Bernardo Rapoport - MASCC · 2018-07-16 · BL Rapoport Disclosure Company Name Advisory Honoraria/...
37
Febrile Neutropenia – Guidelines Update and Approach to Management of Both High- and Intermediate-Risk PaBents Bernardo Rapoport The Medical Oncology Centre of Rosebank, Johannesburg and Department of Immunology, Faculty of Health Sciences, University of Pretoria SOUTH AFRICA
Transcript of Bernardo Rapoport - MASCC · 2018-07-16 · BL Rapoport Disclosure Company Name Advisory Honoraria/...

FebrileNeutropenia–GuidelinesUpdateandApproachtoManagementofBothHigh-and
Intermediate-RiskPaBents
Bernardo Rapoport
TheMedicalOncologyCentreofRosebank,Johannesburg
andDepartmentofImmunology,FacultyofHealthSciences,UniversityofPretoria
SOUTHAFRICA

BL Rapoport Disclosure Company Name Honoraria/
Expenses
Consulting/ Advisory
Board
Contract Research
Funded Research
Royalties/ Patent
Stock Options
Ownership/ Equity Position
Employee
Other (please specify)
Merck & Co., Inc x x x Speakers’ bureau
Roche x x x x Speakers’ bureau
Sandoz x x x
Tesaro x x x x Speakers’ bureau
Teva x x Speakers’ bureau
Heron Therapeutics x x
BMS South Africa x x x Speakers’ bureau
Novartis South Africa x x x Speakers’ bureau
Amgem South Africa x x x Speakers’ bureau
Bayer South Africa x x x Speakers’ bureau
Merck Serono S.Africa x x
Astellas South Africa x x Speakers’ bureau
Sanofi Aventis S. Africa x x x
Astra Zeneca S. Africa x x x Speakers’ bureau
Eli-Lilly South Africa x

• Despitemajoradvancesinpreven1onandtreatment,FNremainsoneofthemostfrequentandseriouscomplica1onsofcancerchemotherapy
• Majorcauseofmorbidity,healthcareresourceuse
• Compromisedtreatmentefficacyresul1ngfromdelaysanddosereduc1onsofcancerchemotherapy
• MortalityfromFNhasdiminishedsteadily,butremains
significant
Introduction

4
G.P. Bodey, Ann Int Med, 1966
The risk of infection increases with the severity and duration of neutropenia

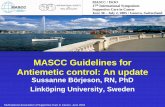
Complications of Myelosuppressive Cancer Chemotherapy
Kuderer NM et al. Cancer 2006;106:2258–2266 Chirivella I et al. J Clin Oncol 2006;24;abstract 668
Bosly A et al. Ann Hematol 2007
Myelosuppressive chemotherapy
Febrile neutropenia (FN) Chemotherapy dose delays and dose reductions
Decreased relative dose intensity (RDI)
Complicated life-threatening infection and prolonged hospitalization
Neutropenia
Reduced survival
Short-termeffects Long-termeffects

Thereisaclearrela1onshipbetweentheseverityofneutropenia(whichdirectlyinfluencestheincidenceofFN)andtheintensityofchemotherapyCurrently,thedifferentregimensareclassified• Highrisk(>20%)
• Intermediaterisk(10%–20%)
• Lowrisk(<10%)ofFN
ESMO Guidelines Neutropenia Risk

• Lymphoma R-ICE • Adjuvantbreast FEC100• Adjuvantbreast FEC100T• Neo-adjuvantorAdjuvantbreast TAC• BurkiXsLymphoma R-CODOX-M• Bladder MVAC• Sarcoma MAID• Sarcoma Doxorubicin-ifosfamide• Small-celllungcancer CAE• Tes1cularcancer VIP
FNRiskof>20%

MorethanhalfoftheFNepisodesoccurinthefirstcycleofchemotherapy

• Star1ngwiththefirstcycleandcon1nuingthroughsubsequent
cyclesofchemotherapyisrecommendedinpa1entswhohaveanapproximately20%orhigherriskforfebrileneutropeniaonbasisofpa1ent-,disease-,andtreatment-relatedfactors
• PrimaryCSFtheprophylaxisshouldalsobegiveninpa1entsreceivingdose-densechemotherapywhenconsideredappropriate
PrimaryProphylaxiswithaCSF

FNRiskof10-20%

• AgeplaysamajorroleintheriskofFNanditscomplica1ons
• Olderpa1entshaveahigherriskofFNfollowingchemotherapy
• Olderpa1entshavetheworsemorbidityandmortalityrates
• RiskofFNanditscomplica1onsincreaseswhenoneorseveralco-morbidi1esarepresentinthepa1ent
ESMO Guidelines Age and co-morbidities

• FNcanbeeffec1velypreventedbytheuseofG-CSFs• ItisrecommendedtouseG-CSF’sinpa1entsreceiving
chemotherapieswitha10-20%riskofdevelopingFN
• Seriousco-morbidi1esand/oraged>60years
• Dosereduc1ondeemeddetrimentaltooutcome
FN Prophylaxis

Prophylac1cG-CSFforpa1entswithdiffuseaggressivelymphomaage65yearsandoldertreatedwithcura1vechemotherapy(CHOP-R)shouldbeconsidered,par1cularlyinthepresenceofcomorbidi1es
CSFforpaBentswithdiffuseaggressivelymphomaage65yearsandolder

MulBpleChronicCondiBons• InthecaseofFN,observa1onalstudieshaveprovidedimportant
informa1onabouttheimpactofcomorbidity
• A2014systema1creviewreportedthatthepresenceofcomorbidcondi1onsincreasedtheriskofFNamongpa1entswithcancertreatedwithchemotherapy
• Comparedwithpa1entswithnocomorbidcondi1ons,pa1entswiththreeormorecomorbidcondi1onshadan81%increasedriskofFN
• Thepresenceofrenal,hepa1c,andcardiovasculardiseasehaveeachbeenassociatedwithFNorFN–relatedhospitaliza1on

• Advanceddisease• HistoryofpriorFN• Noan1bio1cprophylaxisorG-CSFuse• Mucosi1s
• PoorPS• Cardiovasculardisease
ESMO Guidelines Neutropenia Risk
Other Risk Factors

• Isrecommendedforpa1entswhoexperiencedaneutropenic
complica1onfromapreviouscycleofchemotherapy(forwhichprimaryprophylaxiswasnotreceived)
• Areduceddoseortreatmentdelaymaycompromisedisease-freeoroverallsurvivalortreatmentoutcome
• Inmanyclinicalsitua1ons,dosereduc1onordelaymaybeareasonablealterna1ve
SecondaryProphylaxiswithG-CSFs

G-CSFsshouldnotberou1nelyusedforpa1entswithneutropeniawhoareafebrileG-CSFsshouldnotberou1nelyusedasadjunc1vetreatmentwithan1bio1ctherapyforpa1entswithuncomplicatedfeverandneutropenia
G-CSFsinAfebrilePaBentsGuidelineRecommendaBons

G-CSFsshouldbeconsideredinpaBentswithFN
• Prognos1cfactorsthatarepredic1veofpoorclinicaloutcomes• High-riskfeaturesincludeexpectedprolonged(>10days)• Profoundneutropenia(<0.1×109/L) • Ageolderthan65years• Uncontrolledprimarydisease • Pneumonia• Hypotensionandmul1organdysfunc1on(sepsissyndrome) • Invasivefungalinfec1on• Beinghospitalizedatthe1meofthedevelopmentoffever
HighRiskforInfecBon-AssociatedComplicaBons

KlasterskyJ,JClinOncol2000;18:3038–51.
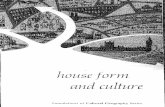
MASCCIndex
• Mul1na1onalAssocia1onforSuppor1veCareinCancer• Prospec1velyvalidatedtooltorapidlyassessriskbefore
accesstoneutrophilcount• Scores≥21areatlowriskofcomplica1onsMASCCscoring
index:– Burdenofillness:noormildsymptoms5– Burdenofillness:moderatesymptoms3– Burdenofillness:severesymptoms0– Nohypotension(systolicBP>90mmHg)5– Nochronicobstruc1vepulmonarydisease4– Solidtumour/lymphomawithnopreviousfungalinfec1on4– Nodehydra1on3– Outpa1entstatusatonsetoffever3– Age<60years(notvalidinchildren<18years)2
MASCCScore=26

• An1microbialshavebeenusedforalong1meforthepreven1onofepisodesofFNinchemotherapytreatedpa1ents
• Thisapproachhasbeensomewhatsuccessful
• Ledtotheemergenceofresistantstrains
• Limi1ngitsefficacy
Chemoprophylaxis

• GuidelinesfromtheEORTC&ASCOrecommendthatclinicianslimittheuseofan1bacterialprophylaxistopa1entsathighriskforFN
• Cochranemeta-analysiss1llrecommendedtheuseofciprofloxacin
orlevofloxacinincancerpa1entsundergoingintensivechemotherapy
• Othersrecommendavoidance
• Fluoroquinolones,shouldbediscouraged
Chemoprophylaxis

• Severalmeta-analysesindicatethatprimaryG-CSFprophylaxis(administeredaoercycle1)reducestheFNriskbyatleast50%insolidtumorspa1ents
• GuidelinesrecommendG-CSFbeadministeredprophylac1callyifthe
riskofFNis>20%
• FNintermediaterisk(10%–20%)considertheage,coexis1ngmorbidi1es,otherriskfactors
G-CSFprophylaxis

• Autologousstem-celltransplant Common
• Allogeneicstem-celltransplant Common
• Duringgraofailure Common
• AMLatDX 35%–48%
• ALLduringALLinduc1on 30%
ESMO Guidelines FNinhigh-risksituaBons

• Autologoustransplant 0%–10%
• Allogeneictransplant highlyvariable
• ALLduringinduc1on 2%–10%
• AMLduringthefirst2months 20%–26%
• Graofailure 80%
ESMO Guidelines FN-relatedmortalityinhigh-risksituaBons

• Autologoustransplant Yes
• Allogeneictransplant Yes
• Graofailure Yes
• AML No
• MDS No
• ALL Controversial
ESMO Guidelines G-CSF high-risksituaBons

TheUpdateCommiXeedidnotproviderecommenda1onsregardingtheuseofG-CSFsinadultswithacutemyeloidleukemiaormyelodysplas1csyndromes
AML+MDS

FN Management ESMO Clinical Practice Guidelines
Adapted from European Organisation for Research and Treatment of Cancer guidelines. FN, febrile neutropaenia; G-CSF, granulocyte colony-stimulating factor
Ann Oncol. 2016;27(suppl_5):v111-v118. doi:10.1093/annonc/mdw325

EvaluaBonPriortotheFirstCycleofChemotherapy

• Pegfilgras1matatotaldoseof6mg
• Equivalentdoseoffilgras1mis5μg/kg/dayfor∼10days
• EMA/FDAapprovedbiosimilarscanbeconsidered
G-CSFandpegfilgrasBmdoseschedule,routeofapplicaBon

G-CSFSideEffects
• BonePain 25%
• Painintheextremi1es 5-10%

G-CSFSideEffects

• PrimaryprophylaxiswithG-CSFisnotindicatedduringchemoradiotherapytothechestduetotheincreasedrateofbonemarrowsuppressionassociatedwithanincreasedriskofcomplica1onsanddeath
• ThereisalsoariskofworseningthrombocytopeniawhenG-CGFs
aregivenimmediatelybeforeorsimultaneouslywithchemotherapy
ESMOG-CSFContraindicaBons

FN risk ESMO ASCO NCCN Moderate to high (> 20 %)
Use G-CSFs Use G-CSFs Use G-CSFs
Intermediate (10-20 %)
Consider
Consider
Consider
Consider other risk factors
+++
++
++
Low (< 10 %)
Not
specified
Not
recommended
Not
recommended
Conclusion

ConclusionTakehomemessage
1. Myelosuppresivechemotherapyisassociatedwithseveremorbidityandmortality
2. ESMOGuidelines(ASCO&NCCN)recommendstheusageG-CSFtopreventFNandseriousinfec1vecomplica1onsassociatedwithchemotherapy
3. Clinicalevalua1onofpa1entsriskfactorswitheverycycleofchemotherapyisimpera1ve

Thank You

PersonalisedCancerCare

542-03-#37
QuesBons?