Dental News June 2013
86
-
Upload
dental-news -
Category
Documents
-
view
227 -
download
6
description
Dental News June 2013 issue
Transcript of Dental News June 2013


KaVo ESTETICA® E30
KaVo Dental GmbH · D-88400 Biberach/Riß · Telefon +49 7351 56-0 · Fax +49 7351 56-1488 · www.kavo.com
You will love it.
KaVo ESTETICA® E30 – everything your heart desires, within your reach.
KaVo ESTETICA E30 - looks good, feels excellent.The KaVo ESTETICA E30 opens a new dimension of Dental Excellence: the essence of high KaVo quality, reliability and efficiency at affordable entry level pricing.
Easy and intuitive to use, safe and economical to operate. This treatment unit combines convenience and efficiency as part of your daily workload.
Clever technology and a love for detail.Each detail of the KaVo ESTETICA E30 is aimed at efficiency, flexi bility and ease of use. The perfectly matched components ensure cost- efficient operation with high reliability. The integrated service functions lead to low costs and operational safety.
The KaVo ESTETICA E30 opens a new dimension of Dental Excellence: the essence of high
Easy and intuitive to use, safe and economical to operate. This treatment unit combines
www.kavo.com/e30
More information:



www.ivoclarvivadent.comIvoclar Vivadent AGBendererstr. 2 | FL-9494 Schaan | Liechtenstein | Tel.: +423 / 235 35 35 | Fax: +423 / 235 33 60
Significantly improvedadhesion to enamel
Now featuring afill-level indicator
Economical – around120 applications per VivaPen
AdheSE® One FClick & Bond® with the VivaPen®
Fluoride-releasing, self-etching all-in-one adhesive


3
ADVERTISING INDEX
ARTICLES CONGRESSES54.
70.
68.
Maintaining Missing Central Space Using Tad
Eruption Of Oral Lichen Planus After Interferon Therapy For Hepatitis C Infection: Case Report
Steam As The Preferred Tabletop Sterilizing Agent, And The Raging Controversy Between The “B” And “S” Approaches
Vita Enamic The First Hybrid Dental Ceramic In The World With A Dual-Network Structure
The Importance Of The Contact Point In Class II Restorations
Dr. Faraj A. Sedeqi
Scican
VITA
Dr. Marco Calabrese
Al Bustan Hotel, Muscat February 27-28, 2013
Radisson Blu Hotel, KuwaitApril 13-15, 2013
Koelnmesse, Cologne, Germany March 12-16, 2013
Oman International Dental Congress
Kuwait Dental Association Conference
35th International Dental Show
ACE Surgical 15ACTEON 23 A-DEC 79AL TURKI 40BA Intl 19BIEN AIR 39 BISCO 62CARESTREAM 55 CAVEX 29COLTENE 27E4D 17DENTSPLY 47DISCUS PHILIPS 67 DURR 57EMOFORM 5GC 52 GSK C3, 31, 51, 61 GENDEX 6HENRY SCHEIN 63HU FRIEDY 37IVOCLAR 1, C4JDENTAL CARE 21
KAVO C2KERR 72LISTERINE 77MEDESY 34MICRO MEGA 53 MORITA 41NSK C1 ORTHO ORGANIZERS 80PLANMECA 45 RITTER 13SCI CAN 43SIRONA 25SULTAN 59 SOREDEX 9THOMMEN 10 TEBODONT 4ULTRADENT 35VITA 49VOCO 7W&H 8ZHERMACK 2
30.
36.
12.
20.
42.
48.
Dental News, Volume XX, Number II, 2013
Dr. Wafa Ali Al-Shamali,Dr. Mohamed Ahmed,Dr. Rasha Matter, Dr. Saqer Abdulrahman
Using Microabrasion And In-Offi ce Bleaching To Treat Fluorosis In Permanent Anterior TeethDr. Mayada Jemâa, Pr. Sonia Zouiten, Pr. Neila Zokkar, Ms. Belkhir, Pr. Abdellatif Boughzala
74.April 24-26, 2013
Quintessence Dental Arab CongressAl Faisaliah, Riyadh, KSA

a herbal alternative in gum problems no discoloration of the teeth no change of the sense of taste
Melaleuca alternifolia (tea tree oil)
antimicrobial fungicidal antiviral antiseptic
Swiss made
Dr. Wild’s Mideast Regional Office:Actco, P.O. Box 40746, Larnaca 6306, Cyprus, Tel.: (24) 623515 / 654252, Fax: (24) 623844. E-Mail: [email protected]
Dr. Wild & Co. AG, CH-4132 Muttenz/Switzerland www.wild-pharma.com
Swiss professional oral care

Special toothpaste and mouthbath with Ems salts for sensitive teeth and denuded toothnecks, irritations ofthe gums, plaque
desensitizes teeth and denuded toothnecks
firms up the gums and combats dental plaque
neutralizes acids harmful to the teeth
Special toothpaste and mouthbathfor sensitive teeth and denuded toothnecks, caries prophylaxis andgum care
desensitizes teeth and denuded toothnecks
caries prophylaxis
stimulates salivation
Alcoholfree
Alcoholfree
Swiss made
Swiss made
Bahrain: Awal Pharmacy, East Riffa, Bahrain. Egypt: Sesic, Alexandria. Jordan: Areel for Cosmetics Trading, Amman. Kuwait: Al-Maseela Pharmaceutical Co., Safat. Lebanon:A.M.G. Medical.Jdeideh-Azur Center. Libya: Al Osra, Benghazi. Oman: Ibn Sina Pharmacy L.L.C., Muscat. Qatar: Ahmed Khalil Al Baker & Sons, Doha. Saudi Arabia: Depot Phar-maceutique du Moyen Orient, Jeddah. Sudan: Pharma Care Co, Khartoum. United Arab Emirates: Al Hayat Pharmaceuticals, Sharjah. Yemen: Al Rawdha Trading Group, Sana’a.
Dr. Wild & Co. AG www.wild-pharma.com Swiss professional oral care


.πjóÑdG äRƒÑªμdG
:á«Ø∏ÿG ¿Éæ°SCÓd Ö∏°üàdG »Fƒ°V äRƒÑªμdG IÒÑμdG º¨∏eC’G äGƒ°û◊ πãeC’G πjóÑdG
øeõHh º∏e 4 ácɪ°S äGP äÉ≤Ñ£H ≥«Ñ£àdG á«fÉμeEG :º«eÎdG RÉ‚EG áYô°S¿GƒK 10 Ö«∏°üJ
π°†ØH á«©«Ñ£dG ¿Éæ°SC’G ™e RÉટG ʃ∏dG ≥HÉ£àdG øeDƒj :πeÉ°ûdG ¿ƒ∏dGAÉHô◊G á«°UÉN
πμ°ûdÉH kÉ«dÉM ôaƒàe…OÉ°üàb’G …QÉéàdG



The perfect harmony of Swiss precision, innovation and functional design.
SWISS PRECISION AND INNOVATION.www.thommenmedical.com
Tune in to Swiss precision and innovation with
Thommen! Based on more than 25 years of clinical
experience, in-house research and development
as well as high-quality Swiss manufacturing, you will
fi nd that the Thommen Implant System excels
through its proverbial simplicity!
E Exclusive distributor in the Middle East:
Star Science International GmbH
Jupiterstrasse 57
3015 Bern | Switzerland
Tel. +41 31 941 07 31

International Calendar 11
The AAED 38th Annual meeting
FDI Annual World Dental Congress
10th Annual Meeting of ESCD
16th International Dental Congress of the Egyptian Dental Association
The Lebanese Orthodontic Society
AEEDC
GNYDM 2013
International Congress Digital Dentistry ICDD
3rd Pan Arab Endodontic Conference
DFCIC 2013
BIDM 2013
National Guard Health Affairs
August 7 – 10, 2013at the Ritz-Carlton, Washington DC, [email protected]
August 28 – 30, 2013Istanbul, TurkeyEmail:[email protected] Website: www.fdi2013istanbul.org
October 3 – 5, 2013 at Cinema Lux Turin/ItalyEmail: www.escdonline.eu
November 5 – 8, 2013at InterContinental Citystars Hotel, Cairo, EgyptWebsite: www.eda-egypt.org
September 26 – 28, 2013Campus President RAFIC HARIRI, Hadath, Lebanon Email: [email protected]: www.bidm-lda.com
September 29 – October 1, 2013at the King Saud University, College of Medicine, RiyadhWebsite: [email protected]
November 28 – 30, 2013at the Hilton Habtoor, Beirut, Lebanon Email: [email protected] Website: www.paec2013.org
February 4 – 6, 2014at Dubai International Convention & Exhibition Centre (DICEC), UAE Website: www.aeedc.com
November 29 – December 4, 2013New York, NY, USAEmail: [email protected] Website: www.gnydm.com
September 6 – 7, 2013at K3, Josef-Herold-Strasse 12, A-6370 Kitzbühel, Austriawww.icdd-2013.com
October 8 – 9, 2013at Jumeirah Beach Hotel, Dubai, UAE Website: www.cappmea.com
October 31 – November 3, 2013at Movenpick Resort©Raouch Beirut, Lebanon Email: [email protected] Website: www.leborthosoc.com
DENTAL NEWS – Sami Solh Ave., G. Younis Bldg.POB: 116-5515 Beirut, Lebanon.Tel: 961-3-30 30 48Fax: 961-1-38 46 57Email: [email protected]: www.dentalnews.comwww.facebook.com/dentalnews1
www.facebook.com/dentalnews1
twitter.com/dentalnews
Dental News App on both Appstore & Google play
DENTAL NEWS IS A QUARTERLY MAGAZINE DISTRIBUTED MAINLY IN THE MIDDLE EAST & NORTH AFRICA IN COLLABORATION WITH THE COUNCIL OF DENTAL SOCIETIES FOR THE GCC.Statements and opinions expressed in the articles and communications herein are those of the author(s) and not necessarily those of the Editor(s) or publisher. No part of this magazine may be reproduced in any form, either electronic or mechanical, without the express written permission of the publisher.
Alfred Naaman, Nada Naaman,Jihad Fakhoury, Dona Raad, Antoine Saadé, Lina Chamseddine, Tarek Kotob, Mohammed Rifai, Bilal Koleilat, Mohammad H. Al-JammazSuha NaderIbrahim MantoufehMicheline Assaf, Nariman NehmehJosiane YounesAlbert SaykaliGisèle Wakim, Marielle KhouryTony Dib1026-261X
EDITORIAL TEAM
COORDINATORART DEPARTMENT
SUBSCRIPTIONADVERTISING
PHOTOGRAPHYTRANSLATION
DIRECTORISSN
Volume XX, Number II, 2013
w w w . d e n t a l n e w s . c o m

Dental News, Volume XX, Number II, 2013
12
CASE REPORT
Oral Pathology
ERUPTION OF ORAL LICHEN PLANUS AFTER INTERFERON THERAPY FOR HEPATITIS C INFECTION: CASE REPORT
AbstractBackground: The association between oral lichen planus (LP) and hepatitis C virus infection (HCV) has been discussed in several papers worldwide. The exact pathogenesis of oral LP in HCV-positive patients is still uncertain. There are several studies, which highlight the role of alpha-interferon (INF) being used for treatment of HCV- positive patients, resulting in eruption or exacerbation of oral LP. Case description: We present a case of erosive LP limited to oral cavity in a 44-year-old Egyptian man with chronic HCV infection who was treated with INF and ribavirin. Despite an extended period of treatment, there was no significant effect on the viral activity (viral load). Interestingly, following five months of termination of anti-hepatitis therapy, there was recurrence of oral LP lesions which was confirmed histopathologically. His condition improved dramatically by Protopic cream 0.1%. Conclusion: Altered immunogenicity of HCV appears to be the likely explanation, hence understanding the importance of follow-up of the patient post anti-hepatitis C therapy.
IntroductionOral lichen planus (LP) is a relatively common chronic inflammatory condition that affects the oral mucous membrane with variable clinical traits. Since the first description of oral LP associated with hepatitis C infection was reported in 1991,1
there have been several reports suggesting the association between HCV infection and oral LP.2
Many studies have showed higher prevalence (1.6-20%) of oral LP in HCV-positive patients (2-7). In contrast, some researchers found weak or no correlation between chronic HCV infection and LP. 8-11
A region-based correlation between HCV infection and LP has been described by some
Dr. Wafa Ali Al-Shamali
Dr. Mohamed Ahmed
El-Khalawany
Dr. Saqer Abdulrahman
Al-Surayei
Dr. Rasha Matter
Al-Shemmari
researchers worldwide.12 However, the possible etiopathogenic mechanism that links the two diseases remains unclear. Immunogenic dysregulation of host infected with HCV, reaction to anti-hepatitis medications particularly alpha-interferon or viral infection are considered to be the current acceptable etiopathogenic factors causing oral LP. 12-13
The clinical and histological features of oral LP associated with hepatitis C infection subjects are no different from the control patients. Although, erosive form of oral LP is common clinical phenotype noted in seropositive hepatitis C individuals, the management of oral LP in patients with or without hepatitis remains the same.
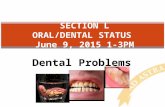
Case reportA 44-year-old Egyptian male was referred from dermatology department at Farwaniya hospital to oral medicine clinic, who presented with painful and swollen ulcerated lower lip on March 2010. On examination, there was apparent swollen lower lip with central erosive areas oozing fresh blood from the eroded surfaces on light palpation, and there were white fine and coarse lace-like mucosal changes abutting the eroded lesions (fig 1). Also, there was bilateral lymphadenopathy with mobile, tender lymph nodes palpable in the submandibular triangular region. Intra-oral examination revealed
fi g 1
A swollen lower lip with central erosive and hemorrhagic areas.

Rene Zakhem, Representative Middle East / AfricaRitter®Concept GmbH · Bahnhofstraße 65 08297 Zwoenitz / GermanyGER +49 15 258 967 247LB +961 3 593 187KSA +966 582 646 [email protected], www.ritterimplants.com
Please contact directly:
Best German Implant System.
TEST IT!
Ritter Implants Ivory Line - the German Implant System:Two-Piece Implants QSI/TFI and One-Piece Implants MCI with full range of all prosthetic components and abutments.Clever, easy and beneficial !

Dental News, Volume XX, Number II, 2013
14
LICHEN PLANUS
Oral Pathology
bilateral white and red lesions on posterior part of the buccal mucosa. These lesions had striking reticular pattern (reminiscent of LP) centered on erythematous mucosal areas. The lesion on right buccal mucosa was found rubbing against heavily restored molar tooth with amalgam (figs 2 and 3). No other lesions were seen on the rest of oral cavity mucosa. The clinical presentation of the lip
fi g 2
fi g 3
A
B
and oral cavity lesions were consistent with LP. On reviewing his medical history, he had been diagnosed with hepatitis due to HCV infection (genotype 4) in 2008 for which he received combined therapy of pegylated interferon-alpha (180 mcg SC, weekly for 48 weeks) and ribavirin (1000 mg PO daily for 48 weeks). The patient reported an oral soreness and burning sensation after one month of the anti-hepatitis therapy inception for the first time. The exact diagnosis of oral lesion and subsequent therapy provided by dermatology department had not been known to us. Nevertheless, oral condition was quiescent through the period of the therapy. The oral symptoms reappeared five months following discontinuation of anti-hepatitis therapy with increased severity resulting in severe pain, difficulty in eating, swallowing and speaking. In addition, he noticed progressive swelling of the lower lip with bleeding ulcers over the next 6 weeks. Besides his known medical condition, he is on insulin to manage his diabetes (type II).
Furthermore, he is not a cigarette smoker and he does not drink alcohol. An incision biopsy of lower lip lesion revealed interface dermatitis confirming our clinical provisional diagnosis. Microscopically, the specimen exhibited ortho-keratosis with prominent granular layer, intense band-like lymphohistiocytic infiltrate with plasma cell predominance and hydropic degeneration of basal cell layer with scattered Civatte bodies.
(Figs 4-6). The patient was treated with protopic cream 0.1% three-four times daily for 2 weeks. The lower lip status improved dramatically.
fi g 4
fi g 5
fi g 6
fi g 7
Fig 2, 3: Exhibit lichenoid changes “reticular pattern” on right (A) and left (B) buccal mucosae.
Dramatic improvement of lower lip lesion after two weeks of topical tacrolimus use.
Prominent Civatte body (*).
Reveals hydropic degeneration with intense lympho-histoicytic infi ltrates. (Hematoxylin and eosin stain at higher magnifi cation 20X)
Exhibit lichenoid changes “reticular pattern” on right (A) and left (B) buccal mucosae.

For over 45 years, ACE Surgical Supply has been committed to providing our customers with the best possible products available at unbeatable prices. We are the only multi-disciplinary surgical supply company. ACE continues to develop and
manufacture the highest quality, state-of-the-art products, while keeping a focus on customer service. Our highly qualified team is always available to answer any questions you may have about our extensive product line.

Dental News, Volume XX, Number II, 2013
16
LICHEN PLANUS
Oral Pathology
DiscussionAmong viruses, human herpes viruses, human papilloma virus and hepatitis viruses have been linked with oral LP, albeit on the basis of equivocal data.12 There have been several studies, which suggest an association between LP and HCV infection.3,7 In a recent review the pooled data from all studies revealed a statically significant difference in the population of HCV seropositive subjects among LP patients when compared with the controls. Interestingly, geographic heterogeneity seems to play an important role in this LP-HCV association. As indicated by studies from the Mediterranean basin showing a significant association whereas studies from Northern Europe did not present any such association. Furthermore, in studies from countries with high prevalence such as Egypt, negative or insignificant association between HCV infection and oral LP has been reported12,14 The discrepancy may be explained by genetic differences among the population studies and this may possibly be the reason for development of LP in our patient. The exact etiopathogenesis of oral LP in HCV-positive individual is still uncertain. Nonetheless, eruption of oral LP in our case could have resulted from a lichenoid reaction to the medication used in the treatment of hepatitis C, particularly alpha-interferon. This hypothesis (i.e. drug reaction) was plausible in some studies.15,20 Most of these case reports demonstrate the aggravating effect of the interferon rather than causative effect for the development of oral LP in patient with HCV infection. Besides, in our case, reappearance of severe erosive oral LP while not receiving INF therapy, suggests that it may not have played a significant role in its pathogenesis. Nonetheless, this may be viewed as it having more aggravating rather than causal effect. Therefore, it would be a good practice to screen the oral cavity of HCV-positive patients prior to initiating antiviral therapy. So, the possible eruption of oral LP can be anticipated and managed appropriately especially in those with quiescent LP. Besides INF therapy, other confounding factors appeared to have contributed to the possible initiation or aggravating already present of oral LP in our case, such as presence of amalgam on left mandibular molar and chronic rubbing of buccal mucosa. Unfortunately, we are not aware of the intra-oral examination findings of the patient prior to
anti-hepatitis treatment. Also, there is plethora of literature suggesting role of immune dysregulation in the pathogenesis of oral LP involving the cell-mediated immunity. However, viral factors, such as genotypes of HCV and HCV-RNA levels, are less important pathogenic cause.12 Why oral mucosa is most frequently affected is still unknown. Several experimental studies conducted proposing a theory of “compartmentalization of mucosa” that still does not give a clear explanation to this phenomenon.21,22 In HCV seropositive subjects, erosive oral LP is commonly prevalent lesion.23,24
Mega et al. 25 noted three types of OLP. He found lymphocytic inflammation deeply infiltrating lamina propria in OLP associated with a HCV infection and that could be associated with the erosive trait, as noted in our case. Management of HCV associated oral LP lesion is no different from oral LP in HCV-negative subjects. Since there is no cure different therapies are aimed primarily to ameliorate the signs and symptoms of oral LP. Although corticosteroids have been the mainstay of management, other immunosuppressant and immunomodulatory agents have also contributed significantly towards treatment of the disease.12,26,27,28 A comparative systemic review of 28 randomised controlled clinical trials of therapy for symptomatic oral LP has concluded that there is insufficient evidence to support the effectiveness of any specific treatment as being superior.26, 29 A plausible therapeutic approach should be guided by severity of the patient’s condition. In our case, tacrolimus cream (0.1%) was prescribed and used three to four times daily for 2 weeks. Some studies recommend use of tacrolimus as second line of treatment especially in reluctant lesion. We preferred to use it due to severity of the lesion, which is found to be effective in other studies. 12,26 In order to prevent a flare up of the condition, we avoided use of systemic immunosuppressant therapy. Many researchers have emphasised on maintenance of good oral hygiene, relief of mechanical trauma by dental procedure or dentition itself, and discrete use of dental allergen materials (e.g. amalgam) for preventing development or irritating already existing oral LP . Up to the time of writing this case report, his oral condition is fairly controlled with topical steroids in addition to tacrolimus. Due to chronicity of LP, relapses of his oral condition did

NOTHING FITS YOUR PRACTICE BETTER.
For Quality, It’s The Perfect FitE4D Dentist —
With its advanced scanning, design and milling capability, the E4D creates a high quality, exceptionally well-fitting restoration.
Visit E4D.com/perfectfit to learn how E4D is the perfect fit for your practice.
For quality and accuracy, the E4D chairside CAD CAM system stands alone. Independent studies and clinicians confirm the accurate fit and clinical efficacy of the E4D restoration. What’s more, the E4D gives you the flexibility to practice on your own terms and your own schedule. And our hands-on training and support assures you of flawless integration. Which means it perfectly fits your success.
Stay Connected with E4D
SCAN
Powder-free ScannerE4D is the original powder-free scanner that captures the true anatomy
MILL
Precision MillIn-office restoration milling means same day dentistry – a great fit for both you and your patient
SUPPORT
Support-On-SightE4D is backed by a dedicated support team of clinical and technical experts to optimize your result
EDUCATION
At E4D University, you and your staff receive comprehensive, hands-on training to maximize your skills
DESIGN
Intuitive User InterfaceE4D’s design tools and easy-to-follow navigation guideyou through the entire process

Dental News, Volume XX, Number II, 2013
18
LICHEN PLANUS
Oral Pathology
occur but with lesser frequency and severity. The potential for malignant transformation of OLP is still controversial. The frequency ranges from 0.4% to 6.25% with the highest rates in the erythematous and erosive lesions.30,31,32 Follow up is mandatory not only to control his oral LP but also to detect early malignant transformation.
REFERENCES
1. MOKNI M, RYBOJAD M, PUPPIN D. LICHEN PLANUS AND HEPATITIS C VIRUS. J AM
ACAD DERMATOL. 1991; 24 (5 PT 1): 792.2. NITA CHAINANI-WU, FRANCINA LOZADA-NUR, NORAH TERRAULT. HEPATITIS C VIRUS
AND LICHEN PLANUS: A REVIEW. ORAL SURG ORAL MED ORAL PATHOL ORAL RADIOL
ENDOD. 2004; 98 (2):171-183.3. LC FIGUEIREDO, F CARRILHO, HF DE ANDRADE, DA MIGLIAN. ORAL DISEASES.2002 JAN; 8 (1): 42- 6.4. GHADERI R, MAKHMALBAF Z. SHIRAZ E-MEDICAL JOURNAL. 2007; 8(2): 72-9.5. SANCHEZ-PEREZ J, DE CASTRO M, BUEZO GF, FERNANDEZ-HERRERA J, BORQUE
MJ, GARCIA-DIEZ A. LICHEN PLANUS AND HEPATITIS C VIRUS: PREVALENCE AND CLINICAL
PRESENTATION OF PATIENTS WITH LICHEN PLANUS AND HEPATITIS C VIRUS INFECTION. BR J DERMATOL. 1996 APR; 134(4):715-9.6. THAIS DIAS TAVARES GUERREIRO, MARILIA MOURA MACHADO, THAIS HELENA PRO-ENCA DE FREITES. ASSOCIATION BETWEEN LICHEN PLANUS AND HEPATITIS C VIRUS INFEC-TION: A PROSPECTIVE STUDY WITH 66 PATIENTS OF THE DERMATOLOGY DEPARTMENT OF THE
HOSPITAL SANTA CASA DE MISERICORDIA DE SAO PAULO. AN BRAS DERMATOL. 2005; 80(5):475-80.7. NIMA MAHBOOBI, FARZANEH AGA-HOSSEINI, KAMRAN BAGHERI LANKARANI.HEPATITIS C VIRUS AND LICHEN PLANUS: THE REAL ASSOCIATION. HEPAT MON. 2010; 10(3):161-4.8. SIMON C, TUCKER AND IAN H. COULSON. LICHEN PLANUS IS NOT ASSOCIATED WITH
HEPATITIS C VIRUS INFECTION IN PATIENTS FROM NORTH WEST ENGLAND. ACTA DERM
VENEREOL. 1999; 79:378-9.9. KARIN SOARES GONCALVES CUNHA, ANGELA CORREA MANSO, ABEL SILVEIRA CAR-DOSO, JACQUELINE BITTENCOURT ALTHOFF PAIXAO, HENRIQUE SERGIO M. COELHO, SAN-DRA REGINA TORRES, AND RIO DE JANEIRO. ORAL SURG ORAL MED ORAL PATHOL ORAL
RADIOL ENDOD. 2005; 100:330-3.10. YU ZHOU, LU JIANG, JIE LIU, XIN ZENG, QIAN-MING CHEN. THE PREVALENCE OF
HEPATITIS C VIRUS INFECTION IN ORAL LICHEN PLANUS IN AN ETHNIC CHINESE COHORT OF
232 PATIENTS. INT J ORAL SCI. 2010; 2(2): 90-97.11. DEL OLMO JA, PASCUAL I, BAGAN V, SERRA MA, ESCUDERO A, RODRIGUEZ F, RO-DRIGO JM. PREVALENCE OF HEPATITIS C VIRUS IN PATIENTS WITH LICHEN PLANUS OF THE ORAL
CAVITY AND CHRONIC LIVER DISEASE. EUR J ORAL SCI. 2000 OCT; 108(5):378-2.12. GIOVANNI LODI, CRISPIAN SCULLY, MARCO CARROZZOO, MARK GRIFFITHS, PHILIP
B. SUGERMAN, AND KOBKAN THONGPRASOM. CURRENT CONTROVERSIES IN ORAL LICHEN
PLANUS: REPORT OF AN INTERNATIONAL CONSENSUS MEETING. PART1. VIRAL INFECTIONS
AND ETIOPATHOGENESIS. ORAL SURG ORAL MED ORAL PATHOL ORAL RADIOL ENDOD.2005; 100:40-51.13. A. A. AL ROBAEE AND A. A. AL ZOLIBANI, ET AL. ORAL LICHEN PLANUS AND
HEPATITIS C VIRUS: IS THERE REAL ASSOCIATION? ACTA DERMATOVEN APA. 2005; 15(NO1):14-9.14. G. LODI, M. GIULIANI, A. MAJORANA, A. SARDELLA, C. BEZ, F. DEMAROSI, A. CARRASSI, ET AL. LICHEN PLANUS AND HEPATITIS C VIRUS: A MULTICENTRE STUDY OF PA-TIENTS WITH ORAL LESIONS AND A SYSTEMATIC REVIEW. BRITISH JOURNAL OF DREMATOLOGY.2004 DEC; 151 (6): 1172-81.15. NAGAO Y, SATA M, IDE T, SUZUKI H, TANIKAWA K, ITOH K, KAMEYAMA T. DEVELOPMENT AND EXACERBATION OF ORAL LICHEN PLANUS DURING AND AFTER INTERFERON
THERAPY FOR HEPATITIS C. EUR J CLIN INVEST. 1996 DEC; 26 (12): 1171-4.16. NAGAO Y, KAWAGUCHI T, IDE T, KUMASHIRO R, SATA M. EXACERBATION OF ORAL
EROSIVE LICHEN PLANUS BY COMBINATION OF INTERFERON AND RIBAVIRIN THERAPY FOR
CHRONIC HEPATITIS C. INT J MOL MED. 2005 FEB; 15(2):237-41.17. GROSSMANN SDE M, TEIXEIRA R, DE AGUIAR MC, DO CARMO MA. EXACERBATION
OF LICHEN PLANUS LESIONS DURING TREATMENT OF CHRONIC HEPATITIS C WITH PEGYLATED
INTERFERON AND RIBAVIRIN. EUR J GASTROENTEROL HEPATOL. 2008 JUL; 20(7):702-6.18. BARRECA T, CORSINI G, FRANCESCHINI R, GAMBINI C, GARIBALDI A, ROLANDI E. LICHEN PLANUS INDUCED BY INTERFERON-ALPHA-2A THERAPY FOR CHRONIC ACTIVE HEPATITIS
C. EUR J GASTROENTEROL HEPATOL. 1995 APR; 7(4): 367-8.19. PROTZER U, OCHSENDORF FR, LEOPOLDER-OCHSENDORFA, HOLTERMULLER KH. EX-ACERBATION OF LICHEN PLANUS DURING INTERFERON ALFA-2A THERAPY FOR CHRONIC ACTIVE
HEPATITIS C. GASTROENTEROLOGY. 1993 MAR; 104(3): 903-5. 20. AREIAS J, VELHO GC, CERQUEIRA R, BARBEDO C, AMARAL B, SANCHES M,
MASSA A, SARAIVA AM. LICHEN PLANUS AND CHRONIC HEPATITIS C: EXACERBATION
OF THE LICHEN PLANUS UNDER INTERFERON-ALPHA-2A THERAPY. EUR J GASTROENTEROL
HEPATOL. 1996 AUG; 8(8); 825-8.21. CARROZZO M, QUADRI R, LATORRE P, PENTENERO M, PAGANIN S, BERTOLSSO G. MOLECULAR EVIDENCE THAT THE HEPATITIS C VIRUS REPLICATES IN THE ORAL MUCOSA. J HEPATOL. 2002;37: 364-9.22. PILLI M, PENNA A, ZERBINI A, VESCOVI P, MANFREDI M, NEGRO F. ORAL LICHEN
PLANUS PATHOGENESIS: A ROLE FOR THE HCV-SPECIFIC CELLULAR IMMUNE RESPONSE. HEPA-TOLOGY. 2002; 36:1446-52.23. CARROZZO M, GRANDOLFO S, CARBONE N, COLOMBATTO P, BROCCOLETTI R, GARZINO-DEMO P, GHISETTI V. J ORAL PATHOL MED. 1996 NOV; 25(10):527-33.24. MICHELE D, MIGNOGNA MD, LUCIO LO RUSSO, ET AL. ORAL LICHEN PLANUS:DIFFERENT CLINICAL FEATURES IN HCV-POSITIVE AND HCV-NEGATIVE PATIENTS. INT J DER-MATOL. 2000 FEB. 39(2):134-9.25. MEGA H, JIANG W, TAKAGI M. IMMUNOHISTOCHEMICAL STUDY OF ORAL LICHEN
PLANUS ASSOCIATED WITH HEPATITIS C VIRUS INFECTION, ORAL LICHENOID CONTACT SEN-SITIVITY REACTION AND IDIOPATHIC ORAL LICHEN PLANUS. ORAL DISEASES. 2006;7(5): 296-305.26. THONGPRASOM K, CARROZZO M, FURNESSS, LODI G. INTERVENSION FOR TREATING
ORAL LICHEN PLANUS. COCHRANE DATABASE OF SYSTEMIC REVIEWS 2011, ISSUE 7.27. N LAVANYA, P JAYANTHI, UMADEVI K RAO, K RANGANATHAN. ORAL LICHEN
PLANUS: AN UPDATE ON PATHOGENESIS AND TREATMENT. J ORAL MAXILLOFAC PATHOL.2011; 15: 127-132.28. MAHNAZ SAHEBJAMEE, FATEMEH ARBABI-KALATI. MANAGEMENT OF ORAL LICHEN
PLANUS. ARCHIVES OF IRANIAN MEDICINE. 2005; 8(4): 52-6.29. ANALIA VEITZ KEENAN AND DEBRA FERRAIOLO. INSUFFICIENT EVIDENCE FOR EFFECTIVE-NESS OF ANY TREATMENT FOR ORAL LICHEN PLANUS. EVIDENCE-BASED DENTISTRY. 2011; 12: 85-86.30. GIOVANNI LODI, CRISPIAN SCULLY, MARCO CARROZZOO, MARK GRIFFITHS, PHILIP
B. SUGERMAN, AND KOBKAN THONGPRASOM. CURRENT CONTROVERSIES IN ORAL LICHEN
PLANUS: REPORT OF AN INTERNATIONAL CONSENSUS MEETING. PART1. VIRAL INFECTIONS
AND ETIOPATHOGENESIS. ORAL SURG ORAL MED ORAL PATHOL ORAL RADIOL ENDOD.2005; 100:164-78.31. ATESSA PAKFETRAT, ABBAS JAVADZADEH-BOLOURI, SAMIRA BASIR-SHABESTARI, FAR-NAZ FALAKI. ORAL LICHEN PLANUS: A RETROSPECTIVE STUDY OF 420 IRANIAN PATIENTS.MED ORAL PATOL ORAL CIR BUCAL. 2009 JUL; 14(7):E315-8.32. MARIJA BOKOR-BRATIC, IVANA PICURIC. THE PREVALENCE OF PRECANCEROUS ORAL
LESIONS. ORAL LICHEN PLANUS. ARCHIVE OF ONCOLOGY. 2001; 9(2):107-9.
www.fdi2013istanbul.org
Bridging Continents for Global Oral Health
FDI 2013 Istanbul Annual World Dental Congress
28 to 31 August 2013 - Istanbul, Turkey


Dental News, Volume XX, Number II, 2013
20
TREATING FLUOROSIS
Aesthetic Dentistry
USING MICROABRASION AND IN-OFFICE BLEACHING TO TREAT FLUOROSIS IN PERMANENT ANTERIOR TEETH
Dr. Mayada Jemâa
Pr. Neila Zokkar
Ms. Belkhir
Pr. Abdellatif Boughzala
Pr. Sonia Zouiten
AbstractIn today’s world, there is a strong focus on perfect physical appearance. (Didier Dietsch, 2008).Different esthetic dental procedures have been developed since many patients are very dissatisfied with their appearance.3
Discolored teeth affected by fluorosis, due to the fluoridation of drinking water, are frequently seen in our population. This kind of pathology leads to the whitish, opaque, unpleasant appearance of enamel which is often visible at speaking distance. Proposed treatments, depending on fluorosis severity, range from expensive ceramic veneers to free hand bonding restorations and abrasive chemical treatments. (S.Ardu et al, 2009)Bleaching is considered before porcelain veneer placement to either eliminate the need for veneers, reduce the amount of opacifiers needed to mask discoloration, or to give the patient the option of attempting a less expensive/ invasive treatment before committing to veneers. (Van B. Haywood, 2003). The aim of this article is to describe an easy technique for managing enamel discoloration via microabrasion followed by in-office dental bleaching.
Key wordsDental fluorosis, Microabrasion, in-office bleaching
IntroductionThe intrinsic discoloration is incorporated into the structure of enamel or dentine and can’t be eliminated by simple prophylaxis using pumice or tooth paste.4 Dental fluorosis which is an intrinsic discoloration is defined as hypomineralization of enamel resulting from excessive ingestion of fluoride during tooth development. It is characterized by diffuse opacities on the enamel surface. These are differentiated from
other conditions by the characteristic bilaterally symmetric distribution of the enamel defects. (Howard E. Strassler et al. 2011). Current research suggests that superfluous amounts of fluoride cause retention of amelogenin proteins in the developing tooth structure, there by inhibiting enamel maturation. This interference results in porosities in the enamel at the time of tooth eruption. (Howard E. Strassler et al. 2011). The enamel affected by fluorosis contains higher levels of protein content than normal enamel. When normal enamel protein content ranges from 0.07 to 0.14 per cent, fluorosed enamel content ranges from 0.03 to 0.56 per cent.11 The safe level for daily fluoride intake is 0.05 to 0.07 mg F/Kg/day. Above this level, the risk of developing fluorosis due to chronic fluoride consumption will be evident.12 Dental fluorosis has been categorized under various grades as follows: (Naveen Chhabra et al. 2010). Grade 0: Normal, translucent, smooth, and glossy teeth; Grade I: White opacities, faint yellow line; Grade II: Changes as in Grade I and brown stains; Grade III: Brown line, pitting, and chipped off edges; Grade IV: Brown, black and/or loss of teeth The severity of dental fluorosis depends on when and for how long the overexposure to fluoride occurs, the individual response, weight, degree of physical activity, nutritional factors and bone growth, suggesting that similar dose of fluoride may lead to different levels of dental fluorosis. (Jenny Abanto Alvarez et al. 2009). It is very difficult to correct deeper enamel fluorosis via only Microabrasion. For this reason, a combination of different techniques such as microabrasion/in-office bleaching is recommended to mask deeper defects since they are conservative, provide highly satisfactory results, without excessive wear of sound dental tissue. 12


Dental News, Volume XX, Number II, 2013
22
Aesthetic DentistryTREATING FLUOROSIS
Examination for bleachingWe should undertake a standard extra-oral and intra-oral examination.4 The initial examination and diagnosis are very important before starting the treatment. And of course they cannot be performed without the patient consulting the dentist.8 Proper examination and diagnosis, including radiographs, are needed to rule out pathology that will require completely different treatment from bleaching. (Van B. Haywood, 2003). The differential diagnosis between fluorosis and non-fluoride-induced opacities needs to establish differences between symmetrical and asymmetrical and/or discrete patterns of opaque defects. These criteria imply that all symmetrically distributed and non-discrete opaque conditions of enamel are fluorosis. (Jenny Abanto Alvarez et al. 2009). A history of eventual tooth sensitivity should be investigated.9 No bleaching procedure should be initiated without appropriate dental examination.
MicroabrasionMicroabrasion is a procedure developed by Dr. Theodore Croll6 helping in removing superficial stains related to discrete or moderate fluorosis.1
It is composed of a mixture of hydrochloric acid and pumice that is rubbed onto the surface of the tooth repetitively until the outer layers of the enamel containing the stains are abraded away. The stains in the outer layers of enamel can be removed, leaving a smooth, glassy enamel surface.6 It is recommended to use a rubber dam so as to protect the gums from the acid.After that, the pumice-acid slurry is then applied to the teeth and rubbed with a very slow speed rubber cup. After a few layers of enamel are removed, the slurry is rinsed with water and the result is evaluated. This process is repeated until the stain is gone or the process must be stopped for other reasons such as enamel getting too thin or tooth getting sensitive.6 At the end, it is recommended to bath teeth with a fluoride gel so as to reduce eventual post-operative sensitivity.6 This technique is simple to perform and the depth of enamel removed in 10 applications is approximately 100 μm. (0.1 mm.).4
Microabrasion is a time-proven technique that is safe and effective for the atraumatic removal of superficial enamel defects. (HO Heymann, 1997).
In Office bleachingIn-office vital tooth bleaching has been used for many years in dentistry and is known to be a reliable technique for quickly lightening discolored teeth. (Ruta Zekonis et al. 2003). For this technique, we use higher concentration of hydrogen peroxide (35%) than we can use at-home bleaching and for this reason, the bleaching agent will penetrate the tooth more rapidly with in-office bleaching.14 In general, the in-office bleaching procedure for vital teeth involves several necessary and important steps: (M. S. Gutmann and J. L. Gutmann, 2001)
dam along with a petroleum jelly to protect the gingival tissues.
placement of the bleaching agent. A gel or liquid bleaching agent, usually 35% hydrogen peroxide, is then applied to the enamel surface. If the liquid form is used, gauze squares saturated with the bleaching agent are placed on the facial surfaces. Allow the bleaching agent to remain on the teeth for 20-30 minutes. Apply a heat source, usually a visible light curing lamp or a laser, to accelerate the chemical reaction
and monitor patient discomfort to avoid tissue burns or excess heat build-up in the pulp. Analgesics, such as ibuprofen, acetaminophen, or aspirin, may be recommended for the first 24 hours if any tooth sensitivity is noted.
bleaching agent should be removed with water before removing the rubber dam.Different studies reveal that, 2-6 visits with about 45 minutes application per time in-office bleaching are necessary to obtain acceptable results.14 We also should take into account the possible appearance of tooth sensitivity that is why we must wait at least one week between visits.14 The use of bleaching light may lead to the augmentation of pulpal temperature which depends on the exposure time and the light source.9 In addition to that, tooth sensitivity and pulpal irritation may be higher with the use of bleaching light or even heat application.9,15 One of the most safety advantages of the in-office dental bleaching is that it is under dentist’s control.16
The disadvantages are: the cost which can be considered as expensive for some patients, the

A company of ACTEON Group • 17 av. Gustave Eiffel • BP 30216 • 33708 MERIGNAC cedex • FRANCEE-mail : [email protected] • www.acteongroup.com
Middle East Office • PO Box 468 • Amman 11953 • JORDANTel +962 6 553 4401 • Fax +962 6 553 7833 • E-mail: [email protected]
Discover MeToo, a totally new range ofprofessional whitening products, bothcomprehensive and wide-ranging tocover all your patient’s requirements!
Visit www.metoo-teeth-whitening.comand discover the great advantages ofMeToo along with innovative tools tosupport you in your practice.
I wantto smile
Download MeToosimulation software
Read the instructions in the notice carefully – The compulsory information requested for good use of this deviceare in the Summary of Product Characteristics available on the laboratory's website - Not reimbursed by healthinsurance organisations. Class I and IIa (SGS - MeToo Light) Medical devices. Creation date: January 2013
Because everybody deserves to smile, ACTEON created MeToo!
Download our unique whiteningsimulator and show your patients howgreat they could look after a procedure.

Dental News, Volume XX, Number II, 2013
Aesthetic DentistryTREATING FLUOROSIS
2424
duration of the treatment and the unpredictable results.16 Some dangerous features may be the post-treatment sensitivity, the increasing temperature of the pulp and eventual discomfort concerning the gingival barrier.16
Case reportsCase N°1A 30-year old male patient with complaints of dissatisfaction about the discolored teeth (Figure 1) came to the department of conservative dentistry. Patient gave history of discoloration from his childhood. No other relevant medical history was reported by the patient. His oral hygiene was good.Diagnosis: Dental fluorosis (Grade III: Brown line, pitting, and chipped off edges) Treatment plan: Microabrasion followed by in-office dental bleaching.
Case N°2:A 47-year old female patient was unsatisfied with the discolored upper front teeth (Figure 5) came to the department of conservative dentistry. Patient gave history of discoloration since her
Fig1: Initial view of a patient’s teeth affected by fl uorosis
Fig 5: Labial view showing the severely discolored maxillary incisors.
Fig 6: Microabrasion procedure ( Placement of the gingival barrier + application of the micro abra-sion gel on the surface of the enamel of the upper anterior teeth for stain removal + the gel was rubbed with a slow speed rubber cup + the teeth was rinsed off and air dried Examination)
Fig 7: Intra-oral view of the maxillary incisors after two Treatments (4 visits): Microabrasion and in-offi ce tooth whitening (Hydrogen Peroxide 35%)
Fig 2: Light curing rubber dam application and Micro-abrasion with Opalustre ®
Fig 3: After 2 visits (of Mi-croabrasion procedure)
Fig 4: Final view of the clinical case after the end of the In-offi ce bleaching (with Hydrogen Peroxide 35%) in 3 visits
childhood. Good oral hygiene.Diagnosis: Dental fluorosis (Grade III: Brown line, pitting, and chipped off edges)Treatment proposed was Microabrasion followed by in-office dental bleaching.
Fig 8: Post-treatment view illustrating the improved aesthetics following tooth whitening, microabrasion and restoration with resin composite of the two central incisors.
fi g 1
fi g 2
fi g 3
fi g 4
fi g 5
fi g 6
fi g 7
fi g 8

C-64
4-76
-V0CEREC Omnicam
POWDER-FREE SCANNING INNATURAL COLOR.
SIRONA.COM
The new CEREC Omnicam combines powder-free ease of handling with natural color reproduction to provide an inspiring treatment experience for the patient. Discover the new simplicity of digital dentistry. Enjoy every day. With Sirona.

Dental News, Volume XX, Number II, 2013
TREATING FLUOROSIS
Aesthetic Dentistry
26
Fig 9: sensitivity occurred and we stopped it with the use of Flor Opal ® gel
Fig 10: After 14 months
Fig 11: Before
Fig 12: After
fi g 9
fi g 10
fi g 11
fi g 12
DiscussionDue to the recent increase in dental fluorosis, extensive research has been performed to understand the aetiology and pathogenesis of this systemic disease. (S. Ardu et al. 2009)The aetiology is well established and based on the excessive consumption of fluoride during specific critical ages.7 Browne indicated that this critical period is 15 to 24 months of age for males and 21 to 30 months of age for females.18
Bleaching may represent a conservative first approach for many cosmetic conditions. (Kevin J. Donly et al. 2002) Conservative treatment options such as microabrasion and/or tooth whitening can produce dramatic improvements in brown and yellow discoloration, providing a satisfactory interim result before more invasive procedures are considered, if necessary.(F Ng et al. 2007) The microabrasion procedure is considered as safe
and simple. It allows us to obtain excellent results when treating superficial enamel stains.19
It does not require the use of anesthesia that is why dentist can have a better relationship with patients.20 The Opalustre™ microabrasion slurry (Ultradent Products Inc, Utah, USA) is composed of 6.6% hydrochloric acid and silicon carbide microparticles.11 According to (F Ng et al. 2007), the Hydrogen peroxide (HP) is an oxidizing agent which breaks down into free radicals that will combine to create oxygen and water. And that the HP oxidizes, carboxylates and lightens chromophores, particularly within the dentine. Most current in-office whitening systems are based on HP solutions of 25 to 35 per cent.Higher peroxide concentrations also have been shown to be effective in tooth whitening; however, these are professionally supervised to a greater extent. (Kevin J. Donly et al. 2002) The higher concentrations of peroxide lead to faster rate of bleaching, but added to that a possible higher incidence of dental sensibility.8 While the higher concentrations may reach the end point sooner, they also “overshoot” the color and have a greater relapse, and a longer time for the color to become stable. (Van B. Haywood, 2003)One of the common adverses of vital bleaching is dental sensitivity because the peroxide can penetrate the enamel, dentine and even the pulp chamber.11 Other side effects such as irreversible pulpitis and pulp necrosis can occur with the uses of 35% of hydrogen peroxide.3
When the concentration of PH increase, the degree of penetration in dental structure will increase, also we can note a greater penetration in hypomineralized enamel.11 The patient in the second case reported sensitivity with the in-office whitening system containing 35% of HP that is why we opted for desensitizing gel Flor Opal ®.This may have been because of the relatively higher concentration of HP used (35%).According to (HO Heymann, 1997), we must wait a minimum of one week after bleaching procedure before placing any resin-bonded restoration on tooth structure because the strength of resin bonds to freshly bleached enamel and dentine are reduced. A study of (Christian Hannig et al. 2006) showed that bleaching procedure has an impact not only on surface micro-hardness of composites but also for deeper layers of adhesive filling materials. Bleaching


28
TREATING FLUOROSIS
Aesthetic Dentistry
versus Porcelain veneers? Dentists should make a choice for their patients between teeth whitening or veneers. If there is any regression in whitening after esthetic translucent veneers are placed, the teeth can be relightened from the lingual. (Van B. Haywood, 2003). In cases when teeth bleaching didn’t produce the expected result, the patient is confident since the most conservative options have been attempted first, and that porcelain veneers are the best option they have for an esthetic smile.8 We shouldn’t also ignore the minor cost of bleaching compared with the expensive cost of dental veneers that is why the bleaching procedure is usually the first choice for patients to retrieve better smile.8
ConclusionThis combined approach (Micro abrasion and in office bleaching) may be considered an interesting alternative to more invasive prosthetic techniques such as ceramic veneers.In addition to that, this minimal invasive technique allows acceptable aesthetic results and even a possible cost reduction for these patients.
REFERENCES 1. OPTIMIZING SMILE COMPOSITION AND ESTHETICS WITH RESIN COMPOSITES AND OTHERS
CONSERVATIVE ESTHETIC PROCEDURES DIDIER DIETSCH, DMD, PHDTHE EUROPEAN JOURNAL OF ESTHETIC DENTISTRY, VOLUME3, NUMBER1,SPRING 20082. VIABLE APPROACH TO MANAGE SUPERFICIAL ENAMEL DISCOLORATION
NAVEEN CHHABRA AND KIRAN P. SINGBAL CLIN DENT. 2010 OCT-DEC; 1(4): 284–287.3. SOME CURRENT PERSPECTIVES ON TOOTH BLEACHING AND MANAGEMENT OF TOOTH
STAINS PR. M. S. GUTMANN - PR. J. L. GUTMANN
DENTAL NEWS, VOLUME VIII, NUMBER III, 20014. TREATMENT OF INTRINSIC DISCOLORATION IN PERMANENT ANTERIOR TEETH IN CHILDREN
AND ADOLESCENTS ALYSON WRAY AND RICHARD WELBURY.INTERNATIONAL JOURNAL OF PAEDIATRIC DENTISTRYVOLUME 11, ISSUE 4, JULY 2001, PAGES: 309–3155. MANAGEMENT OF FLUOROSIS USING MACRO- AND MICROABRASION
HOWARD E. STRASSLER, DMD; AUTUMN GRIFFIN, DDS; AND MARGRIT MAGGIO,DMD DENTALCETODAY.COM
6. HTTP://WWW.DENTALARTANDSCIENCE.COM/MICROABRASION/MICROABRASION.HTM
7. A COMBINED CHEMO-MECHANICAL APPROACH FOR AESTHETIC MANAGEMENT OF SU-PERFICIAL ENAMEL DEFECTS
S. ARDU, N. BENBACHIR, M. STAVRIDAKIS,D. DIETSCHI, I. KREJCI AND A. FEILZER
BRITISH DENTAL JOURNAL VOLUME 206 NO. 4 FEB 28 2009 2058. FREQUENTLY ASKED QUESTIONS ABOUT BLEACHING
VAN B. HAYWOOD, DMD COMPENDIUM / APRIL 2003 VOL. 24, NO. 4A9. TOOTH WHITENING/BLEACHING: TREATMENT CONSIDERATIONS FOR DENTISTS AND THEIR
PATIENTS ADA COUNCIL ON SCIENTIFIC AFFAIRS SEPTEMBER 2009 (REVISED NOVEMBER
2010) 2009 AMERICAN DENTAL ASSOCIATION.10. NONRESTORATIVE TREATMENT OF DISCOLORED TEETH:REPORTS FROM AN INTERNATIONAL
SYMPOSIUM HO HEYMANN JADA 1997;128(6):710-71111. AESTHETIC MANAGEMENT OF SEVERELY FLUOROSED INCISORS IN AN ADOLESCENT FEMALE
F NG, DJ MANTON AUSTRALIAN DENTAL JOURNAL 2007;52:3.12. DENTAL FLUOROSIS: EXPOSURE, PREVENTION AND MANAGEMENT
JENNY ABANTO ALVAREZ , KARLA MAYRA P. C. REZENDE , SUSANA MARÍA SALAZAR
MAROCHO , FABIANA B. T. ALVES ,PAULA CELIBERTI , ANA LIDIA CIAMPONI
MED ORAL PATOL ORAL CIR BUCAL. 2009 FEB 1;14 (2):E103-7.
13. CLINICAL EVALUATION OF IN-OFFICE AND AT-HOME
BLEACHING TREATMENTS RUTA ZEKONIS, BRUCE A MATIS ,MICHAEL A COCHRAN, SALAH
E AL SHETRI, GEORGE J ECKERT, TIMOTHY J CARLSON,OPERATIVE DENTISTRY, 2003, 28-2, 114-12114. A COMPARISON OF AT-HOME AND IN-OFFICE BLEACHING VAN B. HAYWOOD
DENTISTRY TODAY 2000:19(4):44-5315. EXTERNAL BLEACHING THERAPY WITH ACTIVATION BY HEAT, LIGHT OR LASER—A SYS-TEMATIC REVIEW. BUCHALLA W, ATTIN T. DENT MATER 2007;23:586-96.16. HISTORY, SAFETY, AND EFFECTIVENESS OF CURRENT BLEACHING TECHNIQUES AND A
PLICATIONS OF THE NIGHTGUARD VITAL BLEACHING TECHNIQUE VAN B. HAYWOOD
QUINTESSENCE INT 1992;23:471 488.17. EFFECT OF BLEACHING ON SUBSURFACE MICRO-HARDNESS OF COMPOSITE AND A POLY-ACID MODIFIED COMPOSITE CHRISTIAN HANNIG, SEBASTIAN DUONG, KLAUS BECKER, ED-GAR BRUNNER, ELKE KAHLER, THOMAS ATTIN 2006 ACADEMY OF DENTAL MATERIALS.PUBLISHED BY ELSEVIER LTD.18. FLUORIDE METABOLISM AND FLUOROSIS. BROWNE D, WHELTON H, O’MULLANE D.J DENT 2005; 33: 177-18619. ASSOCIATION OF MINIMALLY INVASIVE PROCEDURES FOR THE REHABILITATION OF DIS-COLORED PERMANENT TEETH. CLINICAL CASE REPORT MAIRA ATHAIDE, LEONARDO MUNIZ
MAGAZINE FGMNEWS – EDITION 2- OCTOBER 200920. MICROABRASION OF TOOTH4.4 WITH WHITENESS RMENRICO COGO, PIETRO SIBILLA, ROBERTO TURRINI MAGAZINE FGMNEWS – EDITION 2- OCTOBER 2009
Dental News, Volume XX, Number II, 2013

READY 2 USE
NEW
Cavex Bite&White Ready 2 Use – prefi lled whitening trays
Home whitening has never been easier!
The Cavex Bite&White professional home whitening system is a safe,
rapid and easy-to-use dental whitening system for use at home and is
exclusively available through the dentist. Simply tear open the bag,
place the tray in your mouth for an hour and enjoy the result. How
easy is that? Cavex Bite&White contains 6% hydrogen peroxide (partly
as carbamide peroxide), a material that has proven itself as a whitening
agent on a global basis. Potassium nitrate has been added to sooth in
case of sensitivity. www.biteandwhite.nl or [email protected]
Cavex Bite&WhiteReady 2 UseArt. nr. BW030(6 trays per box)
CAVEX
Bite&White
Professional Dental Whitening System
A COMPLETE WHITENING TREATMENT IN A BOX
READY 2 USE
Bite&WhiteReady2Use

Dental News, Volume XX, Number II, 2013
Case report
Restorative Dentistry
Dr. Marco Calabrese
Clinical caseClass II restorations using composite resins present a number of technical problems, including the creation of a tight interproximal contact points.A tight proximal contact will balance the mesial and distal forces and prevent food impaction.For a while now, the use of preformed matrices and separator rings, in combination with wedges, has made it possible to obtain good restorations with satisfactory morphology. An even more efficient system has recently been introduced, which combines preformed matrices, innovatively designed wedges, and nickel-titanium rings providing optimum separation that remains consistent over time.This clinical case demonstrates the procedure for conservative restoration of teeth 15 and 14 using this innovative system.
The radiograph (Figure 1) shows that the patient has a distal carious lesion of 14 and a mesial lesion of 15 (Figure 2). After isolating the operative field with a rubber dam (Figure 3), the cavity on 14 is prepared (Figures 4 and 5)
THE IMPORTANCE OF THE CONTACT POINT IN CLASS II RESTORATIONS
30
Fig 1: Distal carious lesion of 14 and mesial lesion of 15.
Fig 2: Occlusal view.
Fig 3: Isolating the operative fi eld with a rubber dam .
Fig 4: Accessing the carious lesion .
fi g 1
Fig 2
Fig 3
Fig 4


Dental News, Volume XX, Number II, 2013
32
Case report
Restorative Dentistry
Fig 5: Finished cavity on 14.
Fig 7:Final restoration of 15.
Fig 6: Mesial lesion on 15.
Fig 8:Fitting the Palodent® Plus matrix to tooth 14, place-ment of wedge and ring .
Fig 9: Excellent adaptation of the matrix around 14 thanks to the ring design with V-shaped tines that accommo-date the wedge perfectly .
Fig 10: Bonding phase: applying conditioner (DE-TREY® Conditioner 36).
Fig 11: Partial fi lling of the cavity with SDR® - Smart Dentin Replacement.
Fig 12: Creating the distal wall with Ceram-X®mono+ composite
through which the mesial lesion on 15 can be reached (Figure 6) and the tooth is restored (Figure 7). The Palodent® Plus matrix is then placed on tooth 14, with simultaneous placement of a wedge and ring (Figure 8). The unique design of the nickel-titanium ring means that the matrix fits perfectly around the tooth (Figure 9). Next comes the bonding phase; DETREY® Conditioner 36 (36% phosphoric acid) is applied first (Figure 10), followed by XP-Bond® adhesive (wet bonding method). The cavity is then partially filled with SDR® – Smart Dentin Replacement (Figure 11); after waiting a few seconds for the products to self-level perfectly inside the cavity, it is polymerised.The distal wall is created with Ceram.X®mono+ composite, shade A2 (Figure 12). The matrix is removed, leaving minimal amounts of excess material to be removed (Figure 13). The restoration is then completed using Ceram X®mono+ composite, and finished (Figure 14).
Fig 5
Fig 6
Fig 7
Fig 8
Fig 9
Fig 10
Fig 11
Fig 12

GC EUROPE N.V.
GC Glass Ionomer Restoratives:essential in every dental practice
GC Fuji IX GPGC Fuji II LC Improved GC Fuji VIII GP GC Fuji IX GP Extra P-L
NEW
The power of
advanced Glass Ionomer
technology, with
the simplicityof powder and liquid delivery.

Dental News, Volume XX, Number II, 2013
34
Case report
Restorative Dentistry
Fig 13: Applying a fi nal layer of Ceram-X® mono+ shade A2 and removing the matrix. Note that there is minimal excess material to be removed during fi nishing.
Fig 14: Final restoration of tooth 14, perfect inter-proximal contacts and bite check.
ConclusionComposite restorations performed using techniques designed for amalgams (round matrices) do not create the correct anatomical contours. However, with the use of Palodent® Plus sectional matrices it is now possible to create a proximal contact that is elliptical in the buccolingual direction about 1 mm apical to the height of the marginal ridge. The interdental papilla fills the space apical to this contact and prevents lateral food impaction. The Palodent® Plus system makes it possible to create a good tooth contour adjacent to the papilla, which is necessary to reproduce the original shape.The use of the innovative DENTSPLY sectional matrix in Class II restorations allows the dentist to produce more predictable and morphologically correct restorations.
Fig 13
Fig 14
For additional information about EXOMED™
and to see all the clinical cases kindly visit www.exomed.it
Or address your questions to [email protected]
EXOMED™ allows the extraction of teeth and roots with minimal trauma: it preserves the periodontal and alveolar tissues,which remain fully undamaged!
SIMPLE AND REVOLUTIONARY:
SIMPLY NO STRESS.
PERFECT ALVEOLUSafter extraction with
Minimal Trauma
is glad to introduce

EXPERIENCE THE NEW STANDARD FOR OUR PREMIUM
DENTAL UNITS: With vision U – the future tool for best
practice.
EACH NEW ULTRADENT PREMIUM CLASS UNIT NOW
COMES WITH VISION U: The revolutionary, interactive,
touchscreen-based multimedia system.
WITH VISION U, THE DOORS OF THE FUTURE OPEN TO
YOUR PRACTICE:
> Large 21.5“ multi-touch screen – responds to „Smart-
Touch“ gestures
> Innovative patient entertainment – all informations
are freely selectable
> Optical support – digital intraoral camera with auto-
focus and barcode reader, 2- and 3D x-ray viewer
> Simple quality assurance – automatic recording of all
performance data before, during, and after treatment
> Integrated maintenance and service platform – reduces
downtime and saves costs
YOUR NEW TREATMENT UNIT:
INSPIRED EXCLUSIVELY BY YOUR
PERSONAL DESIRES. The Ultradent Premium Class offers treatment
units that you can configure as individually
as your dream car. We are a modern dental
company that flexibly manufactures our prod-
ucts based on your needs. In Germany. With
outstanding quality. And absolute perfection.
We are the experienced partner of completely
satisfied dentists. Providing exceptional reli-
ability and intuitive operation. With the new-
est technologies and multimedia. Ultradent
Premium units will captivate you.
www.ultradent.de
Ask yourULTRADENT dealer about
our IDS innovations!
Jae
ge
r &
Ta
len
te, M
un
ich

Dental News, Volume XX, Number II, 2013
MAINTAINING MISSING CENTRAL SPACE USING TAD
36
Case report
Orthodontics
Dr. Faraj A. Sedeqi
[email protected] Typically developmental anomalies are not uncommon in orthodontic cases. One of the most common contributor to malocclusion is hypodontia. Maxillary lateral incisors are known to be some of the most common congenital missing teeth. This introduces an imbalance to the maxillary and mandibular dental arch length.1 Treatment for the replacement of the missing tooth depends on a number of factors, such as arch length, the number of missing teeth, patient profile and smile line. Treatment options are either to close the space by positioning the adjacent tooth into the missing tooth site, close it with a fixed bridge2 or an implant supported crown. Treatment plans for patients with missing maxillary incisors have traditionally included either space closure or space opening for future restoration. The most common objectives to orthodontic space closure are that the treatment outcome may not look “natural”, making retention questionable, also making the functional occlusion compromised. Clinicians in general prefer to create space for the missing lateral incisor with single-tooth implants or resin-bonded bridges.3-12 Implants are becoming the treatment of choice for replacing missing teeth. One disadvantage with implants is that they should not be placed until all residual growth has subsided. That, however, means for most orthodontics patients who are adolescent, have to wait 4-6 years until the appropriate age of 18 for the implants. Maintaining the space for a long time can be challenging especially with teenagers if their cooperation and the retainer wear is compromised. Gradually with time the bone at the missing tooth site remodels thereby making it thin and may not support or be wide enough for the Implant.13 TAD or
mini screws are commonly used in orthodontic cases for anchorage ; they are relatively cheap and have proved their success in supporting tooth movement. Orthodontic management of a congenital missing upper lateral incisor is the subject of this case report. The primary orthodontic consideration was to maintain the space for the Implant and maintain bone integrity where a TAD with an acrylic prosthetic tooth was placed as a space maintainer.
Treatment Objectives Ideally, the treatment objectives for the final restoration of the missing tooth would be commenced only after there is a downward incline towards to any residual remaining growth.14 However, achievement of this objective would lead to further bone loss, thereby making it unsuitable for either an implant or a fixed bridge prosthesis at the suitable age. Therefore to preserve the bone height and thickness a temporary anchorage implant was thought of.The alternative method to reestablish normal alveolar process is by tooth transplantation which can inherent a potential for bone induction as indicated by B.U. Zachrisson et al.15
Treatment ProcedureThe clinical patient is a 14 year old female with congenitally missing left central incisor, generalized spacing on the upper anterior with a midline shift to the left. On examination she presented a straight profile and a Class I molar relation. After the alignment and the midlines were coincided with the space opened up, the braces were removed and spaces were maintained using removable retainers (fig. 1,2). In order to avoid collapsing of the arch and


Dental News, Volume XX, Number II, 2013
38
A Clinical Report
Orthodontics
further degradation of the bone height, a TAD with an acrylic tooth was shaped and trimmed accordingly to preserve the present conditions (fig. 3,4,5). As the radiographs showed that there was enough bone thickness; the roots were diverged and it had sufficient bone shelf in the edentulous area. An 8 mm screw of IMTEC® was placed parallel to the adjacent roots in alignment with the adjacent teeth. The head was placed and checked for clearance from the lower incisors. The acrylic tooth was trimmed and checked for occlusal interferences. Wax was placed in between to check for the approximate fit prior to placing it firmly with composite (fig. 4,5).
Treatment results After the 3 months’ through the retention period, the TAD was placed. The radiographs showed fairly good response without any occlusal interference from the lower anteriors. There weren’t any significant loosening, infection or damage to the underlying structures (fig. 6,7). The shape and color of the prosthetic tooth had a significant matching to the adjacent teeth. This helped in avoiding a collapse of the facial fullness and her profile. Thus improving her smile and gaining her confidence drastically (fig. 5,8,9).
Fig 1
Fig 2
Fig 3
Fig 4
Fig 5
Fig 6
Fig 7
Fig: 1 Space created for the TAD Prosthetic tooth placed firmly over the TAD
Fig: 2 Occlusal view (mirror image) space created for the TAD
Fig: 3 TAD in place
Fig: 4 Occlusal view (mirror image) - TAD in place with the pros-thetic tooth placed over it to check for interference
Occlusal Radiograph showing the TAD in place
Radiograph showing the TAD in place

Bien-Air Dental SALänggasse 60 P.O. Box 2500 Bienne 6, Switzerland Phone +41 (0)32 344 64 64 Fax +41 (0)32 344 64 91 [email protected] www.bienair.com
Micro-Series: welcome to a new dimension.30% shorter and 23% lighter, Micro-Series offers perfect balance, exceptional power and versatility.
The new Bien-Air Micro-Series offers ultra-short contra-angles andstraight hand pieces combined with the new state-of-the-art MX2 LEDmicro motor. With its ultra-compact size, the MX2 offers the same per-formance as our world leading MX micromotor. This includes power,versatility, and perfect speed control, as well as auto-reverse andtorque limitation capabilities ideal for endo.
Micro-Series: welcome to a new dimension.
Micro-Series
Turbine
Standardversion
MICRO-SERIESCOMPACT & POWERFUL

Dental News, Volume XX, Number II, 2013
40
A Clinical Report
Prosthodontic Dentistry
ConclusionTreatment of congenitally missing anterior teeth by the use of TAD is fairly a new idea which has little supporting literature. Our idea and our credit goes to Dr. John Graham for his concept on bone preservation using TAD, which was presented in the AAO annual meet 2009. ® 3M IMTEC corporation
REFERENCES
1. MCNEILL, R.W.; JOONDEPH, D.R.:CONGENITALLY ABSENT MAXILLARY LATERAL INCI-SORS: TREATMENT PLANNING CONSIDERATION, ANGLE ORTHOD.43:24–29,1973.2. TURPIN, D.L.:TREATMENT OF MISSING LATERAL INCISORS, AM. J. ORTHOD. DENTOFACIAL
ORTHOP.125:129, 2004. 3. ROSA, M.; ZACHRISSON, B.U.:INTEGRATING ESTHETIC DENTISTRY AND SPACE CLOSURE
IN PATIENTS WITH MISSING MAXILLARY LATERAL INCISORS, J. CLIN. ORTHOD. 35:221–234,2001.4. CARLSON, H.: SUGGESTED TREATMENT FOR MISSING INCISOR CASES, ANGLE ORTHOD.22:205-216,1952.5. ASHER, C.;LEWIS, D.H.: THE INTEGRATION OF ORTHODONTIC AND RESTORATIVE PRO-CEDURES IN CASES WITH MISSING MAXILLARY INCISORS. BR. DENT. J. 160(7):241-245, 1986.6. TUVERSON, D.L.: ORTHODONTIC TREATMENT USING CANINES IN PLACE OF MISSING MAX-ILLARY LATERAL INCISORS. AM. J. ORTHOD.58:109-127, 1970.7. MC NEIL, R.W.;JOONDEPH, D.R: CONGENITALLY ABSENT MAXILLARY LATERAL INCISORS:TREATMENT PLANNING CONSIDERATIONS. ANGLE ORTHOD.43: 24-29, 1973.8. ZACHRISSON, B.U.;MJOR, I.A.: REMODELLING OF TEETH BY GRINDING. AM. J. OR-THOD. 68: 545-553, 1975.9. SENTY, E.L.:THE MAXILLARY CUSPID AND MISSING LATERAL INCISORS: ESTHETICS AND
OCCLUSION. ANGLE ORTHOD.46:365-371, 1976.10. ZACHRISSON, B.U.: IMPROVING ORTHODONTIC RESULTS IN CASES WITH MAXILLARY
INCISORS MISSING. AM. J. ORTHOD.73:274-289, 1978.11. BALSHI, T.J.: OSSEOINTEGRATION AND ORTHODONTICS: MODERN TREATMENT FOR
CONGENITALLY MISSING TEETH. INT. J. PERIODONT. RESTOR. DENT.13:499-505, 1993.12. SABRI, R.: MANAGEMENT OF MISSING MAXILLARY LATERAL INCISORS. J. AMER. DENT.ASSOC.130:80-84, 1999.13. IKUYA, M.;YOICHI, T.; EISHIN, W.; HIROHIKO, S.; TADAHIKO, I.: INFLUENCE OF
CORTICAL BONE THICKNESS AND IMPLANT LENGTH ON IMPLANT STABILITY AT THE TIME OF
SURGERY – CLINICAL, PROSPECTIVE, BIOMECHANICAL AND IMAGING STUDY, BONE. 37: 776-780, DECEMBER 2005.14. ZACHRISSON, B.U.: LETTERS TO THE EDITOR; SINGLE IMPLANTS—OPTIMAL THERAPY FOR
MISSING LATERAL INCISORS?.AM. J. ORTHOD.126(6):A13-A15, 2004.15. EWA, M.C.;ARILD, S.;BJØRN, A.;ZACHRISSON, B.U.: AUTOTRANSPLANTATION OF
PREMOLARS TO REPLACE MAXILLARY INCISORS: A COMPARISON WITH NATURAL INCISORS. AM.J. ORTHOD.118: 592-600,2000.
Fig 8
Fig 9
Facial photograph after firmly fixing the prosthetic tooth to the TAD
Facial photograph prior to TAD placement


Dental News, Volume XX, Number II, 2013
Scican
General Dentistry
42
Table top sterilizers in a clinical setting have been around since the time of Louis Pasteur. The beginnings of preservation and sterilization techniques go back to ancient years. Aristotle recommended to Alexander the Great, his troops should boil water before they drank it. The beneficial effect of passing surgical instruments through flame was well known to ancient civilizations. Heat as a preservative method in medical industry was introduced in 1809 by Nicholas Appert, with his method of sealing vegetables and fruits in glass jars and then heating them. Louis Pasteur recommended to French vintners heating the new wine at 55°C in the absence of air in order to avoid serious problems. Later he noticed that moist heat was more effective than dry heat. The proposition of sterilization (1879) was simple enough: an integrated chamber with burners located at the bottom, and a serpentine connection to an adjacent water tank that would deliver a fixed amount of distilled water to the chamber at the outset of each cycle…the autoclave was developed. An autoclave is a device used to sterilize equipment and supplies by subjecting them to high pressure saturated steam at set temperature for a set time depending on the size of the load and the contents. The name comes from Greek auto - ultimately meaning self, and Latin clavis meaning key — a self-locking device.
STEAM AS THE PREFERRED TABLETOP STERILIZING AGENT, AND THE RAGING CONTROVERSY BETWEEN THE “B” AND “S” APPROACHES
Under this 19th century theory, the burners would then bring the temperature up to 121°C, the internationally accepted minimum for sterility to take place, and the resulting steam would permeate every corner, nook and cranny within and annihilate any pathogenic or non-pathogenic organism in this enclosed environment. A brilliant idea indeed that has been with us since the 1880s and that allowed for the notion of sterile instruments at or in the vicinity of clinical point-of-use to be actively pursued by the pioneers of microbiology. In order to understand the implications of cross contamination, and because of the forgetful nature of the human brain, it would be prudent to review basic definitions. Sterilization (when applied to the eradication of microorganisms): The total annihilation of pathogenic and non-pathogenic organisms in any given environment rendering a product free of viable microorganisms.* Disinfection: The reduction in numbers of pathogenic and non-pathogenic organisms in any given environment that may or may not be detrimental to human health.** As we can see, the first (sterilization) is an absolute as there are no degrees of sterility inherent to the definition, whereas the second (disinfection) is not an absolute, and we can thus speak of low, medium, and high levels of disinfection. This indicates that in the proposition “total annihilation” the key word is “total.” And here we begin to understand why steam has made it as the predominant sterilizing agent. A word on steam: It is commonly accepted that the ideal sterilization process is one that can be used between patient procedures; one that does not damage or corrode heat-sensitive instruments; one that is inexpensive; and one that consistently

For more information about SciCan products, please contact our area manager Dr. Ashraf Suleiman at [email protected] or at 0020122 2100 516.
STA
TIM
is a
regi
ster
ed tr
adem
ark
and
Your
Infe
ctio
n C
ontr
ol s
peci
alis
t is
a tr
adem
ark
of S
ciC
an L
td.
www.scican.com
Watch the product video.
STATIM, the world’s fastest autoclave from start to sterile.
A large touch screen offers communication between the unit and the user, allowing for easy operation, and
tutorial viewing.
SPEED TOUCH
G4 collects all cycle data and service history,
protecting your offi ce and patients.
COLLECT
Connect to anyone from anywhere...
your STATIM is now accessible online.
CONNECT
Introducing the new generation STATIM®... the STATIM G4 Series

Dental News, Volume XX, Number II, 2013
Scican
General Dentistry
44
penetrates narrow orifices, channels, and the lumen of instruments of certain complexity.All of the above makes pressurized steam the perfect candidate for the job as it is cost-effective, presents with no environmental concerns, and it proves to be highly pervasive. An important concept to remember regarding steam is that the increase in temperature from boiling point to 134°C is instant, and that the temperature of moist heat can be raised by increasing chamber pressure, with the accepted formula as follows: 121°C sustained for thirty minutes will bring about sterility, but if we are able to increase the temperature to 132°C, we may decrease the time of exposure down to four minutes with the same result, that is, sterility. The main objection to the traditional approach of steam in an integrated chamber was exposed in 1989 by Professor Fodder, who demonstrated that leaving 5 percent or more of air in the chamber effectively prevents a true claim of sterility. The rationale behind this is that steam tends to spread out in layers, and because steam is lighter than air, all air must vacate the chamber in order to avoid the formation of air-pockets, into which steam could not penetrate. Obviously, without such penetration sterilization could not happen and would be particularly absent within the hollow of instruments. So, it is established then that air removal is a condition sine qua non for sterility to occur. Effective air removal was achieved in 1990 with the advent of STATIM®, a revolutionary design that moved away from the integrated chamber approach to the removable cassette-based chamber, where sterile instruments can be aseptically transported right to the point of use. This is air removal by positive pressure pulse displacement (dynamic air removal), where a steam generator injects pressurized steam into the chamber. Saturated steam*** now forces the air out through a valve, with the remainder of the air being removed by opening this valve at intervals. The effect is the creation of positive pressure pulses.
EN13060EN13060 is the European Standard for small steam sterilizers, i.e. steam sterilizers whose chamber volume does not exceed 60 litres. As a long-standing, active member of the working group responsible for this standard, SciCan is intimately familiar with the requirements of EN13060+A2
2010This European Standard specifies the performance requirements and test methods for small steam sterilizers and sterilization cycles which are used for medical and dental purposes or for materials that are likely to come into contact with blood or body fluids. This Standard is intended for sterilizer manufacturers and is also used and referenced by many non-European health/regulatory authorities and sterilizer users. At the heart of this Standard is the definition of the types of approved cycles: B, S, and N, as is defined in the beginning of EN13060**** :B cycle – The sterilization of all wrapped or non-wrapped solid, hollow load products type A and porous products as represented by the test loads in the standard S cycle – The sterilization of products as specified by the manufacturer of the sterilizerN cycle – The sterilization of non-wrapped solid products.B-cycles use a vacuum pump to create a vacuum that ensures air removal before the chamber is pressurized with steam. The process is known as fractionated vacuum (negative pressure) and, relative to gravity displacement cycles, allows for better steam penetration through the entire load, but it must be tested daily for adequate air removal by using an approved process challenge device.S-cycles can use a variety of technologies to ensure air removal before the chamber is pressurized with steam. The STATIM Cassette Autoclave, as stated above, uses positive pressure pulse displacement

Planmeca ProMax®3DUnique product family
More information
www.planmeca.com
Planmeca Middle East306, City Tower 1, Sheikh Zayed Road P.O.Box 28826, Dubai tel. +971 4 33 27 682, mob. +971 50 450 2821, fax +971 4 33 27 [email protected]
Perfect sizes for all needs3D X-ray • 3D photo • panoramic • cephalometric
Romexis® software completes 3D perfectionRom
exis®PlanScan™ ProMax® 3D
ProFace™
Unique 3D combination for open CAD/CAM

Dental News, Volume XX, Number II, 2013
Scican
General Dentistry
46
(dynamic air removal). S-cycles do not require daily air removal testing. In accordance with EN13060:2004+A2 2010 Section 7.1, STATIM sterilizers are tested on a microbiological basis and have proven to consistently achieve a sterility assurance level of 10-6 (or a 6-log reduction in microorganisms) for a variety of loads (solid, hollow, hinged, etc.). Furthermore, as required by Section 7.2 and 7.3, STATIMs 2000S and 5000S have passed Type testing, and each unit shipped has successfully undergone Works testing (the results of the Works test are provided with each unit).N-cycles do not use multiple steam purges during the preparation phase of the cycle that would ensure air was removed from cavities of instruments such as found in dental handpieces. Here the trapping of air is a real concern and the formation of air pockets a possibility and therefore N-cycles, similar to gravity displacement cycles are only adequate for solid instruments.
Microbiological TestingBecause STATIMs are S-cycle machines, they are very likely the sterilizers that have the most microbiological test data to prove their efficacy in destroying microorganisms, especially in medical and dental environments, while other autoclave manufactures (B-cycles) rely on EN867-5:2001 approved PCDs (process challenge device) to claim load processing. STATIM users can therefore have the utmost assurance in the sterilization efficacy of the STATIMs. They have been microbiologically tested and proven to successfully and effectively sterilize a variety of instruments. A PCD is a mechanical device which simulates the worst case of conditions for attainment of the specified sterilization conditions within the items to be sterilized as defined by EN867-5:2001, definition 3.2. The device is constructed so that a biological or non-biological indicator system can be placed within the device in the position which it is most difficult for the sterilizing agent to reach. The design of the process challenge device depends on the nature of the goods to be sterilized and the sterilization procedure. The performance of the STATIM autoclaves have been validated via microbiological testing, conducted by a well respected researcher and leader in the field of infection control. To regularly
validate the STATIMs and ensure they continue to attain the specified sterilization conditions, the STATIM Process Challenge Device (PCD) has been designed in order to demonstrate that the sterilization parameters required and validated during microbiological testing have indeed been obtained. This device tests the unit and ensures that the mechanical components and software controls are functioning correctly and match those of the units tested during microbiological testing. In sum, the removal of the air***** from the chamber prior to the commencement of “killing” time is the fundamental consideration in selecting the best autoclave for any clinical practice. The methodology through which this removal is achieved is of secondary importance. The fact remains, in spite of the opinions of manufacturers, advocates, partisans and others, that both the S and the B cycles expel the air from the sterilization chamber to such an extent where sterilization of hollow instruments (such as dental handpieces) can be attained. Where the removal of air through positive pressure (STATIM) establishes its dominance is in the reduced duration of the cycle, aspect this rightly coveted by most professionals, since the instrument turn-around time could be as short as 10 minutes. This is achieved as a result of having the technological capability of injecting steam at will, and of creating conditions of sterility (temperature and pressure) through a chamber whose walls are extremely thin. In mechanical terms, the effect of this approach is a gentler sterilization process for your expensive instruments.
* Definitions of sterility in the medical literature vary in composition depending on the source, but the definition given here encompasses general consensus.** Definitions of disinfection in the medical literature vary in composition depending on the source, but the definition given here encompasses general consensus.*** EN 13060 2004+A2 2010, § 3.34**** EN 13060 2004+A2 2010, Table 1***** EN 13060 2004+A2 2010, § 3.3


Dental News, Volume XX, Number II, 2013
Esthetic Dentistry
48
VITA
VITA ENAMIC THE FIRST HYBRID DENTAL CERAMIC IN THE WORLD WITH A DUAL-NETWORK STRUCTURE
In January 2013, a new generation of materials for chairside treatment using CAD/CAM technology were made available. The future of chairside CAD/CAM restoration is VITA ENAMIC (Fig. 1). A
composite material that is unique worldwide in combining the benefits of conventional ceramic and composite materials. Both scientific studies and initial clinical experience confirm that with the VITA ENAMIC hybrid ceramic, a new dimension in stability, reliability, precision and cost-efficiency can be achieved.
Material conceptWith the development of VITA ENAMIC, a whole new approach has been adopted, creating a hybrid ceramic comprised of a dominant ceramic network reinforced by a polymer network structure. With both networks fully integrated with one another, VITA ENAMIC offers considerable benefits for patients and for practice and laboratory use – from a lower tendency towards brittle fracture than pure ceramics, through to greater abrasion resistance than composite materials.
Findings of materials scienceWith flexural strength values of approximately 150-160 MPa, the results for VITA ENAMIC
are within the same range as those for silicate ceramics. And at 30 GPa, the material also offers a modulus of elasticity comparable to that of human dentin. Up until now, no dental restoration material has matched this “natural” elastic range. The result is unusually high stability as demonstrated by internal and external studies. Thanks to the elasticity provided by the integrated polymer network, VITA ENAMIC absorbs the applied load, achieving the best results (approx. 2890 Newtons, see Fig. 2) in a fracture load study
of any of the materials tested. This result also correlates with the study results published by Dr. Petra Güß of the clinic for oral and maxillofacial surgery at the University of Freiburg. Here it was found that when a dynamic load is applied in a chewing simulator, VITA ENAMIC crowns demonstrate a 100 % survival rate, both for walls of normal and of reduced thickness (Fig. 3). As a measure of the reliability of a material, the Weibull modulus indicates the benefits of VITA ENAMIC particularly effectively. An internal study conducted by the VITA Research & Development
Fig. 1: With its dual-net-work structure, the VITA ENAMIC hybrid ceramic represents a new class of materials.
Fig. 2: In this test setup, VITA ENAMIC demonstrates the highest fracture load of approx. 2890 Newtons and the lowest standard deviation.Source: Internal study, VITA R&D
fig 2
fig 1

VITA ENAMIC® creates a new definition for resistanceThe first hybrid ceramic with dual network structure for unsurpassed absorption of masticatory forces
VITA ENAMIC sets new standards for resistance by
combining strength and elasticity and providing unsur-
passed absorption of masticatory forces. VITA ENAMIC
ensures utmost dependability and efficient processing
for dental practices and laboratories. And patients feel
The En formula for success: strength + elasticity = reliability²
3411
E
that VITA ENAMIC restorations are identical to natu-
ral teeth. VITA ENAMIC is particularly suited for crown
restorations in the posterior area and minimally invasive
restorations. More information at www.vita-enamic.com
facebook.com/vita.zahnfabrik

50
VITA
Esthetic Dentistry
department shows that at a value of 20, the Weibull modulus for the VITA ENAMIC hybrid ceramic is more than double that of comparable materials for the fabrication of monolithic single-tooth restorations (Fig. 4).
In practical application, the superior properties of the new hybrid ceramic make it ideally suited to crown restorations in areas with high occlusal load, and facilitate reduced wall thickness for minimally-invasive restorations. They also enable greater precision, improved edge stability and, as a result, finer, more accurate milling results than previously possible using conventional CAD/CAM ceramics. SEM images illustrate the difference compared to conventional ceramics (Fig. 5).
At the same time, the innovative composite material can also be milled more cost-effectively than comparable CAD/CAM materials – the milling times for VITA ENAMIC restorations are the shortest both in normal and in fast milling mode, while also ensuring a longer service life for diamond milling tools. It is also important to note
that in the same way as silicate ceramics, VITA ENAMIC also facilitates superior-quality etching using hydrofluoric acid gel. This is an important factor in ensuring permanent and tight contact adhesion between the restoration and the tooth substance.
Processing VITA ENAMIC will be available initially in block size EM-14 (12 x 14 x 18 mm), as well as in the shades 0M1, 1M1, 1M2, 2M2 and 3M2, and in two degrees of translucency. The hybrid ceramic can be processed in the usual manner using the CEREC and inLab MC XL systems, for example. Software version V4.0 or higher is prerequisite. For easy, efficient pre-polishing and high-gloss polishing of VITA ENAMIC restorations that is gentle on the material, a special polishing set is provided (Fig. 6).
The VITA ENAMIC STAINS KIT, which contains six stains as well as accessories (Fig. 7), can be used for characterization. The stains are bonded to the restoration as part of a polymerization process. Surface sealing can be performed using the chemical glaze material VITA ENAMIC GLAZE, which increases the durability and brilliance of the shade in the oral environment. Processing could not be easier – simply condition the surface of the
Fig. 3: The survival rate of VITA ENAMIC crowns with walls of normal and reduced thickness is 100%.Source: University of Freiburg, Dr. Güß
Fig. 4: Of the materials examined in this test, VITA ENAMIC offered the great-est reliability. The Weibull modulus is 20.Source: Internal study, VITA R&D
Fig. 5: VITA ENAMIC exhibits high edge stability even in areas with thin margins. Top view: 30° wedges: left: VITA ENAMIC, right: e.max CAD Fig. 6: These instruments, which have been devel-
oped especially with VITA ENAMIC in mind, allow superior, plaque-resistant surface results to be achieved.
fig 3
fig 4
fig 5
fig 6
Dental News, Volume XX, Number II, 2013


52
restoration, mix and apply the shades, perform intermediate polymerization, apply chemical glaze and complete final polymerization. Firing is not required.
SummaryThanks to the dual ceramic-polymer network, the new VITA ENAMIC composite combines the benefits of ceramic and composite materials in one outstanding product, providing a quantum leap in the development of CAD/CAM materials. It is approved for single-tooth restorations such as inlays, onlays, veneers and crowns, and is also distinguished not least by the superior comfort it offers to patients, thanks to material properties similar to those of natural dentition.
fi g 7
Fig. 7: Simply apply the VITA ENAMIC stains to the restoration and polymerize – that’s all that’s required to quickly characterize the shade of VITA ENAMIC restorations.
VITA
Esthetic Dentistry
With Fuji IX GP Extra in powder-liquid, GC, the glass ionomer world leader, is providing the most advanced GI technology to Powder Liquid users.Actually, advances in glass technology have resulted in the development of GC Fuji IX GP EXTRA, a high strength glass ionomer cement with a new generation of glass fi ller which gives the restorations a very high translucency that changes little over time. The result is natural aesthet-ics never before achievable with conventional glass ionomer. GC special glass fi ller used in GC Fuji IX GP EXTRA releases three times more fl uo-ride than conventional glass ionomers so it provides even better protec-tion against caries. The comfortable working time combined with a fast setting time mean you can start fi nishing and polishing just two and a half minutes after mixing.
The indications of Fuji IX GP Extra are for permanent and temporary teeth. It can be used for Class I and II restorations in children’s teeth, non-load-bearing Class I and II restorations in adult teeth, Class V and root surface restorations, core build-up and for use with a composite or an inlay in the immediate or delayed sandwich technique.
Find out more about Fuji IX GP Extra powder-liquid at www.gceurope.com
GC Fuji IX GP EXTRA from GC
Improved Fast-Setting Packable Glass Ionomer Restorative now available in powder-liquid delivery
Dental News, Volume XX, Number II, 2013


Dental News, Volume XX, Number II, 2013
54
DR. JASIM AL SAIDI
OmanInternational Dental Conference
www.facebook.com/dentalnews1
More PicturesAvailable OnFebruary 27-28, 2013
Al Bustan Hotel, Muscat, Sultanate of Oman
On behalf of the whole team of the “Oman International Dental Conference 2013”, I would like to extend my warm welcome to all of you participating in this rich scientific event, which is intended to be held regularly every two years. It is also my great honor on this occasion to express my heartfelt thanks to all of those who spared their valuable time, to those who came up with new ideas and especially to those who made this conference a reality. We welcome you all in Oman so we can experience together the rich culture, the history and the hospitality of the Sultanate.
Dr. Jasim Al SaidiChairman of the Organizing committee
MINISTER DR. AHMED AL SAIDI IN THE MIDST OF THE GUESTS AT THE OPENING CEREMONY
MINISTER DR. AHMED AL SAIDI CUTTING THE RIBBON OF THE EXHIBITS DR. LOUIS HARDAN LECTURING ON ESTHETICS

We go further todeliver completewaterproof durability
5 YEARWARRANTYAVAILABLEOver 30 years ago, we redefined dental intraoral radiography with the inventionof the RVG sensor. Since then, every sensor we make is even stronger than the last.Our years of testing and continuous development assure you of a level of durabilityand image quality that is simply second to none.
Instant, high-quality image output with an unsurpassed true resolution of up to >20 lp/mm
Waterproof and fully submersible sensor head for optimal disinfection and increased durability
Flexible and robust cable, designed and tested to withstand strong bends and pulls
Shock-resistant casing and silicon padding offer extra protection from falls, bites and other damage
Available from participating Dealers.
Call +44 1442 838908 or e-mail [email protected] arrange a demonstration.
You can also visit: www.carestreamdental.com© Carestream Heath, 2013

Dental News, Volume XX, Number II, 2013
PICTURES FROM THEEXHIBITION FLOOR
OMAN INTERNATIONALDENTAL CONFERENCE

The Power. The Silence. The new TornadoSuper
Silent
COMPRESSED AIR
SUCTION
IMAGING
DENTAL CARE
HYGIENE
Tornado – the new generation of compressors from Dürr Dental
Dürr Dental, the inventor of oil-free dental compressors, presents an
unbelievably quiet and powerful compressor for dentistry in the form
of the new “Made in Germany“ Tornado.
▪ Oil-free, dry, and hygienic
▪ One of the quietest of its kind
▪ Dust- and Sandresistant
▪ Antibacterial inner tank coating
▪ Low-maintenance thanks to membrane-drying unit
Duerr Dental Middle East, P.O.Box: 87355, Al Ain - U.A.E.,
Mobile: +971 (0) 50 - 550 84 12, Fax: +971 (0) 3 767 - 5615,
email: [email protected]

Dental News, Volume XX, Number II, 2013
More PicturesAvailable OnMarch 12-16, 2013
Koelnmesse, Cologne, Germany www.facebook.com/dentalnews1
125,000 VISITORS FROM 149 COUNTRIES & 2,058 SUPPLIERS
FROM 56 COUNTRIES
IDS 2013 SETS NEWRECORDS
58


Dental News, Volume XX, Number II, 2013
MASTER DENTAL TECHNICIANS ANDDENTISTS, WILL HAVE TO WORK TOGETHER
MORE CLOSELY IN THE FUTURE


Dental News, Volume XX, Number II, 2013
1mm layer TheraCal LC
Regenerative layer stimulates hydroxyapatite
stays where it is placed
calcium hydroxide and RMGI
technique
TheraCal LC is an internal flowablepulpal protectant material knownas Resin Modified Calcium Silicates(RMCS).
Surrounding enamel is etched
All-Bond Universal single-bottlelight-cured adhesive can be usedfor any dental procedure.
Core-Flo DC is a radiopaquedual-cured flowable materialideal for core build-up, postcementation and dentinreplacement.
To learn more e-mail [email protected] visit www.bisco.com
TheraCal LC
NEW Products from BISCO
All-Bond Universal Core-Flo DC

HENRY SCHEIN BRAND Beyond Satisfaction!Henry Schein Brand products offer our clients maximum value withoutcompromising on quality. We offer quality products you can trust to fulfill your practice merchandise needs—each bearing the Henry Schein Seal of Excellence, your guarantee of satisfaction.
Henry Schein, Inc. is the world’s largest provider of healthcare products and services to office-based dental, medical,and animal health practitioners.

The 17th Kuwait Dental Association Conference
More PicturesAvailable OnApril 13-15, 2013
Radisson Blu Hotel, Kuwait www.facebook.com/dentalnews1
TROPHY TO DR. MOHAMAD HAFEED TROPHY TO DR. FADIA DEEB
DR. IBRAHIM TAQI HEAD OF THEORGANIZING COMMITTEE
TROPHY TO DR. ELIE MAALOUF TROPHY TO DR. DOMINIKI CHATZOPOULO
TROPHY TO DR. TONI DIB
TROPHY TO DR. AZIM QADDOMI TROPHY TO DR. AISHA SULTAN

THE KUWAIT DENTAL ASSOCIATION BOARD MEMBERS AND THE ORGANIZING COMMITTEES GROUP PICTURE
PHOTO OF THE LEBANESE DELEGATION WITH THE ORGANIZERS DURING THE CLOSING CEREMONY


The #1 patient-requested professional whitening system*
is now better than ever.
New Philips Zoom offers advanced light technology that gives you more control and your patients even greater results. And with a worldwide public awareness campaign to drive patients to you and new programs to help you easily integrate Philips Zoom WhiteSpeed light-activated whitening into your practice, you’ll have the answer to the confident, beautiful smile your patients are asking for.
Ask about the new Philips Zoom WhiteSpeed today. Visit philipsoralhealthcare.com. For more information, contact your local sales representative or call +971 50 643 1707.
*In the United States. Philips is a registered trademark of Koninklijke Philips Electronics N.V. ©2012 Discus Dental, LLC. All rights reserved. To be dispensed by or on the order of a dental professional only. ADV-3545ARA 101912
EGYPTElsafaaTel: 2 (0) 10 1466997
JORDAN Al GhadMedical Supplies Tel: +962 6 552 6358
KUWAIT Alpha Medical Co. Tel: +965 2247 8611
LEBANON G. Tamer HoldingTel: 961 1 694000
MOROCCO Ortho-Rama +21 2 22862086
SAUDI ARABIABashir Shakib Al Jabri & Co. Tel: +966 26700430
TUNISIAMSITel: +216 73 449 401
UNITED ARAB EMIRATES Al Hayat PharmaceuticalsTel: +971 6 5592 481

Int’l Quintessence Dental Arab Congress
More PicturesAvailable OnApril 24-26, 2013
Riyadh, KSA www.facebook.com/dentalnews1
The Second International Quintessence Dental Arab Congress jointly organized by the Riyadh Colleges of Dentistry and Pharmacy (RCsDP) and the Quintessence International Publishing Group and the 8th Riyadh International Dentistry Meeting (RIDM) closed on 26 April 2013. The meeting was held at the Al Faisaliah Hotel in Riyadh City and covered eleven scientific papers presented by internationally known dental experts and authors of dental books from Switzerland, Italy, Germany and Great Britain. The program also included a short ceremony for the GCC Preventive Dental Program. President Tawfik Ahmad Khoja, President of the Executive Board of the Health Ministers Council for GCC was on hand to officiate at this ceremony.
68
PROF. ABDULLAH AL SHAMMERYTHE RECTOR OF THE RIYADH
COLLEGES OF DENTISTRY ANDPHARMACY
DR. ESAM TASHKANDI GIVING THETROPHY TO DR. ANDREA RICCI
PRESIDENT TAWFIK AHMAD KHOJA RECEIVING THE TROPHY FROM PROF. ABDULLAH AL SHAMMERY
TROPHY TO DR. FEDERICOFERRARIS FROM ITALY THE GCC HEALTH MINISTERS WERE AWARDED PLAQUES AND TOKENS OF APPRECIATION AS A FITTING CAP TO THE CEREMONY

PICTURES FROM THEEXHIBITION FLOOR
LEFT TO RIGHT DRS. MASSIRONI, RASPERINI, RICCI, FERRARIS



OptiBond™ XTRUnmatched power for all your direct and indirect restorations.
OptiBond XTR Self-Etch, Light-Cure Univesal Adhesive.
Extraordinary performance for long-lasting restorations.
Minimizes post-operative sensitivity, maximizes patient comfort.
A true universal adhesive.
Enables use with all cements, core build-up materials and substrates.
For more information visit:
Your practice is our inspiration.™KerrHawe SA P.O. Box 268 6934 Bioggio Switzerland Freephone: 00800 41 05 05 05 Fax: ++41 91 610 05 14 www.kerrdental.eu
Clear, long resin tags with penetration intolateral dentin tubule branches (2,000x).
OptiBond XTR Self-Etch, Light-Cure Universal Adhesive.




Dental News, Volume XX, Number II, 2013
The Next Generation of the Endo Gold Standard
The AngleFix concept provides the tioLogic© implant system with yet another indication it enables edentulous patients to be treated with immediate restorations such as screw retained bridges or a bar constructions in the maxilla or mandible. It consists of various fully compatible prosthetic components, which enable the tioLogic© implants to be inserted at an angle, in order to avoid augmentation in the posterior region and enable anatomically critical areas to be treated with care. The prosthetic supporting surface is displaced in a distal direction, the prosthesis is additionally supported and the local bone substance is put to best possible use. The AngleFix abutments are available for the implant lines S, M and L in straight (0°) and angled at 18° and 32°. The angled abutments can be positioned exactly using the integrated PentaStop®. The design of the abutments is such, that implant axis deviations of up to 44° to one another are possible. There are closure screws, impression copings, laboratory analogs and acrylic and titanium copings available for the extended prosthetic restoration. There are two angle aids available in 18° and 32° for the exact alignment of the implants. Alternatively, the implant axis can also be determined using the navigation system tioLogic© pOsition and the drilling template made with this. If you should have any questions, the Dentaurum Implants Hotline is available with experienced implantologists and dental technicians to give assistance. For more information www.dentaurum-implants.de
PROTAPER NEXT is the newest innovation to the DENTSPLY Maillefer PROTAPER system, which has been the gold standard in endodontics for many years. It is still based on the PROTAPER philosophy, including a single file sequence for all clinical cases, variable tapers for optimised crown-down technique and commonly approved apical finishing diameters.PROTAPER NEXT has an off-centred rectangular cross section, providing a snake-like “swaggering” movement of the file in the root canal. The DENTSPLY proprietary M-WIRE NiTi provides improved flexibility to the file as well as greater resistance to cyclic fatigue. As a result, PROTAPER NEXT covers more difficult clinical cases, improves safety and also shortens the shaping time. For more information www.dentsplymea.com
#76
AngleFix ConceptProsthetic Restorations on angled tioLogic© Implants
Hu-Friedy’s SlimCollection, which consists in a full line of sleek new orthodondic instruments that feature smaller, thinner, lighter working ends for more maneuverability. Slim collection consists in eight new instruments, which guarantee the orthodontist a more efficient and precise working method. The pliers, tweezers and cutters of the new product line are considerably narrower, thinner and lighter than conventional products to greatly improve intraoral adaptation, flexibility and view. The result: More maneuverability, more patient confort and time savings for doctor and patient.For more information www.hufriedy.eu
SlimCollection


Dental News, Volume XX, Number II, 2013
#78
Exomed™
NEW! Cavex Bite&White Ready 2 Use ‘pre-filled whitening trays’
VITA ENAMIC the first hybrid dental ceramic in the world
From our R&D department a new company has been created, Medesy Engineering,whose unique mission is to develop new materials and new products.Exomed™ is the extraordinary result of Medesy Engineering, Exomed™is an instrument which allows the extraction of teeth and roots with minimal trauma.Among the most important advantages: - The periodontal and alveolar tissues remain fully undamaged after the extraction, the neighbouring tissues are practically intact after the operation - No need of forceps and root elevators, nor to perform a luxation and syndesmotomy before extraction!- The implant insertions are possible even immediately after the extraction: the alveolar sites have no lacerations - The patient will recover from the extraction in a much shorter time. - The extraction of roots is really easier and faster … THE MORE YOU KNOW IT, THE MORE YOU USE IT! SIMPLE & REVOLUTIONARY. EXOMED™, SIMPLY NO STRESS.For more information www.exomed.it
VITA Zahnfabrik have created a new generation in ceramic materials: VITA ENAMIC is the first hybrid dental ceramic in the world with a dual-network structure that combines the best of what ceramic and composite materials have to offer. The CAD/CAM blocks are not only suitable for fabricating conventional inlays, onlays, veneers and crowns for anterior and posterior applications, but they can also be used for minimally-invasive restorations such as non-prep veneers and for restorations in areas where space is limited.For more information www.vita-zahnfabrik.com
The Cavex Bite&White Ready 2 Use professional home whitening system is a fast, safe and above all very simple whitening system for use at home. Just open the packaging, place the pre-filled tray in your mouth and enjoy the result after an hour. Mere child’s play! The highly viscous Cavex Bite&White Ready 2 Use whitening gel contains 6% hydrogen peroxide (partly as carbamide peroxide), a sustainable and active combination of effective whitening substances with a proven reputation worldwide as an effective whitening agent. Adding potassium nitrate avoids sensitivity. The unique ‹one-size-fits-all› Dryflex® whitening tray is made of a special type of plastic which the mouth tolerates well. Thanks to its 95% compatibility, the whitening tray is suited to almost everyone. Cavex Bite&White Ready 2 Use complies totally with new European legislation for teeth whitening agents. For more information www.biteandwhite.eu


Turn Complex Class II into Simple Class I Cases
* Images courtesy of Dr. Clark Colville.
© 2012 Ortho Organizers, Inc. All rights reserved.
With its non-invasive design, the Carriere Distalizer Appliance corrects Class II malocclusion at
the beginning of treatment, prior to bracket placement when patient motivation is highest.
Call us today at 888.851.0533 or visit us online at OrthoOrganizers.com.
Carriere Ortho 3D A FREE App. for iPads, iPhones, and
Android tablets and phones
Carriere
Self-Ligating Bracket
* Typical case: Patient 16 years
Start of treatment, prior to placement
of Carriere Distalizer Appliance 5.10.10
Class II to Class I achieved, and
Carriere Distalizer Appliance treatment
completed 8.30.10
Total orthodontic treatment
completed 3.7.12
SHIFTING THE WAY YOU THINK ABOUT ORTHODONTICS.The Carriere® Distalizer™ Appliance