, fail to
follow safe practices and not work well
in teams.” Through the Eyes of the Workforce: Creating Joy,
Meaning, and Safer Health Care. The Lucian Leape
Institute at the National Patient Safety Foundation Feb
2013
http://www.npsf.org/about-us/lucian-leape-institute-at-
npsf/lli-reports-and-statements/eyes-of-the-workforce/
18
Creating a Culture of Safety in
Health Care
The Joint Commission
2012

4 Reproduced with permission from HumanFit, LLC © 2014.
Reproduced with permission from HumanFit, LLC © 2014.
19
Why the Increasing Focus on Safe Patient
Mobilization in Health Care?
Increasing incidence of back injuries & other
musculoskeletal disorders (MSDs) in health care
workers across the continuum
The cost of work related MSDs
The changing patient population
SPH legislation
Current research & evidence base
Aging workforce & nursing shortage
Traditional methods of addressing back injuries in
health care are ineffective
19
Reproduced with permission from HumanFit, LLC © 2014.
20
Legislation & Guidelines
Safe Patient Handling Legislation– TX, WA, RI, MD, MN, NJ, CA, IL
(NY, OH, HI). Other states are seeking to pass legislation
ADA: Access To Medical Care For Individuals With Mobility
Disabilities Standard (2010) – Use of patient lifting equipment in
http://www.ada.gov/medcare_ta.htm
OSHA Ergonomics Guidelines for Nursing Homes (2003 rev. 2009)
Facilities Guideline Institute: Health Care Design and Construction
Guidelines (2010) – Incorporate Safe Patient Handling & Movement
www.fgiguidelines.org
NIOSH/ANA/VHA: SPM curriculum for schools of nursing
http://www.cdc.gov/niosh/docs/2009-127/
The American Nurses National Safe Patient Handling and Mobility
Standards, 2013 http://www.nursingworld.org/handlewithcare
20 20 20
Reproduced with permission from HumanFit, LLC © 2014.
21
Back Injuries related to
Manual Patient Handling are the # 1
cause of Health Care Worker Injury in the
USA
Why is Manual Patient Handling
so Hazardous?
Reproduced with permission from HumanFit, LLC © 2014.
22
What are Musculoskeletal Disorders (MSDs)?
(Cumulative Trauma Disorder, Repetitive Strain Injury
Overexertion or Overuse Injury)
Chronic or Cumulative:
Injuries that occur over a period of time (months/years)
& are caused by a combination of risk factors
Acute:
A sudden or one-time traumatic event or incident,
e.g., slip, trip, fall or car wreck
MSDs affect ligaments, muscles,
tendons, cartilage, blood vessels &
nerves & spinal discs
Reproduced with permission from HumanFit, LLC © 2014.
Some Common MSDs
Tendinitis &
Tenosynivitis (upper
extremities)
Epicondylitis (Tennis
Elbow/Golfer’s elbow)
Rotator Cuff Tear
(shoulder)
Vibration White
Finger
Computer Vision
Syndrome - CVS
(Headaches)
Strains and Sprains
(neck, back, shoulder)
Low Back Pain &
Sciatica
Bulging or Herniated
Spinal Discs
Carpal Tunnel Syndrome
Trapezius Myalgia
(tension neck syndrome)
Bursitis (shoulder or
knees)
Reproduced with permission from HumanFit, LLC © 2014.
Physical Demands in Health Care
The EMS Work Environment Risk Factors that can contribute to the development
of Musculoskeletal Disorders
24
+ + + =
P o s t u r e
MSD S
Musculoskeletal
Disorders
Awkward, Static
& Poor Postures
Force
(Lift, Push,
Pull, Carry,
Grip)
Repetition Duration
Additional factors:
Contact Stress
Environmental Factors
Lack of Adequate Rest
Poor Physical Condition
Psychosocial Factors
Work Organization

5 Reproduced with permission from HumanFit, LLC © 2014.
Reproduced with permission from HumanFit, LLC © 2014.
The EMS Work Environment Risk Factors that can contribute to the
development of Musculoskeletal Disorders
The unpredictability of the location and
patient status
Sedentary work followed by sudden
physically demanding activities
High Risk Tasks for MSDs:
– Patient handling
– Lifting gurneys in/out ambulances
– Patient evacuation
– Materials/equipment handling
25
Reproduced with permission from HumanFit, LLC © 2014.
26
The Cumulative Effect
When the musculoskeletal system is
exposed to a combination of these risk
factors (too quickly, too often and for too
long) without sufficient recovery or rest
time, damage occurs
Duration of Exposure to Risk Factors (Time) Affected by: Working through breaks
Overtime
Task variability
Reproduced with permission from HumanFit, LLC © 2014.
1 x 8 Hour shift = cumulative
average weight of 1.8 tons
(Tuohy-Main, 1997)
= 28 Double Decker buses
= or 150 F350 trucks
= or 1 Airbus A380 with 50% load
Physical Demands in Health Care
How Much Does A Nurse (or EMS Worker) Lift?
1 Week (40 hours) = 9 ton
50 weeks/year = 450 tons
27
Reproduced with permission from HumanFit, LLC © 2014.
10 years = 4500 tons = 280 Double Decker buses
= or 1500 F350 trucks
= or 7.5 Airbus A380s fully loaded
= 560 Double Decker buses
= or 3000 F350 trucks
= or 15 x Airbus A380s fully loaded
20 years = 9000 tons
28
Physical Demands in Health Care
How Much Does A Nurse (or EMS Worker) Lift?
Reproduced with permission from HumanFit, LLC © 2014. 29
When Physical and/or Cognitive Demands Exceed
Capabilities of Health Care Workers
Fatigue (physical & mental) which can lead to:
Cumulative Musculoskeletal Disorders (MSDs) e.g. back injuries
Accidents, Errors, Near Misses
A few seconds/mins time lost
Damaged/waste product
Quality of care issues
(Incorrect & missed care)
Traumatic or acute injury
(to user or others)
Death
$$$ Lost: Insurance costs, staff replacement costs, legal
costs, regulatory fines, loss of market share, etc.
Stress
Burnout
Impact on
Organization
29
Reproduced with permission from HumanFit, LLC © 2014.
Why is Manual Patient Handling So
Hazardous?
Patient
Characteristics
- Weight (heavy load)
- Shape (bulky and
awkward)
- Behavior (unpredictable,
confused, fragile, in
pain)
30

6 Reproduced with permission from HumanFit, LLC © 2014.
Reproduced with permission from HumanFit, LLC © 2014.
Why is Manual Patient Handling So
Hazardous?
Task Characteristics – High compressive force and
shear at lumbar spine L5/S1
– Awkward postures compounded by constricted space
– Static trunk flexion
– Trunk rotation
– Sudden shift in load (Resident)
– Duration of the task
– Repetitive exposure to risk factors
(Nelson et al, 2003, Marras, 1999)
31
Reproduced with permission from HumanFit, LLC © 2014.
Poor Work Practices
Why is Manual Patient Handling So
Hazardous?
32
Poor Design of the Work
Space and Equipment
Challenges
Reproduced with permission from HumanFit, LLC © 2014.
33
Compression
3400-6400 N (764lbs) Limit
A-P and Lateral Shearing
1000 N (224lbs) Limit
Arrows show
direction of load or
force on lower
back (L5/S1) when
manually lifting
and moving
Residents
Repetitive exposure to risk factors can cause: Muscle, ligament and facet
joint damage
Micro-fractures in end-plates of vertebra
Disc damage
Force exceeds human
tolerance at L5/S1
Cumulative Impact of Manual Patient
Handling
Rotation
Reproduced with permission from HumanFit, LLC © 2014.
The maximum weight limit for patient handling
is 35lb if the patient is cooperative and
load close to the body
(NIOSH, 2007)
Cumulative Impact of Patient Handling
The physical effort required to repeatedly lift and
move patients manually is greater than the
musculoskeletal system can tolerate.
Therefore there is No Safe method to lift
and transfer patients manually
Using good body mechanics is not enough to prevent back injuries and other MSDs caused by
manual patient handling.
34
Reproduced with permission from HumanFit, LLC © 2014.
35
Some Perspective…….
NIOSH Guidelines:
Load limit for lifting material (non patient) loads: 51 lb
Spine compression force: 764 lb
Spine compression forces for patient handling activities:
– Pulling 105 lb patient (with bedsheet) from
bed to stretcher: 832-1708 lb
– Carrying 105 lb patient down stairs using
stretcher: 1012-1281 lb (source: Hess 2006)
Reproduced with permission from HumanFit, LLC © 2014.
Consequences of Manual Handling For
Patients
Increase risk of
– Skin and joint damage
– Falls
– Pain
– Combative behaviors
– Loss of dignity
– Bowel & bladder dysfunction
Negative impact on clinical outcomes from decrease in ambulation and repositioning in bed (especially if patients are larger and/or lack of staff available to assist)
36

7 Reproduced with permission from HumanFit, LLC © 2014.
Reproduced with permission from HumanFit, LLC © 2014.
37
Patient Handling
Higher Risk Tasks
Lifting a patient/resident
up from the floor
Repositioning patient in
bed or chair
Transfer from bed to chair
(and in/out vehicles)
Lateral Transfers (bed to
stretcher)
Transporting patients
Lifting/supporting limbs
during care tasks
Making occupied bed
Applying anti embolism
stockings
Moving occupied bed or
stretcher
Bathing a confused or
totally dependent
resident
Nelson, 2005 Reproduced with permission from HumanFit, LLC © 2014.
38
How Do We Typically Address
Work Related MSDs?
Narrow Focus = Blame the Worker (Human Error)
Manual patient lifting
Body mechanics classes
Training in safe lifting techniques (inc. use of slider boards, gait belts)
Back belts
Evidence shows that these ‘fixes’ do not work (Reason, 1991,
2000 & Nelson, 2006)
Reproduced with permission from HumanFit, LLC © 2014.
Effective Safe Patient Handling
Programs: Reducing the Risk of
MSDs
39
Reproduced with permission from HumanFit, LLC © 2014.
Designing Tasks, Equipment,
Work Environments &
Systems to be compatible
with the Users’
Physical & Cognitive
Capabilities and Psychosocial
Characteristics
Users in Health Care:
• Employees
• Patients
• Families
Ergonomics and Work Systems
Preventing User
Injury & Error; Improving Comfort &
Efficiency/Quality
Fitting
the
Task
to the
User
40
Reproduced with permission from HumanFit, LLC © 2014.
41
Secondary Controls:
2. Work Practice changes
3. Administrative - Reduce exposure of person to the job
4. Warnings (not very effective)
5. Training(staff and patients)
6. Personal Protective equipment
7. Wellness & Fitness
Primary Controls:
1. Eliminate the risk factor (s) through design
Engineering of the:
Task
Tools
Equipment
Facilities Design
Examples of this approach in Healthcare: Bloodborne Pathogens &
Needlestick Policies; Hazardous Communications Program
Mo
st
Eff
ecti
ve
Least Effective
Addressing Hazards for MSDs Hierarchy of Controls
Reproduced with permission from HumanFit, LLC © 2014.
Eliminate/reduce risk factor(s) through design
e.g., use equipment such as ceiling and portable
floor lifts, friction reducing devices, etc)
Must match equipment with:
- Patient dependency
(physical and cognitive abilities),
- The type of lift, transfer or movement
- The number of staff available
- Facility and medical equipment design
Primary Solutions
Engineering Controls
42

8 Reproduced with permission from HumanFit, LLC © 2014.
Reproduced with permission from HumanFit, LLC © 2014.
43 43 43 43
The level of injury risk reduction
varies by type of equipment
Not all interventions are created
equally!
Tare care not to create a new hazard
Reproduced with permission from HumanFit, LLC © 2014.
44 44
Power loaders; motorized winch &
cable systems
Powered height adjustable gurneys
Ceiling Lifts in ER –
Ambulance/Vehicle Bay
Bariatric ambulance (e.g. AMR)
Loading and Unloading an
Ambulance
Reproduced with permission from HumanFit, LLC © 2014.
Friction Reducing Devices
– Air Assist mats (powered)
– Battery powered motors
Single & reusable friction reducing
sheets - Some self inflating air bag
Slider boards (Caution!)
Repositioning/ Lateral Transfer
Devices for EMS
45
Reproduced with permission from HumanFit, LLC © 2014.
Lateral Transfer Devices
Use of a device reduces the stress to the low back by reducing the friction.
It eliminates the need for the 3rd person on the bed
Drawsheet only
Drawsheet with lateral transfer device
Reproduced with permission from HumanFit, LLC © 2014.
- HoverJack™ - Can also be used as an
evacuation device e.g. moving a patient
down stairways
- ELK & CAMEL (LTC)
47
Equipment to Lift Patients from
the Floor - EMS
Reproduced with permission from HumanFit, LLC © 2014.
Other Tasks:
Evacuation
Wound care, Catheterization – Pannus sling
Other

9 Reproduced with permission from HumanFit, LLC © 2014.
Reproduced with permission from HumanFit, LLC © 2014.
49 49 49
Choosing Solutions - SPH Equipment
Ergo & Safety Design Features
(Designing for the User)
Is the equipment intuitive
to use & user friendly? Is it designed to fit 90% of
the worker population physical capabilities?
Does it meet Safety Regulations & Codes?
What services will the vendor provide?
Cleaning, Storage & Maintenance Considerations
Reproduced with permission from HumanFit, LLC © 2014.
Secondary Solutions:
Work Practice Controls
Reduce employee exposure to primary risk factors by using best work methods, e.g., Plan work organization Assess the patient – ask if they can assist Assess & prepare the environment Get necessary equipment & help Perform the lift or movement safely
50
Reproduced with permission from HumanFit, LLC © 2014.
Secondary Solutions:
Work Practice Controls
Use patient lifting/transfer devices if available
Use the best body mechanics possible
Take regular microbreaks and stretch when seated for
more than 30 minutes
Change position frequently (every few minutes) if
holding a limb, sitting forward over a patient, etc.
Report Ergo/Safety Related Problems to Your
Supervisor
Apply MSD Prevention Principles to Your Off -The-Job
Activities
Report Any Physical Problems Early = Quicker Recovery
51
Reproduced with permission from HumanFit, LLC © 2014.
What Else Can You Do?
Exercise regularly (Strength, Flexibility,
Cardiovascular)
Maintain a balanced diet and drink plenty of water
Don't forget to relax and get enough sleep
Wash you hands!
Work smart at work & at home
52
Reproduced with permission from HumanFit, LLC © 2014.
Implementation and Evaluation Plan
– Don’t forget to involve all stakeholders including patients & families
Plan for program sustainability
Choose evidence-based interventions
and use existing resources
……….don’t reinvent the wheel
Start small, test pilot and demonstrate successes
Market & communicate the program and its’ success
Best Practices for Implementing and Sustaining a SPH/SRH Program
Remember: Purchasing Equipment Will Not Ensure a
Successful SPH Program Reproduced with permission from HumanFit, LLC © 2014.
54
54 Benefits of Health Care Ergonomics & Safe Patient Handling
...for Employees & Patients
(Reduced Risk of Falls; Pressure
Ulcers & Pain etc; Improved
Mobility & Dignity)
..for Health Care
Organizations
Improved
Quality Performance
Efficiency
Flexibility
Recruitment (Larger
Labor Pool) &
Retention
Reg. Compliance
Reduced WC Injury
Costs & Liability
Well-being of
Employees &
Patients
Well-being of
organization
Less absenteeism and
labor turnover.
More involvement and
commitment to
change.
Health
Safety
Comfort
Satisfaction
Adapted from: Corlett, 1995; Nelson
2008; Gallagher, 2009, Enos 2013

10 Reproduced with permission from HumanFit, LLC © 2014.
Reproduced with permission from HumanFit, LLC © 2014.
Potential Program Funding Sources
Employee at Injury Fund (EAIP) ($2500 per injured
worker while on transitional duty- in Oregon
http://www.cbs.state.or.us/wcd/rdrs/rau/3525eaip.
html
Preferred Worker Program – to $25,000 (Oregon)
http://www.cbs.state.or.us/wcd/rdrs/rau/pwp/pwp
_index.html
Local Foundations
55
Reproduced with permission from HumanFit, LLC © 2014.
56 56
Questions
Reproduced with permission from HumanFit, LLC © 2014.
Selected References & Resources
Evaluation of Medical Cot Design Considering the
Biomechanical Impact on Emergency Response
Personnel. Tycho K. Fredericks, T.K et. al. The XXVth
Annual Occupational Ergonomics and Safety Conference,
2013
Evaluation of Back Problems Among Emergency
Medical Services Professionals. Dissertation. Jonathan R.
Studnek, The Ohio State University 2008
Handbook of Human Factors and Ergonomics in Health
Care and Patient Safety 2nd Edition (2012). Edited by
Pascale Carayon. Lawrence Erlbaum Associate
Identification of Factors that Affect the Adoption of
Ergonomic Interventions among EMS Workers. Monica
R. Johnson. Proceedings of the Human Factors and
Ergonomics Society 55th Annual Meeting 2011
57
Reproduced with permission from HumanFit, LLC © 2014.
Selected References & Resources
The Illustrated Guide to Safe Patient Handling and
Movement. Nelson, A.L., Motacki , K, Menzel, N. (2009). New
York, NY: Springer Publishing.
Making the Business Case to Initiate, Sustain and Evaluate
Safe Patient Handling Programs. L. Enos (2011). Part 1,
American Journal of Safe Patient Handling and Movement, I,
(3): 8-15 and Part 2 AJSPHM, I, (4): 22-30.
National Occupational Research Agenda (NORA):National
Public Safety Agenda for Occupational Safety and Health
Research and Practice in the US Public Safety Sector
October 2013
Musculoskeletal Disorders in EMS Creating Employee
Awareness. Thomas F. Fisher and Stephen F. Wintermeyer.
Professional Safety VOL. 57, NO. 7
58
Reproduced with permission from HumanFit, LLC © 2014.
59
Selected References & Resources Organization of work in interaction between the paramedics
and the patient. Petra Auvinena,* and Hannele Palukkab. Work
41 (2012) 42-48
Patient Care Ergonomics Resource Guide: Safe patient
handling and movement. Nelson, A.L. (Ed). (2001 rev 2005).
Tampa, FL: Veterans Administration Patient Safety Center of
Inquiry.
Safe Patient Handling and Movement: A Practical Guide For
Health Care Professionals (2006). Audrey Nelson Editor.
Springer Publishing http://www.springerpub.com/
Safe Patient Handling Equipment Purchasing Checklist. L.
Enos (2013). American Journal of Safe Patient Handling and
Movement, 3, (1): S1-16. Reproduced with permission from HumanFit, LLC © 2014.
60
Selected References & Resources
The Working Back: A Systems View (2008). William S. Marras.
John Wiley & Sons, Inc.,
When is it Safe to Manually Lift a Patient? (2007).Waters, T.R.
American Journal of Nursing, 107(8), 53-59.