Diagnosis andTreatment ofStreptococcal Pharyngitis
8
Diagnosis and Treatment of Streptococcal Pharyngitis BETH A.(HOBY, MD, Unn'c..-sity oflennessee College ofMediww-Chnttanooga, Clw_ttalwagl1,Thmcssee Common signs and symptoms of streptococcnl pharyngitis include sore throat, temperature greater than lOOAoF (38°C), tonsillar exudates, and cerviull aclcnopaUl}'. Cough, coryza, and diarrhea are more common with viral phar- yngitis. Available diagno.'itic tests inc:1udethroat cultllf<'. Jnd rapid antigen detection testing. ThroaL cullure is coll:;iu- ercd the diagnostic standard, although the sensirivity oJ. nd specificity of rapidantigen detection testing have improwd ~jgJllfi(.:anlly. Themodified Centol' SCQ1'eC~n be llsed to help physici<H1S decide which 1-1J.Li~Jlts m:cd no lesLing, Lhroal cllltllre/nlpid ~ntjgell detection testing, or empiric antibiotic therapy, Penicillin (10 days of 01"3 1therapy or Olle injec- tion of intramuscular benwthine penicillin) is thetreatmcnt of choice becauseof cost, narrow spectrum of activity, and effecliveness. Amoxicillin is eqn~lly effec6ve and more palatable. Erythromycin anJ Jlr~l-generationcephalospo- rins are options in patients with penicillin allergy. IncrcascJ groupA beta-hemolytic streptocoCCllS (GABHS) treatment failure with peni- cillin has been reported. Although current guidelines recommend first-gencratiuIl ccphalosporins for persons with penicillin allergy, some advocate the use of cephalosporins in "li! nonallergic patients bCUlm<: of b<:tter GABHS eradication and effectivencs~ against chronicGABBS caniage. Chronic GABHS colonization is common despite appropriate use of antibiotic therapy.Chronic carriers arc at low risk of lr;J:llsmiLLingdiseaseordeveloping invasive GABHS in[{Tliolls, and there is generally noneed to treat carrier:;. 'Whether tonsillectomy oradenoidectomy dec(cu:;cs the incidence of GABBS pharyngitis i~ poorlyunderstood. At this time, the benefits arc too small to oUlwclgh the associJted costsand surgical fish. (A.m Pam Physldun. 2009;?9(5):585-390. Copyright ~~; 2009 American Acad- emy of Family Physicians.) ~ P,ltient information: Ahalldou! on strep thmai:, mitten by theauthor of this arlick isJvailable ~t hnp:!l'Nww.a.lfp. o rg!afpI200~03 0 11383·sl P h<.i.r)'Ilgilis is diagnosed inll mil- ,.' lion patients in U.S. emergency departments and ~Jlllbul"'tory set- lin;!s MIDllJlly_' .~.j05t ellisodcs arc ~ . e viral. Gnmp Abeta-hemolytic; str"eptococcus (GABHS), themost common bactcrial etiol- 01:\).', account~ for 15 to 30 pew:llt of cases of acute pharyngitis in children and.5 to 20 per- ccn Lin adults. 2 Among school-aged children, the inddellc(::b ofacute sorethroat, ~wab- positive GABHS, Llm.l serologic)ll), C011 nrmeJ GABHSinfcchon arc 33, 13, and fight per lOU child-years, respectively.3 Thus, aOOllt one in fOlll-rlllkll"1:,n with lKLlte S01"e throat has serologically couflflmu G-A8HS phar- yngitis. Fonr-ihn~e peT('('nt of filmilieswith :lTl lnclex C8se of CABHS pharyngiti5 have n secondary case,3 Late wlllter imrl early spring ar~ pe,!\z GAI)HS sensons. Tht mfection is lrallSmilled via reSplratory secretiQ!l$, alJd the incubation period is 24 to 72 hours. Diagnosisof 5tr~ptoco((al Pharyngitis CLINICAL DIAGNOSIS Becausethe signs and symptoms of GABHS pharyngiti5 overlap extensively 'Nith other infectious causes, IIlLlking a diagnosis ba"fO solely on clinical findings is difficult_ In patit:nts 'Nith de ule 1\;brileres FiIatory illness, ph\'sicians <lcCLHJtely difierenti<lk Gact,~rial from viral infections using only tlie Imlory ,Ind physical hndillO:;C, abouL one half of the ti me.'l No slllglc dement ot"the patient's his- tory or phYSIcal exammation reliably con- films or txdudes GARHS rhnryngitis_" Sore III rua(, kver "~lith sudd-en onsd (ll;!l!lpt'fClill rf grtater tiulllOO.1°F [_'lSOC]), rmd exposme to ,SLnpuxoccus ,v-ithinthe preceding 1 IVO 11Clwnlo~d"d('Ullr lire rmC'rlr~n FQmirj rhy"cl~n Web sit" at \'.",Wi a~h'"'Qidv, Cwyri)h( I) 2ml'1 Amerrcan ACdUeJllY of Fo;J1il~ ;'Ily,i(iam, Fo: lh~ rfi,'or~_ nnn:O"''''.;c;ol w,e <.if ~"u InOI'IICunl mer ot tll~ Wei) ,;\e. All oll,~, 'i~I!~, r~i~fYGO,CUIl;;]C[ mrynGr,tS(';>il~tp,org For C'J"'}.,-iQill '1uu\lio,,~ J1d-'r.r r"rrr.il1I'~r. r~qu"s:s.
Transcript of Diagnosis andTreatment ofStreptococcal Pharyngitis
Diagnosis and Treatmentof Streptococcal PharyngitisBETH A. (HOBY, MD, Unn'c..-sityoflennessee College ofMediww-Chnttanooga, Clw_ttalwagl1, Thmcssee
Common signs and symptoms of streptococcnl pharyngitis include sore throat, temperature greater than lOOAoF(38°C), tonsillar exudates, and cerviull aclcnopaUl}'. Cough, coryza, and diarrhea are more common with viral phar-yngitis. Available diagno.'itic tests inc:1udethroat cultllf<'. Jnd rapid antigen detection testing. ThroaL cullure is coll:;iu-ercd the diagnostic standard, although the sensirivity oJ. nd specificity of rapid antigen detection testing have improwd~jgJllfi(.:anlly. The modified Centol' SCQ1'eC~n be llsed to help physici<H1S decide which 1-1J.Li~Jltsm:cd no lesLing, Lhroalcllltllre/nlpid ~ntjgell detection testing, or empiric antibiotic therapy, Penicillin (10 days of 01"31therapy or Olle injec-tion of intramuscular benwthine penicillin) is the treatmcnt of choice because of cost, narrow spectrum of activity,and effecliveness. Amoxicillin is eqn~lly effec6ve and more palatable. Erythromycin anJ Jlr~l-generation cephalospo-rins are options in patients with penicillin allergy. IncrcascJ group Abeta-hemolytic streptocoCCllS (GABHS) treatment failure with peni-cillin has been reported. Although current guidelines recommendfirst-gencratiuIl ccphalosporins for persons with penicillin allergy,some advocate the use of cephalosporins in "li! nonallergic patientsbCUlm<: of b<:tter GABHS eradication and effectivencs~ againstchronic GABBS caniage. Chronic GABHS colonization is commondespite appropriate use of antibiotic therapy. Chronic carriers arcat low risk of lr;J:llsmiLLingdisease or developing invasive GABHSin[{Tliolls, and there is generally no need to treat carrier:;. 'Whethertonsillectomy or adenoidectomy dec(cu:;cs the incidence of GABBSpharyngitis i~poorly understood. At this time, the benefits arc toosmall to oUlwclgh the associJted costs and surgical fish. (A.m PamPhysldun. 2009;?9(5):585-390. Copyright ~~;2009 American Acad-emy of Family Physicians.)
~ P,ltient information:A halldou! on strep thmai:,mitten by the author ofthis arlick is Jvailable~thnp:!l'Nww.a.lfp.o rg!afpI200~03 011383·sl
Ph<.i.r)'Ilgilis is diagnosed inll mil-,.' lion patients in U.S. emergency
departments and ~Jlllbul"'tory set-lin;!s MIDllJlly_' .~.j05t ellisodcs arc~ . e
viral. Gnmp A beta-hemolytic; str"eptococcus(GABHS), the most common bactcrial etiol-01:\).',account~ for 15 to 30 pew:llt of cases ofacute pharyngitis in children and.5 to 20 per-ccn Lin adults.2 Among school-aged children,the inddellc(::b of acute sore throat, ~wab-positive GABHS, Llm.lserologic)ll), C011 nrmeJGABHS infcchon arc 33, 13, and fight perlOU child-years, respectively.3 Thus, aOOlltone in fOlll- rlllkll"1:,n with lKLlte S01"ethroathas serologically couflflmu G-A8HS phar-yngitis. Fonr-ihn~e peT('('nt of filmilies with:lTl lnclex C8se of CABHS pharyngiti5 have nsecondary case,3 Late wlllter imrl early springar~ pe,!\z GAI)HS sensons. Tht mfection
is lrallSmilled via reSplratory secretiQ!l$, alJdthe incubation period is 24 to 72 hours.
Diagnosis of 5tr~ptoco((al PharyngitisCLINICAL DIAGNOSIS
Because the signs and symptoms of GABHSpharyngiti5 overlap extensively 'Nith otherinfectious causes, IIlLlking a diagnosis ba"fOsolely on clinical findings is difficult_ Inpatit:nts 'Nith de ule 1\;brile res FiIatory illness,ph\'sicians <lcCLHJtely difierenti<lk Gact,~rialfrom viral infections using only tlie Imlory,Ind physical hndillO:;C, abouL one half of theti me.'l No slllglc dement ot"the patient's his-tory or phYSIcal exammation reliably con-films or txdudes GARHS rhnryngitis_" SoreIII rua(, kver "~lithsudd-en onsd (ll;!l!lpt'fClill rf
grtater tiulllOO.1°F [_'lSOC]), rmd exposmeto ,SLnpuxoccus ,v-ithin the preceding 1IVO
11Clwnlo~d"d('Ullr lire rmC'rlr~n FQmirj rhy"cl~n Web sit" at \'.",Wi a~h'"'Qidv,Cwyri)h( I) 2ml'1 Amerrcan ACdUeJllY of Fo;J1il~;'Ily,i(iam, Fo: lh~ rfi,'or~_ nnn:O"''''.;c;olw,e <.if ~"u InOI'IICunlmer ot tll~ Wei) ,;\e. All oll,~, 'i~I!~, r~i~fYGO,CUIl;;]C[mrynGr,tS(';>il~tp,org ForC'J"'}.,-iQill'1uu\lio,,~ J1d-'r.r r"rrr.il1I'~r. r~qu"s:s.
Streptococcal Pharyngitis
Ciill/cal recomme".dJ;:;on
A 5-8, 13,37,38
el'ic!cncefating References
U5~ur clinical ucr.:isi811rull" for diagnosing GABHSpharyngitis irnpr;)ves quality nf care INhile reducingunwarranted trEatm~nt al1d 0'/2011co;t,
Peni~illinis the tr~atmeM of chOICe for GAllH5 pharyngitiS in persons who ale noL all~r9ic 10 renicillin
Tre0tmelli is 110t,yplcally indi[~led ill ,:hronic CJITil'1I01 phdyll~eJI G!'lBHS
GABH'>"group A be'G-hemolytic 5fr~ptococCll.1_
A = consistl2"!.. 0'()(,(i-'1u",",'ly p~licn!<'ri(,.'l:0d evidence: () = iilconsisrenr 0.' ,"imit·c!-qu2lit'l (lillic,'rrl-on'er;+ed ~v.'o'ence: C" consensL's, disease-Iyiempa"vic.lence, usuai pr;JClice, exµer~ (J~";'Ji(JlI, u«(,15e s2ries, For information ah.,,,t the SONT e\'I'cienre rJlin,:SyS:'e"', go fa hrrp:li',".-W'N.e:aip.orgiafpson.xmi_
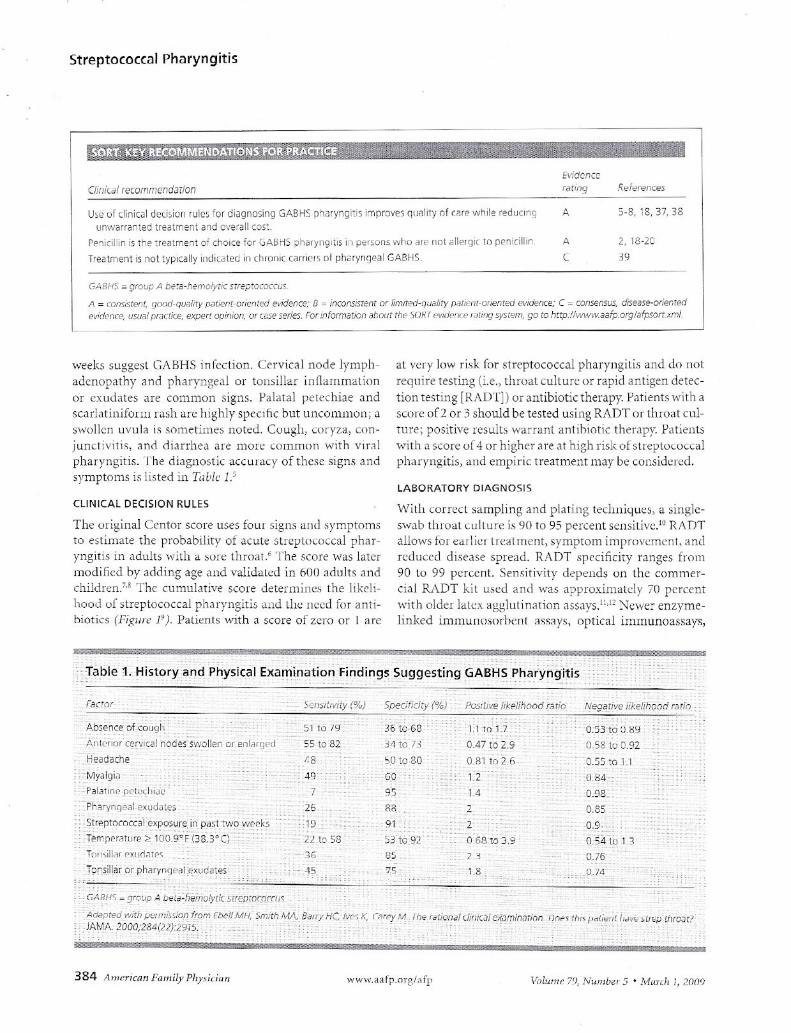
weeks sLlggesLC;,I\SHS lnrection. C:ervic~1 node lymph-adenopathy ~nd phiHyngeaJ or tomillar lflfhlIlllllallOnor eXLldakS are common signs. P,datal pekchlae :mdSC<lrblinifonn ElSh <In: hlg,h II' spcClflC but U1JCOl1HHOn; a
swolkn uvu 13 is sometimt"s nOlted. Cuugh, coryza, con-junctivitIs, 8nd diJrrhe,l He more common \,vith vlr~lpharyngitis. The c1ingnostic ,l(CL-lrac), ofthcsc ,<;igns;]l1dsymptoms is listed in TIlL'ic 1:'
CLINICAL DECISION RULES
The original Centor score uses fOllJ'signs and symptomsto eSlimate the probability of acule slreplococcal phar-yngitis in adult, wilh a son;; Iluo:;!." The score was litternl()(iiiicu oy Mk1ing age and valid~L!;J in 6011:1dults :ll1dchildn:n.7•s The cuml1Lnive score determillt:~ the likeli-hood u[streptococcal ph"l'yngitis o!1d lll'.: llecd for anti-biotics (F,;gilIC J")_ Patients INith J score ot"zero or I al'C
Facto!"
A
C2, 1i3-20
3'i
at very low risk rOT ~lreptococCJ.l pharyngltis and do nol,regui re testing (Le., tlnoJ.t culLufe or rapid antigen detee-tion testing [I~I\DT]l or ~llltibiotic therapy. I-'ntients with aSC(JI"C~01'2 or:~ should be tested using RADT ol-l11ro<l1 CLd-ture; positive results warranl antibiotic therapy. PJliellb'''ith a score of4 or higher 3rt' 3t high risk (.t streptococcalpkH),ngitis, <llid emplrlC treatment may be considered.
LABORATORY DIAGNOSIS
\Nith correcL ,arnpling Jnd plJtlng tE'chniqw;:;, a slllgle-swab throaL cullure is 90 to 95 percent sensitive.I'J R/\ rnallows h:!I-earl it: I' Irt:;:-llillent,symptom improvern<:n I, amIreduu:d d15eJse spread_ RADT ~pecificity ranges from90 to 99 percent. Sensitivity depends on the COlllmer-(i,-d RADT kit used and was ilPproximuLd!' 70 percentwith older lakx ogghllin.1tion assays.ll,l" Nc\l'c enzyme-hnked immunmorhenl .1SS.lYS, optical immunoassays,
Sp':cificiry (%) Pos,'liv~iikplihood CMio Nf3gativ('? Iike/ihoJ,j mrio
o s:ftcijS90.5" Iv 0.92
--'')'b:;ence of ('Sugii
_AnLc"or cc-,YlCdln des. swollEn Q! erii~rged-Headache
:;,,:r1y~l\)i:1:"J'alatillc pdi:d'iJ<':
-Pharyn<]ea l_exudJ te~
',,5!repl:XClCcaleXpD\Ure in Pilst t,'.'ow('cbTemp"rature i-i(jo,9~~'n8_3'C) ,Tonsillar exudJrl'o;Jpr,silliir ol_phil'-YIl<]",'I.'!K,ldaie~'
51 1679
-55 to 52'
liS
7
n.to 58
36
36;t~'6S3~ 1073
50t030150;
OAi
0.81 to 2.6 0_55 lG 1
1.2
14
'(U;4
0_9D._
0.85
91
53k92'
8S
2
o 68_to'J's
J. 3
0.9-
Sfrepmcoccm
"Adapred ,·,irh P~!Il.''':,si(;,,! ~:om F.bellJvIN, Smith"Jt,MA iCOQ;2?,<J{J.J.):Z915,

Treatment of GABHS PharyngitisJUSTIFICATION rOR TREATMENT
GAEHS pharyngitis is self lillukd andf(:~olvts withill a ft>w days, even withouttre;HTIlellt_" Argumenls for antibiotic treal-ment Include nCHle symplom relief-, prevell-lwu of suppur"tive cmd llUUsupPLlrativecomplICations, ~llld leducI'd cummunicabil-ity (['llil" 2). 1,1~-1! AnLihiutics shorten symp-tom chlrulion by ahom 16 hours, the numoerTlt'"t'"ded to treal (NNT) for symptom n:lid at72 hOlll-S is fOlll !lllhus!: with po,:;itivethronl
s',vabs.1? In JUdlllllll, fClle,; of suppurative peritonsill",and rdrophafyngenl ahscc55cs flrc redu..:;cd IdptJl I1.\ilIl:lteJy one in 1,000 cases).l"l
Antibiotics also reduce the IIlcidcncc of acute r11eI1-matie fever (rehtive risk reductiun - O.28).~'1 AlthoughdH:!UmJlic heilr1 disc(lSC is a major pulillL iJt!(IlLhL;:,uc in 1011'- and midJle-income cfHlnrrir; (annual
Clinical DeCISion Rule lor Managementof Sore Throat
PaLient witli 'UI ~ lIliUdlApplystreQlococ,al'(Q,e
,c-,
(ritNi~ Points
Absen,~ of cough
Swollen and te[ld~, ,lHl~riOire'·"io.,,1 nodes
T~,1l~€ratur~;' 100A"F (38°C)
Tonsillar ~:<ud"tes or 5we lir,~
/',ge
"' to 14 yE~"15 to 44 ye2rs
,1S y~J"and old~r
Cumubl;ve swrc:
I r l- I"(Ore f. 0 Score ~ 1 Score = 2 Seok = 3
I I j IRisk of Risk oi Ri,k of r,;sk :Jf(;ABHS GABHS GA~HS GA3HSph~r}'''0Ili'' ph~, Y"9'tis pharyngili, phJ'Y">J,I,c.I lu 25% 5lJiU"'" II i<l 17% 28 to J:;%
IScore 2 4
jRiSk ofGABflSjJioclfyngitis51 to S}%y
N'J furtherlc,ti"9 or~Iltlb,u!<~,i,,\lic;11"("]
I:.....u~,."'...rP~rform throal cultu.e or RAC-T
Comldc, empirictrpatment 'NitI',all\lbioIIC,
I lPO';i;ive
INegallv,?
Ir-Jodntibiotic5 indi,:~'~d Tr~at '."ItilJntit:,iotic,
Figure 1. Modified Centm scor~ <:lfldmanagement options using clini-cal decisiDn flile. Other factors should lw CUflsiucrr:,d (e.g.. a score of 1,but recent family contact 'Nith documented streptococcal infection).(GABHS = group A beta-hemolytic streptococcus; RADT" rapid anti-gen detection testing.)
Ad~p!~d Will;;Jc·,m,~~ionilum Mc1S02( '1/J. Vihit2 D, Taw,enb;;um D. Low DE.A clinical ,(oreto redlle>2 unnecessary an/ibio(.', ll:~ in patients with ';me U"oat (MAJ. 1998;158(1):19
and CI,el[1 illlJllinescmt DNA probes J.n: '-;II)to 99 percentsellsrilve.!l.l' Hm'I'evel, newer le'il~ lWIV lw mnrr cxpen-sive, (lnd not alllt-sb ail:: 1Y1l1Ye(1 hy the Clinical LabDrd-lory lmprovement Acl \)1' 19:-:S
VV"hether negalive kADT rf'~l1lrs in childlen and aclo-lr.;ccnts requJre c011JHm:J.lory throat (nltn,.!" is contro-WTSJaI. T!Jt: Amerieiln i\ci1dcmy of' Pediatncs (AAP)
M.1rrh J, 20(.1:> • \ltll!lr,'I~ 79, ,",'Hl11ncr S II' \\'w.nnfr.org/~fp
Strepto[Q((ul Pharyngitis
reCUJlllllt:ndB that n~gJlive Ri\ DT l"e:.uhe,Ul (hildrtn be <.onJ-iuneu usmg Lhru:ll cul-tUT(' Ilnk'i,~ phy.'i'-I~ll$ can gllarantee thatkADT seJl,;lliv ily i~ ~imilar to rll::n of throat'Cl1lture in their practi(e.'~ blse-negativeRADT I-e&ults may le<lrJ 10 ITllsdiagnosls
and GABBS spread :)Ild, vt"'r-y r;[rely, 10increased suppurative and nODSuppurativecomplicJtions Other sludJes suggest thatthe Sen$ilivity of newcr optical1ll1munoas-says ,lpproachcs that of single-plate throatcullure, obv Elling the need for back-up cul-hne."';; IJt IIldllY clinical practicc:s, contir--malo IT Ihl'oClI culturi.:' is not pcrl'ormed 111chlldren :it low risk for GABHS infectiun.The pn:clpllom drop In rhi'uTIlJtic fever inthe United SUJ\es, si!',nificant costs of add i-tional le~ling <lnJ follow-up, and concernsaboLlllllappropriate autibioric USE' Jre v.llidLeasons why back-up cultures are not IOU-
tinely performed.I'Strcpt()cncc;ll .l'ltibody titers ow: nuL U3C-
hll tell diagnosing streptococcal plurYl1-gilis and arc not routinely Iecollllllcnd..:J.They may be indic~Terl tel confirm previousInfection in persons wil'h suspec·ted <lcut..:poslsLrcptococcal glomerulonephritis orrheumaric fi'vi'r They ITldy a],o hi.!lp dlstin-glli.sh .lCllt:e iJlrCcllOn from chroni,: ,:,llliel
sblus, :lIt\tuugh they arc not routinely I-ec-On11l1rnded for this purpose.
Am~,.irr'"Family PI'ysici",~ 385

inciJcn.:;c of five per IUU,UUUpersons), it has largely beencOl1trolled in industrialized nations since the 19505.2j Iti5 estimated that 3,000 In 4,000 p:llif:JlIS TTIII~1be given:.tntibiotics to prevent one case of acute rheumatic feverin developed nations.'" Rates of acme rheUillatic fevercmd n>tIopharyugca! abKc~~ hav!,; not mCTcascd fol·lowing more judicious antibiotic l-rsein children withrespir~tory infecliom:" Children with Cl\BHS phar·yngitis may return to school after 24 hours of all tibiatictherapy_"
Non-gnJup t\ h,-:I:~-hfmolytic streptococ(:i (groups Calld G) ;1150 GlI1 CJUSt JClltt phar-yngitis; these sLrains,11"1" lIsu~llI!,tYeakd with antibiotics, althollgh good clini-cal trials are lacking. FusolmCerwfn IIcaophoTlim causesendemic acute pharyngitic;, peritonsilb t- c,bsce'ss, ,mdpersistent sOl'e LhrD,tL.UnLreated Fusobw:;tenuli1 infec-tions rnay leaD to Lem ierre sYJlllrDme, ,Ill inlernali llgularvein thrombm caused by inttamm~tion Complicationsoccur whi'n septic plaqUE'S br('"k 100~(; ;"ml i::lTlhnhze.Empi.ric antibiotic therapy mll)' rednce the L;;cidence ofwmplications.
ANTIBIOTIC SELECTION
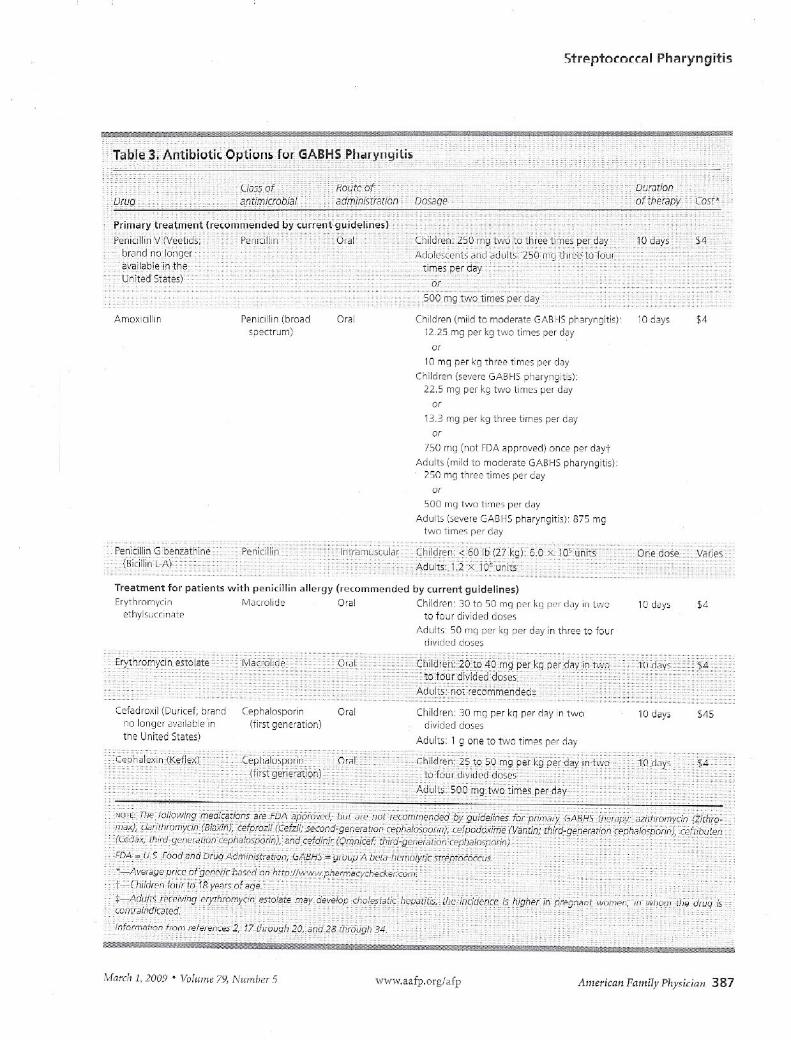
Efftctiven(:ss, spectrum of activity, safeLy, do~in~ sched-ule, cost, alld cOIIlpliance i~sm:s ;111require considcr-ation. Penicillin, penicillin cOllg(;;m;rs (ampicillin ora1l1micillinJ, dimbm)'o:.:in (Ckocin), and certain .:epha-losporim Jnd lll.lLrolicles ~ue effective agalOst GABi-IS.Bas;:d on COSt, narrow speclTllm of 8ctivity. s8fety, andr.::flicctlVcness,penicillil) is recommended by the Arneri-can Academy of family Physicians (AAFp),18 the AAP,dthe American Heart Association,'" the Infectious Dis-eases Society of Am~nca (lDSf\),' and ,he vl/orld HealthOrganizatinl1 for the tr('~tment of streptococcal phM-YllSiLi~Y Options for penicillin dosinR an:: liskd 1;1Table 3.""·1'!,lk'i \Vhen p8Ticnts 81'(' unlikely to completetll~ entire ClItJJ'~t' of antibiotics, a single Lntramuscu-LJr (!()SC of penicillin G bell<.<.tLhine (Riel! liT)L-A) is 8 noption. A preiIllxed renicillin G bCT1zathineiprocaine
386 Amcriwfl Pal1li/y P/'y,jcinl!
llII~clioH (Hicillill C-R) lesM:llb lIIJediull-:nwnaled dib-comfort_ Over the past 50 years, n() incrca~c in minimaliIlhibilurl' concentration OT re5Lstance to GABHS ha~ueen JUl,;ulllenLeu Curpl'Oi;.:illim or cephalobporins.;'
Oral amoxicillin suspension is often substituted forpelllcillin l)(:'calJScit tastes better. The illcdi(~ation isalso available as chewable tablets. live of eight trials(1966 to 2000) shmvcd gTe~ltf.rth~11~'iperctllt (~ABHSendic.ltion with the use of i\luoxi;::il1ill.19Ten days ofthef8py is sl,lIldard; common dosages are provided inTable 3.),l7-2~).8-J.!Amoxicillin taken once per day is likelyas effective as a regimen of three times per day. Gne ran-domized controlled trial (ReT) JemOllstrated uHnpa-rable symptom reJiefwith ollce-daily dosing, althOllghlike almost all studies of pharyngitis lH:alrnenL, the trialwas llot poweH:d Lo detect nonsuppurarive complic3-tions.)Q A recent stud\, of children three to l8 years of~ge shm\'ed that once-d_lily dosing of alUoxicillin 'VOl,uotinferior to twice-d~ily dosing; both regimens had failurerates of llho1112.0percent. 11 It should be noted that Ollce-daily ther,)py i~IJOL approved by the U.S. Food Jnd DrugAoministrJtion (FDA).
CUi'leuL U.S. treatment snide1ines recomn1,"noerythromycin for p8tients with pelllcilllJl <!lL:r.>;)f.G<l~-trointestin,)l side cffeds of (;rythromyon emse manyphysicians to insteM] prescllbc the FDA-apprOlreJsecond-gem:rlltion macrolidE'S nithromycin (Zith-romJ-x) and cbrithromycin (Biaxm). Azithromycinreaches higher cOlll.enrr,1I:iQJ)s in ph'Ir-Yll)!,caJ Li~~u(;and rt:4uires only fiw days of tre,lImenl Miluolideresist;lnce is J!Krt'd$in:s umong CAB}.!::! isohte5 in theUnited SLaLe:"likely b"_(\'l.\1seof .uithromycin ovo:nr,c.'"RepurLeu (:ARHS resistanc¢ iD certain areas nf L"lH'United Stales and Canada ~ppmJc,hes 8 to 9 percent JJ
MosL guiddincs l'ccommend reserving t:ryllEolll,'Cinfor patients who are allergic Lopemcillin.
Firsl-gcnerMion or:,] ceph,dosp',Jrill~ <In: n::(;Uill-mended for t'.rlil'IlLs with pemcillm allergy who donot hal/I; lIumcdiate-type hypersen~itivity to bela-L1Ct,1lD cmtibioLlcs. BacknologlC f~ihHe rate,; torpenicillin-tl'edll:'cl GABBS pharyngitis increased fromabout' 10 percent III the J970s to more than 30 percentin the past decaJe,'~ Several studies suggest that cepha-losporins are more efff'ctiw against GABHS than peni-cillin. Hlgh12r rate~ of GADHS eradicltion Clnd shortercou r~;ef;of ther-upr Lhat arc possible with ceplla 1.x;purillsIIFty lll' lleneficial. One meta-anJly~I., nl'j5 11-1<1]s COUl-
varin:; V~~fI{)lhc_ephnlosporins against penicillin noted,~lgllilintn lI)imore bacterioloslC and din 1[<11[<1res in thecephalosponn group (NNT = 13) ,; However, the poorquaLity of mclllded stndie.'l limited these fiJlJi11t:~, clUJ
viww,uafp.org/afp V",umr 79, NW'1htr S * ,vIr",,;!, J, 1009
Strpptorcrral PhAryngitis
urugi)!Jr.niOI)8fthfiijbii
""T.~'~1¢~,:Ah_ijpi9tI~_optl~:h~f4.i~K~~~-:PJ,-,~rYI_1~ iri'~~_n •••• _ ....... _ ... __ - "'".,',., " __ "",,":," ..... __ .... _
-Prim<lry t~,~:::,:.:,,:t{'''m''::":;~,~~by-P-e!;iLlli'l',"
brancil1oJDi~gc_ri;'vailab!e:i!i the:-Ur.it~d Slates}
--time, per
PFnlcillill (broad"pectrurn)
Or~1
500 mg t.wo .limes ~e:- day-
Childr"r, (mild to) madera;:e GI~BHSphoryngiti,}12_25 m9 per kg twe limes :J2r clc/
f<l
10 mg per kg 1hre2 times per d"yCnildren (severe GJl.BHS ?:laryngiti;;)'
22.5 m9 pCI' kg two li",~,; P"" dJy
"13,3 ITig per kg th,-ee times per G~y
"750 'ng (n(]l FDA "ppro~ed) once per d~ytAduilS (mild tll fnoder-ate GA[iHS pharYrJgitis)_
250 mg three limps per dey
"soa mg two li(,-,ro<,PC" dcly
Adults i58',8re CADI'IS pharyngiti.\)' 875 ~",gh"iC j"ncs PCI d~y
Penibllin Gbenzat'lir,e"n{Gic'iiiili
:- Pe,nidlir-(::- ::;.ci..x}ii5ij'ililS~--
Treatment fOI" patients with f'f"nicillin allergy (rec",nn",nued by ClIrrent gu idelines)Erythrnmvcin M~crolicl~ O,al Children: 30 til 50 mel p.,,, klJ pel" dely in 1','/0
,'thyhjwn~ie tD f'JUf divided Go,esl\clullS 50 1m]µe, k,l µer day ill three tc bur
di\fldcd duor,:;
1:J deyo
C'o'lcdrD/ii (Duricef; Drar,jn[lloIl9~' a'_'0ikbl~-inthe Unilee Siates)
Cer,halosporin(firs'( genEration)
Children: 30 mg pEr kg per d?y inlwooi'Jid2d doses
eral 10 days
Adults: 1 9 olle -::0t'NO tim'!5 per (let!
-'wi"
h''''roe,o, ''-omw'e'''c', 2 -Americrw Family PI!piril111 387
Streptococcal Pharyngitis
rewlls rn~r ue hkewed ly~o,;dLlbe o.:.ephalvsponns morEeffeclively erJdicJle GABI-IS cMrlage lhan penicilLi.ndoes. Although ccphalosporins arc cf£~ctiv,~, the shiftHnviH!.1('xrrn"iv(', hroild-"pectrum second- and third-generation [ephJ.lo~;porin usc is increasing. \,\-'hether("(:'phalosporins \\/ill replace penioUin 8S primM)'GABHS therapy remains to be seen.
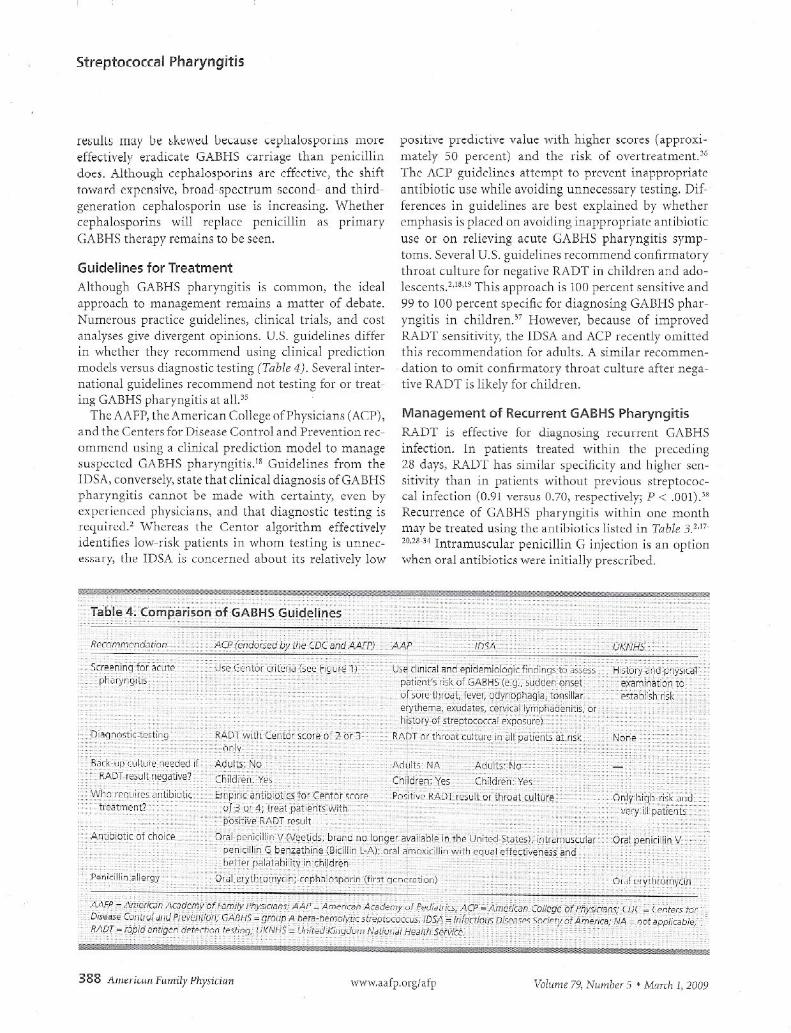
Guidelines for TreatmentAlthougll CABHS pharyngitis 1, common, the dealapproach to management remains a matter of debate.Nlunnous praclic(:' guidelines, clinical Lrials, ~md CDslJnJlyses give diyerg~nt opil'.ions. U.S. guidelines differin whether they recommend using clinical predictionmodels versus diagnostic testing (Table 4). Several inter-!1Jtionctl guidelines recommend not testing for or treat-ing GABHS pharyngiLi~ (.)l<Ill."
Th" AAFP, Lht:/l., m(;:ric:m Colkgt: ofrhYSlCl.1nS (i,en,;t.nOthe Centers for DiseJ.';e Control Jl1d Prevention l"tC-
omm('ncl using ,1 clinical pn:diclion model to managesuspecled CABHS ph:lryngitis.1i Guidelines from thelDSA, conversely, state that cli.nical diagnosis ofGABHSph;nyngitis CGlll10t be made wilh certainty.. c\'en byt::\'p~Ti.~Jlu~\1pb)'~.i.C1dn~,and that diagnostic: testing isr"lol{uircJ." \'\'herelS ["he: CenWr ~lgori.thm effectivelyidentifies ]O\\;-,'is],:patients ill whom 1esting is llHnec-f'SS;] Iy, th..., IDSA 1~ COclCcrueJ llbuul its relatively IOV'l
positive pledictiye value with lllgher scores (a.pproXl-matdy 50 percent) and the risk of oyertreatment.J6The ..I\C1' gl.li(kline3 Attempt to prevent in8ppropri<1teantibiotic use while avoiding unnecessary testing. Dif-ferences in gui.delines are best explained by whetheremphasis is plclCedon Jvoicling inappropriJte antibioticuse or on relieving acute GABHS pharyngitis symp-toms. Several u.s. guidelines recommend confirmatorythroallultu[c for l1cgalivl:RADT II1 chilJn:n aEd ado-lescents. !,lU) ThIS approach is 1(l() percent sensitive and99 to 100 percent specific for diagnosing GABHS phar-yngilis in chlJdren.37 However, because of Lillproved1\AD'1' sensitivity, the IDSA and ACP recently om.i.ttedthis rrcommencl:ltion Coradlllts. A slmilar recommen-dation to omit confirmatory throat cultLlre after nega-tive RADT is lihly for children.
Management of Recurrent GABHS PharyngitisRi\DT is effecLive fOJ Ji<lgno~in3 Ecurn:nt GABHSmfection. In patients treaT.ed \vithin the prec~dl11g26 (bys, RADT hJ.s similar specificily and higher sell-sitivity th811 111 patients wil;hout previolls streptococ-cal infection (0.91 verSllS 0.70, respectively; P < .001)."RecurrelKe of Gf\BHS pl1alynglu~ wi.thin one L10nthmay be trea.led using Lhe:antibiotic., listed in Tobh :-;Y"'20.23-3-1 IntramuS(ular penicillin G injection is an opt.ionwheJ1 OJ"JI JJ1tibiotic., wcre illLtiJ11y prtcSlTibed.
388 ."IIJ~riwflfrmriiy Physicilm "\vww,aaip,OlgJatp Voiume 79, NrwliJer S • M~ITCllJ, 20U9

Chronic Pharyngeal CarriageClnuHlI.. Fh"lyug<:dl carna.g<: 1& lh~ p~rslst~nt pres-ence of pharyngeal GABHS wll hU1l1 'Kliy<, Illft:cLiul1 urimmunciintlammatory nsponse. Patients may carryGABHS (01 one year d~spite treatment, Chronic car-riers ~re ~t little to no risk ()( imillune-mediated post-streptococcal complications because no active immuneresponse occurS.39 Risk of GABHS transmission is verylow and is not linked to invasive group A streptowccal(GAS) infections. Unproven therapies such a~long-lnmantibIOtic usc, treatmE'11t of pets, and exclusion fromschool and other activities have proved jneffective andare best avoided.)O Carriage of one GABl-{Sserotype Joesnot preclude infection by another; therefore, throat cul-tme or RADT is appropriilte wllen GA BHS pharyngitisis suspected. Testing is unnecessary if clinical symptomssuggest viral upper respiratory infection.
Antibiotic treatment may be appropri'lte III the fol-lowing persons or situations: rCCurr(~nl GABBS infec-tion ·within a family; personal history of or dose contactwith someone ,vho h8S had acute rheumatic fever oracute poststreptococcal glomerulonephritis; closecontact willi sorn~OIJ(: whu has GAS inkClion: com-munity outiJre,lk of acute rheumiittC fever, poststrcpto-COCCJl glomerulonephritis, 01· invasive GAS infection;health care workers or paticEb i.n hospitals, chroniccalc facilil·ies, or nur·SUlg homes; L-Imilies who CHl110tbe reassured, clild children ~t nsk of tonsillectomy forrepeated GABHS ph'Lryngitis.·<9Small RCTs suggest that
intramuscular benzaLiu nt: pen lulll [1 comblncd wllllfom days of or,d rifampin (Rifadin) or <l lO-day courseof oral dindamyci.n effectively eradicates the carrierstate.'" Oral din<iJ.llIycl11, J.lilitromycin, ,Hid cephalo-sporins ~re.~lso efftctivt'.
TonsillectomyThe effect of tonsillectomy on decreasing risk tor chronicor recurrent tousillitis is poorly Ilildentood. One trial inchildren showed that the frequency of recurrent tomil-litis decre<1.~eciin the tOJ)silJectomyiadenoiclectomy andcontrol groups.'o The surgical group had onc fewer epi-sode of severe GABHS pharyngitis annually; the authorsconcluded that this small potential beneflL did not justifythe risks or cost of ~urgery. A met~-analysjs of childrenand <ldLlltswith chronic pharyngitis comparing tonsil-lectomy ·with lloluurgicul lrc:alrncill \·\iJS inconclusive"AnuLher It'Lwspectivt' study based on data from theR\,cheSL.oI· fl'idemlulugy P!:O)l2cl found that childrenwitll tonsils are threE' times more likely to develop sub-SeCjlk'nt CABHS pharyngitis than those \"<'-hohad under-gone tonsillectomies (odds ratio = 3.1, P < .nn I).'12
Streptococcal Pharynqjtis
The AuthorSETHIl.. CH08Y, r"m, FAAFP is a board-certified famil~ pnysici,y, and riir2[-toorof I""s~al"d alld procedural training ill the Departmentol Family rliiedicine,UiliversiiyotTennessee-Chattanooga. Sh~receiv~d hei·medical degreefmlllWest Virginia UniVelSilY School of Medicine in Mi}rqamCl'Nn, ami mlJlill~lda tamil", medicine re,idency at tne UnivEsil"/ uf TrolllleS5~~-McI1Jphi"alld~ fellowship in :ldv;onccd ','Jomen', hCJlth Jlld [)bst~tr;(s ill thr~ Uniw,J',ityof Tennessee-51. Francis Hospital, Memphis. She alse completed a 1dClitydevelopment fellowship at thE Waco (Tex.) FaculW DeveloClmentCentH
Addre~, correspondence [0 Beth .4. Choi.'y. MD. FI'../JFP, iiT FamilyPractice Center, 1100 E. 3rd St., Cilattanooga, TN 37403 (e-rr:a.'l:helh.choby@erlangerorgj. Reprints a.cenot a'iailable from [he author.
Author disclosure: llr. Choby is Jil J55is,,,llt editor of Th,c (or·2 (omentReview of F"lTlily Medicine.
REFERENCES
Hing E, CherTY DK, I/Iioodwell DA. N"t;onal Am'oul"torv 1,,'oedic~1(J,eSurvey: 2003 Summary. Adv D~!a. 20C'5:~.f5:'L-:08
2. ~IS"W AL, Ce,bEr MA, (".'nltn~'i .![v·II,.:<ilrldClEl, Sch·,'iarLZ I\H. for tileInlecliOO'J, i);s"",e$ Soci~ly 01 AnoellCc. P"ictIC~guit!~iin.,\ Lr Ih~ diag-nO,;5 and rnam'~~IH""l "I g'''''p A slreplu,:m:Cdl pharyng;t;,. Gin .lnfeC1Dis. 2002:35(2): 113-125
3 Danc:1;n MH. Ro,I'YS S, Keipic L, el ~I. Burde,1cI xute sore li1ru"l andgroup (:0. strep,oco(cal pharyngitis on SCI1Col-<ly2d cnik:J,en 3nd th~irtamilies in Austr.1lia. i'pdi~l;ic2n07;p-J(5):9~O-957
4. L;eberm~n 0, Shval"tzman P, KmsoollS~y I, LierJrorman D. Ac·tiology ofr~,p;,ator\, Ifact irrjec,iorr~: clinical asse'isme(], '.'ersl" serological ,est,.8r j Gen P["Jet 2001 :51 (473i:J%-1 ooe.
5. Ebell MH. Smith IvIA, Barr}, H-:::, Iv€S K, Ce'e:.' [vi The r"tio~alclin;cal exam;~ction. OOES ihis p~te~t have strep thro2fi JArvi/'21)00: 284 (22):2912-2 918.
G Cen10r RM, V\,;thecspoon JM, Gal;on HP,2roliy CE, li~k I~.The diagnosisof strep til,od ill adui's in Ihe "FH~r'Jen~ym~"'. Med Deci5MJkir:g1'981;1(3)::.!3!oi-246.
7. MclscclC WJ, Goel V, To T, ~c·w DE. Toe veliaity of c SOr~ -::hrD3t scor~ ;nfam;ly practice. CMA'. :o'OOO;lF3:-o811-815.
fl. Eb~[[IvlH. lViaUng decision, a: Th~p:'''11 of .:,;re. ,·,m,.' II-"-u,,t. I-'-Jin ~r"ciIVlan.'1g Zf:()3;1(r(3)·68 69
9. J\ilcls~uc \fI'J, V,.'hite D, T1'~nel1!:>aull1 l), Low DL .". ,jiniL,1 ,COr~ Lareduce u,m~c~5silfyant;b;nt;c u,~ in palie~bwid·, ,·ore t~ro~t. C.'0,sU.l<;~il;lSo(l )75-33.
10 Gerber MA. Conlp"';SOrl of th,."~t r.ulture, and rapid ;L"~p test,io' diagncsis oj sueµLcccc~1 pharyngiti". Pediar, infect DIS !. 1989;8(11j:82Q-32'1.
11 Ezike E"I. Rongkavilit c.. Faid.;x ~"IR, Tho"'", RL. ;:,".',~fBI. Effect ofusillg 2 thro2.1 sv;abs 'is 1 till"ooal s~db vii detEction ~iWOI!r,~ 5trer-tOCOCCU5by a ["pic antiqf'n rle,Ftion t2,,' Arch Pes.'Jir Adoiesc '·ded.2005 ;159( C,): 486 -490
12 l\Jeuner .lIlIi, hamd MB, Ph;ll;p, Ro. Bona K, Aronson MD. OiJgn05is am:manJgemenL 01 allults ",·;til pha,yng;tis. A cCl5t-etfecc;ve~2ss an.".I,.,;,A."I.~imern Ivied. 2003:139(2):113-122
13. Mirzc fl, Wludyka P, -:::tlilln, Rathore MH. Hiroel cuiture is r,eces-$ary aiter ne~ative rapid Cifll1gen rlete~t;nn t~ot;;. Oin PCO"iJF (Phii~)2007J.6(3): .141-24 6
14 Gerber MA, Tanz RR. K~"O~(W H al. Optical irTnu'lo~ssay test ior~JuuiJ !-\ bet~-h~rTln'ylic screptococcOiI phrvnqitis. An 'Jific~"·~a$€d.mllltlc~nter investigation, )!lJ,Y1. 1997;27((11 ):ESS-90~.
15. V,ln 1·1(1·,./Jer;" I',·u~ni€r LP II. [I;o]nGs;$ ~Ild I\ldrl~~~"'~"'i ~'I pilolillyi-li; ill ~ p~cii",ric popul,"l'ion bJ:,d on (QJ1-eii~(ti'i,?r,e,s and proiect~cIh",.,lth Cli,;mm.;s. P"diMncs. 20C>6;117(J):609-C19.
';;w w. aalp.org! 2.fp .1mericarl Family Physician 389

Streptococcal pharyngitis
)6. Fisch('r p, !:-'dcm:!ing ill-c I'cdl <;iJlldaru uf '~~I~. F3"1 Pfii~[ Ivla!i<1b'.2nOil: I~ (;»:.:1.8. ht1f1:liWWW_,l~fr .mgifpmi 200302 OQ/48dcfc ,~.lml./\tleS,~,j S~~lellllJel2.4,20(lg,
17 ~;~ulm"n Sl, Gerber Iv1.'\_Sc, ',',hat's wron9 with ,~er"CIII:n for 5Trepthro~t! !'edfmrics. ~UU4:-:Uf6):Hll;;-liJI'J
18. C"oper RJ, H?fiman JR, Bartlett! !G, et al. for ",he American A~ad~myul ,"",iii P;"IC'ieiJn,;, AII'~ricJ;1 (ulbjE ur Pil,'5ician, A""erica" Soc;-eeY of Internal Medicine, Cen,~I$ Ic'r D;,ea,2 Control a~d Preve~1ion,Pri,,(,pl~$ of "PPl"op,iate antiblCtic u,e for cCl'te phc!),~9itis in adults:be,;kg,,,und. Ann ,Intern i',1ed. 20GI :13,1 :6:,:509·517.
1t}.American AcaJe;n:, ul Ped>atrKs, Committee on Infectiouo Dis€a,es.Red BOOK. 26th ed. Elk Gro,E Vill"ge, III.: !'-.mHI~a;14cddem'i d ,~d;at-Tics; 2003:578-58C
20. Dajani:', Tauber! K, ferrieri~, Pel~r G, Shul",,,,, S. T;e~tr"~"1 .", aculpsirertoG1c.(~1 pn3t).-n<)iti, Jilt; prevemion d rheum"tic fe\'H a 'tace-"'~nl fDr ho"lti', proi€s;ianals, C2mmit1e~ on Rheumatic F""ler, ::nc'J-carc'itis, 2nd :<o)\,a.,aki Dis€ase oj thE CounCJi on '~ardiovas~ular Diseasei~ the Y-:'Lh10. the /',mHinn Heart AsooJciation. f'edia!ncs El':lS;S514 pt 117S8-76.:l
i.'I. (2ntor i(M. AlliSDn JJ. Coh~n S. f,laryngitis mcnag~mem deji~ing the(Qnlro'fero,' ..j Ger. I~tcr,.Mec'. 2007:22·~j):127-1~0.
22 D~I M~r CB, Gb:;7.;olJPP,5p;nks AB. Anbclctics ior sxe thrnat. Cochre""i'Jwba.'p Sy" Fe'i. ~1106;(~:I;CDDO(l(ln
23 M~rriil B, KF.I,benj G. JJnkow,k, TA, Dani; P. ClInical inQL'lrie<;. II','r,,,l isthe mo,t effectl')? di"'lltu,tir. e'j~IUction ct <;treplococ':al phary~gi'is7j ,'ar", .Praci. 20i14;53(9):734·74o]
24. Cooper ru, I-Iofb-,all lEO:. 8arLINl JG, et al jar the Centers 101' Ci,-(''''e (onllol ;;J.J I'rev?,,!i,,". Frincipl'20 ot JPpr~"ri2te OiT;ibiotic l'Sefur dCUt'2 ph<lrvngitis i~ ~dults: bac\:,lround. Ann Em~rgMeJ, 1U01,37(5:'711-719
25 Rimoi" ;:':,.,\', rlam2a HS, Vince /0., ei al. E-Jaluation 01 the \11/1-:0 clini-cal decisio~ r"le b, ,,;eotocccCill pharyngitis. Ar,-I~ Dis Chi.'d. 2~"()S;90(10):1llGG-1070
26 Sharlend M, Kendall H, Yeat~' D, et ai, An!;:~ioJ!ic prp.,ccibillg in ger,-eral p'iictice and ho,pi,,,1 ~~jmission:, 121 perit'Jnsillar aGs-:~ss, rn~:-tQidilis, and rilelJ;r.'llic it'lcr in d'ildren: ,Ime tre"d an~il'sis. 81'vU2005;331 (7~12):323-329.
27. Snellman LW, <;l~llg ""I, S,ang Jlvl, !Qhn,on Df., tUµlci;! EL, Durationoi pmiti,'c ihro2.l cullw", Jor group A 5,r~pt~,~~,~ci oiter i~i'ti~ti'8n ofantiniOlic tiler~p\, :',:diMr,'c,'. IS'S3;9'1(6):IIi1fi-1170
28 K"plan EL. Joh",oll GP" 0",1 ~QSan8 MC, Hem CL. Suscepli;,ilil,' (,Ivroup A. ben-hemol:,tic strepocnr.o lO lr""e'?n antibioti,:s: exomir;Jlion
390 Ameriwn P".,,,,ily Physiciall
01 301 $LI~irr$ i$vlatd ill LII~ Urrit~J SLiil'c" l!~tWt'cil 199.1 ""U 1997,PCafO[f InfcG Dis.'. 1999: 18( 12): ID69-i072
2.9. Casey JR. S~lectiliv L);€ uplilTldl '1IIIil'il)ti[ i" L(I(' Trf'~,ITli"lil of gf()U[,.t:; '~AtJ-hemolyll( strep;n(OCcl rMrY~CI'lIS n'n 1'",d.'!'Jtr{I'iui,,;2007; 46(suppll ):25$-3 5S,
30 F",d2r Hi'A J" Gerber HA, RZ1doll'h MF. ~telm<ch 1'5, l(a.~lan I:L, Once-daily thera8Y for streptococcal ~har,'n'liti5 wiih alT1o,licillin, P",li",l.-i':51999:103(1):47-S1
31 Clegg H\N, RY2,n AG. Dallas S0, ~tal. Tr<2~tm~~t~f,t'e~tQcoc<:al.~;lar-yngiti5 with onc~-deil:1 compared ,,",;th tv,ke-c~ily arlloxi:iliin, a n~"l-infeciority triDI. Pedlatr Jnfecr Ois J 2oJ06;2S{S)761-161'.
32, Martin JM, Gre~n M, 8abac,~ra :<A, ·Nold ER. E'-j'thrc-lT,ycin-r":,j,,cn1group fA ,treptococ<:i in schoolchildren ill ~ilL{~,-"g'L tv' Eilf:.1 j ,%-,J.2U01;346(1O):1200-1206,
33, Marcy Slvl. Trf'i'.'m~nt olltlo,1'. tor >trcptococcJI ph~rJ·ngik. Gin PcdiJtt(Phi/a), LOU7;46I,suµpIIU6S-45S.
J~ Ca,ey JR, PichichNO iI.'1E.MRt~-~n,"ly"" or c,;ph.'I~:'.:)(, ..in """"'; ,)O'"iol-lin LCC'dime"t of grou.~ fl. str'O,)lOcoccal t'Jnsillophacyngi,i" in childT2nPediatrics. 2004;113(,,):866-882
35 Linder JA, Chan JC, Botes DVV.Evaluation and treoime~t ~fph~r'ingitisin primar:{ Care wa(tice: tile diii€r0ncc '"pll'.','en qLJirJelin~s is l~r'Jelya·cademic Aid, .Ir,!era .rv1",~'.LC-OE:166(i3): 1374-1379
30. Bisno 4L. Diagnosing sHep throd If>th~ adult patiem: do cllnr-:ai :ritcria,eolly suitice' Ann inrer~'M"d. 2003;139(2):15'..1-1 S1
37 Mcl5;;ac \NJ, Kellner JD. -".ulrich! p. V"nja~<a A, Low DO:. Empiriol 'ialidi'-tion Gi ,;uidelincs fOl the mar'''9pment ')j pharyngitis in (hil~r~n and~d'"ljs [published correcti"ln appears in JA,'IiA 20U3;2S4(21):Z;;OQ].JANik 20()~;291 (131.1587-15SS
~5,SheeiN RD, Houston MS, Rdd'<e S, Da10 K, A.d~m5"n Sc. A(cur~(y atr"pid ,LI~p te5ting in patients 'Nho haw had (E'cent Sl'-Cpl"'~~'~c~1 phar-yngitis.,' Am 80""; Film P,'aG. 2002:15<:4):201-265
39, Tar'" RR, Shulman ST. Chronic pharYllg€al [&li2ge oi gro'Jµ ,'" sm'pto-cocci. ,De~'iatcInfen Di, .I. 2007;26:2).11'5-176
40. P'''ildisEO JL, BluestonE :::D, Colborn DK, Bem~rc BS. ROCkeTt', HE, Kur:;-Lasky M. Tonsillectomy and 2.jenOlOn$ill~(to<nyiGr rH'_"'~"t ,t;ro~t infcc-ti"" in mocer:ltely aif~ded children. Pedi,,~r.i~.,.2002:11[1(1 u' 1)7-15.
41 BurLon lvI), T"wl~1 B, GIJS2iou;" Ton,illp(tomy versus non.S'Jrgic"ll,-eat-ment for cl110niclrecurrent acllte lonsilliti,. Coc!."iJr"~ O",ab,'se 5yst !lev1999;(3):CDOOI802,
42. CI,vi(k; LJ, 51 Sauve, .II., \J,haver ,~.L. Eificacy of colljll~U(j"l'i in L'ea'-mel·,t of recurrent gmLlp t, bet~-IK·rHolyLi, :;treptococcal pna,yngijis,Laryngocwpe, 2006;1.6(11 ):1946-1950
wW1V.aafp,org,,' Il'