Biomarkers Managing IBD Stephen B. Hanauer, MD University of Chicago.
31
Biomarkers Managing IBD Stephen B. Hanauer, MD University of Chicago
-
Upload
delilah-manlove -
Category
Documents
-
view
214 -
download
1
Transcript of Biomarkers Managing IBD Stephen B. Hanauer, MD University of Chicago.

Biomarkers Managing IBD
Stephen B. Hanauer, MD
University of Chicago

+
IBD subtype:
UC UC
1 23
412
3 41 2 3
CD/UCCD/UC
Crohn’s Diseases
and
Ulcerative Colitides
Traditional Clinical Parameters:
CDCD
Genetic markers
Serum immune markers
Cytokine profile
Enzyme activity
Metabolite levels
Genetic, Serologic, and Biochemical Profiles:

Role of Biomarkers in IBD
• Disease Classification
• Disease Activity
• Prognosis

Defining IBD
CDCDUCUC
20th Century
Classic names
Abreu MT, et al. Clin Perspect Gastroenterol. May/June 2001;155-164.
IBD1IBD1 IBD2IBD2 IBD3IBD3 IBD4IBD4
SevereDisease
MildDisease
21st Century
Names based on mechanisms

IBD Serologies
pANCA
ASCA
OMPc
Anti-I2
CBir1

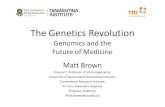
Differential Diagnosis: Serological Markers
Quinton J-F et al. Gut. 1998;42:788.
% P
atie
nts
wit
h P
osi
tive
AS
CA
and
AN
CA
Tes
t R
esu
lts
100
80
60
40
20
0CD UC Miscellaneous Controls
(n=100) (n=101) non-IBD (n=163) (n=28)
Anti-saccharomycescervisiae antibody(ASCA)
Perinuclear anti-neutrophilcytoplasmic antibody(p-ANCA)
ASCA Specific for CD
ANCA Sensitive For Colitis

Per
cen
tag
e (%
)
100
40
60
20
80
6969
9191
7878
50505656
4444
8888
6060
Accuracy of ANCA and ASCA to Differentiate UC from CD
Peeters M, et al. Am J Gastroenterol. 2001;96:730-734.
ASCA+(CD)
pANCA+(UC)
ASCA+/pANCA-(CD)
pANCA+/ASCA-(UC)
0
Sensitivity Specificity PPV
9595 94949797
9191

The Value of Serologic Markers in Indeterminate Colitis (IC)
Study Design: 97 patients with IC from 3 centers analyzed for pANCA and ASCA Patients prospectively analyzed since 1996 Follow-up time from inclusion 1 year for each patient Mean disease duration at time of publication, 10.7 years
Marker Diagnosis Sensitivity Specificity PPV NPV
ASCA+/pANCA– CD 67% 78% 80% 64%
ASCA–/pANCA+ UC 78% 67% 64% 80%
Joossens S, et al. Gastroenterology. 2002;122:1242-1247.

The Value of Serologic Markers in IC
pANCA+/ASCA–
ASCA+/pANCA–
Standard Markers
70%UC
67%CD
PPVDiagnosis
83%
75%
PPV
pANCA+/ASCA-/OmpC-
/I2-
OmpC
New Markers
72% remain IC
Joossens SB, et al. Gastroenterology. 2003;124(suppl1):A-323. Abstract M1174.

Summary of pANCA/ASCA
• pANCA is sensitive for “colitis”– Does not differentiate UC from CD– High titers associated with risk of pouchitis
• ASCA is specific for “classic” (small bowel) Crohn’s– Rarely positive in indeterminate colitis without
small bowel disease

Antibody AntigenNon-
IBD (%)CD (%)
UC (%)
DNase Sensitive pANCA
Histone H1, bacterial antigen?
<5%10–25%
50–65%
ASCA
Anti-Saccharomyces cerevisiae antibody
5%55–65%
5%
OmpC E. coli <5%38–50%
2%
Anti-I2Pseudomonas fluorescens
<5% 54% 2%
Anti-Flagellin CBir 1 Antigen 8-14% 50% 6%
IBD Specific Serologic Immune Markers

Interrelationships of Serum Immune Responses toMicrobial Antigens in CD
ASCA+
I 2 +
OmpC+
Landers et al, Gastro. 123:689-699, 2002
All Negative22%
12%
2%
7%26%
9%
9% 13%
CBir1???

Serology as a predictor of Disease Behavior

0
20
40
60
80
100F
req
ue
ncy
of
Dis
ea
se B
eh
av
ior
%
Number of Immune Responses
Antibody Sum and Disease Behavior
NPNSIPS
* Odds Ratio
0N=199
1N=262
2N=194
3N=57
Surgery
P trend < 0.0001
*2.2
*1.0
*5.0
*9.5
*1.7
*1.0
*4.2
*6.1
P trend < 0.0001
Dubinsky et al, Gastroenterology 2007; 132: 82

ASCA and Surgery
Amre et al, Am J Gastroenterol. 2006;101:645.
Significant difference in time to first surgery observed in patients ASCA positive
Time in Days
Pro
po
rtio
n A
cqu
irin
g F
irst
S
urg
ery
5000 1000 20000.00
0.25
0.50
0.75
1.00
P < 0.001
Either ASCA negativeEither ASCA positive

56
22 16
22
19
6
0
10
20
30
40
50
60
70
80
90
High (100) Medium (40-100)
Low (< 40)
Acute pouchitis
Chronic pouchitis
78 %
22 %
High Level Pre-operative pANCA Predicts Chronic Pouchitis
Incidence of Pouchitis (%)
41 %
P=0.03
Fleshner PR et al., Gut 2001;49

IBD-7 Panel
• Combines pANCA/ASCA/OmpC/Anti-I2/CBir1 profiles
• Provides composite prediction of UC/CD patterns vs. non-IBD
• Does NOT provide individual probabilities
• Not clinically intuitive– e.g. Low titer OmpC + alone may predict UC?

New serologic markers: carbohydrate antigens
Anti-glycan antibodies:• Anti-laminaribioside
carbohydrate (ALCA)• Anti-chitobioside
carbohydrate (ACCA)• Anti-mannobiodside
(AMCA)
• IgG gASCA• IgA Omp
ALCA8.9%
2.7%
4.9%
8.0%
15.9%
AMCA
6.8%
ACCA
gASCA positive CD
n=515
Ferrante M, et al. DDW 2006, Los Angeles. Abstract #129
913 well-characterized patients
Only gASCA 43.9%
8.9%

Serological markers can be used to discriminate IBD vs non-IBD
gASCA ALCA ACCA AMCA
Sens Spec PPV Sens Spec PPV Sens Spec PPV Sens Spec PPV
CD vs UC 56 90 95 18 93 90 21 85 82 28 82 84
IBD vs non-IBD
GI45 98 100 15 99 99 19 84 93 26 93 98
IBD vs HC 45 99 100 15 99 98 19 86 89 26 91 95
CSS ≥1.0 CSS ≥1.5 CSS ≥2.0 CSS ≥2.5
Sens Spec PPV Sens Spec PPV Sens Spec PPV Sens Spec PPV
CD vs UC 74 61 86 54 83 91 37 93 94 20 97 96
IBD vs non-IBD
GI66 82 98 45 98 100 30 100 100 16 100 100
IBD vs HC 66 86 97 45 99 99 30 100 100 16 100 100
Individual markers
Combined scores
Ferrante M, et al. DDW 2006, Los Angeles. Abstract #129

Serological markers to carbohydrate Ags can be used to predict CD course
42.0
71.7
83.2
56.0
0
25
50
75
100
Group A(n=181)
Group B(n=200)
Group C(n=184)
Group D(n=173)
Complicated disease course
OR: 2.00p=0.001
OR: 1.96p=0.010
Ferrante M, et al. DDW 2006, Los Angeles. Abstract #129
% p
atie
nts
38.1
58.2
79.8
49.0
0
25
50
75
100
Group A(n=181)
Group B(n=200)
Group C(n=184)
Group D(n=173)
Need for abdominal surgery
OR: 1.56p=0.033
OR: 1.45p=0.072
OR: 2.81p<0.001
Score <1.5
Score 1.5 or 2.0
Score 2.5 or 3.0
Score >3.0
Score <1.5
Score 1.5 or 2.0
Score 2.5 or 3.0
Score >3.0
OR=odds ratio; p-value (Chi-square)
OR: 1.76p=0.006

Serologic Markers: Current Status
• pANCA is sensitive for colitis and high titers are bad prognosis for pouchitis
• ASCA is specific for small bowel Crohn’s disease and high titers are bad prognosis for transmural complications
• OmpC, Anti-Flagellin and I2 add sensitivity and specificity for Crohn’s disease
• Predictive value is too low for clinical utility

ECCO Recommendations
• No evidence based recommendation can be made with regards to the routine clinical use of:- genetic tests- stool markers- serologic markers (ASCA, ANCA,…ompC, I2, flagellin)- permeability testing- Phenotype driven classifications
• (5,D)

C-Reactive Protein
• High CRP better separates placebo from drug responders– Natiluzimab, CDP-571, CDP-870, Infliximab,
Adalimumab, HuZaf
• No distinct cut-off for CRP• Other biologic markers if low CRP
– Fistula response, mucosal healing?
• Currently not a regulatory criteria but improves “efficiency” of trials

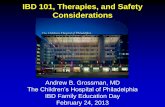
CDAI and CRP Relationship at Baseline
(logarithmic scale)
Baseline CDAI
150 200 250 300 350 400 450 500
Lo
g C
RP
mg
/L
0.01
0.1
1
10
100
1000

How to assess/treat these patients?CDAI/CRP at Baseline
ULN
High CDAI-High CRP
High CDAI-Low CRP
Low CDAI-High CRP
Low CDAI-Low CRP
Baseline CDAI
150 200 250 300 350 400 450 500
Log C
RP
mg/L
0.01
0.1
1
10
100

How to assess/treat these patients?CDAI/CRP at Baseline
ULN
High CDAI-High CRP
High CDAI-Low CRP
Low CDAI-High CRP
Low CDAI-Low CRP
Baseline CDAI
150 200 250 300 350 400 450 500
Log C
RP
mg/L
0.01
0.1
1
10
100
High Responder

How to assess/treat these patients?CDAI/CRP at Baseline
ULN
High CDAI-High CRP
High CDAI-Low CRP
Low CDAI-High CRP
Low CDAI-Low CRP
Baseline CDAI
150 200 250 300 350 400 450 500
Log C
RP
mg/L
0.01
0.1
1
10
100
High PlaceboResponse

How to assess/treat these patients?CDAI/CRP at Baseline
ULN
High CDAI-High CRP
High CDAI-Low CRP
Low CDAI-High CRP
Low CDAI-Low CRP
Baseline CDAI
150 200 250 300 350 400 450 500
Log C
RP
mg/L
0.01
0.1
1
10
100
ClinicalRemission

How to treat these various patients?CDAI/CRP at Baseline
ULN
High CDAI-High CRP
High CDAI-Low CRP
Low CDAI-High CRP
Low CDAI-Low CRP
Baseline CDAI
150 200 250 300 350 400 450 500
Log C
RP
mg/L
0.01
0.1
1
10
100Early Relapse

Conclusions CRP
• CRP is a predictor of placebo response
• Efficacy signals in recent clinical trails may have been obscured by placebo responses in CRPlow patients

ECCO Recommendations Regarding CRP
• Serum levels of CRP are useful to assess the patients’ risk for a relapse (B).
• High CRP levels are indicative of active disease (B) or a bacterial complication (C).
• CRP levels can be assessed to guide therapy and follow up (B).