Dr John E. Williams Consultant in Anaesthesia and Pain ... · Epidemic of CPSP (Katz,2017) 5....
53
Chronic pain after breast surgery Dr John E. Williams Consultant in Anaesthesia and Pain Management Royal Marsden Hospital
Transcript of Dr John E. Williams Consultant in Anaesthesia and Pain ... · Epidemic of CPSP (Katz,2017) 5....

Chronic pain after breast surgery
Dr John E Williams
Consultant in Anaesthesia and Pain Management
Royal Marsden Hospital
GOOD NEWS Most patients heal normally after surgery
amp return to baseline functional status
BAD NEWS 1 Some operations amp some patientshellip
hellipat risk of developing chronic pain +- long term opioid use
2 Significant impacthellipphysically amp socially economically $1m in a 30yr old (Labatt 2000)
3 Predictive factorshellipbut we are a long way from determining precise rolehellip
4 lsquoEpidemic of CPSPrsquo (Katz2017)
5 lsquoComplex area aetiologically and clinicallyrsquo (Macrae 1998 2008)
Questions
bull Why is this an important topic bull How big a problem is it bull Why do some people develop the problem and not others bull Clinical manifestations and impact bull Why is Pain predictive of more Pain bull Does the pain get better bull What can we do as Anaesthetists AHPrsquos prevention and
treatment bull What can we discuss with SurgeonsPatients bull What is the way forward
Is this a real problem
amp Why is it important
1 COMMON
bull Once thought to be rare ndash recently reported incidence gt 50 under-recognised misdiagnosed amp neglected
bull Survivor population increasing huge impact for humanitarian medical amp economic reasons
bull Causes additional disability amp psychological distress
bull Chemo- amp radio-therapy additional causes of pain
bull Spectre of recurrent disease
2 PREVENTION
bull New focus on treatment amp prevention
bull Model of lsquoacute to chronicrsquo mechanisms
bull Integration of pain services with other clinical groups
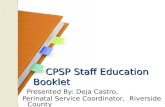
Case Vignette
bull Mrs MB age 45
bull Mastectomy amp axillary dissection RT
bull Presents with severe chronic pain
bull Severe limitation of movement
bull MRI excludes recurrent disease
Pain amp disability
Muscle spasm
Pain
Capsulitis
lsquoCordingrsquo
History Sherman et al PAIN (1984) Chronic phantom pain in 5000 American Veterans 80 pain 1 lasting effect of treatments
Crombie et al PAIN (1998) Cut and Thrust antecedent surgery among patients attending a chronic pain clinic Surgery caused pain in 23 Macrea BJA (1998 2008) Chronic postsurgical pain
Incidence - operations
Type of operation Incidence of chronic pain
No of ops (2006)
1 Amputation 30-50 15000
2 Mastectomy 20-30 18000
3 Thoracotomy 30-60
Heart bypass surgery 30-50 30000
Caesarean section 6 139000
Cholecystectomy 5-50 51000
Hernia 5-35 75000
Laparotomy 30000
Dental root canal surgery (PAIN 2016)
10
Prevalence of chronic pain after breast surgery author year prevalence time
Jamison 1979 44 2 years
Kroner 1989 23 1 year
Vecht 1990 18 6 months
Polinsky 1994 22-32 mean 8 years
Tasmuth 1995 gt50 1 year
Wallace 1996 22- 49 1 year
Smith 1999 43 6 years
Johansen 2000 15 6 years
Fassoulaki 2002 33 3 months
Reuben 2004 50 6 months
Fassoulaki 2005 57 6 months
Kairaluomma 2006 8 1 year
Burton 2007 50 1 year
Hofso 2012 50 1 year
New Definition Old
Macrea BJA 2008 New
Pain April 2017
1 Pain after surgical procedure
1 Pain after a surgical procedure or increases in intensity after a surgical procedure
2 Pain after 2 months 2 Pain after at least 3-6 months hellipwith significant impact on Quality of Life
3 Exclude other causes of the pain
3 Exclude other causes of the pain
4 Exclude pre-existing causes
4 The pain is either a continuation of post surgery pain or develops after an asymptomatic period
5 The pain is either i) localised to the surgical field ii) projected to the innervation territory of a
nerve in the field
Classification of lsquopost mastectomyrsquo pain
1 Pre-existing pain
Osteorheumatoid arthritis Fibromyalgia
Costo-chondritis Cervical radiculopathy
2 Tumour
involvement
Recurrence Metastasis
Cervical radiculopathy due to tumour
3 Post-surgical
Intercostobrachial neuralgia Other neuralgias Persistent lsquoacutersquo pain Scar pain
Phantom breast Intercostal neuromas
Carpal tunnel syndrome Radiation induced plexopathy
Transient brachial neuritis Complex regional pain syndrome
4 Neuropathic
5 Pain due to
implants amp
reconstruction
Capsulitis Capsular contraction and hardening
Foreign body reaction Referred pain Implant migration
Atypical chest pain syndrome Reconstruction lsquoissuesrsquo
6 Other causes
Psychological factors Lymphoedema Pericapsulitis
Muscle spasm lsquoShoulder painrsquo Post-chemo Post- radiotherapy Idiopathic
Myofascial pain dysfunction syndrome
How big a problem is it
In a population of chronic pain patientshelliphow many had pain as a result of surgery Crombie et al Pain 1998 5000 chronic pain patients 23 = CPSP (high proportion with disability) How many people with acute pain go on to get pain at 1 year Hayes et al Acute Pain 2002 5000 patients undergoing surgery Acute neuropathic pain 2 Feature= high intensity 910 Follow up Hayes et al Acute Pain 2002 Pain at 6 months 78 Pain at 1 year 56 lsquo26 million operations year in USA (2008) 1 of all patients develop CPSPrsquo (Katz 2011)
What this study adds bull 3 of patients who had not used opioids previously continued to use them for more than 90 days after major elective surgery bullImportant public health concern because millions of patients undergo major surgery every year
Clarke et al British Medical Journal 2014
Risk factorshellip 1 Causal Modifiable Risk factors (Katz Anesth amp Analg 2011)
Acute pain
Pre-existing pain
Psychological factors
2 Correlated risk factors (Katz Anesth amp Analg 2011)
Younger age
Gender
Psychological distress
Pain
Risk factors
1 Patient related
2 Surgery related
Patient-related risk factors lsquohellippain predicts painrsquo
bull Preoperative pain (Forsythe 2008)
bull Intensity of acute pain (Masselin-Dubois 2013)
bull Acute neuropathic pain (Haroutiounian 2013)
bull High opioid consumption perioperatively (Kalso 2001)
bull Pain in other body parts (Pinto 2012)
bull Younger age (Masselin-Dubois 2013)
bull Female (Ochroch 2006)
Psychological risk factors
bull Pre-op anxiety and catastrophizing meta analysis (2x likelihood of developing CPSP (Theunissen Clin J Pain 2012)
bull Depression (Attal 2014)
bull Catastrophizing (Masselin-Dubois 2013)
bull Sensitivity to pain traumatisation (Page 2013)
bull Anxiety (Kleimann 2011)
bull Fear of long term consequences of surgery (Peters 2007)
Surgical risk factors
bull Low vs high volume surgical unit 13 increase in risk of CPSP (Tasmuth1999)
bull Duration of surgery (Kalso 2007)
bull Minimally invasive surgery (Grant 2004)
bull Stitch types (Cerfolio 2003)
bull Nerve damage preservation (Jensen 1985)
Predictive factors for chronic pain after breast surgery
Anderson et al Pain 2015 n=575
Pain at 1 year
bull Moderate- severe post op pain (50)
bull Axillary lymph node with ICB nerve preservation (30)
bull Neuropathic pain 1 week (18)
bull Age lt 65 (18)
Wang Canadian Medical Assoc Journal 2016 bull Young age bull Axillary lymph node dissection bull Acute pain High quality evidence showed no association
with BMI Type of breast surgery Chemotherapy Reconstruction
Clinical Prediction Model and Tool for Assessing Risk of Persistent Pain After Breast Cancer Surgery Tuomo J Meretoja Kenneth Geving Andersen Julie Bruce Lassi Haasio Reetta Sipilauml Neil W Scott Samuli Ripatti Henrik Kehlet and Eija Kalso
March 2017
Risk Factors ndash what can we discuss with surgeons
bull Information for patients
bull Pre-assessment pain clinic
bull Pre-op anaesthetic strategies algorithms PVB
bull Surgical technique ()
(eg mesh preservation of nerves
minimally invasive etc)
bull Enhanced recovery hellip
eg Kehlet et al Br J Surgery 2005
Fast Track Surgery
bull Pain clinic follow up
Pathophysiology lsquowhat is it about pain that causes more painrsquo
lsquohelliptransition to chronicityhelliprsquo
1 Nociceptive inflammation ischaemia oedema pressure traction
2 Neuropathic peripheral amp central sensitisation
spinal cord neuroplasticity
neuroma
3 Psychological amp social
4 Genetic
The neuropathic component in persistent pain after surgery
systematic review Haroutiunian PAIN 2013
CPSP after 11 types of surgery
bull Amount of pain depends
bull on likelihood of nerve damage
Neuropathic pain
bull in 65 of thoracotomy patients
bull 33 groin surgery
bull 6 knee surgery
Post surgical breast pain
Jung PAIN 2003
1 Intercostobrachial neuralgia
2 Other nerve injury
3 Neuroma
4 Phantom breast
Natural History
Long-term follow-up of breast cancer survivors with post-mastectomy pain syndrome
Macdonald et al British J of Cancer 2005
1996helliphellip 43 pain 3 years 2002 hellip21 pain 9 years
Persistent pain after breast surgery 6-year nationwide
follow up
Mejdahl Kehlet et al BMJ 2013
2008hellip47 pain 1 year
2013hellip37 pain 6 years
Treatment - prevention
helliphellipfrom Pre-emptive Analgesia (blocking preoperative stimuli)
helliphellipto Preventative Analgesia (blocking noxious stimuli central sensitisation across the entire perioperative period)
Preventative treatments
1 Nerve blocks Regional
2 Drugs
Regional anaesthesia to prevent chronic pain after surgery a Cochrane systematic review and meta-analysisdagger M H Andreae1 and D A Andreae2
BJA 2013
bull 23 RCTrsquos
bull Epidural anaesthesia and
paravertebral blocks may be effective
in preventing chronic pain at 1 year
bull Effective in about 1 in 4
patients treated
Preincisional Paravertebral Block Reduces the Prevalence of Chronic
Pain After Breast Surgery Kairaluoma et al Anesth Analg 2006103703-708
bull Preincisional paravertebral block provides significant immediate postoperative analgesia
bull In the same patients (n = 60) 12 months sig less pain in the PVB group
bull In addition to providing acute postoperative pain relief preoperative PVB reduces the prevalence of chronic pain 1 yr after breast cancer surgery
Epidurals Intraoperative epidural analgesia provides preventative analgesia in
abdominal surgery Lavandrsquohomme et al Anaesthesiology 2005
bull Clear benefit of epidural in preventing chronic pain 1 year
bull Intraoperative epidural better than postoperative epidural
bull Effective epidural better than effective parenteral only analgesia one year
Systematic review of therapeutic interventions to reduce chronic post surgical pain (32 RCTrsquos)
Humble et al European J of Pain (2015)
POSITIVE
Gabapentinoids
Lidocaine
iv lidocaine EMLA
Regional
TIVA
NEGATIVE
Ketamine
Cryoanalgesia
Local anaesthetic infiltration
Remifentanil (increased chronic pain)
1 Gabapentin around time of surgery
lsquono effect on chronic painrsquo
POSITIVE
NEGATIVE
Meta analysis (Clarke 2012) 48 RCTrsquos positive effect at 2 months
Cochrane Systematic Review (Chaparro 2013) 280 patients analysed pain at 6 months No effect
RCT Gabapentin 1200mg prior to Thyroidectomy Sig less pain at 3 months (Brogley 2008)
RCT Gabapentin vs Placebo Knee replacement No effect on chronic pain (Clarke 2014)
2 Pregabalin ndash around time of surgery lsquoNot a recommended treatment can cause post operative somnolencersquo
Positive
Negative
Meta-analysis of 3 studies (Clarke 2012) All showed improvement in pain 2 RCTrsquoshellipvery large decrease in CPSP (p=0007)
3 unpublished RCTrsquos from Pfizer (2010-2014) hellipall negative for acute and chronic pain i) 307 patients undergoing knee replacement ii) 501 patients hysterectomy iii) 425 patient hernia
Cochrane Systematic Review (Chaparro 2013) 25 RCTrsquos significant benefit
Systematic review (Martinez May 2017) No difference between pregabalin and placebo 3 months Use for acute pain in pro-nociceptive surgery Side effects a problem
Multimodal analgesia
bull Standard protocols now widely used eg Paravertebral blocks at MD Anderson bull Pre-assessment clinic screening for pain psychological factors pain catastrophising scale helliphellipgenetic screening tests bull Education patients surgeons anaesthetists nurses psychologists
General treatment strategies for chronic postsurgical neuropathic pain
Preventative Perkins amp Kehlet Anesthesiology 2000
bullSurgical procedure preservation
sentinel node biopsy
bullBetter postoperative pain management
bullInformed consent preparatory
information
Established Dworkin Archives Neurol 2003 60
1524
bull Amitriptyline
bull Gabapentin
bull Opioids
bull Tramadol
bull 5 Lidoderm patch EMLA
Positive therapies for Prevention of PSBP
1 EMLA applied to chest wall prior
to surgery less pain 3 months
Fassoulaki 2000
2 Venlafaxine XR 70mg before
and for 2 weeks post surgeryno diff
acute pain significantly less chronic
pain 6 months
Reuben 2004
3 Aggressive acute pain
management
Iohom 2006
4 Preincisional paravertebral
block
Kairaluoma 2006
5 Multimodal analgesia with
gabapentin EMLA ropivacaine less
acute pain amp pain 6 months
Fassoulaki 2005
A pain management programme for chronic cancer-
treatment-related pain Robb Williams Duvivier Newham
Journal of Pain 2006775-150
bull Theory of cancer-related pain
bull Pain pathways
bull Overunder activity cycle
bull Pacing
bull Exercise and fitness
bull TENS
bull Posture and manual handling
bull Relapse and prevention
Psychology interventions
bull Goal setting
bull Role of factors involved in pain
bull Homework assignments
bull Relaxation techniques
bull Cognitive skills
bull Relapse and prevention
Results
significant (plt005) improvements in
bull Pain severity
bull Psychological distress
bull Pain amp psychological coping indices
bull Activities of daily living
bull General fitness
Research Proposal
Exercise to prevent shoulder conditions in patients
undergoing breast cancer treatment
bull Aim to conduct a randomised controlled trial (RCT) supported with qualitative research to investigate the clinical and cost-effectiveness of early supervised exercise on outcomes of arm function chronic pain and quality of life at one year in women undergoing treatment for breast cancer
Intervention
bull A physiotherapy-led structured exercise programme incorporating behavioural strategies and monitoring to encourage adherence
bull A minimum of 4 face-to-face specialist treatment sessions with individual participants will be
delivered within 12 weeks of surgery bull Access to interim telephone support will be provided The programme will restrict to controlled early
stretching and ROM exercises with subsequent progression to maintain strength and function (weeks 2 to 12)
bull Qualitative interviews will be used during the feasibility phase of the trial to explore acceptability of
to the intervention
Outcomes
bull arm shoulder and hand function at 12 months using the 30-item Disability Arm Shoulder Hand (DASH) questionnaire
bull quality of life
bull Functional Assessment of Cancer Treatment-Breast (FACT-B)
bull Short-Form-12 and EQ-5D-5L
bull Data on postoperative adverse events surgical site infection and healthcare resource use will be collected at 6 and 12 months after surgery
Positive therapies for Prevention of PSBP
1 EMLA applied to chest wall prior
to surgery less pain 3 months
Fassoulaki 2000
2 Venlafaxine XR 70mg before
and for 2 weeks post surgeryno diff
acute pain significantly less chronic
pain 6 months
Reuben 2004
3 Aggressive acute pain
management
Iohom 2006
4 Preincisional paravertebral
block
Kairaluoma 2006
5 Multimodal analgesia with
gabapentin EMLA ropivacaine less
acute pain amp pain 6 months
Fassoulaki 2005
Current Treatment Paradigms
The Toronto General Hospital
Transitional Pain Service
development and implementation
of a multidisciplinary program
to prevent chronic postsurgical pain (Katz J Pain Res 2015)
bull Nurse navigator
bull Psychologists (ACT)
Clinical Manifestations hellipour approach to the patient with CPSP
bull Type of pain Cause
bull Exclude other causes (infection recurrence)
bull Psychological and social factors
bull Temporal Context
Electronic Patient Record
Future Directions
bull Identify Causative Modifiable risk factors vs Associative risk factors
bull Measure psychological variables
bull Genetic assays to identify genes controlling the variability in developing chronic pain
Aim is lsquoto identify susceptibility to chronic pain and sensitivity to analgesicsrsquo
Chronic pain lsquoheritabilityrsquo is variable
Conclusions
bull 1 year incidence = 05 -10 bull Avoid pain before during and after surgery lsquohelliphelliptranslate advances in acute pain to chronic settinghelliphelliprsquo bull Psychological pre-assessment bull Education discussion with patients surgeons bull In some cases preventive analgesia may be beneficial bull Transitional Pain Servicehelliptrackinghellipdatabase lsquoPragmatic approachrsquo lsquoAll diseases have an acute phasersquo lsquoDrugs good for acute pain must be good for chronic painrsquo

GOOD NEWS Most patients heal normally after surgery
amp return to baseline functional status
BAD NEWS 1 Some operations amp some patientshellip
hellipat risk of developing chronic pain +- long term opioid use
2 Significant impacthellipphysically amp socially economically $1m in a 30yr old (Labatt 2000)
3 Predictive factorshellipbut we are a long way from determining precise rolehellip
4 lsquoEpidemic of CPSPrsquo (Katz2017)
5 lsquoComplex area aetiologically and clinicallyrsquo (Macrae 1998 2008)
Questions
bull Why is this an important topic bull How big a problem is it bull Why do some people develop the problem and not others bull Clinical manifestations and impact bull Why is Pain predictive of more Pain bull Does the pain get better bull What can we do as Anaesthetists AHPrsquos prevention and
treatment bull What can we discuss with SurgeonsPatients bull What is the way forward
Is this a real problem
amp Why is it important
1 COMMON
bull Once thought to be rare ndash recently reported incidence gt 50 under-recognised misdiagnosed amp neglected
bull Survivor population increasing huge impact for humanitarian medical amp economic reasons
bull Causes additional disability amp psychological distress
bull Chemo- amp radio-therapy additional causes of pain
bull Spectre of recurrent disease
2 PREVENTION
bull New focus on treatment amp prevention
bull Model of lsquoacute to chronicrsquo mechanisms
bull Integration of pain services with other clinical groups
Case Vignette
bull Mrs MB age 45
bull Mastectomy amp axillary dissection RT
bull Presents with severe chronic pain
bull Severe limitation of movement
bull MRI excludes recurrent disease
Pain amp disability
Muscle spasm
Pain
Capsulitis
lsquoCordingrsquo
History Sherman et al PAIN (1984) Chronic phantom pain in 5000 American Veterans 80 pain 1 lasting effect of treatments
Crombie et al PAIN (1998) Cut and Thrust antecedent surgery among patients attending a chronic pain clinic Surgery caused pain in 23 Macrea BJA (1998 2008) Chronic postsurgical pain
Incidence - operations
Type of operation Incidence of chronic pain
No of ops (2006)
1 Amputation 30-50 15000
2 Mastectomy 20-30 18000
3 Thoracotomy 30-60
Heart bypass surgery 30-50 30000
Caesarean section 6 139000
Cholecystectomy 5-50 51000
Hernia 5-35 75000
Laparotomy 30000
Dental root canal surgery (PAIN 2016)
10
Prevalence of chronic pain after breast surgery author year prevalence time
Jamison 1979 44 2 years
Kroner 1989 23 1 year
Vecht 1990 18 6 months
Polinsky 1994 22-32 mean 8 years
Tasmuth 1995 gt50 1 year
Wallace 1996 22- 49 1 year
Smith 1999 43 6 years
Johansen 2000 15 6 years
Fassoulaki 2002 33 3 months
Reuben 2004 50 6 months
Fassoulaki 2005 57 6 months
Kairaluomma 2006 8 1 year
Burton 2007 50 1 year
Hofso 2012 50 1 year
New Definition Old
Macrea BJA 2008 New
Pain April 2017
1 Pain after surgical procedure
1 Pain after a surgical procedure or increases in intensity after a surgical procedure
2 Pain after 2 months 2 Pain after at least 3-6 months hellipwith significant impact on Quality of Life
3 Exclude other causes of the pain
3 Exclude other causes of the pain
4 Exclude pre-existing causes
4 The pain is either a continuation of post surgery pain or develops after an asymptomatic period
5 The pain is either i) localised to the surgical field ii) projected to the innervation territory of a
nerve in the field
Classification of lsquopost mastectomyrsquo pain
1 Pre-existing pain
Osteorheumatoid arthritis Fibromyalgia
Costo-chondritis Cervical radiculopathy
2 Tumour
involvement
Recurrence Metastasis
Cervical radiculopathy due to tumour
3 Post-surgical
Intercostobrachial neuralgia Other neuralgias Persistent lsquoacutersquo pain Scar pain
Phantom breast Intercostal neuromas
Carpal tunnel syndrome Radiation induced plexopathy
Transient brachial neuritis Complex regional pain syndrome
4 Neuropathic
5 Pain due to
implants amp
reconstruction
Capsulitis Capsular contraction and hardening
Foreign body reaction Referred pain Implant migration
Atypical chest pain syndrome Reconstruction lsquoissuesrsquo
6 Other causes
Psychological factors Lymphoedema Pericapsulitis
Muscle spasm lsquoShoulder painrsquo Post-chemo Post- radiotherapy Idiopathic
Myofascial pain dysfunction syndrome
How big a problem is it
In a population of chronic pain patientshelliphow many had pain as a result of surgery Crombie et al Pain 1998 5000 chronic pain patients 23 = CPSP (high proportion with disability) How many people with acute pain go on to get pain at 1 year Hayes et al Acute Pain 2002 5000 patients undergoing surgery Acute neuropathic pain 2 Feature= high intensity 910 Follow up Hayes et al Acute Pain 2002 Pain at 6 months 78 Pain at 1 year 56 lsquo26 million operations year in USA (2008) 1 of all patients develop CPSPrsquo (Katz 2011)
What this study adds bull 3 of patients who had not used opioids previously continued to use them for more than 90 days after major elective surgery bullImportant public health concern because millions of patients undergo major surgery every year
Clarke et al British Medical Journal 2014
Risk factorshellip 1 Causal Modifiable Risk factors (Katz Anesth amp Analg 2011)
Acute pain
Pre-existing pain
Psychological factors
2 Correlated risk factors (Katz Anesth amp Analg 2011)
Younger age
Gender
Psychological distress
Pain
Risk factors
1 Patient related
2 Surgery related
Patient-related risk factors lsquohellippain predicts painrsquo
bull Preoperative pain (Forsythe 2008)
bull Intensity of acute pain (Masselin-Dubois 2013)
bull Acute neuropathic pain (Haroutiounian 2013)
bull High opioid consumption perioperatively (Kalso 2001)
bull Pain in other body parts (Pinto 2012)
bull Younger age (Masselin-Dubois 2013)
bull Female (Ochroch 2006)
Psychological risk factors
bull Pre-op anxiety and catastrophizing meta analysis (2x likelihood of developing CPSP (Theunissen Clin J Pain 2012)
bull Depression (Attal 2014)
bull Catastrophizing (Masselin-Dubois 2013)
bull Sensitivity to pain traumatisation (Page 2013)
bull Anxiety (Kleimann 2011)
bull Fear of long term consequences of surgery (Peters 2007)
Surgical risk factors
bull Low vs high volume surgical unit 13 increase in risk of CPSP (Tasmuth1999)
bull Duration of surgery (Kalso 2007)
bull Minimally invasive surgery (Grant 2004)
bull Stitch types (Cerfolio 2003)
bull Nerve damage preservation (Jensen 1985)
Predictive factors for chronic pain after breast surgery
Anderson et al Pain 2015 n=575
Pain at 1 year
bull Moderate- severe post op pain (50)
bull Axillary lymph node with ICB nerve preservation (30)
bull Neuropathic pain 1 week (18)
bull Age lt 65 (18)
Wang Canadian Medical Assoc Journal 2016 bull Young age bull Axillary lymph node dissection bull Acute pain High quality evidence showed no association
with BMI Type of breast surgery Chemotherapy Reconstruction
Clinical Prediction Model and Tool for Assessing Risk of Persistent Pain After Breast Cancer Surgery Tuomo J Meretoja Kenneth Geving Andersen Julie Bruce Lassi Haasio Reetta Sipilauml Neil W Scott Samuli Ripatti Henrik Kehlet and Eija Kalso
March 2017
Risk Factors ndash what can we discuss with surgeons
bull Information for patients
bull Pre-assessment pain clinic
bull Pre-op anaesthetic strategies algorithms PVB
bull Surgical technique ()
(eg mesh preservation of nerves
minimally invasive etc)
bull Enhanced recovery hellip
eg Kehlet et al Br J Surgery 2005
Fast Track Surgery
bull Pain clinic follow up
Pathophysiology lsquowhat is it about pain that causes more painrsquo
lsquohelliptransition to chronicityhelliprsquo
1 Nociceptive inflammation ischaemia oedema pressure traction
2 Neuropathic peripheral amp central sensitisation
spinal cord neuroplasticity
neuroma
3 Psychological amp social
4 Genetic
The neuropathic component in persistent pain after surgery
systematic review Haroutiunian PAIN 2013
CPSP after 11 types of surgery
bull Amount of pain depends
bull on likelihood of nerve damage
Neuropathic pain
bull in 65 of thoracotomy patients
bull 33 groin surgery
bull 6 knee surgery
Post surgical breast pain
Jung PAIN 2003
1 Intercostobrachial neuralgia
2 Other nerve injury
3 Neuroma
4 Phantom breast
Natural History
Long-term follow-up of breast cancer survivors with post-mastectomy pain syndrome
Macdonald et al British J of Cancer 2005
1996helliphellip 43 pain 3 years 2002 hellip21 pain 9 years
Persistent pain after breast surgery 6-year nationwide
follow up
Mejdahl Kehlet et al BMJ 2013
2008hellip47 pain 1 year
2013hellip37 pain 6 years
Treatment - prevention
helliphellipfrom Pre-emptive Analgesia (blocking preoperative stimuli)
helliphellipto Preventative Analgesia (blocking noxious stimuli central sensitisation across the entire perioperative period)
Preventative treatments
1 Nerve blocks Regional
2 Drugs
Regional anaesthesia to prevent chronic pain after surgery a Cochrane systematic review and meta-analysisdagger M H Andreae1 and D A Andreae2
BJA 2013
bull 23 RCTrsquos
bull Epidural anaesthesia and
paravertebral blocks may be effective
in preventing chronic pain at 1 year
bull Effective in about 1 in 4
patients treated
Preincisional Paravertebral Block Reduces the Prevalence of Chronic
Pain After Breast Surgery Kairaluoma et al Anesth Analg 2006103703-708
bull Preincisional paravertebral block provides significant immediate postoperative analgesia
bull In the same patients (n = 60) 12 months sig less pain in the PVB group
bull In addition to providing acute postoperative pain relief preoperative PVB reduces the prevalence of chronic pain 1 yr after breast cancer surgery
Epidurals Intraoperative epidural analgesia provides preventative analgesia in
abdominal surgery Lavandrsquohomme et al Anaesthesiology 2005
bull Clear benefit of epidural in preventing chronic pain 1 year
bull Intraoperative epidural better than postoperative epidural
bull Effective epidural better than effective parenteral only analgesia one year
Systematic review of therapeutic interventions to reduce chronic post surgical pain (32 RCTrsquos)
Humble et al European J of Pain (2015)
POSITIVE
Gabapentinoids
Lidocaine
iv lidocaine EMLA
Regional
TIVA
NEGATIVE
Ketamine
Cryoanalgesia
Local anaesthetic infiltration
Remifentanil (increased chronic pain)
1 Gabapentin around time of surgery
lsquono effect on chronic painrsquo
POSITIVE
NEGATIVE
Meta analysis (Clarke 2012) 48 RCTrsquos positive effect at 2 months
Cochrane Systematic Review (Chaparro 2013) 280 patients analysed pain at 6 months No effect
RCT Gabapentin 1200mg prior to Thyroidectomy Sig less pain at 3 months (Brogley 2008)
RCT Gabapentin vs Placebo Knee replacement No effect on chronic pain (Clarke 2014)
2 Pregabalin ndash around time of surgery lsquoNot a recommended treatment can cause post operative somnolencersquo
Positive
Negative
Meta-analysis of 3 studies (Clarke 2012) All showed improvement in pain 2 RCTrsquoshellipvery large decrease in CPSP (p=0007)
3 unpublished RCTrsquos from Pfizer (2010-2014) hellipall negative for acute and chronic pain i) 307 patients undergoing knee replacement ii) 501 patients hysterectomy iii) 425 patient hernia
Cochrane Systematic Review (Chaparro 2013) 25 RCTrsquos significant benefit
Systematic review (Martinez May 2017) No difference between pregabalin and placebo 3 months Use for acute pain in pro-nociceptive surgery Side effects a problem
Multimodal analgesia
bull Standard protocols now widely used eg Paravertebral blocks at MD Anderson bull Pre-assessment clinic screening for pain psychological factors pain catastrophising scale helliphellipgenetic screening tests bull Education patients surgeons anaesthetists nurses psychologists
General treatment strategies for chronic postsurgical neuropathic pain
Preventative Perkins amp Kehlet Anesthesiology 2000
bullSurgical procedure preservation
sentinel node biopsy
bullBetter postoperative pain management
bullInformed consent preparatory
information
Established Dworkin Archives Neurol 2003 60
1524
bull Amitriptyline
bull Gabapentin
bull Opioids
bull Tramadol
bull 5 Lidoderm patch EMLA
Positive therapies for Prevention of PSBP
1 EMLA applied to chest wall prior
to surgery less pain 3 months
Fassoulaki 2000
2 Venlafaxine XR 70mg before
and for 2 weeks post surgeryno diff
acute pain significantly less chronic
pain 6 months
Reuben 2004
3 Aggressive acute pain
management
Iohom 2006
4 Preincisional paravertebral
block
Kairaluoma 2006
5 Multimodal analgesia with
gabapentin EMLA ropivacaine less
acute pain amp pain 6 months
Fassoulaki 2005
A pain management programme for chronic cancer-
treatment-related pain Robb Williams Duvivier Newham
Journal of Pain 2006775-150
bull Theory of cancer-related pain
bull Pain pathways
bull Overunder activity cycle
bull Pacing
bull Exercise and fitness
bull TENS
bull Posture and manual handling
bull Relapse and prevention
Psychology interventions
bull Goal setting
bull Role of factors involved in pain
bull Homework assignments
bull Relaxation techniques
bull Cognitive skills
bull Relapse and prevention
Results
significant (plt005) improvements in
bull Pain severity
bull Psychological distress
bull Pain amp psychological coping indices
bull Activities of daily living
bull General fitness
Research Proposal
Exercise to prevent shoulder conditions in patients
undergoing breast cancer treatment
bull Aim to conduct a randomised controlled trial (RCT) supported with qualitative research to investigate the clinical and cost-effectiveness of early supervised exercise on outcomes of arm function chronic pain and quality of life at one year in women undergoing treatment for breast cancer
Intervention
bull A physiotherapy-led structured exercise programme incorporating behavioural strategies and monitoring to encourage adherence
bull A minimum of 4 face-to-face specialist treatment sessions with individual participants will be
delivered within 12 weeks of surgery bull Access to interim telephone support will be provided The programme will restrict to controlled early
stretching and ROM exercises with subsequent progression to maintain strength and function (weeks 2 to 12)
bull Qualitative interviews will be used during the feasibility phase of the trial to explore acceptability of
to the intervention
Outcomes
bull arm shoulder and hand function at 12 months using the 30-item Disability Arm Shoulder Hand (DASH) questionnaire
bull quality of life
bull Functional Assessment of Cancer Treatment-Breast (FACT-B)
bull Short-Form-12 and EQ-5D-5L
bull Data on postoperative adverse events surgical site infection and healthcare resource use will be collected at 6 and 12 months after surgery
Positive therapies for Prevention of PSBP
1 EMLA applied to chest wall prior
to surgery less pain 3 months
Fassoulaki 2000
2 Venlafaxine XR 70mg before
and for 2 weeks post surgeryno diff
acute pain significantly less chronic
pain 6 months
Reuben 2004
3 Aggressive acute pain
management
Iohom 2006
4 Preincisional paravertebral
block
Kairaluoma 2006
5 Multimodal analgesia with
gabapentin EMLA ropivacaine less
acute pain amp pain 6 months
Fassoulaki 2005
Current Treatment Paradigms
The Toronto General Hospital
Transitional Pain Service
development and implementation
of a multidisciplinary program
to prevent chronic postsurgical pain (Katz J Pain Res 2015)
bull Nurse navigator
bull Psychologists (ACT)
Clinical Manifestations hellipour approach to the patient with CPSP
bull Type of pain Cause
bull Exclude other causes (infection recurrence)
bull Psychological and social factors
bull Temporal Context
Electronic Patient Record
Future Directions
bull Identify Causative Modifiable risk factors vs Associative risk factors
bull Measure psychological variables
bull Genetic assays to identify genes controlling the variability in developing chronic pain
Aim is lsquoto identify susceptibility to chronic pain and sensitivity to analgesicsrsquo
Chronic pain lsquoheritabilityrsquo is variable
Conclusions
bull 1 year incidence = 05 -10 bull Avoid pain before during and after surgery lsquohelliphelliptranslate advances in acute pain to chronic settinghelliphelliprsquo bull Psychological pre-assessment bull Education discussion with patients surgeons bull In some cases preventive analgesia may be beneficial bull Transitional Pain Servicehelliptrackinghellipdatabase lsquoPragmatic approachrsquo lsquoAll diseases have an acute phasersquo lsquoDrugs good for acute pain must be good for chronic painrsquo

Questions
bull Why is this an important topic bull How big a problem is it bull Why do some people develop the problem and not others bull Clinical manifestations and impact bull Why is Pain predictive of more Pain bull Does the pain get better bull What can we do as Anaesthetists AHPrsquos prevention and
treatment bull What can we discuss with SurgeonsPatients bull What is the way forward
Is this a real problem
amp Why is it important
1 COMMON
bull Once thought to be rare ndash recently reported incidence gt 50 under-recognised misdiagnosed amp neglected
bull Survivor population increasing huge impact for humanitarian medical amp economic reasons
bull Causes additional disability amp psychological distress
bull Chemo- amp radio-therapy additional causes of pain
bull Spectre of recurrent disease
2 PREVENTION
bull New focus on treatment amp prevention
bull Model of lsquoacute to chronicrsquo mechanisms
bull Integration of pain services with other clinical groups
Case Vignette
bull Mrs MB age 45
bull Mastectomy amp axillary dissection RT
bull Presents with severe chronic pain
bull Severe limitation of movement
bull MRI excludes recurrent disease
Pain amp disability
Muscle spasm
Pain
Capsulitis
lsquoCordingrsquo
History Sherman et al PAIN (1984) Chronic phantom pain in 5000 American Veterans 80 pain 1 lasting effect of treatments
Crombie et al PAIN (1998) Cut and Thrust antecedent surgery among patients attending a chronic pain clinic Surgery caused pain in 23 Macrea BJA (1998 2008) Chronic postsurgical pain
Incidence - operations
Type of operation Incidence of chronic pain
No of ops (2006)
1 Amputation 30-50 15000
2 Mastectomy 20-30 18000
3 Thoracotomy 30-60
Heart bypass surgery 30-50 30000
Caesarean section 6 139000
Cholecystectomy 5-50 51000
Hernia 5-35 75000
Laparotomy 30000
Dental root canal surgery (PAIN 2016)
10
Prevalence of chronic pain after breast surgery author year prevalence time
Jamison 1979 44 2 years
Kroner 1989 23 1 year
Vecht 1990 18 6 months
Polinsky 1994 22-32 mean 8 years
Tasmuth 1995 gt50 1 year
Wallace 1996 22- 49 1 year
Smith 1999 43 6 years
Johansen 2000 15 6 years
Fassoulaki 2002 33 3 months
Reuben 2004 50 6 months
Fassoulaki 2005 57 6 months
Kairaluomma 2006 8 1 year
Burton 2007 50 1 year
Hofso 2012 50 1 year
New Definition Old
Macrea BJA 2008 New
Pain April 2017
1 Pain after surgical procedure
1 Pain after a surgical procedure or increases in intensity after a surgical procedure
2 Pain after 2 months 2 Pain after at least 3-6 months hellipwith significant impact on Quality of Life
3 Exclude other causes of the pain
3 Exclude other causes of the pain
4 Exclude pre-existing causes
4 The pain is either a continuation of post surgery pain or develops after an asymptomatic period
5 The pain is either i) localised to the surgical field ii) projected to the innervation territory of a
nerve in the field
Classification of lsquopost mastectomyrsquo pain
1 Pre-existing pain
Osteorheumatoid arthritis Fibromyalgia
Costo-chondritis Cervical radiculopathy
2 Tumour
involvement
Recurrence Metastasis
Cervical radiculopathy due to tumour
3 Post-surgical
Intercostobrachial neuralgia Other neuralgias Persistent lsquoacutersquo pain Scar pain
Phantom breast Intercostal neuromas
Carpal tunnel syndrome Radiation induced plexopathy
Transient brachial neuritis Complex regional pain syndrome
4 Neuropathic
5 Pain due to
implants amp
reconstruction
Capsulitis Capsular contraction and hardening
Foreign body reaction Referred pain Implant migration
Atypical chest pain syndrome Reconstruction lsquoissuesrsquo
6 Other causes
Psychological factors Lymphoedema Pericapsulitis
Muscle spasm lsquoShoulder painrsquo Post-chemo Post- radiotherapy Idiopathic
Myofascial pain dysfunction syndrome
How big a problem is it
In a population of chronic pain patientshelliphow many had pain as a result of surgery Crombie et al Pain 1998 5000 chronic pain patients 23 = CPSP (high proportion with disability) How many people with acute pain go on to get pain at 1 year Hayes et al Acute Pain 2002 5000 patients undergoing surgery Acute neuropathic pain 2 Feature= high intensity 910 Follow up Hayes et al Acute Pain 2002 Pain at 6 months 78 Pain at 1 year 56 lsquo26 million operations year in USA (2008) 1 of all patients develop CPSPrsquo (Katz 2011)
What this study adds bull 3 of patients who had not used opioids previously continued to use them for more than 90 days after major elective surgery bullImportant public health concern because millions of patients undergo major surgery every year
Clarke et al British Medical Journal 2014
Risk factorshellip 1 Causal Modifiable Risk factors (Katz Anesth amp Analg 2011)
Acute pain
Pre-existing pain
Psychological factors
2 Correlated risk factors (Katz Anesth amp Analg 2011)
Younger age
Gender
Psychological distress
Pain
Risk factors
1 Patient related
2 Surgery related
Patient-related risk factors lsquohellippain predicts painrsquo
bull Preoperative pain (Forsythe 2008)
bull Intensity of acute pain (Masselin-Dubois 2013)
bull Acute neuropathic pain (Haroutiounian 2013)
bull High opioid consumption perioperatively (Kalso 2001)
bull Pain in other body parts (Pinto 2012)
bull Younger age (Masselin-Dubois 2013)
bull Female (Ochroch 2006)
Psychological risk factors
bull Pre-op anxiety and catastrophizing meta analysis (2x likelihood of developing CPSP (Theunissen Clin J Pain 2012)
bull Depression (Attal 2014)
bull Catastrophizing (Masselin-Dubois 2013)
bull Sensitivity to pain traumatisation (Page 2013)
bull Anxiety (Kleimann 2011)
bull Fear of long term consequences of surgery (Peters 2007)
Surgical risk factors
bull Low vs high volume surgical unit 13 increase in risk of CPSP (Tasmuth1999)
bull Duration of surgery (Kalso 2007)
bull Minimally invasive surgery (Grant 2004)
bull Stitch types (Cerfolio 2003)
bull Nerve damage preservation (Jensen 1985)
Predictive factors for chronic pain after breast surgery
Anderson et al Pain 2015 n=575
Pain at 1 year
bull Moderate- severe post op pain (50)
bull Axillary lymph node with ICB nerve preservation (30)
bull Neuropathic pain 1 week (18)
bull Age lt 65 (18)
Wang Canadian Medical Assoc Journal 2016 bull Young age bull Axillary lymph node dissection bull Acute pain High quality evidence showed no association
with BMI Type of breast surgery Chemotherapy Reconstruction
Clinical Prediction Model and Tool for Assessing Risk of Persistent Pain After Breast Cancer Surgery Tuomo J Meretoja Kenneth Geving Andersen Julie Bruce Lassi Haasio Reetta Sipilauml Neil W Scott Samuli Ripatti Henrik Kehlet and Eija Kalso
March 2017
Risk Factors ndash what can we discuss with surgeons
bull Information for patients
bull Pre-assessment pain clinic
bull Pre-op anaesthetic strategies algorithms PVB
bull Surgical technique ()
(eg mesh preservation of nerves
minimally invasive etc)
bull Enhanced recovery hellip
eg Kehlet et al Br J Surgery 2005
Fast Track Surgery
bull Pain clinic follow up
Pathophysiology lsquowhat is it about pain that causes more painrsquo
lsquohelliptransition to chronicityhelliprsquo
1 Nociceptive inflammation ischaemia oedema pressure traction
2 Neuropathic peripheral amp central sensitisation
spinal cord neuroplasticity
neuroma
3 Psychological amp social
4 Genetic
The neuropathic component in persistent pain after surgery
systematic review Haroutiunian PAIN 2013
CPSP after 11 types of surgery
bull Amount of pain depends
bull on likelihood of nerve damage
Neuropathic pain
bull in 65 of thoracotomy patients
bull 33 groin surgery
bull 6 knee surgery
Post surgical breast pain
Jung PAIN 2003
1 Intercostobrachial neuralgia
2 Other nerve injury
3 Neuroma
4 Phantom breast
Natural History
Long-term follow-up of breast cancer survivors with post-mastectomy pain syndrome
Macdonald et al British J of Cancer 2005
1996helliphellip 43 pain 3 years 2002 hellip21 pain 9 years
Persistent pain after breast surgery 6-year nationwide
follow up
Mejdahl Kehlet et al BMJ 2013
2008hellip47 pain 1 year
2013hellip37 pain 6 years
Treatment - prevention
helliphellipfrom Pre-emptive Analgesia (blocking preoperative stimuli)
helliphellipto Preventative Analgesia (blocking noxious stimuli central sensitisation across the entire perioperative period)
Preventative treatments
1 Nerve blocks Regional
2 Drugs
Regional anaesthesia to prevent chronic pain after surgery a Cochrane systematic review and meta-analysisdagger M H Andreae1 and D A Andreae2
BJA 2013
bull 23 RCTrsquos
bull Epidural anaesthesia and
paravertebral blocks may be effective
in preventing chronic pain at 1 year
bull Effective in about 1 in 4
patients treated
Preincisional Paravertebral Block Reduces the Prevalence of Chronic
Pain After Breast Surgery Kairaluoma et al Anesth Analg 2006103703-708
bull Preincisional paravertebral block provides significant immediate postoperative analgesia
bull In the same patients (n = 60) 12 months sig less pain in the PVB group
bull In addition to providing acute postoperative pain relief preoperative PVB reduces the prevalence of chronic pain 1 yr after breast cancer surgery
Epidurals Intraoperative epidural analgesia provides preventative analgesia in
abdominal surgery Lavandrsquohomme et al Anaesthesiology 2005
bull Clear benefit of epidural in preventing chronic pain 1 year
bull Intraoperative epidural better than postoperative epidural
bull Effective epidural better than effective parenteral only analgesia one year
Systematic review of therapeutic interventions to reduce chronic post surgical pain (32 RCTrsquos)
Humble et al European J of Pain (2015)
POSITIVE
Gabapentinoids
Lidocaine
iv lidocaine EMLA
Regional
TIVA
NEGATIVE
Ketamine
Cryoanalgesia
Local anaesthetic infiltration
Remifentanil (increased chronic pain)
1 Gabapentin around time of surgery
lsquono effect on chronic painrsquo
POSITIVE
NEGATIVE
Meta analysis (Clarke 2012) 48 RCTrsquos positive effect at 2 months
Cochrane Systematic Review (Chaparro 2013) 280 patients analysed pain at 6 months No effect
RCT Gabapentin 1200mg prior to Thyroidectomy Sig less pain at 3 months (Brogley 2008)
RCT Gabapentin vs Placebo Knee replacement No effect on chronic pain (Clarke 2014)
2 Pregabalin ndash around time of surgery lsquoNot a recommended treatment can cause post operative somnolencersquo
Positive
Negative
Meta-analysis of 3 studies (Clarke 2012) All showed improvement in pain 2 RCTrsquoshellipvery large decrease in CPSP (p=0007)
3 unpublished RCTrsquos from Pfizer (2010-2014) hellipall negative for acute and chronic pain i) 307 patients undergoing knee replacement ii) 501 patients hysterectomy iii) 425 patient hernia
Cochrane Systematic Review (Chaparro 2013) 25 RCTrsquos significant benefit
Systematic review (Martinez May 2017) No difference between pregabalin and placebo 3 months Use for acute pain in pro-nociceptive surgery Side effects a problem
Multimodal analgesia
bull Standard protocols now widely used eg Paravertebral blocks at MD Anderson bull Pre-assessment clinic screening for pain psychological factors pain catastrophising scale helliphellipgenetic screening tests bull Education patients surgeons anaesthetists nurses psychologists
General treatment strategies for chronic postsurgical neuropathic pain
Preventative Perkins amp Kehlet Anesthesiology 2000
bullSurgical procedure preservation
sentinel node biopsy
bullBetter postoperative pain management
bullInformed consent preparatory
information
Established Dworkin Archives Neurol 2003 60
1524
bull Amitriptyline
bull Gabapentin
bull Opioids
bull Tramadol
bull 5 Lidoderm patch EMLA
Positive therapies for Prevention of PSBP
1 EMLA applied to chest wall prior
to surgery less pain 3 months
Fassoulaki 2000
2 Venlafaxine XR 70mg before
and for 2 weeks post surgeryno diff
acute pain significantly less chronic
pain 6 months
Reuben 2004
3 Aggressive acute pain
management
Iohom 2006
4 Preincisional paravertebral
block
Kairaluoma 2006
5 Multimodal analgesia with
gabapentin EMLA ropivacaine less
acute pain amp pain 6 months
Fassoulaki 2005
A pain management programme for chronic cancer-
treatment-related pain Robb Williams Duvivier Newham
Journal of Pain 2006775-150
bull Theory of cancer-related pain
bull Pain pathways
bull Overunder activity cycle
bull Pacing
bull Exercise and fitness
bull TENS
bull Posture and manual handling
bull Relapse and prevention
Psychology interventions
bull Goal setting
bull Role of factors involved in pain
bull Homework assignments
bull Relaxation techniques
bull Cognitive skills
bull Relapse and prevention
Results
significant (plt005) improvements in
bull Pain severity
bull Psychological distress
bull Pain amp psychological coping indices
bull Activities of daily living
bull General fitness
Research Proposal
Exercise to prevent shoulder conditions in patients
undergoing breast cancer treatment
bull Aim to conduct a randomised controlled trial (RCT) supported with qualitative research to investigate the clinical and cost-effectiveness of early supervised exercise on outcomes of arm function chronic pain and quality of life at one year in women undergoing treatment for breast cancer
Intervention
bull A physiotherapy-led structured exercise programme incorporating behavioural strategies and monitoring to encourage adherence
bull A minimum of 4 face-to-face specialist treatment sessions with individual participants will be
delivered within 12 weeks of surgery bull Access to interim telephone support will be provided The programme will restrict to controlled early
stretching and ROM exercises with subsequent progression to maintain strength and function (weeks 2 to 12)
bull Qualitative interviews will be used during the feasibility phase of the trial to explore acceptability of
to the intervention
Outcomes
bull arm shoulder and hand function at 12 months using the 30-item Disability Arm Shoulder Hand (DASH) questionnaire
bull quality of life
bull Functional Assessment of Cancer Treatment-Breast (FACT-B)
bull Short-Form-12 and EQ-5D-5L
bull Data on postoperative adverse events surgical site infection and healthcare resource use will be collected at 6 and 12 months after surgery
Positive therapies for Prevention of PSBP
1 EMLA applied to chest wall prior
to surgery less pain 3 months
Fassoulaki 2000
2 Venlafaxine XR 70mg before
and for 2 weeks post surgeryno diff
acute pain significantly less chronic
pain 6 months
Reuben 2004
3 Aggressive acute pain
management
Iohom 2006
4 Preincisional paravertebral
block
Kairaluoma 2006
5 Multimodal analgesia with
gabapentin EMLA ropivacaine less
acute pain amp pain 6 months
Fassoulaki 2005
Current Treatment Paradigms
The Toronto General Hospital
Transitional Pain Service
development and implementation
of a multidisciplinary program
to prevent chronic postsurgical pain (Katz J Pain Res 2015)
bull Nurse navigator
bull Psychologists (ACT)
Clinical Manifestations hellipour approach to the patient with CPSP
bull Type of pain Cause
bull Exclude other causes (infection recurrence)
bull Psychological and social factors
bull Temporal Context
Electronic Patient Record
Future Directions
bull Identify Causative Modifiable risk factors vs Associative risk factors
bull Measure psychological variables
bull Genetic assays to identify genes controlling the variability in developing chronic pain
Aim is lsquoto identify susceptibility to chronic pain and sensitivity to analgesicsrsquo
Chronic pain lsquoheritabilityrsquo is variable
Conclusions
bull 1 year incidence = 05 -10 bull Avoid pain before during and after surgery lsquohelliphelliptranslate advances in acute pain to chronic settinghelliphelliprsquo bull Psychological pre-assessment bull Education discussion with patients surgeons bull In some cases preventive analgesia may be beneficial bull Transitional Pain Servicehelliptrackinghellipdatabase lsquoPragmatic approachrsquo lsquoAll diseases have an acute phasersquo lsquoDrugs good for acute pain must be good for chronic painrsquo

Is this a real problem
amp Why is it important
1 COMMON
bull Once thought to be rare ndash recently reported incidence gt 50 under-recognised misdiagnosed amp neglected
bull Survivor population increasing huge impact for humanitarian medical amp economic reasons
bull Causes additional disability amp psychological distress
bull Chemo- amp radio-therapy additional causes of pain
bull Spectre of recurrent disease
2 PREVENTION
bull New focus on treatment amp prevention
bull Model of lsquoacute to chronicrsquo mechanisms
bull Integration of pain services with other clinical groups
Case Vignette
bull Mrs MB age 45
bull Mastectomy amp axillary dissection RT
bull Presents with severe chronic pain
bull Severe limitation of movement
bull MRI excludes recurrent disease
Pain amp disability
Muscle spasm
Pain
Capsulitis
lsquoCordingrsquo
History Sherman et al PAIN (1984) Chronic phantom pain in 5000 American Veterans 80 pain 1 lasting effect of treatments
Crombie et al PAIN (1998) Cut and Thrust antecedent surgery among patients attending a chronic pain clinic Surgery caused pain in 23 Macrea BJA (1998 2008) Chronic postsurgical pain
Incidence - operations
Type of operation Incidence of chronic pain
No of ops (2006)
1 Amputation 30-50 15000
2 Mastectomy 20-30 18000
3 Thoracotomy 30-60
Heart bypass surgery 30-50 30000
Caesarean section 6 139000
Cholecystectomy 5-50 51000
Hernia 5-35 75000
Laparotomy 30000
Dental root canal surgery (PAIN 2016)
10
Prevalence of chronic pain after breast surgery author year prevalence time
Jamison 1979 44 2 years
Kroner 1989 23 1 year
Vecht 1990 18 6 months
Polinsky 1994 22-32 mean 8 years
Tasmuth 1995 gt50 1 year
Wallace 1996 22- 49 1 year
Smith 1999 43 6 years
Johansen 2000 15 6 years
Fassoulaki 2002 33 3 months
Reuben 2004 50 6 months
Fassoulaki 2005 57 6 months
Kairaluomma 2006 8 1 year
Burton 2007 50 1 year
Hofso 2012 50 1 year
New Definition Old
Macrea BJA 2008 New
Pain April 2017
1 Pain after surgical procedure
1 Pain after a surgical procedure or increases in intensity after a surgical procedure
2 Pain after 2 months 2 Pain after at least 3-6 months hellipwith significant impact on Quality of Life
3 Exclude other causes of the pain
3 Exclude other causes of the pain
4 Exclude pre-existing causes
4 The pain is either a continuation of post surgery pain or develops after an asymptomatic period
5 The pain is either i) localised to the surgical field ii) projected to the innervation territory of a
nerve in the field
Classification of lsquopost mastectomyrsquo pain
1 Pre-existing pain
Osteorheumatoid arthritis Fibromyalgia
Costo-chondritis Cervical radiculopathy
2 Tumour
involvement
Recurrence Metastasis
Cervical radiculopathy due to tumour
3 Post-surgical
Intercostobrachial neuralgia Other neuralgias Persistent lsquoacutersquo pain Scar pain
Phantom breast Intercostal neuromas
Carpal tunnel syndrome Radiation induced plexopathy
Transient brachial neuritis Complex regional pain syndrome
4 Neuropathic
5 Pain due to
implants amp
reconstruction
Capsulitis Capsular contraction and hardening
Foreign body reaction Referred pain Implant migration
Atypical chest pain syndrome Reconstruction lsquoissuesrsquo
6 Other causes
Psychological factors Lymphoedema Pericapsulitis
Muscle spasm lsquoShoulder painrsquo Post-chemo Post- radiotherapy Idiopathic
Myofascial pain dysfunction syndrome
How big a problem is it
In a population of chronic pain patientshelliphow many had pain as a result of surgery Crombie et al Pain 1998 5000 chronic pain patients 23 = CPSP (high proportion with disability) How many people with acute pain go on to get pain at 1 year Hayes et al Acute Pain 2002 5000 patients undergoing surgery Acute neuropathic pain 2 Feature= high intensity 910 Follow up Hayes et al Acute Pain 2002 Pain at 6 months 78 Pain at 1 year 56 lsquo26 million operations year in USA (2008) 1 of all patients develop CPSPrsquo (Katz 2011)
What this study adds bull 3 of patients who had not used opioids previously continued to use them for more than 90 days after major elective surgery bullImportant public health concern because millions of patients undergo major surgery every year
Clarke et al British Medical Journal 2014
Risk factorshellip 1 Causal Modifiable Risk factors (Katz Anesth amp Analg 2011)
Acute pain
Pre-existing pain
Psychological factors
2 Correlated risk factors (Katz Anesth amp Analg 2011)
Younger age
Gender
Psychological distress
Pain
Risk factors
1 Patient related
2 Surgery related
Patient-related risk factors lsquohellippain predicts painrsquo
bull Preoperative pain (Forsythe 2008)
bull Intensity of acute pain (Masselin-Dubois 2013)
bull Acute neuropathic pain (Haroutiounian 2013)
bull High opioid consumption perioperatively (Kalso 2001)
bull Pain in other body parts (Pinto 2012)
bull Younger age (Masselin-Dubois 2013)
bull Female (Ochroch 2006)
Psychological risk factors
bull Pre-op anxiety and catastrophizing meta analysis (2x likelihood of developing CPSP (Theunissen Clin J Pain 2012)
bull Depression (Attal 2014)
bull Catastrophizing (Masselin-Dubois 2013)
bull Sensitivity to pain traumatisation (Page 2013)
bull Anxiety (Kleimann 2011)
bull Fear of long term consequences of surgery (Peters 2007)
Surgical risk factors
bull Low vs high volume surgical unit 13 increase in risk of CPSP (Tasmuth1999)
bull Duration of surgery (Kalso 2007)
bull Minimally invasive surgery (Grant 2004)
bull Stitch types (Cerfolio 2003)
bull Nerve damage preservation (Jensen 1985)
Predictive factors for chronic pain after breast surgery
Anderson et al Pain 2015 n=575
Pain at 1 year
bull Moderate- severe post op pain (50)
bull Axillary lymph node with ICB nerve preservation (30)
bull Neuropathic pain 1 week (18)
bull Age lt 65 (18)
Wang Canadian Medical Assoc Journal 2016 bull Young age bull Axillary lymph node dissection bull Acute pain High quality evidence showed no association
with BMI Type of breast surgery Chemotherapy Reconstruction
Clinical Prediction Model and Tool for Assessing Risk of Persistent Pain After Breast Cancer Surgery Tuomo J Meretoja Kenneth Geving Andersen Julie Bruce Lassi Haasio Reetta Sipilauml Neil W Scott Samuli Ripatti Henrik Kehlet and Eija Kalso
March 2017
Risk Factors ndash what can we discuss with surgeons
bull Information for patients
bull Pre-assessment pain clinic
bull Pre-op anaesthetic strategies algorithms PVB
bull Surgical technique ()
(eg mesh preservation of nerves
minimally invasive etc)
bull Enhanced recovery hellip
eg Kehlet et al Br J Surgery 2005
Fast Track Surgery
bull Pain clinic follow up
Pathophysiology lsquowhat is it about pain that causes more painrsquo
lsquohelliptransition to chronicityhelliprsquo
1 Nociceptive inflammation ischaemia oedema pressure traction
2 Neuropathic peripheral amp central sensitisation
spinal cord neuroplasticity
neuroma
3 Psychological amp social
4 Genetic
The neuropathic component in persistent pain after surgery
systematic review Haroutiunian PAIN 2013
CPSP after 11 types of surgery
bull Amount of pain depends
bull on likelihood of nerve damage
Neuropathic pain
bull in 65 of thoracotomy patients
bull 33 groin surgery
bull 6 knee surgery
Post surgical breast pain
Jung PAIN 2003
1 Intercostobrachial neuralgia
2 Other nerve injury
3 Neuroma
4 Phantom breast
Natural History
Long-term follow-up of breast cancer survivors with post-mastectomy pain syndrome
Macdonald et al British J of Cancer 2005
1996helliphellip 43 pain 3 years 2002 hellip21 pain 9 years
Persistent pain after breast surgery 6-year nationwide
follow up
Mejdahl Kehlet et al BMJ 2013
2008hellip47 pain 1 year
2013hellip37 pain 6 years
Treatment - prevention
helliphellipfrom Pre-emptive Analgesia (blocking preoperative stimuli)
helliphellipto Preventative Analgesia (blocking noxious stimuli central sensitisation across the entire perioperative period)
Preventative treatments
1 Nerve blocks Regional
2 Drugs
Regional anaesthesia to prevent chronic pain after surgery a Cochrane systematic review and meta-analysisdagger M H Andreae1 and D A Andreae2
BJA 2013
bull 23 RCTrsquos
bull Epidural anaesthesia and
paravertebral blocks may be effective
in preventing chronic pain at 1 year
bull Effective in about 1 in 4
patients treated
Preincisional Paravertebral Block Reduces the Prevalence of Chronic
Pain After Breast Surgery Kairaluoma et al Anesth Analg 2006103703-708
bull Preincisional paravertebral block provides significant immediate postoperative analgesia
bull In the same patients (n = 60) 12 months sig less pain in the PVB group
bull In addition to providing acute postoperative pain relief preoperative PVB reduces the prevalence of chronic pain 1 yr after breast cancer surgery
Epidurals Intraoperative epidural analgesia provides preventative analgesia in
abdominal surgery Lavandrsquohomme et al Anaesthesiology 2005
bull Clear benefit of epidural in preventing chronic pain 1 year
bull Intraoperative epidural better than postoperative epidural
bull Effective epidural better than effective parenteral only analgesia one year
Systematic review of therapeutic interventions to reduce chronic post surgical pain (32 RCTrsquos)
Humble et al European J of Pain (2015)
POSITIVE
Gabapentinoids
Lidocaine
iv lidocaine EMLA
Regional
TIVA
NEGATIVE
Ketamine
Cryoanalgesia
Local anaesthetic infiltration
Remifentanil (increased chronic pain)
1 Gabapentin around time of surgery
lsquono effect on chronic painrsquo
POSITIVE
NEGATIVE
Meta analysis (Clarke 2012) 48 RCTrsquos positive effect at 2 months
Cochrane Systematic Review (Chaparro 2013) 280 patients analysed pain at 6 months No effect
RCT Gabapentin 1200mg prior to Thyroidectomy Sig less pain at 3 months (Brogley 2008)
RCT Gabapentin vs Placebo Knee replacement No effect on chronic pain (Clarke 2014)
2 Pregabalin ndash around time of surgery lsquoNot a recommended treatment can cause post operative somnolencersquo
Positive
Negative
Meta-analysis of 3 studies (Clarke 2012) All showed improvement in pain 2 RCTrsquoshellipvery large decrease in CPSP (p=0007)
3 unpublished RCTrsquos from Pfizer (2010-2014) hellipall negative for acute and chronic pain i) 307 patients undergoing knee replacement ii) 501 patients hysterectomy iii) 425 patient hernia
Cochrane Systematic Review (Chaparro 2013) 25 RCTrsquos significant benefit
Systematic review (Martinez May 2017) No difference between pregabalin and placebo 3 months Use for acute pain in pro-nociceptive surgery Side effects a problem
Multimodal analgesia
bull Standard protocols now widely used eg Paravertebral blocks at MD Anderson bull Pre-assessment clinic screening for pain psychological factors pain catastrophising scale helliphellipgenetic screening tests bull Education patients surgeons anaesthetists nurses psychologists
General treatment strategies for chronic postsurgical neuropathic pain
Preventative Perkins amp Kehlet Anesthesiology 2000
bullSurgical procedure preservation
sentinel node biopsy
bullBetter postoperative pain management
bullInformed consent preparatory
information
Established Dworkin Archives Neurol 2003 60
1524
bull Amitriptyline
bull Gabapentin
bull Opioids
bull Tramadol
bull 5 Lidoderm patch EMLA
Positive therapies for Prevention of PSBP
1 EMLA applied to chest wall prior
to surgery less pain 3 months
Fassoulaki 2000
2 Venlafaxine XR 70mg before
and for 2 weeks post surgeryno diff
acute pain significantly less chronic
pain 6 months
Reuben 2004
3 Aggressive acute pain
management
Iohom 2006
4 Preincisional paravertebral
block
Kairaluoma 2006
5 Multimodal analgesia with
gabapentin EMLA ropivacaine less
acute pain amp pain 6 months
Fassoulaki 2005
A pain management programme for chronic cancer-
treatment-related pain Robb Williams Duvivier Newham
Journal of Pain 2006775-150
bull Theory of cancer-related pain
bull Pain pathways
bull Overunder activity cycle
bull Pacing
bull Exercise and fitness
bull TENS
bull Posture and manual handling
bull Relapse and prevention
Psychology interventions
bull Goal setting
bull Role of factors involved in pain
bull Homework assignments
bull Relaxation techniques
bull Cognitive skills
bull Relapse and prevention
Results
significant (plt005) improvements in
bull Pain severity
bull Psychological distress
bull Pain amp psychological coping indices
bull Activities of daily living
bull General fitness
Research Proposal
Exercise to prevent shoulder conditions in patients
undergoing breast cancer treatment
bull Aim to conduct a randomised controlled trial (RCT) supported with qualitative research to investigate the clinical and cost-effectiveness of early supervised exercise on outcomes of arm function chronic pain and quality of life at one year in women undergoing treatment for breast cancer
Intervention
bull A physiotherapy-led structured exercise programme incorporating behavioural strategies and monitoring to encourage adherence
bull A minimum of 4 face-to-face specialist treatment sessions with individual participants will be
delivered within 12 weeks of surgery bull Access to interim telephone support will be provided The programme will restrict to controlled early
stretching and ROM exercises with subsequent progression to maintain strength and function (weeks 2 to 12)
bull Qualitative interviews will be used during the feasibility phase of the trial to explore acceptability of
to the intervention
Outcomes
bull arm shoulder and hand function at 12 months using the 30-item Disability Arm Shoulder Hand (DASH) questionnaire
bull quality of life
bull Functional Assessment of Cancer Treatment-Breast (FACT-B)
bull Short-Form-12 and EQ-5D-5L
bull Data on postoperative adverse events surgical site infection and healthcare resource use will be collected at 6 and 12 months after surgery
Positive therapies for Prevention of PSBP
1 EMLA applied to chest wall prior
to surgery less pain 3 months
Fassoulaki 2000
2 Venlafaxine XR 70mg before
and for 2 weeks post surgeryno diff
acute pain significantly less chronic
pain 6 months
Reuben 2004
3 Aggressive acute pain
management
Iohom 2006
4 Preincisional paravertebral
block
Kairaluoma 2006
5 Multimodal analgesia with
gabapentin EMLA ropivacaine less
acute pain amp pain 6 months
Fassoulaki 2005
Current Treatment Paradigms
The Toronto General Hospital
Transitional Pain Service
development and implementation
of a multidisciplinary program
to prevent chronic postsurgical pain (Katz J Pain Res 2015)
bull Nurse navigator
bull Psychologists (ACT)
Clinical Manifestations hellipour approach to the patient with CPSP
bull Type of pain Cause
bull Exclude other causes (infection recurrence)
bull Psychological and social factors
bull Temporal Context
Electronic Patient Record
Future Directions
bull Identify Causative Modifiable risk factors vs Associative risk factors
bull Measure psychological variables
bull Genetic assays to identify genes controlling the variability in developing chronic pain
Aim is lsquoto identify susceptibility to chronic pain and sensitivity to analgesicsrsquo
Chronic pain lsquoheritabilityrsquo is variable
Conclusions
bull 1 year incidence = 05 -10 bull Avoid pain before during and after surgery lsquohelliphelliptranslate advances in acute pain to chronic settinghelliphelliprsquo bull Psychological pre-assessment bull Education discussion with patients surgeons bull In some cases preventive analgesia may be beneficial bull Transitional Pain Servicehelliptrackinghellipdatabase lsquoPragmatic approachrsquo lsquoAll diseases have an acute phasersquo lsquoDrugs good for acute pain must be good for chronic painrsquo

Case Vignette
bull Mrs MB age 45
bull Mastectomy amp axillary dissection RT
bull Presents with severe chronic pain
bull Severe limitation of movement
bull MRI excludes recurrent disease
Pain amp disability
Muscle spasm
Pain
Capsulitis
lsquoCordingrsquo
History Sherman et al PAIN (1984) Chronic phantom pain in 5000 American Veterans 80 pain 1 lasting effect of treatments
Crombie et al PAIN (1998) Cut and Thrust antecedent surgery among patients attending a chronic pain clinic Surgery caused pain in 23 Macrea BJA (1998 2008) Chronic postsurgical pain
Incidence - operations
Type of operation Incidence of chronic pain
No of ops (2006)
1 Amputation 30-50 15000
2 Mastectomy 20-30 18000
3 Thoracotomy 30-60
Heart bypass surgery 30-50 30000
Caesarean section 6 139000
Cholecystectomy 5-50 51000
Hernia 5-35 75000
Laparotomy 30000
Dental root canal surgery (PAIN 2016)
10
Prevalence of chronic pain after breast surgery author year prevalence time
Jamison 1979 44 2 years
Kroner 1989 23 1 year
Vecht 1990 18 6 months
Polinsky 1994 22-32 mean 8 years
Tasmuth 1995 gt50 1 year
Wallace 1996 22- 49 1 year
Smith 1999 43 6 years
Johansen 2000 15 6 years
Fassoulaki 2002 33 3 months
Reuben 2004 50 6 months
Fassoulaki 2005 57 6 months
Kairaluomma 2006 8 1 year
Burton 2007 50 1 year
Hofso 2012 50 1 year
New Definition Old
Macrea BJA 2008 New
Pain April 2017
1 Pain after surgical procedure
1 Pain after a surgical procedure or increases in intensity after a surgical procedure
2 Pain after 2 months 2 Pain after at least 3-6 months hellipwith significant impact on Quality of Life
3 Exclude other causes of the pain
3 Exclude other causes of the pain
4 Exclude pre-existing causes
4 The pain is either a continuation of post surgery pain or develops after an asymptomatic period
5 The pain is either i) localised to the surgical field ii) projected to the innervation territory of a
nerve in the field
Classification of lsquopost mastectomyrsquo pain
1 Pre-existing pain
Osteorheumatoid arthritis Fibromyalgia
Costo-chondritis Cervical radiculopathy
2 Tumour
involvement
Recurrence Metastasis
Cervical radiculopathy due to tumour
3 Post-surgical
Intercostobrachial neuralgia Other neuralgias Persistent lsquoacutersquo pain Scar pain
Phantom breast Intercostal neuromas
Carpal tunnel syndrome Radiation induced plexopathy
Transient brachial neuritis Complex regional pain syndrome
4 Neuropathic
5 Pain due to
implants amp
reconstruction
Capsulitis Capsular contraction and hardening
Foreign body reaction Referred pain Implant migration
Atypical chest pain syndrome Reconstruction lsquoissuesrsquo
6 Other causes
Psychological factors Lymphoedema Pericapsulitis
Muscle spasm lsquoShoulder painrsquo Post-chemo Post- radiotherapy Idiopathic
Myofascial pain dysfunction syndrome
How big a problem is it
In a population of chronic pain patientshelliphow many had pain as a result of surgery Crombie et al Pain 1998 5000 chronic pain patients 23 = CPSP (high proportion with disability) How many people with acute pain go on to get pain at 1 year Hayes et al Acute Pain 2002 5000 patients undergoing surgery Acute neuropathic pain 2 Feature= high intensity 910 Follow up Hayes et al Acute Pain 2002 Pain at 6 months 78 Pain at 1 year 56 lsquo26 million operations year in USA (2008) 1 of all patients develop CPSPrsquo (Katz 2011)
What this study adds bull 3 of patients who had not used opioids previously continued to use them for more than 90 days after major elective surgery bullImportant public health concern because millions of patients undergo major surgery every year
Clarke et al British Medical Journal 2014
Risk factorshellip 1 Causal Modifiable Risk factors (Katz Anesth amp Analg 2011)
Acute pain
Pre-existing pain
Psychological factors
2 Correlated risk factors (Katz Anesth amp Analg 2011)
Younger age
Gender
Psychological distress
Pain
Risk factors
1 Patient related
2 Surgery related
Patient-related risk factors lsquohellippain predicts painrsquo
bull Preoperative pain (Forsythe 2008)
bull Intensity of acute pain (Masselin-Dubois 2013)
bull Acute neuropathic pain (Haroutiounian 2013)
bull High opioid consumption perioperatively (Kalso 2001)
bull Pain in other body parts (Pinto 2012)
bull Younger age (Masselin-Dubois 2013)
bull Female (Ochroch 2006)
Psychological risk factors
bull Pre-op anxiety and catastrophizing meta analysis (2x likelihood of developing CPSP (Theunissen Clin J Pain 2012)
bull Depression (Attal 2014)
bull Catastrophizing (Masselin-Dubois 2013)
bull Sensitivity to pain traumatisation (Page 2013)
bull Anxiety (Kleimann 2011)
bull Fear of long term consequences of surgery (Peters 2007)
Surgical risk factors
bull Low vs high volume surgical unit 13 increase in risk of CPSP (Tasmuth1999)
bull Duration of surgery (Kalso 2007)
bull Minimally invasive surgery (Grant 2004)
bull Stitch types (Cerfolio 2003)
bull Nerve damage preservation (Jensen 1985)
Predictive factors for chronic pain after breast surgery
Anderson et al Pain 2015 n=575
Pain at 1 year
bull Moderate- severe post op pain (50)
bull Axillary lymph node with ICB nerve preservation (30)
bull Neuropathic pain 1 week (18)
bull Age lt 65 (18)
Wang Canadian Medical Assoc Journal 2016 bull Young age bull Axillary lymph node dissection bull Acute pain High quality evidence showed no association
with BMI Type of breast surgery Chemotherapy Reconstruction
Clinical Prediction Model and Tool for Assessing Risk of Persistent Pain After Breast Cancer Surgery Tuomo J Meretoja Kenneth Geving Andersen Julie Bruce Lassi Haasio Reetta Sipilauml Neil W Scott Samuli Ripatti Henrik Kehlet and Eija Kalso
March 2017
Risk Factors ndash what can we discuss with surgeons
bull Information for patients
bull Pre-assessment pain clinic
bull Pre-op anaesthetic strategies algorithms PVB
bull Surgical technique ()
(eg mesh preservation of nerves
minimally invasive etc)
bull Enhanced recovery hellip
eg Kehlet et al Br J Surgery 2005
Fast Track Surgery
bull Pain clinic follow up
Pathophysiology lsquowhat is it about pain that causes more painrsquo
lsquohelliptransition to chronicityhelliprsquo
1 Nociceptive inflammation ischaemia oedema pressure traction
2 Neuropathic peripheral amp central sensitisation
spinal cord neuroplasticity
neuroma
3 Psychological amp social
4 Genetic
The neuropathic component in persistent pain after surgery
systematic review Haroutiunian PAIN 2013
CPSP after 11 types of surgery
bull Amount of pain depends
bull on likelihood of nerve damage
Neuropathic pain
bull in 65 of thoracotomy patients
bull 33 groin surgery
bull 6 knee surgery
Post surgical breast pain
Jung PAIN 2003
1 Intercostobrachial neuralgia
2 Other nerve injury
3 Neuroma
4 Phantom breast
Natural History
Long-term follow-up of breast cancer survivors with post-mastectomy pain syndrome
Macdonald et al British J of Cancer 2005
1996helliphellip 43 pain 3 years 2002 hellip21 pain 9 years
Persistent pain after breast surgery 6-year nationwide
follow up
Mejdahl Kehlet et al BMJ 2013
2008hellip47 pain 1 year
2013hellip37 pain 6 years
Treatment - prevention
helliphellipfrom Pre-emptive Analgesia (blocking preoperative stimuli)
helliphellipto Preventative Analgesia (blocking noxious stimuli central sensitisation across the entire perioperative period)
Preventative treatments
1 Nerve blocks Regional
2 Drugs
Regional anaesthesia to prevent chronic pain after surgery a Cochrane systematic review and meta-analysisdagger M H Andreae1 and D A Andreae2
BJA 2013
bull 23 RCTrsquos
bull Epidural anaesthesia and
paravertebral blocks may be effective
in preventing chronic pain at 1 year
bull Effective in about 1 in 4
patients treated
Preincisional Paravertebral Block Reduces the Prevalence of Chronic
Pain After Breast Surgery Kairaluoma et al Anesth Analg 2006103703-708
bull Preincisional paravertebral block provides significant immediate postoperative analgesia
bull In the same patients (n = 60) 12 months sig less pain in the PVB group
bull In addition to providing acute postoperative pain relief preoperative PVB reduces the prevalence of chronic pain 1 yr after breast cancer surgery
Epidurals Intraoperative epidural analgesia provides preventative analgesia in
abdominal surgery Lavandrsquohomme et al Anaesthesiology 2005
bull Clear benefit of epidural in preventing chronic pain 1 year
bull Intraoperative epidural better than postoperative epidural
bull Effective epidural better than effective parenteral only analgesia one year
Systematic review of therapeutic interventions to reduce chronic post surgical pain (32 RCTrsquos)
Humble et al European J of Pain (2015)
POSITIVE
Gabapentinoids
Lidocaine
iv lidocaine EMLA
Regional
TIVA
NEGATIVE
Ketamine
Cryoanalgesia
Local anaesthetic infiltration
Remifentanil (increased chronic pain)
1 Gabapentin around time of surgery
lsquono effect on chronic painrsquo
POSITIVE
NEGATIVE
Meta analysis (Clarke 2012) 48 RCTrsquos positive effect at 2 months
Cochrane Systematic Review (Chaparro 2013) 280 patients analysed pain at 6 months No effect
RCT Gabapentin 1200mg prior to Thyroidectomy Sig less pain at 3 months (Brogley 2008)
RCT Gabapentin vs Placebo Knee replacement No effect on chronic pain (Clarke 2014)
2 Pregabalin ndash around time of surgery lsquoNot a recommended treatment can cause post operative somnolencersquo
Positive
Negative
Meta-analysis of 3 studies (Clarke 2012) All showed improvement in pain 2 RCTrsquoshellipvery large decrease in CPSP (p=0007)
3 unpublished RCTrsquos from Pfizer (2010-2014) hellipall negative for acute and chronic pain i) 307 patients undergoing knee replacement ii) 501 patients hysterectomy iii) 425 patient hernia
Cochrane Systematic Review (Chaparro 2013) 25 RCTrsquos significant benefit
Systematic review (Martinez May 2017) No difference between pregabalin and placebo 3 months Use for acute pain in pro-nociceptive surgery Side effects a problem
Multimodal analgesia
bull Standard protocols now widely used eg Paravertebral blocks at MD Anderson bull Pre-assessment clinic screening for pain psychological factors pain catastrophising scale helliphellipgenetic screening tests bull Education patients surgeons anaesthetists nurses psychologists
General treatment strategies for chronic postsurgical neuropathic pain
Preventative Perkins amp Kehlet Anesthesiology 2000
bullSurgical procedure preservation
sentinel node biopsy
bullBetter postoperative pain management
bullInformed consent preparatory
information
Established Dworkin Archives Neurol 2003 60
1524
bull Amitriptyline
bull Gabapentin
bull Opioids
bull Tramadol
bull 5 Lidoderm patch EMLA
Positive therapies for Prevention of PSBP
1 EMLA applied to chest wall prior
to surgery less pain 3 months
Fassoulaki 2000
2 Venlafaxine XR 70mg before
and for 2 weeks post surgeryno diff
acute pain significantly less chronic
pain 6 months
Reuben 2004
3 Aggressive acute pain
management
Iohom 2006
4 Preincisional paravertebral
block
Kairaluoma 2006
5 Multimodal analgesia with
gabapentin EMLA ropivacaine less
acute pain amp pain 6 months
Fassoulaki 2005
A pain management programme for chronic cancer-
treatment-related pain Robb Williams Duvivier Newham
Journal of Pain 2006775-150
bull Theory of cancer-related pain
bull Pain pathways
bull Overunder activity cycle
bull Pacing
bull Exercise and fitness
bull TENS
bull Posture and manual handling
bull Relapse and prevention
Psychology interventions
bull Goal setting
bull Role of factors involved in pain
bull Homework assignments
bull Relaxation techniques
bull Cognitive skills
bull Relapse and prevention
Results
significant (plt005) improvements in
bull Pain severity
bull Psychological distress
bull Pain amp psychological coping indices
bull Activities of daily living
bull General fitness
Research Proposal
Exercise to prevent shoulder conditions in patients
undergoing breast cancer treatment
bull Aim to conduct a randomised controlled trial (RCT) supported with qualitative research to investigate the clinical and cost-effectiveness of early supervised exercise on outcomes of arm function chronic pain and quality of life at one year in women undergoing treatment for breast cancer
Intervention
bull A physiotherapy-led structured exercise programme incorporating behavioural strategies and monitoring to encourage adherence
bull A minimum of 4 face-to-face specialist treatment sessions with individual participants will be
delivered within 12 weeks of surgery bull Access to interim telephone support will be provided The programme will restrict to controlled early
stretching and ROM exercises with subsequent progression to maintain strength and function (weeks 2 to 12)
bull Qualitative interviews will be used during the feasibility phase of the trial to explore acceptability of
to the intervention
Outcomes
bull arm shoulder and hand function at 12 months using the 30-item Disability Arm Shoulder Hand (DASH) questionnaire
bull quality of life
bull Functional Assessment of Cancer Treatment-Breast (FACT-B)
bull Short-Form-12 and EQ-5D-5L
bull Data on postoperative adverse events surgical site infection and healthcare resource use will be collected at 6 and 12 months after surgery
Positive therapies for Prevention of PSBP
1 EMLA applied to chest wall prior
to surgery less pain 3 months
Fassoulaki 2000
2 Venlafaxine XR 70mg before
and for 2 weeks post surgeryno diff
acute pain significantly less chronic
pain 6 months
Reuben 2004
3 Aggressive acute pain
management
Iohom 2006
4 Preincisional paravertebral
block
Kairaluoma 2006
5 Multimodal analgesia with
gabapentin EMLA ropivacaine less
acute pain amp pain 6 months
Fassoulaki 2005
Current Treatment Paradigms
The Toronto General Hospital
Transitional Pain Service
development and implementation
of a multidisciplinary program
to prevent chronic postsurgical pain (Katz J Pain Res 2015)
bull Nurse navigator
bull Psychologists (ACT)
Clinical Manifestations hellipour approach to the patient with CPSP
bull Type of pain Cause
bull Exclude other causes (infection recurrence)
bull Psychological and social factors
bull Temporal Context
Electronic Patient Record
Future Directions
bull Identify Causative Modifiable risk factors vs Associative risk factors
bull Measure psychological variables
bull Genetic assays to identify genes controlling the variability in developing chronic pain
Aim is lsquoto identify susceptibility to chronic pain and sensitivity to analgesicsrsquo
Chronic pain lsquoheritabilityrsquo is variable
Conclusions
bull 1 year incidence = 05 -10 bull Avoid pain before during and after surgery lsquohelliphelliptranslate advances in acute pain to chronic settinghelliphelliprsquo bull Psychological pre-assessment bull Education discussion with patients surgeons bull In some cases preventive analgesia may be beneficial bull Transitional Pain Servicehelliptrackinghellipdatabase lsquoPragmatic approachrsquo lsquoAll diseases have an acute phasersquo lsquoDrugs good for acute pain must be good for chronic painrsquo

Pain amp disability
Muscle spasm
Pain
Capsulitis
lsquoCordingrsquo
History Sherman et al PAIN (1984) Chronic phantom pain in 5000 American Veterans 80 pain 1 lasting effect of treatments
Crombie et al PAIN (1998) Cut and Thrust antecedent surgery among patients attending a chronic pain clinic Surgery caused pain in 23 Macrea BJA (1998 2008) Chronic postsurgical pain
Incidence - operations
Type of operation Incidence of chronic pain
No of ops (2006)
1 Amputation 30-50 15000
2 Mastectomy 20-30 18000
3 Thoracotomy 30-60
Heart bypass surgery 30-50 30000
Caesarean section 6 139000
Cholecystectomy 5-50 51000
Hernia 5-35 75000
Laparotomy 30000
Dental root canal surgery (PAIN 2016)
10
Prevalence of chronic pain after breast surgery author year prevalence time
Jamison 1979 44 2 years
Kroner 1989 23 1 year
Vecht 1990 18 6 months
Polinsky 1994 22-32 mean 8 years
Tasmuth 1995 gt50 1 year
Wallace 1996 22- 49 1 year
Smith 1999 43 6 years
Johansen 2000 15 6 years
Fassoulaki 2002 33 3 months
Reuben 2004 50 6 months
Fassoulaki 2005 57 6 months
Kairaluomma 2006 8 1 year
Burton 2007 50 1 year
Hofso 2012 50 1 year
New Definition Old
Macrea BJA 2008 New
Pain April 2017
1 Pain after surgical procedure
1 Pain after a surgical procedure or increases in intensity after a surgical procedure
2 Pain after 2 months 2 Pain after at least 3-6 months hellipwith significant impact on Quality of Life
3 Exclude other causes of the pain
3 Exclude other causes of the pain
4 Exclude pre-existing causes
4 The pain is either a continuation of post surgery pain or develops after an asymptomatic period
5 The pain is either i) localised to the surgical field ii) projected to the innervation territory of a
nerve in the field
Classification of lsquopost mastectomyrsquo pain
1 Pre-existing pain
Osteorheumatoid arthritis Fibromyalgia
Costo-chondritis Cervical radiculopathy
2 Tumour
involvement
Recurrence Metastasis
Cervical radiculopathy due to tumour
3 Post-surgical
Intercostobrachial neuralgia Other neuralgias Persistent lsquoacutersquo pain Scar pain
Phantom breast Intercostal neuromas
Carpal tunnel syndrome Radiation induced plexopathy
Transient brachial neuritis Complex regional pain syndrome
4 Neuropathic
5 Pain due to
implants amp
reconstruction
Capsulitis Capsular contraction and hardening
Foreign body reaction Referred pain Implant migration
Atypical chest pain syndrome Reconstruction lsquoissuesrsquo
6 Other causes
Psychological factors Lymphoedema Pericapsulitis
Muscle spasm lsquoShoulder painrsquo Post-chemo Post- radiotherapy Idiopathic
Myofascial pain dysfunction syndrome
How big a problem is it
In a population of chronic pain patientshelliphow many had pain as a result of surgery Crombie et al Pain 1998 5000 chronic pain patients 23 = CPSP (high proportion with disability) How many people with acute pain go on to get pain at 1 year Hayes et al Acute Pain 2002 5000 patients undergoing surgery Acute neuropathic pain 2 Feature= high intensity 910 Follow up Hayes et al Acute Pain 2002 Pain at 6 months 78 Pain at 1 year 56 lsquo26 million operations year in USA (2008) 1 of all patients develop CPSPrsquo (Katz 2011)
What this study adds bull 3 of patients who had not used opioids previously continued to use them for more than 90 days after major elective surgery bullImportant public health concern because millions of patients undergo major surgery every year
Clarke et al British Medical Journal 2014
Risk factorshellip 1 Causal Modifiable Risk factors (Katz Anesth amp Analg 2011)
Acute pain
Pre-existing pain
Psychological factors
2 Correlated risk factors (Katz Anesth amp Analg 2011)
Younger age
Gender
Psychological distress
Pain
Risk factors
1 Patient related
2 Surgery related
Patient-related risk factors lsquohellippain predicts painrsquo
bull Preoperative pain (Forsythe 2008)
bull Intensity of acute pain (Masselin-Dubois 2013)
bull Acute neuropathic pain (Haroutiounian 2013)
bull High opioid consumption perioperatively (Kalso 2001)
bull Pain in other body parts (Pinto 2012)
bull Younger age (Masselin-Dubois 2013)
bull Female (Ochroch 2006)
Psychological risk factors
bull Pre-op anxiety and catastrophizing meta analysis (2x likelihood of developing CPSP (Theunissen Clin J Pain 2012)
bull Depression (Attal 2014)
bull Catastrophizing (Masselin-Dubois 2013)
bull Sensitivity to pain traumatisation (Page 2013)
bull Anxiety (Kleimann 2011)
bull Fear of long term consequences of surgery (Peters 2007)
Surgical risk factors
bull Low vs high volume surgical unit 13 increase in risk of CPSP (Tasmuth1999)
bull Duration of surgery (Kalso 2007)
bull Minimally invasive surgery (Grant 2004)
bull Stitch types (Cerfolio 2003)
bull Nerve damage preservation (Jensen 1985)
Predictive factors for chronic pain after breast surgery
Anderson et al Pain 2015 n=575
Pain at 1 year
bull Moderate- severe post op pain (50)
bull Axillary lymph node with ICB nerve preservation (30)
bull Neuropathic pain 1 week (18)
bull Age lt 65 (18)
Wang Canadian Medical Assoc Journal 2016 bull Young age bull Axillary lymph node dissection bull Acute pain High quality evidence showed no association
with BMI Type of breast surgery Chemotherapy Reconstruction
Clinical Prediction Model and Tool for Assessing Risk of Persistent Pain After Breast Cancer Surgery Tuomo J Meretoja Kenneth Geving Andersen Julie Bruce Lassi Haasio Reetta Sipilauml Neil W Scott Samuli Ripatti Henrik Kehlet and Eija Kalso
March 2017
Risk Factors ndash what can we discuss with surgeons
bull Information for patients
bull Pre-assessment pain clinic
bull Pre-op anaesthetic strategies algorithms PVB
bull Surgical technique ()
(eg mesh preservation of nerves
minimally invasive etc)
bull Enhanced recovery hellip
eg Kehlet et al Br J Surgery 2005
Fast Track Surgery
bull Pain clinic follow up
Pathophysiology lsquowhat is it about pain that causes more painrsquo
lsquohelliptransition to chronicityhelliprsquo
1 Nociceptive inflammation ischaemia oedema pressure traction
2 Neuropathic peripheral amp central sensitisation
spinal cord neuroplasticity
neuroma
3 Psychological amp social
4 Genetic
The neuropathic component in persistent pain after surgery
systematic review Haroutiunian PAIN 2013
CPSP after 11 types of surgery
bull Amount of pain depends
bull on likelihood of nerve damage
Neuropathic pain
bull in 65 of thoracotomy patients
bull 33 groin surgery
bull 6 knee surgery
Post surgical breast pain
Jung PAIN 2003
1 Intercostobrachial neuralgia
2 Other nerve injury
3 Neuroma
4 Phantom breast
Natural History
Long-term follow-up of breast cancer survivors with post-mastectomy pain syndrome
Macdonald et al British J of Cancer 2005
1996helliphellip 43 pain 3 years 2002 hellip21 pain 9 years
Persistent pain after breast surgery 6-year nationwide
follow up
Mejdahl Kehlet et al BMJ 2013
2008hellip47 pain 1 year
2013hellip37 pain 6 years
Treatment - prevention
helliphellipfrom Pre-emptive Analgesia (blocking preoperative stimuli)
helliphellipto Preventative Analgesia (blocking noxious stimuli central sensitisation across the entire perioperative period)
Preventative treatments
1 Nerve blocks Regional
2 Drugs
Regional anaesthesia to prevent chronic pain after surgery a Cochrane systematic review and meta-analysisdagger M H Andreae1 and D A Andreae2
BJA 2013
bull 23 RCTrsquos
bull Epidural anaesthesia and
paravertebral blocks may be effective
in preventing chronic pain at 1 year
bull Effective in about 1 in 4
patients treated
Preincisional Paravertebral Block Reduces the Prevalence of Chronic
Pain After Breast Surgery Kairaluoma et al Anesth Analg 2006103703-708
bull Preincisional paravertebral block provides significant immediate postoperative analgesia
bull In the same patients (n = 60) 12 months sig less pain in the PVB group
bull In addition to providing acute postoperative pain relief preoperative PVB reduces the prevalence of chronic pain 1 yr after breast cancer surgery
Epidurals Intraoperative epidural analgesia provides preventative analgesia in
abdominal surgery Lavandrsquohomme et al Anaesthesiology 2005
bull Clear benefit of epidural in preventing chronic pain 1 year
bull Intraoperative epidural better than postoperative epidural
bull Effective epidural better than effective parenteral only analgesia one year
Systematic review of therapeutic interventions to reduce chronic post surgical pain (32 RCTrsquos)
Humble et al European J of Pain (2015)
POSITIVE
Gabapentinoids
Lidocaine
iv lidocaine EMLA
Regional
TIVA
NEGATIVE
Ketamine
Cryoanalgesia
Local anaesthetic infiltration
Remifentanil (increased chronic pain)
1 Gabapentin around time of surgery
lsquono effect on chronic painrsquo
POSITIVE
NEGATIVE
Meta analysis (Clarke 2012) 48 RCTrsquos positive effect at 2 months
Cochrane Systematic Review (Chaparro 2013) 280 patients analysed pain at 6 months No effect
RCT Gabapentin 1200mg prior to Thyroidectomy Sig less pain at 3 months (Brogley 2008)
RCT Gabapentin vs Placebo Knee replacement No effect on chronic pain (Clarke 2014)
2 Pregabalin ndash around time of surgery lsquoNot a recommended treatment can cause post operative somnolencersquo
Positive
Negative
Meta-analysis of 3 studies (Clarke 2012) All showed improvement in pain 2 RCTrsquoshellipvery large decrease in CPSP (p=0007)
3 unpublished RCTrsquos from Pfizer (2010-2014) hellipall negative for acute and chronic pain i) 307 patients undergoing knee replacement ii) 501 patients hysterectomy iii) 425 patient hernia
Cochrane Systematic Review (Chaparro 2013) 25 RCTrsquos significant benefit
Systematic review (Martinez May 2017) No difference between pregabalin and placebo 3 months Use for acute pain in pro-nociceptive surgery Side effects a problem
Multimodal analgesia
bull Standard protocols now widely used eg Paravertebral blocks at MD Anderson bull Pre-assessment clinic screening for pain psychological factors pain catastrophising scale helliphellipgenetic screening tests bull Education patients surgeons anaesthetists nurses psychologists
General treatment strategies for chronic postsurgical neuropathic pain
Preventative Perkins amp Kehlet Anesthesiology 2000
bullSurgical procedure preservation
sentinel node biopsy
bullBetter postoperative pain management
bullInformed consent preparatory
information
Established Dworkin Archives Neurol 2003 60
1524
bull Amitriptyline
bull Gabapentin
bull Opioids
bull Tramadol
bull 5 Lidoderm patch EMLA
Positive therapies for Prevention of PSBP
1 EMLA applied to chest wall prior
to surgery less pain 3 months
Fassoulaki 2000
2 Venlafaxine XR 70mg before
and for 2 weeks post surgeryno diff
acute pain significantly less chronic
pain 6 months
Reuben 2004
3 Aggressive acute pain
management
Iohom 2006
4 Preincisional paravertebral
block
Kairaluoma 2006
5 Multimodal analgesia with
gabapentin EMLA ropivacaine less
acute pain amp pain 6 months
Fassoulaki 2005
A pain management programme for chronic cancer-
treatment-related pain Robb Williams Duvivier Newham
Journal of Pain 2006775-150
bull Theory of cancer-related pain
bull Pain pathways
bull Overunder activity cycle
bull Pacing
bull Exercise and fitness
bull TENS
bull Posture and manual handling
bull Relapse and prevention
Psychology interventions
bull Goal setting
bull Role of factors involved in pain
bull Homework assignments
bull Relaxation techniques
bull Cognitive skills
bull Relapse and prevention
Results
significant (plt005) improvements in
bull Pain severity
bull Psychological distress
bull Pain amp psychological coping indices
bull Activities of daily living
bull General fitness
Research Proposal
Exercise to prevent shoulder conditions in patients
undergoing breast cancer treatment
bull Aim to conduct a randomised controlled trial (RCT) supported with qualitative research to investigate the clinical and cost-effectiveness of early supervised exercise on outcomes of arm function chronic pain and quality of life at one year in women undergoing treatment for breast cancer
Intervention
bull A physiotherapy-led structured exercise programme incorporating behavioural strategies and monitoring to encourage adherence
bull A minimum of 4 face-to-face specialist treatment sessions with individual participants will be
delivered within 12 weeks of surgery bull Access to interim telephone support will be provided The programme will restrict to controlled early
stretching and ROM exercises with subsequent progression to maintain strength and function (weeks 2 to 12)
bull Qualitative interviews will be used during the feasibility phase of the trial to explore acceptability of
to the intervention
Outcomes
bull arm shoulder and hand function at 12 months using the 30-item Disability Arm Shoulder Hand (DASH) questionnaire
bull quality of life
bull Functional Assessment of Cancer Treatment-Breast (FACT-B)
bull Short-Form-12 and EQ-5D-5L
bull Data on postoperative adverse events surgical site infection and healthcare resource use will be collected at 6 and 12 months after surgery
Positive therapies for Prevention of PSBP
1 EMLA applied to chest wall prior
to surgery less pain 3 months
Fassoulaki 2000
2 Venlafaxine XR 70mg before
and for 2 weeks post surgeryno diff
acute pain significantly less chronic
pain 6 months
Reuben 2004
3 Aggressive acute pain
management
Iohom 2006
4 Preincisional paravertebral
block
Kairaluoma 2006
5 Multimodal analgesia with
gabapentin EMLA ropivacaine less
acute pain amp pain 6 months
Fassoulaki 2005
Current Treatment Paradigms
The Toronto General Hospital
Transitional Pain Service
development and implementation
of a multidisciplinary program
to prevent chronic postsurgical pain (Katz J Pain Res 2015)
bull Nurse navigator
bull Psychologists (ACT)
Clinical Manifestations hellipour approach to the patient with CPSP
bull Type of pain Cause
bull Exclude other causes (infection recurrence)
bull Psychological and social factors
bull Temporal Context
Electronic Patient Record
Future Directions
bull Identify Causative Modifiable risk factors vs Associative risk factors
bull Measure psychological variables
bull Genetic assays to identify genes controlling the variability in developing chronic pain
Aim is lsquoto identify susceptibility to chronic pain and sensitivity to analgesicsrsquo
Chronic pain lsquoheritabilityrsquo is variable
Conclusions
bull 1 year incidence = 05 -10 bull Avoid pain before during and after surgery lsquohelliphelliptranslate advances in acute pain to chronic settinghelliphelliprsquo bull Psychological pre-assessment bull Education discussion with patients surgeons bull In some cases preventive analgesia may be beneficial bull Transitional Pain Servicehelliptrackinghellipdatabase lsquoPragmatic approachrsquo lsquoAll diseases have an acute phasersquo lsquoDrugs good for acute pain must be good for chronic painrsquo

lsquoCordingrsquo
History Sherman et al PAIN (1984) Chronic phantom pain in 5000 American Veterans 80 pain 1 lasting effect of treatments
Crombie et al PAIN (1998) Cut and Thrust antecedent surgery among patients attending a chronic pain clinic Surgery caused pain in 23 Macrea BJA (1998 2008) Chronic postsurgical pain
Incidence - operations
Type of operation Incidence of chronic pain
No of ops (2006)
1 Amputation 30-50 15000
2 Mastectomy 20-30 18000
3 Thoracotomy 30-60
Heart bypass surgery 30-50 30000
Caesarean section 6 139000
Cholecystectomy 5-50 51000
Hernia 5-35 75000
Laparotomy 30000
Dental root canal surgery (PAIN 2016)
10
Prevalence of chronic pain after breast surgery author year prevalence time
Jamison 1979 44 2 years
Kroner 1989 23 1 year
Vecht 1990 18 6 months
Polinsky 1994 22-32 mean 8 years
Tasmuth 1995 gt50 1 year
Wallace 1996 22- 49 1 year
Smith 1999 43 6 years
Johansen 2000 15 6 years
Fassoulaki 2002 33 3 months
Reuben 2004 50 6 months
Fassoulaki 2005 57 6 months
Kairaluomma 2006 8 1 year
Burton 2007 50 1 year
Hofso 2012 50 1 year
New Definition Old
Macrea BJA 2008 New
Pain April 2017
1 Pain after surgical procedure
1 Pain after a surgical procedure or increases in intensity after a surgical procedure
2 Pain after 2 months 2 Pain after at least 3-6 months hellipwith significant impact on Quality of Life
3 Exclude other causes of the pain
3 Exclude other causes of the pain
4 Exclude pre-existing causes
4 The pain is either a continuation of post surgery pain or develops after an asymptomatic period
5 The pain is either i) localised to the surgical field ii) projected to the innervation territory of a
nerve in the field
Classification of lsquopost mastectomyrsquo pain
1 Pre-existing pain
Osteorheumatoid arthritis Fibromyalgia
Costo-chondritis Cervical radiculopathy
2 Tumour
involvement
Recurrence Metastasis
Cervical radiculopathy due to tumour
3 Post-surgical
Intercostobrachial neuralgia Other neuralgias Persistent lsquoacutersquo pain Scar pain
Phantom breast Intercostal neuromas
Carpal tunnel syndrome Radiation induced plexopathy
Transient brachial neuritis Complex regional pain syndrome
4 Neuropathic
5 Pain due to
implants amp
reconstruction
Capsulitis Capsular contraction and hardening
Foreign body reaction Referred pain Implant migration
Atypical chest pain syndrome Reconstruction lsquoissuesrsquo
6 Other causes
Psychological factors Lymphoedema Pericapsulitis
Muscle spasm lsquoShoulder painrsquo Post-chemo Post- radiotherapy Idiopathic
Myofascial pain dysfunction syndrome
How big a problem is it
In a population of chronic pain patientshelliphow many had pain as a result of surgery Crombie et al Pain 1998 5000 chronic pain patients 23 = CPSP (high proportion with disability) How many people with acute pain go on to get pain at 1 year Hayes et al Acute Pain 2002 5000 patients undergoing surgery Acute neuropathic pain 2 Feature= high intensity 910 Follow up Hayes et al Acute Pain 2002 Pain at 6 months 78 Pain at 1 year 56 lsquo26 million operations year in USA (2008) 1 of all patients develop CPSPrsquo (Katz 2011)
What this study adds bull 3 of patients who had not used opioids previously continued to use them for more than 90 days after major elective surgery bullImportant public health concern because millions of patients undergo major surgery every year
Clarke et al British Medical Journal 2014
Risk factorshellip 1 Causal Modifiable Risk factors (Katz Anesth amp Analg 2011)
Acute pain
Pre-existing pain
Psychological factors
2 Correlated risk factors (Katz Anesth amp Analg 2011)
Younger age
Gender
Psychological distress
Pain
Risk factors
1 Patient related
2 Surgery related
Patient-related risk factors lsquohellippain predicts painrsquo
bull Preoperative pain (Forsythe 2008)
bull Intensity of acute pain (Masselin-Dubois 2013)
bull Acute neuropathic pain (Haroutiounian 2013)
bull High opioid consumption perioperatively (Kalso 2001)
bull Pain in other body parts (Pinto 2012)
bull Younger age (Masselin-Dubois 2013)
bull Female (Ochroch 2006)
Psychological risk factors
bull Pre-op anxiety and catastrophizing meta analysis (2x likelihood of developing CPSP (Theunissen Clin J Pain 2012)
bull Depression (Attal 2014)
bull Catastrophizing (Masselin-Dubois 2013)
bull Sensitivity to pain traumatisation (Page 2013)
bull Anxiety (Kleimann 2011)
bull Fear of long term consequences of surgery (Peters 2007)
Surgical risk factors
bull Low vs high volume surgical unit 13 increase in risk of CPSP (Tasmuth1999)
bull Duration of surgery (Kalso 2007)
bull Minimally invasive surgery (Grant 2004)
bull Stitch types (Cerfolio 2003)
bull Nerve damage preservation (Jensen 1985)
Predictive factors for chronic pain after breast surgery
Anderson et al Pain 2015 n=575
Pain at 1 year
bull Moderate- severe post op pain (50)
bull Axillary lymph node with ICB nerve preservation (30)
bull Neuropathic pain 1 week (18)
bull Age lt 65 (18)
Wang Canadian Medical Assoc Journal 2016 bull Young age bull Axillary lymph node dissection bull Acute pain High quality evidence showed no association
with BMI Type of breast surgery Chemotherapy Reconstruction
Clinical Prediction Model and Tool for Assessing Risk of Persistent Pain After Breast Cancer Surgery Tuomo J Meretoja Kenneth Geving Andersen Julie Bruce Lassi Haasio Reetta Sipilauml Neil W Scott Samuli Ripatti Henrik Kehlet and Eija Kalso
March 2017
Risk Factors ndash what can we discuss with surgeons
bull Information for patients
bull Pre-assessment pain clinic
bull Pre-op anaesthetic strategies algorithms PVB
bull Surgical technique ()
(eg mesh preservation of nerves
minimally invasive etc)
bull Enhanced recovery hellip
eg Kehlet et al Br J Surgery 2005
Fast Track Surgery
bull Pain clinic follow up
Pathophysiology lsquowhat is it about pain that causes more painrsquo
lsquohelliptransition to chronicityhelliprsquo
1 Nociceptive inflammation ischaemia oedema pressure traction
2 Neuropathic peripheral amp central sensitisation
spinal cord neuroplasticity
neuroma
3 Psychological amp social
4 Genetic
The neuropathic component in persistent pain after surgery
systematic review Haroutiunian PAIN 2013
CPSP after 11 types of surgery
bull Amount of pain depends
bull on likelihood of nerve damage
Neuropathic pain
bull in 65 of thoracotomy patients
bull 33 groin surgery
bull 6 knee surgery
Post surgical breast pain
Jung PAIN 2003
1 Intercostobrachial neuralgia
2 Other nerve injury
3 Neuroma
4 Phantom breast
Natural History
Long-term follow-up of breast cancer survivors with post-mastectomy pain syndrome
Macdonald et al British J of Cancer 2005
1996helliphellip 43 pain 3 years 2002 hellip21 pain 9 years
Persistent pain after breast surgery 6-year nationwide
follow up
Mejdahl Kehlet et al BMJ 2013
2008hellip47 pain 1 year
2013hellip37 pain 6 years
Treatment - prevention
helliphellipfrom Pre-emptive Analgesia (blocking preoperative stimuli)
helliphellipto Preventative Analgesia (blocking noxious stimuli central sensitisation across the entire perioperative period)
Preventative treatments
1 Nerve blocks Regional
2 Drugs
Regional anaesthesia to prevent chronic pain after surgery a Cochrane systematic review and meta-analysisdagger M H Andreae1 and D A Andreae2
BJA 2013
bull 23 RCTrsquos
bull Epidural anaesthesia and
paravertebral blocks may be effective
in preventing chronic pain at 1 year
bull Effective in about 1 in 4
patients treated
Preincisional Paravertebral Block Reduces the Prevalence of Chronic
Pain After Breast Surgery Kairaluoma et al Anesth Analg 2006103703-708
bull Preincisional paravertebral block provides significant immediate postoperative analgesia
bull In the same patients (n = 60) 12 months sig less pain in the PVB group
bull In addition to providing acute postoperative pain relief preoperative PVB reduces the prevalence of chronic pain 1 yr after breast cancer surgery
Epidurals Intraoperative epidural analgesia provides preventative analgesia in
abdominal surgery Lavandrsquohomme et al Anaesthesiology 2005
bull Clear benefit of epidural in preventing chronic pain 1 year
bull Intraoperative epidural better than postoperative epidural
bull Effective epidural better than effective parenteral only analgesia one year
Systematic review of therapeutic interventions to reduce chronic post surgical pain (32 RCTrsquos)
Humble et al European J of Pain (2015)
POSITIVE
Gabapentinoids
Lidocaine
iv lidocaine EMLA
Regional
TIVA
NEGATIVE
Ketamine
Cryoanalgesia
Local anaesthetic infiltration
Remifentanil (increased chronic pain)
1 Gabapentin around time of surgery
lsquono effect on chronic painrsquo
POSITIVE
NEGATIVE
Meta analysis (Clarke 2012) 48 RCTrsquos positive effect at 2 months
Cochrane Systematic Review (Chaparro 2013) 280 patients analysed pain at 6 months No effect
RCT Gabapentin 1200mg prior to Thyroidectomy Sig less pain at 3 months (Brogley 2008)
RCT Gabapentin vs Placebo Knee replacement No effect on chronic pain (Clarke 2014)
2 Pregabalin ndash around time of surgery lsquoNot a recommended treatment can cause post operative somnolencersquo
Positive
Negative
Meta-analysis of 3 studies (Clarke 2012) All showed improvement in pain 2 RCTrsquoshellipvery large decrease in CPSP (p=0007)
3 unpublished RCTrsquos from Pfizer (2010-2014) hellipall negative for acute and chronic pain i) 307 patients undergoing knee replacement ii) 501 patients hysterectomy iii) 425 patient hernia
Cochrane Systematic Review (Chaparro 2013) 25 RCTrsquos significant benefit
Systematic review (Martinez May 2017) No difference between pregabalin and placebo 3 months Use for acute pain in pro-nociceptive surgery Side effects a problem
Multimodal analgesia
bull Standard protocols now widely used eg Paravertebral blocks at MD Anderson bull Pre-assessment clinic screening for pain psychological factors pain catastrophising scale helliphellipgenetic screening tests bull Education patients surgeons anaesthetists nurses psychologists
General treatment strategies for chronic postsurgical neuropathic pain
Preventative Perkins amp Kehlet Anesthesiology 2000
bullSurgical procedure preservation
sentinel node biopsy
bullBetter postoperative pain management
bullInformed consent preparatory
information
Established Dworkin Archives Neurol 2003 60
1524
bull Amitriptyline
bull Gabapentin
bull Opioids
bull Tramadol
bull 5 Lidoderm patch EMLA
Positive therapies for Prevention of PSBP
1 EMLA applied to chest wall prior
to surgery less pain 3 months
Fassoulaki 2000
2 Venlafaxine XR 70mg before
and for 2 weeks post surgeryno diff
acute pain significantly less chronic
pain 6 months
Reuben 2004
3 Aggressive acute pain
management
Iohom 2006
4 Preincisional paravertebral
block
Kairaluoma 2006
5 Multimodal analgesia with
gabapentin EMLA ropivacaine less
acute pain amp pain 6 months
Fassoulaki 2005
A pain management programme for chronic cancer-
treatment-related pain Robb Williams Duvivier Newham
Journal of Pain 2006775-150
bull Theory of cancer-related pain
bull Pain pathways
bull Overunder activity cycle
bull Pacing
bull Exercise and fitness
bull TENS
bull Posture and manual handling
bull Relapse and prevention
Psychology interventions
bull Goal setting
bull Role of factors involved in pain
bull Homework assignments
bull Relaxation techniques
bull Cognitive skills
bull Relapse and prevention
Results
significant (plt005) improvements in
bull Pain severity
bull Psychological distress
bull Pain amp psychological coping indices
bull Activities of daily living
bull General fitness
Research Proposal
Exercise to prevent shoulder conditions in patients
undergoing breast cancer treatment
bull Aim to conduct a randomised controlled trial (RCT) supported with qualitative research to investigate the clinical and cost-effectiveness of early supervised exercise on outcomes of arm function chronic pain and quality of life at one year in women undergoing treatment for breast cancer
Intervention
bull A physiotherapy-led structured exercise programme incorporating behavioural strategies and monitoring to encourage adherence
bull A minimum of 4 face-to-face specialist treatment sessions with individual participants will be
delivered within 12 weeks of surgery bull Access to interim telephone support will be provided The programme will restrict to controlled early
stretching and ROM exercises with subsequent progression to maintain strength and function (weeks 2 to 12)
bull Qualitative interviews will be used during the feasibility phase of the trial to explore acceptability of
to the intervention
Outcomes
bull arm shoulder and hand function at 12 months using the 30-item Disability Arm Shoulder Hand (DASH) questionnaire
bull quality of life
bull Functional Assessment of Cancer Treatment-Breast (FACT-B)
bull Short-Form-12 and EQ-5D-5L
bull Data on postoperative adverse events surgical site infection and healthcare resource use will be collected at 6 and 12 months after surgery
Positive therapies for Prevention of PSBP
1 EMLA applied to chest wall prior
to surgery less pain 3 months
Fassoulaki 2000
2 Venlafaxine XR 70mg before
and for 2 weeks post surgeryno diff
acute pain significantly less chronic
pain 6 months
Reuben 2004
3 Aggressive acute pain
management
Iohom 2006
4 Preincisional paravertebral
block
Kairaluoma 2006
5 Multimodal analgesia with
gabapentin EMLA ropivacaine less
acute pain amp pain 6 months
Fassoulaki 2005
Current Treatment Paradigms
The Toronto General Hospital
Transitional Pain Service
development and implementation
of a multidisciplinary program
to prevent chronic postsurgical pain (Katz J Pain Res 2015)
bull Nurse navigator
bull Psychologists (ACT)
Clinical Manifestations hellipour approach to the patient with CPSP
bull Type of pain Cause
bull Exclude other causes (infection recurrence)
bull Psychological and social factors
bull Temporal Context
Electronic Patient Record
Future Directions
bull Identify Causative Modifiable risk factors vs Associative risk factors
bull Measure psychological variables
bull Genetic assays to identify genes controlling the variability in developing chronic pain
Aim is lsquoto identify susceptibility to chronic pain and sensitivity to analgesicsrsquo
Chronic pain lsquoheritabilityrsquo is variable
Conclusions
bull 1 year incidence = 05 -10 bull Avoid pain before during and after surgery lsquohelliphelliptranslate advances in acute pain to chronic settinghelliphelliprsquo bull Psychological pre-assessment bull Education discussion with patients surgeons bull In some cases preventive analgesia may be beneficial bull Transitional Pain Servicehelliptrackinghellipdatabase lsquoPragmatic approachrsquo lsquoAll diseases have an acute phasersquo lsquoDrugs good for acute pain must be good for chronic painrsquo

History Sherman et al PAIN (1984) Chronic phantom pain in 5000 American Veterans 80 pain 1 lasting effect of treatments
Crombie et al PAIN (1998) Cut and Thrust antecedent surgery among patients attending a chronic pain clinic Surgery caused pain in 23 Macrea BJA (1998 2008) Chronic postsurgical pain
Incidence - operations
Type of operation Incidence of chronic pain
No of ops (2006)
1 Amputation 30-50 15000
2 Mastectomy 20-30 18000
3 Thoracotomy 30-60
Heart bypass surgery 30-50 30000
Caesarean section 6 139000
Cholecystectomy 5-50 51000
Hernia 5-35 75000
Laparotomy 30000
Dental root canal surgery (PAIN 2016)
10
Prevalence of chronic pain after breast surgery author year prevalence time
Jamison 1979 44 2 years
Kroner 1989 23 1 year
Vecht 1990 18 6 months
Polinsky 1994 22-32 mean 8 years
Tasmuth 1995 gt50 1 year
Wallace 1996 22- 49 1 year
Smith 1999 43 6 years
Johansen 2000 15 6 years
Fassoulaki 2002 33 3 months
Reuben 2004 50 6 months
Fassoulaki 2005 57 6 months
Kairaluomma 2006 8 1 year
Burton 2007 50 1 year
Hofso 2012 50 1 year
New Definition Old
Macrea BJA 2008 New
Pain April 2017
1 Pain after surgical procedure
1 Pain after a surgical procedure or increases in intensity after a surgical procedure
2 Pain after 2 months 2 Pain after at least 3-6 months hellipwith significant impact on Quality of Life
3 Exclude other causes of the pain
3 Exclude other causes of the pain
4 Exclude pre-existing causes
4 The pain is either a continuation of post surgery pain or develops after an asymptomatic period
5 The pain is either i) localised to the surgical field ii) projected to the innervation territory of a
nerve in the field
Classification of lsquopost mastectomyrsquo pain
1 Pre-existing pain
Osteorheumatoid arthritis Fibromyalgia
Costo-chondritis Cervical radiculopathy
2 Tumour
involvement
Recurrence Metastasis
Cervical radiculopathy due to tumour
3 Post-surgical
Intercostobrachial neuralgia Other neuralgias Persistent lsquoacutersquo pain Scar pain
Phantom breast Intercostal neuromas
Carpal tunnel syndrome Radiation induced plexopathy
Transient brachial neuritis Complex regional pain syndrome
4 Neuropathic
5 Pain due to
implants amp
reconstruction
Capsulitis Capsular contraction and hardening
Foreign body reaction Referred pain Implant migration
Atypical chest pain syndrome Reconstruction lsquoissuesrsquo
6 Other causes
Psychological factors Lymphoedema Pericapsulitis
Muscle spasm lsquoShoulder painrsquo Post-chemo Post- radiotherapy Idiopathic
Myofascial pain dysfunction syndrome
How big a problem is it
In a population of chronic pain patientshelliphow many had pain as a result of surgery Crombie et al Pain 1998 5000 chronic pain patients 23 = CPSP (high proportion with disability) How many people with acute pain go on to get pain at 1 year Hayes et al Acute Pain 2002 5000 patients undergoing surgery Acute neuropathic pain 2 Feature= high intensity 910 Follow up Hayes et al Acute Pain 2002 Pain at 6 months 78 Pain at 1 year 56 lsquo26 million operations year in USA (2008) 1 of all patients develop CPSPrsquo (Katz 2011)
What this study adds bull 3 of patients who had not used opioids previously continued to use them for more than 90 days after major elective surgery bullImportant public health concern because millions of patients undergo major surgery every year
Clarke et al British Medical Journal 2014
Risk factorshellip 1 Causal Modifiable Risk factors (Katz Anesth amp Analg 2011)
Acute pain
Pre-existing pain
Psychological factors
2 Correlated risk factors (Katz Anesth amp Analg 2011)
Younger age
Gender
Psychological distress
Pain
Risk factors
1 Patient related
2 Surgery related
Patient-related risk factors lsquohellippain predicts painrsquo
bull Preoperative pain (Forsythe 2008)
bull Intensity of acute pain (Masselin-Dubois 2013)
bull Acute neuropathic pain (Haroutiounian 2013)
bull High opioid consumption perioperatively (Kalso 2001)
bull Pain in other body parts (Pinto 2012)
bull Younger age (Masselin-Dubois 2013)
bull Female (Ochroch 2006)
Psychological risk factors
bull Pre-op anxiety and catastrophizing meta analysis (2x likelihood of developing CPSP (Theunissen Clin J Pain 2012)
bull Depression (Attal 2014)
bull Catastrophizing (Masselin-Dubois 2013)
bull Sensitivity to pain traumatisation (Page 2013)
bull Anxiety (Kleimann 2011)
bull Fear of long term consequences of surgery (Peters 2007)
Surgical risk factors
bull Low vs high volume surgical unit 13 increase in risk of CPSP (Tasmuth1999)
bull Duration of surgery (Kalso 2007)
bull Minimally invasive surgery (Grant 2004)
bull Stitch types (Cerfolio 2003)
bull Nerve damage preservation (Jensen 1985)
Predictive factors for chronic pain after breast surgery
Anderson et al Pain 2015 n=575
Pain at 1 year
bull Moderate- severe post op pain (50)
bull Axillary lymph node with ICB nerve preservation (30)
bull Neuropathic pain 1 week (18)
bull Age lt 65 (18)
Wang Canadian Medical Assoc Journal 2016 bull Young age bull Axillary lymph node dissection bull Acute pain High quality evidence showed no association
with BMI Type of breast surgery Chemotherapy Reconstruction
Clinical Prediction Model and Tool for Assessing Risk of Persistent Pain After Breast Cancer Surgery Tuomo J Meretoja Kenneth Geving Andersen Julie Bruce Lassi Haasio Reetta Sipilauml Neil W Scott Samuli Ripatti Henrik Kehlet and Eija Kalso
March 2017
Risk Factors ndash what can we discuss with surgeons
bull Information for patients
bull Pre-assessment pain clinic
bull Pre-op anaesthetic strategies algorithms PVB
bull Surgical technique ()
(eg mesh preservation of nerves
minimally invasive etc)
bull Enhanced recovery hellip
eg Kehlet et al Br J Surgery 2005
Fast Track Surgery
bull Pain clinic follow up
Pathophysiology lsquowhat is it about pain that causes more painrsquo
lsquohelliptransition to chronicityhelliprsquo
1 Nociceptive inflammation ischaemia oedema pressure traction
2 Neuropathic peripheral amp central sensitisation
spinal cord neuroplasticity
neuroma
3 Psychological amp social
4 Genetic
The neuropathic component in persistent pain after surgery
systematic review Haroutiunian PAIN 2013
CPSP after 11 types of surgery
bull Amount of pain depends
bull on likelihood of nerve damage
Neuropathic pain
bull in 65 of thoracotomy patients
bull 33 groin surgery
bull 6 knee surgery
Post surgical breast pain
Jung PAIN 2003
1 Intercostobrachial neuralgia
2 Other nerve injury
3 Neuroma
4 Phantom breast
Natural History
Long-term follow-up of breast cancer survivors with post-mastectomy pain syndrome
Macdonald et al British J of Cancer 2005
1996helliphellip 43 pain 3 years 2002 hellip21 pain 9 years
Persistent pain after breast surgery 6-year nationwide
follow up
Mejdahl Kehlet et al BMJ 2013
2008hellip47 pain 1 year
2013hellip37 pain 6 years
Treatment - prevention
helliphellipfrom Pre-emptive Analgesia (blocking preoperative stimuli)
helliphellipto Preventative Analgesia (blocking noxious stimuli central sensitisation across the entire perioperative period)
Preventative treatments
1 Nerve blocks Regional
2 Drugs
Regional anaesthesia to prevent chronic pain after surgery a Cochrane systematic review and meta-analysisdagger M H Andreae1 and D A Andreae2
BJA 2013
bull 23 RCTrsquos
bull Epidural anaesthesia and
paravertebral blocks may be effective
in preventing chronic pain at 1 year
bull Effective in about 1 in 4
patients treated
Preincisional Paravertebral Block Reduces the Prevalence of Chronic
Pain After Breast Surgery Kairaluoma et al Anesth Analg 2006103703-708
bull Preincisional paravertebral block provides significant immediate postoperative analgesia
bull In the same patients (n = 60) 12 months sig less pain in the PVB group
bull In addition to providing acute postoperative pain relief preoperative PVB reduces the prevalence of chronic pain 1 yr after breast cancer surgery
Epidurals Intraoperative epidural analgesia provides preventative analgesia in
abdominal surgery Lavandrsquohomme et al Anaesthesiology 2005
bull Clear benefit of epidural in preventing chronic pain 1 year
bull Intraoperative epidural better than postoperative epidural
bull Effective epidural better than effective parenteral only analgesia one year
Systematic review of therapeutic interventions to reduce chronic post surgical pain (32 RCTrsquos)
Humble et al European J of Pain (2015)
POSITIVE
Gabapentinoids
Lidocaine
iv lidocaine EMLA
Regional
TIVA
NEGATIVE
Ketamine
Cryoanalgesia
Local anaesthetic infiltration
Remifentanil (increased chronic pain)
1 Gabapentin around time of surgery
lsquono effect on chronic painrsquo
POSITIVE
NEGATIVE
Meta analysis (Clarke 2012) 48 RCTrsquos positive effect at 2 months
Cochrane Systematic Review (Chaparro 2013) 280 patients analysed pain at 6 months No effect
RCT Gabapentin 1200mg prior to Thyroidectomy Sig less pain at 3 months (Brogley 2008)
RCT Gabapentin vs Placebo Knee replacement No effect on chronic pain (Clarke 2014)
2 Pregabalin ndash around time of surgery lsquoNot a recommended treatment can cause post operative somnolencersquo
Positive
Negative
Meta-analysis of 3 studies (Clarke 2012) All showed improvement in pain 2 RCTrsquoshellipvery large decrease in CPSP (p=0007)
3 unpublished RCTrsquos from Pfizer (2010-2014) hellipall negative for acute and chronic pain i) 307 patients undergoing knee replacement ii) 501 patients hysterectomy iii) 425 patient hernia
Cochrane Systematic Review (Chaparro 2013) 25 RCTrsquos significant benefit
Systematic review (Martinez May 2017) No difference between pregabalin and placebo 3 months Use for acute pain in pro-nociceptive surgery Side effects a problem
Multimodal analgesia
bull Standard protocols now widely used eg Paravertebral blocks at MD Anderson bull Pre-assessment clinic screening for pain psychological factors pain catastrophising scale helliphellipgenetic screening tests bull Education patients surgeons anaesthetists nurses psychologists
General treatment strategies for chronic postsurgical neuropathic pain
Preventative Perkins amp Kehlet Anesthesiology 2000
bullSurgical procedure preservation
sentinel node biopsy
bullBetter postoperative pain management
bullInformed consent preparatory
information
Established Dworkin Archives Neurol 2003 60
1524
bull Amitriptyline
bull Gabapentin
bull Opioids
bull Tramadol
bull 5 Lidoderm patch EMLA
Positive therapies for Prevention of PSBP
1 EMLA applied to chest wall prior
to surgery less pain 3 months
Fassoulaki 2000
2 Venlafaxine XR 70mg before
and for 2 weeks post surgeryno diff
acute pain significantly less chronic
pain 6 months
Reuben 2004
3 Aggressive acute pain
management
Iohom 2006
4 Preincisional paravertebral
block
Kairaluoma 2006
5 Multimodal analgesia with
gabapentin EMLA ropivacaine less
acute pain amp pain 6 months
Fassoulaki 2005
A pain management programme for chronic cancer-
treatment-related pain Robb Williams Duvivier Newham
Journal of Pain 2006775-150
bull Theory of cancer-related pain
bull Pain pathways
bull Overunder activity cycle
bull Pacing
bull Exercise and fitness
bull TENS
bull Posture and manual handling
bull Relapse and prevention
Psychology interventions
bull Goal setting
bull Role of factors involved in pain
bull Homework assignments
bull Relaxation techniques
bull Cognitive skills
bull Relapse and prevention
Results
significant (plt005) improvements in
bull Pain severity
bull Psychological distress
bull Pain amp psychological coping indices
bull Activities of daily living
bull General fitness
Research Proposal
Exercise to prevent shoulder conditions in patients
undergoing breast cancer treatment
bull Aim to conduct a randomised controlled trial (RCT) supported with qualitative research to investigate the clinical and cost-effectiveness of early supervised exercise on outcomes of arm function chronic pain and quality of life at one year in women undergoing treatment for breast cancer
Intervention
bull A physiotherapy-led structured exercise programme incorporating behavioural strategies and monitoring to encourage adherence
bull A minimum of 4 face-to-face specialist treatment sessions with individual participants will be
delivered within 12 weeks of surgery bull Access to interim telephone support will be provided The programme will restrict to controlled early
stretching and ROM exercises with subsequent progression to maintain strength and function (weeks 2 to 12)
bull Qualitative interviews will be used during the feasibility phase of the trial to explore acceptability of
to the intervention
Outcomes
bull arm shoulder and hand function at 12 months using the 30-item Disability Arm Shoulder Hand (DASH) questionnaire
bull quality of life
bull Functional Assessment of Cancer Treatment-Breast (FACT-B)
bull Short-Form-12 and EQ-5D-5L
bull Data on postoperative adverse events surgical site infection and healthcare resource use will be collected at 6 and 12 months after surgery
Positive therapies for Prevention of PSBP
1 EMLA applied to chest wall prior
to surgery less pain 3 months
Fassoulaki 2000
2 Venlafaxine XR 70mg before
and for 2 weeks post surgeryno diff
acute pain significantly less chronic
pain 6 months
Reuben 2004
3 Aggressive acute pain
management
Iohom 2006
4 Preincisional paravertebral
block
Kairaluoma 2006
5 Multimodal analgesia with
gabapentin EMLA ropivacaine less
acute pain amp pain 6 months
Fassoulaki 2005
Current Treatment Paradigms
The Toronto General Hospital
Transitional Pain Service
development and implementation
of a multidisciplinary program
to prevent chronic postsurgical pain (Katz J Pain Res 2015)
bull Nurse navigator
bull Psychologists (ACT)
Clinical Manifestations hellipour approach to the patient with CPSP
bull Type of pain Cause
bull Exclude other causes (infection recurrence)
bull Psychological and social factors
bull Temporal Context
Electronic Patient Record
Future Directions
bull Identify Causative Modifiable risk factors vs Associative risk factors
bull Measure psychological variables
bull Genetic assays to identify genes controlling the variability in developing chronic pain
Aim is lsquoto identify susceptibility to chronic pain and sensitivity to analgesicsrsquo
Chronic pain lsquoheritabilityrsquo is variable
Conclusions
bull 1 year incidence = 05 -10 bull Avoid pain before during and after surgery lsquohelliphelliptranslate advances in acute pain to chronic settinghelliphelliprsquo bull Psychological pre-assessment bull Education discussion with patients surgeons bull In some cases preventive analgesia may be beneficial bull Transitional Pain Servicehelliptrackinghellipdatabase lsquoPragmatic approachrsquo lsquoAll diseases have an acute phasersquo lsquoDrugs good for acute pain must be good for chronic painrsquo

Incidence - operations
Type of operation Incidence of chronic pain
No of ops (2006)
1 Amputation 30-50 15000
2 Mastectomy 20-30 18000
3 Thoracotomy 30-60
Heart bypass surgery 30-50 30000
Caesarean section 6 139000
Cholecystectomy 5-50 51000
Hernia 5-35 75000
Laparotomy 30000
Dental root canal surgery (PAIN 2016)
10
Prevalence of chronic pain after breast surgery author year prevalence time
Jamison 1979 44 2 years
Kroner 1989 23 1 year
Vecht 1990 18 6 months
Polinsky 1994 22-32 mean 8 years
Tasmuth 1995 gt50 1 year
Wallace 1996 22- 49 1 year
Smith 1999 43 6 years
Johansen 2000 15 6 years
Fassoulaki 2002 33 3 months
Reuben 2004 50 6 months
Fassoulaki 2005 57 6 months
Kairaluomma 2006 8 1 year
Burton 2007 50 1 year
Hofso 2012 50 1 year
New Definition Old
Macrea BJA 2008 New
Pain April 2017
1 Pain after surgical procedure
1 Pain after a surgical procedure or increases in intensity after a surgical procedure
2 Pain after 2 months 2 Pain after at least 3-6 months hellipwith significant impact on Quality of Life
3 Exclude other causes of the pain
3 Exclude other causes of the pain
4 Exclude pre-existing causes
4 The pain is either a continuation of post surgery pain or develops after an asymptomatic period
5 The pain is either i) localised to the surgical field ii) projected to the innervation territory of a
nerve in the field
Classification of lsquopost mastectomyrsquo pain
1 Pre-existing pain
Osteorheumatoid arthritis Fibromyalgia
Costo-chondritis Cervical radiculopathy
2 Tumour
involvement
Recurrence Metastasis
Cervical radiculopathy due to tumour
3 Post-surgical
Intercostobrachial neuralgia Other neuralgias Persistent lsquoacutersquo pain Scar pain
Phantom breast Intercostal neuromas
Carpal tunnel syndrome Radiation induced plexopathy
Transient brachial neuritis Complex regional pain syndrome
4 Neuropathic
5 Pain due to
implants amp
reconstruction
Capsulitis Capsular contraction and hardening
Foreign body reaction Referred pain Implant migration
Atypical chest pain syndrome Reconstruction lsquoissuesrsquo
6 Other causes
Psychological factors Lymphoedema Pericapsulitis
Muscle spasm lsquoShoulder painrsquo Post-chemo Post- radiotherapy Idiopathic
Myofascial pain dysfunction syndrome
How big a problem is it
In a population of chronic pain patientshelliphow many had pain as a result of surgery Crombie et al Pain 1998 5000 chronic pain patients 23 = CPSP (high proportion with disability) How many people with acute pain go on to get pain at 1 year Hayes et al Acute Pain 2002 5000 patients undergoing surgery Acute neuropathic pain 2 Feature= high intensity 910 Follow up Hayes et al Acute Pain 2002 Pain at 6 months 78 Pain at 1 year 56 lsquo26 million operations year in USA (2008) 1 of all patients develop CPSPrsquo (Katz 2011)
What this study adds bull 3 of patients who had not used opioids previously continued to use them for more than 90 days after major elective surgery bullImportant public health concern because millions of patients undergo major surgery every year
Clarke et al British Medical Journal 2014
Risk factorshellip 1 Causal Modifiable Risk factors (Katz Anesth amp Analg 2011)
Acute pain
Pre-existing pain
Psychological factors
2 Correlated risk factors (Katz Anesth amp Analg 2011)
Younger age
Gender
Psychological distress
Pain
Risk factors
1 Patient related
2 Surgery related
Patient-related risk factors lsquohellippain predicts painrsquo
bull Preoperative pain (Forsythe 2008)
bull Intensity of acute pain (Masselin-Dubois 2013)
bull Acute neuropathic pain (Haroutiounian 2013)
bull High opioid consumption perioperatively (Kalso 2001)
bull Pain in other body parts (Pinto 2012)
bull Younger age (Masselin-Dubois 2013)
bull Female (Ochroch 2006)
Psychological risk factors
bull Pre-op anxiety and catastrophizing meta analysis (2x likelihood of developing CPSP (Theunissen Clin J Pain 2012)
bull Depression (Attal 2014)
bull Catastrophizing (Masselin-Dubois 2013)
bull Sensitivity to pain traumatisation (Page 2013)
bull Anxiety (Kleimann 2011)
bull Fear of long term consequences of surgery (Peters 2007)
Surgical risk factors
bull Low vs high volume surgical unit 13 increase in risk of CPSP (Tasmuth1999)
bull Duration of surgery (Kalso 2007)
bull Minimally invasive surgery (Grant 2004)
bull Stitch types (Cerfolio 2003)
bull Nerve damage preservation (Jensen 1985)
Predictive factors for chronic pain after breast surgery
Anderson et al Pain 2015 n=575
Pain at 1 year
bull Moderate- severe post op pain (50)
bull Axillary lymph node with ICB nerve preservation (30)
bull Neuropathic pain 1 week (18)
bull Age lt 65 (18)
Wang Canadian Medical Assoc Journal 2016 bull Young age bull Axillary lymph node dissection bull Acute pain High quality evidence showed no association
with BMI Type of breast surgery Chemotherapy Reconstruction
Clinical Prediction Model and Tool for Assessing Risk of Persistent Pain After Breast Cancer Surgery Tuomo J Meretoja Kenneth Geving Andersen Julie Bruce Lassi Haasio Reetta Sipilauml Neil W Scott Samuli Ripatti Henrik Kehlet and Eija Kalso
March 2017
Risk Factors ndash what can we discuss with surgeons
bull Information for patients
bull Pre-assessment pain clinic
bull Pre-op anaesthetic strategies algorithms PVB
bull Surgical technique ()
(eg mesh preservation of nerves
minimally invasive etc)
bull Enhanced recovery hellip
eg Kehlet et al Br J Surgery 2005
Fast Track Surgery
bull Pain clinic follow up
Pathophysiology lsquowhat is it about pain that causes more painrsquo
lsquohelliptransition to chronicityhelliprsquo
1 Nociceptive inflammation ischaemia oedema pressure traction
2 Neuropathic peripheral amp central sensitisation
spinal cord neuroplasticity
neuroma
3 Psychological amp social
4 Genetic
The neuropathic component in persistent pain after surgery
systematic review Haroutiunian PAIN 2013
CPSP after 11 types of surgery
bull Amount of pain depends
bull on likelihood of nerve damage
Neuropathic pain
bull in 65 of thoracotomy patients
bull 33 groin surgery
bull 6 knee surgery
Post surgical breast pain
Jung PAIN 2003
1 Intercostobrachial neuralgia
2 Other nerve injury
3 Neuroma
4 Phantom breast
Natural History
Long-term follow-up of breast cancer survivors with post-mastectomy pain syndrome
Macdonald et al British J of Cancer 2005
1996helliphellip 43 pain 3 years 2002 hellip21 pain 9 years
Persistent pain after breast surgery 6-year nationwide
follow up
Mejdahl Kehlet et al BMJ 2013
2008hellip47 pain 1 year
2013hellip37 pain 6 years
Treatment - prevention
helliphellipfrom Pre-emptive Analgesia (blocking preoperative stimuli)
helliphellipto Preventative Analgesia (blocking noxious stimuli central sensitisation across the entire perioperative period)
Preventative treatments
1 Nerve blocks Regional
2 Drugs
Regional anaesthesia to prevent chronic pain after surgery a Cochrane systematic review and meta-analysisdagger M H Andreae1 and D A Andreae2
BJA 2013
bull 23 RCTrsquos
bull Epidural anaesthesia and
paravertebral blocks may be effective
in preventing chronic pain at 1 year
bull Effective in about 1 in 4
patients treated
Preincisional Paravertebral Block Reduces the Prevalence of Chronic
Pain After Breast Surgery Kairaluoma et al Anesth Analg 2006103703-708
bull Preincisional paravertebral block provides significant immediate postoperative analgesia
bull In the same patients (n = 60) 12 months sig less pain in the PVB group
bull In addition to providing acute postoperative pain relief preoperative PVB reduces the prevalence of chronic pain 1 yr after breast cancer surgery
Epidurals Intraoperative epidural analgesia provides preventative analgesia in
abdominal surgery Lavandrsquohomme et al Anaesthesiology 2005
bull Clear benefit of epidural in preventing chronic pain 1 year
bull Intraoperative epidural better than postoperative epidural
bull Effective epidural better than effective parenteral only analgesia one year
Systematic review of therapeutic interventions to reduce chronic post surgical pain (32 RCTrsquos)
Humble et al European J of Pain (2015)
POSITIVE
Gabapentinoids
Lidocaine
iv lidocaine EMLA
Regional
TIVA
NEGATIVE
Ketamine
Cryoanalgesia
Local anaesthetic infiltration
Remifentanil (increased chronic pain)
1 Gabapentin around time of surgery
lsquono effect on chronic painrsquo
POSITIVE
NEGATIVE
Meta analysis (Clarke 2012) 48 RCTrsquos positive effect at 2 months
Cochrane Systematic Review (Chaparro 2013) 280 patients analysed pain at 6 months No effect
RCT Gabapentin 1200mg prior to Thyroidectomy Sig less pain at 3 months (Brogley 2008)
RCT Gabapentin vs Placebo Knee replacement No effect on chronic pain (Clarke 2014)
2 Pregabalin ndash around time of surgery lsquoNot a recommended treatment can cause post operative somnolencersquo
Positive
Negative
Meta-analysis of 3 studies (Clarke 2012) All showed improvement in pain 2 RCTrsquoshellipvery large decrease in CPSP (p=0007)
3 unpublished RCTrsquos from Pfizer (2010-2014) hellipall negative for acute and chronic pain i) 307 patients undergoing knee replacement ii) 501 patients hysterectomy iii) 425 patient hernia
Cochrane Systematic Review (Chaparro 2013) 25 RCTrsquos significant benefit
Systematic review (Martinez May 2017) No difference between pregabalin and placebo 3 months Use for acute pain in pro-nociceptive surgery Side effects a problem
Multimodal analgesia
bull Standard protocols now widely used eg Paravertebral blocks at MD Anderson bull Pre-assessment clinic screening for pain psychological factors pain catastrophising scale helliphellipgenetic screening tests bull Education patients surgeons anaesthetists nurses psychologists
General treatment strategies for chronic postsurgical neuropathic pain
Preventative Perkins amp Kehlet Anesthesiology 2000
bullSurgical procedure preservation
sentinel node biopsy
bullBetter postoperative pain management
bullInformed consent preparatory
information
Established Dworkin Archives Neurol 2003 60
1524
bull Amitriptyline
bull Gabapentin
bull Opioids
bull Tramadol
bull 5 Lidoderm patch EMLA
Positive therapies for Prevention of PSBP
1 EMLA applied to chest wall prior
to surgery less pain 3 months
Fassoulaki 2000
2 Venlafaxine XR 70mg before
and for 2 weeks post surgeryno diff
acute pain significantly less chronic
pain 6 months
Reuben 2004
3 Aggressive acute pain
management
Iohom 2006
4 Preincisional paravertebral
block
Kairaluoma 2006
5 Multimodal analgesia with
gabapentin EMLA ropivacaine less
acute pain amp pain 6 months
Fassoulaki 2005
A pain management programme for chronic cancer-
treatment-related pain Robb Williams Duvivier Newham
Journal of Pain 2006775-150
bull Theory of cancer-related pain
bull Pain pathways
bull Overunder activity cycle
bull Pacing
bull Exercise and fitness
bull TENS
bull Posture and manual handling
bull Relapse and prevention
Psychology interventions
bull Goal setting
bull Role of factors involved in pain
bull Homework assignments
bull Relaxation techniques
bull Cognitive skills
bull Relapse and prevention
Results
significant (plt005) improvements in
bull Pain severity
bull Psychological distress
bull Pain amp psychological coping indices
bull Activities of daily living
bull General fitness
Research Proposal
Exercise to prevent shoulder conditions in patients
undergoing breast cancer treatment
bull Aim to conduct a randomised controlled trial (RCT) supported with qualitative research to investigate the clinical and cost-effectiveness of early supervised exercise on outcomes of arm function chronic pain and quality of life at one year in women undergoing treatment for breast cancer
Intervention
bull A physiotherapy-led structured exercise programme incorporating behavioural strategies and monitoring to encourage adherence
bull A minimum of 4 face-to-face specialist treatment sessions with individual participants will be
delivered within 12 weeks of surgery bull Access to interim telephone support will be provided The programme will restrict to controlled early
stretching and ROM exercises with subsequent progression to maintain strength and function (weeks 2 to 12)
bull Qualitative interviews will be used during the feasibility phase of the trial to explore acceptability of
to the intervention
Outcomes
bull arm shoulder and hand function at 12 months using the 30-item Disability Arm Shoulder Hand (DASH) questionnaire
bull quality of life
bull Functional Assessment of Cancer Treatment-Breast (FACT-B)
bull Short-Form-12 and EQ-5D-5L
bull Data on postoperative adverse events surgical site infection and healthcare resource use will be collected at 6 and 12 months after surgery
Positive therapies for Prevention of PSBP
1 EMLA applied to chest wall prior
to surgery less pain 3 months
Fassoulaki 2000
2 Venlafaxine XR 70mg before
and for 2 weeks post surgeryno diff
acute pain significantly less chronic
pain 6 months
Reuben 2004
3 Aggressive acute pain
management
Iohom 2006
4 Preincisional paravertebral
block
Kairaluoma 2006
5 Multimodal analgesia with
gabapentin EMLA ropivacaine less
acute pain amp pain 6 months
Fassoulaki 2005
Current Treatment Paradigms
The Toronto General Hospital
Transitional Pain Service
development and implementation
of a multidisciplinary program
to prevent chronic postsurgical pain (Katz J Pain Res 2015)
bull Nurse navigator
bull Psychologists (ACT)
Clinical Manifestations hellipour approach to the patient with CPSP
bull Type of pain Cause
bull Exclude other causes (infection recurrence)
bull Psychological and social factors
bull Temporal Context
Electronic Patient Record
Future Directions
bull Identify Causative Modifiable risk factors vs Associative risk factors
bull Measure psychological variables
bull Genetic assays to identify genes controlling the variability in developing chronic pain
Aim is lsquoto identify susceptibility to chronic pain and sensitivity to analgesicsrsquo
Chronic pain lsquoheritabilityrsquo is variable
Conclusions
bull 1 year incidence = 05 -10 bull Avoid pain before during and after surgery lsquohelliphelliptranslate advances in acute pain to chronic settinghelliphelliprsquo bull Psychological pre-assessment bull Education discussion with patients surgeons bull In some cases preventive analgesia may be beneficial bull Transitional Pain Servicehelliptrackinghellipdatabase lsquoPragmatic approachrsquo lsquoAll diseases have an acute phasersquo lsquoDrugs good for acute pain must be good for chronic painrsquo

Prevalence of chronic pain after breast surgery author year prevalence time
Jamison 1979 44 2 years
Kroner 1989 23 1 year
Vecht 1990 18 6 months
Polinsky 1994 22-32 mean 8 years
Tasmuth 1995 gt50 1 year
Wallace 1996 22- 49 1 year
Smith 1999 43 6 years
Johansen 2000 15 6 years
Fassoulaki 2002 33 3 months
Reuben 2004 50 6 months
Fassoulaki 2005 57 6 months
Kairaluomma 2006 8 1 year
Burton 2007 50 1 year
Hofso 2012 50 1 year
New Definition Old
Macrea BJA 2008 New
Pain April 2017
1 Pain after surgical procedure
1 Pain after a surgical procedure or increases in intensity after a surgical procedure
2 Pain after 2 months 2 Pain after at least 3-6 months hellipwith significant impact on Quality of Life
3 Exclude other causes of the pain
3 Exclude other causes of the pain
4 Exclude pre-existing causes
4 The pain is either a continuation of post surgery pain or develops after an asymptomatic period
5 The pain is either i) localised to the surgical field ii) projected to the innervation territory of a
nerve in the field
Classification of lsquopost mastectomyrsquo pain
1 Pre-existing pain
Osteorheumatoid arthritis Fibromyalgia
Costo-chondritis Cervical radiculopathy
2 Tumour
involvement
Recurrence Metastasis
Cervical radiculopathy due to tumour
3 Post-surgical
Intercostobrachial neuralgia Other neuralgias Persistent lsquoacutersquo pain Scar pain
Phantom breast Intercostal neuromas
Carpal tunnel syndrome Radiation induced plexopathy
Transient brachial neuritis Complex regional pain syndrome
4 Neuropathic
5 Pain due to
implants amp
reconstruction
Capsulitis Capsular contraction and hardening
Foreign body reaction Referred pain Implant migration
Atypical chest pain syndrome Reconstruction lsquoissuesrsquo
6 Other causes
Psychological factors Lymphoedema Pericapsulitis
Muscle spasm lsquoShoulder painrsquo Post-chemo Post- radiotherapy Idiopathic
Myofascial pain dysfunction syndrome
How big a problem is it
In a population of chronic pain patientshelliphow many had pain as a result of surgery Crombie et al Pain 1998 5000 chronic pain patients 23 = CPSP (high proportion with disability) How many people with acute pain go on to get pain at 1 year Hayes et al Acute Pain 2002 5000 patients undergoing surgery Acute neuropathic pain 2 Feature= high intensity 910 Follow up Hayes et al Acute Pain 2002 Pain at 6 months 78 Pain at 1 year 56 lsquo26 million operations year in USA (2008) 1 of all patients develop CPSPrsquo (Katz 2011)
What this study adds bull 3 of patients who had not used opioids previously continued to use them for more than 90 days after major elective surgery bullImportant public health concern because millions of patients undergo major surgery every year
Clarke et al British Medical Journal 2014
Risk factorshellip 1 Causal Modifiable Risk factors (Katz Anesth amp Analg 2011)
Acute pain
Pre-existing pain
Psychological factors
2 Correlated risk factors (Katz Anesth amp Analg 2011)
Younger age
Gender
Psychological distress
Pain
Risk factors
1 Patient related
2 Surgery related
Patient-related risk factors lsquohellippain predicts painrsquo
bull Preoperative pain (Forsythe 2008)
bull Intensity of acute pain (Masselin-Dubois 2013)
bull Acute neuropathic pain (Haroutiounian 2013)
bull High opioid consumption perioperatively (Kalso 2001)
bull Pain in other body parts (Pinto 2012)
bull Younger age (Masselin-Dubois 2013)
bull Female (Ochroch 2006)
Psychological risk factors
bull Pre-op anxiety and catastrophizing meta analysis (2x likelihood of developing CPSP (Theunissen Clin J Pain 2012)
bull Depression (Attal 2014)
bull Catastrophizing (Masselin-Dubois 2013)
bull Sensitivity to pain traumatisation (Page 2013)
bull Anxiety (Kleimann 2011)
bull Fear of long term consequences of surgery (Peters 2007)
Surgical risk factors
bull Low vs high volume surgical unit 13 increase in risk of CPSP (Tasmuth1999)
bull Duration of surgery (Kalso 2007)
bull Minimally invasive surgery (Grant 2004)
bull Stitch types (Cerfolio 2003)
bull Nerve damage preservation (Jensen 1985)
Predictive factors for chronic pain after breast surgery
Anderson et al Pain 2015 n=575
Pain at 1 year
bull Moderate- severe post op pain (50)
bull Axillary lymph node with ICB nerve preservation (30)
bull Neuropathic pain 1 week (18)
bull Age lt 65 (18)
Wang Canadian Medical Assoc Journal 2016 bull Young age bull Axillary lymph node dissection bull Acute pain High quality evidence showed no association
with BMI Type of breast surgery Chemotherapy Reconstruction
Clinical Prediction Model and Tool for Assessing Risk of Persistent Pain After Breast Cancer Surgery Tuomo J Meretoja Kenneth Geving Andersen Julie Bruce Lassi Haasio Reetta Sipilauml Neil W Scott Samuli Ripatti Henrik Kehlet and Eija Kalso
March 2017
Risk Factors ndash what can we discuss with surgeons
bull Information for patients
bull Pre-assessment pain clinic
bull Pre-op anaesthetic strategies algorithms PVB
bull Surgical technique ()
(eg mesh preservation of nerves
minimally invasive etc)
bull Enhanced recovery hellip
eg Kehlet et al Br J Surgery 2005
Fast Track Surgery
bull Pain clinic follow up
Pathophysiology lsquowhat is it about pain that causes more painrsquo
lsquohelliptransition to chronicityhelliprsquo
1 Nociceptive inflammation ischaemia oedema pressure traction
2 Neuropathic peripheral amp central sensitisation
spinal cord neuroplasticity
neuroma
3 Psychological amp social
4 Genetic
The neuropathic component in persistent pain after surgery
systematic review Haroutiunian PAIN 2013
CPSP after 11 types of surgery
bull Amount of pain depends
bull on likelihood of nerve damage
Neuropathic pain
bull in 65 of thoracotomy patients
bull 33 groin surgery
bull 6 knee surgery
Post surgical breast pain
Jung PAIN 2003
1 Intercostobrachial neuralgia
2 Other nerve injury
3 Neuroma
4 Phantom breast
Natural History
Long-term follow-up of breast cancer survivors with post-mastectomy pain syndrome
Macdonald et al British J of Cancer 2005
1996helliphellip 43 pain 3 years 2002 hellip21 pain 9 years
Persistent pain after breast surgery 6-year nationwide
follow up
Mejdahl Kehlet et al BMJ 2013
2008hellip47 pain 1 year
2013hellip37 pain 6 years
Treatment - prevention
helliphellipfrom Pre-emptive Analgesia (blocking preoperative stimuli)
helliphellipto Preventative Analgesia (blocking noxious stimuli central sensitisation across the entire perioperative period)
Preventative treatments
1 Nerve blocks Regional
2 Drugs
Regional anaesthesia to prevent chronic pain after surgery a Cochrane systematic review and meta-analysisdagger M H Andreae1 and D A Andreae2
BJA 2013
bull 23 RCTrsquos
bull Epidural anaesthesia and
paravertebral blocks may be effective
in preventing chronic pain at 1 year
bull Effective in about 1 in 4
patients treated
Preincisional Paravertebral Block Reduces the Prevalence of Chronic
Pain After Breast Surgery Kairaluoma et al Anesth Analg 2006103703-708
bull Preincisional paravertebral block provides significant immediate postoperative analgesia
bull In the same patients (n = 60) 12 months sig less pain in the PVB group
bull In addition to providing acute postoperative pain relief preoperative PVB reduces the prevalence of chronic pain 1 yr after breast cancer surgery
Epidurals Intraoperative epidural analgesia provides preventative analgesia in
abdominal surgery Lavandrsquohomme et al Anaesthesiology 2005
bull Clear benefit of epidural in preventing chronic pain 1 year
bull Intraoperative epidural better than postoperative epidural
bull Effective epidural better than effective parenteral only analgesia one year
Systematic review of therapeutic interventions to reduce chronic post surgical pain (32 RCTrsquos)
Humble et al European J of Pain (2015)
POSITIVE
Gabapentinoids
Lidocaine
iv lidocaine EMLA
Regional
TIVA
NEGATIVE
Ketamine
Cryoanalgesia
Local anaesthetic infiltration
Remifentanil (increased chronic pain)
1 Gabapentin around time of surgery
lsquono effect on chronic painrsquo
POSITIVE
NEGATIVE
Meta analysis (Clarke 2012) 48 RCTrsquos positive effect at 2 months
Cochrane Systematic Review (Chaparro 2013) 280 patients analysed pain at 6 months No effect
RCT Gabapentin 1200mg prior to Thyroidectomy Sig less pain at 3 months (Brogley 2008)
RCT Gabapentin vs Placebo Knee replacement No effect on chronic pain (Clarke 2014)
2 Pregabalin ndash around time of surgery lsquoNot a recommended treatment can cause post operative somnolencersquo
Positive
Negative
Meta-analysis of 3 studies (Clarke 2012) All showed improvement in pain 2 RCTrsquoshellipvery large decrease in CPSP (p=0007)
3 unpublished RCTrsquos from Pfizer (2010-2014) hellipall negative for acute and chronic pain i) 307 patients undergoing knee replacement ii) 501 patients hysterectomy iii) 425 patient hernia
Cochrane Systematic Review (Chaparro 2013) 25 RCTrsquos significant benefit
Systematic review (Martinez May 2017) No difference between pregabalin and placebo 3 months Use for acute pain in pro-nociceptive surgery Side effects a problem
Multimodal analgesia
bull Standard protocols now widely used eg Paravertebral blocks at MD Anderson bull Pre-assessment clinic screening for pain psychological factors pain catastrophising scale helliphellipgenetic screening tests bull Education patients surgeons anaesthetists nurses psychologists
General treatment strategies for chronic postsurgical neuropathic pain
Preventative Perkins amp Kehlet Anesthesiology 2000
bullSurgical procedure preservation
sentinel node biopsy
bullBetter postoperative pain management
bullInformed consent preparatory
information
Established Dworkin Archives Neurol 2003 60
1524
bull Amitriptyline
bull Gabapentin
bull Opioids
bull Tramadol
bull 5 Lidoderm patch EMLA
Positive therapies for Prevention of PSBP
1 EMLA applied to chest wall prior
to surgery less pain 3 months
Fassoulaki 2000
2 Venlafaxine XR 70mg before
and for 2 weeks post surgeryno diff
acute pain significantly less chronic
pain 6 months
Reuben 2004
3 Aggressive acute pain
management
Iohom 2006
4 Preincisional paravertebral
block
Kairaluoma 2006
5 Multimodal analgesia with
gabapentin EMLA ropivacaine less
acute pain amp pain 6 months
Fassoulaki 2005
A pain management programme for chronic cancer-
treatment-related pain Robb Williams Duvivier Newham
Journal of Pain 2006775-150
bull Theory of cancer-related pain
bull Pain pathways
bull Overunder activity cycle
bull Pacing
bull Exercise and fitness
bull TENS
bull Posture and manual handling
bull Relapse and prevention
Psychology interventions
bull Goal setting
bull Role of factors involved in pain
bull Homework assignments
bull Relaxation techniques
bull Cognitive skills
bull Relapse and prevention
Results
significant (plt005) improvements in
bull Pain severity
bull Psychological distress
bull Pain amp psychological coping indices
bull Activities of daily living
bull General fitness
Research Proposal
Exercise to prevent shoulder conditions in patients
undergoing breast cancer treatment
bull Aim to conduct a randomised controlled trial (RCT) supported with qualitative research to investigate the clinical and cost-effectiveness of early supervised exercise on outcomes of arm function chronic pain and quality of life at one year in women undergoing treatment for breast cancer
Intervention
bull A physiotherapy-led structured exercise programme incorporating behavioural strategies and monitoring to encourage adherence
bull A minimum of 4 face-to-face specialist treatment sessions with individual participants will be
delivered within 12 weeks of surgery bull Access to interim telephone support will be provided The programme will restrict to controlled early
stretching and ROM exercises with subsequent progression to maintain strength and function (weeks 2 to 12)
bull Qualitative interviews will be used during the feasibility phase of the trial to explore acceptability of
to the intervention
Outcomes
bull arm shoulder and hand function at 12 months using the 30-item Disability Arm Shoulder Hand (DASH) questionnaire
bull quality of life
bull Functional Assessment of Cancer Treatment-Breast (FACT-B)
bull Short-Form-12 and EQ-5D-5L
bull Data on postoperative adverse events surgical site infection and healthcare resource use will be collected at 6 and 12 months after surgery
Positive therapies for Prevention of PSBP
1 EMLA applied to chest wall prior
to surgery less pain 3 months
Fassoulaki 2000
2 Venlafaxine XR 70mg before
and for 2 weeks post surgeryno diff
acute pain significantly less chronic
pain 6 months
Reuben 2004
3 Aggressive acute pain
management
Iohom 2006
4 Preincisional paravertebral
block
Kairaluoma 2006
5 Multimodal analgesia with
gabapentin EMLA ropivacaine less
acute pain amp pain 6 months
Fassoulaki 2005
Current Treatment Paradigms
The Toronto General Hospital
Transitional Pain Service
development and implementation
of a multidisciplinary program
to prevent chronic postsurgical pain (Katz J Pain Res 2015)
bull Nurse navigator
bull Psychologists (ACT)
Clinical Manifestations hellipour approach to the patient with CPSP
bull Type of pain Cause
bull Exclude other causes (infection recurrence)
bull Psychological and social factors
bull Temporal Context
Electronic Patient Record
Future Directions
bull Identify Causative Modifiable risk factors vs Associative risk factors
bull Measure psychological variables
bull Genetic assays to identify genes controlling the variability in developing chronic pain
Aim is lsquoto identify susceptibility to chronic pain and sensitivity to analgesicsrsquo
Chronic pain lsquoheritabilityrsquo is variable
Conclusions
bull 1 year incidence = 05 -10 bull Avoid pain before during and after surgery lsquohelliphelliptranslate advances in acute pain to chronic settinghelliphelliprsquo bull Psychological pre-assessment bull Education discussion with patients surgeons bull In some cases preventive analgesia may be beneficial bull Transitional Pain Servicehelliptrackinghellipdatabase lsquoPragmatic approachrsquo lsquoAll diseases have an acute phasersquo lsquoDrugs good for acute pain must be good for chronic painrsquo

New Definition Old
Macrea BJA 2008 New
Pain April 2017
1 Pain after surgical procedure
1 Pain after a surgical procedure or increases in intensity after a surgical procedure
2 Pain after 2 months 2 Pain after at least 3-6 months hellipwith significant impact on Quality of Life
3 Exclude other causes of the pain
3 Exclude other causes of the pain
4 Exclude pre-existing causes
4 The pain is either a continuation of post surgery pain or develops after an asymptomatic period
5 The pain is either i) localised to the surgical field ii) projected to the innervation territory of a
nerve in the field
Classification of lsquopost mastectomyrsquo pain
1 Pre-existing pain
Osteorheumatoid arthritis Fibromyalgia
Costo-chondritis Cervical radiculopathy
2 Tumour
involvement
Recurrence Metastasis
Cervical radiculopathy due to tumour
3 Post-surgical
Intercostobrachial neuralgia Other neuralgias Persistent lsquoacutersquo pain Scar pain
Phantom breast Intercostal neuromas
Carpal tunnel syndrome Radiation induced plexopathy
Transient brachial neuritis Complex regional pain syndrome
4 Neuropathic
5 Pain due to
implants amp
reconstruction
Capsulitis Capsular contraction and hardening
Foreign body reaction Referred pain Implant migration
Atypical chest pain syndrome Reconstruction lsquoissuesrsquo
6 Other causes
Psychological factors Lymphoedema Pericapsulitis
Muscle spasm lsquoShoulder painrsquo Post-chemo Post- radiotherapy Idiopathic
Myofascial pain dysfunction syndrome
How big a problem is it
In a population of chronic pain patientshelliphow many had pain as a result of surgery Crombie et al Pain 1998 5000 chronic pain patients 23 = CPSP (high proportion with disability) How many people with acute pain go on to get pain at 1 year Hayes et al Acute Pain 2002 5000 patients undergoing surgery Acute neuropathic pain 2 Feature= high intensity 910 Follow up Hayes et al Acute Pain 2002 Pain at 6 months 78 Pain at 1 year 56 lsquo26 million operations year in USA (2008) 1 of all patients develop CPSPrsquo (Katz 2011)
What this study adds bull 3 of patients who had not used opioids previously continued to use them for more than 90 days after major elective surgery bullImportant public health concern because millions of patients undergo major surgery every year
Clarke et al British Medical Journal 2014
Risk factorshellip 1 Causal Modifiable Risk factors (Katz Anesth amp Analg 2011)
Acute pain
Pre-existing pain
Psychological factors
2 Correlated risk factors (Katz Anesth amp Analg 2011)
Younger age
Gender
Psychological distress
Pain
Risk factors
1 Patient related
2 Surgery related
Patient-related risk factors lsquohellippain predicts painrsquo
bull Preoperative pain (Forsythe 2008)
bull Intensity of acute pain (Masselin-Dubois 2013)
bull Acute neuropathic pain (Haroutiounian 2013)
bull High opioid consumption perioperatively (Kalso 2001)
bull Pain in other body parts (Pinto 2012)
bull Younger age (Masselin-Dubois 2013)
bull Female (Ochroch 2006)
Psychological risk factors
bull Pre-op anxiety and catastrophizing meta analysis (2x likelihood of developing CPSP (Theunissen Clin J Pain 2012)
bull Depression (Attal 2014)
bull Catastrophizing (Masselin-Dubois 2013)
bull Sensitivity to pain traumatisation (Page 2013)
bull Anxiety (Kleimann 2011)
bull Fear of long term consequences of surgery (Peters 2007)
Surgical risk factors
bull Low vs high volume surgical unit 13 increase in risk of CPSP (Tasmuth1999)
bull Duration of surgery (Kalso 2007)
bull Minimally invasive surgery (Grant 2004)
bull Stitch types (Cerfolio 2003)
bull Nerve damage preservation (Jensen 1985)
Predictive factors for chronic pain after breast surgery
Anderson et al Pain 2015 n=575
Pain at 1 year
bull Moderate- severe post op pain (50)
bull Axillary lymph node with ICB nerve preservation (30)
bull Neuropathic pain 1 week (18)
bull Age lt 65 (18)
Wang Canadian Medical Assoc Journal 2016 bull Young age bull Axillary lymph node dissection bull Acute pain High quality evidence showed no association
with BMI Type of breast surgery Chemotherapy Reconstruction
Clinical Prediction Model and Tool for Assessing Risk of Persistent Pain After Breast Cancer Surgery Tuomo J Meretoja Kenneth Geving Andersen Julie Bruce Lassi Haasio Reetta Sipilauml Neil W Scott Samuli Ripatti Henrik Kehlet and Eija Kalso
March 2017
Risk Factors ndash what can we discuss with surgeons
bull Information for patients
bull Pre-assessment pain clinic
bull Pre-op anaesthetic strategies algorithms PVB
bull Surgical technique ()
(eg mesh preservation of nerves
minimally invasive etc)
bull Enhanced recovery hellip
eg Kehlet et al Br J Surgery 2005
Fast Track Surgery
bull Pain clinic follow up
Pathophysiology lsquowhat is it about pain that causes more painrsquo
lsquohelliptransition to chronicityhelliprsquo
1 Nociceptive inflammation ischaemia oedema pressure traction
2 Neuropathic peripheral amp central sensitisation
spinal cord neuroplasticity
neuroma
3 Psychological amp social
4 Genetic
The neuropathic component in persistent pain after surgery
systematic review Haroutiunian PAIN 2013
CPSP after 11 types of surgery
bull Amount of pain depends
bull on likelihood of nerve damage
Neuropathic pain
bull in 65 of thoracotomy patients
bull 33 groin surgery
bull 6 knee surgery
Post surgical breast pain
Jung PAIN 2003
1 Intercostobrachial neuralgia
2 Other nerve injury
3 Neuroma
4 Phantom breast
Natural History
Long-term follow-up of breast cancer survivors with post-mastectomy pain syndrome
Macdonald et al British J of Cancer 2005
1996helliphellip 43 pain 3 years 2002 hellip21 pain 9 years
Persistent pain after breast surgery 6-year nationwide
follow up
Mejdahl Kehlet et al BMJ 2013
2008hellip47 pain 1 year
2013hellip37 pain 6 years
Treatment - prevention
helliphellipfrom Pre-emptive Analgesia (blocking preoperative stimuli)
helliphellipto Preventative Analgesia (blocking noxious stimuli central sensitisation across the entire perioperative period)
Preventative treatments
1 Nerve blocks Regional
2 Drugs
Regional anaesthesia to prevent chronic pain after surgery a Cochrane systematic review and meta-analysisdagger M H Andreae1 and D A Andreae2
BJA 2013
bull 23 RCTrsquos
bull Epidural anaesthesia and
paravertebral blocks may be effective
in preventing chronic pain at 1 year
bull Effective in about 1 in 4
patients treated
Preincisional Paravertebral Block Reduces the Prevalence of Chronic
Pain After Breast Surgery Kairaluoma et al Anesth Analg 2006103703-708
bull Preincisional paravertebral block provides significant immediate postoperative analgesia
bull In the same patients (n = 60) 12 months sig less pain in the PVB group
bull In addition to providing acute postoperative pain relief preoperative PVB reduces the prevalence of chronic pain 1 yr after breast cancer surgery
Epidurals Intraoperative epidural analgesia provides preventative analgesia in
abdominal surgery Lavandrsquohomme et al Anaesthesiology 2005
bull Clear benefit of epidural in preventing chronic pain 1 year
bull Intraoperative epidural better than postoperative epidural
bull Effective epidural better than effective parenteral only analgesia one year
Systematic review of therapeutic interventions to reduce chronic post surgical pain (32 RCTrsquos)
Humble et al European J of Pain (2015)
POSITIVE
Gabapentinoids
Lidocaine
iv lidocaine EMLA
Regional
TIVA
NEGATIVE
Ketamine
Cryoanalgesia
Local anaesthetic infiltration
Remifentanil (increased chronic pain)
1 Gabapentin around time of surgery
lsquono effect on chronic painrsquo
POSITIVE
NEGATIVE
Meta analysis (Clarke 2012) 48 RCTrsquos positive effect at 2 months
Cochrane Systematic Review (Chaparro 2013) 280 patients analysed pain at 6 months No effect
RCT Gabapentin 1200mg prior to Thyroidectomy Sig less pain at 3 months (Brogley 2008)
RCT Gabapentin vs Placebo Knee replacement No effect on chronic pain (Clarke 2014)
2 Pregabalin ndash around time of surgery lsquoNot a recommended treatment can cause post operative somnolencersquo
Positive
Negative
Meta-analysis of 3 studies (Clarke 2012) All showed improvement in pain 2 RCTrsquoshellipvery large decrease in CPSP (p=0007)
3 unpublished RCTrsquos from Pfizer (2010-2014) hellipall negative for acute and chronic pain i) 307 patients undergoing knee replacement ii) 501 patients hysterectomy iii) 425 patient hernia
Cochrane Systematic Review (Chaparro 2013) 25 RCTrsquos significant benefit
Systematic review (Martinez May 2017) No difference between pregabalin and placebo 3 months Use for acute pain in pro-nociceptive surgery Side effects a problem
Multimodal analgesia
bull Standard protocols now widely used eg Paravertebral blocks at MD Anderson bull Pre-assessment clinic screening for pain psychological factors pain catastrophising scale helliphellipgenetic screening tests bull Education patients surgeons anaesthetists nurses psychologists
General treatment strategies for chronic postsurgical neuropathic pain
Preventative Perkins amp Kehlet Anesthesiology 2000
bullSurgical procedure preservation
sentinel node biopsy
bullBetter postoperative pain management
bullInformed consent preparatory
information
Established Dworkin Archives Neurol 2003 60
1524
bull Amitriptyline
bull Gabapentin
bull Opioids
bull Tramadol
bull 5 Lidoderm patch EMLA
Positive therapies for Prevention of PSBP
1 EMLA applied to chest wall prior
to surgery less pain 3 months
Fassoulaki 2000
2 Venlafaxine XR 70mg before
and for 2 weeks post surgeryno diff
acute pain significantly less chronic
pain 6 months
Reuben 2004
3 Aggressive acute pain
management
Iohom 2006
4 Preincisional paravertebral
block
Kairaluoma 2006
5 Multimodal analgesia with
gabapentin EMLA ropivacaine less
acute pain amp pain 6 months
Fassoulaki 2005
A pain management programme for chronic cancer-
treatment-related pain Robb Williams Duvivier Newham
Journal of Pain 2006775-150
bull Theory of cancer-related pain
bull Pain pathways
bull Overunder activity cycle
bull Pacing
bull Exercise and fitness
bull TENS
bull Posture and manual handling
bull Relapse and prevention
Psychology interventions
bull Goal setting
bull Role of factors involved in pain
bull Homework assignments
bull Relaxation techniques
bull Cognitive skills
bull Relapse and prevention
Results
significant (plt005) improvements in
bull Pain severity
bull Psychological distress
bull Pain amp psychological coping indices
bull Activities of daily living
bull General fitness
Research Proposal
Exercise to prevent shoulder conditions in patients
undergoing breast cancer treatment
bull Aim to conduct a randomised controlled trial (RCT) supported with qualitative research to investigate the clinical and cost-effectiveness of early supervised exercise on outcomes of arm function chronic pain and quality of life at one year in women undergoing treatment for breast cancer
Intervention
bull A physiotherapy-led structured exercise programme incorporating behavioural strategies and monitoring to encourage adherence
bull A minimum of 4 face-to-face specialist treatment sessions with individual participants will be
delivered within 12 weeks of surgery bull Access to interim telephone support will be provided The programme will restrict to controlled early
stretching and ROM exercises with subsequent progression to maintain strength and function (weeks 2 to 12)
bull Qualitative interviews will be used during the feasibility phase of the trial to explore acceptability of
to the intervention
Outcomes
bull arm shoulder and hand function at 12 months using the 30-item Disability Arm Shoulder Hand (DASH) questionnaire
bull quality of life
bull Functional Assessment of Cancer Treatment-Breast (FACT-B)
bull Short-Form-12 and EQ-5D-5L
bull Data on postoperative adverse events surgical site infection and healthcare resource use will be collected at 6 and 12 months after surgery
Positive therapies for Prevention of PSBP
1 EMLA applied to chest wall prior
to surgery less pain 3 months
Fassoulaki 2000
2 Venlafaxine XR 70mg before
and for 2 weeks post surgeryno diff
acute pain significantly less chronic
pain 6 months
Reuben 2004
3 Aggressive acute pain
management
Iohom 2006
4 Preincisional paravertebral
block
Kairaluoma 2006
5 Multimodal analgesia with
gabapentin EMLA ropivacaine less
acute pain amp pain 6 months
Fassoulaki 2005
Current Treatment Paradigms
The Toronto General Hospital
Transitional Pain Service
development and implementation
of a multidisciplinary program
to prevent chronic postsurgical pain (Katz J Pain Res 2015)
bull Nurse navigator
bull Psychologists (ACT)
Clinical Manifestations hellipour approach to the patient with CPSP
bull Type of pain Cause
bull Exclude other causes (infection recurrence)
bull Psychological and social factors
bull Temporal Context
Electronic Patient Record
Future Directions
bull Identify Causative Modifiable risk factors vs Associative risk factors
bull Measure psychological variables
bull Genetic assays to identify genes controlling the variability in developing chronic pain
Aim is lsquoto identify susceptibility to chronic pain and sensitivity to analgesicsrsquo
Chronic pain lsquoheritabilityrsquo is variable
Conclusions
bull 1 year incidence = 05 -10 bull Avoid pain before during and after surgery lsquohelliphelliptranslate advances in acute pain to chronic settinghelliphelliprsquo bull Psychological pre-assessment bull Education discussion with patients surgeons bull In some cases preventive analgesia may be beneficial bull Transitional Pain Servicehelliptrackinghellipdatabase lsquoPragmatic approachrsquo lsquoAll diseases have an acute phasersquo lsquoDrugs good for acute pain must be good for chronic painrsquo

Classification of lsquopost mastectomyrsquo pain
1 Pre-existing pain
Osteorheumatoid arthritis Fibromyalgia
Costo-chondritis Cervical radiculopathy
2 Tumour
involvement
Recurrence Metastasis
Cervical radiculopathy due to tumour
3 Post-surgical
Intercostobrachial neuralgia Other neuralgias Persistent lsquoacutersquo pain Scar pain
Phantom breast Intercostal neuromas
Carpal tunnel syndrome Radiation induced plexopathy
Transient brachial neuritis Complex regional pain syndrome
4 Neuropathic
5 Pain due to
implants amp
reconstruction
Capsulitis Capsular contraction and hardening
Foreign body reaction Referred pain Implant migration
Atypical chest pain syndrome Reconstruction lsquoissuesrsquo
6 Other causes
Psychological factors Lymphoedema Pericapsulitis
Muscle spasm lsquoShoulder painrsquo Post-chemo Post- radiotherapy Idiopathic
Myofascial pain dysfunction syndrome
How big a problem is it
In a population of chronic pain patientshelliphow many had pain as a result of surgery Crombie et al Pain 1998 5000 chronic pain patients 23 = CPSP (high proportion with disability) How many people with acute pain go on to get pain at 1 year Hayes et al Acute Pain 2002 5000 patients undergoing surgery Acute neuropathic pain 2 Feature= high intensity 910 Follow up Hayes et al Acute Pain 2002 Pain at 6 months 78 Pain at 1 year 56 lsquo26 million operations year in USA (2008) 1 of all patients develop CPSPrsquo (Katz 2011)
What this study adds bull 3 of patients who had not used opioids previously continued to use them for more than 90 days after major elective surgery bullImportant public health concern because millions of patients undergo major surgery every year
Clarke et al British Medical Journal 2014
Risk factorshellip 1 Causal Modifiable Risk factors (Katz Anesth amp Analg 2011)
Acute pain
Pre-existing pain
Psychological factors
2 Correlated risk factors (Katz Anesth amp Analg 2011)
Younger age
Gender
Psychological distress
Pain
Risk factors
1 Patient related
2 Surgery related
Patient-related risk factors lsquohellippain predicts painrsquo
bull Preoperative pain (Forsythe 2008)
bull Intensity of acute pain (Masselin-Dubois 2013)
bull Acute neuropathic pain (Haroutiounian 2013)
bull High opioid consumption perioperatively (Kalso 2001)
bull Pain in other body parts (Pinto 2012)
bull Younger age (Masselin-Dubois 2013)
bull Female (Ochroch 2006)
Psychological risk factors
bull Pre-op anxiety and catastrophizing meta analysis (2x likelihood of developing CPSP (Theunissen Clin J Pain 2012)
bull Depression (Attal 2014)
bull Catastrophizing (Masselin-Dubois 2013)
bull Sensitivity to pain traumatisation (Page 2013)
bull Anxiety (Kleimann 2011)
bull Fear of long term consequences of surgery (Peters 2007)
Surgical risk factors
bull Low vs high volume surgical unit 13 increase in risk of CPSP (Tasmuth1999)
bull Duration of surgery (Kalso 2007)
bull Minimally invasive surgery (Grant 2004)
bull Stitch types (Cerfolio 2003)
bull Nerve damage preservation (Jensen 1985)
Predictive factors for chronic pain after breast surgery
Anderson et al Pain 2015 n=575
Pain at 1 year
bull Moderate- severe post op pain (50)
bull Axillary lymph node with ICB nerve preservation (30)
bull Neuropathic pain 1 week (18)
bull Age lt 65 (18)
Wang Canadian Medical Assoc Journal 2016 bull Young age bull Axillary lymph node dissection bull Acute pain High quality evidence showed no association
with BMI Type of breast surgery Chemotherapy Reconstruction
Clinical Prediction Model and Tool for Assessing Risk of Persistent Pain After Breast Cancer Surgery Tuomo J Meretoja Kenneth Geving Andersen Julie Bruce Lassi Haasio Reetta Sipilauml Neil W Scott Samuli Ripatti Henrik Kehlet and Eija Kalso
March 2017
Risk Factors ndash what can we discuss with surgeons
bull Information for patients
bull Pre-assessment pain clinic
bull Pre-op anaesthetic strategies algorithms PVB
bull Surgical technique ()
(eg mesh preservation of nerves
minimally invasive etc)
bull Enhanced recovery hellip
eg Kehlet et al Br J Surgery 2005
Fast Track Surgery
bull Pain clinic follow up
Pathophysiology lsquowhat is it about pain that causes more painrsquo
lsquohelliptransition to chronicityhelliprsquo
1 Nociceptive inflammation ischaemia oedema pressure traction
2 Neuropathic peripheral amp central sensitisation
spinal cord neuroplasticity
neuroma
3 Psychological amp social
4 Genetic
The neuropathic component in persistent pain after surgery
systematic review Haroutiunian PAIN 2013
CPSP after 11 types of surgery
bull Amount of pain depends
bull on likelihood of nerve damage
Neuropathic pain
bull in 65 of thoracotomy patients
bull 33 groin surgery
bull 6 knee surgery
Post surgical breast pain
Jung PAIN 2003
1 Intercostobrachial neuralgia
2 Other nerve injury
3 Neuroma
4 Phantom breast
Natural History
Long-term follow-up of breast cancer survivors with post-mastectomy pain syndrome
Macdonald et al British J of Cancer 2005
1996helliphellip 43 pain 3 years 2002 hellip21 pain 9 years
Persistent pain after breast surgery 6-year nationwide
follow up
Mejdahl Kehlet et al BMJ 2013
2008hellip47 pain 1 year
2013hellip37 pain 6 years
Treatment - prevention
helliphellipfrom Pre-emptive Analgesia (blocking preoperative stimuli)
helliphellipto Preventative Analgesia (blocking noxious stimuli central sensitisation across the entire perioperative period)
Preventative treatments
1 Nerve blocks Regional
2 Drugs
Regional anaesthesia to prevent chronic pain after surgery a Cochrane systematic review and meta-analysisdagger M H Andreae1 and D A Andreae2
BJA 2013
bull 23 RCTrsquos
bull Epidural anaesthesia and
paravertebral blocks may be effective
in preventing chronic pain at 1 year
bull Effective in about 1 in 4
patients treated
Preincisional Paravertebral Block Reduces the Prevalence of Chronic
Pain After Breast Surgery Kairaluoma et al Anesth Analg 2006103703-708
bull Preincisional paravertebral block provides significant immediate postoperative analgesia
bull In the same patients (n = 60) 12 months sig less pain in the PVB group
bull In addition to providing acute postoperative pain relief preoperative PVB reduces the prevalence of chronic pain 1 yr after breast cancer surgery
Epidurals Intraoperative epidural analgesia provides preventative analgesia in
abdominal surgery Lavandrsquohomme et al Anaesthesiology 2005
bull Clear benefit of epidural in preventing chronic pain 1 year
bull Intraoperative epidural better than postoperative epidural
bull Effective epidural better than effective parenteral only analgesia one year
Systematic review of therapeutic interventions to reduce chronic post surgical pain (32 RCTrsquos)
Humble et al European J of Pain (2015)
POSITIVE
Gabapentinoids
Lidocaine
iv lidocaine EMLA
Regional
TIVA
NEGATIVE
Ketamine
Cryoanalgesia
Local anaesthetic infiltration
Remifentanil (increased chronic pain)
1 Gabapentin around time of surgery
lsquono effect on chronic painrsquo
POSITIVE
NEGATIVE
Meta analysis (Clarke 2012) 48 RCTrsquos positive effect at 2 months
Cochrane Systematic Review (Chaparro 2013) 280 patients analysed pain at 6 months No effect
RCT Gabapentin 1200mg prior to Thyroidectomy Sig less pain at 3 months (Brogley 2008)
RCT Gabapentin vs Placebo Knee replacement No effect on chronic pain (Clarke 2014)
2 Pregabalin ndash around time of surgery lsquoNot a recommended treatment can cause post operative somnolencersquo
Positive
Negative
Meta-analysis of 3 studies (Clarke 2012) All showed improvement in pain 2 RCTrsquoshellipvery large decrease in CPSP (p=0007)
3 unpublished RCTrsquos from Pfizer (2010-2014) hellipall negative for acute and chronic pain i) 307 patients undergoing knee replacement ii) 501 patients hysterectomy iii) 425 patient hernia
Cochrane Systematic Review (Chaparro 2013) 25 RCTrsquos significant benefit
Systematic review (Martinez May 2017) No difference between pregabalin and placebo 3 months Use for acute pain in pro-nociceptive surgery Side effects a problem
Multimodal analgesia
bull Standard protocols now widely used eg Paravertebral blocks at MD Anderson bull Pre-assessment clinic screening for pain psychological factors pain catastrophising scale helliphellipgenetic screening tests bull Education patients surgeons anaesthetists nurses psychologists
General treatment strategies for chronic postsurgical neuropathic pain
Preventative Perkins amp Kehlet Anesthesiology 2000
bullSurgical procedure preservation
sentinel node biopsy
bullBetter postoperative pain management
bullInformed consent preparatory
information
Established Dworkin Archives Neurol 2003 60
1524
bull Amitriptyline
bull Gabapentin
bull Opioids
bull Tramadol
bull 5 Lidoderm patch EMLA
Positive therapies for Prevention of PSBP
1 EMLA applied to chest wall prior
to surgery less pain 3 months
Fassoulaki 2000
2 Venlafaxine XR 70mg before
and for 2 weeks post surgeryno diff
acute pain significantly less chronic
pain 6 months
Reuben 2004
3 Aggressive acute pain
management
Iohom 2006
4 Preincisional paravertebral
block
Kairaluoma 2006
5 Multimodal analgesia with
gabapentin EMLA ropivacaine less
acute pain amp pain 6 months
Fassoulaki 2005
A pain management programme for chronic cancer-
treatment-related pain Robb Williams Duvivier Newham
Journal of Pain 2006775-150
bull Theory of cancer-related pain
bull Pain pathways
bull Overunder activity cycle
bull Pacing
bull Exercise and fitness
bull TENS
bull Posture and manual handling
bull Relapse and prevention
Psychology interventions
bull Goal setting
bull Role of factors involved in pain
bull Homework assignments
bull Relaxation techniques
bull Cognitive skills
bull Relapse and prevention
Results
significant (plt005) improvements in
bull Pain severity
bull Psychological distress
bull Pain amp psychological coping indices
bull Activities of daily living
bull General fitness
Research Proposal
Exercise to prevent shoulder conditions in patients
undergoing breast cancer treatment
bull Aim to conduct a randomised controlled trial (RCT) supported with qualitative research to investigate the clinical and cost-effectiveness of early supervised exercise on outcomes of arm function chronic pain and quality of life at one year in women undergoing treatment for breast cancer
Intervention
bull A physiotherapy-led structured exercise programme incorporating behavioural strategies and monitoring to encourage adherence
bull A minimum of 4 face-to-face specialist treatment sessions with individual participants will be
delivered within 12 weeks of surgery bull Access to interim telephone support will be provided The programme will restrict to controlled early
stretching and ROM exercises with subsequent progression to maintain strength and function (weeks 2 to 12)
bull Qualitative interviews will be used during the feasibility phase of the trial to explore acceptability of
to the intervention
Outcomes
bull arm shoulder and hand function at 12 months using the 30-item Disability Arm Shoulder Hand (DASH) questionnaire
bull quality of life
bull Functional Assessment of Cancer Treatment-Breast (FACT-B)
bull Short-Form-12 and EQ-5D-5L
bull Data on postoperative adverse events surgical site infection and healthcare resource use will be collected at 6 and 12 months after surgery
Positive therapies for Prevention of PSBP
1 EMLA applied to chest wall prior
to surgery less pain 3 months
Fassoulaki 2000
2 Venlafaxine XR 70mg before
and for 2 weeks post surgeryno diff
acute pain significantly less chronic
pain 6 months
Reuben 2004
3 Aggressive acute pain
management
Iohom 2006
4 Preincisional paravertebral
block
Kairaluoma 2006
5 Multimodal analgesia with
gabapentin EMLA ropivacaine less
acute pain amp pain 6 months
Fassoulaki 2005
Current Treatment Paradigms
The Toronto General Hospital
Transitional Pain Service
development and implementation
of a multidisciplinary program
to prevent chronic postsurgical pain (Katz J Pain Res 2015)
bull Nurse navigator
bull Psychologists (ACT)
Clinical Manifestations hellipour approach to the patient with CPSP
bull Type of pain Cause
bull Exclude other causes (infection recurrence)
bull Psychological and social factors
bull Temporal Context
Electronic Patient Record
Future Directions
bull Identify Causative Modifiable risk factors vs Associative risk factors
bull Measure psychological variables
bull Genetic assays to identify genes controlling the variability in developing chronic pain
Aim is lsquoto identify susceptibility to chronic pain and sensitivity to analgesicsrsquo
Chronic pain lsquoheritabilityrsquo is variable
Conclusions
bull 1 year incidence = 05 -10 bull Avoid pain before during and after surgery lsquohelliphelliptranslate advances in acute pain to chronic settinghelliphelliprsquo bull Psychological pre-assessment bull Education discussion with patients surgeons bull In some cases preventive analgesia may be beneficial bull Transitional Pain Servicehelliptrackinghellipdatabase lsquoPragmatic approachrsquo lsquoAll diseases have an acute phasersquo lsquoDrugs good for acute pain must be good for chronic painrsquo

How big a problem is it
In a population of chronic pain patientshelliphow many had pain as a result of surgery Crombie et al Pain 1998 5000 chronic pain patients 23 = CPSP (high proportion with disability) How many people with acute pain go on to get pain at 1 year Hayes et al Acute Pain 2002 5000 patients undergoing surgery Acute neuropathic pain 2 Feature= high intensity 910 Follow up Hayes et al Acute Pain 2002 Pain at 6 months 78 Pain at 1 year 56 lsquo26 million operations year in USA (2008) 1 of all patients develop CPSPrsquo (Katz 2011)
What this study adds bull 3 of patients who had not used opioids previously continued to use them for more than 90 days after major elective surgery bullImportant public health concern because millions of patients undergo major surgery every year
Clarke et al British Medical Journal 2014
Risk factorshellip 1 Causal Modifiable Risk factors (Katz Anesth amp Analg 2011)
Acute pain
Pre-existing pain
Psychological factors
2 Correlated risk factors (Katz Anesth amp Analg 2011)
Younger age
Gender
Psychological distress
Pain
Risk factors
1 Patient related
2 Surgery related
Patient-related risk factors lsquohellippain predicts painrsquo
bull Preoperative pain (Forsythe 2008)
bull Intensity of acute pain (Masselin-Dubois 2013)
bull Acute neuropathic pain (Haroutiounian 2013)
bull High opioid consumption perioperatively (Kalso 2001)
bull Pain in other body parts (Pinto 2012)
bull Younger age (Masselin-Dubois 2013)
bull Female (Ochroch 2006)
Psychological risk factors
bull Pre-op anxiety and catastrophizing meta analysis (2x likelihood of developing CPSP (Theunissen Clin J Pain 2012)
bull Depression (Attal 2014)
bull Catastrophizing (Masselin-Dubois 2013)
bull Sensitivity to pain traumatisation (Page 2013)
bull Anxiety (Kleimann 2011)
bull Fear of long term consequences of surgery (Peters 2007)
Surgical risk factors
bull Low vs high volume surgical unit 13 increase in risk of CPSP (Tasmuth1999)
bull Duration of surgery (Kalso 2007)
bull Minimally invasive surgery (Grant 2004)
bull Stitch types (Cerfolio 2003)
bull Nerve damage preservation (Jensen 1985)
Predictive factors for chronic pain after breast surgery
Anderson et al Pain 2015 n=575
Pain at 1 year
bull Moderate- severe post op pain (50)
bull Axillary lymph node with ICB nerve preservation (30)
bull Neuropathic pain 1 week (18)
bull Age lt 65 (18)
Wang Canadian Medical Assoc Journal 2016 bull Young age bull Axillary lymph node dissection bull Acute pain High quality evidence showed no association
with BMI Type of breast surgery Chemotherapy Reconstruction
Clinical Prediction Model and Tool for Assessing Risk of Persistent Pain After Breast Cancer Surgery Tuomo J Meretoja Kenneth Geving Andersen Julie Bruce Lassi Haasio Reetta Sipilauml Neil W Scott Samuli Ripatti Henrik Kehlet and Eija Kalso
March 2017
Risk Factors ndash what can we discuss with surgeons
bull Information for patients
bull Pre-assessment pain clinic
bull Pre-op anaesthetic strategies algorithms PVB
bull Surgical technique ()
(eg mesh preservation of nerves
minimally invasive etc)
bull Enhanced recovery hellip
eg Kehlet et al Br J Surgery 2005
Fast Track Surgery
bull Pain clinic follow up
Pathophysiology lsquowhat is it about pain that causes more painrsquo
lsquohelliptransition to chronicityhelliprsquo
1 Nociceptive inflammation ischaemia oedema pressure traction
2 Neuropathic peripheral amp central sensitisation
spinal cord neuroplasticity
neuroma
3 Psychological amp social
4 Genetic
The neuropathic component in persistent pain after surgery
systematic review Haroutiunian PAIN 2013
CPSP after 11 types of surgery
bull Amount of pain depends
bull on likelihood of nerve damage
Neuropathic pain
bull in 65 of thoracotomy patients
bull 33 groin surgery
bull 6 knee surgery
Post surgical breast pain
Jung PAIN 2003
1 Intercostobrachial neuralgia
2 Other nerve injury
3 Neuroma
4 Phantom breast
Natural History
Long-term follow-up of breast cancer survivors with post-mastectomy pain syndrome
Macdonald et al British J of Cancer 2005
1996helliphellip 43 pain 3 years 2002 hellip21 pain 9 years
Persistent pain after breast surgery 6-year nationwide
follow up
Mejdahl Kehlet et al BMJ 2013
2008hellip47 pain 1 year
2013hellip37 pain 6 years
Treatment - prevention
helliphellipfrom Pre-emptive Analgesia (blocking preoperative stimuli)
helliphellipto Preventative Analgesia (blocking noxious stimuli central sensitisation across the entire perioperative period)
Preventative treatments
1 Nerve blocks Regional
2 Drugs
Regional anaesthesia to prevent chronic pain after surgery a Cochrane systematic review and meta-analysisdagger M H Andreae1 and D A Andreae2
BJA 2013
bull 23 RCTrsquos
bull Epidural anaesthesia and
paravertebral blocks may be effective
in preventing chronic pain at 1 year
bull Effective in about 1 in 4
patients treated
Preincisional Paravertebral Block Reduces the Prevalence of Chronic
Pain After Breast Surgery Kairaluoma et al Anesth Analg 2006103703-708
bull Preincisional paravertebral block provides significant immediate postoperative analgesia
bull In the same patients (n = 60) 12 months sig less pain in the PVB group
bull In addition to providing acute postoperative pain relief preoperative PVB reduces the prevalence of chronic pain 1 yr after breast cancer surgery
Epidurals Intraoperative epidural analgesia provides preventative analgesia in
abdominal surgery Lavandrsquohomme et al Anaesthesiology 2005
bull Clear benefit of epidural in preventing chronic pain 1 year
bull Intraoperative epidural better than postoperative epidural
bull Effective epidural better than effective parenteral only analgesia one year
Systematic review of therapeutic interventions to reduce chronic post surgical pain (32 RCTrsquos)
Humble et al European J of Pain (2015)
POSITIVE
Gabapentinoids
Lidocaine
iv lidocaine EMLA
Regional
TIVA
NEGATIVE
Ketamine
Cryoanalgesia
Local anaesthetic infiltration
Remifentanil (increased chronic pain)
1 Gabapentin around time of surgery
lsquono effect on chronic painrsquo
POSITIVE
NEGATIVE
Meta analysis (Clarke 2012) 48 RCTrsquos positive effect at 2 months
Cochrane Systematic Review (Chaparro 2013) 280 patients analysed pain at 6 months No effect
RCT Gabapentin 1200mg prior to Thyroidectomy Sig less pain at 3 months (Brogley 2008)
RCT Gabapentin vs Placebo Knee replacement No effect on chronic pain (Clarke 2014)
2 Pregabalin ndash around time of surgery lsquoNot a recommended treatment can cause post operative somnolencersquo
Positive
Negative
Meta-analysis of 3 studies (Clarke 2012) All showed improvement in pain 2 RCTrsquoshellipvery large decrease in CPSP (p=0007)
3 unpublished RCTrsquos from Pfizer (2010-2014) hellipall negative for acute and chronic pain i) 307 patients undergoing knee replacement ii) 501 patients hysterectomy iii) 425 patient hernia
Cochrane Systematic Review (Chaparro 2013) 25 RCTrsquos significant benefit
Systematic review (Martinez May 2017) No difference between pregabalin and placebo 3 months Use for acute pain in pro-nociceptive surgery Side effects a problem
Multimodal analgesia
bull Standard protocols now widely used eg Paravertebral blocks at MD Anderson bull Pre-assessment clinic screening for pain psychological factors pain catastrophising scale helliphellipgenetic screening tests bull Education patients surgeons anaesthetists nurses psychologists
General treatment strategies for chronic postsurgical neuropathic pain
Preventative Perkins amp Kehlet Anesthesiology 2000
bullSurgical procedure preservation
sentinel node biopsy
bullBetter postoperative pain management
bullInformed consent preparatory
information
Established Dworkin Archives Neurol 2003 60
1524
bull Amitriptyline
bull Gabapentin
bull Opioids
bull Tramadol
bull 5 Lidoderm patch EMLA
Positive therapies for Prevention of PSBP
1 EMLA applied to chest wall prior
to surgery less pain 3 months
Fassoulaki 2000
2 Venlafaxine XR 70mg before
and for 2 weeks post surgeryno diff
acute pain significantly less chronic
pain 6 months
Reuben 2004
3 Aggressive acute pain
management
Iohom 2006
4 Preincisional paravertebral
block
Kairaluoma 2006
5 Multimodal analgesia with
gabapentin EMLA ropivacaine less
acute pain amp pain 6 months
Fassoulaki 2005
A pain management programme for chronic cancer-
treatment-related pain Robb Williams Duvivier Newham
Journal of Pain 2006775-150
bull Theory of cancer-related pain
bull Pain pathways
bull Overunder activity cycle
bull Pacing
bull Exercise and fitness
bull TENS
bull Posture and manual handling
bull Relapse and prevention
Psychology interventions
bull Goal setting
bull Role of factors involved in pain
bull Homework assignments
bull Relaxation techniques
bull Cognitive skills
bull Relapse and prevention
Results
significant (plt005) improvements in
bull Pain severity
bull Psychological distress
bull Pain amp psychological coping indices
bull Activities of daily living
bull General fitness
Research Proposal
Exercise to prevent shoulder conditions in patients
undergoing breast cancer treatment
bull Aim to conduct a randomised controlled trial (RCT) supported with qualitative research to investigate the clinical and cost-effectiveness of early supervised exercise on outcomes of arm function chronic pain and quality of life at one year in women undergoing treatment for breast cancer
Intervention
bull A physiotherapy-led structured exercise programme incorporating behavioural strategies and monitoring to encourage adherence
bull A minimum of 4 face-to-face specialist treatment sessions with individual participants will be
delivered within 12 weeks of surgery bull Access to interim telephone support will be provided The programme will restrict to controlled early
stretching and ROM exercises with subsequent progression to maintain strength and function (weeks 2 to 12)
bull Qualitative interviews will be used during the feasibility phase of the trial to explore acceptability of
to the intervention
Outcomes
bull arm shoulder and hand function at 12 months using the 30-item Disability Arm Shoulder Hand (DASH) questionnaire
bull quality of life
bull Functional Assessment of Cancer Treatment-Breast (FACT-B)
bull Short-Form-12 and EQ-5D-5L
bull Data on postoperative adverse events surgical site infection and healthcare resource use will be collected at 6 and 12 months after surgery
Positive therapies for Prevention of PSBP
1 EMLA applied to chest wall prior
to surgery less pain 3 months
Fassoulaki 2000
2 Venlafaxine XR 70mg before
and for 2 weeks post surgeryno diff
acute pain significantly less chronic
pain 6 months
Reuben 2004
3 Aggressive acute pain
management
Iohom 2006
4 Preincisional paravertebral
block
Kairaluoma 2006
5 Multimodal analgesia with
gabapentin EMLA ropivacaine less
acute pain amp pain 6 months
Fassoulaki 2005
Current Treatment Paradigms
The Toronto General Hospital
Transitional Pain Service
development and implementation
of a multidisciplinary program
to prevent chronic postsurgical pain (Katz J Pain Res 2015)
bull Nurse navigator
bull Psychologists (ACT)
Clinical Manifestations hellipour approach to the patient with CPSP
bull Type of pain Cause
bull Exclude other causes (infection recurrence)
bull Psychological and social factors
bull Temporal Context
Electronic Patient Record
Future Directions
bull Identify Causative Modifiable risk factors vs Associative risk factors
bull Measure psychological variables
bull Genetic assays to identify genes controlling the variability in developing chronic pain
Aim is lsquoto identify susceptibility to chronic pain and sensitivity to analgesicsrsquo
Chronic pain lsquoheritabilityrsquo is variable
Conclusions
bull 1 year incidence = 05 -10 bull Avoid pain before during and after surgery lsquohelliphelliptranslate advances in acute pain to chronic settinghelliphelliprsquo bull Psychological pre-assessment bull Education discussion with patients surgeons bull In some cases preventive analgesia may be beneficial bull Transitional Pain Servicehelliptrackinghellipdatabase lsquoPragmatic approachrsquo lsquoAll diseases have an acute phasersquo lsquoDrugs good for acute pain must be good for chronic painrsquo

What this study adds bull 3 of patients who had not used opioids previously continued to use them for more than 90 days after major elective surgery bullImportant public health concern because millions of patients undergo major surgery every year
Clarke et al British Medical Journal 2014
Risk factorshellip 1 Causal Modifiable Risk factors (Katz Anesth amp Analg 2011)
Acute pain
Pre-existing pain
Psychological factors
2 Correlated risk factors (Katz Anesth amp Analg 2011)
Younger age
Gender
Psychological distress
Pain
Risk factors
1 Patient related
2 Surgery related
Patient-related risk factors lsquohellippain predicts painrsquo
bull Preoperative pain (Forsythe 2008)
bull Intensity of acute pain (Masselin-Dubois 2013)
bull Acute neuropathic pain (Haroutiounian 2013)
bull High opioid consumption perioperatively (Kalso 2001)
bull Pain in other body parts (Pinto 2012)
bull Younger age (Masselin-Dubois 2013)
bull Female (Ochroch 2006)
Psychological risk factors
bull Pre-op anxiety and catastrophizing meta analysis (2x likelihood of developing CPSP (Theunissen Clin J Pain 2012)
bull Depression (Attal 2014)
bull Catastrophizing (Masselin-Dubois 2013)
bull Sensitivity to pain traumatisation (Page 2013)
bull Anxiety (Kleimann 2011)
bull Fear of long term consequences of surgery (Peters 2007)
Surgical risk factors
bull Low vs high volume surgical unit 13 increase in risk of CPSP (Tasmuth1999)
bull Duration of surgery (Kalso 2007)
bull Minimally invasive surgery (Grant 2004)
bull Stitch types (Cerfolio 2003)
bull Nerve damage preservation (Jensen 1985)
Predictive factors for chronic pain after breast surgery
Anderson et al Pain 2015 n=575
Pain at 1 year
bull Moderate- severe post op pain (50)
bull Axillary lymph node with ICB nerve preservation (30)
bull Neuropathic pain 1 week (18)
bull Age lt 65 (18)
Wang Canadian Medical Assoc Journal 2016 bull Young age bull Axillary lymph node dissection bull Acute pain High quality evidence showed no association
with BMI Type of breast surgery Chemotherapy Reconstruction
Clinical Prediction Model and Tool for Assessing Risk of Persistent Pain After Breast Cancer Surgery Tuomo J Meretoja Kenneth Geving Andersen Julie Bruce Lassi Haasio Reetta Sipilauml Neil W Scott Samuli Ripatti Henrik Kehlet and Eija Kalso
March 2017
Risk Factors ndash what can we discuss with surgeons
bull Information for patients
bull Pre-assessment pain clinic
bull Pre-op anaesthetic strategies algorithms PVB
bull Surgical technique ()
(eg mesh preservation of nerves
minimally invasive etc)
bull Enhanced recovery hellip
eg Kehlet et al Br J Surgery 2005
Fast Track Surgery
bull Pain clinic follow up
Pathophysiology lsquowhat is it about pain that causes more painrsquo
lsquohelliptransition to chronicityhelliprsquo
1 Nociceptive inflammation ischaemia oedema pressure traction
2 Neuropathic peripheral amp central sensitisation
spinal cord neuroplasticity
neuroma
3 Psychological amp social
4 Genetic
The neuropathic component in persistent pain after surgery
systematic review Haroutiunian PAIN 2013
CPSP after 11 types of surgery
bull Amount of pain depends
bull on likelihood of nerve damage
Neuropathic pain
bull in 65 of thoracotomy patients
bull 33 groin surgery
bull 6 knee surgery
Post surgical breast pain
Jung PAIN 2003
1 Intercostobrachial neuralgia
2 Other nerve injury
3 Neuroma
4 Phantom breast
Natural History
Long-term follow-up of breast cancer survivors with post-mastectomy pain syndrome
Macdonald et al British J of Cancer 2005
1996helliphellip 43 pain 3 years 2002 hellip21 pain 9 years
Persistent pain after breast surgery 6-year nationwide
follow up
Mejdahl Kehlet et al BMJ 2013
2008hellip47 pain 1 year
2013hellip37 pain 6 years
Treatment - prevention
helliphellipfrom Pre-emptive Analgesia (blocking preoperative stimuli)
helliphellipto Preventative Analgesia (blocking noxious stimuli central sensitisation across the entire perioperative period)
Preventative treatments
1 Nerve blocks Regional
2 Drugs
Regional anaesthesia to prevent chronic pain after surgery a Cochrane systematic review and meta-analysisdagger M H Andreae1 and D A Andreae2
BJA 2013
bull 23 RCTrsquos
bull Epidural anaesthesia and
paravertebral blocks may be effective
in preventing chronic pain at 1 year
bull Effective in about 1 in 4
patients treated
Preincisional Paravertebral Block Reduces the Prevalence of Chronic
Pain After Breast Surgery Kairaluoma et al Anesth Analg 2006103703-708
bull Preincisional paravertebral block provides significant immediate postoperative analgesia
bull In the same patients (n = 60) 12 months sig less pain in the PVB group
bull In addition to providing acute postoperative pain relief preoperative PVB reduces the prevalence of chronic pain 1 yr after breast cancer surgery
Epidurals Intraoperative epidural analgesia provides preventative analgesia in
abdominal surgery Lavandrsquohomme et al Anaesthesiology 2005
bull Clear benefit of epidural in preventing chronic pain 1 year
bull Intraoperative epidural better than postoperative epidural
bull Effective epidural better than effective parenteral only analgesia one year
Systematic review of therapeutic interventions to reduce chronic post surgical pain (32 RCTrsquos)
Humble et al European J of Pain (2015)
POSITIVE
Gabapentinoids
Lidocaine
iv lidocaine EMLA
Regional
TIVA
NEGATIVE
Ketamine
Cryoanalgesia
Local anaesthetic infiltration
Remifentanil (increased chronic pain)
1 Gabapentin around time of surgery
lsquono effect on chronic painrsquo
POSITIVE
NEGATIVE
Meta analysis (Clarke 2012) 48 RCTrsquos positive effect at 2 months
Cochrane Systematic Review (Chaparro 2013) 280 patients analysed pain at 6 months No effect
RCT Gabapentin 1200mg prior to Thyroidectomy Sig less pain at 3 months (Brogley 2008)
RCT Gabapentin vs Placebo Knee replacement No effect on chronic pain (Clarke 2014)
2 Pregabalin ndash around time of surgery lsquoNot a recommended treatment can cause post operative somnolencersquo
Positive
Negative
Meta-analysis of 3 studies (Clarke 2012) All showed improvement in pain 2 RCTrsquoshellipvery large decrease in CPSP (p=0007)
3 unpublished RCTrsquos from Pfizer (2010-2014) hellipall negative for acute and chronic pain i) 307 patients undergoing knee replacement ii) 501 patients hysterectomy iii) 425 patient hernia
Cochrane Systematic Review (Chaparro 2013) 25 RCTrsquos significant benefit
Systematic review (Martinez May 2017) No difference between pregabalin and placebo 3 months Use for acute pain in pro-nociceptive surgery Side effects a problem
Multimodal analgesia
bull Standard protocols now widely used eg Paravertebral blocks at MD Anderson bull Pre-assessment clinic screening for pain psychological factors pain catastrophising scale helliphellipgenetic screening tests bull Education patients surgeons anaesthetists nurses psychologists
General treatment strategies for chronic postsurgical neuropathic pain
Preventative Perkins amp Kehlet Anesthesiology 2000
bullSurgical procedure preservation
sentinel node biopsy
bullBetter postoperative pain management
bullInformed consent preparatory
information
Established Dworkin Archives Neurol 2003 60
1524
bull Amitriptyline
bull Gabapentin
bull Opioids
bull Tramadol
bull 5 Lidoderm patch EMLA
Positive therapies for Prevention of PSBP
1 EMLA applied to chest wall prior
to surgery less pain 3 months
Fassoulaki 2000
2 Venlafaxine XR 70mg before
and for 2 weeks post surgeryno diff
acute pain significantly less chronic
pain 6 months
Reuben 2004
3 Aggressive acute pain
management
Iohom 2006
4 Preincisional paravertebral
block
Kairaluoma 2006
5 Multimodal analgesia with
gabapentin EMLA ropivacaine less
acute pain amp pain 6 months
Fassoulaki 2005
A pain management programme for chronic cancer-
treatment-related pain Robb Williams Duvivier Newham
Journal of Pain 2006775-150
bull Theory of cancer-related pain
bull Pain pathways
bull Overunder activity cycle
bull Pacing
bull Exercise and fitness
bull TENS
bull Posture and manual handling
bull Relapse and prevention
Psychology interventions
bull Goal setting
bull Role of factors involved in pain
bull Homework assignments
bull Relaxation techniques
bull Cognitive skills
bull Relapse and prevention
Results
significant (plt005) improvements in
bull Pain severity
bull Psychological distress
bull Pain amp psychological coping indices
bull Activities of daily living
bull General fitness
Research Proposal
Exercise to prevent shoulder conditions in patients
undergoing breast cancer treatment
bull Aim to conduct a randomised controlled trial (RCT) supported with qualitative research to investigate the clinical and cost-effectiveness of early supervised exercise on outcomes of arm function chronic pain and quality of life at one year in women undergoing treatment for breast cancer
Intervention
bull A physiotherapy-led structured exercise programme incorporating behavioural strategies and monitoring to encourage adherence
bull A minimum of 4 face-to-face specialist treatment sessions with individual participants will be
delivered within 12 weeks of surgery bull Access to interim telephone support will be provided The programme will restrict to controlled early
stretching and ROM exercises with subsequent progression to maintain strength and function (weeks 2 to 12)
bull Qualitative interviews will be used during the feasibility phase of the trial to explore acceptability of
to the intervention
Outcomes
bull arm shoulder and hand function at 12 months using the 30-item Disability Arm Shoulder Hand (DASH) questionnaire
bull quality of life
bull Functional Assessment of Cancer Treatment-Breast (FACT-B)
bull Short-Form-12 and EQ-5D-5L
bull Data on postoperative adverse events surgical site infection and healthcare resource use will be collected at 6 and 12 months after surgery
Positive therapies for Prevention of PSBP
1 EMLA applied to chest wall prior
to surgery less pain 3 months
Fassoulaki 2000
2 Venlafaxine XR 70mg before
and for 2 weeks post surgeryno diff
acute pain significantly less chronic
pain 6 months
Reuben 2004
3 Aggressive acute pain
management
Iohom 2006
4 Preincisional paravertebral
block
Kairaluoma 2006
5 Multimodal analgesia with
gabapentin EMLA ropivacaine less
acute pain amp pain 6 months
Fassoulaki 2005
Current Treatment Paradigms
The Toronto General Hospital
Transitional Pain Service
development and implementation
of a multidisciplinary program
to prevent chronic postsurgical pain (Katz J Pain Res 2015)
bull Nurse navigator
bull Psychologists (ACT)
Clinical Manifestations hellipour approach to the patient with CPSP
bull Type of pain Cause
bull Exclude other causes (infection recurrence)
bull Psychological and social factors
bull Temporal Context
Electronic Patient Record
Future Directions
bull Identify Causative Modifiable risk factors vs Associative risk factors
bull Measure psychological variables
bull Genetic assays to identify genes controlling the variability in developing chronic pain
Aim is lsquoto identify susceptibility to chronic pain and sensitivity to analgesicsrsquo
Chronic pain lsquoheritabilityrsquo is variable
Conclusions
bull 1 year incidence = 05 -10 bull Avoid pain before during and after surgery lsquohelliphelliptranslate advances in acute pain to chronic settinghelliphelliprsquo bull Psychological pre-assessment bull Education discussion with patients surgeons bull In some cases preventive analgesia may be beneficial bull Transitional Pain Servicehelliptrackinghellipdatabase lsquoPragmatic approachrsquo lsquoAll diseases have an acute phasersquo lsquoDrugs good for acute pain must be good for chronic painrsquo

Risk factorshellip 1 Causal Modifiable Risk factors (Katz Anesth amp Analg 2011)
Acute pain
Pre-existing pain
Psychological factors
2 Correlated risk factors (Katz Anesth amp Analg 2011)
Younger age
Gender
Psychological distress
Pain
Risk factors
1 Patient related
2 Surgery related
Patient-related risk factors lsquohellippain predicts painrsquo
bull Preoperative pain (Forsythe 2008)
bull Intensity of acute pain (Masselin-Dubois 2013)
bull Acute neuropathic pain (Haroutiounian 2013)
bull High opioid consumption perioperatively (Kalso 2001)
bull Pain in other body parts (Pinto 2012)
bull Younger age (Masselin-Dubois 2013)
bull Female (Ochroch 2006)
Psychological risk factors
bull Pre-op anxiety and catastrophizing meta analysis (2x likelihood of developing CPSP (Theunissen Clin J Pain 2012)
bull Depression (Attal 2014)
bull Catastrophizing (Masselin-Dubois 2013)
bull Sensitivity to pain traumatisation (Page 2013)
bull Anxiety (Kleimann 2011)
bull Fear of long term consequences of surgery (Peters 2007)
Surgical risk factors
bull Low vs high volume surgical unit 13 increase in risk of CPSP (Tasmuth1999)
bull Duration of surgery (Kalso 2007)
bull Minimally invasive surgery (Grant 2004)
bull Stitch types (Cerfolio 2003)
bull Nerve damage preservation (Jensen 1985)
Predictive factors for chronic pain after breast surgery
Anderson et al Pain 2015 n=575
Pain at 1 year
bull Moderate- severe post op pain (50)
bull Axillary lymph node with ICB nerve preservation (30)
bull Neuropathic pain 1 week (18)
bull Age lt 65 (18)
Wang Canadian Medical Assoc Journal 2016 bull Young age bull Axillary lymph node dissection bull Acute pain High quality evidence showed no association
with BMI Type of breast surgery Chemotherapy Reconstruction
Clinical Prediction Model and Tool for Assessing Risk of Persistent Pain After Breast Cancer Surgery Tuomo J Meretoja Kenneth Geving Andersen Julie Bruce Lassi Haasio Reetta Sipilauml Neil W Scott Samuli Ripatti Henrik Kehlet and Eija Kalso
March 2017
Risk Factors ndash what can we discuss with surgeons
bull Information for patients
bull Pre-assessment pain clinic
bull Pre-op anaesthetic strategies algorithms PVB
bull Surgical technique ()
(eg mesh preservation of nerves
minimally invasive etc)
bull Enhanced recovery hellip
eg Kehlet et al Br J Surgery 2005
Fast Track Surgery
bull Pain clinic follow up
Pathophysiology lsquowhat is it about pain that causes more painrsquo
lsquohelliptransition to chronicityhelliprsquo
1 Nociceptive inflammation ischaemia oedema pressure traction
2 Neuropathic peripheral amp central sensitisation
spinal cord neuroplasticity
neuroma
3 Psychological amp social
4 Genetic
The neuropathic component in persistent pain after surgery
systematic review Haroutiunian PAIN 2013
CPSP after 11 types of surgery
bull Amount of pain depends
bull on likelihood of nerve damage
Neuropathic pain
bull in 65 of thoracotomy patients
bull 33 groin surgery
bull 6 knee surgery
Post surgical breast pain
Jung PAIN 2003
1 Intercostobrachial neuralgia
2 Other nerve injury
3 Neuroma
4 Phantom breast
Natural History
Long-term follow-up of breast cancer survivors with post-mastectomy pain syndrome
Macdonald et al British J of Cancer 2005
1996helliphellip 43 pain 3 years 2002 hellip21 pain 9 years
Persistent pain after breast surgery 6-year nationwide
follow up
Mejdahl Kehlet et al BMJ 2013
2008hellip47 pain 1 year
2013hellip37 pain 6 years
Treatment - prevention
helliphellipfrom Pre-emptive Analgesia (blocking preoperative stimuli)
helliphellipto Preventative Analgesia (blocking noxious stimuli central sensitisation across the entire perioperative period)
Preventative treatments
1 Nerve blocks Regional
2 Drugs
Regional anaesthesia to prevent chronic pain after surgery a Cochrane systematic review and meta-analysisdagger M H Andreae1 and D A Andreae2
BJA 2013
bull 23 RCTrsquos
bull Epidural anaesthesia and
paravertebral blocks may be effective
in preventing chronic pain at 1 year
bull Effective in about 1 in 4
patients treated
Preincisional Paravertebral Block Reduces the Prevalence of Chronic
Pain After Breast Surgery Kairaluoma et al Anesth Analg 2006103703-708
bull Preincisional paravertebral block provides significant immediate postoperative analgesia
bull In the same patients (n = 60) 12 months sig less pain in the PVB group
bull In addition to providing acute postoperative pain relief preoperative PVB reduces the prevalence of chronic pain 1 yr after breast cancer surgery
Epidurals Intraoperative epidural analgesia provides preventative analgesia in
abdominal surgery Lavandrsquohomme et al Anaesthesiology 2005
bull Clear benefit of epidural in preventing chronic pain 1 year
bull Intraoperative epidural better than postoperative epidural
bull Effective epidural better than effective parenteral only analgesia one year
Systematic review of therapeutic interventions to reduce chronic post surgical pain (32 RCTrsquos)
Humble et al European J of Pain (2015)
POSITIVE
Gabapentinoids
Lidocaine
iv lidocaine EMLA
Regional
TIVA
NEGATIVE
Ketamine
Cryoanalgesia
Local anaesthetic infiltration
Remifentanil (increased chronic pain)
1 Gabapentin around time of surgery
lsquono effect on chronic painrsquo
POSITIVE
NEGATIVE
Meta analysis (Clarke 2012) 48 RCTrsquos positive effect at 2 months
Cochrane Systematic Review (Chaparro 2013) 280 patients analysed pain at 6 months No effect
RCT Gabapentin 1200mg prior to Thyroidectomy Sig less pain at 3 months (Brogley 2008)
RCT Gabapentin vs Placebo Knee replacement No effect on chronic pain (Clarke 2014)
2 Pregabalin ndash around time of surgery lsquoNot a recommended treatment can cause post operative somnolencersquo
Positive
Negative
Meta-analysis of 3 studies (Clarke 2012) All showed improvement in pain 2 RCTrsquoshellipvery large decrease in CPSP (p=0007)
3 unpublished RCTrsquos from Pfizer (2010-2014) hellipall negative for acute and chronic pain i) 307 patients undergoing knee replacement ii) 501 patients hysterectomy iii) 425 patient hernia
Cochrane Systematic Review (Chaparro 2013) 25 RCTrsquos significant benefit
Systematic review (Martinez May 2017) No difference between pregabalin and placebo 3 months Use for acute pain in pro-nociceptive surgery Side effects a problem
Multimodal analgesia
bull Standard protocols now widely used eg Paravertebral blocks at MD Anderson bull Pre-assessment clinic screening for pain psychological factors pain catastrophising scale helliphellipgenetic screening tests bull Education patients surgeons anaesthetists nurses psychologists
General treatment strategies for chronic postsurgical neuropathic pain
Preventative Perkins amp Kehlet Anesthesiology 2000
bullSurgical procedure preservation
sentinel node biopsy
bullBetter postoperative pain management
bullInformed consent preparatory
information
Established Dworkin Archives Neurol 2003 60
1524
bull Amitriptyline
bull Gabapentin
bull Opioids
bull Tramadol
bull 5 Lidoderm patch EMLA
Positive therapies for Prevention of PSBP
1 EMLA applied to chest wall prior
to surgery less pain 3 months
Fassoulaki 2000
2 Venlafaxine XR 70mg before
and for 2 weeks post surgeryno diff
acute pain significantly less chronic
pain 6 months
Reuben 2004
3 Aggressive acute pain
management
Iohom 2006
4 Preincisional paravertebral
block
Kairaluoma 2006
5 Multimodal analgesia with
gabapentin EMLA ropivacaine less
acute pain amp pain 6 months
Fassoulaki 2005
A pain management programme for chronic cancer-
treatment-related pain Robb Williams Duvivier Newham
Journal of Pain 2006775-150
bull Theory of cancer-related pain
bull Pain pathways
bull Overunder activity cycle
bull Pacing
bull Exercise and fitness
bull TENS
bull Posture and manual handling
bull Relapse and prevention
Psychology interventions
bull Goal setting
bull Role of factors involved in pain
bull Homework assignments
bull Relaxation techniques
bull Cognitive skills
bull Relapse and prevention
Results
significant (plt005) improvements in
bull Pain severity
bull Psychological distress
bull Pain amp psychological coping indices
bull Activities of daily living
bull General fitness
Research Proposal
Exercise to prevent shoulder conditions in patients
undergoing breast cancer treatment
bull Aim to conduct a randomised controlled trial (RCT) supported with qualitative research to investigate the clinical and cost-effectiveness of early supervised exercise on outcomes of arm function chronic pain and quality of life at one year in women undergoing treatment for breast cancer
Intervention
bull A physiotherapy-led structured exercise programme incorporating behavioural strategies and monitoring to encourage adherence
bull A minimum of 4 face-to-face specialist treatment sessions with individual participants will be
delivered within 12 weeks of surgery bull Access to interim telephone support will be provided The programme will restrict to controlled early
stretching and ROM exercises with subsequent progression to maintain strength and function (weeks 2 to 12)
bull Qualitative interviews will be used during the feasibility phase of the trial to explore acceptability of
to the intervention
Outcomes
bull arm shoulder and hand function at 12 months using the 30-item Disability Arm Shoulder Hand (DASH) questionnaire
bull quality of life
bull Functional Assessment of Cancer Treatment-Breast (FACT-B)
bull Short-Form-12 and EQ-5D-5L
bull Data on postoperative adverse events surgical site infection and healthcare resource use will be collected at 6 and 12 months after surgery
Positive therapies for Prevention of PSBP
1 EMLA applied to chest wall prior
to surgery less pain 3 months
Fassoulaki 2000
2 Venlafaxine XR 70mg before
and for 2 weeks post surgeryno diff
acute pain significantly less chronic
pain 6 months
Reuben 2004
3 Aggressive acute pain
management
Iohom 2006
4 Preincisional paravertebral
block
Kairaluoma 2006
5 Multimodal analgesia with
gabapentin EMLA ropivacaine less
acute pain amp pain 6 months
Fassoulaki 2005
Current Treatment Paradigms
The Toronto General Hospital
Transitional Pain Service
development and implementation
of a multidisciplinary program
to prevent chronic postsurgical pain (Katz J Pain Res 2015)
bull Nurse navigator
bull Psychologists (ACT)
Clinical Manifestations hellipour approach to the patient with CPSP
bull Type of pain Cause
bull Exclude other causes (infection recurrence)
bull Psychological and social factors
bull Temporal Context
Electronic Patient Record
Future Directions
bull Identify Causative Modifiable risk factors vs Associative risk factors
bull Measure psychological variables
bull Genetic assays to identify genes controlling the variability in developing chronic pain
Aim is lsquoto identify susceptibility to chronic pain and sensitivity to analgesicsrsquo
Chronic pain lsquoheritabilityrsquo is variable
Conclusions
bull 1 year incidence = 05 -10 bull Avoid pain before during and after surgery lsquohelliphelliptranslate advances in acute pain to chronic settinghelliphelliprsquo bull Psychological pre-assessment bull Education discussion with patients surgeons bull In some cases preventive analgesia may be beneficial bull Transitional Pain Servicehelliptrackinghellipdatabase lsquoPragmatic approachrsquo lsquoAll diseases have an acute phasersquo lsquoDrugs good for acute pain must be good for chronic painrsquo

2 Correlated risk factors (Katz Anesth amp Analg 2011)
Younger age
Gender
Psychological distress
Pain
Risk factors
1 Patient related
2 Surgery related
Patient-related risk factors lsquohellippain predicts painrsquo
bull Preoperative pain (Forsythe 2008)
bull Intensity of acute pain (Masselin-Dubois 2013)
bull Acute neuropathic pain (Haroutiounian 2013)
bull High opioid consumption perioperatively (Kalso 2001)
bull Pain in other body parts (Pinto 2012)
bull Younger age (Masselin-Dubois 2013)
bull Female (Ochroch 2006)
Psychological risk factors
bull Pre-op anxiety and catastrophizing meta analysis (2x likelihood of developing CPSP (Theunissen Clin J Pain 2012)
bull Depression (Attal 2014)
bull Catastrophizing (Masselin-Dubois 2013)
bull Sensitivity to pain traumatisation (Page 2013)
bull Anxiety (Kleimann 2011)
bull Fear of long term consequences of surgery (Peters 2007)
Surgical risk factors
bull Low vs high volume surgical unit 13 increase in risk of CPSP (Tasmuth1999)
bull Duration of surgery (Kalso 2007)
bull Minimally invasive surgery (Grant 2004)
bull Stitch types (Cerfolio 2003)
bull Nerve damage preservation (Jensen 1985)
Predictive factors for chronic pain after breast surgery
Anderson et al Pain 2015 n=575
Pain at 1 year
bull Moderate- severe post op pain (50)
bull Axillary lymph node with ICB nerve preservation (30)
bull Neuropathic pain 1 week (18)
bull Age lt 65 (18)
Wang Canadian Medical Assoc Journal 2016 bull Young age bull Axillary lymph node dissection bull Acute pain High quality evidence showed no association
with BMI Type of breast surgery Chemotherapy Reconstruction
Clinical Prediction Model and Tool for Assessing Risk of Persistent Pain After Breast Cancer Surgery Tuomo J Meretoja Kenneth Geving Andersen Julie Bruce Lassi Haasio Reetta Sipilauml Neil W Scott Samuli Ripatti Henrik Kehlet and Eija Kalso
March 2017
Risk Factors ndash what can we discuss with surgeons
bull Information for patients
bull Pre-assessment pain clinic
bull Pre-op anaesthetic strategies algorithms PVB
bull Surgical technique ()
(eg mesh preservation of nerves
minimally invasive etc)
bull Enhanced recovery hellip
eg Kehlet et al Br J Surgery 2005
Fast Track Surgery
bull Pain clinic follow up
Pathophysiology lsquowhat is it about pain that causes more painrsquo
lsquohelliptransition to chronicityhelliprsquo
1 Nociceptive inflammation ischaemia oedema pressure traction
2 Neuropathic peripheral amp central sensitisation
spinal cord neuroplasticity
neuroma
3 Psychological amp social
4 Genetic
The neuropathic component in persistent pain after surgery
systematic review Haroutiunian PAIN 2013
CPSP after 11 types of surgery
bull Amount of pain depends
bull on likelihood of nerve damage
Neuropathic pain
bull in 65 of thoracotomy patients
bull 33 groin surgery
bull 6 knee surgery
Post surgical breast pain
Jung PAIN 2003
1 Intercostobrachial neuralgia
2 Other nerve injury
3 Neuroma
4 Phantom breast
Natural History
Long-term follow-up of breast cancer survivors with post-mastectomy pain syndrome
Macdonald et al British J of Cancer 2005
1996helliphellip 43 pain 3 years 2002 hellip21 pain 9 years
Persistent pain after breast surgery 6-year nationwide
follow up
Mejdahl Kehlet et al BMJ 2013
2008hellip47 pain 1 year
2013hellip37 pain 6 years
Treatment - prevention
helliphellipfrom Pre-emptive Analgesia (blocking preoperative stimuli)
helliphellipto Preventative Analgesia (blocking noxious stimuli central sensitisation across the entire perioperative period)
Preventative treatments
1 Nerve blocks Regional
2 Drugs
Regional anaesthesia to prevent chronic pain after surgery a Cochrane systematic review and meta-analysisdagger M H Andreae1 and D A Andreae2
BJA 2013
bull 23 RCTrsquos
bull Epidural anaesthesia and
paravertebral blocks may be effective
in preventing chronic pain at 1 year
bull Effective in about 1 in 4
patients treated
Preincisional Paravertebral Block Reduces the Prevalence of Chronic
Pain After Breast Surgery Kairaluoma et al Anesth Analg 2006103703-708
bull Preincisional paravertebral block provides significant immediate postoperative analgesia
bull In the same patients (n = 60) 12 months sig less pain in the PVB group
bull In addition to providing acute postoperative pain relief preoperative PVB reduces the prevalence of chronic pain 1 yr after breast cancer surgery
Epidurals Intraoperative epidural analgesia provides preventative analgesia in
abdominal surgery Lavandrsquohomme et al Anaesthesiology 2005
bull Clear benefit of epidural in preventing chronic pain 1 year
bull Intraoperative epidural better than postoperative epidural
bull Effective epidural better than effective parenteral only analgesia one year
Systematic review of therapeutic interventions to reduce chronic post surgical pain (32 RCTrsquos)
Humble et al European J of Pain (2015)
POSITIVE
Gabapentinoids
Lidocaine
iv lidocaine EMLA
Regional
TIVA
NEGATIVE
Ketamine
Cryoanalgesia
Local anaesthetic infiltration
Remifentanil (increased chronic pain)
1 Gabapentin around time of surgery
lsquono effect on chronic painrsquo
POSITIVE
NEGATIVE
Meta analysis (Clarke 2012) 48 RCTrsquos positive effect at 2 months
Cochrane Systematic Review (Chaparro 2013) 280 patients analysed pain at 6 months No effect
RCT Gabapentin 1200mg prior to Thyroidectomy Sig less pain at 3 months (Brogley 2008)
RCT Gabapentin vs Placebo Knee replacement No effect on chronic pain (Clarke 2014)
2 Pregabalin ndash around time of surgery lsquoNot a recommended treatment can cause post operative somnolencersquo
Positive
Negative
Meta-analysis of 3 studies (Clarke 2012) All showed improvement in pain 2 RCTrsquoshellipvery large decrease in CPSP (p=0007)
3 unpublished RCTrsquos from Pfizer (2010-2014) hellipall negative for acute and chronic pain i) 307 patients undergoing knee replacement ii) 501 patients hysterectomy iii) 425 patient hernia
Cochrane Systematic Review (Chaparro 2013) 25 RCTrsquos significant benefit
Systematic review (Martinez May 2017) No difference between pregabalin and placebo 3 months Use for acute pain in pro-nociceptive surgery Side effects a problem
Multimodal analgesia
bull Standard protocols now widely used eg Paravertebral blocks at MD Anderson bull Pre-assessment clinic screening for pain psychological factors pain catastrophising scale helliphellipgenetic screening tests bull Education patients surgeons anaesthetists nurses psychologists
General treatment strategies for chronic postsurgical neuropathic pain
Preventative Perkins amp Kehlet Anesthesiology 2000
bullSurgical procedure preservation
sentinel node biopsy
bullBetter postoperative pain management
bullInformed consent preparatory
information
Established Dworkin Archives Neurol 2003 60
1524
bull Amitriptyline
bull Gabapentin
bull Opioids
bull Tramadol
bull 5 Lidoderm patch EMLA
Positive therapies for Prevention of PSBP
1 EMLA applied to chest wall prior
to surgery less pain 3 months
Fassoulaki 2000
2 Venlafaxine XR 70mg before
and for 2 weeks post surgeryno diff
acute pain significantly less chronic
pain 6 months
Reuben 2004
3 Aggressive acute pain
management
Iohom 2006
4 Preincisional paravertebral
block
Kairaluoma 2006
5 Multimodal analgesia with
gabapentin EMLA ropivacaine less
acute pain amp pain 6 months
Fassoulaki 2005
A pain management programme for chronic cancer-
treatment-related pain Robb Williams Duvivier Newham
Journal of Pain 2006775-150
bull Theory of cancer-related pain
bull Pain pathways
bull Overunder activity cycle
bull Pacing
bull Exercise and fitness
bull TENS
bull Posture and manual handling
bull Relapse and prevention
Psychology interventions
bull Goal setting
bull Role of factors involved in pain
bull Homework assignments
bull Relaxation techniques
bull Cognitive skills
bull Relapse and prevention
Results
significant (plt005) improvements in
bull Pain severity
bull Psychological distress
bull Pain amp psychological coping indices
bull Activities of daily living
bull General fitness
Research Proposal
Exercise to prevent shoulder conditions in patients
undergoing breast cancer treatment
bull Aim to conduct a randomised controlled trial (RCT) supported with qualitative research to investigate the clinical and cost-effectiveness of early supervised exercise on outcomes of arm function chronic pain and quality of life at one year in women undergoing treatment for breast cancer
Intervention
bull A physiotherapy-led structured exercise programme incorporating behavioural strategies and monitoring to encourage adherence
bull A minimum of 4 face-to-face specialist treatment sessions with individual participants will be
delivered within 12 weeks of surgery bull Access to interim telephone support will be provided The programme will restrict to controlled early
stretching and ROM exercises with subsequent progression to maintain strength and function (weeks 2 to 12)
bull Qualitative interviews will be used during the feasibility phase of the trial to explore acceptability of
to the intervention
Outcomes
bull arm shoulder and hand function at 12 months using the 30-item Disability Arm Shoulder Hand (DASH) questionnaire
bull quality of life
bull Functional Assessment of Cancer Treatment-Breast (FACT-B)
bull Short-Form-12 and EQ-5D-5L
bull Data on postoperative adverse events surgical site infection and healthcare resource use will be collected at 6 and 12 months after surgery
Positive therapies for Prevention of PSBP
1 EMLA applied to chest wall prior
to surgery less pain 3 months
Fassoulaki 2000
2 Venlafaxine XR 70mg before
and for 2 weeks post surgeryno diff
acute pain significantly less chronic
pain 6 months
Reuben 2004
3 Aggressive acute pain
management
Iohom 2006
4 Preincisional paravertebral
block
Kairaluoma 2006
5 Multimodal analgesia with
gabapentin EMLA ropivacaine less
acute pain amp pain 6 months
Fassoulaki 2005
Current Treatment Paradigms
The Toronto General Hospital
Transitional Pain Service
development and implementation
of a multidisciplinary program
to prevent chronic postsurgical pain (Katz J Pain Res 2015)
bull Nurse navigator
bull Psychologists (ACT)
Clinical Manifestations hellipour approach to the patient with CPSP
bull Type of pain Cause
bull Exclude other causes (infection recurrence)
bull Psychological and social factors
bull Temporal Context
Electronic Patient Record
Future Directions
bull Identify Causative Modifiable risk factors vs Associative risk factors
bull Measure psychological variables
bull Genetic assays to identify genes controlling the variability in developing chronic pain
Aim is lsquoto identify susceptibility to chronic pain and sensitivity to analgesicsrsquo
Chronic pain lsquoheritabilityrsquo is variable
Conclusions
bull 1 year incidence = 05 -10 bull Avoid pain before during and after surgery lsquohelliphelliptranslate advances in acute pain to chronic settinghelliphelliprsquo bull Psychological pre-assessment bull Education discussion with patients surgeons bull In some cases preventive analgesia may be beneficial bull Transitional Pain Servicehelliptrackinghellipdatabase lsquoPragmatic approachrsquo lsquoAll diseases have an acute phasersquo lsquoDrugs good for acute pain must be good for chronic painrsquo

Risk factors
1 Patient related
2 Surgery related
Patient-related risk factors lsquohellippain predicts painrsquo
bull Preoperative pain (Forsythe 2008)
bull Intensity of acute pain (Masselin-Dubois 2013)
bull Acute neuropathic pain (Haroutiounian 2013)
bull High opioid consumption perioperatively (Kalso 2001)
bull Pain in other body parts (Pinto 2012)
bull Younger age (Masselin-Dubois 2013)
bull Female (Ochroch 2006)
Psychological risk factors
bull Pre-op anxiety and catastrophizing meta analysis (2x likelihood of developing CPSP (Theunissen Clin J Pain 2012)
bull Depression (Attal 2014)
bull Catastrophizing (Masselin-Dubois 2013)
bull Sensitivity to pain traumatisation (Page 2013)
bull Anxiety (Kleimann 2011)
bull Fear of long term consequences of surgery (Peters 2007)
Surgical risk factors
bull Low vs high volume surgical unit 13 increase in risk of CPSP (Tasmuth1999)
bull Duration of surgery (Kalso 2007)
bull Minimally invasive surgery (Grant 2004)
bull Stitch types (Cerfolio 2003)
bull Nerve damage preservation (Jensen 1985)
Predictive factors for chronic pain after breast surgery
Anderson et al Pain 2015 n=575
Pain at 1 year
bull Moderate- severe post op pain (50)
bull Axillary lymph node with ICB nerve preservation (30)
bull Neuropathic pain 1 week (18)
bull Age lt 65 (18)
Wang Canadian Medical Assoc Journal 2016 bull Young age bull Axillary lymph node dissection bull Acute pain High quality evidence showed no association
with BMI Type of breast surgery Chemotherapy Reconstruction
Clinical Prediction Model and Tool for Assessing Risk of Persistent Pain After Breast Cancer Surgery Tuomo J Meretoja Kenneth Geving Andersen Julie Bruce Lassi Haasio Reetta Sipilauml Neil W Scott Samuli Ripatti Henrik Kehlet and Eija Kalso
March 2017
Risk Factors ndash what can we discuss with surgeons
bull Information for patients
bull Pre-assessment pain clinic
bull Pre-op anaesthetic strategies algorithms PVB
bull Surgical technique ()
(eg mesh preservation of nerves
minimally invasive etc)
bull Enhanced recovery hellip
eg Kehlet et al Br J Surgery 2005
Fast Track Surgery
bull Pain clinic follow up
Pathophysiology lsquowhat is it about pain that causes more painrsquo
lsquohelliptransition to chronicityhelliprsquo
1 Nociceptive inflammation ischaemia oedema pressure traction
2 Neuropathic peripheral amp central sensitisation
spinal cord neuroplasticity
neuroma
3 Psychological amp social
4 Genetic
The neuropathic component in persistent pain after surgery
systematic review Haroutiunian PAIN 2013
CPSP after 11 types of surgery
bull Amount of pain depends
bull on likelihood of nerve damage
Neuropathic pain
bull in 65 of thoracotomy patients
bull 33 groin surgery
bull 6 knee surgery
Post surgical breast pain
Jung PAIN 2003
1 Intercostobrachial neuralgia
2 Other nerve injury
3 Neuroma
4 Phantom breast
Natural History
Long-term follow-up of breast cancer survivors with post-mastectomy pain syndrome
Macdonald et al British J of Cancer 2005
1996helliphellip 43 pain 3 years 2002 hellip21 pain 9 years
Persistent pain after breast surgery 6-year nationwide
follow up
Mejdahl Kehlet et al BMJ 2013
2008hellip47 pain 1 year
2013hellip37 pain 6 years
Treatment - prevention
helliphellipfrom Pre-emptive Analgesia (blocking preoperative stimuli)
helliphellipto Preventative Analgesia (blocking noxious stimuli central sensitisation across the entire perioperative period)
Preventative treatments
1 Nerve blocks Regional
2 Drugs
Regional anaesthesia to prevent chronic pain after surgery a Cochrane systematic review and meta-analysisdagger M H Andreae1 and D A Andreae2
BJA 2013
bull 23 RCTrsquos
bull Epidural anaesthesia and
paravertebral blocks may be effective
in preventing chronic pain at 1 year
bull Effective in about 1 in 4
patients treated
Preincisional Paravertebral Block Reduces the Prevalence of Chronic
Pain After Breast Surgery Kairaluoma et al Anesth Analg 2006103703-708
bull Preincisional paravertebral block provides significant immediate postoperative analgesia
bull In the same patients (n = 60) 12 months sig less pain in the PVB group
bull In addition to providing acute postoperative pain relief preoperative PVB reduces the prevalence of chronic pain 1 yr after breast cancer surgery
Epidurals Intraoperative epidural analgesia provides preventative analgesia in
abdominal surgery Lavandrsquohomme et al Anaesthesiology 2005
bull Clear benefit of epidural in preventing chronic pain 1 year
bull Intraoperative epidural better than postoperative epidural
bull Effective epidural better than effective parenteral only analgesia one year
Systematic review of therapeutic interventions to reduce chronic post surgical pain (32 RCTrsquos)
Humble et al European J of Pain (2015)
POSITIVE
Gabapentinoids
Lidocaine
iv lidocaine EMLA
Regional
TIVA
NEGATIVE
Ketamine
Cryoanalgesia
Local anaesthetic infiltration
Remifentanil (increased chronic pain)
1 Gabapentin around time of surgery
lsquono effect on chronic painrsquo
POSITIVE
NEGATIVE
Meta analysis (Clarke 2012) 48 RCTrsquos positive effect at 2 months
Cochrane Systematic Review (Chaparro 2013) 280 patients analysed pain at 6 months No effect
RCT Gabapentin 1200mg prior to Thyroidectomy Sig less pain at 3 months (Brogley 2008)
RCT Gabapentin vs Placebo Knee replacement No effect on chronic pain (Clarke 2014)
2 Pregabalin ndash around time of surgery lsquoNot a recommended treatment can cause post operative somnolencersquo
Positive
Negative
Meta-analysis of 3 studies (Clarke 2012) All showed improvement in pain 2 RCTrsquoshellipvery large decrease in CPSP (p=0007)
3 unpublished RCTrsquos from Pfizer (2010-2014) hellipall negative for acute and chronic pain i) 307 patients undergoing knee replacement ii) 501 patients hysterectomy iii) 425 patient hernia
Cochrane Systematic Review (Chaparro 2013) 25 RCTrsquos significant benefit
Systematic review (Martinez May 2017) No difference between pregabalin and placebo 3 months Use for acute pain in pro-nociceptive surgery Side effects a problem
Multimodal analgesia
bull Standard protocols now widely used eg Paravertebral blocks at MD Anderson bull Pre-assessment clinic screening for pain psychological factors pain catastrophising scale helliphellipgenetic screening tests bull Education patients surgeons anaesthetists nurses psychologists
General treatment strategies for chronic postsurgical neuropathic pain
Preventative Perkins amp Kehlet Anesthesiology 2000
bullSurgical procedure preservation
sentinel node biopsy
bullBetter postoperative pain management
bullInformed consent preparatory
information
Established Dworkin Archives Neurol 2003 60
1524
bull Amitriptyline
bull Gabapentin
bull Opioids
bull Tramadol
bull 5 Lidoderm patch EMLA
Positive therapies for Prevention of PSBP
1 EMLA applied to chest wall prior
to surgery less pain 3 months
Fassoulaki 2000
2 Venlafaxine XR 70mg before
and for 2 weeks post surgeryno diff
acute pain significantly less chronic
pain 6 months
Reuben 2004
3 Aggressive acute pain
management
Iohom 2006
4 Preincisional paravertebral
block
Kairaluoma 2006
5 Multimodal analgesia with
gabapentin EMLA ropivacaine less
acute pain amp pain 6 months
Fassoulaki 2005
A pain management programme for chronic cancer-
treatment-related pain Robb Williams Duvivier Newham
Journal of Pain 2006775-150
bull Theory of cancer-related pain
bull Pain pathways
bull Overunder activity cycle
bull Pacing
bull Exercise and fitness
bull TENS
bull Posture and manual handling
bull Relapse and prevention
Psychology interventions
bull Goal setting
bull Role of factors involved in pain
bull Homework assignments
bull Relaxation techniques
bull Cognitive skills
bull Relapse and prevention
Results
significant (plt005) improvements in
bull Pain severity
bull Psychological distress
bull Pain amp psychological coping indices
bull Activities of daily living
bull General fitness
Research Proposal
Exercise to prevent shoulder conditions in patients
undergoing breast cancer treatment
bull Aim to conduct a randomised controlled trial (RCT) supported with qualitative research to investigate the clinical and cost-effectiveness of early supervised exercise on outcomes of arm function chronic pain and quality of life at one year in women undergoing treatment for breast cancer
Intervention
bull A physiotherapy-led structured exercise programme incorporating behavioural strategies and monitoring to encourage adherence
bull A minimum of 4 face-to-face specialist treatment sessions with individual participants will be
delivered within 12 weeks of surgery bull Access to interim telephone support will be provided The programme will restrict to controlled early
stretching and ROM exercises with subsequent progression to maintain strength and function (weeks 2 to 12)
bull Qualitative interviews will be used during the feasibility phase of the trial to explore acceptability of
to the intervention
Outcomes
bull arm shoulder and hand function at 12 months using the 30-item Disability Arm Shoulder Hand (DASH) questionnaire
bull quality of life
bull Functional Assessment of Cancer Treatment-Breast (FACT-B)
bull Short-Form-12 and EQ-5D-5L
bull Data on postoperative adverse events surgical site infection and healthcare resource use will be collected at 6 and 12 months after surgery
Positive therapies for Prevention of PSBP
1 EMLA applied to chest wall prior
to surgery less pain 3 months
Fassoulaki 2000
2 Venlafaxine XR 70mg before
and for 2 weeks post surgeryno diff
acute pain significantly less chronic
pain 6 months
Reuben 2004
3 Aggressive acute pain
management
Iohom 2006
4 Preincisional paravertebral
block
Kairaluoma 2006
5 Multimodal analgesia with
gabapentin EMLA ropivacaine less
acute pain amp pain 6 months
Fassoulaki 2005
Current Treatment Paradigms
The Toronto General Hospital
Transitional Pain Service
development and implementation
of a multidisciplinary program
to prevent chronic postsurgical pain (Katz J Pain Res 2015)
bull Nurse navigator
bull Psychologists (ACT)
Clinical Manifestations hellipour approach to the patient with CPSP
bull Type of pain Cause
bull Exclude other causes (infection recurrence)
bull Psychological and social factors
bull Temporal Context
Electronic Patient Record
Future Directions
bull Identify Causative Modifiable risk factors vs Associative risk factors
bull Measure psychological variables
bull Genetic assays to identify genes controlling the variability in developing chronic pain
Aim is lsquoto identify susceptibility to chronic pain and sensitivity to analgesicsrsquo
Chronic pain lsquoheritabilityrsquo is variable
Conclusions
bull 1 year incidence = 05 -10 bull Avoid pain before during and after surgery lsquohelliphelliptranslate advances in acute pain to chronic settinghelliphelliprsquo bull Psychological pre-assessment bull Education discussion with patients surgeons bull In some cases preventive analgesia may be beneficial bull Transitional Pain Servicehelliptrackinghellipdatabase lsquoPragmatic approachrsquo lsquoAll diseases have an acute phasersquo lsquoDrugs good for acute pain must be good for chronic painrsquo

Patient-related risk factors lsquohellippain predicts painrsquo
bull Preoperative pain (Forsythe 2008)
bull Intensity of acute pain (Masselin-Dubois 2013)
bull Acute neuropathic pain (Haroutiounian 2013)
bull High opioid consumption perioperatively (Kalso 2001)
bull Pain in other body parts (Pinto 2012)
bull Younger age (Masselin-Dubois 2013)
bull Female (Ochroch 2006)
Psychological risk factors
bull Pre-op anxiety and catastrophizing meta analysis (2x likelihood of developing CPSP (Theunissen Clin J Pain 2012)
bull Depression (Attal 2014)
bull Catastrophizing (Masselin-Dubois 2013)
bull Sensitivity to pain traumatisation (Page 2013)
bull Anxiety (Kleimann 2011)
bull Fear of long term consequences of surgery (Peters 2007)
Surgical risk factors
bull Low vs high volume surgical unit 13 increase in risk of CPSP (Tasmuth1999)
bull Duration of surgery (Kalso 2007)
bull Minimally invasive surgery (Grant 2004)
bull Stitch types (Cerfolio 2003)
bull Nerve damage preservation (Jensen 1985)
Predictive factors for chronic pain after breast surgery
Anderson et al Pain 2015 n=575
Pain at 1 year
bull Moderate- severe post op pain (50)
bull Axillary lymph node with ICB nerve preservation (30)
bull Neuropathic pain 1 week (18)
bull Age lt 65 (18)
Wang Canadian Medical Assoc Journal 2016 bull Young age bull Axillary lymph node dissection bull Acute pain High quality evidence showed no association
with BMI Type of breast surgery Chemotherapy Reconstruction
Clinical Prediction Model and Tool for Assessing Risk of Persistent Pain After Breast Cancer Surgery Tuomo J Meretoja Kenneth Geving Andersen Julie Bruce Lassi Haasio Reetta Sipilauml Neil W Scott Samuli Ripatti Henrik Kehlet and Eija Kalso
March 2017
Risk Factors ndash what can we discuss with surgeons
bull Information for patients
bull Pre-assessment pain clinic
bull Pre-op anaesthetic strategies algorithms PVB
bull Surgical technique ()
(eg mesh preservation of nerves
minimally invasive etc)
bull Enhanced recovery hellip
eg Kehlet et al Br J Surgery 2005
Fast Track Surgery
bull Pain clinic follow up
Pathophysiology lsquowhat is it about pain that causes more painrsquo
lsquohelliptransition to chronicityhelliprsquo
1 Nociceptive inflammation ischaemia oedema pressure traction
2 Neuropathic peripheral amp central sensitisation
spinal cord neuroplasticity
neuroma
3 Psychological amp social
4 Genetic
The neuropathic component in persistent pain after surgery
systematic review Haroutiunian PAIN 2013
CPSP after 11 types of surgery
bull Amount of pain depends
bull on likelihood of nerve damage
Neuropathic pain
bull in 65 of thoracotomy patients
bull 33 groin surgery
bull 6 knee surgery
Post surgical breast pain
Jung PAIN 2003
1 Intercostobrachial neuralgia
2 Other nerve injury
3 Neuroma
4 Phantom breast
Natural History
Long-term follow-up of breast cancer survivors with post-mastectomy pain syndrome
Macdonald et al British J of Cancer 2005
1996helliphellip 43 pain 3 years 2002 hellip21 pain 9 years
Persistent pain after breast surgery 6-year nationwide
follow up
Mejdahl Kehlet et al BMJ 2013
2008hellip47 pain 1 year
2013hellip37 pain 6 years
Treatment - prevention
helliphellipfrom Pre-emptive Analgesia (blocking preoperative stimuli)
helliphellipto Preventative Analgesia (blocking noxious stimuli central sensitisation across the entire perioperative period)
Preventative treatments
1 Nerve blocks Regional
2 Drugs
Regional anaesthesia to prevent chronic pain after surgery a Cochrane systematic review and meta-analysisdagger M H Andreae1 and D A Andreae2
BJA 2013
bull 23 RCTrsquos
bull Epidural anaesthesia and
paravertebral blocks may be effective
in preventing chronic pain at 1 year
bull Effective in about 1 in 4
patients treated
Preincisional Paravertebral Block Reduces the Prevalence of Chronic
Pain After Breast Surgery Kairaluoma et al Anesth Analg 2006103703-708
bull Preincisional paravertebral block provides significant immediate postoperative analgesia
bull In the same patients (n = 60) 12 months sig less pain in the PVB group
bull In addition to providing acute postoperative pain relief preoperative PVB reduces the prevalence of chronic pain 1 yr after breast cancer surgery
Epidurals Intraoperative epidural analgesia provides preventative analgesia in
abdominal surgery Lavandrsquohomme et al Anaesthesiology 2005
bull Clear benefit of epidural in preventing chronic pain 1 year
bull Intraoperative epidural better than postoperative epidural
bull Effective epidural better than effective parenteral only analgesia one year
Systematic review of therapeutic interventions to reduce chronic post surgical pain (32 RCTrsquos)
Humble et al European J of Pain (2015)
POSITIVE
Gabapentinoids
Lidocaine
iv lidocaine EMLA
Regional
TIVA
NEGATIVE
Ketamine
Cryoanalgesia
Local anaesthetic infiltration
Remifentanil (increased chronic pain)
1 Gabapentin around time of surgery
lsquono effect on chronic painrsquo
POSITIVE
NEGATIVE
Meta analysis (Clarke 2012) 48 RCTrsquos positive effect at 2 months
Cochrane Systematic Review (Chaparro 2013) 280 patients analysed pain at 6 months No effect
RCT Gabapentin 1200mg prior to Thyroidectomy Sig less pain at 3 months (Brogley 2008)
RCT Gabapentin vs Placebo Knee replacement No effect on chronic pain (Clarke 2014)
2 Pregabalin ndash around time of surgery lsquoNot a recommended treatment can cause post operative somnolencersquo
Positive
Negative
Meta-analysis of 3 studies (Clarke 2012) All showed improvement in pain 2 RCTrsquoshellipvery large decrease in CPSP (p=0007)
3 unpublished RCTrsquos from Pfizer (2010-2014) hellipall negative for acute and chronic pain i) 307 patients undergoing knee replacement ii) 501 patients hysterectomy iii) 425 patient hernia
Cochrane Systematic Review (Chaparro 2013) 25 RCTrsquos significant benefit
Systematic review (Martinez May 2017) No difference between pregabalin and placebo 3 months Use for acute pain in pro-nociceptive surgery Side effects a problem
Multimodal analgesia
bull Standard protocols now widely used eg Paravertebral blocks at MD Anderson bull Pre-assessment clinic screening for pain psychological factors pain catastrophising scale helliphellipgenetic screening tests bull Education patients surgeons anaesthetists nurses psychologists
General treatment strategies for chronic postsurgical neuropathic pain
Preventative Perkins amp Kehlet Anesthesiology 2000
bullSurgical procedure preservation
sentinel node biopsy
bullBetter postoperative pain management
bullInformed consent preparatory
information
Established Dworkin Archives Neurol 2003 60
1524
bull Amitriptyline
bull Gabapentin
bull Opioids
bull Tramadol
bull 5 Lidoderm patch EMLA
Positive therapies for Prevention of PSBP
1 EMLA applied to chest wall prior
to surgery less pain 3 months
Fassoulaki 2000
2 Venlafaxine XR 70mg before
and for 2 weeks post surgeryno diff
acute pain significantly less chronic
pain 6 months
Reuben 2004
3 Aggressive acute pain
management
Iohom 2006
4 Preincisional paravertebral
block
Kairaluoma 2006
5 Multimodal analgesia with
gabapentin EMLA ropivacaine less
acute pain amp pain 6 months
Fassoulaki 2005
A pain management programme for chronic cancer-
treatment-related pain Robb Williams Duvivier Newham
Journal of Pain 2006775-150
bull Theory of cancer-related pain
bull Pain pathways
bull Overunder activity cycle
bull Pacing
bull Exercise and fitness
bull TENS
bull Posture and manual handling
bull Relapse and prevention
Psychology interventions
bull Goal setting
bull Role of factors involved in pain
bull Homework assignments
bull Relaxation techniques
bull Cognitive skills
bull Relapse and prevention
Results
significant (plt005) improvements in
bull Pain severity
bull Psychological distress
bull Pain amp psychological coping indices
bull Activities of daily living
bull General fitness
Research Proposal
Exercise to prevent shoulder conditions in patients
undergoing breast cancer treatment
bull Aim to conduct a randomised controlled trial (RCT) supported with qualitative research to investigate the clinical and cost-effectiveness of early supervised exercise on outcomes of arm function chronic pain and quality of life at one year in women undergoing treatment for breast cancer
Intervention
bull A physiotherapy-led structured exercise programme incorporating behavioural strategies and monitoring to encourage adherence
bull A minimum of 4 face-to-face specialist treatment sessions with individual participants will be
delivered within 12 weeks of surgery bull Access to interim telephone support will be provided The programme will restrict to controlled early
stretching and ROM exercises with subsequent progression to maintain strength and function (weeks 2 to 12)
bull Qualitative interviews will be used during the feasibility phase of the trial to explore acceptability of
to the intervention
Outcomes
bull arm shoulder and hand function at 12 months using the 30-item Disability Arm Shoulder Hand (DASH) questionnaire
bull quality of life
bull Functional Assessment of Cancer Treatment-Breast (FACT-B)
bull Short-Form-12 and EQ-5D-5L
bull Data on postoperative adverse events surgical site infection and healthcare resource use will be collected at 6 and 12 months after surgery
Positive therapies for Prevention of PSBP
1 EMLA applied to chest wall prior
to surgery less pain 3 months
Fassoulaki 2000
2 Venlafaxine XR 70mg before
and for 2 weeks post surgeryno diff
acute pain significantly less chronic
pain 6 months
Reuben 2004
3 Aggressive acute pain
management
Iohom 2006
4 Preincisional paravertebral
block
Kairaluoma 2006
5 Multimodal analgesia with
gabapentin EMLA ropivacaine less
acute pain amp pain 6 months
Fassoulaki 2005
Current Treatment Paradigms
The Toronto General Hospital
Transitional Pain Service
development and implementation
of a multidisciplinary program
to prevent chronic postsurgical pain (Katz J Pain Res 2015)
bull Nurse navigator
bull Psychologists (ACT)
Clinical Manifestations hellipour approach to the patient with CPSP
bull Type of pain Cause
bull Exclude other causes (infection recurrence)
bull Psychological and social factors
bull Temporal Context
Electronic Patient Record
Future Directions
bull Identify Causative Modifiable risk factors vs Associative risk factors
bull Measure psychological variables
bull Genetic assays to identify genes controlling the variability in developing chronic pain
Aim is lsquoto identify susceptibility to chronic pain and sensitivity to analgesicsrsquo
Chronic pain lsquoheritabilityrsquo is variable
Conclusions
bull 1 year incidence = 05 -10 bull Avoid pain before during and after surgery lsquohelliphelliptranslate advances in acute pain to chronic settinghelliphelliprsquo bull Psychological pre-assessment bull Education discussion with patients surgeons bull In some cases preventive analgesia may be beneficial bull Transitional Pain Servicehelliptrackinghellipdatabase lsquoPragmatic approachrsquo lsquoAll diseases have an acute phasersquo lsquoDrugs good for acute pain must be good for chronic painrsquo

Psychological risk factors
bull Pre-op anxiety and catastrophizing meta analysis (2x likelihood of developing CPSP (Theunissen Clin J Pain 2012)
bull Depression (Attal 2014)
bull Catastrophizing (Masselin-Dubois 2013)
bull Sensitivity to pain traumatisation (Page 2013)
bull Anxiety (Kleimann 2011)
bull Fear of long term consequences of surgery (Peters 2007)
Surgical risk factors
bull Low vs high volume surgical unit 13 increase in risk of CPSP (Tasmuth1999)
bull Duration of surgery (Kalso 2007)
bull Minimally invasive surgery (Grant 2004)
bull Stitch types (Cerfolio 2003)
bull Nerve damage preservation (Jensen 1985)
Predictive factors for chronic pain after breast surgery
Anderson et al Pain 2015 n=575
Pain at 1 year
bull Moderate- severe post op pain (50)
bull Axillary lymph node with ICB nerve preservation (30)
bull Neuropathic pain 1 week (18)
bull Age lt 65 (18)
Wang Canadian Medical Assoc Journal 2016 bull Young age bull Axillary lymph node dissection bull Acute pain High quality evidence showed no association
with BMI Type of breast surgery Chemotherapy Reconstruction
Clinical Prediction Model and Tool for Assessing Risk of Persistent Pain After Breast Cancer Surgery Tuomo J Meretoja Kenneth Geving Andersen Julie Bruce Lassi Haasio Reetta Sipilauml Neil W Scott Samuli Ripatti Henrik Kehlet and Eija Kalso
March 2017
Risk Factors ndash what can we discuss with surgeons
bull Information for patients
bull Pre-assessment pain clinic
bull Pre-op anaesthetic strategies algorithms PVB
bull Surgical technique ()
(eg mesh preservation of nerves
minimally invasive etc)
bull Enhanced recovery hellip
eg Kehlet et al Br J Surgery 2005
Fast Track Surgery
bull Pain clinic follow up
Pathophysiology lsquowhat is it about pain that causes more painrsquo
lsquohelliptransition to chronicityhelliprsquo
1 Nociceptive inflammation ischaemia oedema pressure traction
2 Neuropathic peripheral amp central sensitisation
spinal cord neuroplasticity
neuroma
3 Psychological amp social
4 Genetic
The neuropathic component in persistent pain after surgery
systematic review Haroutiunian PAIN 2013
CPSP after 11 types of surgery
bull Amount of pain depends
bull on likelihood of nerve damage
Neuropathic pain
bull in 65 of thoracotomy patients
bull 33 groin surgery
bull 6 knee surgery
Post surgical breast pain
Jung PAIN 2003
1 Intercostobrachial neuralgia
2 Other nerve injury
3 Neuroma
4 Phantom breast
Natural History
Long-term follow-up of breast cancer survivors with post-mastectomy pain syndrome
Macdonald et al British J of Cancer 2005
1996helliphellip 43 pain 3 years 2002 hellip21 pain 9 years
Persistent pain after breast surgery 6-year nationwide
follow up
Mejdahl Kehlet et al BMJ 2013
2008hellip47 pain 1 year
2013hellip37 pain 6 years
Treatment - prevention
helliphellipfrom Pre-emptive Analgesia (blocking preoperative stimuli)
helliphellipto Preventative Analgesia (blocking noxious stimuli central sensitisation across the entire perioperative period)
Preventative treatments
1 Nerve blocks Regional
2 Drugs
Regional anaesthesia to prevent chronic pain after surgery a Cochrane systematic review and meta-analysisdagger M H Andreae1 and D A Andreae2
BJA 2013
bull 23 RCTrsquos
bull Epidural anaesthesia and
paravertebral blocks may be effective
in preventing chronic pain at 1 year
bull Effective in about 1 in 4
patients treated
Preincisional Paravertebral Block Reduces the Prevalence of Chronic
Pain After Breast Surgery Kairaluoma et al Anesth Analg 2006103703-708
bull Preincisional paravertebral block provides significant immediate postoperative analgesia
bull In the same patients (n = 60) 12 months sig less pain in the PVB group
bull In addition to providing acute postoperative pain relief preoperative PVB reduces the prevalence of chronic pain 1 yr after breast cancer surgery
Epidurals Intraoperative epidural analgesia provides preventative analgesia in
abdominal surgery Lavandrsquohomme et al Anaesthesiology 2005
bull Clear benefit of epidural in preventing chronic pain 1 year
bull Intraoperative epidural better than postoperative epidural
bull Effective epidural better than effective parenteral only analgesia one year
Systematic review of therapeutic interventions to reduce chronic post surgical pain (32 RCTrsquos)
Humble et al European J of Pain (2015)
POSITIVE
Gabapentinoids
Lidocaine
iv lidocaine EMLA
Regional
TIVA
NEGATIVE
Ketamine
Cryoanalgesia
Local anaesthetic infiltration
Remifentanil (increased chronic pain)
1 Gabapentin around time of surgery
lsquono effect on chronic painrsquo
POSITIVE
NEGATIVE
Meta analysis (Clarke 2012) 48 RCTrsquos positive effect at 2 months
Cochrane Systematic Review (Chaparro 2013) 280 patients analysed pain at 6 months No effect
RCT Gabapentin 1200mg prior to Thyroidectomy Sig less pain at 3 months (Brogley 2008)
RCT Gabapentin vs Placebo Knee replacement No effect on chronic pain (Clarke 2014)
2 Pregabalin ndash around time of surgery lsquoNot a recommended treatment can cause post operative somnolencersquo
Positive
Negative
Meta-analysis of 3 studies (Clarke 2012) All showed improvement in pain 2 RCTrsquoshellipvery large decrease in CPSP (p=0007)
3 unpublished RCTrsquos from Pfizer (2010-2014) hellipall negative for acute and chronic pain i) 307 patients undergoing knee replacement ii) 501 patients hysterectomy iii) 425 patient hernia
Cochrane Systematic Review (Chaparro 2013) 25 RCTrsquos significant benefit
Systematic review (Martinez May 2017) No difference between pregabalin and placebo 3 months Use for acute pain in pro-nociceptive surgery Side effects a problem
Multimodal analgesia
bull Standard protocols now widely used eg Paravertebral blocks at MD Anderson bull Pre-assessment clinic screening for pain psychological factors pain catastrophising scale helliphellipgenetic screening tests bull Education patients surgeons anaesthetists nurses psychologists
General treatment strategies for chronic postsurgical neuropathic pain
Preventative Perkins amp Kehlet Anesthesiology 2000
bullSurgical procedure preservation
sentinel node biopsy
bullBetter postoperative pain management
bullInformed consent preparatory
information
Established Dworkin Archives Neurol 2003 60
1524
bull Amitriptyline
bull Gabapentin
bull Opioids
bull Tramadol
bull 5 Lidoderm patch EMLA
Positive therapies for Prevention of PSBP
1 EMLA applied to chest wall prior
to surgery less pain 3 months
Fassoulaki 2000
2 Venlafaxine XR 70mg before
and for 2 weeks post surgeryno diff
acute pain significantly less chronic
pain 6 months
Reuben 2004
3 Aggressive acute pain
management
Iohom 2006
4 Preincisional paravertebral
block
Kairaluoma 2006
5 Multimodal analgesia with
gabapentin EMLA ropivacaine less
acute pain amp pain 6 months
Fassoulaki 2005
A pain management programme for chronic cancer-
treatment-related pain Robb Williams Duvivier Newham
Journal of Pain 2006775-150
bull Theory of cancer-related pain
bull Pain pathways
bull Overunder activity cycle
bull Pacing
bull Exercise and fitness
bull TENS
bull Posture and manual handling
bull Relapse and prevention
Psychology interventions
bull Goal setting
bull Role of factors involved in pain
bull Homework assignments
bull Relaxation techniques
bull Cognitive skills
bull Relapse and prevention
Results
significant (plt005) improvements in
bull Pain severity
bull Psychological distress
bull Pain amp psychological coping indices
bull Activities of daily living
bull General fitness
Research Proposal
Exercise to prevent shoulder conditions in patients
undergoing breast cancer treatment
bull Aim to conduct a randomised controlled trial (RCT) supported with qualitative research to investigate the clinical and cost-effectiveness of early supervised exercise on outcomes of arm function chronic pain and quality of life at one year in women undergoing treatment for breast cancer
Intervention
bull A physiotherapy-led structured exercise programme incorporating behavioural strategies and monitoring to encourage adherence
bull A minimum of 4 face-to-face specialist treatment sessions with individual participants will be
delivered within 12 weeks of surgery bull Access to interim telephone support will be provided The programme will restrict to controlled early
stretching and ROM exercises with subsequent progression to maintain strength and function (weeks 2 to 12)
bull Qualitative interviews will be used during the feasibility phase of the trial to explore acceptability of
to the intervention
Outcomes
bull arm shoulder and hand function at 12 months using the 30-item Disability Arm Shoulder Hand (DASH) questionnaire
bull quality of life
bull Functional Assessment of Cancer Treatment-Breast (FACT-B)
bull Short-Form-12 and EQ-5D-5L
bull Data on postoperative adverse events surgical site infection and healthcare resource use will be collected at 6 and 12 months after surgery
Positive therapies for Prevention of PSBP
1 EMLA applied to chest wall prior
to surgery less pain 3 months
Fassoulaki 2000
2 Venlafaxine XR 70mg before
and for 2 weeks post surgeryno diff
acute pain significantly less chronic
pain 6 months
Reuben 2004
3 Aggressive acute pain
management
Iohom 2006
4 Preincisional paravertebral
block
Kairaluoma 2006
5 Multimodal analgesia with
gabapentin EMLA ropivacaine less
acute pain amp pain 6 months
Fassoulaki 2005
Current Treatment Paradigms
The Toronto General Hospital
Transitional Pain Service
development and implementation
of a multidisciplinary program
to prevent chronic postsurgical pain (Katz J Pain Res 2015)
bull Nurse navigator
bull Psychologists (ACT)
Clinical Manifestations hellipour approach to the patient with CPSP
bull Type of pain Cause
bull Exclude other causes (infection recurrence)
bull Psychological and social factors
bull Temporal Context
Electronic Patient Record
Future Directions
bull Identify Causative Modifiable risk factors vs Associative risk factors
bull Measure psychological variables
bull Genetic assays to identify genes controlling the variability in developing chronic pain
Aim is lsquoto identify susceptibility to chronic pain and sensitivity to analgesicsrsquo
Chronic pain lsquoheritabilityrsquo is variable
Conclusions
bull 1 year incidence = 05 -10 bull Avoid pain before during and after surgery lsquohelliphelliptranslate advances in acute pain to chronic settinghelliphelliprsquo bull Psychological pre-assessment bull Education discussion with patients surgeons bull In some cases preventive analgesia may be beneficial bull Transitional Pain Servicehelliptrackinghellipdatabase lsquoPragmatic approachrsquo lsquoAll diseases have an acute phasersquo lsquoDrugs good for acute pain must be good for chronic painrsquo

Surgical risk factors
bull Low vs high volume surgical unit 13 increase in risk of CPSP (Tasmuth1999)
bull Duration of surgery (Kalso 2007)
bull Minimally invasive surgery (Grant 2004)
bull Stitch types (Cerfolio 2003)
bull Nerve damage preservation (Jensen 1985)
Predictive factors for chronic pain after breast surgery
Anderson et al Pain 2015 n=575
Pain at 1 year
bull Moderate- severe post op pain (50)
bull Axillary lymph node with ICB nerve preservation (30)
bull Neuropathic pain 1 week (18)
bull Age lt 65 (18)
Wang Canadian Medical Assoc Journal 2016 bull Young age bull Axillary lymph node dissection bull Acute pain High quality evidence showed no association
with BMI Type of breast surgery Chemotherapy Reconstruction
Clinical Prediction Model and Tool for Assessing Risk of Persistent Pain After Breast Cancer Surgery Tuomo J Meretoja Kenneth Geving Andersen Julie Bruce Lassi Haasio Reetta Sipilauml Neil W Scott Samuli Ripatti Henrik Kehlet and Eija Kalso
March 2017
Risk Factors ndash what can we discuss with surgeons
bull Information for patients
bull Pre-assessment pain clinic
bull Pre-op anaesthetic strategies algorithms PVB
bull Surgical technique ()
(eg mesh preservation of nerves
minimally invasive etc)
bull Enhanced recovery hellip
eg Kehlet et al Br J Surgery 2005
Fast Track Surgery
bull Pain clinic follow up
Pathophysiology lsquowhat is it about pain that causes more painrsquo
lsquohelliptransition to chronicityhelliprsquo
1 Nociceptive inflammation ischaemia oedema pressure traction
2 Neuropathic peripheral amp central sensitisation
spinal cord neuroplasticity
neuroma
3 Psychological amp social
4 Genetic
The neuropathic component in persistent pain after surgery
systematic review Haroutiunian PAIN 2013
CPSP after 11 types of surgery
bull Amount of pain depends
bull on likelihood of nerve damage
Neuropathic pain
bull in 65 of thoracotomy patients
bull 33 groin surgery
bull 6 knee surgery
Post surgical breast pain
Jung PAIN 2003
1 Intercostobrachial neuralgia
2 Other nerve injury
3 Neuroma
4 Phantom breast
Natural History
Long-term follow-up of breast cancer survivors with post-mastectomy pain syndrome
Macdonald et al British J of Cancer 2005
1996helliphellip 43 pain 3 years 2002 hellip21 pain 9 years
Persistent pain after breast surgery 6-year nationwide
follow up
Mejdahl Kehlet et al BMJ 2013
2008hellip47 pain 1 year
2013hellip37 pain 6 years
Treatment - prevention
helliphellipfrom Pre-emptive Analgesia (blocking preoperative stimuli)
helliphellipto Preventative Analgesia (blocking noxious stimuli central sensitisation across the entire perioperative period)
Preventative treatments
1 Nerve blocks Regional
2 Drugs
Regional anaesthesia to prevent chronic pain after surgery a Cochrane systematic review and meta-analysisdagger M H Andreae1 and D A Andreae2
BJA 2013
bull 23 RCTrsquos
bull Epidural anaesthesia and
paravertebral blocks may be effective
in preventing chronic pain at 1 year
bull Effective in about 1 in 4
patients treated
Preincisional Paravertebral Block Reduces the Prevalence of Chronic
Pain After Breast Surgery Kairaluoma et al Anesth Analg 2006103703-708
bull Preincisional paravertebral block provides significant immediate postoperative analgesia
bull In the same patients (n = 60) 12 months sig less pain in the PVB group
bull In addition to providing acute postoperative pain relief preoperative PVB reduces the prevalence of chronic pain 1 yr after breast cancer surgery
Epidurals Intraoperative epidural analgesia provides preventative analgesia in
abdominal surgery Lavandrsquohomme et al Anaesthesiology 2005
bull Clear benefit of epidural in preventing chronic pain 1 year
bull Intraoperative epidural better than postoperative epidural
bull Effective epidural better than effective parenteral only analgesia one year
Systematic review of therapeutic interventions to reduce chronic post surgical pain (32 RCTrsquos)
Humble et al European J of Pain (2015)
POSITIVE
Gabapentinoids
Lidocaine
iv lidocaine EMLA
Regional
TIVA
NEGATIVE
Ketamine
Cryoanalgesia
Local anaesthetic infiltration
Remifentanil (increased chronic pain)
1 Gabapentin around time of surgery
lsquono effect on chronic painrsquo
POSITIVE
NEGATIVE
Meta analysis (Clarke 2012) 48 RCTrsquos positive effect at 2 months
Cochrane Systematic Review (Chaparro 2013) 280 patients analysed pain at 6 months No effect
RCT Gabapentin 1200mg prior to Thyroidectomy Sig less pain at 3 months (Brogley 2008)
RCT Gabapentin vs Placebo Knee replacement No effect on chronic pain (Clarke 2014)
2 Pregabalin ndash around time of surgery lsquoNot a recommended treatment can cause post operative somnolencersquo
Positive
Negative
Meta-analysis of 3 studies (Clarke 2012) All showed improvement in pain 2 RCTrsquoshellipvery large decrease in CPSP (p=0007)
3 unpublished RCTrsquos from Pfizer (2010-2014) hellipall negative for acute and chronic pain i) 307 patients undergoing knee replacement ii) 501 patients hysterectomy iii) 425 patient hernia
Cochrane Systematic Review (Chaparro 2013) 25 RCTrsquos significant benefit
Systematic review (Martinez May 2017) No difference between pregabalin and placebo 3 months Use for acute pain in pro-nociceptive surgery Side effects a problem
Multimodal analgesia
bull Standard protocols now widely used eg Paravertebral blocks at MD Anderson bull Pre-assessment clinic screening for pain psychological factors pain catastrophising scale helliphellipgenetic screening tests bull Education patients surgeons anaesthetists nurses psychologists
General treatment strategies for chronic postsurgical neuropathic pain
Preventative Perkins amp Kehlet Anesthesiology 2000
bullSurgical procedure preservation
sentinel node biopsy
bullBetter postoperative pain management
bullInformed consent preparatory
information
Established Dworkin Archives Neurol 2003 60
1524
bull Amitriptyline
bull Gabapentin
bull Opioids
bull Tramadol
bull 5 Lidoderm patch EMLA
Positive therapies for Prevention of PSBP
1 EMLA applied to chest wall prior
to surgery less pain 3 months
Fassoulaki 2000
2 Venlafaxine XR 70mg before
and for 2 weeks post surgeryno diff
acute pain significantly less chronic
pain 6 months
Reuben 2004
3 Aggressive acute pain
management
Iohom 2006
4 Preincisional paravertebral
block
Kairaluoma 2006
5 Multimodal analgesia with
gabapentin EMLA ropivacaine less
acute pain amp pain 6 months
Fassoulaki 2005
A pain management programme for chronic cancer-
treatment-related pain Robb Williams Duvivier Newham
Journal of Pain 2006775-150
bull Theory of cancer-related pain
bull Pain pathways
bull Overunder activity cycle
bull Pacing
bull Exercise and fitness
bull TENS
bull Posture and manual handling
bull Relapse and prevention
Psychology interventions
bull Goal setting
bull Role of factors involved in pain
bull Homework assignments
bull Relaxation techniques
bull Cognitive skills
bull Relapse and prevention
Results
significant (plt005) improvements in
bull Pain severity
bull Psychological distress
bull Pain amp psychological coping indices
bull Activities of daily living
bull General fitness
Research Proposal
Exercise to prevent shoulder conditions in patients
undergoing breast cancer treatment
bull Aim to conduct a randomised controlled trial (RCT) supported with qualitative research to investigate the clinical and cost-effectiveness of early supervised exercise on outcomes of arm function chronic pain and quality of life at one year in women undergoing treatment for breast cancer
Intervention
bull A physiotherapy-led structured exercise programme incorporating behavioural strategies and monitoring to encourage adherence
bull A minimum of 4 face-to-face specialist treatment sessions with individual participants will be
delivered within 12 weeks of surgery bull Access to interim telephone support will be provided The programme will restrict to controlled early
stretching and ROM exercises with subsequent progression to maintain strength and function (weeks 2 to 12)
bull Qualitative interviews will be used during the feasibility phase of the trial to explore acceptability of
to the intervention
Outcomes
bull arm shoulder and hand function at 12 months using the 30-item Disability Arm Shoulder Hand (DASH) questionnaire
bull quality of life
bull Functional Assessment of Cancer Treatment-Breast (FACT-B)
bull Short-Form-12 and EQ-5D-5L
bull Data on postoperative adverse events surgical site infection and healthcare resource use will be collected at 6 and 12 months after surgery
Positive therapies for Prevention of PSBP
1 EMLA applied to chest wall prior
to surgery less pain 3 months
Fassoulaki 2000
2 Venlafaxine XR 70mg before
and for 2 weeks post surgeryno diff
acute pain significantly less chronic
pain 6 months
Reuben 2004
3 Aggressive acute pain
management
Iohom 2006
4 Preincisional paravertebral
block
Kairaluoma 2006
5 Multimodal analgesia with
gabapentin EMLA ropivacaine less
acute pain amp pain 6 months
Fassoulaki 2005
Current Treatment Paradigms
The Toronto General Hospital
Transitional Pain Service
development and implementation
of a multidisciplinary program
to prevent chronic postsurgical pain (Katz J Pain Res 2015)
bull Nurse navigator
bull Psychologists (ACT)
Clinical Manifestations hellipour approach to the patient with CPSP
bull Type of pain Cause
bull Exclude other causes (infection recurrence)
bull Psychological and social factors
bull Temporal Context
Electronic Patient Record
Future Directions
bull Identify Causative Modifiable risk factors vs Associative risk factors
bull Measure psychological variables
bull Genetic assays to identify genes controlling the variability in developing chronic pain
Aim is lsquoto identify susceptibility to chronic pain and sensitivity to analgesicsrsquo
Chronic pain lsquoheritabilityrsquo is variable
Conclusions
bull 1 year incidence = 05 -10 bull Avoid pain before during and after surgery lsquohelliphelliptranslate advances in acute pain to chronic settinghelliphelliprsquo bull Psychological pre-assessment bull Education discussion with patients surgeons bull In some cases preventive analgesia may be beneficial bull Transitional Pain Servicehelliptrackinghellipdatabase lsquoPragmatic approachrsquo lsquoAll diseases have an acute phasersquo lsquoDrugs good for acute pain must be good for chronic painrsquo

Predictive factors for chronic pain after breast surgery
Anderson et al Pain 2015 n=575
Pain at 1 year
bull Moderate- severe post op pain (50)
bull Axillary lymph node with ICB nerve preservation (30)
bull Neuropathic pain 1 week (18)
bull Age lt 65 (18)
Wang Canadian Medical Assoc Journal 2016 bull Young age bull Axillary lymph node dissection bull Acute pain High quality evidence showed no association
with BMI Type of breast surgery Chemotherapy Reconstruction
Clinical Prediction Model and Tool for Assessing Risk of Persistent Pain After Breast Cancer Surgery Tuomo J Meretoja Kenneth Geving Andersen Julie Bruce Lassi Haasio Reetta Sipilauml Neil W Scott Samuli Ripatti Henrik Kehlet and Eija Kalso
March 2017
Risk Factors ndash what can we discuss with surgeons
bull Information for patients
bull Pre-assessment pain clinic
bull Pre-op anaesthetic strategies algorithms PVB
bull Surgical technique ()
(eg mesh preservation of nerves
minimally invasive etc)
bull Enhanced recovery hellip
eg Kehlet et al Br J Surgery 2005
Fast Track Surgery
bull Pain clinic follow up
Pathophysiology lsquowhat is it about pain that causes more painrsquo
lsquohelliptransition to chronicityhelliprsquo
1 Nociceptive inflammation ischaemia oedema pressure traction
2 Neuropathic peripheral amp central sensitisation
spinal cord neuroplasticity
neuroma
3 Psychological amp social
4 Genetic
The neuropathic component in persistent pain after surgery
systematic review Haroutiunian PAIN 2013
CPSP after 11 types of surgery
bull Amount of pain depends
bull on likelihood of nerve damage
Neuropathic pain
bull in 65 of thoracotomy patients
bull 33 groin surgery
bull 6 knee surgery
Post surgical breast pain
Jung PAIN 2003
1 Intercostobrachial neuralgia
2 Other nerve injury
3 Neuroma
4 Phantom breast
Natural History
Long-term follow-up of breast cancer survivors with post-mastectomy pain syndrome
Macdonald et al British J of Cancer 2005
1996helliphellip 43 pain 3 years 2002 hellip21 pain 9 years
Persistent pain after breast surgery 6-year nationwide
follow up
Mejdahl Kehlet et al BMJ 2013
2008hellip47 pain 1 year
2013hellip37 pain 6 years
Treatment - prevention
helliphellipfrom Pre-emptive Analgesia (blocking preoperative stimuli)
helliphellipto Preventative Analgesia (blocking noxious stimuli central sensitisation across the entire perioperative period)
Preventative treatments
1 Nerve blocks Regional
2 Drugs
Regional anaesthesia to prevent chronic pain after surgery a Cochrane systematic review and meta-analysisdagger M H Andreae1 and D A Andreae2
BJA 2013
bull 23 RCTrsquos
bull Epidural anaesthesia and
paravertebral blocks may be effective
in preventing chronic pain at 1 year
bull Effective in about 1 in 4
patients treated
Preincisional Paravertebral Block Reduces the Prevalence of Chronic
Pain After Breast Surgery Kairaluoma et al Anesth Analg 2006103703-708
bull Preincisional paravertebral block provides significant immediate postoperative analgesia
bull In the same patients (n = 60) 12 months sig less pain in the PVB group
bull In addition to providing acute postoperative pain relief preoperative PVB reduces the prevalence of chronic pain 1 yr after breast cancer surgery
Epidurals Intraoperative epidural analgesia provides preventative analgesia in
abdominal surgery Lavandrsquohomme et al Anaesthesiology 2005
bull Clear benefit of epidural in preventing chronic pain 1 year
bull Intraoperative epidural better than postoperative epidural
bull Effective epidural better than effective parenteral only analgesia one year
Systematic review of therapeutic interventions to reduce chronic post surgical pain (32 RCTrsquos)
Humble et al European J of Pain (2015)
POSITIVE
Gabapentinoids
Lidocaine
iv lidocaine EMLA
Regional
TIVA
NEGATIVE
Ketamine
Cryoanalgesia
Local anaesthetic infiltration
Remifentanil (increased chronic pain)
1 Gabapentin around time of surgery
lsquono effect on chronic painrsquo
POSITIVE
NEGATIVE
Meta analysis (Clarke 2012) 48 RCTrsquos positive effect at 2 months
Cochrane Systematic Review (Chaparro 2013) 280 patients analysed pain at 6 months No effect
RCT Gabapentin 1200mg prior to Thyroidectomy Sig less pain at 3 months (Brogley 2008)
RCT Gabapentin vs Placebo Knee replacement No effect on chronic pain (Clarke 2014)
2 Pregabalin ndash around time of surgery lsquoNot a recommended treatment can cause post operative somnolencersquo
Positive
Negative
Meta-analysis of 3 studies (Clarke 2012) All showed improvement in pain 2 RCTrsquoshellipvery large decrease in CPSP (p=0007)
3 unpublished RCTrsquos from Pfizer (2010-2014) hellipall negative for acute and chronic pain i) 307 patients undergoing knee replacement ii) 501 patients hysterectomy iii) 425 patient hernia
Cochrane Systematic Review (Chaparro 2013) 25 RCTrsquos significant benefit
Systematic review (Martinez May 2017) No difference between pregabalin and placebo 3 months Use for acute pain in pro-nociceptive surgery Side effects a problem
Multimodal analgesia
bull Standard protocols now widely used eg Paravertebral blocks at MD Anderson bull Pre-assessment clinic screening for pain psychological factors pain catastrophising scale helliphellipgenetic screening tests bull Education patients surgeons anaesthetists nurses psychologists
General treatment strategies for chronic postsurgical neuropathic pain
Preventative Perkins amp Kehlet Anesthesiology 2000
bullSurgical procedure preservation
sentinel node biopsy
bullBetter postoperative pain management
bullInformed consent preparatory
information
Established Dworkin Archives Neurol 2003 60
1524
bull Amitriptyline
bull Gabapentin
bull Opioids
bull Tramadol
bull 5 Lidoderm patch EMLA
Positive therapies for Prevention of PSBP
1 EMLA applied to chest wall prior
to surgery less pain 3 months
Fassoulaki 2000
2 Venlafaxine XR 70mg before
and for 2 weeks post surgeryno diff
acute pain significantly less chronic
pain 6 months
Reuben 2004
3 Aggressive acute pain
management
Iohom 2006
4 Preincisional paravertebral
block
Kairaluoma 2006
5 Multimodal analgesia with
gabapentin EMLA ropivacaine less
acute pain amp pain 6 months
Fassoulaki 2005
A pain management programme for chronic cancer-
treatment-related pain Robb Williams Duvivier Newham
Journal of Pain 2006775-150
bull Theory of cancer-related pain
bull Pain pathways
bull Overunder activity cycle
bull Pacing
bull Exercise and fitness
bull TENS
bull Posture and manual handling
bull Relapse and prevention
Psychology interventions
bull Goal setting
bull Role of factors involved in pain
bull Homework assignments
bull Relaxation techniques
bull Cognitive skills
bull Relapse and prevention
Results
significant (plt005) improvements in
bull Pain severity
bull Psychological distress
bull Pain amp psychological coping indices
bull Activities of daily living
bull General fitness
Research Proposal
Exercise to prevent shoulder conditions in patients
undergoing breast cancer treatment
bull Aim to conduct a randomised controlled trial (RCT) supported with qualitative research to investigate the clinical and cost-effectiveness of early supervised exercise on outcomes of arm function chronic pain and quality of life at one year in women undergoing treatment for breast cancer
Intervention
bull A physiotherapy-led structured exercise programme incorporating behavioural strategies and monitoring to encourage adherence
bull A minimum of 4 face-to-face specialist treatment sessions with individual participants will be
delivered within 12 weeks of surgery bull Access to interim telephone support will be provided The programme will restrict to controlled early
stretching and ROM exercises with subsequent progression to maintain strength and function (weeks 2 to 12)
bull Qualitative interviews will be used during the feasibility phase of the trial to explore acceptability of
to the intervention
Outcomes
bull arm shoulder and hand function at 12 months using the 30-item Disability Arm Shoulder Hand (DASH) questionnaire
bull quality of life
bull Functional Assessment of Cancer Treatment-Breast (FACT-B)
bull Short-Form-12 and EQ-5D-5L
bull Data on postoperative adverse events surgical site infection and healthcare resource use will be collected at 6 and 12 months after surgery
Positive therapies for Prevention of PSBP
1 EMLA applied to chest wall prior
to surgery less pain 3 months
Fassoulaki 2000
2 Venlafaxine XR 70mg before
and for 2 weeks post surgeryno diff
acute pain significantly less chronic
pain 6 months
Reuben 2004
3 Aggressive acute pain
management
Iohom 2006
4 Preincisional paravertebral
block
Kairaluoma 2006
5 Multimodal analgesia with
gabapentin EMLA ropivacaine less
acute pain amp pain 6 months
Fassoulaki 2005
Current Treatment Paradigms
The Toronto General Hospital
Transitional Pain Service
development and implementation
of a multidisciplinary program
to prevent chronic postsurgical pain (Katz J Pain Res 2015)
bull Nurse navigator
bull Psychologists (ACT)
Clinical Manifestations hellipour approach to the patient with CPSP
bull Type of pain Cause
bull Exclude other causes (infection recurrence)
bull Psychological and social factors
bull Temporal Context
Electronic Patient Record
Future Directions
bull Identify Causative Modifiable risk factors vs Associative risk factors
bull Measure psychological variables
bull Genetic assays to identify genes controlling the variability in developing chronic pain
Aim is lsquoto identify susceptibility to chronic pain and sensitivity to analgesicsrsquo
Chronic pain lsquoheritabilityrsquo is variable
Conclusions
bull 1 year incidence = 05 -10 bull Avoid pain before during and after surgery lsquohelliphelliptranslate advances in acute pain to chronic settinghelliphelliprsquo bull Psychological pre-assessment bull Education discussion with patients surgeons bull In some cases preventive analgesia may be beneficial bull Transitional Pain Servicehelliptrackinghellipdatabase lsquoPragmatic approachrsquo lsquoAll diseases have an acute phasersquo lsquoDrugs good for acute pain must be good for chronic painrsquo

Clinical Prediction Model and Tool for Assessing Risk of Persistent Pain After Breast Cancer Surgery Tuomo J Meretoja Kenneth Geving Andersen Julie Bruce Lassi Haasio Reetta Sipilauml Neil W Scott Samuli Ripatti Henrik Kehlet and Eija Kalso
March 2017
Risk Factors ndash what can we discuss with surgeons
bull Information for patients
bull Pre-assessment pain clinic
bull Pre-op anaesthetic strategies algorithms PVB
bull Surgical technique ()
(eg mesh preservation of nerves
minimally invasive etc)
bull Enhanced recovery hellip
eg Kehlet et al Br J Surgery 2005
Fast Track Surgery
bull Pain clinic follow up
Pathophysiology lsquowhat is it about pain that causes more painrsquo
lsquohelliptransition to chronicityhelliprsquo
1 Nociceptive inflammation ischaemia oedema pressure traction
2 Neuropathic peripheral amp central sensitisation
spinal cord neuroplasticity
neuroma
3 Psychological amp social
4 Genetic
The neuropathic component in persistent pain after surgery
systematic review Haroutiunian PAIN 2013
CPSP after 11 types of surgery
bull Amount of pain depends
bull on likelihood of nerve damage
Neuropathic pain
bull in 65 of thoracotomy patients
bull 33 groin surgery
bull 6 knee surgery
Post surgical breast pain
Jung PAIN 2003
1 Intercostobrachial neuralgia
2 Other nerve injury
3 Neuroma
4 Phantom breast
Natural History
Long-term follow-up of breast cancer survivors with post-mastectomy pain syndrome
Macdonald et al British J of Cancer 2005
1996helliphellip 43 pain 3 years 2002 hellip21 pain 9 years
Persistent pain after breast surgery 6-year nationwide
follow up
Mejdahl Kehlet et al BMJ 2013
2008hellip47 pain 1 year
2013hellip37 pain 6 years
Treatment - prevention
helliphellipfrom Pre-emptive Analgesia (blocking preoperative stimuli)
helliphellipto Preventative Analgesia (blocking noxious stimuli central sensitisation across the entire perioperative period)
Preventative treatments
1 Nerve blocks Regional
2 Drugs
Regional anaesthesia to prevent chronic pain after surgery a Cochrane systematic review and meta-analysisdagger M H Andreae1 and D A Andreae2
BJA 2013
bull 23 RCTrsquos
bull Epidural anaesthesia and
paravertebral blocks may be effective
in preventing chronic pain at 1 year
bull Effective in about 1 in 4
patients treated
Preincisional Paravertebral Block Reduces the Prevalence of Chronic
Pain After Breast Surgery Kairaluoma et al Anesth Analg 2006103703-708
bull Preincisional paravertebral block provides significant immediate postoperative analgesia
bull In the same patients (n = 60) 12 months sig less pain in the PVB group
bull In addition to providing acute postoperative pain relief preoperative PVB reduces the prevalence of chronic pain 1 yr after breast cancer surgery
Epidurals Intraoperative epidural analgesia provides preventative analgesia in
abdominal surgery Lavandrsquohomme et al Anaesthesiology 2005
bull Clear benefit of epidural in preventing chronic pain 1 year
bull Intraoperative epidural better than postoperative epidural
bull Effective epidural better than effective parenteral only analgesia one year
Systematic review of therapeutic interventions to reduce chronic post surgical pain (32 RCTrsquos)
Humble et al European J of Pain (2015)
POSITIVE
Gabapentinoids
Lidocaine
iv lidocaine EMLA
Regional
TIVA
NEGATIVE
Ketamine
Cryoanalgesia
Local anaesthetic infiltration
Remifentanil (increased chronic pain)
1 Gabapentin around time of surgery
lsquono effect on chronic painrsquo
POSITIVE
NEGATIVE
Meta analysis (Clarke 2012) 48 RCTrsquos positive effect at 2 months
Cochrane Systematic Review (Chaparro 2013) 280 patients analysed pain at 6 months No effect
RCT Gabapentin 1200mg prior to Thyroidectomy Sig less pain at 3 months (Brogley 2008)
RCT Gabapentin vs Placebo Knee replacement No effect on chronic pain (Clarke 2014)
2 Pregabalin ndash around time of surgery lsquoNot a recommended treatment can cause post operative somnolencersquo
Positive
Negative
Meta-analysis of 3 studies (Clarke 2012) All showed improvement in pain 2 RCTrsquoshellipvery large decrease in CPSP (p=0007)
3 unpublished RCTrsquos from Pfizer (2010-2014) hellipall negative for acute and chronic pain i) 307 patients undergoing knee replacement ii) 501 patients hysterectomy iii) 425 patient hernia
Cochrane Systematic Review (Chaparro 2013) 25 RCTrsquos significant benefit
Systematic review (Martinez May 2017) No difference between pregabalin and placebo 3 months Use for acute pain in pro-nociceptive surgery Side effects a problem
Multimodal analgesia
bull Standard protocols now widely used eg Paravertebral blocks at MD Anderson bull Pre-assessment clinic screening for pain psychological factors pain catastrophising scale helliphellipgenetic screening tests bull Education patients surgeons anaesthetists nurses psychologists
General treatment strategies for chronic postsurgical neuropathic pain
Preventative Perkins amp Kehlet Anesthesiology 2000
bullSurgical procedure preservation
sentinel node biopsy
bullBetter postoperative pain management
bullInformed consent preparatory
information
Established Dworkin Archives Neurol 2003 60
1524
bull Amitriptyline
bull Gabapentin
bull Opioids
bull Tramadol
bull 5 Lidoderm patch EMLA
Positive therapies for Prevention of PSBP
1 EMLA applied to chest wall prior
to surgery less pain 3 months
Fassoulaki 2000
2 Venlafaxine XR 70mg before
and for 2 weeks post surgeryno diff
acute pain significantly less chronic
pain 6 months
Reuben 2004
3 Aggressive acute pain
management
Iohom 2006
4 Preincisional paravertebral
block
Kairaluoma 2006
5 Multimodal analgesia with
gabapentin EMLA ropivacaine less
acute pain amp pain 6 months
Fassoulaki 2005
A pain management programme for chronic cancer-
treatment-related pain Robb Williams Duvivier Newham
Journal of Pain 2006775-150
bull Theory of cancer-related pain
bull Pain pathways
bull Overunder activity cycle
bull Pacing
bull Exercise and fitness
bull TENS
bull Posture and manual handling
bull Relapse and prevention
Psychology interventions
bull Goal setting
bull Role of factors involved in pain
bull Homework assignments
bull Relaxation techniques
bull Cognitive skills
bull Relapse and prevention
Results
significant (plt005) improvements in
bull Pain severity
bull Psychological distress
bull Pain amp psychological coping indices
bull Activities of daily living
bull General fitness
Research Proposal
Exercise to prevent shoulder conditions in patients
undergoing breast cancer treatment
bull Aim to conduct a randomised controlled trial (RCT) supported with qualitative research to investigate the clinical and cost-effectiveness of early supervised exercise on outcomes of arm function chronic pain and quality of life at one year in women undergoing treatment for breast cancer
Intervention
bull A physiotherapy-led structured exercise programme incorporating behavioural strategies and monitoring to encourage adherence
bull A minimum of 4 face-to-face specialist treatment sessions with individual participants will be
delivered within 12 weeks of surgery bull Access to interim telephone support will be provided The programme will restrict to controlled early
stretching and ROM exercises with subsequent progression to maintain strength and function (weeks 2 to 12)
bull Qualitative interviews will be used during the feasibility phase of the trial to explore acceptability of
to the intervention
Outcomes
bull arm shoulder and hand function at 12 months using the 30-item Disability Arm Shoulder Hand (DASH) questionnaire
bull quality of life
bull Functional Assessment of Cancer Treatment-Breast (FACT-B)
bull Short-Form-12 and EQ-5D-5L
bull Data on postoperative adverse events surgical site infection and healthcare resource use will be collected at 6 and 12 months after surgery
Positive therapies for Prevention of PSBP
1 EMLA applied to chest wall prior
to surgery less pain 3 months
Fassoulaki 2000
2 Venlafaxine XR 70mg before
and for 2 weeks post surgeryno diff
acute pain significantly less chronic
pain 6 months
Reuben 2004
3 Aggressive acute pain
management
Iohom 2006
4 Preincisional paravertebral
block
Kairaluoma 2006
5 Multimodal analgesia with
gabapentin EMLA ropivacaine less
acute pain amp pain 6 months
Fassoulaki 2005
Current Treatment Paradigms
The Toronto General Hospital
Transitional Pain Service
development and implementation
of a multidisciplinary program
to prevent chronic postsurgical pain (Katz J Pain Res 2015)
bull Nurse navigator
bull Psychologists (ACT)
Clinical Manifestations hellipour approach to the patient with CPSP
bull Type of pain Cause
bull Exclude other causes (infection recurrence)
bull Psychological and social factors
bull Temporal Context
Electronic Patient Record
Future Directions
bull Identify Causative Modifiable risk factors vs Associative risk factors
bull Measure psychological variables
bull Genetic assays to identify genes controlling the variability in developing chronic pain
Aim is lsquoto identify susceptibility to chronic pain and sensitivity to analgesicsrsquo
Chronic pain lsquoheritabilityrsquo is variable
Conclusions
bull 1 year incidence = 05 -10 bull Avoid pain before during and after surgery lsquohelliphelliptranslate advances in acute pain to chronic settinghelliphelliprsquo bull Psychological pre-assessment bull Education discussion with patients surgeons bull In some cases preventive analgesia may be beneficial bull Transitional Pain Servicehelliptrackinghellipdatabase lsquoPragmatic approachrsquo lsquoAll diseases have an acute phasersquo lsquoDrugs good for acute pain must be good for chronic painrsquo

Risk Factors ndash what can we discuss with surgeons
bull Information for patients
bull Pre-assessment pain clinic
bull Pre-op anaesthetic strategies algorithms PVB
bull Surgical technique ()
(eg mesh preservation of nerves
minimally invasive etc)
bull Enhanced recovery hellip
eg Kehlet et al Br J Surgery 2005
Fast Track Surgery
bull Pain clinic follow up
Pathophysiology lsquowhat is it about pain that causes more painrsquo
lsquohelliptransition to chronicityhelliprsquo
1 Nociceptive inflammation ischaemia oedema pressure traction
2 Neuropathic peripheral amp central sensitisation
spinal cord neuroplasticity
neuroma
3 Psychological amp social
4 Genetic
The neuropathic component in persistent pain after surgery
systematic review Haroutiunian PAIN 2013
CPSP after 11 types of surgery
bull Amount of pain depends
bull on likelihood of nerve damage
Neuropathic pain
bull in 65 of thoracotomy patients
bull 33 groin surgery
bull 6 knee surgery
Post surgical breast pain
Jung PAIN 2003
1 Intercostobrachial neuralgia
2 Other nerve injury
3 Neuroma
4 Phantom breast
Natural History
Long-term follow-up of breast cancer survivors with post-mastectomy pain syndrome
Macdonald et al British J of Cancer 2005
1996helliphellip 43 pain 3 years 2002 hellip21 pain 9 years
Persistent pain after breast surgery 6-year nationwide
follow up
Mejdahl Kehlet et al BMJ 2013
2008hellip47 pain 1 year
2013hellip37 pain 6 years
Treatment - prevention
helliphellipfrom Pre-emptive Analgesia (blocking preoperative stimuli)
helliphellipto Preventative Analgesia (blocking noxious stimuli central sensitisation across the entire perioperative period)
Preventative treatments
1 Nerve blocks Regional
2 Drugs
Regional anaesthesia to prevent chronic pain after surgery a Cochrane systematic review and meta-analysisdagger M H Andreae1 and D A Andreae2
BJA 2013
bull 23 RCTrsquos
bull Epidural anaesthesia and
paravertebral blocks may be effective
in preventing chronic pain at 1 year
bull Effective in about 1 in 4
patients treated
Preincisional Paravertebral Block Reduces the Prevalence of Chronic
Pain After Breast Surgery Kairaluoma et al Anesth Analg 2006103703-708
bull Preincisional paravertebral block provides significant immediate postoperative analgesia
bull In the same patients (n = 60) 12 months sig less pain in the PVB group
bull In addition to providing acute postoperative pain relief preoperative PVB reduces the prevalence of chronic pain 1 yr after breast cancer surgery
Epidurals Intraoperative epidural analgesia provides preventative analgesia in
abdominal surgery Lavandrsquohomme et al Anaesthesiology 2005
bull Clear benefit of epidural in preventing chronic pain 1 year
bull Intraoperative epidural better than postoperative epidural
bull Effective epidural better than effective parenteral only analgesia one year
Systematic review of therapeutic interventions to reduce chronic post surgical pain (32 RCTrsquos)
Humble et al European J of Pain (2015)
POSITIVE
Gabapentinoids
Lidocaine
iv lidocaine EMLA
Regional
TIVA
NEGATIVE
Ketamine
Cryoanalgesia
Local anaesthetic infiltration
Remifentanil (increased chronic pain)
1 Gabapentin around time of surgery
lsquono effect on chronic painrsquo
POSITIVE
NEGATIVE
Meta analysis (Clarke 2012) 48 RCTrsquos positive effect at 2 months
Cochrane Systematic Review (Chaparro 2013) 280 patients analysed pain at 6 months No effect
RCT Gabapentin 1200mg prior to Thyroidectomy Sig less pain at 3 months (Brogley 2008)
RCT Gabapentin vs Placebo Knee replacement No effect on chronic pain (Clarke 2014)
2 Pregabalin ndash around time of surgery lsquoNot a recommended treatment can cause post operative somnolencersquo
Positive
Negative
Meta-analysis of 3 studies (Clarke 2012) All showed improvement in pain 2 RCTrsquoshellipvery large decrease in CPSP (p=0007)
3 unpublished RCTrsquos from Pfizer (2010-2014) hellipall negative for acute and chronic pain i) 307 patients undergoing knee replacement ii) 501 patients hysterectomy iii) 425 patient hernia
Cochrane Systematic Review (Chaparro 2013) 25 RCTrsquos significant benefit
Systematic review (Martinez May 2017) No difference between pregabalin and placebo 3 months Use for acute pain in pro-nociceptive surgery Side effects a problem
Multimodal analgesia
bull Standard protocols now widely used eg Paravertebral blocks at MD Anderson bull Pre-assessment clinic screening for pain psychological factors pain catastrophising scale helliphellipgenetic screening tests bull Education patients surgeons anaesthetists nurses psychologists
General treatment strategies for chronic postsurgical neuropathic pain
Preventative Perkins amp Kehlet Anesthesiology 2000
bullSurgical procedure preservation
sentinel node biopsy
bullBetter postoperative pain management
bullInformed consent preparatory
information
Established Dworkin Archives Neurol 2003 60
1524
bull Amitriptyline
bull Gabapentin
bull Opioids
bull Tramadol
bull 5 Lidoderm patch EMLA
Positive therapies for Prevention of PSBP
1 EMLA applied to chest wall prior
to surgery less pain 3 months
Fassoulaki 2000
2 Venlafaxine XR 70mg before
and for 2 weeks post surgeryno diff
acute pain significantly less chronic
pain 6 months
Reuben 2004
3 Aggressive acute pain
management
Iohom 2006
4 Preincisional paravertebral
block
Kairaluoma 2006
5 Multimodal analgesia with
gabapentin EMLA ropivacaine less
acute pain amp pain 6 months
Fassoulaki 2005
A pain management programme for chronic cancer-
treatment-related pain Robb Williams Duvivier Newham
Journal of Pain 2006775-150
bull Theory of cancer-related pain
bull Pain pathways
bull Overunder activity cycle
bull Pacing
bull Exercise and fitness
bull TENS
bull Posture and manual handling
bull Relapse and prevention
Psychology interventions
bull Goal setting
bull Role of factors involved in pain
bull Homework assignments
bull Relaxation techniques
bull Cognitive skills
bull Relapse and prevention
Results
significant (plt005) improvements in
bull Pain severity
bull Psychological distress
bull Pain amp psychological coping indices
bull Activities of daily living
bull General fitness
Research Proposal
Exercise to prevent shoulder conditions in patients
undergoing breast cancer treatment
bull Aim to conduct a randomised controlled trial (RCT) supported with qualitative research to investigate the clinical and cost-effectiveness of early supervised exercise on outcomes of arm function chronic pain and quality of life at one year in women undergoing treatment for breast cancer
Intervention
bull A physiotherapy-led structured exercise programme incorporating behavioural strategies and monitoring to encourage adherence
bull A minimum of 4 face-to-face specialist treatment sessions with individual participants will be
delivered within 12 weeks of surgery bull Access to interim telephone support will be provided The programme will restrict to controlled early
stretching and ROM exercises with subsequent progression to maintain strength and function (weeks 2 to 12)
bull Qualitative interviews will be used during the feasibility phase of the trial to explore acceptability of
to the intervention
Outcomes
bull arm shoulder and hand function at 12 months using the 30-item Disability Arm Shoulder Hand (DASH) questionnaire
bull quality of life
bull Functional Assessment of Cancer Treatment-Breast (FACT-B)
bull Short-Form-12 and EQ-5D-5L
bull Data on postoperative adverse events surgical site infection and healthcare resource use will be collected at 6 and 12 months after surgery
Positive therapies for Prevention of PSBP
1 EMLA applied to chest wall prior
to surgery less pain 3 months
Fassoulaki 2000
2 Venlafaxine XR 70mg before
and for 2 weeks post surgeryno diff
acute pain significantly less chronic
pain 6 months
Reuben 2004
3 Aggressive acute pain
management
Iohom 2006
4 Preincisional paravertebral
block
Kairaluoma 2006
5 Multimodal analgesia with
gabapentin EMLA ropivacaine less
acute pain amp pain 6 months
Fassoulaki 2005
Current Treatment Paradigms
The Toronto General Hospital
Transitional Pain Service
development and implementation
of a multidisciplinary program
to prevent chronic postsurgical pain (Katz J Pain Res 2015)
bull Nurse navigator
bull Psychologists (ACT)
Clinical Manifestations hellipour approach to the patient with CPSP
bull Type of pain Cause
bull Exclude other causes (infection recurrence)
bull Psychological and social factors
bull Temporal Context
Electronic Patient Record
Future Directions
bull Identify Causative Modifiable risk factors vs Associative risk factors
bull Measure psychological variables
bull Genetic assays to identify genes controlling the variability in developing chronic pain
Aim is lsquoto identify susceptibility to chronic pain and sensitivity to analgesicsrsquo
Chronic pain lsquoheritabilityrsquo is variable
Conclusions
bull 1 year incidence = 05 -10 bull Avoid pain before during and after surgery lsquohelliphelliptranslate advances in acute pain to chronic settinghelliphelliprsquo bull Psychological pre-assessment bull Education discussion with patients surgeons bull In some cases preventive analgesia may be beneficial bull Transitional Pain Servicehelliptrackinghellipdatabase lsquoPragmatic approachrsquo lsquoAll diseases have an acute phasersquo lsquoDrugs good for acute pain must be good for chronic painrsquo

Pathophysiology lsquowhat is it about pain that causes more painrsquo
lsquohelliptransition to chronicityhelliprsquo
1 Nociceptive inflammation ischaemia oedema pressure traction
2 Neuropathic peripheral amp central sensitisation
spinal cord neuroplasticity
neuroma
3 Psychological amp social
4 Genetic
The neuropathic component in persistent pain after surgery
systematic review Haroutiunian PAIN 2013
CPSP after 11 types of surgery
bull Amount of pain depends
bull on likelihood of nerve damage
Neuropathic pain
bull in 65 of thoracotomy patients
bull 33 groin surgery
bull 6 knee surgery
Post surgical breast pain
Jung PAIN 2003
1 Intercostobrachial neuralgia
2 Other nerve injury
3 Neuroma
4 Phantom breast
Natural History
Long-term follow-up of breast cancer survivors with post-mastectomy pain syndrome
Macdonald et al British J of Cancer 2005
1996helliphellip 43 pain 3 years 2002 hellip21 pain 9 years
Persistent pain after breast surgery 6-year nationwide
follow up
Mejdahl Kehlet et al BMJ 2013
2008hellip47 pain 1 year
2013hellip37 pain 6 years
Treatment - prevention
helliphellipfrom Pre-emptive Analgesia (blocking preoperative stimuli)
helliphellipto Preventative Analgesia (blocking noxious stimuli central sensitisation across the entire perioperative period)
Preventative treatments
1 Nerve blocks Regional
2 Drugs
Regional anaesthesia to prevent chronic pain after surgery a Cochrane systematic review and meta-analysisdagger M H Andreae1 and D A Andreae2
BJA 2013
bull 23 RCTrsquos
bull Epidural anaesthesia and
paravertebral blocks may be effective
in preventing chronic pain at 1 year
bull Effective in about 1 in 4
patients treated
Preincisional Paravertebral Block Reduces the Prevalence of Chronic
Pain After Breast Surgery Kairaluoma et al Anesth Analg 2006103703-708
bull Preincisional paravertebral block provides significant immediate postoperative analgesia
bull In the same patients (n = 60) 12 months sig less pain in the PVB group
bull In addition to providing acute postoperative pain relief preoperative PVB reduces the prevalence of chronic pain 1 yr after breast cancer surgery
Epidurals Intraoperative epidural analgesia provides preventative analgesia in
abdominal surgery Lavandrsquohomme et al Anaesthesiology 2005
bull Clear benefit of epidural in preventing chronic pain 1 year
bull Intraoperative epidural better than postoperative epidural
bull Effective epidural better than effective parenteral only analgesia one year
Systematic review of therapeutic interventions to reduce chronic post surgical pain (32 RCTrsquos)
Humble et al European J of Pain (2015)
POSITIVE
Gabapentinoids
Lidocaine
iv lidocaine EMLA
Regional
TIVA
NEGATIVE
Ketamine
Cryoanalgesia
Local anaesthetic infiltration
Remifentanil (increased chronic pain)
1 Gabapentin around time of surgery
lsquono effect on chronic painrsquo
POSITIVE
NEGATIVE
Meta analysis (Clarke 2012) 48 RCTrsquos positive effect at 2 months
Cochrane Systematic Review (Chaparro 2013) 280 patients analysed pain at 6 months No effect
RCT Gabapentin 1200mg prior to Thyroidectomy Sig less pain at 3 months (Brogley 2008)
RCT Gabapentin vs Placebo Knee replacement No effect on chronic pain (Clarke 2014)
2 Pregabalin ndash around time of surgery lsquoNot a recommended treatment can cause post operative somnolencersquo
Positive
Negative
Meta-analysis of 3 studies (Clarke 2012) All showed improvement in pain 2 RCTrsquoshellipvery large decrease in CPSP (p=0007)
3 unpublished RCTrsquos from Pfizer (2010-2014) hellipall negative for acute and chronic pain i) 307 patients undergoing knee replacement ii) 501 patients hysterectomy iii) 425 patient hernia
Cochrane Systematic Review (Chaparro 2013) 25 RCTrsquos significant benefit
Systematic review (Martinez May 2017) No difference between pregabalin and placebo 3 months Use for acute pain in pro-nociceptive surgery Side effects a problem
Multimodal analgesia
bull Standard protocols now widely used eg Paravertebral blocks at MD Anderson bull Pre-assessment clinic screening for pain psychological factors pain catastrophising scale helliphellipgenetic screening tests bull Education patients surgeons anaesthetists nurses psychologists
General treatment strategies for chronic postsurgical neuropathic pain
Preventative Perkins amp Kehlet Anesthesiology 2000
bullSurgical procedure preservation
sentinel node biopsy
bullBetter postoperative pain management
bullInformed consent preparatory
information
Established Dworkin Archives Neurol 2003 60
1524
bull Amitriptyline
bull Gabapentin
bull Opioids
bull Tramadol
bull 5 Lidoderm patch EMLA
Positive therapies for Prevention of PSBP
1 EMLA applied to chest wall prior
to surgery less pain 3 months
Fassoulaki 2000
2 Venlafaxine XR 70mg before
and for 2 weeks post surgeryno diff
acute pain significantly less chronic
pain 6 months
Reuben 2004
3 Aggressive acute pain
management
Iohom 2006
4 Preincisional paravertebral
block
Kairaluoma 2006
5 Multimodal analgesia with
gabapentin EMLA ropivacaine less
acute pain amp pain 6 months
Fassoulaki 2005
A pain management programme for chronic cancer-
treatment-related pain Robb Williams Duvivier Newham
Journal of Pain 2006775-150
bull Theory of cancer-related pain
bull Pain pathways
bull Overunder activity cycle
bull Pacing
bull Exercise and fitness
bull TENS
bull Posture and manual handling
bull Relapse and prevention
Psychology interventions
bull Goal setting
bull Role of factors involved in pain
bull Homework assignments
bull Relaxation techniques
bull Cognitive skills
bull Relapse and prevention
Results
significant (plt005) improvements in
bull Pain severity
bull Psychological distress
bull Pain amp psychological coping indices
bull Activities of daily living
bull General fitness
Research Proposal
Exercise to prevent shoulder conditions in patients
undergoing breast cancer treatment
bull Aim to conduct a randomised controlled trial (RCT) supported with qualitative research to investigate the clinical and cost-effectiveness of early supervised exercise on outcomes of arm function chronic pain and quality of life at one year in women undergoing treatment for breast cancer
Intervention
bull A physiotherapy-led structured exercise programme incorporating behavioural strategies and monitoring to encourage adherence
bull A minimum of 4 face-to-face specialist treatment sessions with individual participants will be
delivered within 12 weeks of surgery bull Access to interim telephone support will be provided The programme will restrict to controlled early
stretching and ROM exercises with subsequent progression to maintain strength and function (weeks 2 to 12)
bull Qualitative interviews will be used during the feasibility phase of the trial to explore acceptability of
to the intervention
Outcomes
bull arm shoulder and hand function at 12 months using the 30-item Disability Arm Shoulder Hand (DASH) questionnaire
bull quality of life
bull Functional Assessment of Cancer Treatment-Breast (FACT-B)
bull Short-Form-12 and EQ-5D-5L
bull Data on postoperative adverse events surgical site infection and healthcare resource use will be collected at 6 and 12 months after surgery
Positive therapies for Prevention of PSBP
1 EMLA applied to chest wall prior
to surgery less pain 3 months
Fassoulaki 2000
2 Venlafaxine XR 70mg before
and for 2 weeks post surgeryno diff
acute pain significantly less chronic
pain 6 months
Reuben 2004
3 Aggressive acute pain
management
Iohom 2006
4 Preincisional paravertebral
block
Kairaluoma 2006
5 Multimodal analgesia with
gabapentin EMLA ropivacaine less
acute pain amp pain 6 months
Fassoulaki 2005
Current Treatment Paradigms
The Toronto General Hospital
Transitional Pain Service
development and implementation
of a multidisciplinary program
to prevent chronic postsurgical pain (Katz J Pain Res 2015)
bull Nurse navigator
bull Psychologists (ACT)
Clinical Manifestations hellipour approach to the patient with CPSP
bull Type of pain Cause
bull Exclude other causes (infection recurrence)
bull Psychological and social factors
bull Temporal Context
Electronic Patient Record
Future Directions
bull Identify Causative Modifiable risk factors vs Associative risk factors
bull Measure psychological variables
bull Genetic assays to identify genes controlling the variability in developing chronic pain
Aim is lsquoto identify susceptibility to chronic pain and sensitivity to analgesicsrsquo
Chronic pain lsquoheritabilityrsquo is variable
Conclusions
bull 1 year incidence = 05 -10 bull Avoid pain before during and after surgery lsquohelliphelliptranslate advances in acute pain to chronic settinghelliphelliprsquo bull Psychological pre-assessment bull Education discussion with patients surgeons bull In some cases preventive analgesia may be beneficial bull Transitional Pain Servicehelliptrackinghellipdatabase lsquoPragmatic approachrsquo lsquoAll diseases have an acute phasersquo lsquoDrugs good for acute pain must be good for chronic painrsquo

The neuropathic component in persistent pain after surgery
systematic review Haroutiunian PAIN 2013
CPSP after 11 types of surgery
bull Amount of pain depends
bull on likelihood of nerve damage
Neuropathic pain
bull in 65 of thoracotomy patients
bull 33 groin surgery
bull 6 knee surgery
Post surgical breast pain
Jung PAIN 2003
1 Intercostobrachial neuralgia
2 Other nerve injury
3 Neuroma
4 Phantom breast
Natural History
Long-term follow-up of breast cancer survivors with post-mastectomy pain syndrome
Macdonald et al British J of Cancer 2005
1996helliphellip 43 pain 3 years 2002 hellip21 pain 9 years
Persistent pain after breast surgery 6-year nationwide
follow up
Mejdahl Kehlet et al BMJ 2013
2008hellip47 pain 1 year
2013hellip37 pain 6 years
Treatment - prevention
helliphellipfrom Pre-emptive Analgesia (blocking preoperative stimuli)
helliphellipto Preventative Analgesia (blocking noxious stimuli central sensitisation across the entire perioperative period)
Preventative treatments
1 Nerve blocks Regional
2 Drugs
Regional anaesthesia to prevent chronic pain after surgery a Cochrane systematic review and meta-analysisdagger M H Andreae1 and D A Andreae2
BJA 2013
bull 23 RCTrsquos
bull Epidural anaesthesia and
paravertebral blocks may be effective
in preventing chronic pain at 1 year
bull Effective in about 1 in 4
patients treated
Preincisional Paravertebral Block Reduces the Prevalence of Chronic
Pain After Breast Surgery Kairaluoma et al Anesth Analg 2006103703-708
bull Preincisional paravertebral block provides significant immediate postoperative analgesia
bull In the same patients (n = 60) 12 months sig less pain in the PVB group
bull In addition to providing acute postoperative pain relief preoperative PVB reduces the prevalence of chronic pain 1 yr after breast cancer surgery
Epidurals Intraoperative epidural analgesia provides preventative analgesia in
abdominal surgery Lavandrsquohomme et al Anaesthesiology 2005
bull Clear benefit of epidural in preventing chronic pain 1 year
bull Intraoperative epidural better than postoperative epidural
bull Effective epidural better than effective parenteral only analgesia one year
Systematic review of therapeutic interventions to reduce chronic post surgical pain (32 RCTrsquos)
Humble et al European J of Pain (2015)
POSITIVE
Gabapentinoids
Lidocaine
iv lidocaine EMLA
Regional
TIVA
NEGATIVE
Ketamine
Cryoanalgesia
Local anaesthetic infiltration
Remifentanil (increased chronic pain)
1 Gabapentin around time of surgery
lsquono effect on chronic painrsquo
POSITIVE
NEGATIVE
Meta analysis (Clarke 2012) 48 RCTrsquos positive effect at 2 months
Cochrane Systematic Review (Chaparro 2013) 280 patients analysed pain at 6 months No effect
RCT Gabapentin 1200mg prior to Thyroidectomy Sig less pain at 3 months (Brogley 2008)
RCT Gabapentin vs Placebo Knee replacement No effect on chronic pain (Clarke 2014)
2 Pregabalin ndash around time of surgery lsquoNot a recommended treatment can cause post operative somnolencersquo
Positive
Negative
Meta-analysis of 3 studies (Clarke 2012) All showed improvement in pain 2 RCTrsquoshellipvery large decrease in CPSP (p=0007)
3 unpublished RCTrsquos from Pfizer (2010-2014) hellipall negative for acute and chronic pain i) 307 patients undergoing knee replacement ii) 501 patients hysterectomy iii) 425 patient hernia
Cochrane Systematic Review (Chaparro 2013) 25 RCTrsquos significant benefit
Systematic review (Martinez May 2017) No difference between pregabalin and placebo 3 months Use for acute pain in pro-nociceptive surgery Side effects a problem
Multimodal analgesia
bull Standard protocols now widely used eg Paravertebral blocks at MD Anderson bull Pre-assessment clinic screening for pain psychological factors pain catastrophising scale helliphellipgenetic screening tests bull Education patients surgeons anaesthetists nurses psychologists
General treatment strategies for chronic postsurgical neuropathic pain
Preventative Perkins amp Kehlet Anesthesiology 2000
bullSurgical procedure preservation
sentinel node biopsy
bullBetter postoperative pain management
bullInformed consent preparatory
information
Established Dworkin Archives Neurol 2003 60
1524
bull Amitriptyline
bull Gabapentin
bull Opioids
bull Tramadol
bull 5 Lidoderm patch EMLA
Positive therapies for Prevention of PSBP
1 EMLA applied to chest wall prior
to surgery less pain 3 months
Fassoulaki 2000
2 Venlafaxine XR 70mg before
and for 2 weeks post surgeryno diff
acute pain significantly less chronic
pain 6 months
Reuben 2004
3 Aggressive acute pain
management
Iohom 2006
4 Preincisional paravertebral
block
Kairaluoma 2006
5 Multimodal analgesia with
gabapentin EMLA ropivacaine less
acute pain amp pain 6 months
Fassoulaki 2005
A pain management programme for chronic cancer-
treatment-related pain Robb Williams Duvivier Newham
Journal of Pain 2006775-150
bull Theory of cancer-related pain
bull Pain pathways
bull Overunder activity cycle
bull Pacing
bull Exercise and fitness
bull TENS
bull Posture and manual handling
bull Relapse and prevention
Psychology interventions
bull Goal setting
bull Role of factors involved in pain
bull Homework assignments
bull Relaxation techniques
bull Cognitive skills
bull Relapse and prevention
Results
significant (plt005) improvements in
bull Pain severity
bull Psychological distress
bull Pain amp psychological coping indices
bull Activities of daily living
bull General fitness
Research Proposal
Exercise to prevent shoulder conditions in patients
undergoing breast cancer treatment
bull Aim to conduct a randomised controlled trial (RCT) supported with qualitative research to investigate the clinical and cost-effectiveness of early supervised exercise on outcomes of arm function chronic pain and quality of life at one year in women undergoing treatment for breast cancer
Intervention
bull A physiotherapy-led structured exercise programme incorporating behavioural strategies and monitoring to encourage adherence
bull A minimum of 4 face-to-face specialist treatment sessions with individual participants will be
delivered within 12 weeks of surgery bull Access to interim telephone support will be provided The programme will restrict to controlled early
stretching and ROM exercises with subsequent progression to maintain strength and function (weeks 2 to 12)
bull Qualitative interviews will be used during the feasibility phase of the trial to explore acceptability of
to the intervention
Outcomes
bull arm shoulder and hand function at 12 months using the 30-item Disability Arm Shoulder Hand (DASH) questionnaire
bull quality of life
bull Functional Assessment of Cancer Treatment-Breast (FACT-B)
bull Short-Form-12 and EQ-5D-5L
bull Data on postoperative adverse events surgical site infection and healthcare resource use will be collected at 6 and 12 months after surgery
Positive therapies for Prevention of PSBP
1 EMLA applied to chest wall prior
to surgery less pain 3 months
Fassoulaki 2000
2 Venlafaxine XR 70mg before
and for 2 weeks post surgeryno diff
acute pain significantly less chronic
pain 6 months
Reuben 2004
3 Aggressive acute pain
management
Iohom 2006
4 Preincisional paravertebral
block
Kairaluoma 2006
5 Multimodal analgesia with
gabapentin EMLA ropivacaine less
acute pain amp pain 6 months
Fassoulaki 2005
Current Treatment Paradigms
The Toronto General Hospital
Transitional Pain Service
development and implementation
of a multidisciplinary program
to prevent chronic postsurgical pain (Katz J Pain Res 2015)
bull Nurse navigator
bull Psychologists (ACT)
Clinical Manifestations hellipour approach to the patient with CPSP
bull Type of pain Cause
bull Exclude other causes (infection recurrence)
bull Psychological and social factors
bull Temporal Context
Electronic Patient Record
Future Directions
bull Identify Causative Modifiable risk factors vs Associative risk factors
bull Measure psychological variables
bull Genetic assays to identify genes controlling the variability in developing chronic pain
Aim is lsquoto identify susceptibility to chronic pain and sensitivity to analgesicsrsquo
Chronic pain lsquoheritabilityrsquo is variable
Conclusions
bull 1 year incidence = 05 -10 bull Avoid pain before during and after surgery lsquohelliphelliptranslate advances in acute pain to chronic settinghelliphelliprsquo bull Psychological pre-assessment bull Education discussion with patients surgeons bull In some cases preventive analgesia may be beneficial bull Transitional Pain Servicehelliptrackinghellipdatabase lsquoPragmatic approachrsquo lsquoAll diseases have an acute phasersquo lsquoDrugs good for acute pain must be good for chronic painrsquo

Post surgical breast pain
Jung PAIN 2003
1 Intercostobrachial neuralgia
2 Other nerve injury
3 Neuroma
4 Phantom breast
Natural History
Long-term follow-up of breast cancer survivors with post-mastectomy pain syndrome
Macdonald et al British J of Cancer 2005
1996helliphellip 43 pain 3 years 2002 hellip21 pain 9 years
Persistent pain after breast surgery 6-year nationwide
follow up
Mejdahl Kehlet et al BMJ 2013
2008hellip47 pain 1 year
2013hellip37 pain 6 years
Treatment - prevention
helliphellipfrom Pre-emptive Analgesia (blocking preoperative stimuli)
helliphellipto Preventative Analgesia (blocking noxious stimuli central sensitisation across the entire perioperative period)
Preventative treatments
1 Nerve blocks Regional
2 Drugs
Regional anaesthesia to prevent chronic pain after surgery a Cochrane systematic review and meta-analysisdagger M H Andreae1 and D A Andreae2
BJA 2013
bull 23 RCTrsquos
bull Epidural anaesthesia and
paravertebral blocks may be effective
in preventing chronic pain at 1 year
bull Effective in about 1 in 4
patients treated
Preincisional Paravertebral Block Reduces the Prevalence of Chronic
Pain After Breast Surgery Kairaluoma et al Anesth Analg 2006103703-708
bull Preincisional paravertebral block provides significant immediate postoperative analgesia
bull In the same patients (n = 60) 12 months sig less pain in the PVB group
bull In addition to providing acute postoperative pain relief preoperative PVB reduces the prevalence of chronic pain 1 yr after breast cancer surgery
Epidurals Intraoperative epidural analgesia provides preventative analgesia in
abdominal surgery Lavandrsquohomme et al Anaesthesiology 2005
bull Clear benefit of epidural in preventing chronic pain 1 year
bull Intraoperative epidural better than postoperative epidural
bull Effective epidural better than effective parenteral only analgesia one year
Systematic review of therapeutic interventions to reduce chronic post surgical pain (32 RCTrsquos)
Humble et al European J of Pain (2015)
POSITIVE
Gabapentinoids
Lidocaine
iv lidocaine EMLA
Regional
TIVA
NEGATIVE
Ketamine
Cryoanalgesia
Local anaesthetic infiltration
Remifentanil (increased chronic pain)
1 Gabapentin around time of surgery
lsquono effect on chronic painrsquo
POSITIVE
NEGATIVE
Meta analysis (Clarke 2012) 48 RCTrsquos positive effect at 2 months
Cochrane Systematic Review (Chaparro 2013) 280 patients analysed pain at 6 months No effect
RCT Gabapentin 1200mg prior to Thyroidectomy Sig less pain at 3 months (Brogley 2008)
RCT Gabapentin vs Placebo Knee replacement No effect on chronic pain (Clarke 2014)
2 Pregabalin ndash around time of surgery lsquoNot a recommended treatment can cause post operative somnolencersquo
Positive
Negative
Meta-analysis of 3 studies (Clarke 2012) All showed improvement in pain 2 RCTrsquoshellipvery large decrease in CPSP (p=0007)
3 unpublished RCTrsquos from Pfizer (2010-2014) hellipall negative for acute and chronic pain i) 307 patients undergoing knee replacement ii) 501 patients hysterectomy iii) 425 patient hernia
Cochrane Systematic Review (Chaparro 2013) 25 RCTrsquos significant benefit
Systematic review (Martinez May 2017) No difference between pregabalin and placebo 3 months Use for acute pain in pro-nociceptive surgery Side effects a problem
Multimodal analgesia
bull Standard protocols now widely used eg Paravertebral blocks at MD Anderson bull Pre-assessment clinic screening for pain psychological factors pain catastrophising scale helliphellipgenetic screening tests bull Education patients surgeons anaesthetists nurses psychologists
General treatment strategies for chronic postsurgical neuropathic pain
Preventative Perkins amp Kehlet Anesthesiology 2000
bullSurgical procedure preservation
sentinel node biopsy
bullBetter postoperative pain management
bullInformed consent preparatory
information
Established Dworkin Archives Neurol 2003 60
1524
bull Amitriptyline
bull Gabapentin
bull Opioids
bull Tramadol
bull 5 Lidoderm patch EMLA
Positive therapies for Prevention of PSBP
1 EMLA applied to chest wall prior
to surgery less pain 3 months
Fassoulaki 2000
2 Venlafaxine XR 70mg before
and for 2 weeks post surgeryno diff
acute pain significantly less chronic
pain 6 months
Reuben 2004
3 Aggressive acute pain
management
Iohom 2006
4 Preincisional paravertebral
block
Kairaluoma 2006
5 Multimodal analgesia with
gabapentin EMLA ropivacaine less
acute pain amp pain 6 months
Fassoulaki 2005
A pain management programme for chronic cancer-
treatment-related pain Robb Williams Duvivier Newham
Journal of Pain 2006775-150
bull Theory of cancer-related pain
bull Pain pathways
bull Overunder activity cycle
bull Pacing
bull Exercise and fitness
bull TENS
bull Posture and manual handling
bull Relapse and prevention
Psychology interventions
bull Goal setting
bull Role of factors involved in pain
bull Homework assignments
bull Relaxation techniques
bull Cognitive skills
bull Relapse and prevention
Results
significant (plt005) improvements in
bull Pain severity
bull Psychological distress
bull Pain amp psychological coping indices
bull Activities of daily living
bull General fitness
Research Proposal
Exercise to prevent shoulder conditions in patients
undergoing breast cancer treatment
bull Aim to conduct a randomised controlled trial (RCT) supported with qualitative research to investigate the clinical and cost-effectiveness of early supervised exercise on outcomes of arm function chronic pain and quality of life at one year in women undergoing treatment for breast cancer
Intervention
bull A physiotherapy-led structured exercise programme incorporating behavioural strategies and monitoring to encourage adherence
bull A minimum of 4 face-to-face specialist treatment sessions with individual participants will be
delivered within 12 weeks of surgery bull Access to interim telephone support will be provided The programme will restrict to controlled early
stretching and ROM exercises with subsequent progression to maintain strength and function (weeks 2 to 12)
bull Qualitative interviews will be used during the feasibility phase of the trial to explore acceptability of
to the intervention
Outcomes
bull arm shoulder and hand function at 12 months using the 30-item Disability Arm Shoulder Hand (DASH) questionnaire
bull quality of life
bull Functional Assessment of Cancer Treatment-Breast (FACT-B)
bull Short-Form-12 and EQ-5D-5L
bull Data on postoperative adverse events surgical site infection and healthcare resource use will be collected at 6 and 12 months after surgery
Positive therapies for Prevention of PSBP
1 EMLA applied to chest wall prior
to surgery less pain 3 months
Fassoulaki 2000
2 Venlafaxine XR 70mg before
and for 2 weeks post surgeryno diff
acute pain significantly less chronic
pain 6 months
Reuben 2004
3 Aggressive acute pain
management
Iohom 2006
4 Preincisional paravertebral
block
Kairaluoma 2006
5 Multimodal analgesia with
gabapentin EMLA ropivacaine less
acute pain amp pain 6 months
Fassoulaki 2005
Current Treatment Paradigms
The Toronto General Hospital
Transitional Pain Service
development and implementation
of a multidisciplinary program
to prevent chronic postsurgical pain (Katz J Pain Res 2015)
bull Nurse navigator
bull Psychologists (ACT)
Clinical Manifestations hellipour approach to the patient with CPSP
bull Type of pain Cause
bull Exclude other causes (infection recurrence)
bull Psychological and social factors
bull Temporal Context
Electronic Patient Record
Future Directions
bull Identify Causative Modifiable risk factors vs Associative risk factors
bull Measure psychological variables
bull Genetic assays to identify genes controlling the variability in developing chronic pain
Aim is lsquoto identify susceptibility to chronic pain and sensitivity to analgesicsrsquo
Chronic pain lsquoheritabilityrsquo is variable
Conclusions
bull 1 year incidence = 05 -10 bull Avoid pain before during and after surgery lsquohelliphelliptranslate advances in acute pain to chronic settinghelliphelliprsquo bull Psychological pre-assessment bull Education discussion with patients surgeons bull In some cases preventive analgesia may be beneficial bull Transitional Pain Servicehelliptrackinghellipdatabase lsquoPragmatic approachrsquo lsquoAll diseases have an acute phasersquo lsquoDrugs good for acute pain must be good for chronic painrsquo

Natural History
Long-term follow-up of breast cancer survivors with post-mastectomy pain syndrome
Macdonald et al British J of Cancer 2005
1996helliphellip 43 pain 3 years 2002 hellip21 pain 9 years
Persistent pain after breast surgery 6-year nationwide
follow up
Mejdahl Kehlet et al BMJ 2013
2008hellip47 pain 1 year
2013hellip37 pain 6 years
Treatment - prevention
helliphellipfrom Pre-emptive Analgesia (blocking preoperative stimuli)
helliphellipto Preventative Analgesia (blocking noxious stimuli central sensitisation across the entire perioperative period)
Preventative treatments
1 Nerve blocks Regional
2 Drugs
Regional anaesthesia to prevent chronic pain after surgery a Cochrane systematic review and meta-analysisdagger M H Andreae1 and D A Andreae2
BJA 2013
bull 23 RCTrsquos
bull Epidural anaesthesia and
paravertebral blocks may be effective
in preventing chronic pain at 1 year
bull Effective in about 1 in 4
patients treated
Preincisional Paravertebral Block Reduces the Prevalence of Chronic
Pain After Breast Surgery Kairaluoma et al Anesth Analg 2006103703-708
bull Preincisional paravertebral block provides significant immediate postoperative analgesia
bull In the same patients (n = 60) 12 months sig less pain in the PVB group
bull In addition to providing acute postoperative pain relief preoperative PVB reduces the prevalence of chronic pain 1 yr after breast cancer surgery
Epidurals Intraoperative epidural analgesia provides preventative analgesia in
abdominal surgery Lavandrsquohomme et al Anaesthesiology 2005
bull Clear benefit of epidural in preventing chronic pain 1 year
bull Intraoperative epidural better than postoperative epidural
bull Effective epidural better than effective parenteral only analgesia one year
Systematic review of therapeutic interventions to reduce chronic post surgical pain (32 RCTrsquos)
Humble et al European J of Pain (2015)
POSITIVE
Gabapentinoids
Lidocaine
iv lidocaine EMLA
Regional
TIVA
NEGATIVE
Ketamine
Cryoanalgesia
Local anaesthetic infiltration
Remifentanil (increased chronic pain)
1 Gabapentin around time of surgery
lsquono effect on chronic painrsquo
POSITIVE
NEGATIVE
Meta analysis (Clarke 2012) 48 RCTrsquos positive effect at 2 months
Cochrane Systematic Review (Chaparro 2013) 280 patients analysed pain at 6 months No effect
RCT Gabapentin 1200mg prior to Thyroidectomy Sig less pain at 3 months (Brogley 2008)
RCT Gabapentin vs Placebo Knee replacement No effect on chronic pain (Clarke 2014)
2 Pregabalin ndash around time of surgery lsquoNot a recommended treatment can cause post operative somnolencersquo
Positive
Negative
Meta-analysis of 3 studies (Clarke 2012) All showed improvement in pain 2 RCTrsquoshellipvery large decrease in CPSP (p=0007)
3 unpublished RCTrsquos from Pfizer (2010-2014) hellipall negative for acute and chronic pain i) 307 patients undergoing knee replacement ii) 501 patients hysterectomy iii) 425 patient hernia
Cochrane Systematic Review (Chaparro 2013) 25 RCTrsquos significant benefit
Systematic review (Martinez May 2017) No difference between pregabalin and placebo 3 months Use for acute pain in pro-nociceptive surgery Side effects a problem
Multimodal analgesia
bull Standard protocols now widely used eg Paravertebral blocks at MD Anderson bull Pre-assessment clinic screening for pain psychological factors pain catastrophising scale helliphellipgenetic screening tests bull Education patients surgeons anaesthetists nurses psychologists
General treatment strategies for chronic postsurgical neuropathic pain
Preventative Perkins amp Kehlet Anesthesiology 2000
bullSurgical procedure preservation
sentinel node biopsy
bullBetter postoperative pain management
bullInformed consent preparatory
information
Established Dworkin Archives Neurol 2003 60
1524
bull Amitriptyline
bull Gabapentin
bull Opioids
bull Tramadol
bull 5 Lidoderm patch EMLA
Positive therapies for Prevention of PSBP
1 EMLA applied to chest wall prior
to surgery less pain 3 months
Fassoulaki 2000
2 Venlafaxine XR 70mg before
and for 2 weeks post surgeryno diff
acute pain significantly less chronic
pain 6 months
Reuben 2004
3 Aggressive acute pain
management
Iohom 2006
4 Preincisional paravertebral
block
Kairaluoma 2006
5 Multimodal analgesia with
gabapentin EMLA ropivacaine less
acute pain amp pain 6 months
Fassoulaki 2005
A pain management programme for chronic cancer-
treatment-related pain Robb Williams Duvivier Newham
Journal of Pain 2006775-150
bull Theory of cancer-related pain
bull Pain pathways
bull Overunder activity cycle
bull Pacing
bull Exercise and fitness
bull TENS
bull Posture and manual handling
bull Relapse and prevention
Psychology interventions
bull Goal setting
bull Role of factors involved in pain
bull Homework assignments
bull Relaxation techniques
bull Cognitive skills
bull Relapse and prevention
Results
significant (plt005) improvements in
bull Pain severity
bull Psychological distress
bull Pain amp psychological coping indices
bull Activities of daily living
bull General fitness
Research Proposal
Exercise to prevent shoulder conditions in patients
undergoing breast cancer treatment
bull Aim to conduct a randomised controlled trial (RCT) supported with qualitative research to investigate the clinical and cost-effectiveness of early supervised exercise on outcomes of arm function chronic pain and quality of life at one year in women undergoing treatment for breast cancer
Intervention
bull A physiotherapy-led structured exercise programme incorporating behavioural strategies and monitoring to encourage adherence
bull A minimum of 4 face-to-face specialist treatment sessions with individual participants will be
delivered within 12 weeks of surgery bull Access to interim telephone support will be provided The programme will restrict to controlled early
stretching and ROM exercises with subsequent progression to maintain strength and function (weeks 2 to 12)
bull Qualitative interviews will be used during the feasibility phase of the trial to explore acceptability of
to the intervention
Outcomes
bull arm shoulder and hand function at 12 months using the 30-item Disability Arm Shoulder Hand (DASH) questionnaire
bull quality of life
bull Functional Assessment of Cancer Treatment-Breast (FACT-B)
bull Short-Form-12 and EQ-5D-5L
bull Data on postoperative adverse events surgical site infection and healthcare resource use will be collected at 6 and 12 months after surgery
Positive therapies for Prevention of PSBP
1 EMLA applied to chest wall prior
to surgery less pain 3 months
Fassoulaki 2000
2 Venlafaxine XR 70mg before
and for 2 weeks post surgeryno diff
acute pain significantly less chronic
pain 6 months
Reuben 2004
3 Aggressive acute pain
management
Iohom 2006
4 Preincisional paravertebral
block
Kairaluoma 2006
5 Multimodal analgesia with
gabapentin EMLA ropivacaine less
acute pain amp pain 6 months
Fassoulaki 2005
Current Treatment Paradigms
The Toronto General Hospital
Transitional Pain Service
development and implementation
of a multidisciplinary program
to prevent chronic postsurgical pain (Katz J Pain Res 2015)
bull Nurse navigator
bull Psychologists (ACT)
Clinical Manifestations hellipour approach to the patient with CPSP
bull Type of pain Cause
bull Exclude other causes (infection recurrence)
bull Psychological and social factors
bull Temporal Context
Electronic Patient Record
Future Directions
bull Identify Causative Modifiable risk factors vs Associative risk factors
bull Measure psychological variables
bull Genetic assays to identify genes controlling the variability in developing chronic pain
Aim is lsquoto identify susceptibility to chronic pain and sensitivity to analgesicsrsquo
Chronic pain lsquoheritabilityrsquo is variable
Conclusions
bull 1 year incidence = 05 -10 bull Avoid pain before during and after surgery lsquohelliphelliptranslate advances in acute pain to chronic settinghelliphelliprsquo bull Psychological pre-assessment bull Education discussion with patients surgeons bull In some cases preventive analgesia may be beneficial bull Transitional Pain Servicehelliptrackinghellipdatabase lsquoPragmatic approachrsquo lsquoAll diseases have an acute phasersquo lsquoDrugs good for acute pain must be good for chronic painrsquo

Treatment - prevention
helliphellipfrom Pre-emptive Analgesia (blocking preoperative stimuli)
helliphellipto Preventative Analgesia (blocking noxious stimuli central sensitisation across the entire perioperative period)
Preventative treatments
1 Nerve blocks Regional
2 Drugs
Regional anaesthesia to prevent chronic pain after surgery a Cochrane systematic review and meta-analysisdagger M H Andreae1 and D A Andreae2
BJA 2013
bull 23 RCTrsquos
bull Epidural anaesthesia and
paravertebral blocks may be effective
in preventing chronic pain at 1 year
bull Effective in about 1 in 4
patients treated
Preincisional Paravertebral Block Reduces the Prevalence of Chronic
Pain After Breast Surgery Kairaluoma et al Anesth Analg 2006103703-708
bull Preincisional paravertebral block provides significant immediate postoperative analgesia
bull In the same patients (n = 60) 12 months sig less pain in the PVB group
bull In addition to providing acute postoperative pain relief preoperative PVB reduces the prevalence of chronic pain 1 yr after breast cancer surgery
Epidurals Intraoperative epidural analgesia provides preventative analgesia in
abdominal surgery Lavandrsquohomme et al Anaesthesiology 2005
bull Clear benefit of epidural in preventing chronic pain 1 year
bull Intraoperative epidural better than postoperative epidural
bull Effective epidural better than effective parenteral only analgesia one year
Systematic review of therapeutic interventions to reduce chronic post surgical pain (32 RCTrsquos)
Humble et al European J of Pain (2015)
POSITIVE
Gabapentinoids
Lidocaine
iv lidocaine EMLA
Regional
TIVA
NEGATIVE
Ketamine
Cryoanalgesia
Local anaesthetic infiltration
Remifentanil (increased chronic pain)
1 Gabapentin around time of surgery
lsquono effect on chronic painrsquo
POSITIVE
NEGATIVE
Meta analysis (Clarke 2012) 48 RCTrsquos positive effect at 2 months
Cochrane Systematic Review (Chaparro 2013) 280 patients analysed pain at 6 months No effect
RCT Gabapentin 1200mg prior to Thyroidectomy Sig less pain at 3 months (Brogley 2008)
RCT Gabapentin vs Placebo Knee replacement No effect on chronic pain (Clarke 2014)
2 Pregabalin ndash around time of surgery lsquoNot a recommended treatment can cause post operative somnolencersquo
Positive
Negative
Meta-analysis of 3 studies (Clarke 2012) All showed improvement in pain 2 RCTrsquoshellipvery large decrease in CPSP (p=0007)
3 unpublished RCTrsquos from Pfizer (2010-2014) hellipall negative for acute and chronic pain i) 307 patients undergoing knee replacement ii) 501 patients hysterectomy iii) 425 patient hernia
Cochrane Systematic Review (Chaparro 2013) 25 RCTrsquos significant benefit
Systematic review (Martinez May 2017) No difference between pregabalin and placebo 3 months Use for acute pain in pro-nociceptive surgery Side effects a problem
Multimodal analgesia
bull Standard protocols now widely used eg Paravertebral blocks at MD Anderson bull Pre-assessment clinic screening for pain psychological factors pain catastrophising scale helliphellipgenetic screening tests bull Education patients surgeons anaesthetists nurses psychologists
General treatment strategies for chronic postsurgical neuropathic pain
Preventative Perkins amp Kehlet Anesthesiology 2000
bullSurgical procedure preservation
sentinel node biopsy
bullBetter postoperative pain management
bullInformed consent preparatory
information
Established Dworkin Archives Neurol 2003 60
1524
bull Amitriptyline
bull Gabapentin
bull Opioids
bull Tramadol
bull 5 Lidoderm patch EMLA
Positive therapies for Prevention of PSBP
1 EMLA applied to chest wall prior
to surgery less pain 3 months
Fassoulaki 2000
2 Venlafaxine XR 70mg before
and for 2 weeks post surgeryno diff
acute pain significantly less chronic
pain 6 months
Reuben 2004
3 Aggressive acute pain
management
Iohom 2006
4 Preincisional paravertebral
block
Kairaluoma 2006
5 Multimodal analgesia with
gabapentin EMLA ropivacaine less
acute pain amp pain 6 months
Fassoulaki 2005
A pain management programme for chronic cancer-
treatment-related pain Robb Williams Duvivier Newham
Journal of Pain 2006775-150
bull Theory of cancer-related pain
bull Pain pathways
bull Overunder activity cycle
bull Pacing
bull Exercise and fitness
bull TENS
bull Posture and manual handling
bull Relapse and prevention
Psychology interventions
bull Goal setting
bull Role of factors involved in pain
bull Homework assignments
bull Relaxation techniques
bull Cognitive skills
bull Relapse and prevention
Results
significant (plt005) improvements in
bull Pain severity
bull Psychological distress
bull Pain amp psychological coping indices
bull Activities of daily living
bull General fitness
Research Proposal
Exercise to prevent shoulder conditions in patients
undergoing breast cancer treatment
bull Aim to conduct a randomised controlled trial (RCT) supported with qualitative research to investigate the clinical and cost-effectiveness of early supervised exercise on outcomes of arm function chronic pain and quality of life at one year in women undergoing treatment for breast cancer
Intervention
bull A physiotherapy-led structured exercise programme incorporating behavioural strategies and monitoring to encourage adherence
bull A minimum of 4 face-to-face specialist treatment sessions with individual participants will be
delivered within 12 weeks of surgery bull Access to interim telephone support will be provided The programme will restrict to controlled early
stretching and ROM exercises with subsequent progression to maintain strength and function (weeks 2 to 12)
bull Qualitative interviews will be used during the feasibility phase of the trial to explore acceptability of
to the intervention
Outcomes
bull arm shoulder and hand function at 12 months using the 30-item Disability Arm Shoulder Hand (DASH) questionnaire
bull quality of life
bull Functional Assessment of Cancer Treatment-Breast (FACT-B)
bull Short-Form-12 and EQ-5D-5L
bull Data on postoperative adverse events surgical site infection and healthcare resource use will be collected at 6 and 12 months after surgery
Positive therapies for Prevention of PSBP
1 EMLA applied to chest wall prior
to surgery less pain 3 months
Fassoulaki 2000
2 Venlafaxine XR 70mg before
and for 2 weeks post surgeryno diff
acute pain significantly less chronic
pain 6 months
Reuben 2004
3 Aggressive acute pain
management
Iohom 2006
4 Preincisional paravertebral
block
Kairaluoma 2006
5 Multimodal analgesia with
gabapentin EMLA ropivacaine less
acute pain amp pain 6 months
Fassoulaki 2005
Current Treatment Paradigms
The Toronto General Hospital
Transitional Pain Service
development and implementation
of a multidisciplinary program
to prevent chronic postsurgical pain (Katz J Pain Res 2015)
bull Nurse navigator
bull Psychologists (ACT)
Clinical Manifestations hellipour approach to the patient with CPSP
bull Type of pain Cause
bull Exclude other causes (infection recurrence)
bull Psychological and social factors
bull Temporal Context
Electronic Patient Record
Future Directions
bull Identify Causative Modifiable risk factors vs Associative risk factors
bull Measure psychological variables
bull Genetic assays to identify genes controlling the variability in developing chronic pain
Aim is lsquoto identify susceptibility to chronic pain and sensitivity to analgesicsrsquo
Chronic pain lsquoheritabilityrsquo is variable
Conclusions
bull 1 year incidence = 05 -10 bull Avoid pain before during and after surgery lsquohelliphelliptranslate advances in acute pain to chronic settinghelliphelliprsquo bull Psychological pre-assessment bull Education discussion with patients surgeons bull In some cases preventive analgesia may be beneficial bull Transitional Pain Servicehelliptrackinghellipdatabase lsquoPragmatic approachrsquo lsquoAll diseases have an acute phasersquo lsquoDrugs good for acute pain must be good for chronic painrsquo

Preventative treatments
1 Nerve blocks Regional
2 Drugs
Regional anaesthesia to prevent chronic pain after surgery a Cochrane systematic review and meta-analysisdagger M H Andreae1 and D A Andreae2
BJA 2013
bull 23 RCTrsquos
bull Epidural anaesthesia and
paravertebral blocks may be effective
in preventing chronic pain at 1 year
bull Effective in about 1 in 4
patients treated
Preincisional Paravertebral Block Reduces the Prevalence of Chronic
Pain After Breast Surgery Kairaluoma et al Anesth Analg 2006103703-708
bull Preincisional paravertebral block provides significant immediate postoperative analgesia
bull In the same patients (n = 60) 12 months sig less pain in the PVB group
bull In addition to providing acute postoperative pain relief preoperative PVB reduces the prevalence of chronic pain 1 yr after breast cancer surgery
Epidurals Intraoperative epidural analgesia provides preventative analgesia in
abdominal surgery Lavandrsquohomme et al Anaesthesiology 2005
bull Clear benefit of epidural in preventing chronic pain 1 year
bull Intraoperative epidural better than postoperative epidural
bull Effective epidural better than effective parenteral only analgesia one year
Systematic review of therapeutic interventions to reduce chronic post surgical pain (32 RCTrsquos)
Humble et al European J of Pain (2015)
POSITIVE
Gabapentinoids
Lidocaine
iv lidocaine EMLA
Regional
TIVA
NEGATIVE
Ketamine
Cryoanalgesia
Local anaesthetic infiltration
Remifentanil (increased chronic pain)
1 Gabapentin around time of surgery
lsquono effect on chronic painrsquo
POSITIVE
NEGATIVE
Meta analysis (Clarke 2012) 48 RCTrsquos positive effect at 2 months
Cochrane Systematic Review (Chaparro 2013) 280 patients analysed pain at 6 months No effect
RCT Gabapentin 1200mg prior to Thyroidectomy Sig less pain at 3 months (Brogley 2008)
RCT Gabapentin vs Placebo Knee replacement No effect on chronic pain (Clarke 2014)
2 Pregabalin ndash around time of surgery lsquoNot a recommended treatment can cause post operative somnolencersquo
Positive
Negative
Meta-analysis of 3 studies (Clarke 2012) All showed improvement in pain 2 RCTrsquoshellipvery large decrease in CPSP (p=0007)
3 unpublished RCTrsquos from Pfizer (2010-2014) hellipall negative for acute and chronic pain i) 307 patients undergoing knee replacement ii) 501 patients hysterectomy iii) 425 patient hernia
Cochrane Systematic Review (Chaparro 2013) 25 RCTrsquos significant benefit
Systematic review (Martinez May 2017) No difference between pregabalin and placebo 3 months Use for acute pain in pro-nociceptive surgery Side effects a problem
Multimodal analgesia
bull Standard protocols now widely used eg Paravertebral blocks at MD Anderson bull Pre-assessment clinic screening for pain psychological factors pain catastrophising scale helliphellipgenetic screening tests bull Education patients surgeons anaesthetists nurses psychologists
General treatment strategies for chronic postsurgical neuropathic pain
Preventative Perkins amp Kehlet Anesthesiology 2000
bullSurgical procedure preservation
sentinel node biopsy
bullBetter postoperative pain management
bullInformed consent preparatory
information
Established Dworkin Archives Neurol 2003 60
1524
bull Amitriptyline
bull Gabapentin
bull Opioids
bull Tramadol
bull 5 Lidoderm patch EMLA
Positive therapies for Prevention of PSBP
1 EMLA applied to chest wall prior
to surgery less pain 3 months
Fassoulaki 2000
2 Venlafaxine XR 70mg before
and for 2 weeks post surgeryno diff
acute pain significantly less chronic
pain 6 months
Reuben 2004
3 Aggressive acute pain
management
Iohom 2006
4 Preincisional paravertebral
block
Kairaluoma 2006
5 Multimodal analgesia with
gabapentin EMLA ropivacaine less
acute pain amp pain 6 months
Fassoulaki 2005
A pain management programme for chronic cancer-
treatment-related pain Robb Williams Duvivier Newham
Journal of Pain 2006775-150
bull Theory of cancer-related pain
bull Pain pathways
bull Overunder activity cycle
bull Pacing
bull Exercise and fitness
bull TENS
bull Posture and manual handling
bull Relapse and prevention
Psychology interventions
bull Goal setting
bull Role of factors involved in pain
bull Homework assignments
bull Relaxation techniques
bull Cognitive skills
bull Relapse and prevention
Results
significant (plt005) improvements in
bull Pain severity
bull Psychological distress
bull Pain amp psychological coping indices
bull Activities of daily living
bull General fitness
Research Proposal
Exercise to prevent shoulder conditions in patients
undergoing breast cancer treatment
bull Aim to conduct a randomised controlled trial (RCT) supported with qualitative research to investigate the clinical and cost-effectiveness of early supervised exercise on outcomes of arm function chronic pain and quality of life at one year in women undergoing treatment for breast cancer
Intervention
bull A physiotherapy-led structured exercise programme incorporating behavioural strategies and monitoring to encourage adherence
bull A minimum of 4 face-to-face specialist treatment sessions with individual participants will be
delivered within 12 weeks of surgery bull Access to interim telephone support will be provided The programme will restrict to controlled early
stretching and ROM exercises with subsequent progression to maintain strength and function (weeks 2 to 12)
bull Qualitative interviews will be used during the feasibility phase of the trial to explore acceptability of
to the intervention
Outcomes
bull arm shoulder and hand function at 12 months using the 30-item Disability Arm Shoulder Hand (DASH) questionnaire
bull quality of life
bull Functional Assessment of Cancer Treatment-Breast (FACT-B)
bull Short-Form-12 and EQ-5D-5L
bull Data on postoperative adverse events surgical site infection and healthcare resource use will be collected at 6 and 12 months after surgery
Positive therapies for Prevention of PSBP
1 EMLA applied to chest wall prior
to surgery less pain 3 months
Fassoulaki 2000
2 Venlafaxine XR 70mg before
and for 2 weeks post surgeryno diff
acute pain significantly less chronic
pain 6 months
Reuben 2004
3 Aggressive acute pain
management
Iohom 2006
4 Preincisional paravertebral
block
Kairaluoma 2006
5 Multimodal analgesia with
gabapentin EMLA ropivacaine less
acute pain amp pain 6 months
Fassoulaki 2005
Current Treatment Paradigms
The Toronto General Hospital
Transitional Pain Service
development and implementation
of a multidisciplinary program
to prevent chronic postsurgical pain (Katz J Pain Res 2015)
bull Nurse navigator
bull Psychologists (ACT)
Clinical Manifestations hellipour approach to the patient with CPSP
bull Type of pain Cause
bull Exclude other causes (infection recurrence)
bull Psychological and social factors
bull Temporal Context
Electronic Patient Record
Future Directions
bull Identify Causative Modifiable risk factors vs Associative risk factors
bull Measure psychological variables
bull Genetic assays to identify genes controlling the variability in developing chronic pain
Aim is lsquoto identify susceptibility to chronic pain and sensitivity to analgesicsrsquo
Chronic pain lsquoheritabilityrsquo is variable
Conclusions
bull 1 year incidence = 05 -10 bull Avoid pain before during and after surgery lsquohelliphelliptranslate advances in acute pain to chronic settinghelliphelliprsquo bull Psychological pre-assessment bull Education discussion with patients surgeons bull In some cases preventive analgesia may be beneficial bull Transitional Pain Servicehelliptrackinghellipdatabase lsquoPragmatic approachrsquo lsquoAll diseases have an acute phasersquo lsquoDrugs good for acute pain must be good for chronic painrsquo

Regional anaesthesia to prevent chronic pain after surgery a Cochrane systematic review and meta-analysisdagger M H Andreae1 and D A Andreae2
BJA 2013
bull 23 RCTrsquos
bull Epidural anaesthesia and
paravertebral blocks may be effective
in preventing chronic pain at 1 year
bull Effective in about 1 in 4
patients treated
Preincisional Paravertebral Block Reduces the Prevalence of Chronic
Pain After Breast Surgery Kairaluoma et al Anesth Analg 2006103703-708
bull Preincisional paravertebral block provides significant immediate postoperative analgesia
bull In the same patients (n = 60) 12 months sig less pain in the PVB group
bull In addition to providing acute postoperative pain relief preoperative PVB reduces the prevalence of chronic pain 1 yr after breast cancer surgery
Epidurals Intraoperative epidural analgesia provides preventative analgesia in
abdominal surgery Lavandrsquohomme et al Anaesthesiology 2005
bull Clear benefit of epidural in preventing chronic pain 1 year
bull Intraoperative epidural better than postoperative epidural
bull Effective epidural better than effective parenteral only analgesia one year
Systematic review of therapeutic interventions to reduce chronic post surgical pain (32 RCTrsquos)
Humble et al European J of Pain (2015)
POSITIVE
Gabapentinoids
Lidocaine
iv lidocaine EMLA
Regional
TIVA
NEGATIVE
Ketamine
Cryoanalgesia
Local anaesthetic infiltration
Remifentanil (increased chronic pain)
1 Gabapentin around time of surgery
lsquono effect on chronic painrsquo
POSITIVE
NEGATIVE
Meta analysis (Clarke 2012) 48 RCTrsquos positive effect at 2 months
Cochrane Systematic Review (Chaparro 2013) 280 patients analysed pain at 6 months No effect
RCT Gabapentin 1200mg prior to Thyroidectomy Sig less pain at 3 months (Brogley 2008)
RCT Gabapentin vs Placebo Knee replacement No effect on chronic pain (Clarke 2014)
2 Pregabalin ndash around time of surgery lsquoNot a recommended treatment can cause post operative somnolencersquo
Positive
Negative
Meta-analysis of 3 studies (Clarke 2012) All showed improvement in pain 2 RCTrsquoshellipvery large decrease in CPSP (p=0007)
3 unpublished RCTrsquos from Pfizer (2010-2014) hellipall negative for acute and chronic pain i) 307 patients undergoing knee replacement ii) 501 patients hysterectomy iii) 425 patient hernia
Cochrane Systematic Review (Chaparro 2013) 25 RCTrsquos significant benefit
Systematic review (Martinez May 2017) No difference between pregabalin and placebo 3 months Use for acute pain in pro-nociceptive surgery Side effects a problem
Multimodal analgesia
bull Standard protocols now widely used eg Paravertebral blocks at MD Anderson bull Pre-assessment clinic screening for pain psychological factors pain catastrophising scale helliphellipgenetic screening tests bull Education patients surgeons anaesthetists nurses psychologists
General treatment strategies for chronic postsurgical neuropathic pain
Preventative Perkins amp Kehlet Anesthesiology 2000
bullSurgical procedure preservation
sentinel node biopsy
bullBetter postoperative pain management
bullInformed consent preparatory
information
Established Dworkin Archives Neurol 2003 60
1524
bull Amitriptyline
bull Gabapentin
bull Opioids
bull Tramadol
bull 5 Lidoderm patch EMLA
Positive therapies for Prevention of PSBP
1 EMLA applied to chest wall prior
to surgery less pain 3 months
Fassoulaki 2000
2 Venlafaxine XR 70mg before
and for 2 weeks post surgeryno diff
acute pain significantly less chronic
pain 6 months
Reuben 2004
3 Aggressive acute pain
management
Iohom 2006
4 Preincisional paravertebral
block
Kairaluoma 2006
5 Multimodal analgesia with
gabapentin EMLA ropivacaine less
acute pain amp pain 6 months
Fassoulaki 2005
A pain management programme for chronic cancer-
treatment-related pain Robb Williams Duvivier Newham
Journal of Pain 2006775-150
bull Theory of cancer-related pain
bull Pain pathways
bull Overunder activity cycle
bull Pacing
bull Exercise and fitness
bull TENS
bull Posture and manual handling
bull Relapse and prevention
Psychology interventions
bull Goal setting
bull Role of factors involved in pain
bull Homework assignments
bull Relaxation techniques
bull Cognitive skills
bull Relapse and prevention
Results
significant (plt005) improvements in
bull Pain severity
bull Psychological distress
bull Pain amp psychological coping indices
bull Activities of daily living
bull General fitness
Research Proposal
Exercise to prevent shoulder conditions in patients
undergoing breast cancer treatment
bull Aim to conduct a randomised controlled trial (RCT) supported with qualitative research to investigate the clinical and cost-effectiveness of early supervised exercise on outcomes of arm function chronic pain and quality of life at one year in women undergoing treatment for breast cancer
Intervention
bull A physiotherapy-led structured exercise programme incorporating behavioural strategies and monitoring to encourage adherence
bull A minimum of 4 face-to-face specialist treatment sessions with individual participants will be
delivered within 12 weeks of surgery bull Access to interim telephone support will be provided The programme will restrict to controlled early
stretching and ROM exercises with subsequent progression to maintain strength and function (weeks 2 to 12)
bull Qualitative interviews will be used during the feasibility phase of the trial to explore acceptability of
to the intervention
Outcomes
bull arm shoulder and hand function at 12 months using the 30-item Disability Arm Shoulder Hand (DASH) questionnaire
bull quality of life
bull Functional Assessment of Cancer Treatment-Breast (FACT-B)
bull Short-Form-12 and EQ-5D-5L
bull Data on postoperative adverse events surgical site infection and healthcare resource use will be collected at 6 and 12 months after surgery
Positive therapies for Prevention of PSBP
1 EMLA applied to chest wall prior
to surgery less pain 3 months
Fassoulaki 2000
2 Venlafaxine XR 70mg before
and for 2 weeks post surgeryno diff
acute pain significantly less chronic
pain 6 months
Reuben 2004
3 Aggressive acute pain
management
Iohom 2006
4 Preincisional paravertebral
block
Kairaluoma 2006
5 Multimodal analgesia with
gabapentin EMLA ropivacaine less
acute pain amp pain 6 months
Fassoulaki 2005
Current Treatment Paradigms
The Toronto General Hospital
Transitional Pain Service
development and implementation
of a multidisciplinary program
to prevent chronic postsurgical pain (Katz J Pain Res 2015)
bull Nurse navigator
bull Psychologists (ACT)
Clinical Manifestations hellipour approach to the patient with CPSP
bull Type of pain Cause
bull Exclude other causes (infection recurrence)
bull Psychological and social factors
bull Temporal Context
Electronic Patient Record
Future Directions
bull Identify Causative Modifiable risk factors vs Associative risk factors
bull Measure psychological variables
bull Genetic assays to identify genes controlling the variability in developing chronic pain
Aim is lsquoto identify susceptibility to chronic pain and sensitivity to analgesicsrsquo
Chronic pain lsquoheritabilityrsquo is variable
Conclusions
bull 1 year incidence = 05 -10 bull Avoid pain before during and after surgery lsquohelliphelliptranslate advances in acute pain to chronic settinghelliphelliprsquo bull Psychological pre-assessment bull Education discussion with patients surgeons bull In some cases preventive analgesia may be beneficial bull Transitional Pain Servicehelliptrackinghellipdatabase lsquoPragmatic approachrsquo lsquoAll diseases have an acute phasersquo lsquoDrugs good for acute pain must be good for chronic painrsquo

Preincisional Paravertebral Block Reduces the Prevalence of Chronic
Pain After Breast Surgery Kairaluoma et al Anesth Analg 2006103703-708
bull Preincisional paravertebral block provides significant immediate postoperative analgesia
bull In the same patients (n = 60) 12 months sig less pain in the PVB group
bull In addition to providing acute postoperative pain relief preoperative PVB reduces the prevalence of chronic pain 1 yr after breast cancer surgery
Epidurals Intraoperative epidural analgesia provides preventative analgesia in
abdominal surgery Lavandrsquohomme et al Anaesthesiology 2005
bull Clear benefit of epidural in preventing chronic pain 1 year
bull Intraoperative epidural better than postoperative epidural
bull Effective epidural better than effective parenteral only analgesia one year
Systematic review of therapeutic interventions to reduce chronic post surgical pain (32 RCTrsquos)
Humble et al European J of Pain (2015)
POSITIVE
Gabapentinoids
Lidocaine
iv lidocaine EMLA
Regional
TIVA
NEGATIVE
Ketamine
Cryoanalgesia
Local anaesthetic infiltration
Remifentanil (increased chronic pain)
1 Gabapentin around time of surgery
lsquono effect on chronic painrsquo
POSITIVE
NEGATIVE
Meta analysis (Clarke 2012) 48 RCTrsquos positive effect at 2 months
Cochrane Systematic Review (Chaparro 2013) 280 patients analysed pain at 6 months No effect
RCT Gabapentin 1200mg prior to Thyroidectomy Sig less pain at 3 months (Brogley 2008)
RCT Gabapentin vs Placebo Knee replacement No effect on chronic pain (Clarke 2014)
2 Pregabalin ndash around time of surgery lsquoNot a recommended treatment can cause post operative somnolencersquo
Positive
Negative
Meta-analysis of 3 studies (Clarke 2012) All showed improvement in pain 2 RCTrsquoshellipvery large decrease in CPSP (p=0007)
3 unpublished RCTrsquos from Pfizer (2010-2014) hellipall negative for acute and chronic pain i) 307 patients undergoing knee replacement ii) 501 patients hysterectomy iii) 425 patient hernia
Cochrane Systematic Review (Chaparro 2013) 25 RCTrsquos significant benefit
Systematic review (Martinez May 2017) No difference between pregabalin and placebo 3 months Use for acute pain in pro-nociceptive surgery Side effects a problem
Multimodal analgesia
bull Standard protocols now widely used eg Paravertebral blocks at MD Anderson bull Pre-assessment clinic screening for pain psychological factors pain catastrophising scale helliphellipgenetic screening tests bull Education patients surgeons anaesthetists nurses psychologists
General treatment strategies for chronic postsurgical neuropathic pain
Preventative Perkins amp Kehlet Anesthesiology 2000
bullSurgical procedure preservation
sentinel node biopsy
bullBetter postoperative pain management
bullInformed consent preparatory
information
Established Dworkin Archives Neurol 2003 60
1524
bull Amitriptyline
bull Gabapentin
bull Opioids
bull Tramadol
bull 5 Lidoderm patch EMLA
Positive therapies for Prevention of PSBP
1 EMLA applied to chest wall prior
to surgery less pain 3 months
Fassoulaki 2000
2 Venlafaxine XR 70mg before
and for 2 weeks post surgeryno diff
acute pain significantly less chronic
pain 6 months
Reuben 2004
3 Aggressive acute pain
management
Iohom 2006
4 Preincisional paravertebral
block
Kairaluoma 2006
5 Multimodal analgesia with
gabapentin EMLA ropivacaine less
acute pain amp pain 6 months
Fassoulaki 2005
A pain management programme for chronic cancer-
treatment-related pain Robb Williams Duvivier Newham
Journal of Pain 2006775-150
bull Theory of cancer-related pain
bull Pain pathways
bull Overunder activity cycle
bull Pacing
bull Exercise and fitness
bull TENS
bull Posture and manual handling
bull Relapse and prevention
Psychology interventions
bull Goal setting
bull Role of factors involved in pain
bull Homework assignments
bull Relaxation techniques
bull Cognitive skills
bull Relapse and prevention
Results
significant (plt005) improvements in
bull Pain severity
bull Psychological distress
bull Pain amp psychological coping indices
bull Activities of daily living
bull General fitness
Research Proposal
Exercise to prevent shoulder conditions in patients
undergoing breast cancer treatment
bull Aim to conduct a randomised controlled trial (RCT) supported with qualitative research to investigate the clinical and cost-effectiveness of early supervised exercise on outcomes of arm function chronic pain and quality of life at one year in women undergoing treatment for breast cancer
Intervention
bull A physiotherapy-led structured exercise programme incorporating behavioural strategies and monitoring to encourage adherence
bull A minimum of 4 face-to-face specialist treatment sessions with individual participants will be
delivered within 12 weeks of surgery bull Access to interim telephone support will be provided The programme will restrict to controlled early
stretching and ROM exercises with subsequent progression to maintain strength and function (weeks 2 to 12)
bull Qualitative interviews will be used during the feasibility phase of the trial to explore acceptability of
to the intervention
Outcomes
bull arm shoulder and hand function at 12 months using the 30-item Disability Arm Shoulder Hand (DASH) questionnaire
bull quality of life
bull Functional Assessment of Cancer Treatment-Breast (FACT-B)
bull Short-Form-12 and EQ-5D-5L
bull Data on postoperative adverse events surgical site infection and healthcare resource use will be collected at 6 and 12 months after surgery
Positive therapies for Prevention of PSBP
1 EMLA applied to chest wall prior
to surgery less pain 3 months
Fassoulaki 2000
2 Venlafaxine XR 70mg before
and for 2 weeks post surgeryno diff
acute pain significantly less chronic
pain 6 months
Reuben 2004
3 Aggressive acute pain
management
Iohom 2006
4 Preincisional paravertebral
block
Kairaluoma 2006
5 Multimodal analgesia with
gabapentin EMLA ropivacaine less
acute pain amp pain 6 months
Fassoulaki 2005
Current Treatment Paradigms
The Toronto General Hospital
Transitional Pain Service
development and implementation
of a multidisciplinary program
to prevent chronic postsurgical pain (Katz J Pain Res 2015)
bull Nurse navigator
bull Psychologists (ACT)
Clinical Manifestations hellipour approach to the patient with CPSP
bull Type of pain Cause
bull Exclude other causes (infection recurrence)
bull Psychological and social factors
bull Temporal Context
Electronic Patient Record
Future Directions
bull Identify Causative Modifiable risk factors vs Associative risk factors
bull Measure psychological variables
bull Genetic assays to identify genes controlling the variability in developing chronic pain
Aim is lsquoto identify susceptibility to chronic pain and sensitivity to analgesicsrsquo
Chronic pain lsquoheritabilityrsquo is variable
Conclusions
bull 1 year incidence = 05 -10 bull Avoid pain before during and after surgery lsquohelliphelliptranslate advances in acute pain to chronic settinghelliphelliprsquo bull Psychological pre-assessment bull Education discussion with patients surgeons bull In some cases preventive analgesia may be beneficial bull Transitional Pain Servicehelliptrackinghellipdatabase lsquoPragmatic approachrsquo lsquoAll diseases have an acute phasersquo lsquoDrugs good for acute pain must be good for chronic painrsquo

Epidurals Intraoperative epidural analgesia provides preventative analgesia in
abdominal surgery Lavandrsquohomme et al Anaesthesiology 2005
bull Clear benefit of epidural in preventing chronic pain 1 year
bull Intraoperative epidural better than postoperative epidural
bull Effective epidural better than effective parenteral only analgesia one year
Systematic review of therapeutic interventions to reduce chronic post surgical pain (32 RCTrsquos)
Humble et al European J of Pain (2015)
POSITIVE
Gabapentinoids
Lidocaine
iv lidocaine EMLA
Regional
TIVA
NEGATIVE
Ketamine
Cryoanalgesia
Local anaesthetic infiltration
Remifentanil (increased chronic pain)
1 Gabapentin around time of surgery
lsquono effect on chronic painrsquo
POSITIVE
NEGATIVE
Meta analysis (Clarke 2012) 48 RCTrsquos positive effect at 2 months
Cochrane Systematic Review (Chaparro 2013) 280 patients analysed pain at 6 months No effect
RCT Gabapentin 1200mg prior to Thyroidectomy Sig less pain at 3 months (Brogley 2008)
RCT Gabapentin vs Placebo Knee replacement No effect on chronic pain (Clarke 2014)
2 Pregabalin ndash around time of surgery lsquoNot a recommended treatment can cause post operative somnolencersquo
Positive
Negative
Meta-analysis of 3 studies (Clarke 2012) All showed improvement in pain 2 RCTrsquoshellipvery large decrease in CPSP (p=0007)
3 unpublished RCTrsquos from Pfizer (2010-2014) hellipall negative for acute and chronic pain i) 307 patients undergoing knee replacement ii) 501 patients hysterectomy iii) 425 patient hernia
Cochrane Systematic Review (Chaparro 2013) 25 RCTrsquos significant benefit
Systematic review (Martinez May 2017) No difference between pregabalin and placebo 3 months Use for acute pain in pro-nociceptive surgery Side effects a problem
Multimodal analgesia
bull Standard protocols now widely used eg Paravertebral blocks at MD Anderson bull Pre-assessment clinic screening for pain psychological factors pain catastrophising scale helliphellipgenetic screening tests bull Education patients surgeons anaesthetists nurses psychologists
General treatment strategies for chronic postsurgical neuropathic pain
Preventative Perkins amp Kehlet Anesthesiology 2000
bullSurgical procedure preservation
sentinel node biopsy
bullBetter postoperative pain management
bullInformed consent preparatory
information
Established Dworkin Archives Neurol 2003 60
1524
bull Amitriptyline
bull Gabapentin
bull Opioids
bull Tramadol
bull 5 Lidoderm patch EMLA
Positive therapies for Prevention of PSBP
1 EMLA applied to chest wall prior
to surgery less pain 3 months
Fassoulaki 2000
2 Venlafaxine XR 70mg before
and for 2 weeks post surgeryno diff
acute pain significantly less chronic
pain 6 months
Reuben 2004
3 Aggressive acute pain
management
Iohom 2006
4 Preincisional paravertebral
block
Kairaluoma 2006
5 Multimodal analgesia with
gabapentin EMLA ropivacaine less
acute pain amp pain 6 months
Fassoulaki 2005
A pain management programme for chronic cancer-
treatment-related pain Robb Williams Duvivier Newham
Journal of Pain 2006775-150
bull Theory of cancer-related pain
bull Pain pathways
bull Overunder activity cycle
bull Pacing
bull Exercise and fitness
bull TENS
bull Posture and manual handling
bull Relapse and prevention
Psychology interventions
bull Goal setting
bull Role of factors involved in pain
bull Homework assignments
bull Relaxation techniques
bull Cognitive skills
bull Relapse and prevention
Results
significant (plt005) improvements in
bull Pain severity
bull Psychological distress
bull Pain amp psychological coping indices
bull Activities of daily living
bull General fitness
Research Proposal
Exercise to prevent shoulder conditions in patients
undergoing breast cancer treatment
bull Aim to conduct a randomised controlled trial (RCT) supported with qualitative research to investigate the clinical and cost-effectiveness of early supervised exercise on outcomes of arm function chronic pain and quality of life at one year in women undergoing treatment for breast cancer
Intervention
bull A physiotherapy-led structured exercise programme incorporating behavioural strategies and monitoring to encourage adherence
bull A minimum of 4 face-to-face specialist treatment sessions with individual participants will be
delivered within 12 weeks of surgery bull Access to interim telephone support will be provided The programme will restrict to controlled early
stretching and ROM exercises with subsequent progression to maintain strength and function (weeks 2 to 12)
bull Qualitative interviews will be used during the feasibility phase of the trial to explore acceptability of
to the intervention
Outcomes
bull arm shoulder and hand function at 12 months using the 30-item Disability Arm Shoulder Hand (DASH) questionnaire
bull quality of life
bull Functional Assessment of Cancer Treatment-Breast (FACT-B)
bull Short-Form-12 and EQ-5D-5L
bull Data on postoperative adverse events surgical site infection and healthcare resource use will be collected at 6 and 12 months after surgery
Positive therapies for Prevention of PSBP
1 EMLA applied to chest wall prior
to surgery less pain 3 months
Fassoulaki 2000
2 Venlafaxine XR 70mg before
and for 2 weeks post surgeryno diff
acute pain significantly less chronic
pain 6 months
Reuben 2004
3 Aggressive acute pain
management
Iohom 2006
4 Preincisional paravertebral
block
Kairaluoma 2006
5 Multimodal analgesia with
gabapentin EMLA ropivacaine less
acute pain amp pain 6 months
Fassoulaki 2005
Current Treatment Paradigms
The Toronto General Hospital
Transitional Pain Service
development and implementation
of a multidisciplinary program
to prevent chronic postsurgical pain (Katz J Pain Res 2015)
bull Nurse navigator
bull Psychologists (ACT)
Clinical Manifestations hellipour approach to the patient with CPSP
bull Type of pain Cause
bull Exclude other causes (infection recurrence)
bull Psychological and social factors
bull Temporal Context
Electronic Patient Record
Future Directions
bull Identify Causative Modifiable risk factors vs Associative risk factors
bull Measure psychological variables
bull Genetic assays to identify genes controlling the variability in developing chronic pain
Aim is lsquoto identify susceptibility to chronic pain and sensitivity to analgesicsrsquo
Chronic pain lsquoheritabilityrsquo is variable
Conclusions
bull 1 year incidence = 05 -10 bull Avoid pain before during and after surgery lsquohelliphelliptranslate advances in acute pain to chronic settinghelliphelliprsquo bull Psychological pre-assessment bull Education discussion with patients surgeons bull In some cases preventive analgesia may be beneficial bull Transitional Pain Servicehelliptrackinghellipdatabase lsquoPragmatic approachrsquo lsquoAll diseases have an acute phasersquo lsquoDrugs good for acute pain must be good for chronic painrsquo

Systematic review of therapeutic interventions to reduce chronic post surgical pain (32 RCTrsquos)
Humble et al European J of Pain (2015)
POSITIVE
Gabapentinoids
Lidocaine
iv lidocaine EMLA
Regional
TIVA
NEGATIVE
Ketamine
Cryoanalgesia
Local anaesthetic infiltration
Remifentanil (increased chronic pain)
1 Gabapentin around time of surgery
lsquono effect on chronic painrsquo
POSITIVE
NEGATIVE
Meta analysis (Clarke 2012) 48 RCTrsquos positive effect at 2 months
Cochrane Systematic Review (Chaparro 2013) 280 patients analysed pain at 6 months No effect
RCT Gabapentin 1200mg prior to Thyroidectomy Sig less pain at 3 months (Brogley 2008)
RCT Gabapentin vs Placebo Knee replacement No effect on chronic pain (Clarke 2014)
2 Pregabalin ndash around time of surgery lsquoNot a recommended treatment can cause post operative somnolencersquo
Positive
Negative
Meta-analysis of 3 studies (Clarke 2012) All showed improvement in pain 2 RCTrsquoshellipvery large decrease in CPSP (p=0007)
3 unpublished RCTrsquos from Pfizer (2010-2014) hellipall negative for acute and chronic pain i) 307 patients undergoing knee replacement ii) 501 patients hysterectomy iii) 425 patient hernia
Cochrane Systematic Review (Chaparro 2013) 25 RCTrsquos significant benefit
Systematic review (Martinez May 2017) No difference between pregabalin and placebo 3 months Use for acute pain in pro-nociceptive surgery Side effects a problem
Multimodal analgesia
bull Standard protocols now widely used eg Paravertebral blocks at MD Anderson bull Pre-assessment clinic screening for pain psychological factors pain catastrophising scale helliphellipgenetic screening tests bull Education patients surgeons anaesthetists nurses psychologists
General treatment strategies for chronic postsurgical neuropathic pain
Preventative Perkins amp Kehlet Anesthesiology 2000
bullSurgical procedure preservation
sentinel node biopsy
bullBetter postoperative pain management
bullInformed consent preparatory
information
Established Dworkin Archives Neurol 2003 60
1524
bull Amitriptyline
bull Gabapentin
bull Opioids
bull Tramadol
bull 5 Lidoderm patch EMLA
Positive therapies for Prevention of PSBP
1 EMLA applied to chest wall prior
to surgery less pain 3 months
Fassoulaki 2000
2 Venlafaxine XR 70mg before
and for 2 weeks post surgeryno diff
acute pain significantly less chronic
pain 6 months
Reuben 2004
3 Aggressive acute pain
management
Iohom 2006
4 Preincisional paravertebral
block
Kairaluoma 2006
5 Multimodal analgesia with
gabapentin EMLA ropivacaine less
acute pain amp pain 6 months
Fassoulaki 2005
A pain management programme for chronic cancer-
treatment-related pain Robb Williams Duvivier Newham
Journal of Pain 2006775-150
bull Theory of cancer-related pain
bull Pain pathways
bull Overunder activity cycle
bull Pacing
bull Exercise and fitness
bull TENS
bull Posture and manual handling
bull Relapse and prevention
Psychology interventions
bull Goal setting
bull Role of factors involved in pain
bull Homework assignments
bull Relaxation techniques
bull Cognitive skills
bull Relapse and prevention
Results
significant (plt005) improvements in
bull Pain severity
bull Psychological distress
bull Pain amp psychological coping indices
bull Activities of daily living
bull General fitness
Research Proposal
Exercise to prevent shoulder conditions in patients
undergoing breast cancer treatment
bull Aim to conduct a randomised controlled trial (RCT) supported with qualitative research to investigate the clinical and cost-effectiveness of early supervised exercise on outcomes of arm function chronic pain and quality of life at one year in women undergoing treatment for breast cancer
Intervention
bull A physiotherapy-led structured exercise programme incorporating behavioural strategies and monitoring to encourage adherence
bull A minimum of 4 face-to-face specialist treatment sessions with individual participants will be
delivered within 12 weeks of surgery bull Access to interim telephone support will be provided The programme will restrict to controlled early
stretching and ROM exercises with subsequent progression to maintain strength and function (weeks 2 to 12)
bull Qualitative interviews will be used during the feasibility phase of the trial to explore acceptability of
to the intervention
Outcomes
bull arm shoulder and hand function at 12 months using the 30-item Disability Arm Shoulder Hand (DASH) questionnaire
bull quality of life
bull Functional Assessment of Cancer Treatment-Breast (FACT-B)
bull Short-Form-12 and EQ-5D-5L
bull Data on postoperative adverse events surgical site infection and healthcare resource use will be collected at 6 and 12 months after surgery
Positive therapies for Prevention of PSBP
1 EMLA applied to chest wall prior
to surgery less pain 3 months
Fassoulaki 2000
2 Venlafaxine XR 70mg before
and for 2 weeks post surgeryno diff
acute pain significantly less chronic
pain 6 months
Reuben 2004
3 Aggressive acute pain
management
Iohom 2006
4 Preincisional paravertebral
block
Kairaluoma 2006
5 Multimodal analgesia with
gabapentin EMLA ropivacaine less
acute pain amp pain 6 months
Fassoulaki 2005
Current Treatment Paradigms
The Toronto General Hospital
Transitional Pain Service
development and implementation
of a multidisciplinary program
to prevent chronic postsurgical pain (Katz J Pain Res 2015)
bull Nurse navigator
bull Psychologists (ACT)
Clinical Manifestations hellipour approach to the patient with CPSP
bull Type of pain Cause
bull Exclude other causes (infection recurrence)
bull Psychological and social factors
bull Temporal Context
Electronic Patient Record
Future Directions
bull Identify Causative Modifiable risk factors vs Associative risk factors
bull Measure psychological variables
bull Genetic assays to identify genes controlling the variability in developing chronic pain
Aim is lsquoto identify susceptibility to chronic pain and sensitivity to analgesicsrsquo
Chronic pain lsquoheritabilityrsquo is variable
Conclusions
bull 1 year incidence = 05 -10 bull Avoid pain before during and after surgery lsquohelliphelliptranslate advances in acute pain to chronic settinghelliphelliprsquo bull Psychological pre-assessment bull Education discussion with patients surgeons bull In some cases preventive analgesia may be beneficial bull Transitional Pain Servicehelliptrackinghellipdatabase lsquoPragmatic approachrsquo lsquoAll diseases have an acute phasersquo lsquoDrugs good for acute pain must be good for chronic painrsquo

1 Gabapentin around time of surgery
lsquono effect on chronic painrsquo
POSITIVE
NEGATIVE
Meta analysis (Clarke 2012) 48 RCTrsquos positive effect at 2 months
Cochrane Systematic Review (Chaparro 2013) 280 patients analysed pain at 6 months No effect
RCT Gabapentin 1200mg prior to Thyroidectomy Sig less pain at 3 months (Brogley 2008)
RCT Gabapentin vs Placebo Knee replacement No effect on chronic pain (Clarke 2014)
2 Pregabalin ndash around time of surgery lsquoNot a recommended treatment can cause post operative somnolencersquo
Positive
Negative
Meta-analysis of 3 studies (Clarke 2012) All showed improvement in pain 2 RCTrsquoshellipvery large decrease in CPSP (p=0007)
3 unpublished RCTrsquos from Pfizer (2010-2014) hellipall negative for acute and chronic pain i) 307 patients undergoing knee replacement ii) 501 patients hysterectomy iii) 425 patient hernia
Cochrane Systematic Review (Chaparro 2013) 25 RCTrsquos significant benefit
Systematic review (Martinez May 2017) No difference between pregabalin and placebo 3 months Use for acute pain in pro-nociceptive surgery Side effects a problem
Multimodal analgesia
bull Standard protocols now widely used eg Paravertebral blocks at MD Anderson bull Pre-assessment clinic screening for pain psychological factors pain catastrophising scale helliphellipgenetic screening tests bull Education patients surgeons anaesthetists nurses psychologists
General treatment strategies for chronic postsurgical neuropathic pain
Preventative Perkins amp Kehlet Anesthesiology 2000
bullSurgical procedure preservation
sentinel node biopsy
bullBetter postoperative pain management
bullInformed consent preparatory
information
Established Dworkin Archives Neurol 2003 60
1524
bull Amitriptyline
bull Gabapentin
bull Opioids
bull Tramadol
bull 5 Lidoderm patch EMLA
Positive therapies for Prevention of PSBP
1 EMLA applied to chest wall prior
to surgery less pain 3 months
Fassoulaki 2000
2 Venlafaxine XR 70mg before
and for 2 weeks post surgeryno diff
acute pain significantly less chronic
pain 6 months
Reuben 2004
3 Aggressive acute pain
management
Iohom 2006
4 Preincisional paravertebral
block
Kairaluoma 2006
5 Multimodal analgesia with
gabapentin EMLA ropivacaine less
acute pain amp pain 6 months
Fassoulaki 2005
A pain management programme for chronic cancer-
treatment-related pain Robb Williams Duvivier Newham
Journal of Pain 2006775-150
bull Theory of cancer-related pain
bull Pain pathways
bull Overunder activity cycle
bull Pacing
bull Exercise and fitness
bull TENS
bull Posture and manual handling
bull Relapse and prevention
Psychology interventions
bull Goal setting
bull Role of factors involved in pain
bull Homework assignments
bull Relaxation techniques
bull Cognitive skills
bull Relapse and prevention
Results
significant (plt005) improvements in
bull Pain severity
bull Psychological distress
bull Pain amp psychological coping indices
bull Activities of daily living
bull General fitness
Research Proposal
Exercise to prevent shoulder conditions in patients
undergoing breast cancer treatment
bull Aim to conduct a randomised controlled trial (RCT) supported with qualitative research to investigate the clinical and cost-effectiveness of early supervised exercise on outcomes of arm function chronic pain and quality of life at one year in women undergoing treatment for breast cancer
Intervention
bull A physiotherapy-led structured exercise programme incorporating behavioural strategies and monitoring to encourage adherence
bull A minimum of 4 face-to-face specialist treatment sessions with individual participants will be
delivered within 12 weeks of surgery bull Access to interim telephone support will be provided The programme will restrict to controlled early
stretching and ROM exercises with subsequent progression to maintain strength and function (weeks 2 to 12)
bull Qualitative interviews will be used during the feasibility phase of the trial to explore acceptability of
to the intervention
Outcomes
bull arm shoulder and hand function at 12 months using the 30-item Disability Arm Shoulder Hand (DASH) questionnaire
bull quality of life
bull Functional Assessment of Cancer Treatment-Breast (FACT-B)
bull Short-Form-12 and EQ-5D-5L
bull Data on postoperative adverse events surgical site infection and healthcare resource use will be collected at 6 and 12 months after surgery
Positive therapies for Prevention of PSBP
1 EMLA applied to chest wall prior
to surgery less pain 3 months
Fassoulaki 2000
2 Venlafaxine XR 70mg before
and for 2 weeks post surgeryno diff
acute pain significantly less chronic
pain 6 months
Reuben 2004
3 Aggressive acute pain
management
Iohom 2006
4 Preincisional paravertebral
block
Kairaluoma 2006
5 Multimodal analgesia with
gabapentin EMLA ropivacaine less
acute pain amp pain 6 months
Fassoulaki 2005
Current Treatment Paradigms
The Toronto General Hospital
Transitional Pain Service
development and implementation
of a multidisciplinary program
to prevent chronic postsurgical pain (Katz J Pain Res 2015)
bull Nurse navigator
bull Psychologists (ACT)
Clinical Manifestations hellipour approach to the patient with CPSP
bull Type of pain Cause
bull Exclude other causes (infection recurrence)
bull Psychological and social factors
bull Temporal Context
Electronic Patient Record
Future Directions
bull Identify Causative Modifiable risk factors vs Associative risk factors
bull Measure psychological variables
bull Genetic assays to identify genes controlling the variability in developing chronic pain
Aim is lsquoto identify susceptibility to chronic pain and sensitivity to analgesicsrsquo
Chronic pain lsquoheritabilityrsquo is variable
Conclusions
bull 1 year incidence = 05 -10 bull Avoid pain before during and after surgery lsquohelliphelliptranslate advances in acute pain to chronic settinghelliphelliprsquo bull Psychological pre-assessment bull Education discussion with patients surgeons bull In some cases preventive analgesia may be beneficial bull Transitional Pain Servicehelliptrackinghellipdatabase lsquoPragmatic approachrsquo lsquoAll diseases have an acute phasersquo lsquoDrugs good for acute pain must be good for chronic painrsquo

2 Pregabalin ndash around time of surgery lsquoNot a recommended treatment can cause post operative somnolencersquo
Positive
Negative
Meta-analysis of 3 studies (Clarke 2012) All showed improvement in pain 2 RCTrsquoshellipvery large decrease in CPSP (p=0007)
3 unpublished RCTrsquos from Pfizer (2010-2014) hellipall negative for acute and chronic pain i) 307 patients undergoing knee replacement ii) 501 patients hysterectomy iii) 425 patient hernia
Cochrane Systematic Review (Chaparro 2013) 25 RCTrsquos significant benefit
Systematic review (Martinez May 2017) No difference between pregabalin and placebo 3 months Use for acute pain in pro-nociceptive surgery Side effects a problem
Multimodal analgesia
bull Standard protocols now widely used eg Paravertebral blocks at MD Anderson bull Pre-assessment clinic screening for pain psychological factors pain catastrophising scale helliphellipgenetic screening tests bull Education patients surgeons anaesthetists nurses psychologists
General treatment strategies for chronic postsurgical neuropathic pain
Preventative Perkins amp Kehlet Anesthesiology 2000
bullSurgical procedure preservation
sentinel node biopsy
bullBetter postoperative pain management
bullInformed consent preparatory
information
Established Dworkin Archives Neurol 2003 60
1524
bull Amitriptyline
bull Gabapentin
bull Opioids
bull Tramadol
bull 5 Lidoderm patch EMLA
Positive therapies for Prevention of PSBP
1 EMLA applied to chest wall prior
to surgery less pain 3 months
Fassoulaki 2000
2 Venlafaxine XR 70mg before
and for 2 weeks post surgeryno diff
acute pain significantly less chronic
pain 6 months
Reuben 2004
3 Aggressive acute pain
management
Iohom 2006
4 Preincisional paravertebral
block
Kairaluoma 2006
5 Multimodal analgesia with
gabapentin EMLA ropivacaine less
acute pain amp pain 6 months
Fassoulaki 2005
A pain management programme for chronic cancer-
treatment-related pain Robb Williams Duvivier Newham
Journal of Pain 2006775-150
bull Theory of cancer-related pain
bull Pain pathways
bull Overunder activity cycle
bull Pacing
bull Exercise and fitness
bull TENS
bull Posture and manual handling
bull Relapse and prevention
Psychology interventions
bull Goal setting
bull Role of factors involved in pain
bull Homework assignments
bull Relaxation techniques
bull Cognitive skills
bull Relapse and prevention
Results
significant (plt005) improvements in
bull Pain severity
bull Psychological distress
bull Pain amp psychological coping indices
bull Activities of daily living
bull General fitness
Research Proposal
Exercise to prevent shoulder conditions in patients
undergoing breast cancer treatment
bull Aim to conduct a randomised controlled trial (RCT) supported with qualitative research to investigate the clinical and cost-effectiveness of early supervised exercise on outcomes of arm function chronic pain and quality of life at one year in women undergoing treatment for breast cancer
Intervention
bull A physiotherapy-led structured exercise programme incorporating behavioural strategies and monitoring to encourage adherence
bull A minimum of 4 face-to-face specialist treatment sessions with individual participants will be
delivered within 12 weeks of surgery bull Access to interim telephone support will be provided The programme will restrict to controlled early
stretching and ROM exercises with subsequent progression to maintain strength and function (weeks 2 to 12)
bull Qualitative interviews will be used during the feasibility phase of the trial to explore acceptability of
to the intervention
Outcomes
bull arm shoulder and hand function at 12 months using the 30-item Disability Arm Shoulder Hand (DASH) questionnaire
bull quality of life
bull Functional Assessment of Cancer Treatment-Breast (FACT-B)
bull Short-Form-12 and EQ-5D-5L
bull Data on postoperative adverse events surgical site infection and healthcare resource use will be collected at 6 and 12 months after surgery
Positive therapies for Prevention of PSBP
1 EMLA applied to chest wall prior
to surgery less pain 3 months
Fassoulaki 2000
2 Venlafaxine XR 70mg before
and for 2 weeks post surgeryno diff
acute pain significantly less chronic
pain 6 months
Reuben 2004
3 Aggressive acute pain
management
Iohom 2006
4 Preincisional paravertebral
block
Kairaluoma 2006
5 Multimodal analgesia with
gabapentin EMLA ropivacaine less
acute pain amp pain 6 months
Fassoulaki 2005
Current Treatment Paradigms
The Toronto General Hospital
Transitional Pain Service
development and implementation
of a multidisciplinary program
to prevent chronic postsurgical pain (Katz J Pain Res 2015)
bull Nurse navigator
bull Psychologists (ACT)
Clinical Manifestations hellipour approach to the patient with CPSP
bull Type of pain Cause
bull Exclude other causes (infection recurrence)
bull Psychological and social factors
bull Temporal Context
Electronic Patient Record
Future Directions
bull Identify Causative Modifiable risk factors vs Associative risk factors
bull Measure psychological variables
bull Genetic assays to identify genes controlling the variability in developing chronic pain
Aim is lsquoto identify susceptibility to chronic pain and sensitivity to analgesicsrsquo
Chronic pain lsquoheritabilityrsquo is variable
Conclusions
bull 1 year incidence = 05 -10 bull Avoid pain before during and after surgery lsquohelliphelliptranslate advances in acute pain to chronic settinghelliphelliprsquo bull Psychological pre-assessment bull Education discussion with patients surgeons bull In some cases preventive analgesia may be beneficial bull Transitional Pain Servicehelliptrackinghellipdatabase lsquoPragmatic approachrsquo lsquoAll diseases have an acute phasersquo lsquoDrugs good for acute pain must be good for chronic painrsquo

Multimodal analgesia
bull Standard protocols now widely used eg Paravertebral blocks at MD Anderson bull Pre-assessment clinic screening for pain psychological factors pain catastrophising scale helliphellipgenetic screening tests bull Education patients surgeons anaesthetists nurses psychologists
General treatment strategies for chronic postsurgical neuropathic pain
Preventative Perkins amp Kehlet Anesthesiology 2000
bullSurgical procedure preservation
sentinel node biopsy
bullBetter postoperative pain management
bullInformed consent preparatory
information
Established Dworkin Archives Neurol 2003 60
1524
bull Amitriptyline
bull Gabapentin
bull Opioids
bull Tramadol
bull 5 Lidoderm patch EMLA
Positive therapies for Prevention of PSBP
1 EMLA applied to chest wall prior
to surgery less pain 3 months
Fassoulaki 2000
2 Venlafaxine XR 70mg before
and for 2 weeks post surgeryno diff
acute pain significantly less chronic
pain 6 months
Reuben 2004
3 Aggressive acute pain
management
Iohom 2006
4 Preincisional paravertebral
block
Kairaluoma 2006
5 Multimodal analgesia with
gabapentin EMLA ropivacaine less
acute pain amp pain 6 months
Fassoulaki 2005
A pain management programme for chronic cancer-
treatment-related pain Robb Williams Duvivier Newham
Journal of Pain 2006775-150
bull Theory of cancer-related pain
bull Pain pathways
bull Overunder activity cycle
bull Pacing
bull Exercise and fitness
bull TENS
bull Posture and manual handling
bull Relapse and prevention
Psychology interventions
bull Goal setting
bull Role of factors involved in pain
bull Homework assignments
bull Relaxation techniques
bull Cognitive skills
bull Relapse and prevention
Results
significant (plt005) improvements in
bull Pain severity
bull Psychological distress
bull Pain amp psychological coping indices
bull Activities of daily living
bull General fitness
Research Proposal
Exercise to prevent shoulder conditions in patients
undergoing breast cancer treatment
bull Aim to conduct a randomised controlled trial (RCT) supported with qualitative research to investigate the clinical and cost-effectiveness of early supervised exercise on outcomes of arm function chronic pain and quality of life at one year in women undergoing treatment for breast cancer
Intervention
bull A physiotherapy-led structured exercise programme incorporating behavioural strategies and monitoring to encourage adherence
bull A minimum of 4 face-to-face specialist treatment sessions with individual participants will be
delivered within 12 weeks of surgery bull Access to interim telephone support will be provided The programme will restrict to controlled early
stretching and ROM exercises with subsequent progression to maintain strength and function (weeks 2 to 12)
bull Qualitative interviews will be used during the feasibility phase of the trial to explore acceptability of
to the intervention
Outcomes
bull arm shoulder and hand function at 12 months using the 30-item Disability Arm Shoulder Hand (DASH) questionnaire
bull quality of life
bull Functional Assessment of Cancer Treatment-Breast (FACT-B)
bull Short-Form-12 and EQ-5D-5L
bull Data on postoperative adverse events surgical site infection and healthcare resource use will be collected at 6 and 12 months after surgery
Positive therapies for Prevention of PSBP
1 EMLA applied to chest wall prior
to surgery less pain 3 months
Fassoulaki 2000
2 Venlafaxine XR 70mg before
and for 2 weeks post surgeryno diff
acute pain significantly less chronic
pain 6 months
Reuben 2004
3 Aggressive acute pain
management
Iohom 2006
4 Preincisional paravertebral
block
Kairaluoma 2006
5 Multimodal analgesia with
gabapentin EMLA ropivacaine less
acute pain amp pain 6 months
Fassoulaki 2005
Current Treatment Paradigms
The Toronto General Hospital
Transitional Pain Service
development and implementation
of a multidisciplinary program
to prevent chronic postsurgical pain (Katz J Pain Res 2015)
bull Nurse navigator
bull Psychologists (ACT)
Clinical Manifestations hellipour approach to the patient with CPSP
bull Type of pain Cause
bull Exclude other causes (infection recurrence)
bull Psychological and social factors
bull Temporal Context
Electronic Patient Record
Future Directions
bull Identify Causative Modifiable risk factors vs Associative risk factors
bull Measure psychological variables
bull Genetic assays to identify genes controlling the variability in developing chronic pain
Aim is lsquoto identify susceptibility to chronic pain and sensitivity to analgesicsrsquo
Chronic pain lsquoheritabilityrsquo is variable
Conclusions
bull 1 year incidence = 05 -10 bull Avoid pain before during and after surgery lsquohelliphelliptranslate advances in acute pain to chronic settinghelliphelliprsquo bull Psychological pre-assessment bull Education discussion with patients surgeons bull In some cases preventive analgesia may be beneficial bull Transitional Pain Servicehelliptrackinghellipdatabase lsquoPragmatic approachrsquo lsquoAll diseases have an acute phasersquo lsquoDrugs good for acute pain must be good for chronic painrsquo

General treatment strategies for chronic postsurgical neuropathic pain
Preventative Perkins amp Kehlet Anesthesiology 2000
bullSurgical procedure preservation
sentinel node biopsy
bullBetter postoperative pain management
bullInformed consent preparatory
information
Established Dworkin Archives Neurol 2003 60
1524
bull Amitriptyline
bull Gabapentin
bull Opioids
bull Tramadol
bull 5 Lidoderm patch EMLA
Positive therapies for Prevention of PSBP
1 EMLA applied to chest wall prior
to surgery less pain 3 months
Fassoulaki 2000
2 Venlafaxine XR 70mg before
and for 2 weeks post surgeryno diff
acute pain significantly less chronic
pain 6 months
Reuben 2004
3 Aggressive acute pain
management
Iohom 2006
4 Preincisional paravertebral
block
Kairaluoma 2006
5 Multimodal analgesia with
gabapentin EMLA ropivacaine less
acute pain amp pain 6 months
Fassoulaki 2005
A pain management programme for chronic cancer-
treatment-related pain Robb Williams Duvivier Newham
Journal of Pain 2006775-150
bull Theory of cancer-related pain
bull Pain pathways
bull Overunder activity cycle
bull Pacing
bull Exercise and fitness
bull TENS
bull Posture and manual handling
bull Relapse and prevention
Psychology interventions
bull Goal setting
bull Role of factors involved in pain
bull Homework assignments
bull Relaxation techniques
bull Cognitive skills
bull Relapse and prevention
Results
significant (plt005) improvements in
bull Pain severity
bull Psychological distress
bull Pain amp psychological coping indices
bull Activities of daily living
bull General fitness
Research Proposal
Exercise to prevent shoulder conditions in patients
undergoing breast cancer treatment
bull Aim to conduct a randomised controlled trial (RCT) supported with qualitative research to investigate the clinical and cost-effectiveness of early supervised exercise on outcomes of arm function chronic pain and quality of life at one year in women undergoing treatment for breast cancer
Intervention
bull A physiotherapy-led structured exercise programme incorporating behavioural strategies and monitoring to encourage adherence
bull A minimum of 4 face-to-face specialist treatment sessions with individual participants will be
delivered within 12 weeks of surgery bull Access to interim telephone support will be provided The programme will restrict to controlled early
stretching and ROM exercises with subsequent progression to maintain strength and function (weeks 2 to 12)
bull Qualitative interviews will be used during the feasibility phase of the trial to explore acceptability of
to the intervention
Outcomes
bull arm shoulder and hand function at 12 months using the 30-item Disability Arm Shoulder Hand (DASH) questionnaire
bull quality of life
bull Functional Assessment of Cancer Treatment-Breast (FACT-B)
bull Short-Form-12 and EQ-5D-5L
bull Data on postoperative adverse events surgical site infection and healthcare resource use will be collected at 6 and 12 months after surgery
Positive therapies for Prevention of PSBP
1 EMLA applied to chest wall prior
to surgery less pain 3 months
Fassoulaki 2000
2 Venlafaxine XR 70mg before
and for 2 weeks post surgeryno diff
acute pain significantly less chronic
pain 6 months
Reuben 2004
3 Aggressive acute pain
management
Iohom 2006
4 Preincisional paravertebral
block
Kairaluoma 2006
5 Multimodal analgesia with
gabapentin EMLA ropivacaine less
acute pain amp pain 6 months
Fassoulaki 2005
Current Treatment Paradigms
The Toronto General Hospital
Transitional Pain Service
development and implementation
of a multidisciplinary program
to prevent chronic postsurgical pain (Katz J Pain Res 2015)
bull Nurse navigator
bull Psychologists (ACT)
Clinical Manifestations hellipour approach to the patient with CPSP
bull Type of pain Cause
bull Exclude other causes (infection recurrence)
bull Psychological and social factors
bull Temporal Context
Electronic Patient Record
Future Directions
bull Identify Causative Modifiable risk factors vs Associative risk factors
bull Measure psychological variables
bull Genetic assays to identify genes controlling the variability in developing chronic pain
Aim is lsquoto identify susceptibility to chronic pain and sensitivity to analgesicsrsquo
Chronic pain lsquoheritabilityrsquo is variable
Conclusions
bull 1 year incidence = 05 -10 bull Avoid pain before during and after surgery lsquohelliphelliptranslate advances in acute pain to chronic settinghelliphelliprsquo bull Psychological pre-assessment bull Education discussion with patients surgeons bull In some cases preventive analgesia may be beneficial bull Transitional Pain Servicehelliptrackinghellipdatabase lsquoPragmatic approachrsquo lsquoAll diseases have an acute phasersquo lsquoDrugs good for acute pain must be good for chronic painrsquo

Positive therapies for Prevention of PSBP
1 EMLA applied to chest wall prior
to surgery less pain 3 months
Fassoulaki 2000
2 Venlafaxine XR 70mg before
and for 2 weeks post surgeryno diff
acute pain significantly less chronic
pain 6 months
Reuben 2004
3 Aggressive acute pain
management
Iohom 2006
4 Preincisional paravertebral
block
Kairaluoma 2006
5 Multimodal analgesia with
gabapentin EMLA ropivacaine less
acute pain amp pain 6 months
Fassoulaki 2005
A pain management programme for chronic cancer-
treatment-related pain Robb Williams Duvivier Newham
Journal of Pain 2006775-150
bull Theory of cancer-related pain
bull Pain pathways
bull Overunder activity cycle
bull Pacing
bull Exercise and fitness
bull TENS
bull Posture and manual handling
bull Relapse and prevention
Psychology interventions
bull Goal setting
bull Role of factors involved in pain
bull Homework assignments
bull Relaxation techniques
bull Cognitive skills
bull Relapse and prevention
Results
significant (plt005) improvements in
bull Pain severity
bull Psychological distress
bull Pain amp psychological coping indices
bull Activities of daily living
bull General fitness
Research Proposal
Exercise to prevent shoulder conditions in patients
undergoing breast cancer treatment
bull Aim to conduct a randomised controlled trial (RCT) supported with qualitative research to investigate the clinical and cost-effectiveness of early supervised exercise on outcomes of arm function chronic pain and quality of life at one year in women undergoing treatment for breast cancer
Intervention
bull A physiotherapy-led structured exercise programme incorporating behavioural strategies and monitoring to encourage adherence
bull A minimum of 4 face-to-face specialist treatment sessions with individual participants will be
delivered within 12 weeks of surgery bull Access to interim telephone support will be provided The programme will restrict to controlled early
stretching and ROM exercises with subsequent progression to maintain strength and function (weeks 2 to 12)
bull Qualitative interviews will be used during the feasibility phase of the trial to explore acceptability of
to the intervention
Outcomes
bull arm shoulder and hand function at 12 months using the 30-item Disability Arm Shoulder Hand (DASH) questionnaire
bull quality of life
bull Functional Assessment of Cancer Treatment-Breast (FACT-B)
bull Short-Form-12 and EQ-5D-5L
bull Data on postoperative adverse events surgical site infection and healthcare resource use will be collected at 6 and 12 months after surgery
Positive therapies for Prevention of PSBP
1 EMLA applied to chest wall prior
to surgery less pain 3 months
Fassoulaki 2000
2 Venlafaxine XR 70mg before
and for 2 weeks post surgeryno diff
acute pain significantly less chronic
pain 6 months
Reuben 2004
3 Aggressive acute pain
management
Iohom 2006
4 Preincisional paravertebral
block
Kairaluoma 2006
5 Multimodal analgesia with
gabapentin EMLA ropivacaine less
acute pain amp pain 6 months
Fassoulaki 2005
Current Treatment Paradigms
The Toronto General Hospital
Transitional Pain Service
development and implementation
of a multidisciplinary program
to prevent chronic postsurgical pain (Katz J Pain Res 2015)
bull Nurse navigator
bull Psychologists (ACT)
Clinical Manifestations hellipour approach to the patient with CPSP
bull Type of pain Cause
bull Exclude other causes (infection recurrence)
bull Psychological and social factors
bull Temporal Context
Electronic Patient Record
Future Directions
bull Identify Causative Modifiable risk factors vs Associative risk factors
bull Measure psychological variables
bull Genetic assays to identify genes controlling the variability in developing chronic pain
Aim is lsquoto identify susceptibility to chronic pain and sensitivity to analgesicsrsquo
Chronic pain lsquoheritabilityrsquo is variable
Conclusions
bull 1 year incidence = 05 -10 bull Avoid pain before during and after surgery lsquohelliphelliptranslate advances in acute pain to chronic settinghelliphelliprsquo bull Psychological pre-assessment bull Education discussion with patients surgeons bull In some cases preventive analgesia may be beneficial bull Transitional Pain Servicehelliptrackinghellipdatabase lsquoPragmatic approachrsquo lsquoAll diseases have an acute phasersquo lsquoDrugs good for acute pain must be good for chronic painrsquo

A pain management programme for chronic cancer-
treatment-related pain Robb Williams Duvivier Newham
Journal of Pain 2006775-150
bull Theory of cancer-related pain
bull Pain pathways
bull Overunder activity cycle
bull Pacing
bull Exercise and fitness
bull TENS
bull Posture and manual handling
bull Relapse and prevention
Psychology interventions
bull Goal setting
bull Role of factors involved in pain
bull Homework assignments
bull Relaxation techniques
bull Cognitive skills
bull Relapse and prevention
Results
significant (plt005) improvements in
bull Pain severity
bull Psychological distress
bull Pain amp psychological coping indices
bull Activities of daily living
bull General fitness
Research Proposal
Exercise to prevent shoulder conditions in patients
undergoing breast cancer treatment
bull Aim to conduct a randomised controlled trial (RCT) supported with qualitative research to investigate the clinical and cost-effectiveness of early supervised exercise on outcomes of arm function chronic pain and quality of life at one year in women undergoing treatment for breast cancer
Intervention
bull A physiotherapy-led structured exercise programme incorporating behavioural strategies and monitoring to encourage adherence
bull A minimum of 4 face-to-face specialist treatment sessions with individual participants will be
delivered within 12 weeks of surgery bull Access to interim telephone support will be provided The programme will restrict to controlled early
stretching and ROM exercises with subsequent progression to maintain strength and function (weeks 2 to 12)
bull Qualitative interviews will be used during the feasibility phase of the trial to explore acceptability of
to the intervention
Outcomes
bull arm shoulder and hand function at 12 months using the 30-item Disability Arm Shoulder Hand (DASH) questionnaire
bull quality of life
bull Functional Assessment of Cancer Treatment-Breast (FACT-B)
bull Short-Form-12 and EQ-5D-5L
bull Data on postoperative adverse events surgical site infection and healthcare resource use will be collected at 6 and 12 months after surgery
Positive therapies for Prevention of PSBP
1 EMLA applied to chest wall prior
to surgery less pain 3 months
Fassoulaki 2000
2 Venlafaxine XR 70mg before
and for 2 weeks post surgeryno diff
acute pain significantly less chronic
pain 6 months
Reuben 2004
3 Aggressive acute pain
management
Iohom 2006
4 Preincisional paravertebral
block
Kairaluoma 2006
5 Multimodal analgesia with
gabapentin EMLA ropivacaine less
acute pain amp pain 6 months
Fassoulaki 2005
Current Treatment Paradigms
The Toronto General Hospital
Transitional Pain Service
development and implementation
of a multidisciplinary program
to prevent chronic postsurgical pain (Katz J Pain Res 2015)
bull Nurse navigator
bull Psychologists (ACT)
Clinical Manifestations hellipour approach to the patient with CPSP
bull Type of pain Cause
bull Exclude other causes (infection recurrence)
bull Psychological and social factors
bull Temporal Context
Electronic Patient Record
Future Directions
bull Identify Causative Modifiable risk factors vs Associative risk factors
bull Measure psychological variables
bull Genetic assays to identify genes controlling the variability in developing chronic pain
Aim is lsquoto identify susceptibility to chronic pain and sensitivity to analgesicsrsquo
Chronic pain lsquoheritabilityrsquo is variable
Conclusions
bull 1 year incidence = 05 -10 bull Avoid pain before during and after surgery lsquohelliphelliptranslate advances in acute pain to chronic settinghelliphelliprsquo bull Psychological pre-assessment bull Education discussion with patients surgeons bull In some cases preventive analgesia may be beneficial bull Transitional Pain Servicehelliptrackinghellipdatabase lsquoPragmatic approachrsquo lsquoAll diseases have an acute phasersquo lsquoDrugs good for acute pain must be good for chronic painrsquo

Psychology interventions
bull Goal setting
bull Role of factors involved in pain
bull Homework assignments
bull Relaxation techniques
bull Cognitive skills
bull Relapse and prevention
Results
significant (plt005) improvements in
bull Pain severity
bull Psychological distress
bull Pain amp psychological coping indices
bull Activities of daily living
bull General fitness
Research Proposal
Exercise to prevent shoulder conditions in patients
undergoing breast cancer treatment
bull Aim to conduct a randomised controlled trial (RCT) supported with qualitative research to investigate the clinical and cost-effectiveness of early supervised exercise on outcomes of arm function chronic pain and quality of life at one year in women undergoing treatment for breast cancer
Intervention
bull A physiotherapy-led structured exercise programme incorporating behavioural strategies and monitoring to encourage adherence
bull A minimum of 4 face-to-face specialist treatment sessions with individual participants will be
delivered within 12 weeks of surgery bull Access to interim telephone support will be provided The programme will restrict to controlled early
stretching and ROM exercises with subsequent progression to maintain strength and function (weeks 2 to 12)
bull Qualitative interviews will be used during the feasibility phase of the trial to explore acceptability of
to the intervention
Outcomes
bull arm shoulder and hand function at 12 months using the 30-item Disability Arm Shoulder Hand (DASH) questionnaire
bull quality of life
bull Functional Assessment of Cancer Treatment-Breast (FACT-B)
bull Short-Form-12 and EQ-5D-5L
bull Data on postoperative adverse events surgical site infection and healthcare resource use will be collected at 6 and 12 months after surgery
Positive therapies for Prevention of PSBP
1 EMLA applied to chest wall prior
to surgery less pain 3 months
Fassoulaki 2000
2 Venlafaxine XR 70mg before
and for 2 weeks post surgeryno diff
acute pain significantly less chronic
pain 6 months
Reuben 2004
3 Aggressive acute pain
management
Iohom 2006
4 Preincisional paravertebral
block
Kairaluoma 2006
5 Multimodal analgesia with
gabapentin EMLA ropivacaine less
acute pain amp pain 6 months
Fassoulaki 2005
Current Treatment Paradigms
The Toronto General Hospital
Transitional Pain Service
development and implementation
of a multidisciplinary program
to prevent chronic postsurgical pain (Katz J Pain Res 2015)
bull Nurse navigator
bull Psychologists (ACT)
Clinical Manifestations hellipour approach to the patient with CPSP
bull Type of pain Cause
bull Exclude other causes (infection recurrence)
bull Psychological and social factors
bull Temporal Context
Electronic Patient Record
Future Directions
bull Identify Causative Modifiable risk factors vs Associative risk factors
bull Measure psychological variables
bull Genetic assays to identify genes controlling the variability in developing chronic pain
Aim is lsquoto identify susceptibility to chronic pain and sensitivity to analgesicsrsquo
Chronic pain lsquoheritabilityrsquo is variable
Conclusions
bull 1 year incidence = 05 -10 bull Avoid pain before during and after surgery lsquohelliphelliptranslate advances in acute pain to chronic settinghelliphelliprsquo bull Psychological pre-assessment bull Education discussion with patients surgeons bull In some cases preventive analgesia may be beneficial bull Transitional Pain Servicehelliptrackinghellipdatabase lsquoPragmatic approachrsquo lsquoAll diseases have an acute phasersquo lsquoDrugs good for acute pain must be good for chronic painrsquo

Results
significant (plt005) improvements in
bull Pain severity
bull Psychological distress
bull Pain amp psychological coping indices
bull Activities of daily living
bull General fitness
Research Proposal
Exercise to prevent shoulder conditions in patients
undergoing breast cancer treatment
bull Aim to conduct a randomised controlled trial (RCT) supported with qualitative research to investigate the clinical and cost-effectiveness of early supervised exercise on outcomes of arm function chronic pain and quality of life at one year in women undergoing treatment for breast cancer
Intervention
bull A physiotherapy-led structured exercise programme incorporating behavioural strategies and monitoring to encourage adherence
bull A minimum of 4 face-to-face specialist treatment sessions with individual participants will be
delivered within 12 weeks of surgery bull Access to interim telephone support will be provided The programme will restrict to controlled early
stretching and ROM exercises with subsequent progression to maintain strength and function (weeks 2 to 12)
bull Qualitative interviews will be used during the feasibility phase of the trial to explore acceptability of
to the intervention
Outcomes
bull arm shoulder and hand function at 12 months using the 30-item Disability Arm Shoulder Hand (DASH) questionnaire
bull quality of life
bull Functional Assessment of Cancer Treatment-Breast (FACT-B)
bull Short-Form-12 and EQ-5D-5L
bull Data on postoperative adverse events surgical site infection and healthcare resource use will be collected at 6 and 12 months after surgery
Positive therapies for Prevention of PSBP
1 EMLA applied to chest wall prior
to surgery less pain 3 months
Fassoulaki 2000
2 Venlafaxine XR 70mg before
and for 2 weeks post surgeryno diff
acute pain significantly less chronic
pain 6 months
Reuben 2004
3 Aggressive acute pain
management
Iohom 2006
4 Preincisional paravertebral
block
Kairaluoma 2006
5 Multimodal analgesia with
gabapentin EMLA ropivacaine less
acute pain amp pain 6 months
Fassoulaki 2005
Current Treatment Paradigms
The Toronto General Hospital
Transitional Pain Service
development and implementation
of a multidisciplinary program
to prevent chronic postsurgical pain (Katz J Pain Res 2015)
bull Nurse navigator
bull Psychologists (ACT)
Clinical Manifestations hellipour approach to the patient with CPSP
bull Type of pain Cause
bull Exclude other causes (infection recurrence)
bull Psychological and social factors
bull Temporal Context
Electronic Patient Record
Future Directions
bull Identify Causative Modifiable risk factors vs Associative risk factors
bull Measure psychological variables
bull Genetic assays to identify genes controlling the variability in developing chronic pain
Aim is lsquoto identify susceptibility to chronic pain and sensitivity to analgesicsrsquo
Chronic pain lsquoheritabilityrsquo is variable
Conclusions
bull 1 year incidence = 05 -10 bull Avoid pain before during and after surgery lsquohelliphelliptranslate advances in acute pain to chronic settinghelliphelliprsquo bull Psychological pre-assessment bull Education discussion with patients surgeons bull In some cases preventive analgesia may be beneficial bull Transitional Pain Servicehelliptrackinghellipdatabase lsquoPragmatic approachrsquo lsquoAll diseases have an acute phasersquo lsquoDrugs good for acute pain must be good for chronic painrsquo

Research Proposal
Exercise to prevent shoulder conditions in patients
undergoing breast cancer treatment
bull Aim to conduct a randomised controlled trial (RCT) supported with qualitative research to investigate the clinical and cost-effectiveness of early supervised exercise on outcomes of arm function chronic pain and quality of life at one year in women undergoing treatment for breast cancer
Intervention
bull A physiotherapy-led structured exercise programme incorporating behavioural strategies and monitoring to encourage adherence
bull A minimum of 4 face-to-face specialist treatment sessions with individual participants will be
delivered within 12 weeks of surgery bull Access to interim telephone support will be provided The programme will restrict to controlled early
stretching and ROM exercises with subsequent progression to maintain strength and function (weeks 2 to 12)
bull Qualitative interviews will be used during the feasibility phase of the trial to explore acceptability of
to the intervention
Outcomes
bull arm shoulder and hand function at 12 months using the 30-item Disability Arm Shoulder Hand (DASH) questionnaire
bull quality of life
bull Functional Assessment of Cancer Treatment-Breast (FACT-B)
bull Short-Form-12 and EQ-5D-5L
bull Data on postoperative adverse events surgical site infection and healthcare resource use will be collected at 6 and 12 months after surgery
Positive therapies for Prevention of PSBP
1 EMLA applied to chest wall prior
to surgery less pain 3 months
Fassoulaki 2000
2 Venlafaxine XR 70mg before
and for 2 weeks post surgeryno diff
acute pain significantly less chronic
pain 6 months
Reuben 2004
3 Aggressive acute pain
management
Iohom 2006
4 Preincisional paravertebral
block
Kairaluoma 2006
5 Multimodal analgesia with
gabapentin EMLA ropivacaine less
acute pain amp pain 6 months
Fassoulaki 2005
Current Treatment Paradigms
The Toronto General Hospital
Transitional Pain Service
development and implementation
of a multidisciplinary program
to prevent chronic postsurgical pain (Katz J Pain Res 2015)
bull Nurse navigator
bull Psychologists (ACT)
Clinical Manifestations hellipour approach to the patient with CPSP
bull Type of pain Cause
bull Exclude other causes (infection recurrence)
bull Psychological and social factors
bull Temporal Context
Electronic Patient Record
Future Directions
bull Identify Causative Modifiable risk factors vs Associative risk factors
bull Measure psychological variables
bull Genetic assays to identify genes controlling the variability in developing chronic pain
Aim is lsquoto identify susceptibility to chronic pain and sensitivity to analgesicsrsquo
Chronic pain lsquoheritabilityrsquo is variable
Conclusions
bull 1 year incidence = 05 -10 bull Avoid pain before during and after surgery lsquohelliphelliptranslate advances in acute pain to chronic settinghelliphelliprsquo bull Psychological pre-assessment bull Education discussion with patients surgeons bull In some cases preventive analgesia may be beneficial bull Transitional Pain Servicehelliptrackinghellipdatabase lsquoPragmatic approachrsquo lsquoAll diseases have an acute phasersquo lsquoDrugs good for acute pain must be good for chronic painrsquo

Intervention
bull A physiotherapy-led structured exercise programme incorporating behavioural strategies and monitoring to encourage adherence
bull A minimum of 4 face-to-face specialist treatment sessions with individual participants will be
delivered within 12 weeks of surgery bull Access to interim telephone support will be provided The programme will restrict to controlled early
stretching and ROM exercises with subsequent progression to maintain strength and function (weeks 2 to 12)
bull Qualitative interviews will be used during the feasibility phase of the trial to explore acceptability of
to the intervention
Outcomes
bull arm shoulder and hand function at 12 months using the 30-item Disability Arm Shoulder Hand (DASH) questionnaire
bull quality of life
bull Functional Assessment of Cancer Treatment-Breast (FACT-B)
bull Short-Form-12 and EQ-5D-5L
bull Data on postoperative adverse events surgical site infection and healthcare resource use will be collected at 6 and 12 months after surgery
Positive therapies for Prevention of PSBP
1 EMLA applied to chest wall prior
to surgery less pain 3 months
Fassoulaki 2000
2 Venlafaxine XR 70mg before
and for 2 weeks post surgeryno diff
acute pain significantly less chronic
pain 6 months
Reuben 2004
3 Aggressive acute pain
management
Iohom 2006
4 Preincisional paravertebral
block
Kairaluoma 2006
5 Multimodal analgesia with
gabapentin EMLA ropivacaine less
acute pain amp pain 6 months
Fassoulaki 2005
Current Treatment Paradigms
The Toronto General Hospital
Transitional Pain Service
development and implementation
of a multidisciplinary program
to prevent chronic postsurgical pain (Katz J Pain Res 2015)
bull Nurse navigator
bull Psychologists (ACT)
Clinical Manifestations hellipour approach to the patient with CPSP
bull Type of pain Cause
bull Exclude other causes (infection recurrence)
bull Psychological and social factors
bull Temporal Context
Electronic Patient Record
Future Directions
bull Identify Causative Modifiable risk factors vs Associative risk factors
bull Measure psychological variables
bull Genetic assays to identify genes controlling the variability in developing chronic pain
Aim is lsquoto identify susceptibility to chronic pain and sensitivity to analgesicsrsquo
Chronic pain lsquoheritabilityrsquo is variable
Conclusions
bull 1 year incidence = 05 -10 bull Avoid pain before during and after surgery lsquohelliphelliptranslate advances in acute pain to chronic settinghelliphelliprsquo bull Psychological pre-assessment bull Education discussion with patients surgeons bull In some cases preventive analgesia may be beneficial bull Transitional Pain Servicehelliptrackinghellipdatabase lsquoPragmatic approachrsquo lsquoAll diseases have an acute phasersquo lsquoDrugs good for acute pain must be good for chronic painrsquo

Outcomes
bull arm shoulder and hand function at 12 months using the 30-item Disability Arm Shoulder Hand (DASH) questionnaire
bull quality of life
bull Functional Assessment of Cancer Treatment-Breast (FACT-B)
bull Short-Form-12 and EQ-5D-5L
bull Data on postoperative adverse events surgical site infection and healthcare resource use will be collected at 6 and 12 months after surgery
Positive therapies for Prevention of PSBP
1 EMLA applied to chest wall prior
to surgery less pain 3 months
Fassoulaki 2000
2 Venlafaxine XR 70mg before
and for 2 weeks post surgeryno diff
acute pain significantly less chronic
pain 6 months
Reuben 2004
3 Aggressive acute pain
management
Iohom 2006
4 Preincisional paravertebral
block
Kairaluoma 2006
5 Multimodal analgesia with
gabapentin EMLA ropivacaine less
acute pain amp pain 6 months
Fassoulaki 2005
Current Treatment Paradigms
The Toronto General Hospital
Transitional Pain Service
development and implementation
of a multidisciplinary program
to prevent chronic postsurgical pain (Katz J Pain Res 2015)
bull Nurse navigator
bull Psychologists (ACT)
Clinical Manifestations hellipour approach to the patient with CPSP
bull Type of pain Cause
bull Exclude other causes (infection recurrence)
bull Psychological and social factors
bull Temporal Context
Electronic Patient Record
Future Directions
bull Identify Causative Modifiable risk factors vs Associative risk factors
bull Measure psychological variables
bull Genetic assays to identify genes controlling the variability in developing chronic pain
Aim is lsquoto identify susceptibility to chronic pain and sensitivity to analgesicsrsquo
Chronic pain lsquoheritabilityrsquo is variable
Conclusions
bull 1 year incidence = 05 -10 bull Avoid pain before during and after surgery lsquohelliphelliptranslate advances in acute pain to chronic settinghelliphelliprsquo bull Psychological pre-assessment bull Education discussion with patients surgeons bull In some cases preventive analgesia may be beneficial bull Transitional Pain Servicehelliptrackinghellipdatabase lsquoPragmatic approachrsquo lsquoAll diseases have an acute phasersquo lsquoDrugs good for acute pain must be good for chronic painrsquo

Positive therapies for Prevention of PSBP
1 EMLA applied to chest wall prior
to surgery less pain 3 months
Fassoulaki 2000
2 Venlafaxine XR 70mg before
and for 2 weeks post surgeryno diff
acute pain significantly less chronic
pain 6 months
Reuben 2004
3 Aggressive acute pain
management
Iohom 2006
4 Preincisional paravertebral
block
Kairaluoma 2006
5 Multimodal analgesia with
gabapentin EMLA ropivacaine less
acute pain amp pain 6 months
Fassoulaki 2005
Current Treatment Paradigms
The Toronto General Hospital
Transitional Pain Service
development and implementation
of a multidisciplinary program
to prevent chronic postsurgical pain (Katz J Pain Res 2015)
bull Nurse navigator
bull Psychologists (ACT)
Clinical Manifestations hellipour approach to the patient with CPSP
bull Type of pain Cause
bull Exclude other causes (infection recurrence)
bull Psychological and social factors
bull Temporal Context
Electronic Patient Record
Future Directions
bull Identify Causative Modifiable risk factors vs Associative risk factors
bull Measure psychological variables
bull Genetic assays to identify genes controlling the variability in developing chronic pain
Aim is lsquoto identify susceptibility to chronic pain and sensitivity to analgesicsrsquo
Chronic pain lsquoheritabilityrsquo is variable
Conclusions
bull 1 year incidence = 05 -10 bull Avoid pain before during and after surgery lsquohelliphelliptranslate advances in acute pain to chronic settinghelliphelliprsquo bull Psychological pre-assessment bull Education discussion with patients surgeons bull In some cases preventive analgesia may be beneficial bull Transitional Pain Servicehelliptrackinghellipdatabase lsquoPragmatic approachrsquo lsquoAll diseases have an acute phasersquo lsquoDrugs good for acute pain must be good for chronic painrsquo

Current Treatment Paradigms
The Toronto General Hospital
Transitional Pain Service
development and implementation
of a multidisciplinary program
to prevent chronic postsurgical pain (Katz J Pain Res 2015)
bull Nurse navigator
bull Psychologists (ACT)
Clinical Manifestations hellipour approach to the patient with CPSP
bull Type of pain Cause
bull Exclude other causes (infection recurrence)
bull Psychological and social factors
bull Temporal Context
Electronic Patient Record
Future Directions
bull Identify Causative Modifiable risk factors vs Associative risk factors
bull Measure psychological variables
bull Genetic assays to identify genes controlling the variability in developing chronic pain
Aim is lsquoto identify susceptibility to chronic pain and sensitivity to analgesicsrsquo
Chronic pain lsquoheritabilityrsquo is variable
Conclusions
bull 1 year incidence = 05 -10 bull Avoid pain before during and after surgery lsquohelliphelliptranslate advances in acute pain to chronic settinghelliphelliprsquo bull Psychological pre-assessment bull Education discussion with patients surgeons bull In some cases preventive analgesia may be beneficial bull Transitional Pain Servicehelliptrackinghellipdatabase lsquoPragmatic approachrsquo lsquoAll diseases have an acute phasersquo lsquoDrugs good for acute pain must be good for chronic painrsquo

Clinical Manifestations hellipour approach to the patient with CPSP
bull Type of pain Cause
bull Exclude other causes (infection recurrence)
bull Psychological and social factors
bull Temporal Context
Electronic Patient Record
Future Directions
bull Identify Causative Modifiable risk factors vs Associative risk factors
bull Measure psychological variables
bull Genetic assays to identify genes controlling the variability in developing chronic pain
Aim is lsquoto identify susceptibility to chronic pain and sensitivity to analgesicsrsquo
Chronic pain lsquoheritabilityrsquo is variable
Conclusions
bull 1 year incidence = 05 -10 bull Avoid pain before during and after surgery lsquohelliphelliptranslate advances in acute pain to chronic settinghelliphelliprsquo bull Psychological pre-assessment bull Education discussion with patients surgeons bull In some cases preventive analgesia may be beneficial bull Transitional Pain Servicehelliptrackinghellipdatabase lsquoPragmatic approachrsquo lsquoAll diseases have an acute phasersquo lsquoDrugs good for acute pain must be good for chronic painrsquo

Future Directions
bull Identify Causative Modifiable risk factors vs Associative risk factors
bull Measure psychological variables
bull Genetic assays to identify genes controlling the variability in developing chronic pain
Aim is lsquoto identify susceptibility to chronic pain and sensitivity to analgesicsrsquo
Chronic pain lsquoheritabilityrsquo is variable
Conclusions
bull 1 year incidence = 05 -10 bull Avoid pain before during and after surgery lsquohelliphelliptranslate advances in acute pain to chronic settinghelliphelliprsquo bull Psychological pre-assessment bull Education discussion with patients surgeons bull In some cases preventive analgesia may be beneficial bull Transitional Pain Servicehelliptrackinghellipdatabase lsquoPragmatic approachrsquo lsquoAll diseases have an acute phasersquo lsquoDrugs good for acute pain must be good for chronic painrsquo

Conclusions
bull 1 year incidence = 05 -10 bull Avoid pain before during and after surgery lsquohelliphelliptranslate advances in acute pain to chronic settinghelliphelliprsquo bull Psychological pre-assessment bull Education discussion with patients surgeons bull In some cases preventive analgesia may be beneficial bull Transitional Pain Servicehelliptrackinghellipdatabase lsquoPragmatic approachrsquo lsquoAll diseases have an acute phasersquo lsquoDrugs good for acute pain must be good for chronic painrsquo