Diabetic foot
115
Dr. Joe M Das DIABETIC FOOT
-
Upload
joemdas -
Category
Health & Medicine
-
view
1.024 -
download
0
Transcript of Diabetic foot
Slide 1
Dr. Joe M DasDIABETIC FOOT
Every 30 minutes a limb is lost due to a landmine.
Every 30 seconds, a limb is lost due to diabetes.
- Bahara, Mills et al. International Wound Journal 2009.
The theme Diabetes education and prevention (2009 2013)
Statistics 60-70% of those with diabetes will develop peripheral neuropathy, or lose sensation in their feet.
Up to 25% of those with diabetes will develop a foot ulcer.
More than half of all foot ulcers (wounds) will become infected, requiring hospitalization and 1 in 5 will require an amputation.
After a major amputation, 50% of patient will have their other limb amputated within 2 years.
The History of Diabetes1552 BC: the first known mention of diabetes found on the Ebers Papyrus
Egyptian physician Hesy-Ra of the 3rd Dynasty makes
Lists remedies to combat thepassing of too much urine
Wood Carving of Hesy-Ra
The History.. Contd250 BC: Diabetes described as the melting down of flesh and limbs into urine By Greek physician Aretaeus of Cappodocia who gives the first complete medical description of diabetes
1425 AD: Diabetes first appears in the English language as the Middle English word diabete.
16th Century: Swiss physician Phillipus Aureolus considered the Martin Luther of Medicine identifies diabetes as a serious general disorder.
1776: English physician Mathew Dobson of Liverpool evaporates two quarts of urine from a patient with diabetes. The resulting residue is granulated and smells and tastes like sugar, conclusively establishing the presence of saccharine materials as a diagnosis of diabetes.
The History Contd
Phillipus Aureolus
1869German medical student Paul Langerhans
The islet cells of the pancreas but is unable to explain their function.
The find is dubbed the islets of Langerhans.
The History Continues..
1871: French physician Apollinaire Bouchardat notices the disappearance of glycosuria in his diabetes patients during food rationing of food under the Siege of Paris in the Franco-Prussian War, and formulates individualized diets to treat the condition.
1889: Scientists Oskar Minkowski and Joseph von Mering of the University of Strasbourg, France demonstrate how removing a dogs pancreas produces diabetes.
The History Continues..
Apollinaire Bouchardat Oskar Minkowski
1901: American pathologist Eugene Opie of John Hopkins University in Baltimore establishes a connection between the failure of the islets of Langerhans in the pancreas and the occurrence of diabetes.
1913: Prof. John J.R. Macleod writes a monograph on diabetes entitled Diabetes: Its Pathological Physiology.
The History Continues..
Dec. 1916: Boston pathologist Elliott Joslin compiles 1,000 of his own cases and creates the textbook The Treatment of Diabetes Mellitus. In it he reports that the mortality of patients was approximately 20 per cent lower than for the previous year, due to the introduction of fasting and the emphasis on regular exercise.
1919: Dr. Frederick Allen of the Rockefeller Institute in New York publishesTotal Dietary Regulations in the Treatment of Diabetes that introduces a therapy of strict dieting dubbed the starvation treatment - as a way to manage diabetes
The History Continues..
Dr. Frederick AllenElliott Joslin
Oct. 31, 1920Sir Frederick Grant Bantingconceives of the idea of insulin after reading an article in The Journal Surgery, Gynecology and Obstetrics by Moses Barron, by an American pathologist, titled The Relation of Islets of Langerhans to Diabetes with Special Reference to Cases of Pancreatic Lithiasis.
With the support of Prof.. Macleod of the University of Toronto, and the assistance of Best, a medical student he starts his research using a variety of different extracts on depancreatized dogs.
The History Continues..
Summer 1921: Bantings work leads to the discovery of insulin. On July 30, Dog 410 is the first to receive the extract. On August 4 the extract is called Isletin for the first time.
Nov. 14, 1921 Dr. Banting and Charles Best deliver a preliminary report of their research to the Journal Club of the University of Toronto, Department of Physiology.
Nov. 17, 1921: Banting and Best discover that extract from cattle foetal pancreas lowers blood sugar levels of depancreatized dogs, leading them toward plentiful, cheap sources for insulin. Experiments begin to test the long-term effectiveness of insulin treatment.
Dec. 30, 1921 :Banting, Macleod, Best and Dr. James Bertram Collip, a biochemist present the results of their research at a session of the American Physiological Society at Yale University. The paper initially generates little interest. The paper The Internal Secretion of the Pancreas is published two months later in the prestigious Journal of Laboratory and Clinical Medicine
More Of Banting & Best
Oct. 25, 1923 Banting and Macleod The Nobel Prize in Physiology or Medicine.
Banting shares his award with Best Macleod shares his with Collip.
The Nobel Prize Goes To.Banting & Macleod
Banting's and Best's laboratory, where insulin was discovered.
11th January 1922 Leonard Thompson, 14, A charity patient at the Toronto General Hospital, First person to receive and injection of insulin to treat Type 1 diabetes. Thompson lives another 13 years before dying of pneumonia at age 27.
The History Continues..
May 3, 1922: The word insulin is used in public for the first time when Macleod presents the paper The Effect Produced on Diabetes by the Extracts of Pancreas to the
May 30, 1922: Pharmaceutical manufacturer Eli Lilly & Co. of Indianapolis and the University of Toronto enter a deal for the mass production of insulin.The History Continues..
1966
First pancreas transplant
University of ManitobaThe History Continues..
July 7, 1989: Her Majesty Queen Elizabeth The Queen Mother kindles the Flame of Hope at Banting House National Historic Site The Birthplace of Insulin in London, Ontario. As a symbol of hope, the flame will burn until a cure for diabetes is found.
March 1999Scientists conduct the first successful islet transplant at the University of Alberta Hospital.
The Edmonton Protocol. isolating islets from a cadaveric donor pancreas using a mixture of enzymes called Liberase
The History Continues..
Dec. 20, 2006: The United Nations recognizes diabetes as a global threat and designates World Diabetes Day, November 14 in honour of Frederick Bantings birthday as a UN Day to be observed every year starting in 2007.
PathogenesisChronic hyperglycaemiaNerve microvascular dysfunction free radical formation (due to NADPH)Polyol pathway hyperactivity (Glucose sorbitol myoinositol Na-K ATPase)PKC hyperactivityNonenzymatic Abnormalities of nerve growth
Pathology:Axonal loss distally, with a dying back phenomenon
A reduction in myelinated fiber density and
Focal areas of demyelination on teased fiber preparations.
Neuropathy
MotorSensoryAutonomic
nociception Proprioception,Unawarenessof foot position
A-V Shunt* openPermanentIncrease footBlood flowBulging foot veins,Warm footReduced sweating
Dry skinFissures andcracks
Muscle wastingFoot weaknessPostural deviationDeformities, stressand shear pressures
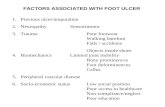
Trauma
Stress on bones & jointsPlantar pressure
Callus formation
InfectionUlcer
Symmetrical neuropathiesAsymmetrical neuropathiesDistal sensory and sensory-motor neuropathyMononeuropathyLarge-fiber typeMononeuropathy multiplexSmall-fiber typeRadiculopathiesDistal small-fiber neuropathyLumbar plexopathy or radiculoplexopathyInsulin neuropathyCIDPCIDP
Distal Symmetrical Neuropathy
The commonest neuropathic syndromeDiabetic neuropathyA length-related pattern of sensory lossToes Feet Leg (stocking pattern)Later motorAutonomic neuropathy is less common
Autonomic neuropathy:
sweating dry skin that is likely to crack easily risk of infection.
Warm because of the arterio-venous shunting Distension of foot veins that fail to collapse even when the foot is elevated
A gangrenous toe in a foot that has bounding arterial pulses may be seen as there is impairment of the nutritive capillary circulation because of arteriovenous shunting.
The oxygen tension of the blood in these veins is typically raised.
Neuropathic edema, which is resistant to treatment with diuretics but may respond to treatment with ephedrine
High blood sugar expeditesartherosclerosis giving peripheral vascular disease (reduction of blood supply to the foot).
The delivery of essential nutrientsand oxygen to the foot iscompromised leading to anaerobic infections and tissue necrosis.Peripheral arterial disease
Artherosclerosis narrows or blocks the arterial lumen
Foot ischaemia
Foot ulcer Necrosis/ GangreneInfection
Artheroma plaque narrowing the arterial lumen
Ischaemic toes due to artherosclerosis
Peripheral Arterial Disease
Clinical features (Contd..)Ulcers vibration senseGlove and stocking distribution of sensory loss+ve Rombergs sign; ankle tendon reflex
Wasting of small muscles of feet Unopposed pulling of long extensors and flexors Clawing of toes Elevated plantar pressure points at the metatarsal heads Callus formation & foot ulceration
Charcot arthropathy
A progressive condition of the musculoskeletal system that is characterized by joint dislocations, pathologic fractures, and debilitating deformities.
Charcot FootMore dramatic less common 1%
Severe non-infective bony collapse with secondary ulceration
Two theoriesNeurotraumaticNeurovascular
Charcot FootNeurotraumaticDecreased sensation + repetitive trauma = joint and bone collapse
NeurovascularIncreased blood flow increased osteoclast activity osteopenia Bony collapseGlycolization of ligaments brittle and fail Joint collapse
Charcots Foot-- ClassificationEichenholtz
1 acute inflammatory processOften mistaken for infection
2 coalescing phase
3 - consolidationLocationForefoot, midfoot (most common) , hindfoot
Atrophic or hypertrophic Radiographic findingLittle treatment implication
Wagners classificationDepth of penetrationExtent of tissue necrosisTreatment given
Grade 1
No open lesion, skin intact
Potential site for ulceration like prominent metatarsal heads, hammer toes, Charcots deformity
Treatment: Education & preventionSelf foot care & proper shoesAntibiotics for cellulitis
Grade 2
Superficial ulcer extension to subcutaneous adipose tissue
Treatment:Wound care + antibioticsRadiological evaluationModified weight bearing bone resection
Grade 3
Ulcer penetrating joint, deep abscess, OM, tendon sheath infection
No digital gangrene
Treatment:HospitalisationDebridement and IV antibioticsJoint and bone resection
Grade 4
Some part of the foot gangrenous
Most part salvagable
Treatment:Similar to that for grade 3 + Local amputation
Grade 5
Extensive gangrene
Limb not salvagable
Treatment:Major amputation
University of Texas Diabetic Wound Classification Stages Stage A: No infection or ischemia Stage B: Infection present Stage C: Ischemia present Stage D: Infection and ischemia present Grading Grade 0: Epithelialized wound Grade 1: Superficial wound Grade 2: Wound penetrates to tendon or capsule Grade 3: Wound penetrates to bone or joint
Depth ClassificationDefinition Treatment 0At-risk foot, no ulceration Patient education, accommodative footwear, regular clinical examination 1Superficial ulceration, not infected Offloading with total contact cast (TCC), walking brace, or special footwear 2Deep ulceration exposing tendons or joints Surgical debridement, wound care, offloading, culture-specific antibiotics 3Extensive ulceration or abscess Debridement or partial amputation, offloading, culture-specific antibiotics
Ischemia ClassificationDefinition Treatment ANot ischemicBIschemia without gangrene Noninvasive vascular testing, vascular consultation if symptomatic CPartial (forefoot) gangrene Vascular consultation DComplete foot gangrene Major extremity amputation, vascular consultation
International Working Group on Diabetic Foot Classification SystemOn the basis of the scientific literature and expert opinion, five categories were identified,which were considered the most relevant items for research projects in diabetic foot ulcers:PerfusionExtent/sizeDepth/ tissue lossInfectionSensation
PEDIS Classification System
History takingAgeMode of onsetBare foot walkingParaesthesiaClaudication painFeverH/o DM Duration, controlled/uncontrolledTreatment historyH/o impotency
Diabetics present to the surgeon in a number of scenarios:with any foot and ankle problem and diabetes as an incidental part of the past medical history - important to assess how much diabetes increases the risk of any proposed surgical or non-surgical treatmentwith an acutely inflamed where the main differential diagnosis is between infection and Charcot arthropathywith an ulcer which may or may not be complicated by deep infection or ischemiawith a deformity which has led to recurrent ulceration, or is felt to be a risk factor for ulceration - important to assess the relative risks of corrective surgery and continuing protective care
Whatever the initial presentation, it is important to ask aboutwhat type of diabetes does the patient have (type 1 or type 2)how is it managed - diet, oral hypoglycaemics, insulin - and what agents and regimewho normally looks after the patient's diabetes - GP/practice nurse/hospital diabetic clinic and therefore who is likely to have the patient's diabetic recordshow well controlled is the diabetes - review the patient's glucose monitoring record and ask when the last HbA1c test was done and what was the result and the previous trenddoes the patient have any of the major complications of diabetescardiovascular diseaserenal diseaseeye diseasehas the patient had an ulcer or Charcot arthropathy before - the single biggest risk factor for either of these conditions is to have had them before
Clinical ExaminationNourishment, pallor
A) Limb affected B) Type of lesion:UlcerGangreneCellulitis / abscess
Ulcer: Malperforant ulcer
SiteSize, shape, marginFloor: Slough Edge: Punched outSurrounding skinBase: May be boneInfected foul smellLocal anesthesia of skin
Gangrene:
Usually wetForefoot LegEdemaFoul smellSkip lesionNo line of demarcationBone may be exposed
Cellulitis / abscess:
Diffuse tenderSwelling
Regional examination:
Deformity of footHigh archingLocal anaesthesiaRegional pulsations: Posterior tibial & Dorsalis pedisLymphadenopathyLocal thrombophlebitisLocal fracture
Nylon monofilament test
For identifying loss of protective sensation
Failure to feel the filament at four of 10 sites is 97 percent sensitive and 83 percent specific
Procedure of NMT10 gram Semmes-Weinstein nylon monofilamentThe patient must not watchTest the monofilament on the patients hand so that he/she knows what to anticipate.Apply the monofilament perpendicular to the Apply sufficient force to cause the filament to bend or buckle, using a smooth, not a jabbing motion.Apply the filament along the perimeter and NOT ON an ulcer site, callus, scar or necrotic tissue
Apply a vibrating 128 Hz tuning fork to the bony prominence of the big toe
If the patient cannot feel the vibration, gradually move the fork upwards
The sensitivity of this test for demonstrating a deficit is ~53%
A biothesiometer is a portable device that measures the vibration perception threshold. A vibration threshold of more than 25V has a sensitivity of 83%. Tuning fork testEither an abnormal 10g monofilament test or a vibration threshold of more than 25V predicts foot ulceration with a sensitivity of 100% , hence the rationale for combining these two tests in clinical practice. Tuning Fork (vibration)
BiothesiometerTo measure simply and accurately the threshold of appreciation of vibration in human subjects.
An "electrical tuning fork" whose amplitude may be set to any predetermined level or whose amplitude may be gradually increased until the threshold of vibratory sensation is reached.
Conversely, the amplitude may be lowered until the vibration is no longer discernible.
To detect neurological changes that are not disclosed with a tuning fork.
Thermal Exam Taking temperature readings on both the plantar and dorsal surfaces of the foot may be a good indicator of foot condition. A wide difference of temperatures between left and right feet can indicate possible infection, injury or circulatory problems. Done with gloves and the patient sitting comfortably, shoes and socks off. a. Dorsal Temp: Take a reading on the dorsum of the foot near the dorsalis pedis artery. Plantar Temp: Take a reading on the plantar aspect of the foot in the medial arch area. Skin & Nail Exam: Done with gloves and the patient sitting comfortably, shoes and socks off. a. Corns & Calluses: Metatarsal heads, Dorsal aspect of 5th toe, Lateral aspect of 1st toe, Heel, Plantar surface b. Skin appearance: Shiny, thin, fragilec. Hair: Normal hair growth / no hair growth d. Skin Features: Bruises, Cracks/breaks in skin, Soggy skin, Dry skin, Blisters, Discoloration, Ulcerations, Previous surgeries, Tinea Pedis (Fungus) e. Nails: Ingrown, Improperly cut, Sharp, Long, Absent
Footwear assessment
Examine the inside of the shoes Look at the type of footwearLook at the fit of the footwearAre there any areas of increased pressure?Are there any accommodations made for any deformities if already present? Is the footwear appropriate in size & shape for the patients feet?Would the patient benefit from corrective footwear? From inserts?
Evaluation of Diabetic footUrine sugar, acetoneFBS, PPBSLocal Radiology deformity, osteomyelitis, #, infectionDoppler & DuplexTranscutaneous oximetryMapping of pressure areas by foot printsC&SMRI, MRAAngiography
Transcutaneous oximetry
Application of heat to skin Localised hyperemia If O2 present in excess of skin requirement (depends on oxygen delivery & blood flow) O2 diffuses across skin Measured by electode
TcPO2 - 40 70 mm Hg (normal)
TcPO2