Distributed Data Analytics & Annual Community Health ... Query Health, ... Ross Lazarus Emma...
91
Distributed Data Analytics & Querying: EHR Value to Health Centers & Public Health Moderator: Rick Shoup, PhD Chief Technology Officer, Massachusetts eHealth Institute Jeffrey Brown, PhD Assistant Professor, Department of Population Medicine, Harvard Medical School & the Harvard Pilgrim Health Care Institute Richard Elmore Coordinator, Query Health, Office of the National Coordinator for Health Information, US Department of Health & Human Services Michael Klompas, MD, MPH Department of Population Medicine, Harvard Medical School & the Harvard Pilgrim Health Care Institute Joshua Vogel, MPH Epidemiologist/Data Analyst, Massachusetts Department of Public Health Annual Community Health Institute May 9-11, 2012 Resort & Conference Center of Hyannis Hyannis, MA
Transcript of Distributed Data Analytics & Annual Community Health ... Query Health, ... Ross Lazarus Emma...

Distributed Data Analytics &
Querying: EHR Value to Health
Centers & Public Health
Moderator:
Rick Shoup, PhD
Chief Technology Officer, Massachusetts eHealth Institute
Jeffrey Brown, PhD Assistant Professor, Department of Population Medicine, Harvard Medical School & the Harvard Pilgrim Health Care Institute
Richard Elmore Coordinator, Query Health, Office of the National Coordinator for Health Information, US Department of Health & Human Services
Michael Klompas, MD, MPH Department of Population Medicine, Harvard Medical School & the Harvard Pilgrim Health Care Institute
Joshua Vogel, MPH Epidemiologist/Data Analyst, Massachusetts Department of Public Health
Annual Community Health Institute
May 9-11, 2012
Resort & Conference Center of Hyannis
Hyannis, MA
PHIConnect CDC Center of Excellence in Public Health Informatics
Michael Klompas MD, MPH, FRCPC CDC Center of Excellence in Public Health Informatics
Harvard Medical School and Harvard Pilgrim Health Care Institute Boston, MA
Community Health Institute May 9, 2012
Electronic Support for Public Health Public Health Surveillance Platform

PHIConnect CDC Center of Excellence in Public Health Informatics
Outline
Background on ESP
Case identification strategies
Reportable diseases
Syndromic surveillance
Chronic diseases

PHIConnect CDC Center of Excellence in Public Health Informatics
“No health department, State or local, can effectively prevent or
control disease without knowledge of when, where, and under what conditions cases are occurring”
Introductory statement printed each week in Public Health Reports, 1913-1951

PHIConnect CDC Center of Excellence in Public Health Informatics
PHIConnect CDC Center of Excellence in Public Health Informatics
Software and architecture to extract, analyze, and transmit electronic health information from providers to public health.
Surveys codified electronic health record data for patients with conditions of public health interest
Generates secure electronic reports for the state health department
Designed to be compatible with any EHR system
JAMIA 2009;16:18-24 MMWR 2008;57:372-375
Advances Disease Surveillance 2007;3:3
Electronic Support for Public Health (ESP)
PHIConnect CDC Center of Excellence in Public Health Informatics
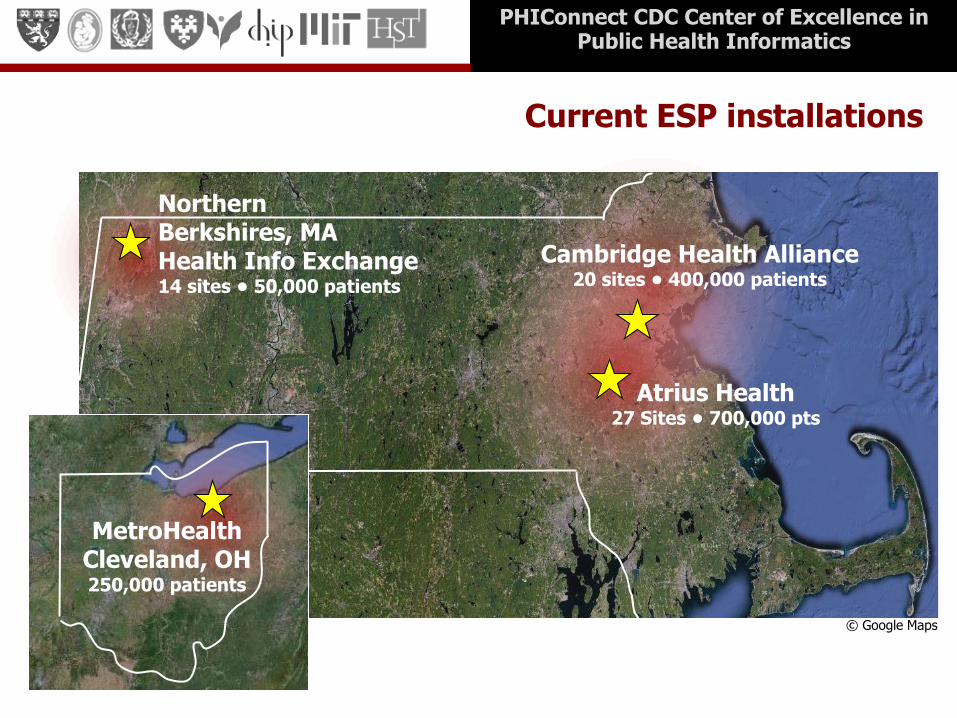
Current ESP installations
Northern Berkshires, MA Health Info Exchange 14 sites • 50,000 patients
Atrius Health 27 Sites • 700,000 pts
© Google Maps
Cambridge Health Alliance 20 sites • 400,000 patients
MetroHealth Cleveland, OH 250,000 patients

PHIConnect CDC Center of Excellence in Public Health Informatics
esphealth.org
Source code and documentation available
free of charge from esphealth.org
PHIConnect CDC Center of Excellence in Public Health Informatics
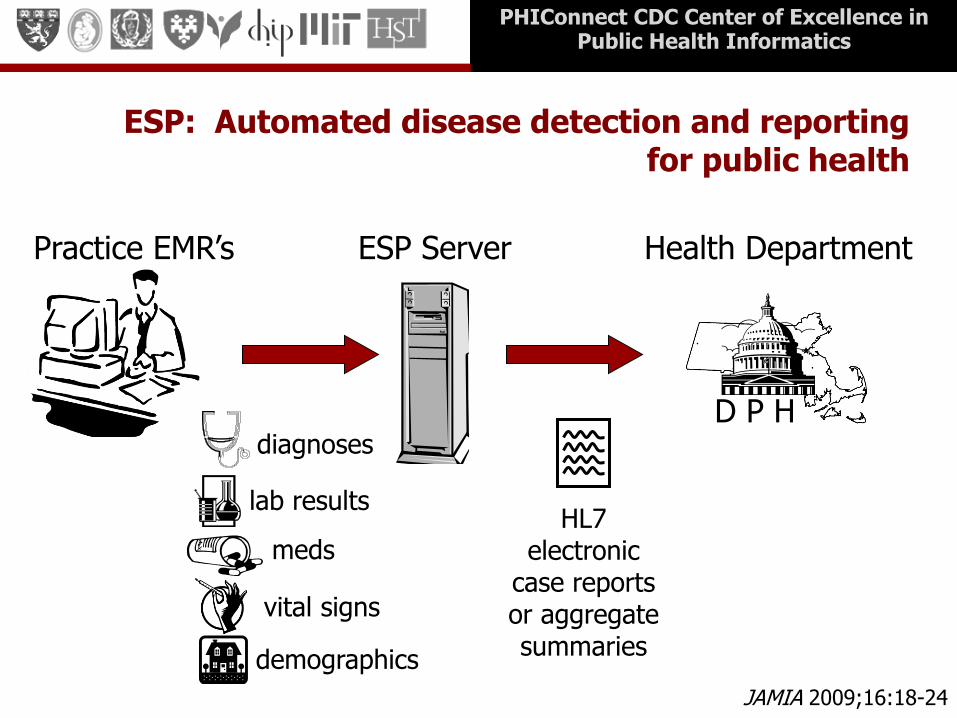
Practice EMR’s ESP Server
D P H
Health Department
HL7 electronic
case reports or aggregate summaries
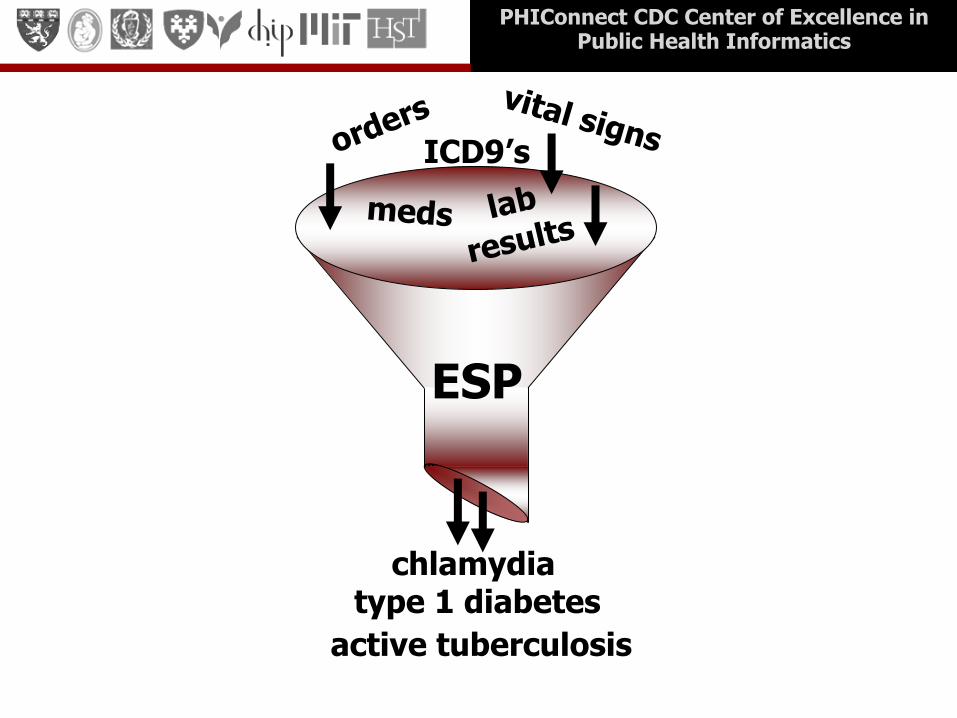
ESP: Automated disease detection and reporting for public health
diagnoses
lab results
meds
demographics
vital signs
JAMIA 2009;16:18-24
PHIConnect CDC Center of Excellence in Public Health Informatics
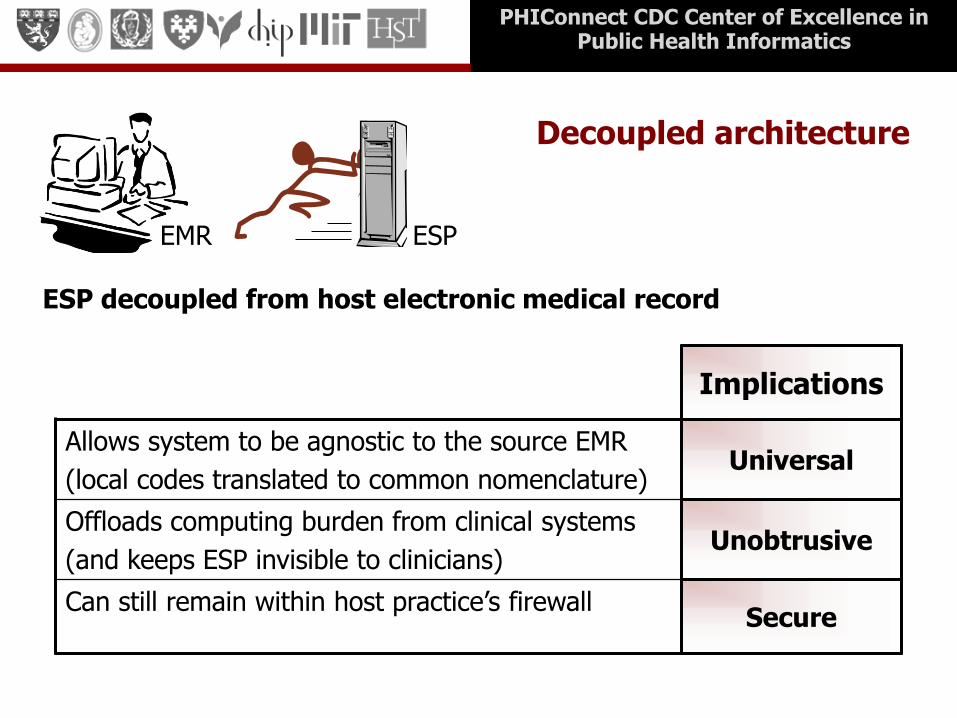
Decoupled architecture
ESP decoupled from host electronic medical record
Implications
Allows system to be agnostic to the source EMR
(local codes translated to common nomenclature) Universal
Offloads computing burden from clinical systems
(and keeps ESP invisible to clinicians) Unobtrusive
Can still remain within host practice’s firewall
Secure
EMR ESP
PHIConnect CDC Center of Excellence in Public Health Informatics
CASE IDENTIFICATION
PHIConnect CDC Center of Excellence in Public Health Informatics
ICD9’s
chlamydia type 1 diabetes
active tuberculosis
ESP

PHIConnect CDC Center of Excellence in Public Health Informatics
Case Identification Limitations of ICD9’s
Condition Sensitivity
Positive
Predictive
Value
Acute hepatitis C 63% 22%
Tuberculosis 100% 17%
Postherpetic neuralgia 59% 84%
Gestational diabetes 91% 53%

PHIConnect CDC Center of Excellence in Public Health Informatics
Case Identification Limitations of lab tests
Blind to purely clinical diagnoses
e.g. culture negative TB, early Lyme, PID
Multiple reports for same episode
e.g. hepatitis C
Poor discriminator between active & resolved, acute & chronic disease
e.g. acute vs chronic hep B, current vs remote Lyme

PHIConnect CDC Center of Excellence in Public Health Informatics
Solution
Integrate multiple streams of data from the EMR to increase sensitivity and specificity
Lab orders
Lab results (present and past)
ICD9 diagnoses (present and past)
Medication prescriptions
PHIConnect CDC Center of Excellence in Public Health Informatics
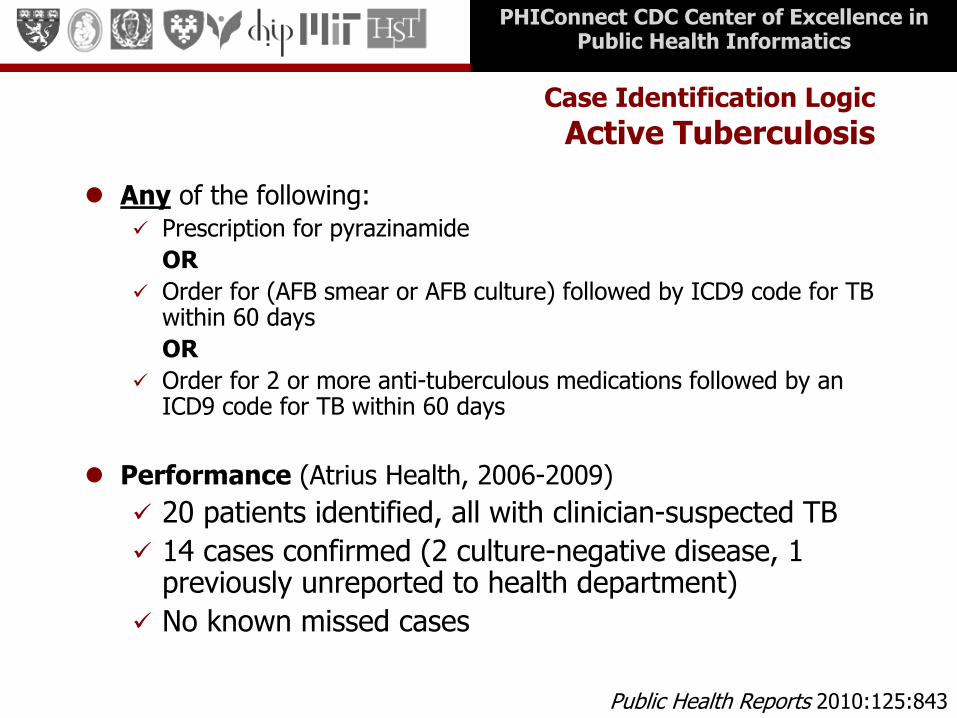
Case Identification Logic
Active Tuberculosis
Any of the following: Prescription for pyrazinamide
OR
Order for (AFB smear or AFB culture) followed by ICD9 code for TB within 60 days
OR
Order for 2 or more anti-tuberculous medications followed by an ICD9 code for TB within 60 days
Performance (Atrius Health, 2006-2009)
20 patients identified, all with clinician-suspected TB
14 cases confirmed (2 culture-negative disease, 1 previously unreported to health department)
No known missed cases
Public Health Reports 2010:125:843

PHIConnect CDC Center of Excellence in Public Health Informatics
Case Identification Logic:
Acute Hepatitis B
Both of the following:
ICD9 for jaundice OR liver function tests > 5x normal
IgM to core antigen
OR
All four of the following:
ICD9 for jaundice OR liver function tests > 5x normal
Hep B surface antigen or ‘e’ antigen present
No prior positive Hep B specific lab tests
No present or prior ICD9 code for chronic hepatitis B
PLoS ONE 2008:3:e2626
Sensitivity: 99% PPV: 97%

PHIConnect CDC Center of Excellence in Public Health Informatics
Sorting through positive Hep B Results - ESP versus ELR
601 distinct patients
8 acute
593 chronic cases
2648 positive test results for hepatitis B
PHIConnect CDC Center of Excellence in Public Health Informatics
INFECTIOUS DISEASE CASE REPORTING

PHIConnect CDC Center of Excellence in Public Health Informatics
ESP Case Reporting Atrius Health and MetroHealth, June 2006-July 2011
Condition Total Cases
Chlamydia 10,406
Gonorrhea 2,056
Pelvic inflammatory disease 122
Acute hepatitis A 21
Acute hepatitis B 56
Acute hepatitis C 74
Tuberculosis 168
Syphilis 313

PHIConnect CDC Center of Excellence in Public Health Informatics
Manual versus electronic reporting Atrius Health (variable time periods)
Manual
Reports* ESP Change
Chlamydia 545 758 39%
Gonorrhea 62 95 53%
Pelvic Inflammatory Disease 0 25
Acute Hepatitis B 3 8 140%
Acute Hepatitis C 14 38 150%
Tuberculosis 13 14 8%
MMWR 2008;57:372-375 PLoS ONE 2008;e2626
Public Health Reports 2010;125:843
PHIConnect CDC Center of Excellence in Public Health Informatics
SYNDROMIC SURVEILLANCE
PHIConnect CDC Center of Excellence in Public Health Informatics
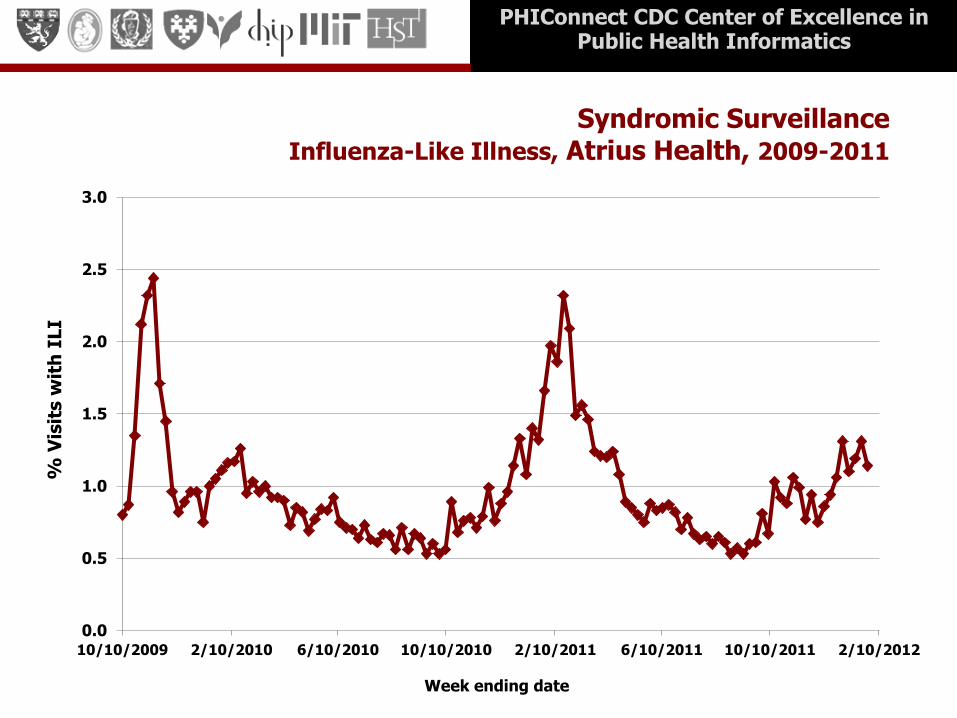
Syndromic Surveillance Influenza-Like Illness, Atrius Health, 2009-2011
0.0
0.5
1.0
1.5
2.0
2.5
3.0
10/10/2009 2/10/2010 6/10/2010 10/10/2010 2/10/2011 6/10/2011 10/10/2011 2/10/2012
% V
isit
s w
ith
ILI
Week ending date

PHIConnect CDC Center of Excellence in Public Health Informatics
CHRONIC DISEASE SURVEILLANCE
PHIConnect CDC Center of Excellence in Public Health Informatics
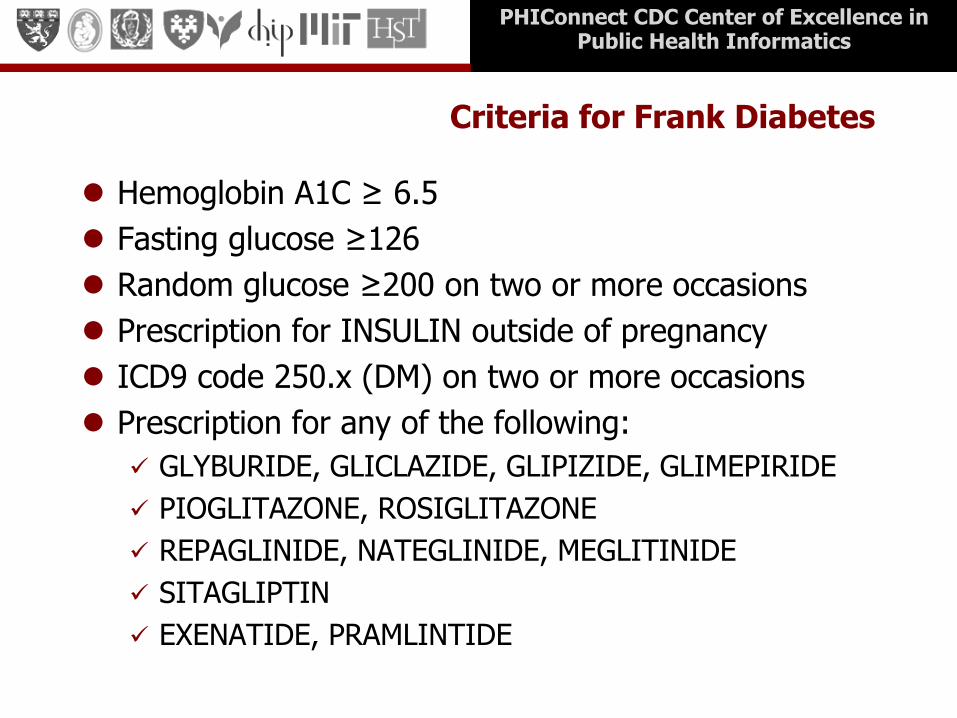
Criteria for Frank Diabetes
Hemoglobin A1C ≥ 6.5
Fasting glucose ≥126
Random glucose ≥200 on two or more occasions
Prescription for INSULIN outside of pregnancy
ICD9 code 250.x (DM) on two or more occasions
Prescription for any of the following:
GLYBURIDE, GLICLAZIDE, GLIPIZIDE, GLIMEPIRIDE
PIOGLITAZONE, ROSIGLITAZONE
REPAGLINIDE, NATEGLINIDE, MEGLITINIDE
SITAGLIPTIN
EXENATIDE, PRAMLINTIDE

PHIConnect CDC Center of Excellence in Public Health Informatics
Summarizing and sharing data: The RiskScape
Web-based interface that automatically displays and analyze chronic disease surveillance data derived from electronic health records
Helps users easily visualize and manipulate surveillance data in order to rapidly identify outliers and trends
Designed to be commensurate with the unique strengths of the data
Electronic and analysis ready
Timely (updated daily)
Clinically rich – includes clinician-measured demographics, vitals (height, weight, blood pressure), lab tests, medications, vaccines, and outcomes

PHIConnect CDC Center of Excellence in Public Health Informatics
Select an Outcome

PHIConnect CDC Center of Excellence in Public Health Informatics
Add Filters (optional)

PHIConnect CDC Center of Excellence in Public Health Informatics
Automatically Map Prevalence by Zip

PHIConnect CDC Center of Excellence in Public Health Informatics
Automatically stratify by age, sex, race, BMI, BP, etc.
Prevalence of type 2 diabetes remains correlated with age in young people
Type 2 diabetes more prevalent in males versus females in people under age 40

PHIConnect CDC Center of Excellence in Public Health Informatics
Hone in on Areas of Particular Interest

PHIConnect CDC Center of Excellence in Public Health Informatics
Hone in on Areas of Particular Interest
Prevalence of type 2 diabetes amongst people under age 40 is 1.0% in this
zipcode versus 0.26% in the full state
PHIConnect CDC Center of Excellence in Public Health Informatics
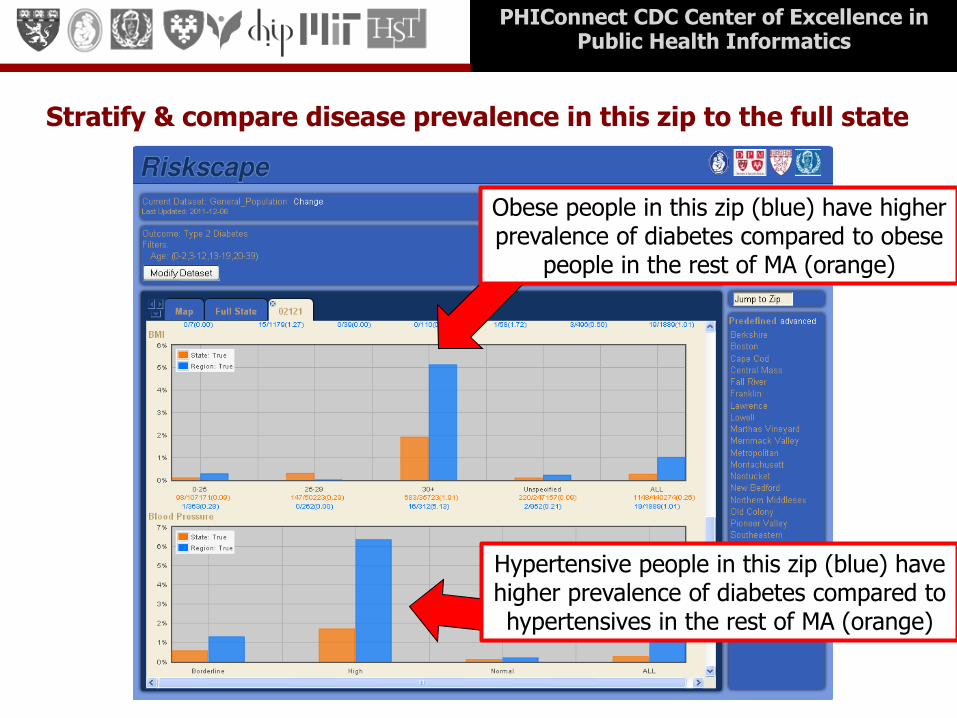
Stratify & compare disease prevalence in this zip to the full state
Obese people in this zip (blue) have higher prevalence of diabetes compared to obese
people in the rest of MA (orange)
Hypertensive people in this zip (blue) have higher prevalence of diabetes compared to hypertensives in the rest of MA (orange)

PHIConnect CDC Center of Excellence in Public Health Informatics
Evaluate whether patients are meeting clinical targets
57% of people with type 2 diabetes have high blood pressure
51% of people with type 2 diabetes have a hemoglobin A1C above 6.5

PHIConnect CDC Center of Excellence in Public Health Informatics
Obesity (BMI >30) in Eastern Massachusetts
PHIConnect CDC Center of Excellence in Public Health Informatics
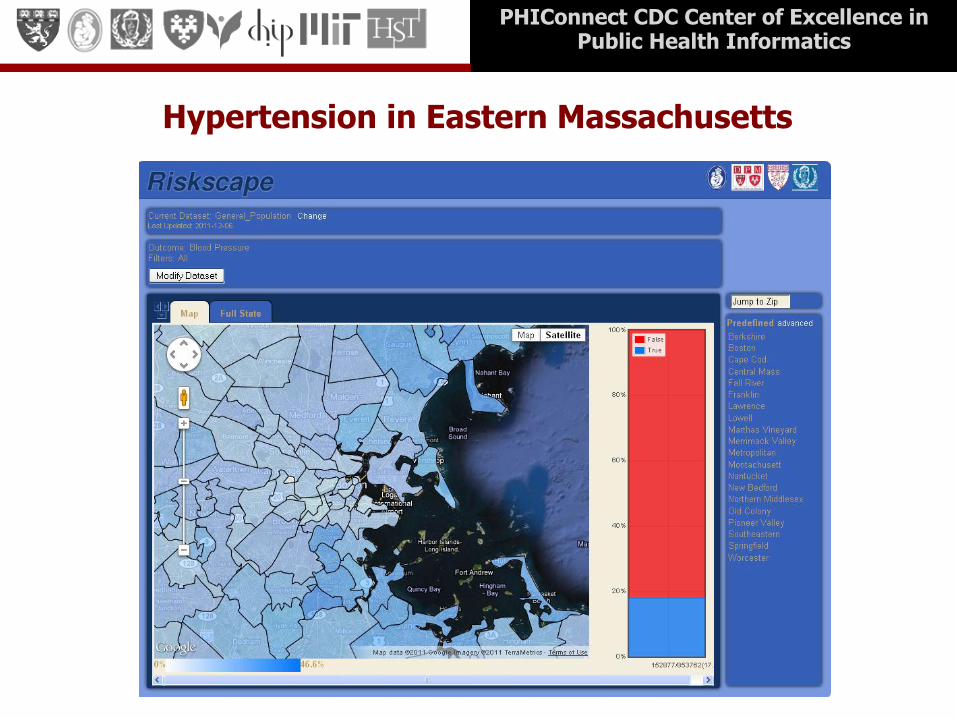
Hypertension in Eastern Massachusetts
PHIConnect CDC Center of Excellence in Public Health Informatics
Summary
Electronic health record systems can facilitate real-time, automated public health surveillance
Automated mapping and stratification can identify geographic areas and subpopulations at increased risk of disease
Potential populations for targeted health interventions
Future Steps:
Increase the number of outcomes and clinical parameters available for display in RiskScape
Add in automated cluster detection using SatScan
Create a distributed network of ESP sites…

PHIConnect CDC Center of Excellence in Public Health Informatics
ESP Team
Harvard Dept of Population Medicine
Richard Platt
Ross Lazarus
Emma Eggleston
Julie Lankiewicz
Michael Murphy
Massachusetts Dept of Public Health Patricia Daly Paul Oppedisano Gillian Haney Josh Vogel
Ohio Department of Health
Lilith Tatham
MetroHealth, OH
David Kaelber
Guptha Baskaran Atrius Health Ben Kruskal Mike Lee
Cambridge Health Alliance Michelle Weiss Brian Herrick Northern Berkshires eHealth Collaborative Don LeBreux
Commonwealth Informatics
Contact: [email protected]

PHIConnect CDC Center of Excellence in Public Health Informatics
MDPHnet Distributed Data Approach
39
Jeffrey Brown, PhD May 9, 2012

Overview
• Background: Approach to Distributed Querying
• Distributed Networks
• Implementing MDPHNet
• MDPHNet Demonstration
40

Approach to Distributed Querying
41

• Data partners maintain control of their data
• Data partners’ ongoing involvement is needed to interpret findings
• Little or no exchange of person-level data is needed
• Secondary use can’t interfere with primary use
• Few data elements are needed to answer most questions
• Sharing computer programs rather than protocols reduces effort and improves consistency
Distributed Querying Guiding Principles
42

• Data partners keep and analyze their own data
• Standardize the data using a common data model
• Distribute code to partners for local execution
• Provide results, not data, to requestor
43
Distributed Data/ Distributed Analysis
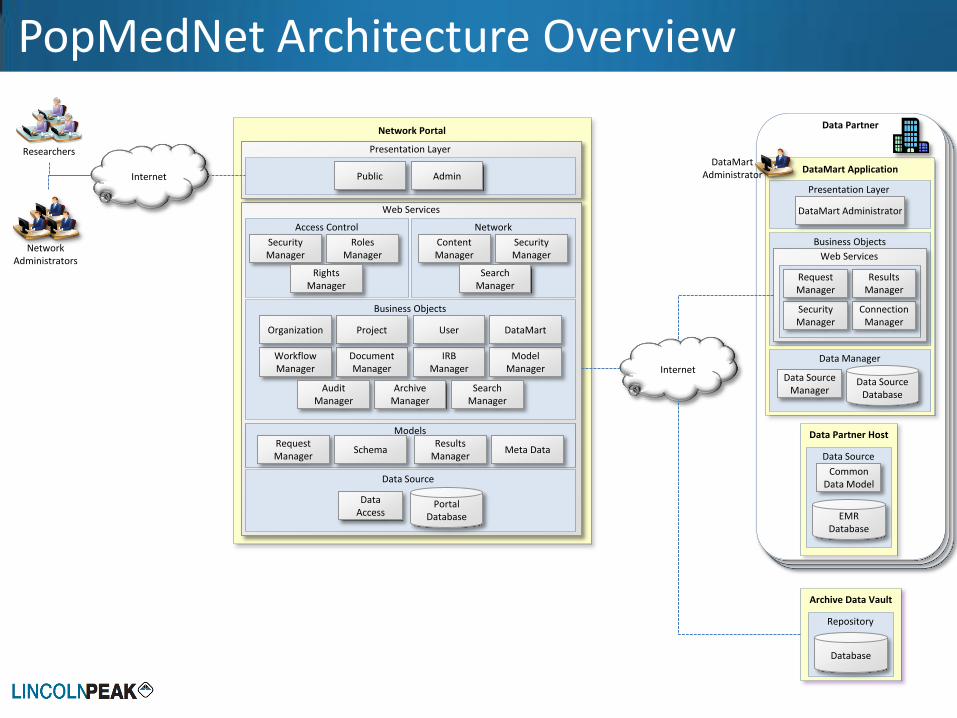
PopMedNet Architecture Overview
Internet
Archive Data Vault
Repository
Database
Web Services
Document Manager
IRB Manager
Model Manager
Workflow Manager
Project Organization User DataMart
Archive Manager
Search Manager
Audit Manager
Request Manager
Schema Results
Manager Meta Data
Business Objects
Security Manager
Roles Manager
Rights Manager
Access Control
Data Source
Data Access
Portal Database
Network Portal
Presentation Layer
Content Manager
Security Manager
Search Manager
Network
Models
Public Admin DataMart Application
Business Objects
Web Services
Connection Manager
Security Manager
Results Manager
Request Manager
Presentation Layer
DataMart Administrator
Data Manager
Data Source Manager
Data Source Database
Data Partner
Data Partner Host
Data Source
Common Data Model
EMR Database
DataMart Administrator
Network Administrators
Researchers
Internet

Technical Protocols and Overview - 1
• Network Portal
– Multi-tiered .NET MS SQL Server application
– Access via HTTPS
– Communications via Web Services
– Role / rights based access
• Hosting and support
– Hosted in a Tier III SAS 70 FISMA certified data center
– Redundant infrastructure
– 99.9% Application uptime SLA
– SAN based data storage & backup
– Remote data replication
– Secure VPN administration via RSA token ID
45
Technical Protocols and Overview - 2
• DataMart Client application
– Small footprint
– Easy to install on desktop or server
– Developed in C#
– Connects to any ODBC compliant data source
– Software updates downloaded from network portal
46
PopMedNet Design Features
• Any data model from any source
• Flexible and secure distributed querying
– Execution of custom analytic code
– Menu-driven queries
• Role-based access control
• Data partner autonomy
• Query execution options range from fully automated to manual
• Auditing
• Software-enabled governance
47

• Secure, private multi-center research network
• Open source application
• Data partners maintain control of their data
• Flexible governance, access control, permissions, auditing
• Secure FISMA-compliant platform
• Mature documentation and set-up procedures
• Scalable: easy to add new data, new partners
• Interoperable with other PopMedNet networks
48
PopMedNet Implementation Features

49
Security Features • FISMA compliant tier III data center
• 3rd-party secure audit completed – Enhanced system procedures
• Securely store credentials as Salted Hashes
• No maximum password length, require expiration, enforce history
• Use cryptographically secure random values for session IDs (.Net Type 4 GUID)
• Cookies marked as ‘SECURE’, ‘SESSION’ & ‘HTTPONLY’ and the cookie domain
– Transmission
• Require/force Secure Socket layer (SSL) for all communications
• Enable strongest cipher suites and Transport Layer Security (TLS) versions
– Web Service and Portal Authorization
• Ensure all submissions are performed via POST method
• Do not publish WSDL
• Limit the number and size of file submissions
• Passed multiple independent security audits and penetration tests

Existing Networks
50
• SPAN: Scalable PArtnering Network for CER (AHRQ) – ADHD, Obesity
• PEAL: Population-Based Effectiveness in Asthma and Lung Diseases Network (AHRQ)
• Mini-Sentinel (FDA) – Safety of marketed medical products
• HMO Research Network
• MDPHNet (ONC): MA Department of Public Health
• ONC QueryHealth Pilots (planned)
PopMedNet Networks
51

PopMedNet and National Standards
• PMN is a key component of the ONC’s QueryHealth Initiative
• ONC national standard for distributed querying
– QueryHealth Initiative uses PMN as the distributed querying platform for policy and governance
• Standards & Interoperability (S&I) Framework: http://wiki.siframework.org/Home
52

QueryHealth – Query Lifecycle
53

PopMedNet Website
54
www.popmednet.org

Implementing MDPHNet
55

Implementing MDPHnet 1. Implement the common data model (ESP)
2. Store files is relational DB (need ODBC connection)
3. Establish settings on the Network secure portal
– Notifications
– Permissions
4. Install the PopMedNet DataMart Client on local system
5. Establish settings on the DM Client software (logins, data connection)
6. Respond to queries via the DM Client
56

MDPHnet Features
1. Menu Driven Querying of ESP Data Model
2. Project Based Network Management
3. Granular Access Control
4. Scheduled Reports
57

1. Menu Driven Query Capability
• Customizable reporting template (menu-driven)
• Menu-driven query interface can identify cohorts of interest based on inclusion and exclusion criteria and Boolean operators
– Time window
– Demographics
– Diagnoses
• Query interface generates standardized executable code for distribution to sites
58
EXAMPLE: Identify and characterize a cohort of patients with a diagnosis of asthma in 2010

2. Project Based Network Management
• Organizational entity “Projects” will be developed
• Combined with users, organizations, and query types, “projects” give more precise query authorization control and role-based access control
• Assigns roles based on projects, thus allowing a user to have multiple roles under a single login credential.
EXAMPLE
Establish projects for ILI and diabetes, assigning specific users, query types, and queries to each project. Users create and distribute queries based on their role within a project, and query response determined based on those factors
59

3. Granular Access Control
Fine-grained control of query authorization that allows data partners to give permission to execute queries to individual users for specific query types and projects
EXAMPLE
Data partner gives specific MDPH staff permission for automated execution of queries for a specified project (e.g., ILI), but would require manual review of the same query coming from a different user, or the same user for a different project
60

4. Scheduled Reports
Capability to
– Store a query
– Schedule routine distribution of the query
– Data partners to specify how they will be processed
EXAMPLE
As part of the ILI project, MDPH develops a query for distribution every Monday morning. Data partners determine how to process the query (manually or automatically) based on the project, user, and query.
61

MDPHnet Demonstration
62

PopMedNet™ Login
63
PopMedNet™ Demonstration Portal

MDPHnet Home Page
65

Request Summary Page
66

Request Selector Dialog Box
67

Request Detail Page
68

ICD-9 Code Selector
69

Request DataMart Routing
70

DataMart Client Application
71

DataMart Client Request Detail
72

DataMart Client Request Detail
73

Response Detail/Results Page
74

Response Detail/Results Page
75

Response Detail/Results Page
76
Thank You
77

Distributed Population Queries – National Strategies
Rich Elmore, Coordinator – Query Health
May 2012
Vision
Enable a learning health system to understand population measures of health, performance, disease and quality, while respecting patient privacy, to improve patient and population health and reduce costs.

Distributed queries unambiguously define a population from a larger set
Questions about
disease outbreaks,
prevention activities,
health research,
quality measures, etc.

Distributed Query Networks Voluntary, No Central Planning
Community of participants that voluntarily
agree to interact with each other. There will be
many networks; requestors and responders may
participate in multiple networks.
Requestors Participating
Responders
Query

Query Health Pilots
Pilot Focus RI Queries
RI Policy Layer
Data Sources Kickoff
NYC & NYS Depts. of Public Health
Diabetes (NYC) Hypertension (NYS)
i2b2 PMN RHIOs (Intersystems & Axolotl) EHRs (eCW to start)
May 2012
FDA Mini-Sentinel
Use of clinical data sources for FDA questions
PMN PMN i2b2/Beth Israel June 2012
CDC Front-end to Bio-Sense 2
TBD TBD Bio-Sense 2 June 2012
Mass. Dept. of Public Health
Diabetes PMN PMN MDPHNet July 2012
CQM Quality Measures
hQuery PMN EHR Vendor July 2012

NYS DOH
NYC PCIP
Information Requestors
Data Sources
Axolotl RHIO
Inter-systems
RHIO
eCWEHR
Sends Query to Data Sources
Distributes Query Results to Information Requestor
New York City / New York State
Pilot
Sends Query to Data Sources
Distributes Query Results to Information Requestor

Vocabulary &
Code Sets
Develop modular, testable portfolio of Query Health standards and specifications that
can adopted by the industry, and support key HITECH and govt. priorities
Content
Structure
Queries &
Responses
Privacy &
Security
Foundation:
Distributed
Query
Solutions
SNOMED-CT
Clinical Element
Data Dictionary
i2b2
The Results
New QRDA 2 & 3
PopMedNet
LOINC ICD-10 RxNorm
84
Query Health Standards and Reference Implementation Stack
Reference
Implementation
Stack
The Question New HQMF
Query Envelope Privacy Policy
Enablement
hQuery
The Query New HQMF
• Health Quality Measure Format
• HQMF newly modified to support the needs for dynamic population queries:
– More executable
– Simplified
• Advantages for query
– Avoids “yet another standard”
– Secure (vs procedural approach)
– Works across diverse platforms
• Benefits – Speed and Cost

The Query Envelope
• Query agnostic
• Content agnostic
• Metadata facilitates privacy guidance from HIT Policy Committee
• RESTful interface specification

The Data Clinical Element Data Dictionary
87
– Demographic
– Patient Contact Information
– Payer Information
– Healthcare Provider
– Allergies & Adverse Reactions
– Encounter
– Surgery
– Diagnosis
– Medication
– Procedure
– Immunization
– Advance Directive
– Vital Signs
– Physical Exam
– Family History
– Social History
– Order
– Result
– Medical Equipment
– Care Setting
– Enrollment
– Facility
• ONC S&I Framework deliverable
• Standards independent dictionary

The Results New QRDA
• Quality Reporting Document Architecture
– Category I – Patient Level
– Category II – Patient Populations
– Category III – Population Measures

Operational Guidance
U.S. Health and Human Services Office of the National Coordinator for Health IT
Standards & Interoperability Framework Query Health Technical Approach Operational Guidelines March 26, 2012

Query Health How it works together
90

The path to critical mass
91
• Today, distributed queries are generally limited to organizations with large IT & research budgets
• Missing: Primary Care, FQHCs, CAHs, HIEs, etc… In other words, most places where clinical care is delivered and recorded
• MDPHNet is strategically important