Different Modalities in First Stage Enhancement of Labor
4
Different Modalities in First Stage Enhancement of Labor Mahmoud Edessy Professor and head of Obstet. & Gynecol. Depart. Faculty of Medicine- Al-Azhar University –Assiut, Egypt. Abd El-Aziz G. EL-Darwish Professor of Obstet. & Gynecol. Depart. Faculty of Medicine- Al-Azhar University –Assiut, Egypt. Ahmed A.M. Nasr Assistant Professor of Obstet. & Gynecol. Depart. Faculty of Medicine- Al-Azhar University –Assiut, Egypt. Abd El-Naser Abd El-Gaber Ali Assistant Professor of Obstet. & Gynecol. Depart. Faculty of Medicine- Al-Azhar University –Assiut, Egypt. Hosam El-Katatny Assistant Professor of Obstet. & Gynecol. Depart. Faculty of Medicine- Al-Azhar University –Assiut, Egypt. M. Tammam MBBCH *Corresponding author: [email protected] Keywords Abstract First stage of labor Drotaverine Hyoscine N-Butylbromide Metoclopramide BACKGROUND: Prolonged labor is one of the most important risk factors for perinatal compromise and, if caused by obstructed labor, it carries the risk of uterine rupture, postpartum hemorrhage [PPH], puerperal sepsis, and maternal death. TYPE OF STUDY: A double-blind, randomized, controlled clinical trial. OBJECTIVE: This study aimed to find out the effect of Drotaverine, Hyoscine-N-Butylbromide and Metoclopramide on enhancement of first stage of labor. SETTING: Obstetrics and Gynecology Departments of Al-Azhar university [Assiut] and Sohag general hospitals. DURATION: From October 2012 to July 2013. PATIENTS&METHDS: 200 full term primigravidae in labor [3-4cm dilation of internal os with regular progressive uterine contractions 3-4 per 10 minutes, each lasting for at least 40 seconds] were recruited to this study. Patients were divided into four groups [50 patients for each group]: Group I: Received [40mg] drotaverine hydrochloride slowly intravenously. Group II: Received [20mg] hyoscine-n-butylbromide slowly intravenously. Group III: Received [20mg] metoclopramide slowly intravenously. Group IV [control]: Received Sterile water for injection [placebo]. RESULTS: There was no statistically significant difference among studied groups as regard to maternal age, BMI, GA, cervical dilatation and cervical effacement at start of study with p value > 0.05. There were highly statistically significant differences among groups as regard to durations of 1st stage of labor, cervical dilatation after start of study and amount of oxytocin augmentation used with p value <0.001. There were moderately significances as regard to neonatal outcome [APGAR score and NICU admission] with p value <0.01 but there was no statistically significant difference among studied groups as regard to, duration of 2nd stage of labor, mode of delivery and birth weight with p value > 0.05. There were mildly statistically significant differences among groups in degree of labor pain and maternal adverse effects of drugs used in this study with p value < 0.05. CONCLUSION: All drugs used in this study had significant effects on shortening of 1st stage of labor with better neonatal outcome but Drotaverine hydrochloride had the upper hand as it was more effective beside it had the strongest labor pain relieve and lesser maternal adverse effects. RECOMMENDATIONS: We recommend using Drotaverine hydrochloride routinely in enhancing first stage of labor as it cheap, effective with mild significant maternal adverse effects. More randomized trials on a larger scale are needed to evaluate the utility and safety of these drugs in labor. 1. Introduction Labor is a natural physiological process characterized by progressive increase in frequency, intensity and duration of uterine contractions, effacement and dilatation of cervix with descent of the fetus through the birth canal [1]. Prolonged labor is one of the most important risk factors for perinatal compromise and, if caused by obstructed labor, it carries the risk of uterine rupture, postpartum hemorrhage [PPH], puerperal sepsis, and maternal death [2]. The two major factors that determine duration of labor are uterine contractility and rate of cervical dilation. In addition to mechanical factors such as sweeping of membranes, cervical stretching [3] and amniotomy [4] various pharmacological agents have been found to facilitate cervical dilation. The role of oxytocin and prostaglandins has been established worldwide in augmentation of labor [5] and the cervical application of hyaluronidase has also been used with some success [6].The cervix is made up of only 10 to 15 percent smooth muscle with the remaining tissue comprised primarily of extracellular connective tissue. Constituents of the latter include type I, III, and IV collagen, glycosaminoglycans, proteoglycans, and elastin [7]. Cervical softening results from increased vascularity, stromal hypertrophy, glandular hypertrophy and hyperplasia, and compositional or structural changes of the extracellular matrix [8]. Drotaverine is highly effective in reducing the duration of active phase of labor by hastening cervical dilatation, more effective when given in more dilated cervix than with less dilatation and more effective in multigravida than in primigravida. There was no interference with uterine contractility and no increase in operative delivery. It reduces the incidence of traumatic postpartum hemorrhage by reducing the incidence of cervical tear. It is a safe drug for the mother as well as for the baby [9]. Only one study was found which looked at hyoscine-n-butylbrmide primarily as an analgesic for the pain associated with labor. The study was shown that intravenous Hyoscine-N-butylbromide smoothens the passage of labor effects by affording pain relive of up to 36% and also shortening the duration of active phase without any fetal or maternal complications [10]. Aim of the Work: This study aimed to find out the effect of Drotaverine, Hyoscine-N-Butylbromide and Metoclopramide on enhancement of first stage of labor. Gen. Health Med. Sci., Vol(2), No (1), February, 2015. pp. 1-4 TI Journals General Health and Medical Sciences www.tijournals.com ISSN: 2409-9856 Copyright © 2015. All rights reserved for TI Journals.
-
Upload
ti-journals-publishing -
Category
Documents
-
view
7 -
download
1
description
BACKGROUND: Prolonged labor is one of the most important risk factors for perinatal compromise and, if caused by obstructed labor, it carries the risk of uterine rupture, postpartum hemorrhage (PPH), puerperal sepsis, and maternal death.TYPE OF STUDY: A double-blind, randomized, controlled clinical trial. OBJECTIVE: This study aimed to find out the effect of Drotaverine, Hyoscine-N-Butylbromide and Metoclopramide on enhancement of first stage of labor. SETTING: Obstetrics and Gynecology Departments of Al-Azhar university (Assiut) and Sohag general hospitals. DURATION: From October 2012 to July 2013. PATIENTS&METHDS: 200 full term primigravidae in labor (3-4cm dilation of internal os with regular progressive uterine contractions 3-4 per 10 minutes, each lasting for at least 40 seconds) were recruited to this study. Patients were divided into four groups (50 patients for each group): Group I: Received (40mg) drotaverine hydrochloride slowly intravenously. Group II: Received (20mg) hyoscine-n-butylbromide slowly intravenously. Group III: Received (20mg) metoclopramide slowly intravenously. Group IV (control): Received Sterile water for injection (placebo). RESULTS: There was no statistically significant difference among studied groups as regard to maternal age, BMI, GA, cervical dilatation and cervical effacement at start of study with p value > 0.05. There were highly statistically significant differences among groups as regard to durations of 1st stage of labor, cervical dilatation after start of study and amount of oxytocin augmentation used with p value 0.05. There were mildly statistically significant differences among groups in degree of labor pain and maternal adverse effects of drugs used in this study with p value CONCLUSION: All drugs used in this study had significant effects on shortening of 1st stage of labor with better neonatal outcome but Drotaverine hydrochloride had the upper hand as it was more effective beside it had the strongest labor pain relieve and lesser maternal adverse effects. RECOMMENDATIONS: We recommend using Drotaverine hydrochloride routinely in enhancing first stage of labor as it cheap, effective with mild significant maternal adverse effects. More randomized trials on a larger scale are needed to evaluate the utility and safety of these drugs in labor.
Transcript of Different Modalities in First Stage Enhancement of Labor

Different Modalities in First Stage Enhancement of Labor Mahmoud Edessy Professor and head of Obstet. & Gynecol. Depart. Faculty of Medicine- Al-Azhar University –Assiut, Egypt. Abd El-Aziz G. EL-Darwish Professor of Obstet. & Gynecol. Depart. Faculty of Medicine- Al-Azhar University –Assiut, Egypt. Ahmed A.M. Nasr Assistant Professor of Obstet. & Gynecol. Depart. Faculty of Medicine- Al-Azhar University –Assiut, Egypt. Abd El-Naser Abd El-Gaber Ali Assistant Professor of Obstet. & Gynecol. Depart. Faculty of Medicine- Al-Azhar University –Assiut, Egypt. Hosam El-Katatny Assistant Professor of Obstet. & Gynecol. Depart. Faculty of Medicine- Al-Azhar University –Assiut, Egypt. M. Tammam MBBCH *Corresponding author: [email protected] Keywords Abstract First stage of labor Drotaverine Hyoscine N-Butylbromide Metoclopramide
BACKGROUND: Prolonged labor is one of the most important risk factors for perinatal compromise and, if caused by obstructed labor, it carries the risk of uterine rupture, postpartum hemorrhage [PPH], puerperal sepsis, and maternal death. TYPE OF STUDY: A double-blind, randomized, controlled clinical trial. OBJECTIVE: This study aimed to find out the effect of Drotaverine, Hyoscine-N-Butylbromide and Metoclopramide on enhancement of first stage of labor. SETTING: Obstetrics and Gynecology Departments of Al-Azhar university [Assiut] and Sohag general hospitals. DURATION: From October 2012 to July 2013. PATIENTS&METHDS: 200 full term primigravidae in labor [3-4cm dilation of internal os with regular progressive uterine contractions 3-4 per 10 minutes, each lasting for at least 40 seconds] were recruited to this study. Patients were divided into four groups [50 patients for each group]: Group I: Received [40mg] drotaverine hydrochloride slowly intravenously. Group II: Received [20mg] hyoscine-n-butylbromide slowly intravenously. Group III: Received [20mg] metoclopramide slowly intravenously. Group IV [control]: Received Sterile water for injection [placebo]. RESULTS: There was no statistically significant difference among studied groups as regard to maternal age, BMI, GA, cervical dilatation and cervical effacement at start of study with p value > 0.05. There were highly statistically significant differences among groups as regard to durations of 1st stage of labor, cervical dilatation after start of study and amount of oxytocin augmentation used with p value <0.001. There were moderately significances as regard to neonatal outcome [APGAR score and NICU admission] with p value <0.01 but there was no statistically significant difference among studied groups as regard to, duration of 2nd stage of labor, mode of delivery and birth weight with p value > 0.05. There were mildly statistically significant differences among groups in degree of labor pain and maternal adverse effects of drugs used in this study with p value < 0.05. CONCLUSION: All drugs used in this study had significant effects on shortening of 1st stage of labor with better neonatal outcome but Drotaverine hydrochloride had the upper hand as it was more effective beside it had the strongest labor pain relieve and lesser maternal adverse effects. RECOMMENDATIONS: We recommend using Drotaverine hydrochloride routinely in enhancing first stage of labor as it cheap, effective with mild significant maternal adverse effects. More randomized trials on a larger scale are needed to evaluate the utility and safety of these drugs in labor.
1. Introduction Labor is a natural physiological process characterized by progressive increase in frequency, intensity and duration of uterine contractions, effacement and dilatation of cervix with descent of the fetus through the birth canal [1]. Prolonged labor is one of the most important risk factors for perinatal compromise and, if caused by obstructed labor, it carries the risk of uterine rupture, postpartum hemorrhage [PPH], puerperal sepsis, and maternal death [2]. The two major factors that determine duration of labor are uterine contractility and rate of cervical dilation. In addition to mechanical factors such as sweeping of membranes, cervical stretching [3] and amniotomy [4] various pharmacological agents have been found to facilitate cervical dilation. The role of oxytocin and prostaglandins has been established worldwide in augmentation of labor [5] and the cervical application of hyaluronidase has also been used with some success [6].The cervix is made up of only 10 to 15 percent smooth muscle with the remaining tissue comprised primarily of extracellular connective tissue. Constituents of the latter include type I, III, and IV collagen, glycosaminoglycans, proteoglycans, and elastin [7]. Cervical softening results from increased vascularity, stromal hypertrophy, glandular hypertrophy and hyperplasia, and compositional or structural changes of the extracellular matrix [8]. Drotaverine is highly effective in reducing the duration of active phase of labor by hastening cervical dilatation, more effective when given in more dilated cervix than with less dilatation and more effective in multigravida than in primigravida. There was no interference with uterine contractility and no increase in operative delivery. It reduces the incidence of traumatic postpartum hemorrhage by reducing the incidence of cervical tear. It is a safe drug for the mother as well as for the baby [9]. Only one study was found which looked at hyoscine-n-butylbrmide primarily as an analgesic for the pain associated with labor. The study was shown that intravenous Hyoscine-N-butylbromide smoothens the passage of labor effects by affording pain relive of up to 36% and also shortening the duration of active phase without any fetal or maternal complications [10]. Aim of the Work: This study aimed to find out the effect of Drotaverine, Hyoscine-N-Butylbromide and Metoclopramide on enhancement of first stage of labor.
Gen. Health Med. Sci., Vol(2), No (1), February, 2015. pp. 1-4
TI Journals
General Health and Medical Scienceswww.tijournals.com
ISSN:
2409-9856
Copyright © 2015. All rights reserved for TI Journals.

2. Patients and methods The study was designed as a double-blind, randomized, controlled, clinical trial comparing four groups of women [50 patients for each]; Group I [Received 40mg of Drotaverine hydrochloride slowly intravenously]. Group II [Received 20mg of Hyoscine-n-butylbromide slowly intravenously]. Group III [Received 20mg of Metoclopramide slowly intravenously. Group IV [control]: Enrolment for this study commenced in October 2012 and was completed in July 2013. Women were recruited from the antenatal clinics of our hospitals and full informed consent was obtained in the antenatal clinic during the patients’ routine visits. Adequate Opportunity was provided at that time for the women to voice any questions or concerns regarding the study. Women included in the study were all 20 years or older, were at term, and had no chronic or pregnancy-induced illnesses. No woman had any contraindication to vaginal delivery, and all women were in established, spontaneous labor. Established labor was defined as the presence of regular uterine contractions associated with progressive cervical effacement and dilatation. The syringes containing the drugs and placebo were prepared by the principal investigator, under aseptic conditions and on a rolling basis [i.e. fresh batches were prepared as additional participants were enrolled]. Each syringe contained either 1 ml of, drotaverine hydrochloride [40mg], hyoscine butylbromide [20 mg], metoclopramide [20mg] or 1 ml of normal saline; all liquids are colorless, so the syringes containing the drugs were indistinguishable from those containing placebo. A computer program was used to generate a random sequence of numbers. Sequentially numbered, sterile syringes were then prepared using the random numbers to determine their content: drugs or placebo. Only the principal investigator knew the correlation between the labels of the syringes and their contents, and this was only showed after the study was completed. Participants received drugs as a single dose, given intravenously, when they were assessed as being in labor, with cervical dilatation of 4–5 cm, as confirmed and documented by residents in the Obstetrics and Gynaecology departments. The woman and the caregivers were blinded as to whether the active drug or placebo was being administered. The progress of the participants was closely documented, with the conduct of labor for both the drugs and control groups in accordance with our normal labor ward protocol, which is based on the principle of active management. Thus, routine amniotomy was performed for all women in established labor who were found to have cervical dilatation of 3 cm or more, and who had not had spontaneous rupture of membranes. Oxytocin augmentation was initiated if the initial progress of labor [as assessed through partographs] was unsatisfactory. Intervention through instrumentation or caesarean delivery was dictated by the usual obstetric determinants. Laboring mothers were monitored in bed, and the use of electronic cardiotocography assisted in the monitoring of fetal wellbeing. All data sheets [containing the raw data obtained during the study] were collected by the principal investigator and kept in a combination locked filing drawer in his office. At the end of the study, the data were disaggregated by the principal investigator, using the record of randomization sequences and the label of the syringes to sort the participants and their data into the appropriate groups [drugs or control]. The data were then analyzed using the Statistical Package for the Social Sciences [SPSS].
3. Results Statistical analysis Data were analyzed by computer using SPSS [Statistical Package for Social Science], version 11. The methods used were:
1. Mean x: To measure the average value of a group of data. 2. Standard deviation SD: To measure the degree of dispersion of data around their mean. 3. Students T test: To test the significant difference between two sample means. 4. Chi-square X² test: To test the significant difference between percentage and qualitative data. 5. ANOVA [ANalysis Of VAriance] F test; To compare two means or more than two means. The P value was: Insignificant result was
considered if P > 0.05. – Mild significant result was considered if P ≤ 0.05. – Moderate significant result was considered if p <0.01 - -High significant result was considered if P ≤ 0.001.
There was no statistically significant difference among studied groups as regard to maternal age, BMI, GA, cervical dilatation and cervical effacement at start of study with p value > 0.05 [Table 1]. There were highly statistically significant differences among groups as regard to durations of 1st stage of labor, cervical dilatation after start of study and amount of oxytocin augmentation used with p value <0.001 [Table 2]. There were moderately significances as regard to neonatal outcome [APGAR score and NICU admission] with p value <0.01 [Table 3] but there was no statistically significant difference among studied groups as regard to mode of delivery, duration of 2nd stage of labor and birth weight with p value > 0.05 [Figure 1 and Tables 2&3 respectively]. There were mildly statistically significant differences among groups in degree of labor pain and maternal adverse effects of drugs used in this study with p value < 0.05[Table 2 & Figure 2].
Table 1. Comparison among studied groups in maternal age, BMI, GA cervical dilatation and effacement at start of study
Group I N=50 Group II N=50 Group III N=50 Group IV N=50 P value Maternal Age in Years M±SD 22.3 ± 2.04 22.5 ± 1.91 22.9 ± 2.10 22.3 ± 1.49 0.339 N.S.
BMI in kg/m2 M±SD 24.1± 0.63 24.0± 0.65 24.2± 0.58 24.2± 0.60 0.425 N.S. Gestational Age in Weeks M±SD 39.1± 0.80 39.0 ± 0.77 39.2 ± 0.77 39.4±0.60 0.092 N.S.
Dilatation at time of injection in cm M±SD 4.4± 0.67 4.4± 0.64 4.4± 0.70 4.3± 0.53 0.452 N.S. Cervical effacement at start of study [NO %]
<50% > 50%
24[48] 26[52]
25[50] 25[50]
24[48] 26[52]
25[50] 25[50]
0.155 N.S.
N.S. =Non significant
Table 2. Comparison among studied groups in cervical effacement, durations of laor [1st and 2nd stages] and in oxytocin augmentation
Group I N=45 Group II N=44 Group III N=44 Group IV N=42 P- value Rate of cervical dilatation in cm/h M±SD 1.9± 0.55 1.8± 0.59 1.9± 0.59 0.98± 0.55 0.001*** Duration of 1st stage in hours M±SD 2.1± 0.55 2.3± 0.62 2.1± 0.59 3.1± 0.78 0.001*** Duration of 2nd stage in minutes M±SD 31.0± 7.52 31.4± 7.18 30.7± 7.80 33.9± 7.4 >0.05 N.S. Oxytocin Augmentation in units M±SD 5.2± 0.54 7.3± 0.74 8.2± 0.72 15.7± 0.65 0.001*** Labor pain [NO %]
Moderate Severe
35 [77.8] 10[22.2]
30[68.2] 14[31.8]
21[47.7] 23[52.3]
18 [42.8] 24[57.2]
< 0.05*
N.S. = Non significant - * mildly significant - *** highly significant
2 Mahmoud Edessy, Abd El-Aziz G. EL-Darwish, Ahemed A. M. Nasr *, Abd El-Naser Abd El-Gaber Ali, Hosam El-Katatny , M. Tammam
General Health and Medical Sciences Vol(2), No (1), February, 2015.

Table 3. Neonatal outcome in studied groups
Neonatal Outcome Group IV N=50 Group III N=50 Group II N=50 Group I N=50 P value Birth weight in kg M±SD 2.9± 0.14 3.0± 0.18 3.1± 0.19 3.0± 0.16 >0.05 N.S. APGAR score at one minute M±SD 7.2± 1.08 6.8± 1.04 7.0± 1.00 6.1± 1.10 0.01** APGAR score at five minute M±SD 9.30.69 8.4± 0.70 8.1± 0.73 7.3± 0.83 0.01** NICU admission NO [%] 1[2] 4[8] 2[4] 8[16] 0.01**
N.S. = Non significant - * mild significant - **moderate significant
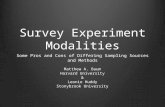
Figure 1. Comparison among studied groups in mode of delivery [p value >0.05]
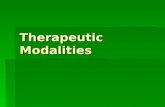
Figure 2. Comparison among studied groups in most common side effects [p value < 0.05].
4. Discussion Programmed labor protocol is based on incorporation of labor analgesia, active management of labor, and monitoring events of labor using a partogram [11]. The process of labor puts great strain on the mother and her fetus. Shortening of labor duration would therefore minimize maternal and fetal morbidity and mortality [12].In this study there was no statistically significant difference among studied groups as regard to maternal age, BMI, GA, cervical dilatation and cervical effacement at start of study with p value > 0.05. Drotaverine hydrochloride is an isoquinolone derivative, which has a powerful spasmolytic action on smooth muscle cells by altering the membrane potential and permeability [13]. In our study Drotaverine hydrochloride showed a significant effect on shortening duration of 1st stage of labor which agreed with many previous studies had shown that it shortens the duration of labor by 54 min [13] and 218 min [14]. Singh et al. [15] also demonstrated a mean reduction of 15% and 19% in the duration of the first and second stages of labor, respectively These results are in sharp contrast to what had been reported by [16] which showed no significant effect of drotaverine hydrochloride on cervical dilation. Other than the study by Singh et al. [15] no other studies have demonstrated the effect of drotaverine hydrochloride in acceleration of the second stage of labor. Hyoscine-N-butylbromide is a muscarinic antagonist that acts as a cervical spasmolytic agent. Our study showed a significant effect of Hyoscine-N-butylbromide on shortening duration of 1st stage of labor which agreed with what had been reported by Sekhavat et al. [17] who showed the mean±SD of first stage duration was [186.8 ± 125.6 minutes] and Baracho and Kamat [18] who stated that the total duration of labor in primigravida and multigravida women was significantly reduced by 2 h and 1 h 37 min, respectively. Similar observations were also noted by Bhattacharya and Joshi [19], who reported a significant reduction in the duration of labor with Buscopan. Sirohiwal et al [20] evaluated the effect of Buscopan suppositories in the active management of labor and found a significant difference in the duration of labor between the control and study groups [368.05 ±133.0 min versus 123.86±68.89 min, respectively], but our results against what had been reported by Al
90% 88% 88%84%
10% 12% 12%16%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
G I G II G III G IV
Normal Delivery
Cesarean Section
2%
6%
2%1%
4%
8%
2% 2%2%
10%
2%1%
4% 4%
6%
4%
0% 0%
5%
0%0%
2%
4%
6%
8%
10%
12%
G I G II G III G IV
dry tongue
tachycardia
flushing
headache
3 Different Modalities in First Stage Enhancement of Labor
General Health and Medical Sciences Vol(2), No (1), February, 2015.

synapses and antagonizing dopamine. The precise mechanism of action of metoclopramide in the first stage of labor is unclear, but it was documented that the mechanism of action of metoclopramide partially increase the catecholamine which are involved in the process of labor, however no evidence base studies proved such action. In our study Metoclopramide had a significant effect on shortening duration of 1st stage of labor and rate of cervical dilatation which agreed with what had reported by Mohamed, [22]. In our study metoclopramide had the least shortening effect in comparison to other drugs used in this study. In this study there was no statistically significant difference among studied groups as regard to rate of cesarean section delivery, duration of 2nd stage of labor and these results agreed with what had reported by Tar et al. [23]. As regard to severity of labor pain, it was lesser in groups I and II [22.2% & 31.8% respectively] than in groups III and IV [52.3% & 57.2% respectively] with p value <0.05 which agreed with that reported by Samuel et al. [10], Sirohiwal et al. [20], Roy et al. [9] and Aggarwal et al. [24]. As regard to adverse effects of drugs used in this study, there was mildly statistically significant difference among groups in adverse effects of drugs used where flushing and tachycardia were more obvious in group II and extra-pyramidal manifestations were only present in group III which agreed with that reported by Davenport et al. [25]. In this study there were moderately significances as regard to neonatal outcome, drotaverine hydrochloride and metoclopramide groups had the best neonatal outcome as regard to high APGAR score and low NICU admission and that agreed with what had reported by Sharma et al. [26] and Tewari et al. [27].
5. Conclusion All drugs used in this study had significant effects on shortening of 1st stage of labor with better neonatal outcome but Drotaverine hydrochloride had the upper hand as it was more effective beside it had the strongest labor pain relieve and lesser maternal adverse effects.
6. Recommendations We recommend using Drotaverine hydrochloride routinely in enhancing first stage of labor as it cheap, effective with mild significant maternal adverse effects. More randomized trials on a larger scale are needed to evaluate the utility and safety of these drugs in labor.
References [1] Archie CL and Biswas MK [2003]: The course and conduct of normal labor and delivery In current Obestetrics and Gynecology diagnosis and treatment.
McGraw Hill Co; 10:213-221. [2] Hofmeyr GJ [2004]: Obstructed labor: using better technologies to reduce mortality. International Journal of Gynecology and Obstetrics;85[Suppl 1]:S62–
S72. [3] Tan pc, Jacob R, Omar SZ [2006]: Membrane sweeping at initiation of formal labor induction: a randomized controlled trial. Obstet and gynecol;107[3]:569–
577. [4] Jenkin G, Young I [2004]: Mechanisms responsible for parturition; the use of experimental models. Anim Reprod Sci;82:567–581. [5] Sharami SH, Milani F, Zahiri Z, Mansour-Ghanaei F [2005]: A randomized trial of prostaglandin E2 gel and extraamniotic saline infusion with high dose
oxytocin for cervical ripening. Med Sci Monit.;11[8]:CR 381–CR 386. [6] Rayburn WF [2002]: Preinduction Cervical Ripening: Basis and Methods of Current Practice. Obstetrical & Gynecological Survey.;57[10]:683–692. [7] Canty EG, Kadler KE [2005]: Procollagen trafficking, processing and fibrillogenesis. Cell Sci 118:1341. [8] Word RA, Landrum CP, Timmons BC, et al [2005]: Transgene insertion on mouse chromosome 6 impairs function of the uterine cervix and causes failure of
parturition. Biol Reprod 73:1046. [9] Roy S, [2007]: Australian Medicines Handbook. Adelaide: Australian Medicines Handbook. ISBN 0-9757919-2-3. [10] Samuels LA, ChristieL and Roberts-Gitten B [2007]: The effect of hyoscine butylbromide on the first stage of labor in term pregnancy. Br J Obstet Gynecol
;114:1542-1546. [11] Meena J, Singhal P, Choudhary D [2006]: The programmed labor. J Obstet Gynecol India;56:53–5. [12] Nicholson JM, Kellar LC, Cronholm PF, Macones GA [2004]: Active anagement of risk in pregnancy at term in an urban population: An association
between a higher induction of labor rate and a lower cesarean delivery rate. American Journal of Obstetrics & Gynecology;191[5]:1516–1528. [13] Bolaji OO, Oneyji CO, Ogundaini AO, Olugbade TA, Ogunbona FA [1996]: Pharmacokinetics and bioavailability of drotaverine in humans. Eur J Drug
Metab Pharmacokinet;21:217–21. [14] Sharma JB, Pundir P, Kumar A, Murthy NS. [2001]: Drotaverine hydrochloride vs alethamate bromide in acceleration of labor. Int J Gynecol Obstet;74:255–
60. [15] Singh KC, Jain P, Goel N, Saxena A [2004]: "Drotaverine hydrochloride for augmentation of labor". International Journal of Gynaecology and Obstetrics 84
[1]: 17–22. [16] Gupta B, Nellore V and Mittal S [2008]: Drotaverine hydrochloride versus hyoscine n butylbromide in augmentation of labor. Int J Gynecol Obestet.
Mar;100[3]:244-247. [17] Sekhavat L, Karbasi SA, and Mirowlia M [2012]: Effect of hyoscine butylbromide first stage of labour in multiparus women Afr Health Sci; 12[4]: 408–411. [18] Baracho HM, Kamat JR [1982]: Buscopan in acceleration of labor. J Obstet Gynecol Ind;34:509–12. [19] Bhattacharya P and Joshi SG [1985]: Acceleration of labor with intramuscular buscopan injection J Obestet Gynecol Ind; 35; 1014-7. [20] Sirohiwal D ,Dahiya K and D.M [2005]: Efficacy of hyoscine n butylbromide [Buscopan] suppositories as a cervical spasmolytics agent in labor. Aus NZ J
obset Gynecol :45:128 - 9. [21] Al Dohami HS, Al Matari FI [2002]: Is Buscopan [hyoscine-N-butylbromide] effective in shortening labor? Presented at: 12th Annual General Meeting of
the Saudi Obstetric and Gynaecological Society; April 17–18. Jeddah, Saudi Arabia. [22] Mohamed Ellaithy [2014]: Use of an Antiemetic to Shorten the Length of Labor in Nulliparous Women. Clinical Trials.gov Identifier NCT01937234. [23] Tar A, Singer J [2002]: "[Safety profile of NO-SPA]". Orvosi Hetilap [in Hungarian] 143 [11]: 559–62. [24] Aggarwal P, Zutshi V and Batra S [2008]: Role of hyosine-n-butylbromide as a labor analgesic. Indian J Med Sci; 62 [5]: 179-184. [25] Davenport K Timoney A and Keeley F [2005]: Conventional and alternative methods for providing in renal colic.BJU Int 95;297-300. [26] Sharma JB, Aruna J, Kumar P, Roy KK, Malhotra N, Kumar S [2009]: "Comparison of efficacy of oral drotaverine plus mefenamic acid with paracervical
block and with intravenous sedation for pain relief during hysteroscopy and endometrial biopsy". Indian Journal of Medical Sciences 63 [6]: 244–52. [27] Tewari k , Jabeen R, Sabzposh MA and Rabbani TThomson AJ, Lunan CB, Cameron AD, et al[2003]: Nitric oxide donors induce ripening of the human
uterine cervix: a randomized controlled trial. Br J Obstet Gynecol 104:1054.
4 Mahmoud Edessy, Abd El-Aziz G. EL-Darwish, Ahemed A. M. Nasr *, Abd El-Naser Abd El-Gaber Ali, Hosam El-Katatny , M. Tammam
General Health and Medical Sciences Vol(2), No (1), February, 2015.