Aoca 448B 71.87 7L.'55YÄ (1500B) 108B era era (3m Isog E*L ...
Upload
randell-morris-richardsonCategory
view
214download
0
BIO 448B: Dengue and Yellow Fever
Date: February 4th, 2008
Presented by: Ashley & Emma

DENGUE: Transmission How does it occur:
Dengue virus belongs to the family, Flaviridae Included in this family are Yellow Fever Virus,
Hepatitis C Virus, West Nile Virus and Japanese Encephalitis Virus
Single stranded, enveloped RNA virus that is 11 000 bases in length
Dengue is transmitted from infected to susceptible humans by the day-biting female Aedes sp. mosquitoes
NOT through human to human contact
Prevention: Stagnant bodies of water serve as breeding sites for the
mosquitoes therefore limiting their access to such environments is key to control of the disease through control of the vector

DENGUE: Reservoir Humans act as an amplifying host for the
Dengue virus
Virus replicates in Aedes sp. mosquito midgut and other organs, infects and replicates in salivary glands Vertical transmission to mosquito
offspring, this can be repeated for a few generations without the adults feeding on an infected host.
The significance of a sylvatic reservoir in wild monkeys has not yet been established.
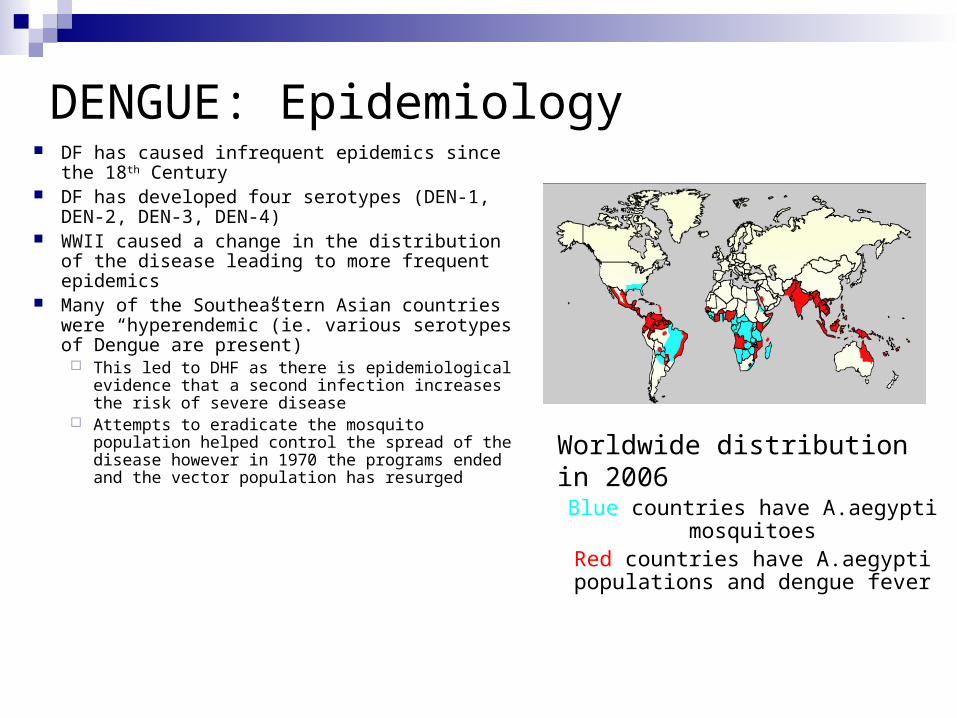
DENGUE: Epidemiology DF has caused infrequent epidemics since the
18th Century DF has developed four serotypes (DEN-1, DEN-
2, DEN-3, DEN-4) WWII caused a change in the distribution of the
disease leading to more frequent epidemics Many of the Southeastern Asian countries were
“hyperendemic”(ie. various serotypes of Dengue are present) This led to DHF as there is epidemiological
evidence that a second infection increases the risk of severe disease
Attempts to eradicate the mosquito population helped control the spread of the disease however in 1970 the programs ended and the vector population has resurged
Worldwide distribution in 2006Blue countries have A.aegypti
mosquitoesRed countries have A.aegypti populations and dengue fever
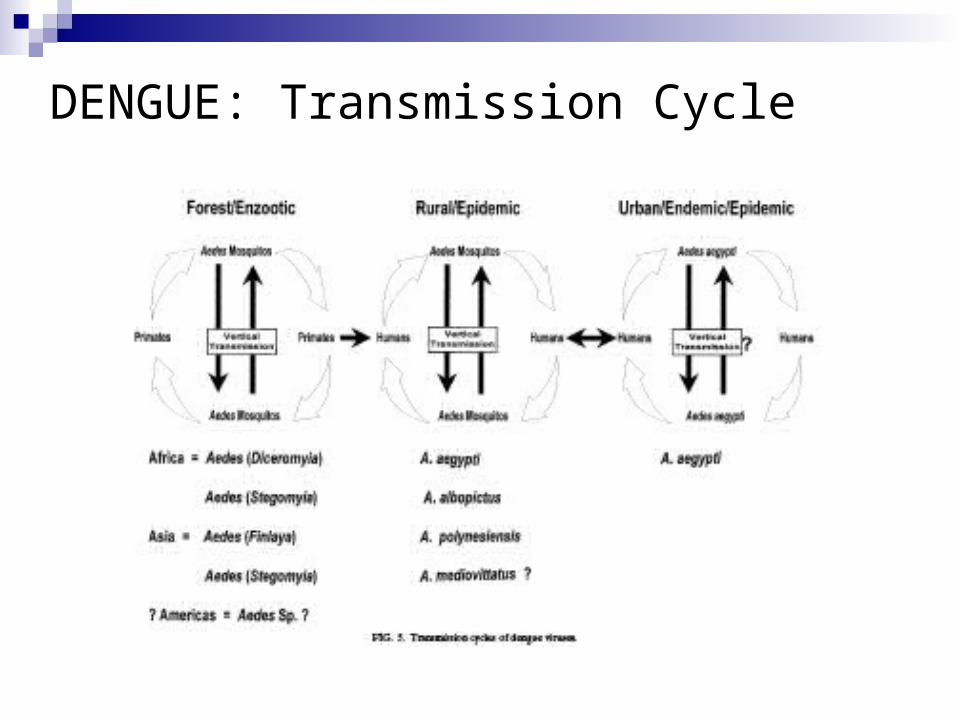
DENGUE: Transmission Cycle

DENGUE: Clinical Features Dengue Fever (DF):
Begins abruptly 3-15 days after bite
The “break bone” fever will resolve in a couple of days and then rebound (saddleback temperature curve)
Accompanied by severe headaches, weakness, retro-orbital pain, intense muscle and joint pain
Heart rate may be lower then expected with the high temperature (relative bradycardia/Faget’s sign)
Transient flushing and pale pink rash is common and is normally seen on starting on the trunk and can be seen on the face
Bleeding is not uncommon with DF and this may be seen as gum bleeding, nose bleeding, GI bleeds and heavy menstrual bleeding
Dengue Fever is a disease typically seen in adults and older children
Self limiting, lasts 4-7 days, followed by complete recovery
DENGUE: Clinical Features Dengue Hemorrhagic Fever (DHF):
DHF show similar symptoms to the onset of DF more serious signs and symptoms appear as the infection progresses
In DHF there is an increased vascular permeability due to host immune factors such as cytokines and chemokines
Increased vascular permeability leads to a decrease in plasma volume this can be seen clinically with a high hematocrit (proportion of RBC compared with blood volume)
Thrombocytopenia (decreased platelets) as well as elevated Aspartate aminotransferase is common
Post mortem studies have shown extensive liver damage which can cause disruption in clotting mechanism and well as an increase in AST
Signs of problematic clotting and hemorrhage include skin hemorrhage (petechiae), nose bleeds, lower GI bleeding (blood in stool), hematuria and more severe bleeding may occur with fresh blood bleeds from upper GI track

DENGUE: WHO grading of DHF
I: Positive tourniquet test and/or easy bruising II: Spontaneous bleeding III: Early signs of circulatory failure IV: Profound shock
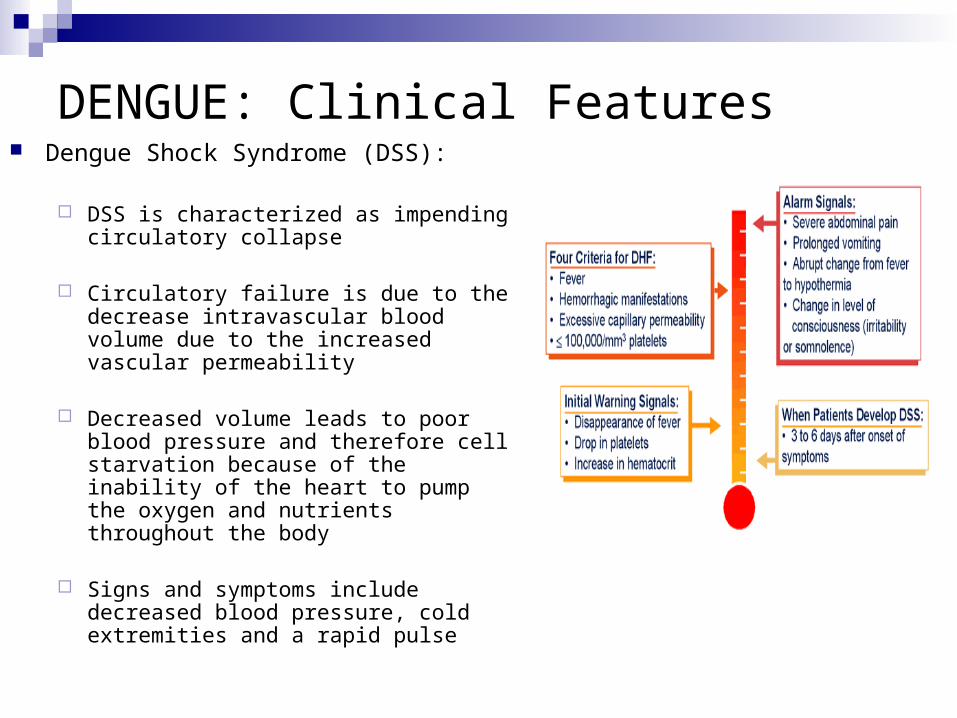
DENGUE: Clinical Features Dengue Shock Syndrome (DSS):
DSS is characterized as impending circulatory collapse
Circulatory failure is due to the decrease intravascular blood volume due to the increased vascular permeability
Decreased volume leads to poor blood pressure and therefore cell starvation because of the inability of the heart to pump the oxygen and nutrients throughout the body
Signs and symptoms include decreased blood pressure, cold extremities and a rapid pulse
DENGUE: Diagnosis Diagnosis of Dengue is done through
serological tests that are unavailable in many of the areas that the disease is prevalent
Bedside test reporting IgM and IgG are being developed however the accuracy of the tests are unknown
Bedside tests are being improved upon to make surveillance easier thereby aiding in proper diagnosis and tracking of the disease
PCR genome amplification is also an option but also requires sophisticated equipment

DENGUE: Management Treatment is supportive => no antivirals for Dengue Patient with DF:
Avoid being bitten until fever has subsided Bedrest Avoidance of Asprin due to its potential to worsen the
bleeding other analgesics maybe used for muscle pain Patients with DHF or DSS
Management of vascular permeability through the use of IV fluids and plasma expansion (Albumin and Blood products may be given if available)
Corticosteriods have been used for their anti immune effects thereby decreasing vascular permeability however they are shown to have no significant effect

DENGUE: Prevention & Control The emphasis of prevention is controlling the vector
In the past large group efforts have eradicated the mosquito population with the use of DDT however once the effort stopped the population returned as did Dengue
Larval habitats can be treated with insecticide. Insecticidal space sprays, using vehicle-mounted or portable machines, are used for emergency control
Community approach of education and ridding domestic areas of stagnant water has shown to be effective and sustainable but slow
A “top down bottom up” approach has been discussed allowing for fast and sustainable eradication of the vector population

DENGUE: Vaccine No vaccine for Dengue …yet.
WHO designated the development of a vaccine that would encompass all four strains a priority
Live attenuated vaccine is in clinical trials in Thailand
Molecular technology has been incorporated in hopes of finding a vaccine against Dengue
DNA vaccine have shown most promise, however the risks associated with DNA vaccines are unknown
DENGUE: Discussion
What are some of the challenges that might have come up when trying to create a vaccine for Dengue Fever?
In the Gubler paper it talks about the epidemiology for Dengue being only tracked as DHF. A foreseeable problem with this is that even though this is a more severe form of the disease it underestimates numbers of infected/affected individuals with dengue fever. As well, DHF is more prevalent in children and since children may have less of an impact on economic productivity,"DALY"s, and therefore morbidity there may be an underreporting that costs the education and eradication efforts funding.

YELLOW FEVER: Transmission Yellow fever is a single serotype enveloped, RNA virus of the
flavivirus family
The vector of this arbovirus is the Aedes aegypti mosquito
No human to human transmission
The virus affects humans and monkeys
Jungle Yellow fever occurs when humans are in the jungle where the virus is normally transmitted from vector to monkey
Urban Yellow fever occurs when mosquitos breed near plastic container in urban centres; virus is transmitted human to human via the mosquito

YELLOW FEVER: Transmission Cont’d
YELLOW FEVER: Epidemiology Yellow fever is common in Africa and South
America => WHO estimates 200,000 cases/year
There are five genotypes (two are S. American and the other three African)
Yellow fever is the first vector-borne viral disease discovered and the ‘original’ viral hemorrhagic fever
There is evidence that it has been around for 3000 years.
Most of the fatalities associated with Yellow fever occur in Africa and are due to poor vector control and in people without access to vaccines
Deaths are associated in unvaccinated travellers

YELLOW FEVER: Epidemiology Cont’d

YELLOW FEVER: Epidemiology Cont’d

YELLOW FEVER: Epidemiology Cont’d Countries requiring proof of yellow fever vaccination from all travellers: Benin Burkina Faso Cameroon Central African Republic Congo Côte d'Ivoire Democratic Republic of the Congo (formerly Zaire) French Guiana Gabon Ghana Liberia Mali Niger Rwanda Sao Tome and Principe Togo Source: International Travel and Health, 2000, World Health Organization

YELLOW FEVER: Pathogenesis
Mosquito bite leading to the inoculation of the virus in the host
Virus will move to the lymph nodes and disseminate towards the target organs
Liver is shown in monkey model to be infected 24 hours post inoculation => midzonal liver cells undergo apoptosis leading to death without inflammation
Kidney cell will also undergo tissue changes that will eventually lead to disruption of the Bowmann’s capsule =>lead to proteins being excreted through the patient’s urine
Cytokines will cause hypotension and shock Hypotension will lead to further kidney damage due to a
decreased perfusion of the renal tubules and this will lead to renal failure with associated decrease urine output

YELLOW FEVER: Clinical Features The extent of Yellow fever varies from non specific illness
to liver and kidney failure
First signs and symptoms are fever, chills, malaise, muscle and back pain
Patients will have relative bradycardia for their elevated temperature (Faget’s Sign)
There may be a brief remission followed by more severe symptoms of vomiting, abdominal pain, dehydration, jaundice, decreased urine output, hypotension and haemtemesis (vomiting of blood)

YELLOW FEVER: Diagnosis Yellow fever is difficult to recognize, especially during the early
stages:
It can easily be confused with malaria, typhoid, rickettsial diseases, haemorrhagic viral fevers (e.g. Lassa, Ebola, Crimean Congo), arboviral infections (e.g. Dengue), leptospirosis, viral hepatitis and poisoning (e.g. carbon tetrachloride).
A laboratory analysis is required to confirm a suspect case. Blood tests (serology assays such as ELISA) can detect yellow
fever antibodies that are produced in response to the infection. Several other techniques such as PCR and antigen assays are
used to identify the virus itself in blood specimens or liver tissue collected after death.
These tests require highly trained laboratory staff using specialized equipment and materials.
YELLOW FEVER: Management Supportive therapy is given to a patient diagnosed with
Yellow Fever
Aggressive fluid management and electrolyte balance is key as the patient’s kidneys may not be functioning optimally
Patients that are hemorrhaging may require blood or blood products to help with anemia and decreased blood volume
Dialysis will be required for patients in renal failure

YELLOW FEVER: Vaccine The single-dose 'live attenuated' vaccine
for yellow fever is safe and effective Passaged through eggs to attenuate,
vaccine is produced in eggs
It is recommended for individuals 9 months of age and older.
The vaccine becomes protective after 10 days, and provides immunity to a vaccinated individual for 10 years or more.
For individuals who are pregnant, immuno-suppressed or allergic to eggs, the yellow fever vaccination may not be recommended.

YELLOW FEVER: Discussion It has been shown that mosquitoes can pass the
Yellow Fever virus vertically to their offspring. Why do you think that this is important and what sort of implications might this have for your control measures?
Do you think that viruses with mosquito vectors should pool some funding to increase education and safe domestic areas for the inhabitants of mosquito areas? **Malaria research get 17 times the funding that dengue gets.