Dental News December 2011
86
ISSN 1026 261X www.dentalnews.com Volume XVIII, Number IV, 2011 Treatment of ANGLE CLASS II FULL ARCH IMPLANT P ARENTAL SEPARATION National Guard Int’l Conference - KSA
-
Upload
dental-news -
Category
Documents
-
view
226 -
download
4
description
Â
Transcript of Dental News December 2011

ISSN
102
6 26
1X
www.dentalnews.com Volume XVIII, Number IV, 2011
Treatment ofANGLE CLASS II
FULL ARCH IMPLANT
PARENTAL SEPARATION
National Guard Int’l Conference - KSA

KaVo ESTETICA® E50
KaVo Dental GmbH · D-88400 Biberach/Riß · Telefon +49 7351 56-0 · Fax +49 7351 1103 · www.kavo.com
Experience the feel of perfection and allow
visionary details and an intuitive operating
system to make your everyday work easier.
Simple to use: user-friendly dentist
element thanks to ideal combination of
direct buttons and menu control.
Simple to upgrade: state-of-the-art
upgrade possibilities and visionary
system solutions.
Simply reliable: 100 years experience
with highest quality, made in Germany.
Simply made to perfection.The new KaVo ESTETICA E50.
The best things in lifeare simple.The new KaVo ESTETICA® E50. Simply top of its class.
1909 – 2009



www.ivoclarvivadent.comIvoclar Vivadent AGBendererstr. 2 | FL-9494 Schaan | Principality of Liechtenstein | Tel.: +423 / 235 35 35 | Fax: +423 / 235 33 60
all ceramic
all you need
“THAT’S ALL I NEED!” Galip Gürel, Dentist, Turkey.
Many different indications and many different materials to choose from – this scenario is a thing of the past. The IPS e.max system allows you to solve all your all-ceramic cases, from thin veneers to 12-unit bridges. Dental professionals all over the world are delighted.

* +
Tel. +39 - 0425 597611 - Fax +39 - 0425 [email protected] - www.zhermack.com
YOUR SMART CHOICE TO CREATE SMILES
Zhermack presents zmack® system, the new universal
light-cured composites line for conservative restoration that has been studied to solve everyday needs of dental practitioners and patients of any age. Born today, as the result of our laboratory experience and know how.
Specially designed to mimetically blend with the surrounding tooth structure, zmack® comp shades become imperceptible, for very natural, aesthetic and lasting results.
zmack® system
zmack® comp shades: A1; A2; A3; A3.5; A2-O; A3.5-O; B1;
B2; B3; C3
*For zmack® intro kits content, contact your local dealer or visit www.zhermack.com
zmack® system
HIG
H QUALITY
FA IR P RIC E
TOTAL CAMOUFLAGE!

Dental News, Volume XVIII, Number IV, 2011
3
13
20
30
34
46
66
72CO
NTE
NTS
CONTENTS Volume XVII I , Number IV, 2011
Alfred Naaman, Nada Naaman, Jihad Fakhoury, Dona Raad, Antoine Saadé, Lina Chamseddine, Tarek Kotob, Mohammed Rifai, Bilal Koleilat, Mohammad H. Al-JammazVanessa AbdelahadKrystel KouyoumdjisMicheline Assaf, Nariman NehmehJosiane YounesAlbert SaykaliGisèle Wakim, Marielle KhouryTony Dib1026-261X
DENTAL NEWS – Sami Solh Ave., G. Younis Bldg.POB: 116-5515 Beirut, Lebanon.Tel: 961-3-30 30 48Fax: 961-1-38 46 57Email: [email protected]: www.dentalnews.comwww.facebook.com/dentalnews1
INTERNATIONAL REVIEW BOARDPr. M.A. Bassiouny BDS, DMD, MSc, Ph.D. Director International Program, Temple University, Philadelphia, USA.Pr. N.F. Bissada D.D.S., M.S.D Professor and Chairman, Department of Periodontics, Case Western Reserve University, USA.Pr. Jean-Louis Brouillet D.C.D, D.S.O. Chairman, Department of Restorative Dentistry, Aix-Marseille II, France.Pierre Colon D.C.D., D.S.O. Maître de conférence des universités, Paris, France.Dr. Jean-Claude Franquin, Directeur de lʼUnité de Recherche ER116, Marseille, France.Pr. Gilles Koubi D.C.D., D.S.O. Department of Restorative Dentistry, Aix-Marseille II, France.Pr. Guido Goracci. University LA SAPIENZA, School of Medicine & Dentistry, Roma, Italia.Brian J. Millar BDS, Ph.D. Guyʼs, Kingʼs, and St. Thomasʼ College School of Medecine & Dentistry, London, UK.Pr. Dr. Klaus Ott, Director of the Clinics of Westfälischen Wilhelms-University, Münster, Germany.Wilhelm-Joseph Pertot DEA, Maître de conférence, Aix-Marseille II, France.Pr. Dr. Alfred Renk, Bayerische Julius-Maximilians-University, Würzburg, Germany.Dr. Philippe Roche-Poggi DEA. Maître de conférence des universités, Aix-Marseille II, France. Michel Sixou D.C.D., D.E.A. Department of Priodontology, Toulouse, France.Pr. M. Sharawy B.D.S., Ph.D. Professor and Director, Department of Oral biology, Medical College of Georgia, Augusta, Georgia, USA.V
EDITORIAL TEAM
COORDINATORART DEPARTMENT
SUBSCRIPTIONADVERTISING
PHOTOGRAPHYTRANSLATION
DIRECTORISSN
DENTAL NEWS IS A QUARTERLY MAGAZINE DISTRIBUTED MAINLY IN
THE MIDDLE EAST & NORTH AFRICA IN COLLABORATION WITH
THE COUNCIL OF DENTAL SOCIETIES FOR THE GCC.Statements and opinions expressed in the articles
and communications herein are those of the author(s) and not necessarily those of the Editor(s) or publisher. No part of
this magazine may be reproduced in any form, either electronic or mechanical, without the express written permission of the publisher.
Treatment of Angle Class II division II maloc-clusion with deep overbiteDr Kholood Alfoudari Full Arch Implant Reconstruction of patient with Combination Syndrome: A clinical Approach Husain Ghadhanfari, Abdulaziz AlSanousi, Edward Monaco
Should Bio-Oss be used as an onlay bone substitute?Abdullah Al-Harkan
Parental Separation Nourah Al-Maheemid
The 3rd National Guard and 1ST Saudi Endodontic Society
EDA - Cairo EGYPT
DFCIC 2011 - Dubai
www.facebook.com/dentalnews1twitter.com/dentalnews1




CAVEXYOUR IMPRESSION IS OUR CONCERN Cavex Holland BV, P.O. Box 852, 2003 RW Haarlem, The Netherlands. Tel +31 23 530 77 00 Fax +31 23 535 64 82 [email protected] www.cavex.nl
Cavex AlginatesSuperior in strength, control and balance
Cavex ColorChange• 5 days dimensional stable• Fast set• Functional colour change
Cavex Impressional• Extremely elastic• Normal and fast set
Cavex Orthotrace• Firm consistency• Developed for the orthodontic practice• Extra fast setting
5 years shelf life
snap-setsuperior tearresistance
Cavex ImpreSafe• Kills bacteria, viruses an fungi in just 3 minutes• 1litre of concentrate for over 30 weeks disinfected impressions• Safe for alginate, polyether and silicone impressions
2011
Top Infection Control Product
Cavex GreenCleanffi cient alginate and gypsum removerlemon aroma
= 500 clean trays!

mectron s.p.a., via Loreto 15/A, 16042 Carasco (Ge), Italia, tel +39 0185 35361, fax +39 0185 351374, [email protected]. www.mectron.com
Û IN 1997 WE INVENTED PIEZOELECTRIC BONE SURGERY. IN 2011 WE DID IT AGAIN.THE NEW MECTRON PIEZOSURGERY® touch
Û EXCLUSIVE GLASS TOUCH SCREEN, HANDPIECE WITH SWIVEL-TYPE LED LIGHT

Micro-Series: welcome to a new dimension.30% shorter and 23% lighter, Micro-Series offers perfect balance, ex cep tional power and versatility.
The new Bien-Air Micro-Series offers ultra-short contra-angles andstraight hand pieces combined with the new state-of-the-art MX2 LEDmi cro motor. With its ultra-compact size, the MX2 offers the same per-formance as our world leading MX micromotor. This includes power,versatility, and perfect speed control, as well as auto-reverse andtorque limitation capabilities ideal for endo.
Micro-Series: welcome to a new dimension.
Micro-Series
Turbine
Standardversion
MICRO-SERIESCOMPACT & BALANCED
Bien-Air Dental SALänggasse 60 P.O. Box 2500 Bienne 6, Switzerland Phone +41 (0)32 344 64 64 Fax +41 (0)32 344 64 91 [email protected] www.bienair.com

©2011 Zimmer Dental Inc. All rights reserved. Please check with a Zimmer Dental representative for availability and additional information.
www.zimmerdental.com
Visit TrabecularMetal.zimmerdental.com to view
a special ingrowth animation and request a
Trabecular Metal Technology demo.
I am the Zimmer® Trabecular Metal™ Dental Implant, the first dental implant to
offer a mid-section with up to 80% porosity—designed to enable bone INGROWTH as well as ONGROWTH.
Through osseoincorporation, I harness the tried-and-true technology of Trabecular Metal Material, used
by Zimmer Orthopedics for over a decade. I add ingrowth to implant dentistry.... and I am Zimmer.
Trabecular Metal Material
Osseoincorporation Trabecular bone
The process of ingrowth
THE IMPLANT FOR
OSSEOINCORPORATION
Artistic Rendering

Dental News, Volume XVIII, Number IV, 2011
11
INTERNATIONAL CALENDAR
www.dentalnews.com
GET YOUR ISSUE ONLINE
ADVERTISING INDEX
January 31 - February 2, 2012AEEDC Dubai 2012www.aeedc.com
January 31, 2012Saudi Orthodontic Society, at the Hayatt, Jeddah, KSA.www.saudiortho.org.sa
February 6 - 8, 201214th King Saud University & 23rd Saudi Dental Society International Dental Conferencewww.sds.org.sa
March 17-19, 2012 The 16th Kuwait Dental Association Dental Conferencewww.kda.org.kw
May 3 - 4, 20126th CAD/CAM & Computerized Dentistry International Conference, Dubaiwww.cappmea.com
May 31, 2012Saint Joseph University, Dental School scientific meetingBeirut, Lebanon Email: [email protected]
August 29 - September 1, 2012FDI 2012 Annual World Dental Congress, Hong Kongwww.fdiworldental.org
September 19 - 22, 2012Beirut International Dental Meeting 2012, Lebanonwww.lda.org.lb
November 7-11, 2012 Alexandria University international meeting, Egypt
November 9 - 10, 20124th Dental - Facial Cosmetic International Conference, Dubaiwww.cappmea.com
ACTEON 67 - A-DEC 27 - ALTURKI 79 - BEYOND 31 - BIEN AIR 9 - BISCO 61- BLUE X 55 - CAVEX 7 - CARESTREAM 6 - COLTENE WHALEDENT 28 - DENTSPLY 39 - DEPURDENT 80 - DR. WILD 4, 5 - DURR 44,69 - GC 37 - GSK C3, 57 - HU-FRIEDY 18 - INIBSA 17 - INTENSIV 32 - IVOCLAR C4 – VIVADENT 1 - KAVO C2 - GENDEX 33 - KERR 58, 63 - KOMET 26 - MECTRON 8 - MEDESY 45 - METASYS 65 - MICRO MEGA 49 - MOCOM 71 - MORITA 29 - NISSIN 77 - Nobel Biocare 53 - NSK C1 - PHILIPS DENTAL 42 - PLANMECA 59 - POLYDENTIA 41 - SARATOGA 78 - SIRONA 21 - SOREDEX 50 - SULTAN 24 - ULTRADENT 12 - VITA 35 - VOCO 52 - W&H 19 - ZHERMACK 2 - ZIMMER 10
w w w . d e n t a l n e w s . c o mT e l : 9 6 1 - 3 - 3 0 3 0 4 8F a x : 9 6 1 - 1 - 3 8 4 6 5 7E m a i l : i n f o @ d e n t a l n e w s . c o mV o l u m e X V I I I , N u m b e r I V , 2 0 1 1w w w . f a c e b o o k . c o m / d e n t a l n e w s 1
Less paper for a sustainable
WORLDGet your Dental News copy
ONLINE!Do you feel concerned about the enviromental impact of the huge amounts of paper still being used in the vast majority of businesses, not least the publishing industry?Now there is something you can do: switch to Dental News from print to digital on www.dentalnews.com

ULTRADENT PRODUCES ITS UNITS IN MUNICH
UNDER GERMAN SUPERVISION. We are a family-
owned and operated company with traditional values
and the highest competency. The result: permanent
innovation.
ULTRADENT PREMIUM TREATMENT UNITS COMBINE
AESTHETICS AND FUNCTION FOR THE MOST
DEMANDING NEEDS: The U 1500 and U 5000 models
are ideal for your personal treatment concept.
IS THE ULTRADENT PREMIUM CLASS THE PERFECT
MATCH FOR YOUR PRACTICE? Your competent dealer
for dental products will be happy to assist you. We are
delighted about your interest!
YOUR NEW TREATMENT UNIT:
INSPIRED EXCLUSIVELY BY YOUR
PERSONAL DESIRES. The Ultradent Premium Class offers treatment
units that you can configure as individually
as your dream car. We are a modern dental
company that flexibly manufactures our prod-
ucts based on your needs. In Germany. With
outstanding quality. And absolute perfection.
We are the experienced partner of completely
satisfied dentists. Providing exceptional reli-
ability and intuitive operation. With the new-
est technologies and multimedia. Ultradent
Premium units will captivate you.
www.ultradent.de
Ask your
participating dealer
about our attractive
fall specials.
ut our attractive
fall specials.
Jae
ge
r &
Ta
len
te, M
un
ich

Dental News, Volume XVIII, Number IV, 2011
13
ORTHODONTICS
TREA
TMEN
T O
F AN
GLE
CLA
SS II
DIV
ISIO
N II
MAL
OCC
LUSI
ON
WIT
H DE
EP O
VERB
ITE
AbstractA 13 years old female presented in the late mixed dentition stage with a Class II division 2 incisor relationship on a moderate Class II skeletal base with average vertical proportions. The upper arch presented with mild crowding and retroclined central incisors. The lower arch was also mildly crowded with proclined labial segment. In occlusion, the overbite was deep and complete with scissor bite involving the upper and lower right 1st premolars. The treatment consisted of an initial sectional fixed appliance involving the upper labial segment followed by a Twin Block appliance. A subsequent second phase of upper and lower pre-adjusted edgewise fixed appliances were used on a non-extraction basis for definitive alignment, levelling and occlusal detailing. Retention consisted of removable upper and lower Essix retainers. Introduction A Class II incisor relationship is defined by the British Standards classification as being present when the lower incisor edges oc-clude posterior to the cingulum plateau of the upper incisors1. In Class II division 2 cases, the upper central incisors are retroclined and the overjet usually minimal but may be increased. Treat-ment of class II div 2 cases of growing patients with moderate to severe skeletal discrepancy usually involves proclination of the upper labial segment, converting the incisal relationship to a Class II division I malocclusion. Then the treatment is followed by a functional appliance phase to correct the sagittal discrepancy. The initial phase of proclination of the upper labial segment is achieved by one of the following methods:1- Expansion and Labial Segment Alignment Appliance (ELSAA) is the most commonly used. 2- Sectional fixed appliance treatment to the upper labial seg-ment only.3- Modified twin block appliance as demonstrated by Dyer and colleagues (2001) where they incorporated an anterior screw and torquing spurs in the twin block appliance for the upper
labial segment. This avoids the need for an initial upper labial segment alignment. The success of treating Class II division 2 incisor relationship depends on the correction of the transverse, anterior- posterior and vertical discrepancies. To achieve stability of the corrected malocclusion, it is important to correct the inter-incisal angle and edge centroid relationship3. Houston (1989) stated that it is essen-tial to reduce the inter-incisal angle towards 125 degrees, bringing the lower incisor tip anterior to the upper incisor centroid. The Twin Block was developed by Clark (1982) and has proved a popular and clinically successful appliance. The correction of the sagittal discrepancy is possible in many patients within 6-9 months. However, it requires patient co-operation and increased daily wear. The correction of the malocclusion is achieved by mandibular skeletal and dentoalveolar changes in addition to normal growth.
Case history A 13 year old female presented to the orthodontic department complaining of crooked upper front teeth. She was very motivated and had no medical condition contra-indicating the provision of orthodontic treatment.
Extra oral examination The patient presented with moderate class II skeletal pattern with average Frankfort-mandibular planes angle and lower anterior face height. The lips were competent with slightly high resting lower lip line, with average upper incisor show at rest and full crown show when smiling. The labiomental fold was prominent. Intra-oral examination The poor oral hygiene resulted in generalised gingivitis and de-calcification of the cervical margins of the upper labial segment. She was in the late mixed dentition stage with a Class II division 2 incisor relationship. All the permanent dentition was present except the unerupted lower second premolars and second molars with
Angle Class II division II
Dr. Kholood Al Foudari BDS
Treatment of
malocclusion with deep overbite

Dental News, Volume XVIII, Number IV, 2011
14
ORTHODONTICS
TREA
TMEN
T O
F AN
GLE
CLA
SS II
DIV
ISIO
N II
MAL
OCC
LUSI
ON
WIT
H DE
EP O
VERB
ITE
retained second deciduous molars. The upper arch presented with mild crowding and retroclined central incisors. The lower arch was also mildly crowded with proclined labial segment. In occlusion, the overbite was deep and traumatic to the upper palatal gingival tissues. There was also a scissor bite involving the upper and lower right 1st premolars. The overjet was 3 mm and upper and lower centre lines were coincident. The buccal segment relationship was class II bilaterally.
Radiographic assessment All the permenant teeth were present including the lower second premolars, lower second molars and all third molars as shown in the Dental Panoramic Tomogram (DPT). The upper standard occlusal view revealed normal morphology of the incisors roots and no supernumerary. The cephalometric analysis supports the clinical finding of a moderate Class II sagittal skeletal relationship
(ANB: 7°). Vertically, the lower face height is in the lower end of the normal range (53%) and the MMPA is increased (32°). Dentally, the upper incisors are retroclined to the maxillary plane (96°) while the lower incisors are proclined to the mandibular plane (105˚). The lower incisor edges lying posteriorly to the up-per root centroid (-1 mm).
Aetiology Mandibular retrognathia is the main aetiological , genetically in-herited, factor. It resulted in moderate Class II skeletal pattern with deep overbite. The lower lip line is slightly resting higher than normal which resulted in the retroclination of the upper central incisors.
Treatment aims and objectives 1- Improve the oral hygiene
Table 1: Cephalometric analysis pre-treatment
SNASNBANBUpper incisors to maxillary plane angle Lower incisor to mandibular plane angleInterincisal angle Maxillary mandibular planes angle Lower facial height %Lower incisor edge to upper root centroid
Pre-treatmentVariable Normal (SD)
79˚72˚7˚
96˚
105˚
126˚32˚
53%-1 mm
81 ± 378 ± 33 ± 2
108 ± 6
93 ± 6
133 ± 10 27 ± 3
55 ± 20-2mm
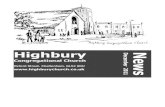
Fig. 2: Pre-treatment radiographs
Fig. 1: Pre-treatment extra oral and intra oral photographs

Dental News, Volume XVIII, Number IV, 2011
15
2- Decompensate upper incisors by proclination 3- Improve the facial profile by orthopaedic therapy 4- Align and level the arches5- Overbite correction6- Overjet reduction7- Arch coordination and occlusal detailing8- Achieve a Class I molar relationship9- Retention10- Monitor eruption of the unerupted teeth
Treatment plan1- Patient referral to school of hygiene for prevention advice
and oral hygiene instruction.2- Sectional fixed Preadjusted Edgewise appliance to procline
the upper labial segment3- Twin Block appliance4- Upper and lower Preadjusted Edgewise appliances with
an MBT prescription and an 0.022” x 0.030” slot 5- Retainers
Treatment rationaleUpper fixed sectional 3/3 and functional appliance therapy:To improve dento-facial aesthetics and occlusal relationships, the initial aim was to improve the sagittal skeletal discrepancy. The sectional fixed appliance encourages proclination of the upper labial segment. The principal advantage of the Twin block was to allow incisor and molar correction and upper arch expansion.
Fixed appliance therapy:A second phase of fixed appliance therapy was used to reduce the remaining overbite and to detail the occlusion. Bonding the lower second molars and the use of Class II inter-maxillary elas-tics were employed to facilitate overbite reduction. The increased lower incisor labial root torque of the MBT prescription will also help resist excessive proclination.
Treatment progress After the functional appliance stage, Cephalometric analysis shows that the sagittal skeletal relationship has improved slightly
ORTHODONTICS
TREA
TMEN
T O
F AN
GLE
CLA
SS II
DIV
ISIO
N II
MAL
OCC
LUSI
ON
WIT
H DE
EP O
VERB
ITE
Fig. 3: Clark Twin Block
Fig. 4: Photographs Post function-al appliance phase with sectional fixed appliance
Fig. 6: Fixed appliances stage
Table 2: Cephalometric analysis post functional applaince phase
SNASNBANBUpper incisors to maxillary plane angle Lower incisor to mandibular plane angleInterincisal angle Maxillary mandibular planes angle Lower facial height %Lower incisor edge to upper root centroid
During treatment
Variable Change during treatment
78˚74˚4˚
107˚
108˚
113˚32˚
53%+2 mm
-1+2-3
+11
+3
-13 0
0+3
Fig.5: Cephalomtric radiograph Post functioanl appliance phase superimposed with the initial cephalometric view. Note the resulted favourable mandibular growth (green tracing line)

Dental News, Volume XVIII, Number IV, 2011
16
TREA
TMEN
T O
F AN
GLE
CLA
SS II
DIV
ISIO
N II
MAL
OCC
LUSI
ON
WIT
H DE
EP O
VERB
ITE
ORTHODONTICS
(ANB: 4). Vertically, there has been no change in the skeletal relationships. There has been significant dento-alveolar changes; the upper incisor teeth have proclined (+11°) to a normal inclina-tion while the lower incisors have proclined but to a lesser extent (+3°; A-Po +2mm).
Treatment result The patient completed the treatment aged 14 years and 7 months. The malocclusion was treated satisfactory and the treat-ment aims were achieved. The functional appliance phase was successful in the improvement of the facial profile, reduction of the OJ, OB and the correction of the molar relationship.
Discussion The sectional fixed appliances allowed for the decompensation of the upper labial segment by proclination which facilitated the functional appliance phase.
The patient had a favourable growth pattern which contributed to the majority of the corrected malocclusion. The fixed appli-ance phase was indicated to detail the occlusion and to close the remaining lateral open bite post functional.
The lower labial segment was proclined at initial presentation. This happened naturally as an attempt to compensate for the underlying moderate Class II skeletal base. The inclination of the lower labial segment was maintained at the end of the treatment and that was achieved with the use of the fixed appliances with an MBT prescription (-6° torque for the lower labial segment).
The patient was provided with upper and lower Essix retainers for full time wear initially. The patient was advised about the late lower labial segment crowding and the importance of the long-term retention.
Conclusion The success of treatment of Class II div II cases with functional appliances depends on:1- Patients co-operation with appliance wear.2- Favourable mandibular growth. 3- Correction of the inter-incisal angle and edge centroid
relationship3,4
1- British Standard Institute. Glossary of Dental Terms 1983. BS9942; BSI London. 2- Dyer, F.M, Mckeown and H.F, Sandler, P.J. (2001) Journal of Orthodontics. 28: 271-2803- Houston, W. and Tulley, J. (1993) A textbook of orthodontics, Wright, Bristol 4- Houston, W. (1989) Incisor edge centroid relationship and overbite depth, Eu-ropean Journal of Orthodontics, 11: 139-1435- Clark, W.J. (1982) The Twin Bock traction technique, European Journal of Orthodontics, 4: 129-138
REFERENCES
Fig. 7: Post treatment extra oral and intra oral clinical photographs

DENTAL ANAESTHESIA
ARTINIBSA 4%
ARTINIBSA 4%
SCANDINIBSA 2% FORTE
SCANDINIBSA 3%
XILONIBSA 2%
XILONIBSA 10%
1:200.000
1:100.000
1:100.000
S/V
1:80.000
SPRAY
Visit us at:
EXPODENTAL Madrid (Spain), February 23-25, 2012.
IDEM Singapore, April 20-22, 2012. Hall 401-404, Stand no. C29
THE SPECIALIST IN

RUBBERDAMCLAMPS
ENDODONTIC INSTRUMENTS
©2011 Hu-Friedy Mfg. Co., LLC. All rights reserved.
For more information on our products please visit our website WWW.HU-FRIEDY.EUor contact us by e-mail: [email protected]
HIGH PERFORMANCE
REMARKABLE BALANCE
Hu-Friedy’s outstanding combination of advanced technology and innovative design gives practitioners clinical precision and efficiency for a flawless performance, every time.
Hu-Friedy’s superior standards for instrument quality and ongoing partnerships with industry thought leaders result in specialized instruments that help the endodontist perform with ever- increasing precision, efficiency and efficacy.
Hygiene must be the top priority
in your practice for the health of
your patients and assistants.
Our seamless and traceable
hygienic chain prevents infection
and protects both your assistants
and your patients by cleaning
instruments safely in the Hu-Friedy
instrument cassette. Unnecessary
handling is now in the past.
Hu-Friedy products are
individually handcrafted for high
performance and remarkable
balance.
Made from a specially blended
steel alloy for maximum durability
and resiliency, our instruments
have uniform tapers for smooth
condensing and spreading action
and exceptional strength through-
out the working ends.
Matte-finish Satin Steel clamps
reduce glare and improve field of
vision.
Our Satin Steel rubber dam clamps
are created with a very bright
beginning - each one is carefully
designed and handcrafted for
superior strength and corrosion
resistance. The dull, matte-finish
comes next.
How the best perform
INSTRUMENTMANAGEMENT

wh.com
With the new Implantmed you perform implant procedures with maximum
precision. The unit is easy to operate and guarantees longer working
without fatigue – thanks to the lightweight, yet powerful motor and the
ergonomically-shaped contra-angle handpiece. And the integrated
thread cutter function helps you with especially hard bone.
Behind every successful implantologist is an Implantmed
Scan the QR code withyour mobile telephone
for more information on Implantmed

Dental News, Volume XVIII, Number IV, 2011
20
PROSTHETIC DENTISTRY
FULL
ARC
H IM
PLA
NT
REC
ON
STRU
CTI
ON
OF
PATI
ENT
WIT
H C
OM
BIN
ATI
ON
SY
ND
ROM
E
Full Arch Implant Reconstruction of patient with Combination Syndrome:
A clinical Approach
Lack of equilibrium between opposite arches in edentulous patient leads sometimes to major problems related to occlusal planes. They can be left untreated or improperly treated. This article re-views one such problem known as Combination Syndrome. The treatment method described involves using a fixed mandibular prosthesis over implants that have been placed immediately after extraction.Rewarding outcomes depend on thorough evaluation and proper diagnosis of a patient’s oral condition. Once the starting point has been determined and the final outcome is designed, the treatment plan merely becomes the method of reaching the desired result.Kelly first described Combination Syndrome in 1972 as destructive changes in hard and soft tissues of patients with complete maxil-lary denture opposing an unstable bilateral free-end mandibular partial denture.1, 2 In different words, Combination Syndrome is a description of a dental condition that is the result of long term use of a few, usually6 remaining lower anterior teeth, #22-27 and a complete upper denture with no other natural remaining teeth and a lower free end Kennedy class I removable partial denture. The normal biting pressure or forces are directed from the remaining lowfrocks teeth and transmitted through the upper anterior denture, with resulting resorption of bone and slow auto-rotation & tilting of the denture upward and backward, with the upper anterior teeth becoming less visible and the upper posterior
teeth becoming more visible as the denture is rotated from func-tion with bone loss of the premaxilla.There may be seven characteristics associated with this syn-drome: 1. Bone loss in the premaxilla. 2. Dropping of the pos-terior maxilla (tuberosities). 3. Extrusion of the lower anterior teeth. 4. Posterior bone loss in the mandible under the RPD. and 5. Papillary hyperplasia of the maxilla. 6. Decreased Oc-clusal Vertical Dimension. and 7. Facial aesthetics often altered dramatically.If not corrected, the unstable occlusion can result in progressive posterior mandibular atrophy leading to greenstick fractures. The method of reestablishing a proper occlusal relationship is discussed in this article using a conventional maxillary denture and fixed mandibular implant restoration to correct the occlusal issues.
CASE REPORTSA healthy 54 year-old female patient presented with a complete maxillary conventional denture and class I Kennedy lower partial denture (Fig. 1). The mandibular residual ridge was shaped in the form of a knife edge and the tissue covering the edentulous ridge appeared loose. The buccal shelf areas were inadequate in size to provide the denture with support. The mandible showed extrusion of both the alveolar process and remaining dentition (Fig. 2). The maxilla showed enlarged tuberosity, atrophic pre maxilla, and Papillary hyperplasia on her hard palate (Fig. 3). A
Husain Ghadhanfari DDS, MS, Abdulaziz AlSanousi, Edward Monaco
Fig 2Fig 1

CAD/CAM SYSTEMS | INSTRUMENTS | HYGIENE SYSTEMS | TREATMENT CENTERS | IMAGING SYSTEMS
www.sirona.com
CEREC – PRECISION AND SIMPLICITY REDEFINED
Seeing CAD/CAMin a new light.The new CEREC AC with CEREC Bluecam captures highly detailed images using a powerful blue light-emitting diode (LED). Rapid, easy imaging results in a quantum leap in CAD/CAM precision[1], clinical reliability and effi ciency. Capture a quadrant in less than one minute. Create precise models and perfect restorations including long-term four unit temporary bridges with CEREC AC.Enjoy every day. With Sirona.
Sirona Dental Systems GmbHP. O. Box 21184DubaiTel. +971 4 375 2355
C-42
5-2K
-V0
[1] T
he re
sult
of a
stu
dy c
arrie
d ou
t by
Prof
esso
r Dr.
Meh
l (Zu
rich
Uni
vers
ity,
200
8): m
easu
ring
dept
h ac
cura
cy o
f up
to 1
9 µm
.

Dental News, Volume XVIII, Number IV, 2011
22
PROSTHETIC DENTISTRY
limited interarch space was evident at the approximate occlusal vertical dimension (Fig. 4). The patient desired restoration of her teeth within her budgetary limits, with a preference for a non-removable prosthesis of lower arch and more stable maxillary prosthesis, if possible. The treatment plan that was developed included a new upper denture opposing a fixed mandibular prosthesis.
Preoperative PlanningInitial treatment planning began with mounted study casts, pan-oramic radiographic film, cephalometric radiographic film, and intraoral photographs. The mandibular cast was duplicated and a diagnostic wax-up was fabricated to identify ideal implant sites. Two surgical templates were fabricated, one involving occlusal window to indicate approximate implant sites and another outlining the buccal limitations3 (Fig. 5, and 6). The mandibular cast was also used to fabricate an immediate complete lower denture.
Surgical phaseThe patient was required to have no food or fluids from midnight before surgery (NPO). The patient was given 0.5 mg sublingual triazolam 1 hour before surgery for sedative purposes. In addi-tion, amoxillin (antibiotic to prevent infections), dexamethasone (corticosteroid used to minimize postoperative swelling) and ibuprofen (nonsteroidal anti-inflammatory drug used to assist in preventing swelling as well as analgesia) were also adminis-tered 1 hour before surgery. The patient’s mouth and face were
scrubbed with chlorhexidine (0.12%). Bilateral inferior alveolar nerve blocks were given with 2% articaine (1:100,000 epinephrine) and local infiltration with 2% lidocaine (1:50,000 epinephrine) to assist with hemostasis. A midcrestal incision was made from the right distal first molar area to the left distal first molar area with midline vertical releasing incision. A full-thickness buccal flap was reflected and tied back to the vestibule using 2-0 silk suture material. The surgical template was inserted to mark the locations on the alveolar crest. The remaining teeth were extracted, and an alveoplasty was performed on the anterior undercuts of the buccal aspect of the ridge to level the extruded segment (Fig. 7). The template was inserted again to prepare the osteot-omy within the buccal confines of the template. Teeth # 34(21), 33(22), 41(25), 43(27) and 44(28) sites were prepared for a 3.5 mm X 10.0 mm (Nobel Direct Groovy, Nobel Biocare) endosteal root form implant and inserted. Healing caps were placed. An Amalgam tattoo at Site no. 4327 was removed using a round bur. The resulting defect was filled with a demineralized freeze-dried bone allograft (DFDBA) (Puros, Zimmer Dental, CA, USA) and covered with a collagen membrane (BioMend, Zimmer Dental, CA, USA).Flap margins were trimmed with scissors to allow primary closure with no redundant tissue. Flaps were reapproximated using 3-0 Vicryl (Johnson & Johnson, Somerville, NJ) in an interrupted and continuous manner. The immediate complete lower denture was relined using CoeSoft tissue conditioner (GC America, Alsip, IL). Ice packs were given to the patient and postoperative toons
FULL
ARC
H IM
PLA
NT
REC
ON
STRU
CTI
ON
OF
PATI
ENT
WIT
H C
OM
BIN
ATI
ON
SY
ND
ROM
E
Fig 3
Fig 5
Fig 4
Fig 6

Dental News, Volume XVIII, Number IV, 2011
23
PROSTHETIC DENTISTRY
were reviewed.Sutures were removed 2 weeks postsurgically, and the immediate lower denture was once again relined using soft chairside liner (GC America, Alsip, IL).
Prosthetic phaseThe patient was instructed not to wear the upper denture for 24 hours before this appointment to permit tissue relaxation.4-6 A final impression of the maxilla using a custom tray and polyvinyl-siloxane was made. Two months later, the patient received a final impression of the implants using impression pick up technique, a custom tray, and polyvinylsiloxane. The midline, incisal edge position, occlusal plane, buccal lip support, and anterior segment were indicated on the acrylic maxillary base and wax rim. Mandibular record base and wax rim was used with the aid of modified temporary abutment to secure the acrylic base for vertical dimension and bite registration record.Temporary Abutments were used on the master cast to wax up the mandibular framework (Fig. 8). Completed framework wax up was sent to be scanned and a milled titanium framework to be fabricated. The milled titanium framework (NobelProcera Implant titanium bridge, Nobel Biocare, NJ) tried in the patient mouth for passive fitness (Fig. 9). Final try-in of the maxillary denture with teeth set in wax was made against mandibular denture teeth try-in set over the tita-nium framework. The occlusal plane (Curve of Spee and Curve
of Wilson) was developed on the mandibular try-in hybrid den-ture using a Circular setup template. This plate is set against the occlusal surfaces of the mandibular teeth and is based on a 3-inch Sphere.Denture teeth were set in a medial-positioned lingualized occlusion. Misch proposed this occlusal design, which is a modification of the occlusal scheme first developed by Payne and Pound. Only the lingual cusps of the maxillary posterior teeth are in contact with the central fossa during centric occlusion. The mandibular molar cusps are positioned medial to a line drawn from the mesial of the canine to the lingual aspect of the retromolar pad.7 The mandibular prosthesis was created in 1 piece with Procera milled titanium framework. The mandibular implants were placed with-in mental foramen area to accommodate mandibular flexure and limit torsion on the implants.8, 9
After esthetics, occlusion, phonetics, and comfort were evalu-ated both dentures were processed in heat-cured acrylic and delivered at the same appointment (Fig. 10).10 Verification of abutments being seated required periapical films. The implant abutments were then torque to 30 Ncm. Cotton was placed over the abutment screws and sealed with Fermit-N (Vivadent, Schaan, Liechtenstein).Final panoramic (Fig. 11) was taken to verify baseline crestal bone levels.The patient was recalled two weeks post delivery to evaluate the occlusion, oral hygiene, and soft tissue.
FULL
ARC
H IM
PLA
NT
REC
ON
STRU
CTI
ON
OF
PATI
ENT
WIT
H C
OM
BIN
ATI
ON
SY
ND
ROM
E
Fig 7
Fig 9
Fig 8
Fig 10

Beauty. Versatility.Performance.
VersaCOMP™
Flowable CompositeVersaCOMP™
Universal Total Etch AdhesiveVersaCOMP™
Universal Hybrid Composite
Sultan Healthcare introduces VersaCOMP™, a complete line of
restorative materials that offers easy handling, versatility and
clinical performance…all at a great price. The result is the
ideal combination of performance and value.
BEFORE AFTER
INTRODUCING

Dental News, Volume XVIII, Number IV, 2011
25
PROSTHETIC DENTISTRY
Discussion Combination Syndrome is an aggressive occlusal problem that slowly develops over time. Once detected, treatment options are evaluated. Different treatment approaches should be suggested for a patient with Combination Syndrome. The choice of treat-ment ultimately depends on the patient, the amount of time and money she is willing to spend for the treatment, her oral condition and her desire for fixed or removable prosthesis. These options must resolve the problems of function, esthetics, and patient desires, as well as economics. To fulfill these requirements, 2 types of prostheses are available: conventional denture or an implant-retained prosthesis. The use of a conventional denture in restoring the mandibular dentition provides the least patient satisfaction as compared with a fixed prosthesis. For this reason, the patient elected to have the mandibular rehabilitation with an
implant-retained prosthesis. The maxillary dentition was restored with a conventional denture because the patient had been wear-ing, had tolerated, and had accepted a complete denture. Also, both esthetics and economics were easily managed with this prosthesis.Post treatment maintenance recalls appointments are essential to assure denture stability, proper occlusal scheme, and mainte-nance of posterior support and vertical dimension of occlusion. The patient should be recalled on 3 months, 6 months, and 12 months intervals during the first year to observe any changes in posterior support. If acrylic tooth wear and support are lost in the posterior regions, accelerated premaxilla atrophy will develop from excessive forces. Bilateral balanced occlusion is essential for long-term success.This case study deals with treatment of Combination Syndrome. Understanding the cause can assist the practitioner in preventing further residual ridge deterioration.
Conclusion The assessment of the risk of developing the combination syndrome depends on past dental history, the condition of the remaining mandibular anterior teeth, and posterior lack of occlusal support. The dentist should study the case carefully in order to assure the irreversibility of this syndrome. Implants provide a predictable method of tooth replacement offering excellent functional and esthetic benefits. Like with any complicated treatment, thorough diagnosis, planning, and implementation of treatment will result in an outstanding outcome for both the patient and dentist.
Fig 5
1. Kelly E. Changes caused by a mandibular removable partial denture opposing a maxillary complete denture. J Prosthet Dent. 1972;27:140–150.2. Saunders TR, Gillis RE, Desjardins RP. The maxillary complete denture oppos-ing the mandibular bilateral distal extension partial denture. Treatment consider-ations. J Prosthet Dent. 1979;41:124–128.3. Cabianca M. Surgical template fabrication and utilization involving steel tubes. Int Magazine Oral Implantology. 2001;2: 31–35.4. Zarb GA, et al. Boucher’s Prosthodontic Treatment for Edentulous Patients,10th ed. St. Louis: Mosby; 1990: 174.5. Lytle RB. Management of abused oral tissues in complete denture construction. J Prosthet Dent. 1957;7:27–42.
6. Kydd WL, Colin HD. The biological and mechanical effects of stress on oral mucosa. J Prosthet Dent. 1982;47:317–329.7. Misch CE. Maxillary denture opposing an implant prosthesis. In: Misch CE, ed. Contemporary Implant Dentistry, 2nd ed. St. Louis: Mosby; 1999:639–644.8. Misch CE. Diagnostic casts, preimplant prosthodontics, treatment prostheses, and surgical templates. In: Misch CE, ed. Contemporary Implant Dentistry, 2nd ed. St. Louis: Mosby; 1999:143–144.9. Goodkind RJ, Heringlake CB. Mandibular flexure in opening and closure move-ments. J Prosthet Dent. 1973;30: 134–138.10. Zarb GA, et al. Boucher’s Prosthodontic Treatment for Edentulous Patients, 10th ed. St. Louis: Mosby; 1990: 400–405.
REFERENCES
FULL
ARC
H IM
PLA
NT
REC
ON
STRU
CTI
ON
OF
PATI
ENT
WIT
H C
OM
BIN
ATI
ON
SY
ND
ROM
E

Small bur, big effect
© 1
0/20
10 ·
BRA/
0 · 4
0532
7V0
GEBR. BRASSELER GmbH & Co. KG · Germany Phone +49 (0) 5261 701-0 · www.brasseler.de
Quality pays off
Round, high-efficiency endodontic bur H1SML for preparing isthmuses
The H1SML is our specialist bur for the prepara-tion of isthmuses. Its particularly sharp working part guarantees efficient preparation during the treatment. Thanks to its long, slim neck, even deep operative sites close to the pulp can be reached with ease. What’s more, the H1SML allows permanent visual control during the preparation to guarantee maximum safety at all times. The H1SML is available in different sizes to suit the morphology of any tooth. All root canals – even initially hidden ones – can be located without problems thanks to the H1SML. Don’t just take our word for it – talk to your Komet representative who will be pleased to give you all the details.
H1SM
L.20
5.00
8
H1SM
L.20
5.01
0

AssuranceInvest in reliability. Focus on the patient.Express your style. From the people who build the most dependable dental equipment in the world, A-dec 200™ provides you with a complete system to secure a successful future.
Discover how you can gain assurance with A-dec 200. Contact your authorised A-dec dealer today.
Discover A-dec 200. Contact your local dealer.
A-dec Inc.2601 Crestview Drive, Newberg, Oregon 97132 USAwww.a-dec.com
visit A-dec at AEEDCstand 230


Dental News, Volume XVIII, Number IV, 2011

Dental News, Volume XVIII, Number IV, 2011
30
IMPLANT DENTISTRY
SHO
ULD
BIO
-OSS
BE
USE
D A
S A
N O
NLA
Y B
ON
E SU
BSTI
TUTE
Often times, dental implant placement is complicated by inad-equacy of bone volume due to tooth loss, periodontal disease, pathology, or trauma. However, more challenging implant cases are being performed due to the advancement in bone augmen-tation procedures and materials to augment deficient alveolar bone.1
Autogenous bone is considered to be the “gold standard”, for alveolar ridge regeneration, due to its osteogenicity.1,2 Howev-er, autogenous bone grafts are associated with rapid rate of resorption3 and donor site morbidity.1 This has led scientists to investigate allogenic and xenogenic bone grafts, as well as allo-plastic materials, such as Hydroxyapatite and Calcium Phosphate Compounds.4
An alternative to autogenous bone is xenograft. Although xeno-grafts have provided acceptable results, they are considered to be inferior in bone generation potential when compared to au-tografts. However, the supply of xenograft is unlimited. Xenografts are usually derived from bovine origin.5
Bio-Oss® (Geistlich Pharmaceutical, Walhusen, Switzerland) is a natural bovine bone derivative that lacks the organic component.6 Bio-Oss® and mineralized human bone are similar in their chemi-cal and morphological structures.2 Bio-Oss® granules are 0.25 to 1.00 mm in diameter.6 Due to its porous structure, Bio-Oss® occupies 25-30% of the defect space initially.7 This facilitates angiogenesis (penetration of the bone augmentation material by blood vessels) and osteoblast migration.8
Along with all of its potential properties, the osteoconductive nature of Bio-Oss® when used as an onlay graft is not well established. The Osteoconductivity of Bio-Oss® has been a topic of debate in the literature.
It is well known that an onlay bone graft is more challenging to maintain clinically than an inlay bone graft. Rosenthal et al. dem-onstrated that onlay bone grafts showed resorption with time,
while inlay bone grafts showed increased volumes overtime.9 In-creased bone to bone contact between the inlay bone graft and the native bone is one explanation to this difference. Another explanation is the fact that inlay bone grafts are surrounded by biological boundaries. This shields them from recoil forces of the surrounding soft tissue. In addition, inlay bone grafts receive identical physical stresses to those received by the surrounding bone.9
Some studies described Bio-Oss® as having osteoconductive properties. In an experiment involving the skull of the rabbit, us-ing histomorphometric analysis, Slotte et al. examined the bone formation in titanium cylinders filled with either autogenous bone or Bio-Oss® as compared to empty titanium cylinders as controls. Significantly more bone tissue was found in the two test groups than the control group.10
Other studies claimed that Bio-Oss® is not osteoconductive when used as an onlay. In an experiment involving the skull of the rat, Slotte and Lundgren studied, histomorphometrically, the bone generation potential of silicone domes grafted with Bio-Oss® compared to empty ones.11 The study demonstrated that Bio-Oss® arrested bone formation.
In two different studies using the mandible of the rat, Stavro-poulos et al. studied the amount of bone generation in Teflon capsules grafted with Bio-Oss® as compared to empty (control) capsules. The capsules were fixed to the mandible using suture material. In both experiments, it was shown that Bio-Oss® had an inhibitory effect on bone formation.12,13
Such results and the results of other studies have led some authors to suggest that dental implant survival in grafted sites may be owed mainly to the function of the native bone rather than the bone graft itself.14
SHOULD BIO-OSS BE USED AS AN ONLAY BONE SUBSTITUTE?Abdullah Al-Harkan DMD, MSc, FRCD (C)
Department of Oral and Maxillofacial Surgery, Farwaniya Hospital, Ministry of Health, Kuwait - [email protected]


IMPLANT DENTISTRY
Araújo et al. found that Bio-Oss® resulted in less bone generation than autogenous bone when used as an onlay in dogs’ mandibles.15 However, they found that Bio-Oss® maintained more volume than autogenous bone did. Due to this fact, some authors sug-gested the use of Bio-Oss® mainly to preserve the architecture of the soft tissue.16
From the discussion above, in my opinion, the use of Bio-Oss® an onlay bone substitute may not have a significant value in bone generation potential, but it may add some value to the way it supports the soft tissue profile. This feature may give the implant a better esthetic outcome.
1- Norton M, Odell EW, Thompson ID, Cook RJ. Efficacy of bovine bone mineral for alveolar augmentation: a human histologic study. Clinical Oral Implant Re-search. 2003; 14: 775-7832- Ewers R, Goriwoda W, Schopper C, Moser D, Spassova E. Histologic findings at augmented bone areas supplied with different bone substitute materials com-bined with sinus floor lifting. Report of one case. Clinical Implant Research. 2004; 15: 96-100.3- Johansson, B., Grepe, A., Wannfors, K. & Hirsch, J-M. (2001) A clinical study of changes in the volume of bone grafts in the atrophic maxilla. Dentomaxillofacial Radiology 30: 157-161.4- Hämmerle, C.H., Chiantella, G.C., Karring, T. & Lang, N.P. (1998) The effect of a deproteinized bovine bone mineral on bone regeneration around titanium dental implants. Clinical Oral Implants Research 3: 151-162.5- Tuominen, T., Jäsmä, T., Tuukkanen, J., Marttinen, A., Lindholm, T.S. & Jalovaara, P. (2001) Bovine bone implant with bovine bone morphogenetic protein in healing a canine ulnar defect. International Orthopaedics 25(1): 5-8.6- Hising, P., Bolin, A. & Branting, C. (2001) Reconstruction of severely resorbed alveolar ridge crests with dental implants using a bovine bone mineral for augmen-tation. The International Journal of Oral & Maxillofacial Implants 16(1): 90-97. 7- Peetz, M (1997) Characterization of xenogenic bone material. In: Boyne, P.J., ed. Osseous reconstruction of the maxilla and the mandible – surgical techniques using titanium mesh and bone mineral, 87-100. Chicago, Berlin: Quintessence.8- Yildirim M, Spiekermann H, Biesterfeld S, Edelhoff D. Maxillary sinus augmen-tation using xenogenic bone substitute material Bio-Oss® in combination with venous blood. A histologic and histomorphometric study in humans. Clinical Oral Implant Research 2000: 11:217-229
9- Rosenthal, A.H. and S.R. Buchman, Volume maintenance of inlay bone grafts in the craniofacial skeleton. Plastic and reconstructiove surgey, 2003. 112(3) p.802811.10- Slotte C, Lundgren D, Burgos PM. Placement of autogenic bone chips or bo-vine bone mineral in guided bone augmentation: A rabbit skull study. The Interna-tional Journal of Oral & Maxillofacial implants, 2003; 18: 795-80611- Slotte C, Lundgren D. Augmentation of calvarial tissue using non-permeable silicone domes and bovine bone mineral. An experimental study in the rat. Clinical Oral Implant Research 1999: 10: 468-47612- Stavropoulos A, Kostopoulos L, Mardas N, Nyengaard JR, Karring T. Depro-teinized bovine bone used as an adjunct to guided bone augmentation (GBA) An experimental study in the rat. Clinical Implant Dentistry and Related Research, 2001a; 3: 156-16513- Stavropoulos A, Kostopoulos L, Nyengaard J R, Karring T. Deproteinized bo-vine bone (Bio-Oss®) and bioactive glass (Biogran®) arrest bone formation when used as an adjunct to guided tissue regeneration (GTR). An experimental study in the rat. Journal of Clinical Periodontology 2003; 30: 636-64314- Aghaloo TL, Moy PK, Which hard tissue augmentation techniques are the most successful in furnishing bony support for implant placement? Int J Oral Max-illofac Implants. 2007; 22 Suppl:49-70.15- Araújo MG, Sonohara M, Hayacibara R, Cardaropoli G, Lindhe J, Lateral ridge augmentation by the use of grafts comprised of autologous bone or a biomate-rial. An experiment in the dog. J Clin Periodontol. 2002 Dec; 29(12):1122-31.16- Schlee M, Esposito M, Aesthetic and patient preference using a bone substi-tute to preserve extraction sockets under pontics. A cross-sectional survey. Eur J Oral Implantol. 2009 Autumn; 2(3):209-17.
REFERENCES
www.intensiv.ch
Constant Superior Quality
Intensiv SA6926 MontagnolaSwitzerland
Intensiv representativefor Gulf and Middle East:Mr. Imad [email protected]. +961 3 288367
Tel. + 41 91 986 50 50Fax + 41 91 986 50 [email protected]


Dental News, Volume XVIII, Number IV, 2011
34
PEDIATRIC DENTISTRY
PARE
NTA
L SE
PAR
ATI
ON
TEC
HN
IQU
E D
URI
NG
DEN
TAL
CA
RE F
OR
CH
ILD
REN
IN K
UW
AIT
Key Words: Parental separation. Behavior management. Pediatric dentists.
AbstractObjective: The aim of this study was to explore the preference of parents and dentists as regards parental presence/absence in a dental clinic during a child’s dental treatment in Kuwait. Methods: Two hundred and twenty seven subjects were includ-ed in this prospective study. The subjects comprised two groups, Group I included parents of 152 child-patients, and Group II, 75 dental care providers (pediatric dentists and general practitioners). The data was collected on a pre-designed questionnaire, which included demographic variables on child-patients and parents, as well as their preference to remain inside or outside the clinic. The dentist’s opinion on this matter was also obtained. Results: Results showed a general preference of parents for being with the child during treatment, a decline was observed with the increasing birth order of child (p<0.046), as well as increasing parental age (p<0.022). This preference was found to be the same between mothers and fathers (p 0.923). Logistic regression anal-ysis revealed that only dental specialty was a significant factor (p<0.013) among dentists. Pediatric dentists’ preference on pa-rental presence was seven times higher than general practitioners (OR = 7.2, CI=1.5-34.8). Also, 115 (76%) parents preferred to be with their child during treatment, as compared to 28 (37%) dentists favoring parental presence (p<0.001; OR=5.2, CI=2.9-9.5). Conclusion: A statistically significant relation was found in terms of parents’ preference, whether to be inside or outside the clinic during their child’s dental treatment, child’s birth order, and age of the parent. Pediatric dentists showed an overall pref-erence towards a parent’s presence inside the clinic during the child’s dental treatment. A majority of general dentists did not prefer parental presence in the clinic.
IntroductionFor children’s treatment, it is essential to have good behav-ioral management techniques, and one of these techniques is to separate the parents from the child(1,2,3). Unfortunately, separation anxiety is a common problem in pediatric dentistry, especially with younger children(4). Many studies tend to sup-port the presence of parents in dental clinic due to the reported augmentation of negative behavior of children when separated from their parents(5-11). Also, an overall increasing preference was observed among pediatric dentists towards parental participation in the clinic during child’s treatment(4). A majority of parents stated that they themselves would feel better if they stayed in the clinic with their child, as this practice would increase the child’s cooperation(9,12,13). However, some studies have reported that a majority of dentists do not prefer parental presence in the dental clinic during their child’s treatment(5,6). Traditionaly, dentists in Kuwait excluded parents from the dental clinic, to help in the elimination of many of the child’s behavior problems. Some dental clinics in Kuwait have this practice as a matter of policy. Kamp had noted that parents’ exclusion from the den-tal clinic was part of the routine pediatric treatment by many practitioners(12). Excluding parents from the clinic was favored by many dentists as they thought that this technique would re-duce conflicts of authority and a child’s negative behaviors(5,12,14). Another reason, reportedly preferring the separation technique, was that some dentists felt uncomfortable using a number of behavior management techniques, especially more advanced behavior management techniques, in parents presence(4,14). Also documented is the parent’s anxiety having a big effect on child’s behavior during dental visit(1,15). While parents have been shown to be more anxious, their presence reportedly resulted in a more apprehensive behavior from their children(16,17). However, there are many reports that found no statistically significant difference
Preference of Parents and Dentists in Using
Parental Separation Techniqueduring Dental Care for Children in KuwaitNourah S. Al-Maheemid, BDS - Mohammad A. Hasan, BA/DDS. MS - Prem N. Sharma, Abdulaziz A. Hasan, BA/DDS. MS.

Find the correct centric quickly and precisely with the new "Multi Functional Teeth"VITA MFT® – no simpler way to set up teeth!
provides ideal static alignment plus many other beneficial fea-
tures. VITA MFT are universally applicable, highly esthetic and
suitable for every indication. The compact shade and mould
assortment is a further guarantee for optimum productivity.
What an attractive prospect! / www.vita-zahnfabrik.com
Simply no-one can resist VITA MFT. Thanks to the 'easy-centric®'
setup concept, even those new to setting up acrylic denture
teeth can achieve optimum occlusion almost automatically –
thanks to their pre-abraded occlusal wear facets that minimize
the horizontal shear forces, their specially molded cusps which
3365
E
VITA shade, VITA made.

Dental News, Volume XVIII, Number IV, 2011
36
PEDIATRIC DENTISTRY
PARE
NTA
L SE
PARA
TIO
N T
ECHN
IQUE
DUR
ING
DEN
TAL
CARE
FO
R CH
ILDR
EN IN
KUW
AIT
between the behavior of children who are separated from their parents, as compared to the behavior of children who are not separated(5,8,15,18,19).Two factors are important and should be considered in the deci-sion concerning inclusion or exclusion of parents during dental treatment: (1) Parental preference, and (2) Dentist preference/office policy(6).A cross-sectional study was designed to study parental and den-tists’ preferences in this regard, in the context of dental clinics in Kuwait. The objective of this study was to explore the preferences of parents and dentists concerning parental presence in a dental clinic during a child’s dental treatment in Kuwait.
Subjects and MethodsThe study was conducted at the: (1) Faculty of Dentistry, Kuwait University, (2) Specialty dental centers at Ministry of Health (Al-Amiri, Benaid Al-Gar, Al-Farwaniya, Al-Jahra), which included multiple pediatric, orthodontic and emergency clinics, and (3) four polyclinics (general dentistry) in the same residential areas as the specialty dental centers. The study was conducted in two groups. Group 1, comprised of 152 children and their parents. These subjects included all parents who accompanied their children to the dental clinic at the specialty dental centers or polyclinics, from 9 a.m. to 10 a.m., during a period of one week. Group 2 consisted of 75 dentists, including 26 pediatric dentists (total number of pediatric dentists in Kuwait at the time of the study), and 49 general dentists (total number of general dentists in the dental centers, where the study was conducted). A pre-designed, close-ended questionnaire was used for data collection. Demographic data on the subjects in Group 1, included child’s age, gender and his/her birth order in the family. Information obtained from the accompanying parent were; age, gender, education level, and their preference to remain inside or outside the clinic, during a child’s dental treatment in normal situations (routine dental visit during normal working hours). Subjects in Group 2, were the dentists, who completed a different
closed-ended questionnaire, that consisted information on their clinic, specialty, age, gender, year of graduation, as well as their preference regarding parent’s presence or absence in the clinic during a child’s dental treatment. All dentists responded to the questions in the survey. For the purpose of this study, all subjects, in both groups (parents and dentists) participated in this blind cross-sectional survey.Statistical software, Statistical Package for Social Sciences (SPSS) version 15.0 was used for data management, analysis and pre-sentation of results. Descriptive statistics have been presented as number, percentages, mean ±standard deviation (SD), and range. Normality of data distribution was ascertained with Kolmogorov-Smirnov test. The association of different characteristics with parents’ or dentists’ preferences was assessed with Chi-square or Fisher’s test. Mean ages were compared with Mann-Whitney nonparametric test. Logistic regression was applied to find the factors influencing the preference of parents being inside the clinic during a child’s treatment. Odds ratio (OR) and 95% confidence interval (CI) were computed. A probability value (p < 0.05) was considered significant at two-tailed level.
ResultsAll 227 subjects, 152 parents and 75 dentists, included in the study, completed the questionnaire with a response rate of 100 percent. In Group I, the mean age of child-patients was 4.7 years, ranging between 2 to 10 years, with male to female ratio of 1.2 :1 (Table1). No significant difference was observed between mean ages of male and female child-patients (4.68±1.42 vs 4.73±1.89, p=0.454). Parents, whether mother or father, in almost equal number, accompanied the children. Parents mean age was 35.2 years, ranging between 21 to 56 years, though fathers had significantly higher mean age (37 years) as compared to mothers, (33 years); ( 37.2±6.4 vs 33.0±5.9; p<0.001). More than half of the parents, 87 (57.2%) had university education, followed by secondary (30.3%) and primary (12.5%).Three-quarters, 115 (75.7%) of parents preferred to remain inside the dental clinic during their child’s treatment, while re-maining 37 (24.3%) either preferred to remain outside (6.6%), with their preference depending on treatment (9.2%), or did not have any preference of being inside or outside the clinic (8.5%)
Table 1 Demographic characteristics of child-patients and their accom-panying parents to the dental clinic (N=152)
Fig 1 Parents’ preference to be inside or outside the dental clinic dur-ing their child’s treatment (N=152)

Create æ-motion with flowables from GC. G-ænial Flo & Universal Flo
Handles like a flowable – Performs like a restorative.

Dental News, Volume XVIII, Number IV, 2011
38
PARE
NTA
L SE
PARA
TIO
N T
ECHN
IQUE
DUR
ING
DEN
TAL
CARE
FO
R CH
ILDR
EN IN
KUW
AIT
PEDIATRIC DENTISTRY
Majority of children 118 (77.6%) were in the age-group (4-6) years, while 20 (13.2%) were three years and below, and 14 (9.2%) were above 6 years (Table 2). A declining trend was observed as regards parents preference for being inside with re-spect to a child’s increasing age, though this was not significant (p<0.558). No significant difference was observed with regard to child’s gender. Chi-square for trend showed a significant declining trend in parent’s preference to remain inside with in-creasing child’s birth order (p<0.045). Similar trend was noticed with regard to increasing age of parents (p<0.022). However, parental preference was found to be same between mothers (76%) and fathers (75.3%), (p=0.923). Parental education did not show any difference in their preferences to be inside the clinic (p<0.882) In Group II, 75 dentists (49 general and 26 pediatric dentists) recorded their opinion about the presence or absence of parents during dental treatment of children (Table 3). More than half of the dentists, 41 (54.7%) were in the age-group (20-29) years, with mean age 32.2 (± 9.4) years ranging between 22 to 54 years. The mean age for pediatric dentists was significantly higher than general practitioners (40.2±8.4 vs 28.0±7.0, p<0.001). Gender-wise, there were 46 females (61.3%) with a mean age of 30.9 (± 9.7) years, and 29 males (38.7%) with mean age 34.3 (± 8.8); p<0.049. Fifty-six percent of the dentists graduated in the year 2000, or after. As regards dentist’s opinion on parents being inside or outside the clinic, 69.2% pediatric dentists preferred parents presence in the clinic as compared to general
practitioners (20.4%), p<0.001. All pediatric dentists were in fa-vor of parents’ presence during a child’s first visit. There was a significant association with dentists increasing age and parent’s presence in the clinic (p<0.01). Also, significantly higher prefer-ence for parental participation was observed among dentists, who graduated before the year 2000 (p< 0.005). However, on logistic regression analysis, only specialty was found to be a sig-nificant factor (p<0.013), where pediatric dentists’ preference on parental presence was seven times higher than general prac-titioners (OR = 7.2, CI=1.5-34.8).In Group I and Group II, 115 (76%) parents preferred to be with their child during treatment as compared to 28 (37%) dentists (pediatric dentists and general practitioners), who favored parental presence (p<0.001; OR=5.2, CI=2.9-9.5).
DiscussionThis study demonstrated that a majority of parents (75.7%) pre-ferred to stay inside the dental clinic during their child’s treatment. Although, the data showed that this preference increased especially when children were 5 years of age or younger, the association be-tween the parental preference and the age of the child was not statistically significant (p<0.558). This suggests that the age of the child patient was not the most important factor that deter-mined the decision of parents to be inside or outside the clinic, as suggested by other studies(4,6). Another finding of this study was the statistically significant relation concerning the parents’ preference, whether to be inside or outside the clinic during their child’s dental treatment, child’s birth order, and age of the parent. Parents’ preference to remain inside the clinic with their child decreased with increasing child’s birth order (p<0.045).
Table 2 General characteristics of child-patients and their accompany-ing parents to the dental clinic according to parental preference on remaining inside or outside the clinic duting child’s treatment
Table 3 Dentist’s characteristics and their perception on parent’s presence inside or outside the clinic during child’s treatment

For better dentistry
Smart Dentin Replacement
24 Month Clinical Trial ResultsPrincipal Investigators: Dr. J. Burgess and Dr. C. Munoz2PPPPPPPPPP
NEW
I I I I II I II I I

Dental News, Volume XVIII, Number IV, 2011
40
PARE
NTA
L SE
PARA
TIO
N T
ECHN
IQUE
DUR
ING
DEN
TAL
CARE
FO
R CH
ILDR
EN IN
KUW
AIT
PEDIATRIC DENTISTRY
Also, this preference decreased with increasing age of parents (p<0.022). Parents who preferred to stay inside the dental clinic with their children reported that the reasons behind this choice were to reduce parental and children’s anxiety and increase the comfort level. This tended to increase parents’ satisfaction, and improved the overall child’s dental experience. There was no significant effect of parents’ gender or level of education.The only statistically significant relation in Group II was found between the opinions of dentists’ for having the parents inside or outside the dental clinic during a child’s treatment and the dental specialty. Most pediatric dentists (69%) showed an over-all preference towards parental presence inside the clinic during the child’s dental treatment, regardless of the child’s age, gender, or behavior. Pediatric dentists felt more comfortable having the parents inside the clinic for many reasons, but mainly, as indicated by most pediatric dentists in this study, was to allow the parents to observe the management techniques utilized by dentists. This was especially true for pediatric dentist; if it was the child’s first visit to the dentist (100% of pediatric dentists preferred the parents to stay inside the clinic during the child’s first dental visit). Many parents in other studies also preferred to be with their children in the dental clinic during the initial visit(12,14).On the other hand, most general practitioners (79.6%), in this study, preferred to exclude the parents from the clinic during the dental treatment of their children. The reason, as indicated by the general practitioners, was to eliminate many of the child’s
behavioral problems, a reason reportedly given by other dentists in some other studies(12,20).The authors of this study recognize that future studies are needed, giving consideration to parental preference concerning the type of dental procedure (initial, follow-up, restorative, surgical or emergency). Also, considerations need to be given to whether the parents remain in or out of the operatory, while collecting the data for future studies.
ConclusionThis study demonstrated that parental preference to stay inside or outside the dental clinic during their child’s treatment signifi-cantly depended on the child’s birth order and the parent’s age. Pediatric dentists’ preference on parental presence was seven times higher than general practitioners. This preference by pe-diatric dentists increased especially if it was the child’s first visit. Based on the findings of the study, it is recommended that the dentists may need to include parents in making the decision of using the parental separation technique. Pediatric dentists also need to report to general practitioners about the rationale be-hind their preference to include the parents in the dental clinic during their child’s treatment.
AcknowledgmentThe authors would like to thank Dr. Muawia Qudiemat for his help and support during this study.
1. Crossley M, Joshi G. An investigation of paediatric dentists’ attitudes towards parental accompaniment and behavioral management techniques in the UK. BDJ 2002; 192:517-21.2. Harrell S. Managing slightly uncooperative pediatric patients. JADA 2003; 134:1613-4. 3. Havelka C, McTigue D, Wilson S, Odom J. The influence of social status and prior explanation on parental attitudes toward behavior management techniques. Pediatr Dent 1992; 14:376-81.4. Guthrie A. Separation anxiety: an overview. Pediatr Dent 1997; 19:486-90.5. Crowley E, Whelton H, O’Mullane D, Cronin M, Kelleher V, Flannery E. Parent’s preference as to whether they would like to accompany their child when receiv-ing dental treatment – results from a national survey. J Irish Dent Assoc 2005; 51:23-4.6. Arathi R, Ashwini R, Mangalore. Parental presence in the dental operatory – parent’s point of view. J Indian Soc Pedo Prev Dent 1999; 17:150-5.7. Frankl S, Shiere R, Fogels H. Should the parent remain with the child in the dental operatory. J Dent Child 1962; 29: 150-63.8. Fenlon W, Dabbs A, Curzon M. Parental presence during treatment of the child patient: a study with British parents. Br Dent J 1993; 174:23-8.9. Peretz B, Zadik D. Parent’s attitudes toward behavior management techniques during dental treatment. Ped Dent 1999; 21:201-4.10. Molinari G, DeYoug A. Parental Presence and Absence as a Behavior Manage-ment Technique. J Michigan Dent. Assoc 2004; 86:30-3.
11. Marzo G, Campanella V, Albani F, Gallusi G. Psychological aspects in paediat-ric dentistry: parental presence. E J Ped. dent 2003; 4:177-80.12. Kamp A. Parent child separation during dental care: a survey of parent’s pref-erence. Pediatr Dent 1992; 14:231-5.13. Certo M, Bernat J, Creighton P. Parental views aboutaccompanying their child into the operatory. J Dent Res 1992;71:236-8 14. Marcum B, Turner C, Frank J. Courts. Pediatric dentists’ attitudes regarding parental presence during dental procedures. Pediatric Dentistry 1995; 17:432-6.15. Certo M, Bernat J. Parents in the Operatory. NYSCJ 1995; 79: 16-1916. Himes M, Munyer K, Henly S. Parental presence during pediatric anesthetic inductions. AANA J 2003; 71:293-8.17. Bevan J, Johnston C, Haig M, et al. Preoperative parental anxiety predicts behavioral and emotional responses to induction of anaesthesia in children. Can J Anaesth 1990; 37:177-182.18. Venham L, Bengston D, Ciphes M. Parental presence and the child’s response to dental stress. J Dent Child 1978; 45: 37-41.19. Plefferle J, Machen J, Fields H, Posnick V, Child behavior in the dental sitting relative to parental presence. Ped Dent 1982; 4: 311-316.20. Wright G, Starkey P, Gardner D. Parent-child separation, in Managing Chil-dren’s Behavior in the Dental Office, GZ Wright, PE Starkey, DE Gardner eds. St. Louis: CV Mosby Co. 1983; pp57-74.
REFERENCES

OPERATIVE DENTISTRY
Dentin hypersensitivity is growing in incidence and can be a major concern for patients. The pain associated with dentin hypersensi-tivity is usually brought on by an external stimulus, and the intensity can differ from patient to patient. The diagnosis of dentin hyper-sensitivity often poses a challenge for the dental professional. The cause and description of the pain reported by the patient can vary and is often not adequate to make a definitive diagno-sis. The dental professional often needs to perform a thorough examination, as well as additional tests, to determine why the pain is occurring. The examination and tests can help develop a definitive diagnosis, which allows the dental professional to rule out other possible causes of the pain (periodontal disease, caries, etc) and then implement an appropriate treatment plan to ad-dress the problem.
Dentin is normally covered by enamel or cementum. As a result of any number of factors, including abrasion or periodontal disease causing gingival recession, or erosion removing the surface of tooth enamel, the underlying dentin and dentin tubules can be-come exposed (Figure 1). An external stimulus such as a change in external temperature, air movement, or physical stimulus can cause discomfort for the patient. The external stimulus is usually transitory, and the discomfort subsides shortly after the stimulus is removed.An accepted theory of how dentin hypersensitivity pain is trans-mitted suggests that pressure or ionic changes in the fluid flow that exists in the dentin tubules stimulates the pain experienced by the patient. This is often referred to as the “hydrodynamic theory.” Inside the dentin tubule, a change in pressure causes a
Dentin HypersensitivityEffective treatment with the breakthrough Pro-ArginTM technologyFotinos Panagakos, DMD, PhD
Director of Clinical Research Relations and Strategy Colgate-Palmolive, CoPiscataway, New Jersey
SWISS QUALITY& PRECISION
FOR YOUR OFFICE
F-Splint-Aid SlimReady to use glassfiber band soakedwith bonding agent
Vista-Tec ultra light
Protective shields
Maximat Plus Matrices tensioning
system
Quickmat DeluxeSectional matrix
system
Quickmatrix ForcepsPrecise placement &
easy removal of sectional matrices
2008 Preferred Product
Vista-Tec

With nearly four million smiles* and counting since 2001, Zoom is the undeniable
world leader in professional chairside whitening systems. Using proven light-activated
technology to provide dramatic results in one surgery visit, it’s no wonder that patients
ask for Zoom by name more than any other professionally dispensed whitening system.
Whether you are looking to attract new patients, energise existing patients, or enhance
your treatment portfolio, Zoom is an excellent choice.
• Clinically proven to whiten an average of 8 shades in 45 minutes†
• Full range of marketing materials to support implementation into your practice
philipsoralhealthcare.com
* Data on file. † Excluding preparation time. © 2011 Discus Dental LLC.
All rights reserved. To be dispensed by a dental professional only. ADV-3493ARA 112111
Nearly 4 million patients have seen the light.How many patients are looking for you?
Visit us at ADEEC Dubai 31 January - 2 February at Stand 680!
EGYPT JORDAN KUWAIT LEBANON Elsafaa Al Ghad Medical Supplies Alpha Medical Co. G. Tamer Holding
Tel: 2 (0) 10 1466997 Tel: +962 6 552 6358 Tel: +965 2247 8611 Tel: 961 1 694000
MOROCCO SAUDI ARABIA TUNISIA UNITED ARAB EMIRATESOrtho-Rama Bashir Shakib MSI Al Hayat Pharmaceuticals
Tel: +21 2 22862086 Al Jabri & Co. Ltd. Tel: +216 73 449 401 Tel: +971 6 5592 481
Tel: +966 26700430

Dental News, Volume XVIII, Number IV, 2011
43
OPERATIVE DENTISTRY
change in fluid movement, and this is transmitted to the odonto-blastic process and fires the afferent nerve ending in the dentin tubule (Figure 2). It is, therefore, understandable that the pain caused by this change is transient once the stimulus is removed or it dissipates, the pressure within the tubule returns to normal and the pain subsides.
Treatment and Prevention MethodsThe treatment and prevention of dentin hypersensitivity has focused on eliminating the ability of the causative agent to stim-ulate discomfort. This has resulted in the development of two major classes of products agents that occlude dentin tubules and desensitizing agents that interfere with the transmission of nerve impulses.
Occluding agents act by physically covering or “plugging” the open, exposed dentin tubules, thus preventing the effect of
thermal changes or physical stimuli caused by the movement of dentin fluid resulting from pressure changes. Some of these agents require professional application in the dental office, while others are incorporated in products that are used by the patient at home.
Desensitizing agents work by altering the levels of charged molecules in the dentin fluid. The most commonly used agent is potassium nitrate, usually delivered in a dentifrice that is applied daily by the patient during regular toothbrushing. The potassium ions must pass from the external dentin surface, through the dentin tubule, and into the pulp in order to reduce the excitation caused by the movement of fluid in the dentin tubules. Most products require continued use over a 4 to 8 week period before the patient realizes significant relief. In addition, use of the prod-uct often needs to be continued in order to maintain the relief afforded by the potassium ions/salts.

The Power. The Silence. The new TornadoSuper
Silent
COMPRESSED AIR
SUCTION
IMAGING
DENTAL CARE
HYGIENE
Tornado – the new generation of compressors from Dürr Dental
Dürr Dental, the inventor of oil-free dental compressors, presents an
unbelievably quiet and powerful compressor for dentistry in the form
of the new “Made in Germany“ Tornado.
▪ Oil-free, dry, and hygienic
▪ One of the quietest of its kind
▪ Dust- and Sandresistant
▪ Antibacterial inner tank coating
▪ Low-maintenance thanks to membrane-drying unit
Duerr Dental Middle East, P.O.Box: 87355, Al Ain - U.A.E.,
Mobile: +971 (0) 50 - 550 84 12, Fax: +971 (0) 3 767 - 5615,
email: [email protected]
AZ_Tornado_205x275 EN ARAB RZ.indd 1 11.07.11 11:56

The pain associated with dentin hypersensitivity is usually brought on by an external stimulus, and the intensity can differ from patient to patient.
Use of Pro-Argin™
Technology to Treat Dentin HypersensitivityAlthough the traditional methods of treating dentin hypersen-sitivity have been found to be somewhat effective in providing relief to patients, dental professionals continue to look for better, more effective, fast acting, and lasting treatments. In 2009, the Colgate-Palmolive Company introduced a new in-office treatment for dentin hypersensitivity called Colgate® Sensitive Pro-Relief™ desensitizing paste, based on the Pro-Argin™ technology. The Pro-Argin™ technology consists of arginine, a naturally occurring amino acid, and an insoluble calcium compound in the form of calcium carbonate. These ingredients are delivered in a prophy paste containing a mild abrasive, and can be applied with a pro-phylaxis cup to teeth that exhibit dentin hypersensitivity. Mechanism of action studies have shown that this technology physically seals dentin tubules with a plug that contains arginine, calcium, car-bonate, and phosphate. This plug, which is resistant to normal pulpal pressures and to acid challenge, effectively reduces dentin fluid flow, and thereby reduces sensitivity (Figure 3).A number of studies have been published recently supporting the launch of this new product. Laboratory tests demonstrating the product’s mode of action, as well as clinical trials demonstrating relief of dentin hypersensitivity immediately and 4 weeks after a single application, have been presented to the dental profession as evidence that the Pro-Argin™ technology provides instant and lasting relief of dentin hypersensitivity.The full range of research studies can be accessed on the Colgate dental professional website, www.colgateprofessional.com.Treatment with Colgate® Sensitive Pro-Relief™ desensitizing paste is simple and easy to incorporate into everyday practice. The paste is gentle to gingival tissues, does not elicit pain when applied, and has a pleasant mint flavor. The dental professional applies a small amount of paste to sensitive tooth surfaces with a slowly rotating, soft prophy cup. The dental professional should carefully burnish Colgate® Sensitive Pro-Relief ™ desensitizing paste into all sensitive areas, focusing on the cemento-enamel junction and exposed dentin. Application of Colgate® Sensitive Pro-Relief™ desensitizing paste results in immediate relief that lasts for 4 weeks after a single application.1
Clinicians encounter patients with dentin hypersensitivity on a regular basis. While every patient is different, dentin hypersensi-tivity is an indication that can be managed.
1. Schiff T, Delgado E, Zhang YP, et al. Clinical evaluation of the efficacy of an in-office desensitizing paste containing 8% arginine and calcium carbonate in providing instant and lasting relief of dentin hypersensitivity.Am J Dent. 2009;22(Special Issue A):8A-15A.
REFERENCES

Dental News, Volume XVIII, Number IV, 2011
In conjunction with the 3rd Meeting of Saudi National Guard and the 1st Meeting of the Saudi Endodontic Society “New Dental Era”, the ICD Middle East Section Meeting was held in Riyadh, KSA at the Marriott Hotel.
All seven lecturers at the continuing education program were ICD fellows or inductees:
Nasser Al Nooh - Stability of Mandibular Bilateral Osteotomy: screws versus plateNassir Hamlan - Back to the Future with Self Ligating BracketsRiad Bacho - STA Computer Controlled Injection Technology in Pediatric DentistryNadim AbouJaoude - Tooth Preparation fo Zirconia-based RestorationsKhali Al Fouzan - Tooth Preparation for Zirconia-Based Restorations Essam Tashkandi - Dental Shade Matching: a guessing Game?Munir Silwadi - Ceramic Veneers: Clinical Bonding Protocol
In the Induction Ceremony that followed, five nominees from Saudi Arabia received the honor of fellowship into the College:Othman Bakkar, Abdulaziz BinAhmed, Abdullah Al Kraidis, Saad AbdulAziz Al Nazhan, and Abdullah Al Shammery.The new fellows were handed their certificates and gold pins by Section President Roy Sabri, Vice President Youssef Talic and President Elect Riad Bacho. Registrar Nadim AbouJaoude, Councilor Cedric Haddad and Regent District 2 Ali AlEhaideb were the other officers taking part in the ceremony.A dinner followed at the traditional Saudi Al Qarya Al Najdah restaurant.
MORE PICTURES AVAILABLE ONwww.facebook.com/dentalnews1
46
THE
3RD N
ATIO
NAL
GUA
RD A
ND
1ST S
AUDI
EN
DODO
NTI
C SO
CIET
Y

Officers and newly inducted fellows: seated from left: Regent Ali Alehaideb, President Elect Riad Bacho, President Roy Sabri, Vice President Youssef Talic. Registrar Nadim AbouJaoude, Councilor Cedric HaddadStanding from left: Abdulaziz BinAhmed, Abdullah Al Shammery, Othman Bakkar, Saad Abdul Aziz Al Nazhan, Abdullah Al Keraidis
Professor Dany Buser lecturing on the latest in implant dentistry
MORE PICTURES AVAILABLE ONwww.facebook.com/dentalnews1
Pr. Gabriele Pecora with Dr. Khaled Al Fouzan Head of the Saudi Endo SocietyPr. Gabriele Pecora with Dr. Khaled Al Fouzan Head of the Saudi Endo Society

With the collaboration of the Iraqi Dental Association IDA,
and the support of the Iraqi Ministry of Health and DENTSPLY,
Tamer Levant Ltd, the official dealer of DENTSPLY in Iraq has
held in Erbil Rotana the “train of trainer” course, for a
group of Endodontists from the different provinces of Iraq,
focusing on the latest techniques of using rotary
instruments for more reliable endodontic treatment.
During this course, the participants were given the title of
“DENTSPLY Maillefer official Trainer” in order to be able to
do their own lectures and workshops in their cities.
It’s been a great privilege to Tamer Levant to invite Professor
Edmond Koyess, Maillefer Opinion Leader and chairman of
endodontics department at the Lebanese University who
animated the two days by delivering lectures and conducting
workshops. It was also honored by the presence of Dr Ghada
Bassil, DENTSPLY Continuous Education Manager, and Mr Diaa
Khreish Managing Director of Tamer Levant in Iraq who
confirmed that Tamer Levant is committed to developing the
dental profession through the latest technology adopted
worldwide and to investing more into the education of the
dentists all over Iraq.
Mr Khreish also revealed that the company contracted with
the Iraqi Dental Association to provide all necessary
equipments and materials for the continuous education
courses, free of charge, and added:
“we are now studying the possibility of investing in larger
dental sectors” Also the company held a lecture and
workshop at the Dental Faculty in Hawler University for the
educational cadre of the faculty with the presence of
Dr Ziwar Kassab, the dean of the faculty.
É¡à`£N QÉ`WEG øª°Vh ,������� ácô°T π«``ch ,âfÉØ«d ôeÉJ ácô°T âeÉbCG
á`«`ª`«`∏`©`J äGQhO á`eÉ`bEG È`Y ¥Gô©`dG »`a ¿É``æ``°SC’G Ö`W á`æ`¡`e å`jó`ë`Jh ô`jƒ`£`à``d
áë°üdG IQGRh øe ºYóHh ,¥Gô©dG »`a ¿Éæ°SC’G AÉÑWCG áHÉ≤f ™e ¿hÉ©àdÉHh ,Iôªà°ùe
Ióª`d á`«`Ñ`jQó``J IQhO â`eÉ``bCG ,��������� ������� ácô`°Th á«`bGô`©`dG
á«bGô©dG äɶaÉë`ª`dG øe ¢UÉ°üàN’G …hP ¿Éæ°SC’G AÉÑWCG øe áYƒªéª`d ø`«eƒj
»`a ∂dPh ,Qhò÷G Iƒ°ûëH á°UÉÿG á«∏ª©dGh ᫪∏©dG äÉ«æ`≤`à`dG çó`MCG ≈∏Y ,á`aÉ``c
.π«HQG ÉfÉJhQ ¥óæa
õcGôeh º¡à¶aÉfi »`a øjôNBG AÉ`Ñ`WCG ÖjQó`à`d ø`«HQó`à`ª`dG AÉÑ`WC’G IQhó`dG â∏ qgCG
.º¡∏ªY
Qhò÷G êÓY º°ùb ¢ù«FQ ¢ùjƒc ¿ƒeOG Qƒ°ù`aÈ`dG Iƒ`YóH á``cô`°û`dG â`aô`°û`J ó`bh
.ø`«eƒj Ióª`d πª©dG ¢TQh QGOCGh äGô°VÉëª`dG ≈≤dCG …òdG á«fÉæÑ∏dG á©eÉ÷G »`a
,π«°SÉH IOÉZ IQƒàcódG ,������� ácô°T »`a ôªà°ùŸG º«∏©àdG Iôjóe äô°†Mh
¿CG ó```` qcCG …òdG ¢û`jô`N AÉ`«`°V ó`«`°ùdG ,¥Gô`©`dG »`a�â`fÉ`Ø`«`d ô`eÉ`J á``cô`°T ô`jó`eh
äÉ«æ≤àdG çóMCG Ëó≤J ÈY ¿Éæ`°SC’G ÖW áæ¡`e ôjƒ£àH kIô`°TÉ`Ñ`e áq `«`æ`©`e ácô`°û`dG
á«bGô©dG äɶaÉëª`dG »`a ¿Éæ°SC’G Ö«ÑW º«∏©J »`a Qɪãà°S’Gh ,kÉ«ª`dÉY Ióªà©ª`dG
.áaÉc
OGó¨H »`a ájõ`côª`dG ¿Éæ`°SC’G AÉÑWCG áHÉ`≤`f ™e äó`bÉ`©`J á``cô`°ûdG ¿CG ¢ûjôN ∞°ûch
≈∏Y ∂dPh ,ôªà°ùª`dG º«∏©àdG äGQhód áeRÓdG ÖjQóàdG OGƒeh Iõ¡LCG πeÉc Òaƒàd
¿CG ±É`°VCGh .äɶaÉëª`dG áaÉ``c »`a äGQhó`dG √ò``g ΩÉ`≤o `J ¿CG ≈`∏`Y ,á`°UÉ`î`dG É``¡`à`≤`Ø`f
.iôNCG äÉ°UÉ°üàNG πª°ûJ ÈcCG á£N OGóYEG Oó°üH ácô°ûdG
- á`«`Ñ`£``dG π`«``HQG á©`eÉ`L »`a πªY äÉ°TQhh ᫪∏Y Iô°VÉfi ácô°ûdG âeÉbCG ,kÉ°†jCG
,ÜÉ°ùc QGƒjR Qƒ`à`có`dG ,á`«``∏`μ`dG ó«`ª`Yh º`«``∏©`à`dG QOÉ`c Égô`°†M ,¿Éæ°SC’G ÖW á«∏``c
. á«∏μdG IQGOEG ¢ù∏›h
Tamer Levant Ltd, Italian City villa 570, Erbil Iraq
Tel: +964 7501 440 400 email: [email protected]
www.tamerholding.com
¿Éæ°S’G ÖW äÉeõ∏à°ùeh ΩRGƒd πμd ¥Gô©dG ‘ ¬H ¥ƒKƒŸG ∂μjô°T�� âæØ«d ôeÉJ ácô°T
+964 7501 440 400 : ∞JÉg . ¥Gô©dG ,π«HQG 570 ,á«dÉ£j’G áæjóŸG :¿Gƒæ©dG
Professor Koyess During the lecture
Professor Koyess during the workshop day
with Tamer Levant Team (right to left)
Dr Ghada Bassil, Prof Koyess, Diaa Khreish,
Elie Bou Dargham, Alan Ibrahim, Fady Farjo
photo of the group with Prof Koyess
lecture at Hawler Dental college- Erbil
workshop at Hawler University – Erbil

Getting to the root of the problem.
Rev
o-S
is a
regi
ster
ed tr
adem
ark
and
“You
r End
o S
peci
alis
t” is
a tr
adem
ark
of M
Icro
-Meg
a Lt
d.
As a world leader in the micro-design of Endo instruments, precision is our business. Our Revo-S™ NiTi rotary system takes precision to new levels. With an easy 1-2-3 sequence, the Revo-S™
MICRO-MEGA® Revo-S™
Join the REVOlution at www.revo-s.com


Dental News, Volume XVIII, Number IV, 2011
MORE PICTURES AVAILABLE ONwww.facebook.com/dentalnews1
51
THE
3RD N
ATIO
NAL
GUA
RD A
ND
1ST S
AUDI
EN
DODO
NTI
C SO
CIET
Y
Saudi Endodontic Society officers

VOCO GmbH · Anton-Flettner-Straße 1-3 · 27472 Cuxhaven · Germany · Tel. +49 (0) 4721 719-0 · www.voco.com

Visit nobelbiocare.com/nobelreplace
© Nobel Biocare Services AG, 2011. All rights reserved. Nobel Biocare, the Nobel Biocare logotype and all other trademarks are, if nothing else is stated or is evident from the context in a certain case,
trademarks of Nobel Biocare. Disclaimer: Some products may not be regulatory cleared/released for sale in all markets. Please contact the local Nobel Biocare sales offi ce for current product assortment
and availability. 1 Source: Millennium Research Group. 2 Dental Product Shopper voted NobelReplace Tapered Best Product 2011. www.dentalproductshopper.com/nobelreplac
2
One implant body, three connections.
Treatment simplicity with one drill protocol.
Most widely used implant system in the world.1
It’s called NobelReplace. Whether you are a new or experienced implant user, this original tapered implant mimicking the shape of a natural tooth offers you a safe and reliable solution for every indication. The color-coded surgical and prosthetic components and the standardized step-by-step drill protocol ensure ease-of-use and predictable outcomes. Depending on indica-tion and your personal preference, choose between the
internal tri-channel connection with or without platform shifting for unrivalled tactile feel and the strong sealed conical connection with built-in platform shifting. After 45 years as a dental innovator we have the experience to bring you future-proof and reliable technologies for effective patient treatment. Their smile, your skill, our solutions.
One implant system for all your needs.
With platform shift
and conical connection
Launch in fall 2011PR
EV
IEW

Dental News, Volume XVIII, Number IV, 2011
MORE PICTURES AVAILABLE ONwww.facebook.com/dentalnews1
54
THE
3RD N
ATIO
NAL
GUA
RD A
ND
1ST S
AUDI
EN
DODO
NTI
C SO
CIET
Y
PICTURES FROM THE EXHIBITION FLOOR


1
NNOVATION. QUALITY. SERVICE. IN NO
VATI
ON.
QUA
LIT
INING. KNOWLEDG
E. P
ON. QUALITY. SE RVICE.
INNO
VAT
EDUC
ATIO NING. KNOWLEDGE.
QUALITY. SERVICE.
INNO
VATI
ON. Q LITY. SERVICE.
Hands-On Workshop Critical Soft Tissue and Bone Grafting Techniques
26/27th March 2012 29/30th March 2012 Winterthur by Zurich, Switzerland
Dr. Maurice Salama, USAZimmer Institute presents


CompothixoTM
Improved Quality Restorations
Smart VibrationsCompothixo™ is a unique generation in compositeplacing and modelling instrument suitable for allclass restorations.
The new Compothixo™ technology optimizes thethixotropic properties of composites by changingviscosity only, without altering the chemical andmechanical characteristics of the material.
• Better wettability
• Superior adaptation of compositeto cavity walls
• Reduction of air bubbles
• Precise application
• Layer thickness control
• Improved sculptability
• Reduced stickiness
Your practice is our inspiration.™ KerrHawe SA P.O. Box 272 6934 Bioggio Switzerland Freephone: 00800 41 05 05 05 Fax: ++41 91 610 05 14 www.kerrdental.eu

Planmeca ProMax 3DUnique product family
1971 - 2011
More informationwww.planmeca.com
Planmeca OyAsentajankatu 6, 00880 Helsinki, Finland tel. +358 20 7795 500, fax +358 20 7795 [email protected]
Perfect sizes for all needs
Romexis • PlanScan • ProMax 3D • ProFace
Romexxxiiisss • Pllan 3D • PProoFFace
Unique 3D combination for open CAD/CAM
3D X-ray • 3D photo • panoramic • cephalometricRomexis software completes 3D perfection

المؤتمر السعودي العالمي الرابع عشر لجامعة الملك سعود لطب األسنانالثالث والعشرون للجمعية السعودية لطب األسنان
King Saud University 14th International Dental Conferencethe 23rd for the Saudi Dental Society
4677763 / 4677743 / 4677764 / 4677534www.sds.org.sa
Venue Riyadh International Exhibition Center14 – 16 Rabi’ 1 1433H . 6 – 8 February 2012
مركز معارض الرياض الدولي خالل الفترة من ١٤-١٦ ربيع األول ١٤٣٣هـ - الموافق ٦ – ٨ فبراير ٢٠١٢م

BisCem®
Dual-Cured Self-Adhesive Resin Cement
Bonds to a multitude of substrates, including metals, composites,
porcelain and amalgam
DUO-LINK�
Dual-Cured Composite Luting Cement
A universal cement ideal for all-ceramic/porcelain, metal and
composites restorations (inlays,onlays, crowns, bridges), as well
as fiber and metal posts
CHOICE� 2Light-Cured
Veneer CementA multitude of shades ensures
the restoration blends well and isnatural looking for any patient
For more information email [email protected] or visit www.bisco.comThe perfect restoration begins with a solid foundation!
BISCO offers the latest technology in cementation and keeps it simple for the clinician byproviding a cement line which covers every Dentist�s indirect restorative needs!


MetaFix™
All·in·One Matrix System
The easiest solution for creating a perfect contact point
• Integrated tensioning and opening device
• Easy creation of contact point
• No additional tools needed
Your practice is our inspiration.™ KerrHawe SA P.O. Box 268 6934 Bioggio Switzerland Freephone: 00800 41 05 05 05 Fax: ++41 91 610 05 14 www.KerrHawe.com



Dental News, Volume XVIII, Number IV, 2011
It is indeed a source of great pleasure to welcome all our esteemed guests in the Egyptian Dental Association’s 15th International Dental Congress.The present Congress is the first Congress to be held after our January 25th revolution and in a new era that is witnessing great democratic upheavals in many Arab nations, but with great turmoil still raging in some other nations.It is, however, through such human interaction such as this Congress that people of different backgrounds are brought together and made to better understand each other, which we are sure will ultimately lead to better understanding between us all, as well as to better relations among all our nations. It is indeed one of the major benefits of scientific exchange to bring different people from all over the world together where they may share common goals and objectives.May we wish all our guests a pleasant and enjoyable stay among us, and we sincerely hope that you may fully enjoy the scientific and social programs we have prepared for you.Professor Tarek Abbas HassanPresident of the EDA and the Congress
MORE PICTURES AVAILABLE ONwww.facebook.com/dentalnews1
Prof T. Abbas’ speech during the opening ceremony
Lebanese delegation with the Egyptian Dental Assosiation Board
66
E
DA 2
011


MORE PICTURES AVAILABLE ONwww.facebook.com/dentalnews1
Audience during the lecture


Dental News, Volume XVIII, Number IV, 2011
MORE PICTURES AVAILABLE ONwww.facebook.com/dentalnews1
EDA
2011
70
EXHIBITION
FLOOR


Dubai gathered for the third time the world experts of Dental - Facial Cosmetic on the 28th - 29th October 2011. An international conference, at the Jumeirah Beach Hotel, open to all aspects and specialists working in the field of aesthetic dentistry.With the excellent ambiance and cozy atmosphere the conference again makes exceptional net-working and connecting the leaders in the field of Aesthetic Dentistry – practitioners, researchers and industry players.
Bringing together industrial leaders and professional practitioners, the conference not only delivered extensive scientific knowledge from across the globe but gave way for an excellent opportunity to present the latest advancements and developments within the Facial Cosmetics practice.The 3rd dental Facial opened the door to open discussion and learning for this knowledge hungry region and allowed the participants to build their skills and use the opportunity for networking and sharing experiences in the application of technology throughout the learning cycle - from primary and secondary education through to professional development and lifelong learning.
MORE PICTURES AVAILABLE ONwww.facebook.com/dentalnews1
Dr. Aisha Sultan with the organizing committee


Dental News, Volume XVIII, Number IV, 2011
Mr. Jamal El Hage President of the Lebanese Dental Technicians Order
Mr. Jean Chiha CMDT receiving the trophy from Dr. Mounir Silwadi
74
DFCI
C 20
11

MORE PICTURES AVAILABLE ONwww.facebook.com/dentalnews1




Thank you for subscribing atdentalnews.comThe winner of the W&H LED Contra - Angle Handpiece(ALEGRA WE - 56 LED G)is Dr. Mayssa Adhami from Lebanon
Dr. Mayssa Adhami Winner of the W&H Hand Piece
The Result were also posted on the Dental News Facebook Page (www.facebook.com/dentalnews1)

®
Dr. Wild’s Mideast Regional Office: Actco, P.O. Box 40746, Larnaca 6306, Cyprus, Tel.: (24) 623515 / 654252, Fax: (24) 623844. E-Mail: [email protected]
• Free from chemical bleaching substances, preservatives and enzymes
• Eliminates easily plaque and stains of tea, nicotine, coffee and fruits
• Contains the natural active ingredient pumice
• For professional and home use
DEPURDENT® cleaning and polishing paste for a brilliant smile
DEPURDENT® Mouthrinse - The perfect supplement to DEPURDENT® cleaning and polishing paste!
• Its special formula prevents the formation of plaque and stains and helps to retain the natural white color of the teeth.
• Fluoride protects against caries.• Refreshing taste for long-lasting fresh breath.
, Fax: (244)4) 62338448448444 . . E-ME-ME-M-ME-M- ailailailaiaila ::::: jojojojojooeiseiseiseiseissa@sa@sa@sa@[email protected] ccommc
New
Dr. Wild & Co. AG www.wild-pharma.com
Bahrain: Awal Pharmacy, East Riffa, Bahrain. Egypt: Sesic, Alexandria. Kuwait: Al-Maseela Pharmaceutical Co., Safat. Lebanon: A.M.G. Medical.Jdeideh-Azur Center Oman: Ibn Sina Pharmacy L.L.C., Muscat. Qatar: Ahmed Khalil Al Baker & Sons, Doha. Saudi Arabia: Depot Pharmaceutique du Moyen Ori-ent, Jeddah. Sudan: Pharma Care Co, Khartoum. United Arab Emirates: Al Hayat Pharmaceuticals, Sharjah. Yemen: Al Rawdha Trading Group, Sana’a.
Swiss professional oral care

new
Welcome to the new science of Sensodyne Repair & Protect
Redefining the science of dentine hypersensitivity
Announcing the arrival of Sensodyne® Repair
& Protect, which brings the unique potential
of NovaMin® calcium phosphate technology
to a daily fluoride toothpaste. NovaMin®
builds a reparative hydroxyapatite-like layer
over exposed dentine and within the tubules1-5
to continually help protect your patients
against the pain of dentine hypersensitivity6-8
Now there’s a major advance
to help you meet the challenge
of dentine hypersensitivity
Specialist in dentine hypersensitivity management
References: 1. Burwell A et al. J Clin Dent 2010; 21(Spec Iss): 66–71. 2. LaTorre G, Greenspan DC. J Clin Dent 2010; in press. 3. Efflant SE et al. J Mater Sci Mater Med 2002; 26(6):557−565. 4. Clark AE et al. J Dent Res 2002; 81 (Spec Iss A): 2182. 5. GSK data on file. 6. Du MQ et al. Am J Dent 2008; 21(4): 210−214. 7. Pradeep AR et al. J Periodontol 2010; 81(8): 1167−1113. 8. Salian S et al. J Clin Dent 2010; in press. SENSODYNE® and the rings device are registered trademarks of the GlaxoSmithKline group of companies. Prepared November 2010. Z-10-175.

VARIOLINK® NThe ESTHETIC dual-/light-curing luting composite system
MULTILINK® NThe UNIVERSAL self-curing luting composite with light-curing option
POWERFUL BONDSPOWERFUL OPTIONS
MULTILINK® SPEEDThe FAST self-adhesive, self-curing resin cement with light-curing option
www.ivoclarvivadent.comIvoclar Vivadent AGBendererstr. 2 | FL-9494 Schaan | Liechtenstein | Tel.: +423 / 235 35 35 | Fax: +423 / 235 33 60