Superficial Thermal Modalities
12
C h a p t e r 1 6 Superficial heat and cold have been used for centuries to manage soft tissue and joint injuries with specific goals of relieving pain, altering the physiologic processes underlying tissue healing, and affecting the plasticity of connective tissue, including muscle, tendon, ligament, and joint capsule. Superficial heat and cold may be delivered through hot or cold packs, hot or cold whirlpools, luminous or nonluminous infrared, ice massage, contrast baths, or cryokinetics. This chapter will focus on the physical principles governing the absorption of heat, the physiologic effects, and the clinical application of heat and cold. The primary goal of any thermal modality is to facilitate the ultimate therapeutic healing modality of exercise. Electrophysical agents may be used for cryotherapy (the application of cold, using cold packs, ice massage, cold whirlpool, vapor coolant sprays, or cold compression units) or thermotherapy (the application of heat using moist heat or hydrocollator packs, paraffin baths, warm whirlpool, or infrared lamps). Cryotherapy is most effectively used immedi- ately following trauma (accidental or inten- tional, as in surgical procedures) to provide analgesia, reduce inflammation and its seque- lae, control bleeding, and reduce muscle spasm. Cryokinetics combines cryotherapy with motion (passive, active-assisted, or active) to facilitate normal, pain-free movement, and to reduce edema through muscle pump action to return lymphatic fluid to the vascular sys- tem. The primary benefit of cryokinetics is to facilitate the patient’s ability to perform pain- free exercise early in the rehabilitation process as long as the level of exercise remains below levels that cause further injury. As signs of acute inflammation begin to subside, the clini- cian may elect to transition to the use of heat. Contrast baths—alternating hot and cold baths—are most appropriate during the early subacute phase of tissue healing or in cases of chronic edema. Superficial heat is best applied before per- forming flexibility exercises to take advantage of the benefits of tissue temperature eleva- tion, including vasodilation that increases tis- sue oxygenation and transport of metabolites to exercising tissue, increased rate of enzy- matic and biochemical reactions that may facilitate tissue healing, and altered viscoelas- tic properties leading to increased soft tissue extensibility, decreased joint stiffness, and increased range of motion. However, heat applied too early in the healing process may result in increased acute inflammation and possibly increase enzymatic activity detrimental to cartilage (e.g., collagenase and protease). The Physics of Thermotherapy Thermotherapy applications fall in the infrared portion of the electromagnetic spec- trum just beyond the wavelength and fre- quency ranges for visible light. 1 The shorter the wavelength, the greater the frequency and depth of penetration. The thermal electro- physical modalities discussed in this chapter fall within the category of “near infrared” and possess shorter wavelengths than electrical stimulating currents. Therefore infrared elec- trophysical agents penetrate to a shallower depth compared to electrical stimulating cur- rents. The biologic effects of electromagnetic radiation depend on the frequency used, 277 Kristinn Heinrichs Superficial Thermal Modalities Ch16.qxd 29/12/03 4:54 pm Page 277
Transcript of Superficial Thermal Modalities

C h a p t e r 1 6
Superficial heat and cold have been used forcenturies to manage soft tissue and jointinjuries with specific goals of relieving pain,altering the physiologic processes underlyingtissue healing, and affecting the plasticity ofconnective tissue, including muscle, tendon,ligament, and joint capsule. Superficial heatand cold may be delivered through hot or coldpacks, hot or cold whirlpools, luminous ornonluminous infrared, ice massage, contrastbaths, or cryokinetics. This chapter will focuson the physical principles governing theabsorption of heat, the physiologic effects, andthe clinical application of heat and cold. Theprimary goal of any thermal modality is tofacilitate the ultimate therapeutic healingmodality of exercise.
Electrophysical agents may be used forcryotherapy (the application of cold, usingcold packs, ice massage, cold whirlpool, vaporcoolant sprays, or cold compression units) orthermotherapy (the application of heat usingmoist heat or hydrocollator packs, paraffinbaths, warm whirlpool, or infrared lamps).Cryotherapy is most effectively used immedi-ately following trauma (accidental or inten-tional, as in surgical procedures) to provideanalgesia, reduce inflammation and its seque-lae, control bleeding, and reduce musclespasm.
Cryokinetics combines cryotherapy withmotion (passive, active-assisted, or active) tofacilitate normal, pain-free movement, and toreduce edema through muscle pump actionto return lymphatic fluid to the vascular sys-tem. The primary benefit of cryokinetics is tofacilitate the patient’s ability to perform pain-free exercise early in the rehabilitation processas long as the level of exercise remains belowlevels that cause further injury. As signs of
acute inflammation begin to subside, the clini-cian may elect to transition to the use of heat.Contrast baths—alternating hot and coldbaths—are most appropriate during the earlysubacute phase of tissue healing or in cases ofchronic edema.
Superficial heat is best applied before per-forming flexibility exercises to take advantageof the benefits of tissue temperature eleva-tion, including vasodilation that increases tis-sue oxygenation and transport of metabolitesto exercising tissue, increased rate of enzy-matic and biochemical reactions that mayfacilitate tissue healing, and altered viscoelas-tic properties leading to increased soft tissueextensibility, decreased joint stiffness, andincreased range of motion. However, heatapplied too early in the healing processmay result in increased acute inflammationand possibly increase enzymatic activitydetrimental to cartilage (e.g., collagenase andprotease).
The Physics of Thermotherapy
Thermotherapy applications fall in theinfrared portion of the electromagnetic spec-trum just beyond the wavelength and fre-quency ranges for visible light.1 The shorterthe wavelength, the greater the frequency anddepth of penetration. The thermal electro-physical modalities discussed in this chapterfall within the category of “near infrared” andpossess shorter wavelengths than electricalstimulating currents. Therefore infrared elec-trophysical agents penetrate to a shallowerdepth compared to electrical stimulating cur-rents. The biologic effects of electromagneticradiation depend on the frequency used,
277
Kristinn Heinrichs
Superficial Thermal Modalities
Ch16.qxd 29/12/03 4:54 pm Page 277

278 THERAPEUTIC MODALITIES
duration of exposure, tissue characteristics,and power density.1
Electromagnetic energy and its transmis-sion through the body are governed by severalphysical laws. The first law is the Arndt-Schultz Principle2: Tissue must absorb theenergy produced by the thermal agent to stim-ulate the tissue’s normal function. If theenergy absorbed is insufficient to stimulatethe tissue, there is no effect. If too muchenergy is absorbed, tissue damage may occur.The second law, related to the first, is the Lawof Grotthus-Draper, which determines the fateof the energy. If a tissue does not absorb theenergy, it is transmitted to deeper tissue lay-ers. If the energy is absorbed more superfi-cially, less energy will be transmitted todeeper layers and less penetration of theenergy occurs. When electromagnetic energyencounters the body’s tissues, it has threepossible fates: it may be reflected (e.g., re-flected from the skin’s surface), it may berefracted (e.g., at the interface between thedermis and subcutaneous fat), or it maybe absorbed (e.g., by muscle). The estimateddepth of penetration for most infrared thermalmodalities (cold or hot packs, whirlpools,paraffin baths, luminous infrared devices) isapproximately 1 cm.
The application of superficial thermalmodalities is governed by the physical laws ofheat transfer, primarily conduction and radia-
tion. Most thermal techniques transfer energyby conduction. Energy travels down a ther-mal gradient, with energy (heat) beingremoved from tissue, rather than cold beingadded. During cryotherapy, heat from bodytissues is transferred to the cold modality viaconduction provided there is direct contactbetween the two bodies. Heat always travelsfrom the warmer object to the cooler.3
According to Knight,4 the rate at which heattransfer occurs depends on the followingfactors:■ The temperature difference between the body and
the modality: The greater the difference, themore quickly the transfer of heat occurs.
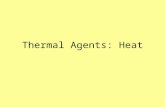
■ Regeneration of body heat and modality cooling:As the body tissue gives up heat, the heatlost is replaced by circulating blood and sur-rounding tissues. Cold penetrates moredeeply than superficial heating modalities.For example, after a 20-minute ice packapplication to the gastrocnemius muscle,the intramuscular temperature declinedmore slowly than the subcutaneous temper-ature (and never reached as cold a tempera-ture as the subcutaneous tissue) (Figure16-1). When the ice pack was removed, thesubcutaneous tissue temperature rosesteeply, whereas the intramuscular temper-ature continued to decline for a period oftime until both tissues were within 2˚ to 3˚ Cof each other.5
35
30
20
Tem
pera
ture
( 8 C
)
10
002
Time (min)
Subcutaneoustemperature
Intramuscular temperature(2.3 cm deep)
604022
Ice packs
Figure 16-1 Intramuscular versus subcutaneous tissue temperature changes with cryotherapy. Intramuscular (gastrocnemius) andsubcutaneous temperatures during and after a 20-min ice pack application. Note that intramuscular temperature declined muchmore slowly than subcutaneous temperature and continued to decrease after the ice pack was removed. (Redrawn from HartviksenK: Ice therapy in spasticity, Acta Neurol Scand 38(suppl 3):79-84, 1962.)
Ch16.qxd 29/12/03 4:54 pm Page 278

■ The heat storage capacity of the cold modality:The more energy it takes to convert a solidto a liquid (e.g., ice to water), the greater itslatent heat of fusion and its capacity toremove heat from a tissue. For example,crushed ice packs require more energy forthis conversion to occur as compared tosemisolid gel packs. Therefore ice packscool tissues for a longer time and to agreater extent than gel packs.
■ The size of the modality: The larger the modal-ity (e.g., cold pack), the greater the energystorage capacity.
■ The area of the body in contact with the modal-ity: For example, cold-water immersionresults in the greatest temperature declinecompared to other methods of cold deliverybecause a greater surface area is in contactwith the cooling modality.6 Ethyl chloridevapocoolant sprays result in the least tem-perature decline and provide only superfi-cial cooling because of the relatively smallsurface area cooled.
■ The application duration: The longer the con-tact time between the two surfaces, the moreopportunity for energy exchange to occurand heat to be removed from the body.
■ Individual variability: Individuals with lowerbody fat percentage exchange heat morequickly than those with greater amounts ofsubcutaneous fat.
Regardless of the cold pack type (ice versuscommercially available cold packs), the surfacetemperature drops immediately after applica-tion of the cold pack and reaches its maximumeffect in approximately 30 minutes in humans.Following removal, the surface temperaturerises rapidly, although it may not reach preap-plication levels for more than 60 minutes afterremoval from the skin.4 Rewarming in animalsfollows a similar pattern, and it may take sev-eral hours after removal of the cold pack forcomplete rewarming to occur. A 30-minutecold gel pack application to the stifle joint of 10healthy bulls decreased the intraarticular tem-perature 6.6˚ ± 1.0˚ C for 215 minutes.7 Studiesin dogs have reported similar decreases inintraarticular temperature.6,8
Physiologic Effects of Cryotherapy
Cryotherapy is used during the acute phase oftissue injury and healing to mitigate the effectsand sequelae of tissue injury, and after
exercise during rehabilitation to minimizeadverse secondary inflammatory responses.The primary physiologic effects of cryother-apy include vasoconstriction, reduced bloodflow, reduced cellular metabolism and perme-ability, decreased sensory and motor nerveconduction velocity, analgesia, prevention orreduction of trauma-induced edema, decrea-sed muscle spasm, and temporary reductionof spasticity before exercise.9,10
During the inflammatory phase of tissuehealing, increased permeability of the micro-vasculature occurs as a result of histamine andbradykinin release. In addition, these chemicalmediators cause vasodilation and increasedblood flow to the area. These events, coupledwith hypoxic cellular changes, are primaryfactors in the formation of edema. (Centrallymediated sympathetic vasoconstriction helpsto reduce edema as a result of decreasedhydrostatic pressure.) The primary role ofcryotherapy during the inflammatory phaseis to reduce the metabolic rate of the injuredtissue, which in turn results in decreasedmetabolite production and metabolic heat.11
In addition, the decreased metabolic rate lim-its further injury and aids the tissue in surviv-ing the cellular hypoxia that occurs afterinjury.4
The Hunting reaction, first described byLewis in 1930, refers to the cyclical tempera-ture oscillation of 2˚ to 6˚ C every 8 to 15 min-utes after the tissue temperature approaches2˚ C. This effect begins 20 to 40 minutes aftercryotherapy application. He attributed theseoscillations to cold-induced vasodilation(CIVD) as an attempt to protect tissues fromcold-induced damage. However, his resultshave been incorrectly and widely applied tothe sports medicine literature in an attempt toexplain the success of cryokinetics.2 Knight etal12 replicated Lewis’ experiment and con-cluded that Lewis’ observation during coldimmersion and subsequent rapid increase intemperature after cryotherapy are due to tem-perature effects, not CIVD and subsequentincreased blood flow. Based on these studies,the primary benefits of cryotherapy aretwofold: decrease in cellular metabolism andanalgesic effects to permit cryoexercise tofacilitate rehabilitation.4,12
The response to cryotherapy treatment isalso mediated by the nervous system. Pe-ripheral thermal receptors are categorized ascutaneous myelinated type III or A delta,which are sensitive to pricking or sharp pain
Chapter 16 SUPERFICIAL THERMAL MODALITIES 279
Ch16.qxd 29/12/03 4:54 pm Page 279

and cold, unmyelinated type IV or C receptorsfor aching pain, and unmyelinated type IV orC cutaneous receptors for pain and tempera-ture (Table 16-1).
The unmyelinated cutaneous receptorsrespond to absolute temperature and the rateof temperature change.13 The cold-sensitivereceptors begin firing at 36˚ C and increasetheir firing rate until reaching their maximumat approximately 25˚ C. The firing frequencydrops sharply at temperatures below 20˚ Cand is minimal by the time the receptors arecooled to 10˚ to 12˚ C. Conversely, the warmreceptors also begin firing at 33˚ to 36˚ C, rap-idly reach their maximum firing frequencyat 43˚ C, and drop to a minimal firing rate at45˚ C.14 Both the hot and cold receptors rap-idly adapt to temperature changes.
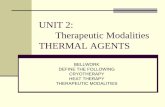
Central thermosensitive neurons in the pre-optic and anterior hypothalamus respondto temperature changes with autonomic re-sponses to stimulate heat retention by thebody by altering cutaneous blood flow andthermoregulatory behavior such as panting.Figure 16-2 illustrates this central hypothala-mic control of thermoregulation. The anterior
hypothalamus also controls thermoinsensitiveneurons, such as those that are sensitive toosmolarity and glucose concentration.15,16
Stimulating the posterior hypothalamus byheating does not result in the autonomicresponses characteristic of the anterior hypo-thalamus, but behavioral responses to the heatload occur. Local warming of the medullaincreases respiratory frequency. Autonomicthermoregulatory responses also take place atthe spinal cord level.16 The sympathetic ner-vous system response to thermal load is alsochemically mediated through the release ofthe neurotransmitters epinephrine and norep-inephrine from the adrenal medulla to inducecutaneous vasoconstriction.15
A primary effect of cryotherapy is analgesiaand the concomitant reduction of reflex mus-cle spasm. This may be due to the decreasednerve conduction velocity that occurs whennerves are cooled. This relationship, knownas the Q10 effect, is thought to be linear until10˚ C, when neural transmission is blocked.17,18
Nerve cooling also increases the duration ofthe refractory period, the time when a nervecannot be stimulated by a second impulse.19
280 THERAPEUTIC MODALITIES
Table 16-1 Sensory Receptors: Anatomy, Location, and FunctionSensory ConductionNerve Diameter Velocity Sensory
Receptor Type Classification Location (mm) (m/sec) Function
Sensory A Ia Muscle 12-20 72-120 Muscle spindle (afferent) primary myelinated ending (or 1-
degree ending)A Ib Tendon 12-20 72-120 Golgi tendon
organRate of muscle
shorteningA II Muscle 6-12 36-72 Muscle spindle,
secondary ending (or 2-degree ending)muscle length changes
A II Skin 6-12 36-72 Vibration, discriminatorytouch, pacinian corpuscles
A III Skin 1-6 6-36 Pricking, sharp pain, temperature (cold), light touch
Unmyelinated C IV Muscle ~1 0.5-2.0 Aching painC IV Skin ~1 0.5-2.0 Pain, temperature
From Guyton AC: Sensory receptors and their basic mechanisms of action. In Textbook of medical physiology, Philadelphia, 1986, WBSaunders, p 578.
Ch16.qxd 29/12/03 4:54 pm Page 280

Conversely, raising the subcutaneous tissuetemperature increases sensory nerve conduc-tion velocity, with the greatest effect occurringduring the initial 2˚ C temperature elevation.20
Another mechanism postulated for the anal-gesic effect afforded by cryotherapy is that thecold receptors are overstimulated by cryother-apy, resulting in pain control at the spinal levelby preventing pain transmission to highercenters via the spinal gate control theory ofpain transmission.
Cryotherapy may also decrease musclespasm through a number of proposed mecha-nisms. Decreasing pain may decrease muscleguarding or spasm associated with an injury.The muscle spindle receptors and Golgi ten-don organ receptors fire more slowly whencooled, although the effect is less pronouncedon the Golgi tendon organs.21 Sudden coolinghas an excitatory effect on the muscle spindle,resulting in increased alpha motoneuron activ-ity and increased muscle guarding. As the tem-perature continues to decrease, primaryspindle afferent activity diminishes.17 Musclespasm, resulting from the pain–spasm–paincycle, stimulates the static stretch response ofthe type II tissue afferents. Applying superfi-cial heat until the temperature is above 42˚ Cdecreases the muscle spindle discharge ratewhile it increases the firing rate of the Golgitendon organ.21 This sequence of events resultsin a decrease in the firing rate of the alphamotor neuron. Thus cold may raise the thresh-
old stimulus for muscle spindle activity,decreasing muscle spasm.22
Thermal effects on strength and endurancehave also been observed by a number ofauthors. The force-velocity curve of musclecontraction shifts downward with decreasingtemperature.23 For a given concentric contrac-tion velocity, cooler muscles have a lowerforce output. Interestingly, proprioception,joint position, and balance remain largelyunaffected by cryotherapy.24-26 Although mostauthors agree that changes in muscle torqueproduction occur with cooling, it is less clearwhether those effects are specific to a particu-lar contraction mode (concentric accelerationor eccentric deceleration). One group ofresearchers reported that eccentric muscleaction is augmented following cryotherapy,27
while another group found increases in con-centric, but not eccentric, torque.28 Still othersfound no effects on peak torque, but increasedmuscle endurance following cooling.29 Func-tionally, vertical jump performance, an indica-tor of lower-extremity explosive power, isadversely affected by cryotherapy.30,31 Thesefindings suggest that caution must be used inmaking recommendations for performancefollowing cryotherapy. Clearly the literatureon this subject is undecided as to the specificeffects of cold (both immediate and delayed)on muscle strength. These findings have themost implication for dogs who are engaged inwork or competitive athletic pursuits. It also
Chapter 16 SUPERFICIAL THERMAL MODALITIES 281
PeripheralWARM
receptors
PeripheralCOLD
receptors
b
c
a
F
TW
Pant,Sweat
Behavior,Skin BloodFlow
Shivering,Non-shiverThermo-genesis
Heatproduction
+
++++
+–
+ +
+
F
TW C
F
TW
+
F
T
37
Heatretention
37
Heatloss
37
Figure 16-2 Central hypothalamic control of thermoregulation. Diagram shows neuronal control of various thermoregulatoryresponses. +, Excitatory input; −, inhibitory control; dashed line, thermoneutral temperature; C, cold-sensitive neuron; F, neuronalfiring rate; T, hypothalamic temperature; W, warm-sensitive neuron. (Redrawn from Boulant JA, Dean JB: Temperature receptors inthe central nervous system, Ann Rev Physiol 48:639-654, 1986.)
Ch16.qxd 29/12/03 4:54 pm Page 281

requires that the clinician understand the phys-iology and biomechanics of muscle actions andsport demands. Cold and exercise are an effec-tive combination in the treatment of acutemusculoskeletal dysfunction unless restric-tions in flexibility are present.32,33 Combiningmovement with cold allows for relativelygreater pain-free exercise and assists in themuscle pump activity to reduce acute injury-related edema.
Cryotherapy Applications
A variety of methods are available for apply-ing cryotherapy to dogs. Selection of themethod depends on the desired effects and isinfluenced by the stage of tissue repair, physi-ologic goals (analgesia, edema reduction, lym-phatic pumping, and so forth), depth ofpenetration desired, treatment area, and activ-ity or exercise goals. Cryotherapy is particu-larly helpful in the management of acuteinflammation (bursitis, tenosynovitis, tendini-tis, and so forth) where application of heatcauses additional pain and edema. Cryo-therapy methods include ice packs (home-made, commercial cryogel packs, elasticwraps), cryomassage, ice bath immersion,contrast baths, and vapor coolant (ethyl chlo-ride) spray (Figure 16-3). To prevent frostbiteor cold-induced injuries, it is critical toobserve the skin for response to cold. Near theend of a 20-minute treatment, the skin maynormally be erythematous, but pale or whiteskin is an indication that cold-induced tissuedamage may be occurring. The range ofexpected sensations during cryotherapyinclude an initial sensation of cold, followedby burn, sting, and ache, and finally a numbsensation.12 For most injuries, applicationtimes of 20 to 30 minutes may not be sufficientto cool the injured tissues; the notion of “max-imum benefit in 20 minutes” has not been sub-stantiated with research.4 Because animalpatients cannot describe these sensations,careful observation of the animal’s behavioralresponses and skin condition every few min-utes during the treatment session is critical.
Ice packsSeveral methods may be used to apply super-ficial cold (see Figure 16-3). The simplestmethod of ice application is to wrap a freezerbag containing crushed ice in a thin dampcloth (such as a pillowcase) and apply directly
over the affected area. Before sealing the bag,remove the excess air. The addition of a com-pression wrap to secure the bag to the bodyalso insulates the body surface against air,resulting in additional reduction of surfacetemperature during cooling and slowerrewarming following removal of the ice.34 Ifcrushed ice is not available, cold packs may beprepared by mixing 3 parts water to 1 partrubbing alcohol, double bagging with sealedbags, and placing in a freezer. The resultingslush may then be molded around irregularbody parts. If the mixture freezes in a house-hold freezer, more alcohol can be added to themix. If it is too liquid, more water can beadded. To prevent skin damage, apply a towelor cloth to prevent direct contact of the icepack with the animal’s skin. Apply thecryotherapy treatment for 15 to 25 minutes ata time, inspecting the tissue for its responseafter the first 5 to 10 minutes. Monitor closelyfor signs of frostbite.
The latent heat of fusion is lower for thealcohol-water mix than for water alone; there-fore it performs similarly to crushed ice alone,but a lower temperature. Use caution with thewater-alcohol mix because the potential forcold-induced injuries is greater. Never applythis mixture directly to the skin; instead applyusing a layer of toweling, either wet or dry
282 THERAPEUTIC MODALITIES
Figure 16-3 Cryotherapy options (clockwise starting topright): Popsicle-type molds for ice massage, alcohol-waterslush plastic bags, cotton wraps, commercial cold wraps,flouromethane cold spray.
Ch16.qxd 29/12/03 4:54 pm Page 282

(wet conducts cold more rapidly). Com-mercial cold packs may also be applied.Packs that freeze solid (e.g., DuraKold) per-form better than frozen gel packs, whichcontain gelatin or antifreeze to make themmore pliable (Figure 16-4).4 Cold packs con-taining ethylene glycol antifreeze should not beused in animals because the contents are toxic ifingested. As with the alcohol-water mixture,use caution because the risk for frostbite isgreater than when using a crushed ice bag(Figure 16-4).
Artificial ice cubes (e.g., Cold Gold), manu-factured by the sheet, may be trimmed to fitthe body part and secured with elastic wrapor used with commercial custom-designedwraps (e.g., CanineIcer, www.canineicer.com)(Figures 16-5 and 16-6). They offer the advan-tage of ice cubes without the mess of meltingice. Used often in postoperative cryotherapyapplications to minimize postoperative edemaand pain, the sheets are somewhat pliable andmay be refrozen.
Cold-Compression UnitsCold compression units, which are commerci-ally available, combine compression withcryotherapy. Cold water circulates in a fabrica-ted sleeve which is snugly applied to providecompression to the area. Combined with ele-vation, this method of treatment is highlyeffective during the acute phase of tissueinflammation and healing.
Cold Immersion and ContrastBathsCold immersion, because it exposes the great-est body surface area to cold, results in thegreatest decreases in tissue temperature. Thebody part is immersed in an ice “slush” bathas part of the immediate first aid followinginjury (Figure 16-7). The analgesia from theimmersion allows the animal to performcryokinetics with relative ease. Contrast baths,in which the affected body part is immersed incold water followed by immersion in hotwater, have long been used as a method toinduce cyclic vasodilation and vasoconstric-tion to facilitate flushing debris and inflam-
Chapter 16 SUPERFICIAL THERMAL MODALITIES 283
35
30
25
Tem
pera
ture
( 8 C
)
20
15
10
5
0–10 0 10 20 30 40 50 60 70 80 90
Time (min)
KeyIce—immediateDuraKold—immediateChattanooga—immediateIce—delayedDuraKold—delayedChattanooga—delayed
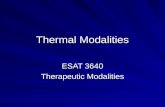
Figure 16-4 The effect of the heat of fusion can be seen in this comparison of several forms of cold packs. The crushed iceand DuraKold packs cool the skin more than the Chattanooga frozen gel pack. The effect is even greater when application isdelayed for 20 min after the packs are removed from their cooling devices. (Knight KL et al: A re-examination of Lewis’ cold-induced vasodilation in the finger and ankle, Athletic Train 15:238-250, 1980.)
Figure 16-5 Canine stifle icer.
Ch16.qxd 29/12/03 4:54 pm Page 283

matory mediators from the injured area.However, some authors do not agree with thisproposed mechanism.4 Clinically, it may beappropriate to use contrast baths during thetransition from acute to subacute injurymanagement. The body part is immersed inalternating cold and hot baths, in a ratio any-where from 4C:1H (4 minutes cold, 1 minutehot) near the end of the acute phase, to 2H:2C(2 minutes hot, 2 minutes cold). This cycle isrepeated three to five times for a total of 15 to30 minutes. If the injury is relatively acute, thefinal cycle should be in the cold bath to helpreduce edema formation. If contrast baths areused before exercise in subacute or chronicconditions, then the final cycle should be inthe hot bath. If used as a transition from theacute to subacute stages of tissue healing, thecold:hot ratio should be weighted moretoward a cold emphasis (e.g., 4C:1H) pro-gressing to 2H:2C and 3H:1C depending on
the clinical evaluation before treatment.Specific ratios of hot to cold depend on theclinical goals of the treatment.
Ice MassageIce massage is a very quick and effectivemethod of applying cryotherapy to theaffected area with the muscle in a position ofgentle stretch (Figure 16-8). Molds to form acylinder of ice with an application stick arecommercially available. Placing tonguedepressors in paper cups filled with water andfreezing them is a low-cost alternative formaking “ice Popsicles” to perform ice mas-sage. Ice massage is applied parallel to themuscle fibers. The pressure from the ice mas-sage stimulates the mechanoreceptors morethan other forms of cryotherapy.4 This tech-nique is particularly useful for small, irregularareas. Treatment time is generally 5 to 10 min-utes or until the affected area is erythematousand numb.
Vapocoolant SpraysVapocoolant sprays have long been used totreat trigger points in humans.35 However,their ability to cool is the least effective of allthe methods and results in cooling only of thesuperficial cutaneous tissue. To use the vapo-coolant spray to treat trigger points, place theaffected muscle in a position of slight stretchand spray from proximal to distal at a rate of10 cm/sec from a distance of 30 cm (12 inches)(Figure 16-9). Repeat four or five times untilthe affected area has been covered. Because ofthe dog’s hair, the effectiveness of this tech-nique is questionable. These sprays can also bepotentially dangerous if they accidentally getin the animal’s eyes or are ingested.
284 THERAPEUTIC MODALITIES
Figure 16-6 Carpal icer.
Figure 16-7 Contrast baths.
Figure 16-8 Ice massage.
Ch16.qxd 29/12/03 4:54 pm Page 284

Indications for CryotherapyCryotherapy is best applied during the acuteinflammatory phase of tissue healing andafter exercise to minimize any inflammatoryresponse. Cryotherapy is effective in reduc-ing pain, particularly acute postoperativepain. In addition, it is effective in reducingedema when combined with compressionand elevation. Cold also decreases the meta-bolic rate of reactions involved in tissueinjury and healing. At joint temperatures of30˚ C (86˚ F) or lower, the activity of cartilage-degrading enzymes, including collagenase,elastase, hyaluronidase, and protease, isinhibited.36 If cryotherapy is applied duringthe subacute or proliferative phase of tissuehealing, recovery may be impaired. Whenthere are minimal signs of inflammation andthe patient tolerates simple range-of-motionand flexibility exercises without an increasein swelling or pain, the treatment mayprogress to heat.
Treatment Duration and FrequencyThe duration and frequency of cryotherapydepend on the severity of the injury, the areaof injury, and the desired outcome. Treatmenttimes may be cycled to 30 to 45 minutes on,followed by an equal amount of time off.Practically, cryotherapy is typically adminis-tered three to six times daily. It should be con-tinued until the healing tissue moves into theproliferative (subacute) phase of healing.Cryotherapy should be applied to support thegoal of pain-free exercise and may also beapplied following an exercise session to mini-mize reactive swelling and pain.
Precautions and ContraindicationsAlthough the application of superficial coldand ice is relatively safe, there are conditions inwhich the use of cryotherapy is contraindi-cated. The clinician is cautioned to observe forsigns of frostbite during and after cryotherapyapplication. If the individual has a history offrostbite to the area, further cold application iscontraindicated. Cryotherapy should not beused in individuals who are cold-sensitive ordemonstrate a response, such as cold urticaria,to the application of cold. Cold urticaria causeswheals and swelling on skin (due to a releaseof histamine) when the animal is exposed to areduction in temperature. In dogs with coldsensitivites, care should be taken not to exposelarge areas of the skin to the cold and shouldnot swim in cold temperatures.
Caution should be exercised when apply-ing cryotherapy around superficial peripheralnerves because cases of cold-induced nervepalsy of the ulnar and superficial peronealnerves have been reported in people. Knightestimates the incidence of cold-induced neu-ropathies to be less than 0.0011%.4 Coldshould also not be used in patients with gen-eralized or localized vascular compromise orwho possess an impaired thermoregulatorycapacity. Use caution in applying cold overopen wounds, areas of poor sensation, or invery young or old dogs.
Physiologic Effects of Heat
Heat is used in rehabilitation for its hemo-dynamic, neuromuscular, metabolic, andconnective-tissue effects. Heat is most appro-priately applied after the acute inflammatoryphase of tissue healing has resolved.Premature application of heat may exacerbateswelling, pain, heat, and functional loss. If indoubt, apply cold or contrast baths until thedog is well into the subacute, or proliferative,stage of tissue healing.
Superficial heating agents such as hot packsor hot baths have the greatest effect on cuta-neous blood vessels, resulting in the greatesttemperature change within the first 1 cm oftissue depth. Increased superficial tissue tem-perature results in the release of chemicalmediators, such as histamine and prosta-glandins, which result in vasodilation. Thesecond mechanism for vasodilation occurswith the stimulation of cutaneous thermore-ceptors that synapse on the cutaneous blood
Chapter 16 SUPERFICIAL THERMAL MODALITIES 285
Figure 16-9 Flourimethane vapocoolant spray.
Ch16.qxd 29/12/03 4:54 pm Page 285

vessels, causing the release of bradykinin torelax the smooth muscle walls, resulting invasodilation. A third mechanism for vasodila-tion involves the reduction in sympatheticactivation via spinal dorsal root ganglia toreduce smooth muscle contraction, resultingin vasodilation at the application site and indi-rectly to the cutaneous blood vessels of theextremities.36 These vasodilatory mechanismsdo not significantly affect blood flow in skele-tal muscle since skeletal muscle blood flow isheavily influenced by other physiologic andmetabolic factors. Exercise is the best means toincrease blood flow to skeletal muscle.37
The neuromuscular effects of heat, in con-trast to those of cold, include increased nerveconduction velocity and decreased latency timefor both sensory and motor nerves. Nerve con-duction velocity increases 2 m/sec for every 1˚C (1.8˚ F) increase in temperature.36 Musclerelaxation occurs as a result of a decreased fir-ing rate of type II muscle spindle afferents andgamma efferents, and an increased firing rate oftype II fibers of the Golgi tendon organs (seeTable 16-1). These, in turn, contribute to adecrease in firing of the alpha motoneuron tothe extrafusal muscle fiber, resulting in musclerelaxation. Heat lowers the stimulus thresholdfor muscle spindle activity.22
The pain threshold may be elevated withlocalized heat application. Stimulation of thecutaneous thermal receptors has been pro-posed to inhibit the transmission of pain at thedorsal horn of the spinal cord via the gatecontrol mechanism. Second, vasodilatationincreases the blood flow to reduce ischemia ofinjured tissue, resulting in decreased activityof the pain receptors. Decreased muscle spasmfurther relieves pressure of the muscles onblood vessels, reducing ischemia and promot-ing blood flow.
Heat accelerates biochemical reactions,both enzymatic and metabolic, up to a tem-perature of 45˚ C (113˚ F); increases above thisresult in decreased activity of these reactions.From 39˚ to 43˚ C (102˚ to 109˚ F), enzymaticactivity increases 13% for every 1˚ C increasein temperature or doubles for every 10˚ Cincrease in temperature.38 Although heatincreases oxygen uptake and accelerates tissuehealing, it also increases the activity ofdestructive enzymes, such as collagenase, andincreases the catabolic rate. The oxygen-hemo-globin dissociation curve shifts to the right,making more oxygen available for tissuerepair or exercise. Combined with theincreased biochemical reaction rate, superfi-
cial heat may accelerate tissue healing if thetissue injury is superficial. For thermal effectsin deeper tissues, ultrasound or diathermy aremost appropriate. The patient’s status and tol-erance to treatment should be evaluated dailyto determine the most appropriate treatment.
Heat causes increased connective tissueextensibility if the tendon, ligament, scar tis-sue, or joint capsule tissues are superficiallylocated. Deeper musculotendinous or jointcapsule structures should be heated usingultrasound or diathermy, which are capable ofelevating tissue temperature at greater depths.For the maximum connective tissue plasticdeformation to occur, the tissue temperaturemust be maintained at 40˚ to 45˚ C (104˚ to113˚ F) for a minimum of 5 to 10 minutes whileapplying the stretch.36 In cases where the vis-coelastic properties of connective tissue are tobe altered, the tissue must be subjected to ade-quate concurrent heat and stretch for a suffi-ciently long period of time to result inpermanent tissue elongation.39 Lower loadsapplied over a longer period of time duringtissue heating and recooling result in less sec-ondary tissue trauma.40 Superficial heat maybe successfully applied to reduce joint stiff-ness and increase the elasticity of superficialjoint capsular structures to facilitate exercise.
Heat Application
Superficial thermal therapy may be appliedusing commercially available packs contain-ing cornhusks, gel material that can be usedfor either hot or cold application, or packscontaining iron filings (activation of suchpacks produces heat for several hours follow-ing a chemical reaction resulting in oxidation)(Figures 16-10, 16-11, and 16-12). Commer-cially available wraps may also be used forheat application by placing heat packs insidethe wraps.
Treatment Duration and FrequencyThe duration and frequency of thermal treat-ment depends on the severity of the injury, thestage of tissue healing, the area of the injuredpart, and the desired outcome. Treatmenttimes may be cycled at 30 to 45 minutes on,followed by an equal amount of time off.Thermal modalities should be applied to sup-port the goal of pain-free exercise, the ultimatetherapeutic modality, to obtain the best resultsin the shortest period of time.
286 THERAPEUTIC MODALITIES
Ch16.qxd 29/12/03 4:54 pm Page 286

Contraindications and Precautionsfor Superficial Heat ApplicationsSuperficial heat is contraindicated duringacute inflammation because it may exacerbatethe inflammatory process, over an area ofsubcutaneous or cutaneous hemorrhage orthrombophlebitis, or over malignant tissue.Superficial heat should be used with cautionin patients with poor thermoregulatory capac-ity, edema, impaired circulation, or over openwounds. Dogs should be monitored closelybecause they cannot verbalize their intoler-ance. A tissue burn may result if the patient isnot able to dissipate the heat load via vasodi-lation or if too much heat (too hot or too long)is applied. Burns can be avoided by usingmaterials that cool as the treatment pro-gresses, by increasing the insulation layerbetween the patient and the hot pack, or bylimiting the initial temperature increase.Monitor the skin condition before, during, andafter treatment for any adverse effects.
Conclusion
Thermal heat therapy and cryotherapy arepowerful adjuncts in the rehabilitation of mus-culoskeletal injuries in dogs. Successful man-agement depends on an accurate assessmentof the dog’s presenting problems at the begin-ning of each treatment session. Cryotherapyand cryokinetics are most useful during theacute inflammatory stages of tissue healing.As tissue healing is established, with rela-tively weak hydrogen bonds it is susceptibleto injury from exercise that is too aggressive orfrom changing from cold to heat too early,thus exacerbating the inflammatory response.After new tissue has been established and thetensile strength of the tissue continues toincrease as the bonds strengthen into covalentbonds, the emphasis shifts to promoting amobile scar, normal range of motion, and nor-mal flexibility. In patients with limitations inthese areas, concurrent application of superfi-cial heat and flexibility exercises results inbeneficial plastic changes to the tissue thatmay be relatively permanent. Superficial coldand heat modalities may be a very usefuladjunct in a rehabilitation program to facilitatenature’s ultimate therapeutic modality: con-trolled exercise. Selection of the appropriatemodality depends largely on an understand-ing and accurate assessment of the stage(acute inflammatory, proliferative, or tissue
Chapter 16 SUPERFICIAL THERMAL MODALITIES 287
Figure 16-10 Superficial hot pack application with com-mercially available hot pack with straps.
Figure 16-11 Shoulder heat pack with custom wrap(Courtesy CanineIcer, Charlottesville, VA, SofTouch hot/coldpack, PI Medical, Athens, TN).
Figure 16-12 Canine shoulder heat application (www.canineicer.com).
Ch16.qxd 29/12/03 4:54 pm Page 287

remodeling) of tissue healing, an accurate clin-ical assessment of the dog’s functional abili-ties, establishing appropriate treatment goals,and continued reevaluation when the patientstatus changes as tissue healing progresses.Any therapeutic modality (heat, cold, ultra-sound, laser, etc.) should be used to facilitatethe ability of the dog to participate withMother Nature’s ultimate therapeutic modal-ity: exercise, first controlled, then free.
REFERENCES
1. Ritter HTM: Instrumentation considerations. InMichlovitz SL, editor: Thermal agents in rehabilitation,Philadelphia, 1996, FA Davis, pp 62-63.
2. Prentice WE: The science of therapeutic modalities. InPrentice WE, editor: Therapeutic modalities in sportsmedicine, New York, 1999, McGraw-Hill.
3. Palmer J. E, Knight KL: Ankle and thigh skin surfacetemperature changes with repeated ice pack applica-tion, J Athletic Train 31:319-323, 1996.
4. Knight KL: Temperature changes resulting from coldapplication. In Cryotherapy in sport injury management,Champaign, Ill, 1995, Human Kinetics Publishers.
5. Hartviksen K: Ice therapy in spasticity, Acta NeurolScand 38(suppl 3):79-84, 1962.
6. Bocobo C et al: The effect of ice on intra-articular tem-perature in the knee of the dog, Am J Phys Med Rehab70:181-185, 1991.
7. Kern H et al: Kryotherapie: das veralten derGelenktemperatur unter Eisapplikation: Grundlagefür die praktische Anwendung, Wien Klin Wochenschr22:832-837, 1984.
8. Cobbold AF, Lewis OJ: Blood flow to the knee joint ofthe dog: effect of heating, cooling, and adrenaline, JPhysiol 121:46-54, 1956.
9. McMaster W: A literary review on ice therapy ininjuries, Am J Sports Med 5:124-126, 1977.
10. Olson J, Stravino V: A review of cryotherapy, PhysTher 62:840-853, 1972.
11. Ho SSW et al: The effect of ice on blood flow and bonemetabolism in knees, Am J Sports Med 22:537-540, 1994.
12. Knight KL et al: A re-examination of Lewis’ cold-induced vasodilation in the finger and ankle, AthleticTrain 15:238-250, 1980.
13. Yarnitsky D, Ochoa JL: Warm and cold specificsomatosensory systems: psychophysical thresholds,reaction times, and peripheral conduction velocities,Brain 114:1819-1826, 1991.
14. Iggo A: Cutaneous thermoreceptors in primates andsub-primates, J Physiol 151:332-341, 1969.
15. Guyton AC: Sensory receptors and their basic mecha-nisms of action. In Guyton AC, editor: Textbook of med-ical physiology, Philadelphia, 1986, WB Saunders, p 578.
16. Boulant JA, Dean JB: Temperature receptors in thecentral nervous system, Ann Rev Physiol 48:639-654,1986.
17. Lippold O, Nicholls J, Redfearn J: A study of the affer-ent discharge produced by cooling a mammalianmuscle spindle, J Physiol 153:218-231, 1960.
18. Lowitzsch K, Hopf HC, Galland J: Changes of sensoryconduction velocity and refractory periods withdecreasing tissue temperature in man, J Neurol216:218-231, 1977.
19. Evans T, Ingersoll C, Knight K: Agility following theapplication of cold therapy, J Athletic Train 30:231-234,1995.
20. Lowdon B, Moore R: Determinants and nature ofintramuscular temperature changes during cold ther-apy, Am J Phys Med 54:223-233, 1975.
21. Currier DP, Kramer JF: Sensory nerve conduction:heating effects of ultrasound and infrared, PhysiotherCanada 34:241, 1982.
22. Mense S: Effects of temperature on the discharges ofmuscle spindles and tendon organs, Pflügers Arch374:159-166, 1978.
23. Ratanunga KW: Influence of temperature on thevelocity of shortening and rate of tension develop-ment in mammalian skeletal muscle, J Physiol 316:35-36, 1981.
24. LaRiviere J, Osternig L: The effect of ice immersion onjoint position sense, J Sports Rehab 3:58-67, 1994.
25. Pincivero D, Gieck J, Saliba E: Rehabilitation of a lat-eral ankle sprain with cryokinetic and functional pro-gressive exercise, J Sports Rehab 2:200-207, 1993.
26. Thieme H, Ingersoll C, Knight K: Cooling does notaffect knee proprioception, J Athletic Train 31:8-11,1996.
27. Catlaw K, Arnold B, Perrin D: Effect of cold treatmenton concentric and eccentric force-velocity relationshipof the quadriceps femoris, Isokinetics Evere Sci 5:157-160, 1996.
28. Ruiz D, Myrer J, Durrant E: Cryotherapy and sequen-tial exercise bouts following cryotherapy on concen-tric and eccentric strength in the quadriceps, J AthleticTrain 28:320-323, 1993.
29. Kimura I, Gulick D, Thompson G: The effect ofcryotherapy on eccentric plantar flexion peak torqueand endurance, J Athletic Train 32:124-126, 1997.
30. Gallant S, Knight K, Ingersoll C: Cryotherapy effectson leg press and vertical jump force production,J Athletic Train 31:S18, 1996.
31. Grecier M, Kendrick Z, Kimura I: Immediate anddelayed effects of cryotherapy on functional powerand agility, J Athletic Train 31:S32, 1996.
32. Dufresne T, Jarzabaski K, Simmons D: Comparison ofsuperficial and deep heating agents followed by apassive stretch on increasing the flexibility of thehamstring muscle group, Phys Ther 74:70, 1994.
33. Taylor B, Waring C, Brasher T: The effects of thera-peutic application of heat or cold followed by staticstretch on hamstring muscle length, J Orthop SportsPhys Ther 21:283-286, 1995.
34. Merrick MA et al: The effects of ice and compressionwraps on intramuscular temperatures at variousdepths, J Athletic Train 28:236-245, 1993.
35. Travell JG, Simons DG: Myofascial pain and dysfunction:the trigger point manual, vols I and II, Baltimore, 1992,Williams & Wilkins.
36. Cameron MH: Physical agents in rehabilitation: fromresearch to practice, Philadelphia, 1999, WB Saunders.
37. McArdle WD, Katch FI, Katch VL: Exercise physiology:energy, nutrition, and human performance, ed 5,Baltimore, 2001, Lippincott Williams and Wilkins.
38. Hocutt JE et al: Cryotherapy in ankle sprains, Am JSports Med 10:316-319, 1992.
39. Lehmann JF: Effect of therapeutic temperatures ontendon extensibility, Arch Phys Med Rehab 51:481-487,1970.
40. Sapega AA: Biophysical factors in range of motionexercises, Phys Sports Med 9:57, 1981.
288 THERAPEUTIC MODALITIES
Ch16.qxd 29/12/03 4:54 pm Page 288