DYNAMO: A PHASE 2 STUDY OF DUVELISIB IN …€¦ · DYNAMO: A PHASE 2 STUDY OF DUVELISIB IN...
20
DYNAMO: A PHASE 2 STUDY OF DUVELISIB IN PATIENTS WITH REFRACTORY INDOLENT NON‐HODGKIN LYMPHOMA Ian Flinn, CB Miller, KM Ardeshna, S Tetreault, SE Assouline, PL Zinzani, J Mayer, M Merli, SD Lunin, AR Pettitt, Z Nagy, O Tournilhac, KE Abou‐Nassar, M Crump, ED Jacobsen, S de Vos, P Santabarbara, W Shi, L Steelman, ND Wagner‐Johnston
Transcript of DYNAMO: A PHASE 2 STUDY OF DUVELISIB IN …€¦ · DYNAMO: A PHASE 2 STUDY OF DUVELISIB IN...

DYNAMO: A PHASE 2 STUDY OF DUVELISIB IN PATIENTS WITH REFRACTORY INDOLENT NON‐HODGKIN LYMPHOMA
Ian Flinn, CB Miller, KM Ardeshna, S Tetreault, SE Assouline, PL Zinzani, J Mayer, M Merli, SD Lunin, AR Pettitt, Z Nagy, O Tournilhac, KE Abou‐Nassar, M Crump, ED Jacobsen, S de Vos, P Santabarbara, W Shi, L Steelman, ND Wagner‐Johnston

DUVELISIB IS AN ORAL PI3K‐δ,γ INHIBITOR
PI3K-δ PI3K-γ
Expression Primarily Leukocytes
Primarily Leukocytes
Biochemical Activity (KD) 23 pM 243 pM
Whole Blood Assay (IC50)96 nM
Anti-FcƐR11028 nM
fMLPduvelisibduvelisib
• Selective for PI3Ks over other protein and lipid kinases
• Impairs malignant B‐ and malignant T‐cell survival– Direct antitumor effects– Disrupts tumor cell interactions within the microenvironment
• Duvelisib showed clinical activity in a phase 1 study in pts with advanced hematologic malignancies (Flinn ASH 2015; O’Brien ASH 2015; Horwitz ASH 2015)

STUDY OVERVIEW
Duvelisib 25 mg BID Continuously
Phase 2, Single arm, n=129Accrual Complete;Analysis as of April 2016
(last pt enrolled + 6 mo.)
Treatment until progression or unacceptable
toxicity
Response Assessments• Baseline, Cycles 3, 5, 7, 10
(cycle = 28 days)
• Every 4 cycles thereafter
• Responses per revised IWG criteria (Cheson 2007) by independent review committee (IRC)
Primary Endpoint• ORR (best response of CR or PR per
IWG criteria) per IRC
Key Secondary Endpoints• Duration of response (DOR)
• Progression-free survival (PFS)
• Overall survival (OS)
• Safety

KEY ELIGIBILITY CRITERIA
• 3 iNHL disease subtypes:
− follicular lymphoma (FL)
− small lymphocytic lymphoma (SLL)
− marginal zone lymphoma (MZL)
• Pts were double refractory to rituximab (monotherapy or in combination) and to chemotherapy* or radioimmunotherapy
- Refractory = no CR or PR, or PD within 6 mo. of last dose of prior therapy
• No eligibility restrictions for cytopenias
* Chemotherapy = alkylating agent or purine analogue

STUDY ENROLLMENT BY REGION / COUNTRY
WESTERN EUROPEItaly 21United Kingdom 11France 6Belgium 2Spain 2
EASTERN EUROPEBelarus 10Czech Republic 9Hungary 7Bulgaria 5Georgia 1
NORTH AMERICAUnited States 46Canada 9

BASELINE CHARACTERISTICS
CATEGORY OVERALLN = 129
FLN = 83
SLLN = 28
MZLN = 18
Age, median (range)65 (30, 90)
64 (30, 82)
63 (48, 83)
67 (41, 90)
Male, % 68 68 68 72
ECOG ‐ 0/1/2, % 47 / 48 / 5 51 /42/ 7 43 / 54 / 4 33 / 67 / 0
Years since diagnosis, median (range) 5 (0.3‐27) 4 (0.3‐27) 6 (0.9‐17) 2 (0.8‐10)
Bulky Disease (≥ 5 cm), % 40 37 47 39
Elevated LDH, % 67 75 57 44
High FLIPI (3‐5 factors), % N/A 34 N/A N/A

PRIOR ANTI‐CANCER TREATMENT
CATEGORY OVERALLN = 129
FLN = 83
SLLN = 28
MZLN = 18
Number of Prior Anticancer Regimens
Median 3 3 3 2
Min, Max 1, 18 1, 10 1, 18 1, 8
≤ 2, % 37 35 28 60
> 2, % 64 65 62 40
Time since completion of last therapy (months)
Median 4 3 3 7
Min, Max 0, 121 0, 121 1, 74 1, 58
• Median PFS on last anticancer therapy was 6.0 months per investigator assessment

PATIENTS REFRACTORY TO SELECT PRIOR ANTI‐CANCER THERAPY
CATEGORY
OverallN=129%
FL N=83%
SLLN=28%
MZLN=18%
Refractory to last therapy 96 94 100 100
Refractory to at least 2 therapies 77 81 71 67
Rituximab 98 99 100 94
Alkylating Agent and/or Purine Analogue 92 90 96 94
Rituximab + Alkylating Agent 91 89 96 89
Bendamustine + rituximab 43 43 43 39
R‐CHOP 28 31 18 28
R‐CVP 26 24 32 28

PATIENT DISPOSITION
CATEGORY OVERALLN = 129
FLN = 83
SLLN = 28
MZLN = 18
Median mo. on study (95% CI) 12 (10, 14) 11 (10, 13) 17 (11, 23) 10 (6, 14)
Median mo. on duvelisib(range) 6 (0.4,24) 5 (0.4, 24) 9 (0.7, 16) 6 (0.9, 15)
≥ 12 mo., % 14 10 29 11
Discontinued Treatment, % 73 76 75 56
Disease Progression, % 41 45 36 33
Adverse Event, % 17 16 21 17
Investigator Decision, % 5 5 7 6
Death, % 5 6 7 0
Patient Withdrawal, % 3 4 4 0
Noncompliance , % 1 1 0 0

OVERALL RESPONSE RATE
OVERALLN = 129
FLN = 83
SLLN = 28
MZLN = 18
ORR per IRC, % 46 41 68 33
P‐value p=0.0001* ‐‐ ‐‐ ‐‐
95% CI (37‐55) ‐‐ ‐‐ ‐‐
Complete Response 0 0 0 0
Partial Response 46 41 68 33
ORR per Investigator, % 58 53 79 50
Complete Response 2 1 4 0
Partial Response 57 52 75 50
* The study met the primary endpoint (p=0.0001 against null hypothesis that ORR was ≤ 30% per IRC)

PERCENT CHANGE IN NODAL TARGET LESIONS
• 83% of pts had reduction in target lymph nodes (per IRC)

OVERALL RESPONSE RATE BY SUBGROUP

DURATION OF RESPONSE PER IRC

PROGRESSION‐FREE SURVIVAL PER IRC
• 6 month median PFS (per investigator) on last previous anticancer therapy

OVERALL SURVIVAL
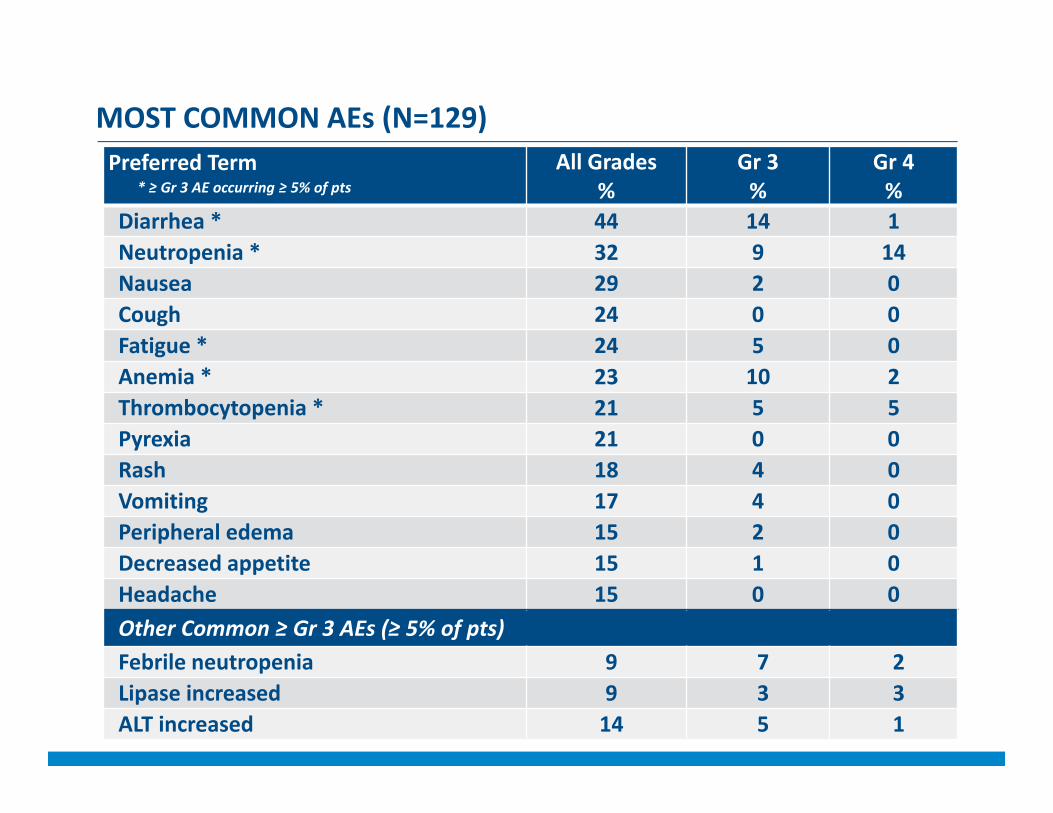
MOST COMMON AEs (N=129)Preferred Term All Grades
%Gr 3 %
Gr 4 %
Diarrhea * 44 14 1Neutropenia * 32 9 14Nausea 29 2 0Cough 24 0 0Fatigue * 24 5 0Anemia * 23 10 2Thrombocytopenia * 21 5 5Pyrexia 21 0 0Rash 18 4 0Vomiting 17 4 0Peripheral edema 15 2 0Decreased appetite 15 1 0Headache 15 0 0Other Common ≥ Gr 3 AEs (≥ 5% of pts)Febrile neutropenia 9 7 2Lipase increased 9 3 3ALT increased 14 5 1
* ≥ Gr 3 AE occurring ≥ 5% of pts

OTHER SIGNIFICANT AEs
* 1 septic shock; 1 viral infection; 1 drug reaction/eosinophilia/ systemic symptoms, 1 toxic epidermic necrolysis/sepsis syndrome
Preferred TermN=129No. pts
Pneumonitis 3
Pneumonia 2
Rash (generalized) 2
AEs Leading to Discontinuation of Duvelisib (≥ 2 pts)
Preferred Term
N=129
Any Gr%
Gr 3/4%
Infection 52 18Diarrhea 44 15Neutropenia 32 28Rash 29 7Anemia 23 12Thrombocytopenia 21 13Pneumonia 18 9Hepatoxicity 16 8Colitis 7 5Pneumonitis 4 2
AEs of Special Interest
• Serious opportunistic infections < 5% (none fatal)
• Pneumocystis (suspected PJP) 1 pt (0.8%)
• CMV 3 pts (2.3%), with 2 pts continuing duvelisib
• 4 treatment‐related AEs had outcome of death *

CONCLUSIONS
• Duvelisib monotherapy is clinically active in double refractory iNHL
– ORR of 46% per IRC (p=0.0001)
– 83% of pts had tumor reduction
– Responses were durable (median 10 months)
• Duvelisib is generally well tolerated, with a manageable safety profile with appropriate risk mitigation
• The DYNAMO study showed that duvelisib monotherapy has a favorable benefit‐risk profile in refractory iNHL pts, and may represent an important treatment option in this population

The Investigators and Sponsor wish to thank all of the study team members, and most importantly, our patients and their families for their participation in this study
. 19

THANK YOU