Dr Paul Lovell and Todd Chenore: Integrating predictive modelling into a whole system approach
21
Virtual Wards and the NHS Devon Experience Integrating Predictive Modelling into a Whole System approach Dr Paul Lovell East Street Surgery, South Molton NHS Devon / North Devon Locality Urgent Care Lead Todd Chenore Clinical Informatics NHS Devon, Torbay and Plymouth
-
Upload
nuffield-trust -
Category
Health & Medicine
-
view
1.125 -
download
0
Transcript of Dr Paul Lovell and Todd Chenore: Integrating predictive modelling into a whole system approach

Virtual Wards and the
NHS Devon Experience
Integrating Predictive Modelling into a Whole System approach
Dr Paul Lovell East Street Surgery, South Molton NHS Devon / North Devon Locality Urgent Care Lead
Todd Chenore Clinical Informatics
NHS Devon, Torbay and Plymouth

Rapid Response
Complex Care Team District Nursing, CRT, Therapy
MIU
Primary Care
Devon Doctors
Community Hospital
Medical Assessment Unit
Emergency Department
SWAST
Ris
k M
anag
emen
t Ski
lls, K
now
ledg
e, D
iagn
ostic
s, C
are
Prov
isio
n
Acute Admission
ED Self Referral £
PbR Non-Elective
ED GP Referral £
Day 0 Admission £
Full Admission £
‘Fixed’ Costs
Community Services £
SWAST £
Primary Care £
DDOC £
End-of-Life £0 £0
IP and © Dr Paul Lovell
Marie Curie / Night sitters
Com
mun
icat
ion
EHR
/ Sh
ared
IT L
inks
/ Vi
ewab
le C
ase-
load
s / I
nter
oper
abili
ty

ED Self Referral £
PbR Non-Elective
ED GP Referral £
Day 0 Admission £
Full Admission £
‘Fixed’ Costs
Community Services £
SWAST £
Primary Care £
DDOC £
£0 £0
Flow and Discharge
Rapid Response
Complex Care Team District Nursing, CRT, Therapy
MIU
Primary Care
Devon Doctors
Community Hospital
Medical Assessment Unit
Emergency Department
SWAST
Ris
k M
anag
emen
t Ski
lls, K
now
ledg
e, D
iagn
ostic
s, C
are
Prov
isio
n
Acute Admission
End-of-Life
IP and © Dr Paul Lovell
Marie Curie / Night sitters
IP and © Dr Paul Lovell
Com
mun
icat
ion
EHR
/ Sh
ared
IT L
inks
/ Vi
ewab
le C
ase-
load
s / I
nter
oper
abili
ty

Robust alternatives to hospital admission
Risk stratification and Case Management
Excellent end of life care
Smooth flow and discharge of patients through the
system
Specialist rehabilitation
5 Key Whole System Principles

Rapid Response 7d Pathfinder Service
Complex Care Team District Nursing, CRT, Therapy
MIU
Primary Care
Devon Doctors
Community Hospital
Medical Assessment Unit
Emergency Department
SWAST
Com
mun
icat
ion
EHR
/ Sh
ared
IT L
inks
/ Vi
ewab
le C
ase-
load
s / I
nter
oper
abili
ty
Ris
k M
anag
emen
t Ski
lls, K
now
ledg
e, D
iagn
ostic
s, C
are
Prov
isio
n
Acute Admission
ED Self Referral £
PbR Non-Elective
ED GP Referral £
Day 0 Admission £
Full Admission £
‘Fixed’ Costs
Community Services £
SWAST £
Primary Care £
DDOC £
End-of-Life £0
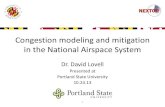
Community Virtual Wards
Falls Team
Special Messages
Consultant Support
Direct Access
GP Team GP Team
TeleMonitoring
Mental Health Liaison
Discharge Planning and Co-ordination of Community Services Discharge Support
24 / 7 Nursing
Early Supported Discharge
Intensive Rehabilitation
£0
Urgent Care Service Model
IP and © Dr Paul Lovell
Marie Curie / Night sitters
Voluntary Sector
Special Messages
IP and © Dr Paul Lovell

Complex Care Teams Developed under DH POPPS Project - started October
2008
23 to cover NHS Devon pop. c750,000
Case Management core to proposed function
Integrated Health and Social Care Team
Vertically Integrated in North Devon from outset
Common Geographical coverage and base
Linked to specified GP Practices (105 in total)
Post-TCS now provided by NDHT and TCT

Community Nursing
Therapy Services
Community Hospitals
OPMH Health Services
Voluntary Sector
Primary Care
Practice
Social Workers /OT
/Community Care
Practice Manager
Vol. Sector Co-ordinator
Community Nurse Team
Leader
Community Nurse Team
Manager ACS Practice Manager
Modern Matron
Therapy Manager
Practices
Complex Care Teams
PLUS: •Cluster Pharmacists •CoE Consultants •Social Care Reablement

Complex Care Teams Evaluation

Virtual Wards
Virtual Ward = Predictive Modelling + Multi-disciplinary Case-Management (Hospital at Home)

Predictive modelling in Devon • Started with PARR and PARR++
• Implemented CPM in house for 2008/09 start of virtual ward pilot
• Built DPM in house for 2010/11 at very low relative cost
• Incorporated local datasets like ambulance, OOH, registration duration, deprivation, etc.
• Improved predictive power

Number (%) patients in ‘at risk’ group predicted by the model who had an emergency admission within 12
months
‘At risk’ sub-group Combined Predictive Model (CPM)
Devon Predictive Model (DPM)
200 top-ranked patients (0·03% of registered population) 143/200 (71.5%) 173/200 (86.5%)
1000 top-ranked patients (0·13% of registered population) 605/1000 (60.5%) 742/1000 (74.2%)
3800 top-ranked patients (0·5% of registered population) 1843/3800 (48.5%) 2286/3800 (60.2%)
7000 top-ranked patients (0·92% of registered population) 2639/7000 (37.7%) 3708/7000 (53.0%)
16000 top-ranked patients (2·1% of registered population) 4896/16000 (30.6%) 6877/16000 (43.1%)

Community Specialist
Nurse Service
Consultant Outreach
Out-patient Review
Ward Assessment
Acute Admission
COPD
ACS Social Worker
ACS OT
ACS CCW
Community Matron
District Nurses
Voluntary Services
Rep
CCT Co-ordinator (VW Ward Clerk)
Mental Health
CRT Nurse
CRT Physio
CRT OT
Practice Nurses
GP
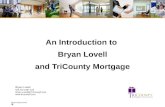
PATIENT
Case Manager
Monthly Devon Predictive Model
Primary Care and Complex Care Team
Joint Meetings
Admit to Virtual Ward
Virtual Ward Staff CCT and
Primary Care
Exacerbation Pathways
Monthly DPM report and VW Bed-state reviews
Daily interactions within team, Regular VW Ward Rounds and Reviews ( Weekly Core Group
Meetings)
Very High and High-Risk Patients Identified
Housing Charities (3rd sector)
Virtual Ward

Enhancing function and co-ordination
Community Services Virtual Ward
Devon Predictive Model
Primary Care
Promoting Integrated, whole system approach

Enhancing function and co-ordination Community-based Integrated Management
Primary Care Community Services Virtual Ward
Devon Predictive Model
CQUIN LES Service Specification & Investment CQUIN LES

Devon-Wide Roll-out Identified as QIPP plan for Urgent Care Devon-wide
Aim to integrate into 23 CCTs to cover Devon pop. c750,000
Roll-out commenced yc 2010/11
Stage 1- Establish (2010/11) • Year 1 CQUIN LES Funded
• Payment to practices by volume (to limit)
Sign up to Devon Predictive Model
Identify target patients and assign a case-manager (Read
Code)
Produce Out of Hours Special Message- active on DDOC
Adastra

Devon-Wide Roll-out Stage 2 - Exert Control on high-risk Group (2011/12)
Year 2 CQUIN LES Funded
Payment to practices by % Bed-state (of bed number limit)
Sign up to Combined Predictive Model
Identify target patients and assign a case-manager (Read Code)
Produce Out of Hours Special Message- active on DDOC Adastra
Full payment- 85% High /Very High Risk and 80% Occupancy over the
year
Devon (Combined) Predictive Model 85%
Direct Referral 15%
3-4 Months Input LTC Self-Management, Education, Social etc (75-80%)
Prolonged Admission 12-18 months (20-25%)
Virtual Ward

Characteristic Locality A Locality B Locality C
Access to Monthly DPM Y Y Y
Complex Care Teams Y Y Y
Full Year LES Y Y N
Designated Project Support Y N N
Locality Leads Buy-in Y Y/N N
Population Size 220,434 165,408 379,682
CCT Provider SDHT NDHT NDHT
CQUIN LES Investment 11/12 £ £ £
Fair Shares Funding Above Below Above
Devon Evaluation (1) The Locality Differences

Locality Average VW occupancy
Average VW occupancy
chosen from top 0.5% risk
Average VW occupancy
chosen from low risk
Percentage of practices
hitting 2011 DPM LES targets
First quarter net admission change 2009 to
2011 for top 0.5% cohort*
Change in actual PbR cost associated with net admission
change*
Locality A 107.4% 45.2% 15.5% 65.5% -22.06% -£845,310
Locality B 98.8% 37.8% 21.6% 42.9% -14.24% -£210,758
Locality C 90.3% 28.7% 26.4% 19.2% 3.91% £151,742
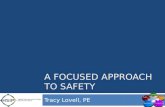
Devon Evaluation (2)

Devon Evaluation (3) Population Profile Changes
DPM Risk Scores - Distribution of risk across the
population when separated into Risk-Buckets (Kaiser
Pyramids)
A
B
C

Devon-Wide Roll-out Stage 3 - Maximise Impact & Responsiveness (2012/13)
Year 3 CQUIN LES Funded
Payment to practices by % Bed-state (of bed number limit) and Top 0.5%
percentage
Ensure named Lead GP in each Practice
Monthly Bed-state meetings
Share DPM results access with CCT Team
Ensure Project Support Role in place from Locality Commissioning Team
Embed and make routine part of work and roles
Community CQUIN -> TIFA, Initial Assessment Summary and Discharge
Summary
Cope with changes in CCG and membership

Next Stages Stage 4 - Upstream targeting
Evolve Model and additional functionality in the Virtual Wards to
identify those at point of take-off (Popcorn Theory)
Increase impact with lower level measures and integrate into LTC
management and whole system approaches e.g. PEAR-Resp
development, Screening, EPP etc
Interoperability of IT systems and communication
A B