Acute Pharyngitis
28
ACUTE PHARYNGITIS Description: - A sudden painful inflammation of the pharynx, the back portion of the throat that includes the posterior third of the tongue, soft palate, and tonsils. - commonly known as SORE THROAT. Incidence: - Increased during winter and early spring. Pathophysiology: VIRAL (most cases) BACTERIAL (10%) PREDISPOSING FACTORS PREDISPOSING FACTORS - Exposure to viral agents - Bacterial upper respiratory tract infections - Poorly ventilated rooms CAUSATIVE AGENTS CAUSATIVE AGENTS Adenovirus, influenza virus, GABHS, Group A Streptococcus Epstein-Barr virus, (GAS) or Streptococcus pharyngitis Herpes simplex virus Others: Mycoplasma pneumoniae Neisseria gonorrhoeae, H. influenzae Type B Enters into the system by way of droplets of coughs and sneezes and unclean hands that have been exposed to the contaminated fluids Lodges in the pharynx and initiates an inflammatory response
-
Upload
ytser-limsiaco-limpicardo -
Category
Documents
-
view
104 -
download
4
Transcript of Acute Pharyngitis

ACUTE PHARYNGITIS
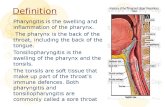
Description: - A sudden painful inflammation of the pharynx, the back portion of the throat that includes the posterior third of the tongue, soft palate, and tonsils.- commonly known as SORE THROAT.
Incidence:- Increased during winter and early spring.
Pathophysiology:
VIRAL (most cases) BACTERIAL (10%)
PREDISPOSING FACTORS PREDISPOSING FACTORS- Exposure to viral agents - Bacterial upper respiratory tract infections - Poorly ventilated rooms
CAUSATIVE AGENTS CAUSATIVE AGENTSAdenovirus, influenza virus, GABHS, Group A Streptococcus Epstein-Barr virus, (GAS) or Streptococcus pharyngitis
Herpes simplex virus Others: Mycoplasma pneumoniaeNeisseria gonorrhoeae, H. influenzaeType B
Enters into the system by way of droplets of coughs and sneezes and unclean hands that have been exposed to
the contaminated fluids
Lodges in the pharynx and initiates an inflammatory response
Pain Fever Malaise Enlarged and tender Vasodilation Edema Tissue damage(High) cervical lymph nodes
(Fiery-red) Redness and swelling of the tonsillar pillars, uvula and soft palate (may demonstrate petechiae of the roof of the mouth
If untreated Formation of creamy exudate in the tonsillar pillars (white-purple exudate)
COMPLICATIONS: Common: Sinusitis, Otitis media Bad breathePeritonsillar abscess,Mastoiditis, Cervical adenitisRare: Bacteremia, Pneumonia,Meningitis, Rheumatic fever, Nephritis
Note: Painful sore throat (1-5 days), headache, myalgia, & nausea are added S/Sx for streptococcal pharyngitis.

CHRONIC PHARYNGITIS
Description:- Is a persistent inflammation of the pharynx
Pathophysiology:
Risk factors:Working in dusty surroundingsExcessive use of voice RECURRING INFLAMMATION Chronic cough OF THE PHARYNXHabitual use of alcohol and tobacco
General thickening and congestion HypertrophicOf the pharyngeal mucous membrane
If it remains untreated and progresses,The membrane becomes thin, whitish, Atrophicglistening, and at times wrinkled
Swollen lymph follicles becomes Chronic granularnumerous in the pharyngeal wall “clergyman’s sore throat”
constant sense of irritation mucus collects in the throat difficulty intermittent postnasalor fullness in the throat (can be expelled by coughing) swallowing drip causing minor
irritation and inflam-
mation of the pharynx

TONSILITIS AND ADENOIDITIS
Description: - Inflammation of the tonsils and adenoids, often thought as a childhood disorder, but can occur in adults.
Pathophysiology:
Risk factors: - Alcohol use, smoking, splenectomy, weakened immune system (DM, Chemotherapy, etc.), sinusitis, exposure to someone with tonsillitis.
CAUSES:Bacteria VirusGABHS Epstein-Barr virus (90% in adults affected) and
Cytomegalovirus
Entry into the system (tonsils and adenoids) and multiplies
Inflammatory process sets-in
ENLARGED
Tonsils Adenoids
Sore throat Mouth-breathing Fills the space behindFever Earache the posterior naresSnoring Draining earsDifficulty swallowing Frequent head colds
Noisy respiration Nasal obstruction
If untreated: Complications
Infection extends to the middle ears Infection extends to the mastoid cells
Acute otitis media Mastoiditis
Rupture of tympanic membrane
Deafness

PERITONSILLAR ABSCESSDescription:
- Also known as “quincy”, a common major suppurative complication of sore throat.
Pathophysiology:
GABHS
Sore throat (an acute tonsillar infection) (as a consequence of previous infections of the tonsils, adenoids, etc.)
If untreated: Complications
Infection spreads causing the collection of Enlarged and tender purulent exudate between the tonsillar cervical lymph nodes
capsule and the surrounding tissues and soft palate
severe sore throat inflammation of the superior inflammation of the medial ptyregoid musclefever constrictor muscle of the pharynxraspy voice
(severe sensation of burning, pain spasm squeezing pain while swallowing)
Odynophagia
difficulty swallowing trismus
(dysphagia) (inability to open mouth) Drooling
local cellulitis and abscess formation pain on lateral head spreads over the palate, the neck and chest movement
Edema in the palate, neck and chest
Respiratory arrest Infection may spread and may cause Mediastinitis, intracranial abscess, Empyemas
Further spread of infection
Death Systemic infection

LARYNGITIS
Description: - Inflammation of the larynx.
Incidence:- Common during winter (viral laryngitis)
Pathophysiology
Risk factors: Predisposing factors:- Voice abuse - Exposure to sudden changes in temperature- Exposure to dust, chemicals, smoke or - Dietary deficienciesother pollutants - Malnutrition- Upper respiratory infection - Immunosuppressed state(allergic rhinitis and pharyngitis)- Infection of the vocal cords- Gastroesophageal reflux (Reflux laryngitis)
Causes:- Causative agents for common colds and pharyngitis (bacteria and virus-common cause)
Presence of predisposing and risk factors
Entry of causative agents
Inflammation and infection of the larynx uvula is visibly edematous
(if with allergies)ACUTE Laryngitis
Hoarseness of voice Severe cough Sudden onset made worse Throat feels ‘tickle’ in the or Aphonia (complete and dry sore by cold dry wind worst in throat made loss of voice) throat morning and worse by cold
improves when air/liquids in a warmer
climate
CHRONIC Laryngitis
Persistent hoarseness

OBSTRUCTION AND TRAUMA OF THE UPPER RESPIRATORY AIRWAY
OBSTRUCTION DURING SLEEP
Obstructive Sleep Apnea (OSA)Description:
- Is a disorder characterized by recurrent episodes of upper airway obstruction and a reduction in ventilation.
- Cessation of breathing (apnea) during sleep usually caused by repetitive upper airway obstruction.
Pathophysiology:
Risk factors:- Obesity - Alterations in the airway (structural changes like tonsillar - Male gender hypertrophy, abnormal posterior positioning of one or - Post-menopausal status both jaws, and variations in craniofacial structures) that- Advanced age contribute to the collapsibility of the upper airways.
Normally the pharynx is a collapsible tube that can be compressed And during sleep the muscles of the upper airway is reduced
Presence of risk factors
Reduction in the diameter of the upper airway
Obstruction
Frequent and loud snoring with Small amounts of negative pressure breathing cessation for 10 secs are generated during inspiration
or long (5 episodes/hour)
Snorting Apnea Upper airway collapse
Gasping Hypoxia and hypercapnia
Choking Sympathetic response
Apneic episodes Hypertension Dysrhythmias in reported clients with CVD
by the partner Increased risk for MI and Stroke
Sudden awakening Chronic fatigue Insomnia and difficulty DEATH going to sleep

Hypersomnolence Early morning awakenings (Daytime sleepiness) with an inability to go back to sleep
EPISTAXISDescription:
- Also known as nosebleed- a hemorrhage from the nose, is caused by the rupture of tiny, distended vessels in the mucous
membrane of any area of the nose.
Pathophysiology:
Risk factors:- Local infections (vestibulitis, rhinitis, sinusitis) - Thrombocytopenia- Systemic infections (scarlet fever, malaria) - Use of aspirin- Drying of nasal mucous membrane - Liver disease- Nasal inhalation of illicit drugs (cocaine) - Redu-Osler-Weber syndrome- Trauma (picking the nose, blunt trauma, (hereditary hemorrhagic
(fracture, forceful nose blowing) telengiectasia)- Arteriosoclerosis - Hypertension- Tumor (sinus or nsapharynx)
Presence of any of the risk factors
Rupture of any of the following
Anterior ethmoidal artery sphenopalatine artery in the internal maxillaryOn the forward part of the roof posterosuperior region branches
Bleeding
NASAL OBSTRUCTION
Description:- Obstruction of the nose
Pathophysiology:Causes:
- Deviation of nasal septum- Hypertrophy of the turbinate bones- Pressure of nasal polyps
Obstruction of the nose Nasopharyngitis
Difficulty in maintaining an adequate airway Infection extends to the
nasal sinuses
Breathing through Sleep deprivation Rhinosinusitis

the mouthDrainage is obstructed
Dryness of the oral mucosa andpersistent, dry, cracked lips Pain
FRACTURE OF THE NOSE- Is the break in the continuity of the nasal bone.
Pathophysiology:
Cause:
Direct assault on the nose
Tearing of the Rupture of Trauma to the Break in the continuitymucous membrane blood vessels nasal area of nasal bone
Nose bleeding Hematoma Fracture
Complications:InfectionAbscessAvascular or septic necrosis

LARYNGEAL OBSTRUCTIONDescription:- Obstruction of the larynx
Pathophysiology:
Precipitating factors:
History of allergies,exposure to medications, anaphylaxis edema of larynxlatex, foods, and bee stings
Foreign bodies lodges into the larynx
Heavy alcohol consumption; causes tumorheavy tobacco use
Family history of airway angioedemaproblems
Use of ACE-inhibitors angioedema of mucous membranes
Recent throat pain or infectious processRecent fever
History of surgery or subglottic stenosisPrevious tracheostomy
History of nasogastric nasogastric tube syndrometube placement
Laryngeal Obstruction
Closes off the opening in the larynx
Air passage is compromised during inspiration and expiration
Lowered oxygen Use of accessory Retractions in the neck or saturation muscles of respiration abdomen during inspirations
Client may faint or collapse Respiratory arrest
Death

CANCER OF THE LARYNXDescription:
Pathophysiology:
Etiology of cancer is unknown.
Risk Factors:
CARCINOGENS: OTHER FACTORS:- Tobacco (smoke or smokeless) - Straining the voice- Combined effects of alcohol and tobacco - Chronic laryngitis- Asbestos - Nutritional deficiencies (riboflavin)- Secondhand smoke - History of alcohol abuse- Paint fumes - Familial predisposition- Wood dust - Age (higher incidence after 60 yo)- Cement dust - Gender (more common in men)- Chemicals - Race (more prevalent-African Americans)- Tar products - Weakened immune system- Mustard gas- Leather and metals
Failure of the regulatory mechanism of normal cells and growth continues in excess
Neoplasia
Benign Malignant
Uncontrolled growth of cells or cell division
Tumor
Because malignant cells Lack of adhesion and are not encapsulated loss of contact inhibition
Expands into surrounding Spreads to distant parts of tissues (Invasion) the body (Metastasis)
Lump in the neck Impedes the action of - Cervical lymph adenopathy

the vocal cords - Unintentional weight loss- A general debilitated state- Pain radiating to the ear
- Hoarseness (harsh, raspy and low in pitch voice)- Persistent cough or sore throat- Pain and burning in the throat when consuming hot liquids or citrus juices
Late symptoms:
- Dysphagia - Dyspnea - Unilateral nasal obstruction/discharge- Persistent hoarseness - Persistent ulceration - Foul breath

ATELECTASIS
Description:- Refers to closure or collapse of alveoli and often described in relation to x-ray findings and clinical signs and symptoms.
Pathophysiology:
Causes:-Altered breathing patterns -Retained secretions -Pain-Alterations in small airway -Prolonged supine -Increased abdominal
functions positioning pressure-Reduced lung volumes due -Restrictive defects -Specific surgical proceduresto musculoskeletal or (i.e. upper abdominal, neurologic disorders thoracic or open heart surgery)
Reduced ventilation or blockage that obstructs passage of air to and from the alveoli
Alveolar air becomes trapped
Trapped air is absorbed into the bloodstream
No additional air can enter into the alveoli
Patchy infiltrates/consolidated areas in Alveoli collapse Predisposes to infection the lungs in the x-ray
Pulmonary infection
Hypoxemia Dyspnea Cough Sputum production
Respiratory distress
- Tachycardia - Tachypnea - Pleural pain - Central cyanosis - Anxious
Acute Respiratory failure

Death
RESPIRATORY INFECTIONS
Acute TracheobronchitisDescription:
- An acute inflammation of the mucous membranes of the trachea and the bronchial tree of, often follows infection of the upper respiratory tract.
Pathophysiology:
Causes:Streptococcus Haemophilus Mycoplasma Fungal infection
pneumoniae influenzae pneumoniae (Aspergillus)
Enters into the system and initiates inflammatory process
Inflammation of the mucosa of trachea and bronchi
Dry and irritating cough Production of - Fever mucopurulent sputum - Chills
sternal soreness - Night sweats Expectoration of scanty - Headache
amount of mucoid spututm - Body malaise
As infection progresses
Shortness of breath Inspiratory stridor Expiratory wheezesExpectoration of purulent sputum
Irritation of the mucosa of airways
Blood-streaked secretions

SEVERE ACUTE RESPIRATORY SYNDROMEDescription:
Pathophysiology
Predisposing factors:- Living or traveling in places with SARS cases- Close contact with infected people
CAUSE Corona virus CAUSE
through respiratory droplets touching contaminated objects orwhich either lodges on mouth, nose, or eyes) surface and then touching ones
mucous membranes
Incubation period (2-7 days)
Enters into the system and multiplies
Inflammatory process sets in (symptoms appear within 10 days)
Fever greater that 38 Celcius Cough Difficulty breathing
Poor prognosis if accompanied with the following factors:- Old age- Comorbid condition (DM, COPD and Chronic Hep B)- Atypical symptoms- Elevated serum lactate dehydrogenase on admission- Acute renal failure

PULMONARY TUBERCULOSISDescription:

LUNG ABSCESSDescription:

PLEURAL CONDITIONSDescription :
- Are disorders that involve the membranes covering the lungs (visceral pleura) and the surface of the chest wall (parietal pleura) or disorders affecting the pleural space.
PLEURISYDescription:- also known as ‘pleuritis’, is the inflammation of both layers of the pleurae (parietal and visceral) which is in conjunction with other disorders of the respiratory system.
Pathophysiology:
Pneumonia URTI TuberculosisCollagen disease Trauma to the chest Pulmonary infarction or embolismAfter thoracotomy Primary or metastatic cancer
Inflammation of the parietal and visceral pleura
With respiration
Rubbing of the two Pleural friction rub upon pleural membranes auscultation (early stage)
Stimulation of the nerve endings on the parietal pleura
Severe, sharp, knifelike pain (pleuritic pain) which worsens when taking a deep breath,
coughing, or sneezing (usually one sided and becomes absent or minimized when the breath is held)

PLEURAL EFFUSIONDescription:
- a collection of fluid in the pleural space, is rarely a primary disease, usually a secondary to other diseases.
Pathophysiology:
Causes: (pre-existing conditions)Heart failure Tuberculosis Pulmonary infection (viral)
Pulmonary infections Pulmonary embolusNeoplastic tumors Nephrotic syndrome(bronchogenic carcinoma) Connective tissue diseasePneumonia
Causing an imbalance in the Inflammation by bacterial products hydrostatic pressure and or tumors of the pleural surfacesoncotic pressure in the lungs
Formation and reabsorption Extravasation of fluid into of pleural fluid is altered tissues or cavity
Effusion of clear fluid
Transudate Exudate (Meaning pleural membranes are not diseased)
Decreased/Absent breath sounds Decreased fremitus Dull, flat sound on percussion
Small effusion Large effusion Malignant effusion- minimal or no dyspnea - Dyspnea (shortness - Dyspnea
of breath – SOB) - Difficulty lying flat- Coughing
Acute respiratory distress Tracheal deviation away from the affected side

Note: Signs and symptoms are dependent on the size of effusion, speed of formation, and underlying lung disease (eg. If the cause of the effusion is pneumonia, the client will also exhibit signs and symptoms of pneumonia).
EMPYEMADescription:
- Is an accumulation of thick, purulent fluid within the pleural space, often with fibrin development and a loculated (walled-off) area where infection is located.
Pathohpysiology:
Causes:Common cause: As a complication of Other causes: Penetrating chest trauma
Bacterial Pneumonia Hematogenous infection ofor Lung abscess the pleural space
Nonbacterial infectionsIatrogenic causes (after thoracic surgery or thoracentesis)
Initial Stage Pleural fluid is thin Low leukocyte count
Progression
Fibropurulent stage Thick exudative membrane -Decreased or absent breath encloses the lung over the affected area (loculated empyema) -Decreased fremitus
-Dullness on chest percussionFever
Night sweats Pleural pain
Cough Dyspnea Anorexia Weight loss


http://nurseslabs.com/pathophysiology/bronchitis-pathophysiology/http://nurseslabs.com/pathophysiology/chronic-obstructive-pulmonary-disease-copd-pathophysiology/