Cord Blood Unit Selection Advisory Panel...as a result of being secondary, less than CR or had mds...
24
Cord Blood Unit Selection Advisory Panel Kay Poulton PhD FRCPath http://bsbmt.org http://www.bshi.org.uk
Transcript of Cord Blood Unit Selection Advisory Panel...as a result of being secondary, less than CR or had mds...

Cord Blood Unit Selection Advisory Panel
Kay Poulton PhD FRCPath
http://bsbmt.org
http://www.bshi.org.uk

Members of the Panel • Kay Poulton, BSHI Chair (Panel Chair) • Sergio Querol, Chair of WMDA CBWG, Vice Chair • Rachael Hough, CBWG Co-Chair • Nigel Russell, CBWG Co-Chair • Vanderson Rocha, Medical Director BBMR/NHSCBB (invited) • Andrew Clarke, Glasgow Royal Infirmary • Irina Evseeva, Anthony Nolan • Colin Brown, Consultant Clinical Scientist, Colindale NHSBT & BBMR • Cristina Navarrete, Consultant Clinical Scientist, Colindale & BBMR • Paul Dunn, Consultant Clinical Scientist, Leicester General Hospital • Katy Latham, Consultant Clinical Scientist, Anthony Nolan. • Ann-Margaret Little, Consultant Clinical Scientist, Glasgow Royal Infirmary • Leigh Keen, Principal Clinical Scientist, Bristol NHSBT, Filton • Pat Taylor, Principal Clinical Scientist, H&I Laboratory, NHSBT, Birmingham • Mike Watts, UCLH (Director Wolfson Cellular Therapy Unit) • Ines Ushiro-Lumb (NHSBT Clinical Microbiology Lead for Organ Donation & Transplantation)

Membership Responsibilities
Members of the CBUSAP are expected to:
• Respond by email to advisory requests in as timely a manner as possible subject to other commitments.
• Ensure that potential conflicts of interest are identified, recorded and managed to ensure advice provided is independent.


Title

Title

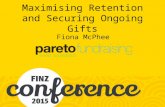
Figure 1: Flow Diagram Summarising Cord Blood Unit Selection
UCB Search indicated (lack of conventional donor, urgency of transplant etc)
UCB search HLA-A, HLA-B, HLA-DRB1, HLA-C (if available)
Prioritise a) according to HLA match and b) cell dose within each level of match
Single unit Allelic HLA match 6-8/8
Cell dose ≥ 3x107 TNC/Kg
Single unit Allelic HLA match 5/8
Cell dose ≥ 5x107 TNC/Kg
Malignant disease Non-malignant disease
Single unit Allelic HLA match 5-8/8
Cell dose ≥ 5x107 TNC/Kg
Yes Select largest unit (TNC) for degree
of HLA match and consider bank accreditation, CD34 dose, ABO
match, HLA Ab, red cell depletion
Yes Select largest unit (TNC) for degree
of HLA match and consider bank accreditation, CD34 dose, ABO
match, HLA Ab, red cell depletion
Yes Select largest unit (TNC) for degree
of HLA match and consider bank accreditation, CD34 dose, ABO
match, HLA Ab, red cell depletion
No No No
Consider double unit graft if each unit is ≥ 4/6 matched with recipient (Antigen level match HLA-A, HLA-B, allelic level HLA-DRB1)
and TNC ≥1.5x107/Kg (total of both units 3.5x107 TNC/Kg) Prioritise a) according to HLA match and b) cell dose within each level of match
c) consider bank accreditation, CD34 dose, ABO match, HLA Ab, red cell depletion

Case Studies http://bsbmt.org
http://www.bshi.org.uk

Case 2
Rank CBU ID
Bank
*FACT
accredite
d
Year
TN
C
x1
07
/kg
CD3
4
x105
/kg
CFU
X106
Viability
%
RB
C
Vo
l
ml
AB
O &
RhD
HLA HLA Match
A* B* DRB1
* C*
DQB
1*
Low
/6
High
/8
Patient HLA type A+ 11:01, 31:01
35:01, 41:02
04:04, 13:03
04:01, 17:03
03;01, 03:02
DUCB23931 Germany* 2013 3.09
1.1 See
below 90 R 53 O+
11:01, 66:01
35:01, 41:02
04:04, 13:03
04:01, 17:03
03:01, 03:02
5 7
992222266
NMDP MD Anderson*
2009 2.09
1.1 1.1 97
D
25 B+ 31:01, 68:02
35:01, 41:02
04:04, 13:03
04:19, 17:01/3
5 6 ?
CY1134284D
CYCORD (Cyprus)
2010 2.04
0.3 Not
stated 95
D 26 O+
11:01, 02:01
35:01, 41:02
04:01, 13:03
04:01, 17:03
03:01, 03:02
4 6
73312
MDA
Israel* 2004
1.57
0.57 Not
stated
Not stated
D
25 O- 02:01,
31:01/2
35:02, 41:02
04:03, 13:03
04:01, 17:01/3
4 5 or 6
290196402 Sydney
Australia* 2014
3.22
0.92 Not
stated 100
D
60 O+ 24, 66:01 35:05, 41:02
04:04, 13:03
04
17
03:01, 03:02
4 6?
Additional Information
High resolution HLA typing is outstanding on Unit 290196402 (Australia) at all loci unless otherwise stated. DUCB23931 CFU-GM: 8.8 x105 and CFU:GEMM: 2.84x104
NMDP do not perform sequencing at exon 1 of HLA-C.
Date Dec 2015
Centre Clinical Contact Clinical contact email
H&I Contact H&I contact email
Patient Details:
Initials Case
#2 Unique
Identifier Age or DOB 38 Weight (Kg) 54
Proposed Transplant Date As soon as possible Diagnosis ALL
HLA-Specific Antibodies HLA specific antibody Negative on sample dated one week ago

Case 2 Clinical Follow Up
• Delayed / Failed Engraftment
TNC Post Cryo CD34 Post Cryo CFU-GM Post Viability 7 AAD Post Thaw
DUCB23931
CBB results 2.91 x 10*7/kg 1.0 x 10*5/kg 1.59 x 10*4/kg 98%
Transplant Centre Results 2.09 x 10*7/kg 0.46 x 10*5/kg 0.8 x 10*4/kg 36%
9922-2226-6
CBB results 1.97 x 10*7/kg 1.0 x 10*5/kg 0.82 x 10*4/kg 98%
Transplant Centre Results 1.57 x 10*7/kg 0.67 x 10*5/kg 1.02 x 10*4/kg 65%
Engraftment Neuts (N=0.5) day +34, Platelets(N=20) day +55 STR 100% DUCB23931 day +30

Case 3
Rank CBU ID
Bank
*FACT
accredit
ed
Year
TN
C
x107
/kg
CD3
4
x105
/kg
CFU
X106
Viabilit
y
%
RB
C
Vol
ml
ABO
&
RhD
HLA HLA
Match
A* B* DRB1* C* DQB1
*
Low
/6
H
i
g
h
/
8
Patient HLA type O 01:01
31:01
07:02
44:03
04:04
09:01
04:01
07:02
03:02
03:03
1
994026517
NMDP
*AABB
24/05/
2005
3.6
1
2.30 D
59
O+ 01:01
31:01
07:02
40:01
04:04
09:01
03:04
07:02
03:02
03:03
5
6
4
FRCBLI691336210
69
FCB
France
*N
24/06/
2013
3.5
6
0.88
D
25
A+ 01:01
23:01
07:02
44:03
03:01
09:01
04:01
07:02 NK
4
6
2
992229899
U1CB
NMDP
*Y
24/11/
2009
2.6
7
3.15
D
25
A+ 23:01
31:01
39:11
07:02
04:04
09:01
07:02
----
03:02
02:02
4
5
3
AU390077924
AUCB
Australia
*Y
15/02/
2007
2.1
3
0.71
D
48.
6
O- 03:01
31:01
07:02
39:01
04:04
09:01
07:02
12:03 NK
4
5
5
EN110555686D
(G180109195396G
)
BSCB
UK
*Y
29/06/
2009
1.5
8
1.18
D
25.
1
O- 01:01
02:22
07:02
44:03
01:02
04:05
04:01
07:02
03:02
05:01
3
5
R/D
R/D
Additional Information
Ranking based, in this order of ‘importance’: cell count + dose, DRB1 allele match, A/B allele match, A/B antigen match, C match
Date Nov 2015 Centre Clinical Contact Clinical contact email
H&I Contact H&I contact email
Patient Details:
Initials Case 3 Unique
Identifier Age or DOB 63y Weight (Kg) 76.4kg
Proposed Transplant Date 3 weeks from submission of request Diagnosis AML
HLA-Specific Antibodies 1 week ago: Anti-A2, B8, B57, B75 ANT Reference No

Case 3 Panel response CBUSAP Recommended Choice:
Cord 1 994026517
Additional comments about this cord: Regarding the issue with the volume, I would say
that this cord has been processed a while ago (2005), when SEPAX or AXP were not well implemented at CBB, so probably a manual process was done. Another aspect to keep in mind for this unit is that as it’s older, probably virology tests were not done following current practices and CBB probably won’t have samples to perform them.
(St Louis Panel) In response to your questions above for CBU SL052660 / 9940-2651-7, currently reserved for RID 271-048-4 through the NMDP:
The initial collected volume was 145 ml with a preprocessing Hct of 37.7%. The product was then RBC/ Plasma reduced during processing
The post processing volume is 47ml + 11.75 ml DMSO/Dextran cocktail (58.75 ml) with a Hct of 40.6% of this more concentrated product, which is stored and frozen in two separate bags of 24 ml (+ 6ml DMSO/Dextran) and 23 ml (+ 5.75 ml DMSO/Dextran)

Case 3 Panel response Alternative Suggestions – Potential Double CBU combinations
992229899 & AU390077924 as a double CBU if Unit 1 is unsuitable due to volume/cell dose
If happy that unit 1 is red cell depleted I’d use 1 (994026517) and 2 FRCBLI69133621069 If not I’d use 2 and 3 992229899 I’d use a double graft as dose of 1 or 2 alone – while meeting the criteria- is borderline ( though would understand if single unit ultimately chosen). If this AML is high risk as a result of being secondary, less than CR or had mds preceeding then even more reason for maximising cell dose as failure to engraft increased.
• I completely agree with the rank already listed, favouring cell dose (especially CD34) and DRB1 match, in this high risk acute leukemia.
• Nothing to add nor comment.
• As above. Ranking based, in this order of ‘importance’: cell count + dose, DRB1 allele match, A/B allele match, A/B antigen match, C match
• Cord 1. 6/8 (and 8/10). Good cell dose and CD34 and ABO compatible. No relevant antibodies
• Having looked at the selected units I agree with the ranking as given. I may have selected different had the third ranked unit had a better CD34 count.

Case 3 Clinical Follow Up
• red cell reduced cord. – Not washed.
– Single unit.
• Engrafted neuts 0.5 day +11
• Day 30 engraftment: PBL 98.6% donor; CD3+ 100% donor
• Day 60 engraftment: PBL 100% donor; CD3+ 100% donor
• Day 90 engraftment: PBL 100% donor; CD3+ 100% donor
• Day 150 engraftment: PBL 100% donor; CD3+ 100% donor

Rank CBU ID
Bank
*FACT
accredited
Year
TNC
x107
/kg
CD34
x105
/kg
CFU
X106
Viability
%
RBC Vol
ml
ABO &
RhD
HLA HLA Match
A* B* DRB1* C* DQB1* Low
/6
High
/8
Patient HLA type A+
03:01
33:03
35:01
53:01
13:03:01
08:06
04:01
16:01
^1 G180114109748G *NHSBT 25.1.14 4.15 0.86 D 27.3 B+ 03:01
33:03
35:01
53:01
04:04
13:03
04:01
04:01
7/8
hvg
2 G180112110827G *NHSBT 27.5.12 2.0 0.55 D 24.7 B+ 03:01
33:01/03
35:01
53:01
11:04
13:03
04:01
04:01 6/8 gvhd
3 9843-3781-7 *MD Anderson 3.1.14 3.35 1.84 D 25 O+ 02:05
33:03
35:01
53:01
03:02
13:03
04:01
04:01
7/8
hvg
4 IT15RC001813 Calabria 1.7.15 4.56 1.9 D 100 A+ 03:01
33:03
35:01
58:01
11:04
13:03
03:02
04:01 6/8 gvhd
$5 G221211102668 *ANT 10.5.11 2.02 0.64 D 115.21 O- 30:01
33:03
35:01
53:01
13:03
14:01
04:01
07:01
6/8
6 G1801131208999 *NHSBT 1.7.13 1.75 0.58 D 23.7 O+ 03:01
33:03
44:02
53:01
04:01
13:03
04:01
05:01
5/8
7 S003110900083 National Swedish
10.2.10 3.5 0.96 D 25 A- 03
68
35
53
04:05
13:03
5/8
8 9944-0089-4 *St Louis 28.6.12 3.9 1.13 D 03:01
30:02
35:01
53:01
08:06
11:01
04:01
04:01
5/8
9 9809-3970-7 *New York 8.3.09 2.75 1.33 D 25 O+ 23:01
33:03
15:03
53:01
08:06
13:03 4/6
Additional Information
^ DRB1 high res to be confirmed
$ Cord is sickle trait
Case 4 Date Jan 2015 Centre Clinical Contact Clinical contact email
H&I Contact H&I contact email
Patient Details:
Initials Case 4 Unique
Identifier Age or DOB Weight (Kg) 52
Proposed Transplant Date 1 month from submission of request Diagnosis Hepatosplenic Non-Hodgkins Lymphoma
HLA-Specific Antibodies Currently negative ANT Reference No

Case 4 Panel response CBUSAP Recommended Choice:
We received responses or comments from 8 panel members . There were no NIMA matches identified. There is consensus that the panel would recommend a double CBU donation. Pending HLA-specific antibody testing results to eliminate the presence of donor-directed antibody the panel had a preference for
The combined donor pair with the closest HLA match:
I. G180114109748G (Ref 1) NHSBT (5/6 (7/8 [6/8 gvh]) CD34:= 0.865/Kg
with
I. G180112110827G (Ref 2) NHSBT (5/6 (7/8 [6/8 gvh]) CD34: 0.555/Kg
Aggregated cell dose with G180114109748G (Ref 1) 1.415/Kg

Case 4 Panel response
Acceptable alternative combinations are listed below:
I. 9944-0089-4 (Ref 8) St Louis (5/6 (6/8 or [5/8gvh]) CD34: 1.95/Kg
This cord is an HLA-A locus antigen match with the patient
Aggregated cell dose with G180112110827G (Ref 2) = 2.455/Kg
II. 9944-0089-4 (Ref 8) St Louis (5/6 (6/8 or [5/8gvh]) CD34: 1.95/Kg Aggregated cell dose with G180114109748G (Ref 1) = 2.765/Kg
Aggregated cell dose with G180112110827G (Ref 2) = 2.455/Kg
Or
III. 9843-3781-7 (Ref 3) MD Anderson (4/6 (6/8)) CD34: 1.845/Kg
Aggregated cell dose with G180114109748G (Ref 1) = 2.75/Kg
Aggregated cell dose with G180112110827G (Ref 2) = 2.395/Kg

Case 4 Clinical Follow Up Day of Transplant -7 Urgent communication from Registry:

Rank CBU ID
Bank
*FACT
accredit
ed
Year
TN
C
x1
07
/kg
CD3
4
x105
/kg
CFU
X106
Viabili
ty
%
RB
C
Vol
ml
AB
O &
RhD
HLA HLA
Match
A* B* DRB1* C* DQB1
*
Low
/6
H
i
g
h
/
8
Patient HLA type 33:03,
68:02
42:01,
44:03
07:01,
15:03
07:01,
17:01
02:02,
06:02
U1CB 9924-1801-3 * NMDP 2012 2.4 2.3 98 D 25 O+ 29:02,
33:03
44:03,
49:01
07:01,
15:03
07:01,
16:01
02:02,
06:02 4 5
G221214126592 AN 2014 2.5 0.5 90-98 D 26 O+ 02:02,
33:03
44:03,
-
07:01,
15:03
04:01,
07:01
02:02,
06:02
4 or
5
5
o
r
6
G1801121043862 BBMR 2012 3.1 0.8 93 D 25 O+ 29:02+,
33:03+
42:01P,
44:03+
01:02,
07:01G
16:01+,
17:01G
02:02,
05:01 4 5
FRCBPL
00000008304P France 2012 1.7 0.7 96 D 25 B+
33:01,
68:02
44:03,
53:01
07:01,
15:03
04:01,
-
02:02,
06:02 5 4
Additional Information
Additional Information
Case 6 is DPB1*01:01, 14:01 *U1CB 9924-1801-3 is DPB1*11:01, 18:01; DSA present: DPB1*18:01 mfi: 14-18,000 (latest sample)
Case 6 Date April 2016 Centre Clinical Contact Clinical contact email
H&I Contact H&I contact email
Patient Details:
Initials Case 6 Unique
Identifier Age or DOB 52 y Weight (Kg) 70Kg
Proposed Transplant Date asap Diagnosis FLT3 ITD+ AML
HLA-Specific Antibodies
All antibodies >2000 MFI from serum sample two weeks ago: B57,DR4,DR8,DR10,DR11,DR12,DR13,DR14,DR17,DR18,DR52,allelicDQB1*02:01,DQ4,allelicDQB1*06:03/09,DQ7,DQ8,DQ9,DP2,DPB1*04:02,DP10,DP18,DP28
ANT Reference No

Case 6 Panel response CBUSAP Recommended Choice:
We received responses or comments from 5 panel members. The blood group of the patient is not stated. Based upon the information provided to the panel, there is consensus that the panel would recommend a double CBU donation.
The cord with the best match which has the highest CD34 dose is U1CB 9924-1801-3 (Rank 4), which carries HLA-DPB1*18:01. The patient has donor-directed HLA-specific antibodies to HLA_DPB1*18:01 present at high MFIs (range 14 000 – 18 000). This cord has been disregarded by the panel due to the presence of the patient’s HLA specific antibody, but there is limited information available concerning the distribution of HLA-DPB1 on CD34 positive cells. CD34 positive cells express HLA-DR, with much weaker expression of HLA-DQ (see ref below). Anecdotally, a transplant was recently carried out across a high titre HLA-DP antibody (MFI 20,000) with no adverse effects at all upon engraftment, although the donor was a volunteer unrelated adult donor rather than UCB. If this cord is regarded as a preferred option by the referring team, it may be worth investigating the antibody titre further, perhaps with apheresis for antibody reduction if the patient could tolerate it.
There were no NIMA matches identified in the BBMR cord G1801121043862.

Case 6 Panel response
Of the remaining cords the panel recommends the following potential combinations based upon match and CD34 dose:
G221214126592 (Rank 1) AN (4 or 5/6 (5 or 6/8) CD34:= 0.5 5/Kg
with
G1801121043862 (Rank 2) BBMR (4/6 (5/8) CD34: 0.85/Kg
Aggregated CD34 dose with G221214126592 (Rank 1) 1.35/Kg
G221214126592 has a low CD34 count but may be acceptable for use once the CFU data are available. It has been ranked in this position as it is the best matched of the remaining units

Case 6 Panel response Acceptable alternative combinations are listed below:
G1801121043862 (Rank 2) BBMR (4/6 (5/8) CD34: 0.85/Kg
With
FRCBPL 0000000830P (Rank 3) France (5/6 (4/8) CD34: 0.75/Kg
Aggregated CD34 dose with G1801121043862 (Rank 2) = 1.55/Kg
FRCBPL 0000000830P has an allele level mismatch at HLA-A with the patient. HLA-A*33:01 differs from A*33:03 by only two amino acids at positions 171 and 186. 171 lies in the A pocket and may affect peptide binding; 186 lies beyond this and may not exhibit any clinical relevance.

Case 6 Clinical Follow Up
• Not available yet

CBUSAP – Where next? • Now on BSHI Website:
– http://www.bshi.org.uk/html/cord_page.html
• Terms Of Reference
• Form for submission (Word)
• Case Studies (Members Only Area)
• Documents shared with BSBMT for publication
• Panel needs constant revision to ensure sufficient members are available for comment