Benedetti F. Placebo and the New Physiology of the Doctor-patient Relationship

of 40
-
Upload
puntocom11 -
Category
Documents
-
view
221 -
download
0
Transcript of Benedetti F. Placebo and the New Physiology of the Doctor-patient Relationship
-
8/13/2019 Benedetti F. Placebo and the New Physiology of the Doctor-patient Relationship
1/40
PLACEBO AND THE NEW PHYSIOLOGY OF THEDOCTOR-PATIENT RELATIONSHIPFabrizio Benedetti
Department of Neuroscience, University of Turin Medical School, and National Institute of Neuroscience,
Turin, Italy
LBenedetti, Fabrizio. Placebo and the New Physiology of the Doctor-Patient Relation-ship. Physiol Rev 93: 12071246, 2013; doi:10.1152/physrev.00043.2012.Modern medicine has progressed in parallel with the advancement of biochemistry,anatomy, and physiology. By using the tools of modern medicine, the physician todaycan treat and prevent a number of diseases through pharmacology, genetics, and
physical interventions. Besides this materia medica, the patients mind, cognitions, and emotionsplay a central part as well in any therapeutic outcome, as investigated by disciplines such aspsychoneuroendocrinoimmunology. This review describes recent findings that give scientific evidence
to the old tenet that patients must be both cured and cared for. In fact, we are today in a good positionto investigate complex psychological factors, like placebo effects and the doctor-patient relationship, byusing a physiological and neuroscientific approach. These intricate psychological factors can be ap-
proached through biochemistry, anatomy, and physiology, thus eliminating the old dichotomy betweenbiology and psychology. This is both a biomedical and a philosophical enterprise that is changing the waywe approach and interpret medicine and human biology. In the first case, curing the disease only is notsufficient, and care of the patient is of tantamount importance. In the second case, the philosophicaldebate about the mind-body interaction can find some important answers in the study of placeboeffects. Therefore, maybe paradoxically, the placebo effect and the doctor-patient relationship can beapproached by using the same biochemical, cellular and physiological tools of the materia medica,which represents an epochal transition from general concepts such as suggestibility and power of mind
to a true physiology of the doctor-patient interaction.
I. WHAT IS A PLACEBO RESPONSE? 1207
II. WHAT IS THE DOCTOR-PATIENT... 1211
III. NEUROPHYSIOLOGICAL MECHANISMS... 1214IV. MECHANISM-BASED CLASSIFICATION... 1219
V. DISEASE-BASED CLASSIFICATION... 1221
VI. NEW EMERGING CONCEPTS... 1234
VII. UNRAVELING PLACEBO... 1238
I. WHAT IS A PLACEBO RESPONSE?
A. Placebos Were Introduced to Validatethe Efficacy of Medical Treatments
Ancient physicians have always used bizarre and odd treat-ments to cure their patients, with scarce, if any, knowledge ofanatomy and physiology. As the anatomical and physiologicaldetails of both the animal and the human body started emerg-ing, the need of a scientific explanation of many medical treat-ments became an imperative objective of physicians and thescientific community. An important historical period wherebyscientific skepticism emerged about the efficacy of some med-ical remedies is approximately in the second half of 1700 andinvolved treatments like mesmerism, perkinism, and homeop-athy (178).
To take mesmerism as an example, this was introduced in the
second half of 1700 by Franz Anton Mesmer, who claimed to
have discovered a healing fluid which he called animal magne-tism. To assess the very nature and the efficacy of mesmerism
in treating many diseasesand symptoms, Louis XVIappointeda commission that was headed by Benjamin Franklin. Thiscommission performed what can be considered one of the first
blind assessments and sham (placebo) interventions in the his-tory of medicine. Some women were blindfolded and askedwhere the mesmeric energy was being applied. As reported
by the members of the commission themselves, while thewoman was permitted to see the operation, she placed hersensations precisely in the part towards which it was directed;
that on the other hand, when she did not see the operation, she
placed them at hazard, and in parts very distant from thosewhich were the object of magnetism. It was natural to con-clude that these sensations, real or pretended, were determined
by the imagination(133, 178).Real mesmerism was found towork as well as sham mesmerism in a subsequent series ofexperiments, thus leading to the conclusion that the mesmeric
fluid had no existence and any effect was attributable to imag-ination.
In the same period, Elisha Perkins introduced perkinism, akind of healing procedure whereby two metal rods were
Physiol Rev93: 12071246, 2013doi:10.1152/physrev.00043.2012
1200031-9333/13 Copyright 2013 the American Physiological Society
http://-/?-http://-/?-http://-/?-http://-/?- -
8/13/2019 Benedetti F. Placebo and the New Physiology of the Doctor-patient Relationship
2/40
supposed to conduct pathogenic fluid away from the body.As done with mesmerism, one of the first sham (placebo)devices in the history of medicine was devised by replacingthe two metal rods with two sham wooden rods. Again, itwas found that both the metal and the wooden rods had thesame probability to induce clinical improvement (160,178), which indicates that the metal rods had no specifictherapeutic effects. Likewise, to test the efficacy of home-
opathy, a novel therapeutic approach introduced by SamuelHahnemann, whereby the belief was that a disease can becured by very small amounts of the same substances thatcause it, in the first half of 1800, bread pills (placebo) wereused by informing the patients that they were a homeo-pathic treatment (323, 178). A positive effect of bread pillswas found, and this was attributed to the natural course ofdisease and to imagination.
Many experiments and assessments of this kind were per-formed in the following years, and they were refined moreand more over time. Physicians became aware that the out-come of many therapies was nothing more than spontane-
ous remission or imagination, and they realized that rigor-ous trials were necessary to validate the efficacy of a medi-cament. The use of the word placebo (which in Latinmeans I shall please) in clinical research emerged gradu-ally over time to indicate a control group that receives asham treatment, as was done with sham mesmerism, shamrods in perkinism, and sham homeopathy. Therefore, thewordshamwas gradually replaced with the word placebo.Another important point that was crucial for the modernuse of placebos in clinical trials was the emerging awarenessthat even physicians and clinical investigators were suscep-tible to imagination and biases. This led to the use of thedouble-blind design, in which neither the investigator northe patient knew the nature of the tested therapy (it could beeither real or sham).
With these elements in their hands, modern clinical investi-gators use the randomized double-blind placebo-controlledtrial, which represents today the tenet of clinical researchfor the validation of a therapy. It contains most of theelements that are necessary to control for suggestion, imag-ination, and biases of both patient and investigator, and tocontrol for other confounding factors such as the spontane-ous fluctuations of diseases and symptoms.
B. Today the Placebo Effect, or Response, Isan Excellent Model to Understand Howthe Brain Works
Not only have placebos been used for the validation oftherapies, but they have also traditionally taken as an ex-ample of the powerful interaction between mind and body.For example, in mesmerism and perkinism, the main con-clusion was that imagination played a major role in thetherapeutic outcome, thus emphasizing the important role
of mind in the modulation of a number of physiologicalfunctions. Following this psychological perspective of theplacebo phenomenon, the placebo concept has permeatedthe psychology literature for many years (76, 156, 292, 293340).
Today placebo researchers tend to use the terms placeboeffectand placebo response interchangeably. Accordingly,
throughout this article I use these two terms as synonyms.In the course of the years, several factors have been consid-ered to be important in the placebo effect. For example,many elements are at work during a placebo response, suchas the relationship between the doctor and his patient, thepatients expectations and needs, the patients personalityand psychological state, the severity and discomfort of thesymptoms, the type of verbal instructions, the preparationcharacteristics, and the environmental milieu (281).
The importance of the mind-body interaction in the placeboeffect clearly emerges in the definition by Brody (76), whodefines the placebo effect as a change in the body, or thebody-mind unit, that occurs as a result of the symbolicsignificance which one attributes to an event or object in thehealing environment. It is important to emphasize that thepsychological conceptualization of the placebo has beenvery important in drawing our attention on what is reallyimportant (the meaning and the symbols of the healingenvironment), and deflecting it from what is not (the inertmedical treatments) (239, 240). Therefore, whereas in theclinical trial setting the conceptualization of placebo fo-cuses on distal and external factors, such as inert treat-ments and inert substances, in the context of psychologythe concept of placebo focalizes on proximal, and inter-
nal, factors, like symbolic representation and mind-bodyrelationship (269).
The merits of the psychological conceptualization of theplacebo effect as a mind-body phenomenon reside in thefact that it makes us understand that the placebo effect isdue to the psychosocial context around the patient and thetherapy. When a placebo (sham treatment), e.g., an inertsubstance like water, is administered, what matters is notthe water, of course, but its symbolic significance, whichcan be attached to practically anything (76). In this sense,the concept of placebo has shifted from the inert content
of the placebo agent to the concept of a simulation of anactive therapy within a psychosocial context.
On the basis of these considerations, when a treatment isgiven to a patient, be it sham or real, it is not administeredin a vacuum, but in a complex set of psychological statesthat vary from patient to patient and from situation tosituation. For example, when a placebo is given to relievepain, it is administered along with a complex set of psycho-social stimuli which tell the patient that a clinical improve-ment should be occurring shortly (FIGURE 1). These psycho-
FABRIZIO BENEDETTI
1208 Physiol Rev VOL 93 JULY 2013 www.prv.org
http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?- -
8/13/2019 Benedetti F. Placebo and the New Physiology of the Doctor-patient Relationship
3/40
-
8/13/2019 Benedetti F. Placebo and the New Physiology of the Doctor-patient Relationship
4/40
of the causes behind the placebo improvement. Although thispragmatic approach is useful in clinical trials, if one is inter-ested in the mechanisms of the real psychobiological placeboeffect, it is necessary to separate it from other phenomena suchas spontaneous remission, regression to the mean, biases (43,44). For example, spontaneous remission is frequently anderroneously defined placebo effect. In fact, in many chronicconditions there is a spontaneous variation in symptom inten-sity that is known as natural history (128). If a subject takes aplacebo just before his symptom starts decreasing, one maybelieve that the placebo is effective, although that decreasewould have occurred anyway. Clearly, this is not a placeboeffect but a misinterpretation of the cause-effect relationship.To avoid this mistake, the natural history must be comparedwitha placebo treatment andan activetreatment. Whereasthedifference between the natural history and the placebo treat-ment represents the real psychological placebo component ofthe therapy, the difference between the placebo treatment andthe active treatment represents the specific component of thetherapy.
Similarly, regression to the mean is a statistical phenome-non that is often misinterpreted as a psychological placeboresponse. It assumes that individuals tend to have extreme
values of a physiological parameter, e.g., glucose, whenenrolled in a clinical trial, and then these extreme valuestend to be lower at a second measurement (97). In this casealso, the improvement cannot be attributed to any interven-tion they might have undergone. An important factor in theregression to the mean phenomenon is represented by theinclusion criteria in a clinical trial, which are often repre-sented by extreme physiological values.
Signal detection ambiguity can sometimes explain symptomreduction. In fact, according to the signal detection theory,
a false-positive error made by either the patient or the phy-sician may explain the illusory improvement occurring insome circumstances (12, 86). Likewise, sometimes patientsand doctors give biased reports of the clinical condition. Forexample, there is some evidence that patients often want toplease doctors for their time and effort to help them so thatsome exaggeration of their feelings of clinical improvementmay be reported (184). This can be overcome by usingobjective measurements, such as electrophysiological re-sponses or blood markers. Finally, cointerventions cansometimes be the cause of improvement. For example, anunidentified concomitant diet may be responsible for theclinical improvement during a placebo treatment.
For all these reasons, classical clinical trials are not good forunderstanding the mechanisms of real psychological pla-cebo effects, for all these phenomena are present in a clinicaltrial. As the context surrounding the patient and the therapyis the crucial factor in placebo responsiveness, and psycho-logical factors are at the core of its magnitude, we shouldnot be surprised that placebo effects in clinical trials arehighly variable. Again, this emphasizes the usefulness of theneuroscientific approach in the laboratory setting to clarifythe biology of different placebo responses, for in the labo-
ratory it is possible to manipulate the context and the pa-tients psychological state under strictly controlled condi-tions.
D. The Nocebo Effect Is the Opposite of thePlacebo Effect
Nocebos are opposite to placebo phenomena, for they in-volve the pathogenic effects of imagination and negativeexpectations. Nocebo phenomena were first described
Co-interventions
Placebo(sham treatment)
Natural
history
Regression
to the mean
Experimenters
and patients biases
Psychobiological
factors
Clinical Improvement
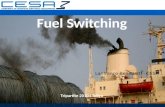
FIGURE 2. The clinical improvement that may be observed after placebo administration is due to many
factors. The real placebo response is attributable only to the psychobiological factors, namely, to psychological
and physiological changes in the patients brain.
FABRIZIO BENEDETTI
1210 Physiol Rev VOL 93 JULY 2013 www.prv.org
http://-/?-http://-/?-http://-/?-http://-/?- -
8/13/2019 Benedetti F. Placebo and the New Physiology of the Doctor-patient Relationship
5/40
within an anthropological context in tribal societies, andtaken as a good example of the power of mind. For exam-ple, in some aboriginal people of Australia, pointing a boneat someone may lead to negative outcomes, and in LatinAmerica and Africa, voodoo death has sometimes been re-lated to the belief of being bewitched (79). It should beemphasized that many of these phenomena are anecdotal(215); nonetheless, they can be explained as a stress-in-
duced activation of the sympathetic nervous system (79).Some anthropologists go further by proposing a sociocul-tural model of illness and healing, whereby placebos andnocebos are crucially involved (152, 153).
Nocebo phenomena and the impact of negative expecta-tions and imagination are not limited to the past and totribal societies, but they are also present in western societ-ies. For example, many side effects both in clinical trials andin clinical practice are psychological, and many healthwarnings by the media may induce negative expectationsand negative outcomes (18, 244, 277). Similarly, anticipa-tory nausea and vomiting in cancer chemotherapy, the neg-
ative effects of negative diagnoses, and patients distrusttowards conventional medicine, all represent examples ofnocebo and nocebo-like phenomena in western societies(159, 309)
The termnocebo(Latin I shall harm) was introduced todescribe the negative effects of placebos (259). However, itis important to stress that in modern terminology true no-cebo effects are considered as the result of negative expec-tations. This conceptualization of nocebo effects is particu-larly useful from a neuroscientific perspective, because no-cebo administration induces negative expectations andthese, in turn, are anxiogenic. In other words, a nocebo is astressor. Therefore, the nocebo response is a good model tounderstand anxiety, particularly anticipatory anxiety.
Not surprisingly, our knowledge about the mechanisms ofthe nocebo response still lags behind the more detailed un-derstanding of the placebo counterpart, mainly due to eth-ical constraints. Inducing negative expectations and inflict-ing pain is certainly unethical; thus many studies are carriedout on healthy volunteers rather than on patients, and neg-ative expectations are triggered without actual administra-tion of any substance (61, 90).
II. WHAT IS THE DOCTOR-PATIENTRELATIONSHIP?
Different disciplines have approached the doctor-patientrelationship, often also labeled patient-provider interactionor therapist-patient encounter, from different perspectives,including psychology, sociology, philosophy, and healthpolicy. What has emerged in the course of the years is thatnot only should health professionals learn technical skills,but they also should develop appropriate social skills to
better interact and communicate with their patients. Withthe recent advances of neuroscience, today we are in a betterposition to approach the doctor-patient relationship from abiological perspective and to consider it as a special type ofsocial interaction. Indeed, this new biological approach isquite interesting because the neurosciences are interested inunderstanding how brains work, and this special social en-counter may uncover the mechanisms of higher brain func-
tions, such as expectations, beliefs, trust, hope, empathy,and compassion. In addition, since any biological system isa product of evolution which has emerged in animals andhumans with a precise purpose, an evolutionary under-standing of why and how these social mechanisms haveemerged and evolved is of paramount importance, for theygive us insights into the relationship between the first socialinteractions in non-human primates and early hominidsand subsequent medical care.
A. The Doctor-Patient Relationship HasEmerged During Evolution as a Unique
Social Interaction
Many simple behavioral repertoires are aimed at protectingthe body from possible damage. For example, the with-drawal reflex and the scratch reflex protect from threaten-ing stimuli, and they are present in both invertebrates andvertebrates, including humans. However, from an evolu-tionary perspective, the two reflexes differ for at least oneimportant aspect. In fact, the scratch reflex is particularlyinteresting because, differently from the withdrawal reflex,the movement is aimed at targeting the potential noxiousstimulus and at removing it from the body. This representsan important evolutionary step toward the more complexbehavior of grooming, which involves behaviors such asscratching, licking, preening, rubbing, nibbling, and wal-lowing (46). Interestingly, whereas the scratch reflex is trig-gered by cutaneous stimuli, such as a bugs bite, grooming isa self-directed behavior that does not require the peripheralstimulation of the skin, for its biological function is the careof the body surface (49, 304). The more complex functionof grooming is also evidenced by the involvement of su-praspinal centers, whilst the scratch reflex only requires thespinal cord. The evolutionary step from the peripherallydriven scratch reflex to the centrally driven grooming be-havior shows how the nervous system developed from a
simple reflex act to a complex motor pattern for the care ofthe whole body surface.
But the big evolutionary jump to social behavior is repre-sented by allogrooming, i.e., taking care of the skin of oth-ers. In fact, not only do animals scratch, rub, and lick them-selves, but they scratch and rub their companions as well.Social grooming has a function in the regulation of socialrelationships, and it is not only involved in the care of bodysurface (304). Individuals who are virtually free of parasitesstill solicit for and submit themselves to being groomed.
PLACEBO AND THE DOCTOR-PATIENT RELATIONSHIP
121Physiol Rev VOL 93 JULY 2013 www.prv.org
http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?- -
8/13/2019 Benedetti F. Placebo and the New Physiology of the Doctor-patient Relationship
6/40
-
8/13/2019 Benedetti F. Placebo and the New Physiology of the Doctor-patient Relationship
7/40
many intricate mechanisms are at work, such as trust and
hope on the one hand and empathy and compassion onthe other. Physiology and neuroscience are beginning tounderstand these complex functions both in the patientsbrain, where expectations, beliefs, trust, and hope arekey elements, and in the doctors brain, in which em-pathic and compassionate behavior represents an essen-tial factor. Finally, the fourth step is when the patientreceives the therapy, the final and perhaps the mostimportant act of the doctor-patient interaction. The mereritual of the therapeutic act may generate therapeuticresponses through the patients expectations and beliefs(placebo responses), which sometimes may be as power-ful as those generated by real medical treatments. Today,these placebo responses can be approached from a bio-logical perspective, whereby the biochemical, anatomi-cal, and physiological link between expectation and ther-apeutic effect has been partially unraveled.
It can be seen in FIGURE 3 that these four steps can beconceived as a homeostatic system in all respects. Thefeeling of sickness is the variable to be controlled. It tellsa motivational system to seek relief. This is aimed atadopting the appropriate behavioral repertoire to elimi-nate the feeling of sickness. In a social group, such abehavioral repertoire is represented by the social contact
with the healer, whose role is to administer a relievingtreatment. It is crucial to understand that this system isalways at work, regardless of whether the healer admin-isters effective or ineffective therapies. Even if the ther-apy is totally ineffective, the patients expectation of ben-efit (the placebo response) may be sufficient to inhibitdiscomfort. The real difference between shamans andmodern doctors is that, whereas shamanic procedures arelikely to lack specific effects completely, at least in mostcircumstances, modern doctors rely on effective proce-dures and medications with specific mechanisms of ac-
tion. But this social-neural system is always there, as an
ancestral system which is ready to come out, both withshamans and with modern doctors.
C. What Is the Link Between Placebo andDoctor-Patient Relationship?
If we look at FIGURES 1 AND 3, the link between placeboand doctor-patient interaction appears straightforward.The main element in the psychosocial context around thepatient that leads to the placebo response is the doctor,and more in general the health professional. Indeed, any
element in FIGURE 1is related to the figure of the doctor,who uses communication, words, and medical instru-ments and administers pills, injections, and medications(41, 67). Likewise, the behavioral repertoire that is ad-opted by the patient inFIGURE 3is aimed at looking for adoctor, who represents the means for relieving discom-fort. Therefore, it is not surprising that a crucial elementthat triggers the placebo response comes from the veryspecial social encounter between the patient and his doc-tor. In FIGURE 3, the crucial steps that need to be ana-lyzed in depth are the third (meeting the therapist) andthe fourth (receiving the therapy). It is here that a new
physiology of the doctor-patient relationship and pla-cebo does emerge. Meeting the doctor involves plenty ofmechanisms in the patients brain that are responsible forexpectations, trust, and hope. Similarly, many mecha-nisms are at work in the doctors brain, such as empathyand compassion. In turn, these lead to the final step ofreceiving the therapy which, regardless of its effective-ness or ineffectiveness, triggers placebo responses. Thephysiological underpinnings of the third and fourthsteps of FIGURE 3 are described in depth in the nextsections.
FEELING SICK
Bottom-up processing (sensory afferents)
Top-down modulation (psychological influences)
SEEKING RELIEF
Motivation to suppress discomfort
Reward mechanisms
RECEIVING THE THERAPY
Placebo and nocebo mechanisms
Brain changes induced by therapeutic rituals
Mechanisms of expectation and learning
MEETING THE THERAPIST
The doctors brain (empathy and compassion)
The patients brain (trust and hope)
1 2
34
+
+
+-
FIGURE 3. The four steps of the doctor-patient relationship. The interaction between the healer/therapist
and his patient can be envisaged as a homeostatic system in which the variable to be controlled is represented
by the feeling of sickness (symptoms). The very act of administering a treatment is a psychological and socialevent that is sometimes capable of inhibiting a symptom such as pain, even though the treatment is fake.
PLACEBO AND THE DOCTOR-PATIENT RELATIONSHIP
121Physiol Rev VOL 93 JULY 2013 www.prv.org
http://-/?-http://-/?-http://-/?-http://-/?- -
8/13/2019 Benedetti F. Placebo and the New Physiology of the Doctor-patient Relationship
8/40
III. NEUROPHYSIOLOGICAL MECHANISMSINVOLVED IN THE INTERACTIONBETWEEN DOCTOR AND PATIENT
A. Exploring the Healers and theDoctors Brain
As the main components of the psychosocial contextaround the patient, the doctors words, attitudes, and be-haviors play a major role in the doctor-patient interactionand in the placebo responses. As briefly described above,altruism, empathy, and compassionate behavior emerged inmankind during the course of evolution, and the shamanassumed the role of caregiver. It is interesting to note thatfacial expressions are likely to have evolved for elicitingmedical attention from others (345). A greater facial ex-pression of pain in the presence of potential caregivers thanin their absence is of primary importance, so that the pres-ence of potential caregivers would prompt the release ofsuppression of pain facial expressions. This, in turn, triggers
the caregivers empathic and compassionate behavior. Thesocial connection between the suffering patient, who ex-presses his discomfort, and the empathic doctor is at thevery heart of the doctor-patient relationship. Empathy thusrefers to an intersubjective process through which the cog-nitive and emotional experiences of another come to beshared, without losing sight of the original source of theexperience (102). It is important to note that empathy isdistinguished from compassion (32, 117, 161). Empathy isnot necessarily linked to prosocial motivation, namely, theconcern about the others well being. In contrast, prosocialmotivation is involved in compassion. In fact, compassionenables individuals to enter into and maintain relationships
of caring and tends to motivate us to help people who areemotionally suffering. In the next sections, empathy andcompassion will be treated separately, for different neuralsystems are involved in these behaviors.
1. There are two different neural systemsfor empathy
Experimental evidence suggests that there are at least twomechanisms of empathy: emotional contagion and cognitiveperspective-taking (101). Whereas the former is thought tosupport our ability to empathize emotionally, i.e., to share the
other persons emotional feelings (I feel what you feel), thelatter involves complex cognitive components, whereby oneinfers the state of the other person (I understand what youfeel), also known as theory of mind (266), or mentalizing(136), or mindreading (29).
Several studies suggest that understanding others on thebasis of cognitive perspective taking and emotional conta-gion recruits different neural networks (161). FIGURE 4shows the two main systems that mediate empathic emo-tional ability on the one hand (light blue) and cognitive
perspective taking on the other (blue). Whereas cognitiveperspective taking activates the medial prefrontal regions,the superior temporal sulcus, the temporal pole, and thetemporo-parietal junction (135, 283), empathizing with an-other person has been found to activate somatosensory andinsular cortices as well as the anterior cingulate cortex(161). In a study by Singer et al. (296), the bilateral anteriorinsula and the rostral anterior cingulate cortex were acti-
Lateralhemisphere
Medialhemisphere
Cognitive perspective taking
ACC
iFG
MFC
TP
TPJ
vmPF
STSAI
SII
asPM
C
piPMC
Empathic emotional ability
Compassion for physical pain and admiration for skills
Compassion for social pain and admiration for virtue
FIGURE 4. Brain regions that are involved in empathy, compas-
sion, and admiration. During the doctor-patient relationship, severa
complex brain functions are involved, such as the doctors empathic
and compassionate behavior and the patients admiration/trust to-
wards the figure of the doctor. iFG, inferior frontal gyrus; AI, anteriorinsula; SII, secondary somatosensory area; TP, temporal pole; STS,
superior temporal sulcus; TPJ, temporal parietal junction; MFC,
medial frontal cortex; vmPF, ventromedial prefrontal cortex; ACC,
anterior cingulate cortex; asPMC, anterosuperior posteromedia
cortex; piPMC, posteroinferior posteromedial cortex.
FABRIZIO BENEDETTI
1214 Physiol Rev VOL 93 JULY 2013 www.prv.org
http://-/?-http://-/?-http://-/?-http://-/?- -
8/13/2019 Benedetti F. Placebo and the New Physiology of the Doctor-patient Relationship
9/40
vated when a female experienced pain herself as well aswhen she saw that her husband had experienced pain. Thesame group (297) showed that the empathic brain responsesin the anterior insula and anterior cingulate cortex were notrestricted to a beloved partner, but also occurred when anunknown but likable person was in pain, which has obviousimplications for the doctor-patient interaction.
The involvement of other regions was demonstrated in sub-jects with lesions either in the ventromedial prefrontal cor-tex or in the inferior frontal gyrus. In fact, a remarkablebehavioral and anatomic double dissociation between def-icits in cognitive empathy (ventromedial prefrontal lesion)and emotional empathy (inferior frontal gyrus lesion) wasfound (291) (FIGURE 4).
While pain is surely the modality that has been investigatedin more detail, similar empathic responses have also beendescribed in other modalities, like touch, taste, and disgust.For example, both observation of touch and first-hand ex-perience of touch activate the secondary somatosensory
cortex (182), and video clips showing people samplingpleasant and unpleasant tastes make observers experiencethe same tastes, along with activation in anterior insulacortex when both observing and experiencing disgust (174).
2. Compassion for social and physical pain involvestwo discrete neural systems
Compassion can be evoked by witnessing situations of per-sonal loss and social deprivation (social pain), or by wit-nessing bodily injury (physical pain). Whereas the formerpertains to social/psychological circumstances, the latter
has to do with immediate physical circumstances (173).Compassion for social and physical pain has been found toengage two different neural circuits. The former is associ-ated with strong activation in the inferior/posterior portionof the posteromedial cortices, whereas the latter produced alarger activation in the superior/anterior portion of the pos-teromedial cortices (173) (FIGURE 4). These neural net-works, one for the emotions related to someone elses psy-chological state and the other for the emotions related tosomeone elses physical state, are engaged by both compas-sion and admiration (see below).
It is interesting to note that compassionate concern towardsa suffering person is related to the motivation to help and,accordingly, a positive intrinsic reward feeling may occur asa result of experiencing compassion for others (303). In-deed, Kim et al. (185) found that compassionate attitudeactivated a neural network in the midbrain/ventral stria-tum/septal network region, a key region involved in proso-cial/social approach motivation and reward mechanisms.These findings emphasize the differences between empathicbehavior, which does not necessarily involve motivationalsystems, and compassionate behavior, whereby the motiva-
tion to alleviate others suffering represents the central ele-ment.
3. Doctors can habituate to others suffering
There is some experimental evidence that habituation toothers suffering occurs in clinical practice. This may haveevolved as a mechanism of self-control that is aimed at
reducing negative emotions while doctors watch the suffer-ing of their patients. This may be particularly true for thosehealth professionals involved in invasive and painful proce-dures. Indeed, Cheng et al. (83) conducted a functionalmagnetic resonance imaging study, in which they comparedphysicians who practice acupuncture with naive partici-pants (controls) while observing the insertion of needlesinto the mouth area, the hands, and the feet. The anteriorinsula, somatosensory cortex, periaqueductal gray, and an-terior cingulate cortex were significantly activated in thecontrol group, whereas the group of acupuncturist physi-cians did not show significant changes. The latter showedactivation of the medial and superior prefrontal cortices
and the temporoparietal junction, which are known to beinvolved in emotion regulation. The difference in brain ac-tivation between the two groups of naive and expert sub-jects is likely to reflect top-down processes related to pastexperience and practice with acupuncture.
B. Different Sensory Systems Are at WorkDuring the Doctor-Patient Interaction
Needless to say, the auditory/language systems play a criti-cal role in the doctor-patient relationship, for verbal com-munication represents one of the most important social in-
teractions between therapists and their patients. The doc-tors words and sentences may have a profound impact onthe patients psychological state. For example, some subtledifferences in verbal communication may produce differenteffects. There is compelling evidence that different sen-tences such as This painkiller may work or Rest assured,this painkiller does work may lead to different therapeuticoutcomes (41, 44). Besides this powerful verbal communi-cation, there are a number of sensory inputs that representthe basis of nonverbal communication, most notably visionand touch.
1. Visual stimuli are crucial innonverbal communication
Facial expressions represent an excellent source of informa-tion and play a fundamental role in signaling social inten-tions from which people infer meaning (134). Several brainregions are involved in detecting subtle differences in facialexpressions, and these regions make up a complex networkwhich is specifically aimed at processing facial emotions,whereas facial identity is processed by a different network(319). The specialness of face processing is shown by the
PLACEBO AND THE DOCTOR-PATIENT RELATIONSHIP
121Physiol Rev VOL 93 JULY 2013 www.prv.org
http://-/?-http://-/?-http://-/?-http://-/?- -
8/13/2019 Benedetti F. Placebo and the New Physiology of the Doctor-patient Relationship
10/40
fact that even a split-second glimpse of a persons face tellsus his/her identity, sex, mood, age, race, and direction ofattention (324). In human brain imaging studies, a numberof works support the idea that the lateral side of the rightmid-fusiform gyrus, the fusiform face area or FFA, isactivated robustly and specifically by faces (177, 324). Itshould be noted, however, that the fusiform face area doesnot respond only to face stimuli but also to non-face object,
albeit less robustly. The information that is gained fromfaces is fundamental for social interaction, including thedoctor-patient encounter, and some more details will bepresented in section IIIC1.
Eye contact, i.e., the mutual eye gaze that connects peopletogether, represents another important aspect of social in-teraction and solicits attention and interest of the interact-ing persons (290). Differently from other animals, wherebyeye contact may represent a potential threat (118), in hu-mans mutual eye gaze triggers attention and interest. Atleast five regions have been found to be activated more bydirect gaze than by averted gaze: the fusiform gyrus (or
fusiform face area), the anterior part of the right superiortemporal sulcus, the posterior part of right superior tempo-ral sulcus, the medial prefrontal cortex and orbitofrontalcortex, and the amygdala (290). These regions may be ac-tivated by direct gaze through different mechanisms, suchas the activation of the arousal system (179), the activationof a communicative intention detector (135), and the acti-vation of a subcortical face detection pathway (290).
Gestures and postures represent another important aspectof social interactions. The perceived behavior of others af-fects ones own behavior unconsciously. For example, peo-ple are likely to rub their face if their conversation partnerdoes so (81). When observing the gestures of others, one caninfer his intentions and, accordingly, adapt his own behav-ior. Mirror neurons are at the very heart of this social be-havior and play a critical role whenever the behavior ofothers is observed (279).
Nonverbal communication, as briefly described here fromfacial expressions to eye contact and from the observationof others gestures to guessing the others intentions, is crit-ical in any social encounter, including the special situationof the doctor-patient interaction. Nonverbal messages andintentions can be communicated either consciously or un-
consciously to others, and indeed gestural communicationmay have represented a primitive form of language, as sug-gested by some (278).
2. Emotionally meaningful tactile stimuli can makepain more bearable
Touch may convey strong emotional information in manycircumstances. For example, in section IIA we have seenthat social grooming is an important mediator of socialrelationships in nonhuman primates. The very act of
grooming, scratching, rubbing, and licking another mem-ber of the same social group is a complex concertation ofneural events that take place in both cortical and subcorticalareas. In humans, a powerful emotional tactile stimulus isrepresented by hand-holding, which can be considered anonverbal supportive social behavior in all respects. A studyinvestigating the biological effects of hand-holding was per-formed on married women who were subjected to the threat
of electric shock in three different conditions: while holdingtheir husbands hand, while holding the hand of an anony-mous male experimenter, or holding no hand at all (87).Holding the spouses hand produced a decrease in unpleas-antness ratings compared with no hand-holding, whilstholding the strangers hand did not decrease unpleasant-ness. Functional magnetic resonance imaging showed re-duced activation in right dorsolateral prefrontal cortex, leftcaudate-nucleus accumbens, and superior colliculus whenthe women held their husbands hand. All these areas arerelated to emotional and behavioral threat responses. Amore limited reduction of activation occurred when theyheld the hand of a stranger, e.g., in the ventral anterior
cingulate cortex, posterior cingulated and right postcentralgyrus. It is interesting to note that these effects of spousalhand-holding were related to marital quality: the higher themarital quality, the lesser the activation in the right anteriorinsula, superior frontal gyrus, and hypothalamus duringspouse hand-holding, but not during stranger hand-hold-ing.
C. Exploring the Patients Brain
On the basis of the healers/doctors words, attitudes, andbehaviors, several cognitive and emotional mechanisms are
activated in the brain of the sick, such as those involved incomplex functions like trust and hope. These, in turn, leadto expectations and beliefs, which represent some of theprincipal elements involved in the placebo responses, whichwill be treated starting from section IV.
1. Trustworthiness decisions involve the amygdalaand oxytocin
Trust can be conceptualized as a set of beliefs that the ther-apist will behave in a certain way (316). Patients usuallybase their trust on the therapists competence, compassion,
confidentiality, reliability, and communication (254). Pa-tients trust in their physicians has always been consideredas an important element that per se may have beneficialeffects on the overall health status. This may occur througha better adherence to treatments as well as the reinforce-ment of clinical relationship and patient satisfaction (254).
Deciding if an unfamiliar person is trustworthy representsone of the most important decisions in everyday life. Eithera good or a bad interaction very much depends on thisdecision. One hundred milliseconds of exposure to a neutral
FABRIZIO BENEDETTI
1216 Physiol Rev VOL 93 JULY 2013 www.prv.org
http://-/?-http://-/?- -
8/13/2019 Benedetti F. Placebo and the New Physiology of the Doctor-patient Relationship
11/40
face is sufficient for this complex task (346). This very shortperiod of time shows that face exploration is not necessaryfor trustworthiness judgments, for a time lag of 100 ms isnot sufficient for exploratory saccadic eye movements(319).
Patients with amygdala damage show an impairment inrecognizing emotional facial expressions (8, 9, 78, 352). In
particular, patients with bilateral amygdala lesion show abias to perceive untrustworthy faces as trustworthy (8). Adissociation between processing of face evaluation and fa-cial identity has been found. There are prosopagnosic pa-tients who can recognize emotional expressions but notidentity (68, 95, 108, 321). Likewise, there is some evidencethat individuals with developmental prosopagnosia canmake normal trustworthiness judgments but show im-paired perception of face identity (319).
Besides these lesion studies, there is accumulating evidenceon the role of the amygdala in trustworthiness judgementsthat comes from imaging studies. For example, in one study,subjects were asked to make either explicit or implicit trust-worthiness judgments of unfamiliar faces. It was foundthat, regardless of the task, the amygdala activity increasedin relation to subjective untrustworthiness, whereas theright superior temporal sulcus activity increased only dur-ing explicit trustworthiness judgments. Thus the automaticengagement of the amygdala and the intentional engage-ment of the superior temporal sulcus are dissociated (348).In a different study, it was found that the amygdala re-sponse to faces increased as the untrustworthiness of thefaces increased (121), thus supporting the notion that theamygdala automatically categorizes faces according to per-
ceived untrustworthiness.
Trust behavior has been found to undergo hormonal mod-ulation by oxytocin. This hormone is known to have proso-cial effects in humans, like the modulation of social inter-action behavior and social cognition (31, 163) and the in-fluence on a persons ability to infer anothers mental state(107). In addition, couples receiving intranasal oxytocinprior to a videotaped conflict discussion show an increasein positive communication behaviors (105). Oxytocin hasalso been found to strengthen the anxiolytic effect of thepresence of a friend during public speaking (162). Genetic
variants of the serotonin transporter (5-HTT SLC6A4 poly-morphism) and the oxytocin receptor (OXTR rs53576polymorphism) have been studied in different populations.For example, mothers with these two polymorphismspresent lower levels of sensitive responsiveness to theirchildren (26).
One of the prosocial behaviors that is affected by oxytocinis trustworthy behavior. An increase in plasma oxytocinwas found in subjects who participated in a trust gamewhereby cooperative behavior can benefit both parties
(353). In a different study, it was found that in a trust gamethe intranasal administration of oxytocin was associatedwith a larger amount of money given by an investor to atrustee (197). Interestingly, oxytocin receptors are abun-dant in the amygdala (171). The neural circuitry of trust-worthy behavior was studied by combining the intranasaladministration of oxytocin with functional magnetic reso-nance imaging (35). The investigators found that oxytocin
induced no change in trusting behavior after the subjectslearned that their trust had been breached several times,while the control subjects who had not received oxytocindecreased their trust. This difference in trust adaptation wasassociated with a reduced activation in the amygdala, themidbrain regions, and the dorsal striatum in subjects receiv-ing oxytocin.
Taken together, the findings on the amygdala and oxytocinreveal a specific neuronal circuitry that is involved in trust-worthy behavior (FIGURE 5). Oxytocin receptors are abun-dant in the amygdala; thus they can modulate its activity.The higher the activity in the amygdala is, the higher an
emotion of untrustworthiness is generated. Oxytocin actson its own receptors in the amygdala by reducing neuralactivity, thereby restoring an emotion of trustworthiness.
2. Admiration for virtue and for skills engages twoseparate neural systems
Admiration differs from trust, yet these two emotional ele-ments are related to each other: if one admires a person, heis likely to trust him. Admiration may represent a very im-
Amy
Untrustworthiness
Oxytocin
Amy
Oxtr Oxtr
+ +
FIGURE 5. One of the key elements during the doctor-patientrelationship is represented by the patients trust. The amygdala
(Amy) is responsible for untrustworthiness: the higher the amygdala
activity, the more untrustworthy the judgments about a person.
Oxytocin increases trust by binding to its own receptors (Oxtr) on the
amygdala and by inhibiting its activity.
PLACEBO AND THE DOCTOR-PATIENT RELATIONSHIP
121Physiol Rev VOL 93 JULY 2013 www.prv.org
-
8/13/2019 Benedetti F. Placebo and the New Physiology of the Doctor-patient Relationship
12/40
portant aspect of the therapist-patient encounter, for it canbe elicited either by observing virtuous behavior towardsthe suffering of others or by displays of virtuosic skill. In thefirst case, admiration has to do with social/psychologicalcircumstances, i.e., virtue, whereas in the second case it isrelated to physical circumstances, i.e., skillful abilities(173).
As for compassion, admiration was found to engage theposteromedial cortices, i.e., the posterior cingulate cortex,the retrosplenial area, and the precuneus. However,whereas admiration for virtue induced activation in the in-ferior/posterior portion of the posteromedial cortices, ad-miration for skills produced a larger activation in the supe-rior/anterior portion of the posteromedial cortices (173)(FIGURE 4).
3. Hope and hopelessness may be related toserotonergic and noradrenergic mechanisms
Hope can be defined as a positive motivational state that is
based on a sense of successful goal-directed energy andplanning to meet goals (301, 302). A key element of hope,although not the only one, seems to be the current unsatis-factory conditions of life, which may involve deprivation,damage, or threat (205). Motivation is central to hope, andactually it interacts with goal-directed behavior. High-hopeindividuals are capable of using alternative pathways if animpediment of any sort occurs in the planned behavior sothat the same goal can be reached in a different way (301).
Some studies indicate that hope has beneficial effects onhealth, for example, better coping with arthritis (301), burninjuries (28), fibromyalgia (10, 313), and pain (75, 300,301). In contrast, hopelessness and pessimism have beenfound to be associated with illness and mortality (120, 255,284, 306). However, since hopelessness is often associatedwith depression, some negative effects can sometimes beattributed to the depressive symptoms and not to hopeless-ness itself.
It is not easy to approach hope and hopelessness from aneurophysiological perspective. For example, hopelessnessand helplessness are often considered together. However,whereas hopelessness can be considered as a negative ex-pectation with respect to the future, helplessness can be
viewed as unrealistically low concepts of the own capabili-ties (e.g., see Ref. 165). In 1967 it was reported that dogsundergoing electric shocks not contingent on their behaviorshowed a subsequent difficulty to escape and avoid theshocks (251). This occurred because the dogs learned thatthe shocks were independent of any responses. This phe-nomenon, which was called learned helplessness, hasbeen used as an animal model of depression, despite a re-formulation in more cognitive terms by Abramson et al. (1,2), in which hopelessness was considered as a subset ofhelplessness.
Serotonin has been found to be involved in learned helpless-ness. For example, in some studies, after the presentation ofuncontrollable shocks, rats could be separated into twodifferent groups. Whereas one group did not learn to escapea controllable shock after previous exposure to uncontrol-lable shocks (learned helpless rats), another group learnedan adequate response (nonlearned helpless rats). Thelearned helpless rats showed an upregulation of serotonin
receptors in some regions of the brain, such as the cortex,hippocampus, septum, and hypothalamus, whereas a down-regulation was observed in the hypothalamus. Changes in pre-synapticactivity at serotonergicsynapses caused by uncontrol-lable shocks have also been described in the hippocampus andhypothalamus of learned helpless rats (20, 113, 114).
Interestingly, a negative correlation between prefrontalbinding to serotonin 5-HT2Areceptors and levels of hope-lessness was found in attempted suicide, according to therule: the lower the binding to serotonin receptors, the higherthe degree of hopelessness (325). An activation of the hy-pothalamus-pituitary-adrenal axis has also been found in a
number of studies that used inescapable shocks as a model(165), and indeed, adverse experiences might lead to stresssensitivity. This, in turn, would lead to excessive norepi-nephrine release and its subsequent depletion, with the con-sequent hopelessness (228).
4. Attributing a positive meaning to pain coactivatesopioid and cannabinoid systems
Empathic and compassionate behavior is not always in-cluded in the doctors background and armamentarium,and bad communication is sometimes the rule in routinemedical practice. The doctors words and behavior mayinduce negative expectations in the patient and may lead toclinical worsening. One good example is represented by theway of communicating negative diagnoses, a task that re-quires good empathic and compassionate abilities. The im-pact of a negative diagnosis on the patients brain and bodycan be substantial and can induce real worsening, e.g., painincrease. Anxiety plays a key role in these situations, and abad interaction may indeed increase the patients negativeemotions. In this regard, the mechanisms underlying anxi-ety- and nocebo-induced hyperalgesia have been investi-gated in some detail and will be described in section VA5.
In this regard, the different meaning that is attributed to asymptom such as pain can be crucial in the global experi-ence of pain. For example, clinicians have long known thatcancer pain can be perceived as more unpleasant than post-operative pain (94, 127, 299), and this can be due to thedifferent meanings of cancer on the one hand and of surgeryon the other. Whereas the former often means death, thelatter is associated with healing and recovery. Likewise,different religions attribute different meanings to pain andsuffering, and this may lead to different pain experiences(164, 194, 342).
FABRIZIO BENEDETTI
1218 Physiol Rev VOL 93 JULY 2013 www.prv.org
-
8/13/2019 Benedetti F. Placebo and the New Physiology of the Doctor-patient Relationship
13/40
Only very recently were different attributions to pain inves-tigated with a neurobiological approach, and this approachmay have profound implications in medical practice, forexample, within the context of negative diagnoses. In fact,how patients interpret their own pain experience can makea big difference. Benedetti et al. (66) changed the meaningof pain from negative to positive in healthy subjects throughverbal suggestions. The subjects had to tolerate ischemic
arm pain as long as possible. However, whereas one groupwas informed about the aversive nature of the task, as donein any pain study, a second group was told that the ischemiawould be beneficial to the muscles, thus stressing the bene-ficial nature of the pain endurance task. In this latter group,pain tolerance was significantly higher compared with thefirst one, an effect that was partially blocked by the opioidantagonist naltrexone alone and by the cannabinoid antag-onist rimonabant alone. However, the increased tolerancewas antagonized completely by the combined administra-tion of naltrexone and rimonabant, which suggests that apositive approach to pain reduces the global pain experi-ence through the coactivation of the opioid and cannabi-
noid systems. These findings show that the way patientsinterpret their own symptoms may have a dramatic effecton their emotional experience.
IV. MECHANISM-BASED CLASSIFICATIONOF PLACEBO RESPONSES
A. Mechanism-Based or Disease-BasedClassification of Placebo Responses?
The final and perhaps the most important step in the doc-tor-patient interaction is represented by the very act of re-ceiving a treatment (FIGURE 3). The ritual of the therapeuticact and the effects that it may have on the therapeutic out-come is the element that has received great attention in thepast few years. As described in section I, the psychosocialcontext and the therapeutic ritual surrounding the treat-ment and the patient (FIGURE 1)have been approached byusing the placebo response as a model to understand theunderlying physiological mechanisms. The doctor, andmore in general the healer, is surely the key element in thistherapeutic ritual, as we have seen in sections II and III.
What we have learned over the past years is that there is nota single mechanism of the placebo response, and actuallythere is not a single placebo response but many, so thatdifferent mechanisms are involved in different medical con-ditions and therapeutic interventions. One of the mainproblems in current placebo research is how these differentmechanisms should be considered and classified. For exam-ple, placebo administration can induce either anxiety reduc-tion or activation of reward mechanisms, depending ondifferent circumstances. Likewise, different forms of learn-ing can take part in placebo responsiveness in different con-
ditions, ranging from classical conditioning to social learn-ing. Therefore, a first approach to the classification of dif-ferent placebo responses might be based on the mechanismthat is involved.
On the other hand, today we do not know exactly when andin which conditions these mechanisms take place. For ex-ample, anxiety reduction might be important only in some
medical conditions but not in others. Or, otherwise, learn-ing might be a common mechanism across all medical con-ditions. Reasoning in this way, a second approach to theclassification of different placebo responses, is a disease-based classification whereby the biological underpinningsare investigated in different conditions such as pain andParkinsons disease.
Therefore, it is not clear whether we should differentiate theplacebo responses on the basis of the mechanism or ratheron the basis of the disease. This will be a future challenge inplacebo research, that is, to understand where (in whichdisease), when (in which circumstance), and how (with
which mechanisms) placebos work. Therefore, due to ourlimited understanding of the relationship between mecha-nisms and diseases, I will present both approaches. In thissection IV, the general mechanisms that have been identifiedare described (FIGURE 6), whereas in section V the placeboresponses will described in different diseases.
B. Expectations of Therapeutic Benefit Playa Key Role in Many Conditions
Most of the studies aimed at identifying the underpinningsof the placebo effect have focused on expectations as themain mechanism, although today we do not know exactly ifexpectations are important in all medical conditions. Ex-pectations of a future outcome are usually held by individ-uals about their own responses. Positive expectations leadto adopting a particular response, whereas negative expec-tations lead to its inhibition (187, 188). Expectations mayalso induce a decrease in self-defeating thoughts when ex-pecting a positive outcome (308), and other factors maycontribute such as motivation (269).
From both a psychological and a neuroscientific standpoint,expecting a future event may involve several brain mecha-
nisms that aim to prepare the body to anticipate that event.For example, expecting a future positive outcome may leadto anxiety reduction and/or reward mechanisms activation,whereas expecting a negative outcome produces anticipa-tory anxiety, which is very important in anticipating a pos-sible threat. Indeed, both subjective anxiety (122, 231, 327)and anxiety-related brain activity (256) have been found tobe reduced after placebo administration.
Expectations may also induce changes through the activa-tion of the reward circuit. These mechanisms are tradition-
PLACEBO AND THE DOCTOR-PATIENT RELATIONSHIP
121Physiol Rev VOL 93 JULY 2013 www.prv.org
http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?- -
8/13/2019 Benedetti F. Placebo and the New Physiology of the Doctor-patient Relationship
14/40
ally studied by using natural rewards, like food, as well asmonetary and drug rewards (176, 241). In the case of theplacebo response, the reward is the therapeutic benefit itselfand the consequent clinical improvement, which representpowerful rewards for the suffering patient. The nucleus ac-cumbens plays a key role in reward mechanisms, and sev-eral studies found an increased activity of the nucleus ac-cumbens and dopaminergic activity after placebo adminis-tration in Parkinsons disease (98, 99, 217), depression(229), and pain (287, 288). A detailed account will be given
in the sections on pain, Parkinsons disease, and depression.
C. The Placebo Response InvolvesLearning Mechanisms
Patients can associate shape, color, and taste of a pill withsymptom amelioration, such as pain decrease. Several otherstimuli can be associated with clinical improvement, such assyringes, stethoscopes, white coats, hospitals, doctors,nurses, and so on. The mechanism that underlies this effectis classical conditioning, whereby a neutral stimulus, e.g.,the color and shape of a pill, can become effective if repeat-
edly associated with an unconditioned stimulus, i.e., thedrug inside the pill. Many placebo responses can be attrib-uted to this associative learning, whereby the placebo is theneutral stimulus itself. In one of the first studies on thebiology of the placebo effect (169), motor changes wereobserved in the rat after an injection of scopolamine, andthe same changes occurred if an injection of saline solution(placebo) was performed after the injection of scopolamine.
In clinical practice, these sequence effects are common (16,22, 33, 34, 204, 312), and they can also be exploited in
clinical practice (106). Learning effects can be reproducedin the experimental setting as well. For example, Voudouriset al. (331, 332) associated a nonanesthetic cream (placebo)with the surreptitious reduction of the intensity of painfulstimulation, so as to make the subjects believe that thecream was an effective anesthetic. These subjects, who hadexperienced a true anesthesia/analgesia, became strongplacebo responders, which suggests that conditioning is im-portant. However, expectation was found to be crucial,because no placebo analgesic effect was found if the subjects
were told that the cream was inert (243). This suggests that,during a conditioning procedure, conscious expectations ofa future outcome play a major role.
Expectation and conditioning are not necessarily mutuallyexclusive, as they may represent two sides of the same coin(308). In other words, a conditioning procedure might leadto placebo responses through a mechanism of reinforcedexpectations. Indeed, in the 1960s, a different interpreta-tion of classical conditioning was put forward. According tothis reinterpretation, conditioning does not depend merelyon the pairing of conditioned and unconditioned stimuli, but
on the cognitive information of the conditioned stimulus(276). Therefore, a conditioning procedure would lead to theexpectation that a given event will follow another event (189,275, 276).
Despite the reinterpretation of conditioning in cognitiveterms, conditioned placebo responses in humans are notalways cognitively mediated. For example, it has been sug-gested that unconscious conditioning is important in thoseplacebo responses that involve unconscious physiologicalfunctions, whereas it is cognitively mediated when con-
Social
learning
Placebo(sham treatment)
Expectation
of reward
Learning-
reinforcedexpectations
Pavlovian
conditioning
Personality
traits
Clinical Improvement
Expectation-
modulatedanxiety Genetics
FIGURE 6. This figure includes only the psychobiological factors ofFIGURE 2. It can be seen that several
psychological and biological factors may be involved in the clinical improvement following administration of a
placebo. Therefore, there is not a single placebo response but many, with different mechanisms across
different medical conditions and therapeutic interventions.
FABRIZIO BENEDETTI
1220 Physiol Rev VOL 93 JULY 2013 www.prv.org
http://-/?-http://-/?-http://-/?-http://-/?- -
8/13/2019 Benedetti F. Placebo and the New Physiology of the Doctor-patient Relationship
15/40
scious processes come into play (65). Therefore, many pla-cebo effects can be explained in the context of conditioningtheories (3, 252, 295). In fact, a placebo is by definition aneutral stimulus with no therapeutic effects, in the sameway as a conditioned stimulus is by definition neutral. Like-wise, a placebo response is by definition elicited by a neutralstimulus, in the same way as a conditioned response is in-duced by a neutral stimulus.
Conditioning is not the only learning mechanism that maybe involved in placebo phenomena. Social learning is an-other form of learning whereby people learn from one an-other by observation and imitation. As it will described inthe section on pain, placebo effects can be elicited by sociallearning through the observation of others who respond toa painkiller (91).
D. Some Placebo Responses May Be Relatedto Personality Traits
A central issue in placebo research is whether individualspossess one or more specific characteristics, which can reli-ably identify them a priori as placebo responders or pla-cebo nonresponders, with important implications for bothclinical trials design and personalized therapy optimization.Some studies have found that individual differences in sug-gestibility may contribute to the magnitude of placebo an-algesia. In fact, the largest placebo responses were found inhighly suggestible subjects who received suggestions pre-sumed to elicit high expectations for drug efficacy (100).Pessimists have been found to be more prone than optimiststo follow a negative placebo (nocebo) expectation, whichsuggests that the personality variable optimism-pessimism
relates to placebo responding (139). In addition, individualswere tested on the basis of their level of optimism, and itwas found that optimism was positively associated withbetter sleep quality after administration of a placebo sleep-ing treatment, thus suggesting that different degrees of op-timism relate to placebo responding (140).
E. Different Genetic Variants AffectPlacebo Responding
Recently, substantial placebo responses have been foundfor some genetic variants, for example in some psychiatric
disorders (137, 274). In one study (137), patients with so-cial anxiety disorder were genotyped with respect tothe serotonin transporter-linked polymorphic region (5-HTTLPR) and the G-703T polymorphism in the trypto-phan hydroxylase-2 (TPH2) gene promoter. With the use offunctional neuroimaging, it was found that only those pa-tients who were homozygous for the long allele of the5-HTTLPR or the G variant of the TPH2 G-703T polymor-phism showed robust placebo responses and reduced activ-ity in the amygdala. Conversely, carriers of short or T allelesdid not show placebo responses.
In another study in patients with major depressive disorder(209), polymorphisms in genes encoding the catabolic en-zymes catechol-O-methyltransferase (COMT) and mono-amine oxidase A were examined. Small placebo responseswere found in those patients with monoamine oxidase AG/T polymorphisms (rs6323) coding for the highest activityform of the enzyme (G or G/G). Similarly, lower placeboresponses were found in those patients with ValMet cat-
echol-O-methyltransferase polymorphisms coding for alower-activity form of the enzyme (2 Met alleles).
In a more recent study, the COMT functional val158metpolymorphism was found to be associated with the placeboeffect in irritable bowel syndrome. The strongest placeboresponse occurred in Met/Met homozygotes (154). There-fore, the role of genetic factors in placebo responding ap-pears to be an important factor across a number of diseases,ranging from neuropsychiatric to gastrointestinal/psycho-somatic disorders.
F. Other Possible Explanations HaveBeen Proposed
In addition to the classical psychological, neuroscientific,and biomedical approach, other perspectives of the placebophenomenon have been proposed. For example, medicalanthropologists have put forward the concept of embodi-ment. According to this view, our experiences are not onlystored as conscious memories, but they are imprinted di-rectly onto our body representation as well, with no con-scious processes involved. Accordingly, placebo and no-cebo effects would represent positive and negative effects ofembodiment, respectively. This process does not need theinvolvement of conscious expectations (317). A body rep-resentation change can be achieved just by the complexityof the ritual of the therapeutic act. Crucial in the therapeuticritual is the doctor-patient relationship, with empathy, at-titudes, behaviors, as well as gesture and recitation all con-tributing to the positive treatment outcome (317).
V. DISEASE-BASED CLASSIFICATIONOF PLACEBO RESPONSES
Differently from the previous section, the disease-based
classification approaches the placebo effect by analyzing asingle medical condition, such as pain and Parkinsons dis-ease. Indeed, most of our knowledge on the physiologicalmechanisms of the placebo response comes from this ap-proach. In many studies, however, placebos were adminis-tered without specifically investigating anxiety modulationor reward mechanisms or learning. Therefore, today we donot know exactly whether or not all these mechanisms takepart in placebo responsiveness in a single condition such aspain. Despite these limitations, the disease-based approachhas been the most productive in the past few years. One of
PLACEBO AND THE DOCTOR-PATIENT RELATIONSHIP
122Physiol Rev VOL 93 JULY 2013 www.prv.org
http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?- -
8/13/2019 Benedetti F. Placebo and the New Physiology of the Doctor-patient Relationship
16/40
the most important future challenges of placebo researchwill be to understand in which medical conditions all themechanisms listed in section IV and FIGURE 6are present.Today the most studied and understood conditions are cer-tainly represented by pain, Parkinsons disease, and the im-mune and hormonal responses.
A. Placebo Analgesia Is the Most
Studied and Understood Type ofPlacebo Response
1. Expectation is the most important factor inplacebo analgesia
The reason why pain is the most studied condition is two-fold. First, pain is a subjective experience that undergoespsychological and social modulation more than any othercondition. The fine tuning of pain by many psychosocialfactors makes pain an excellent model for investigating theplacebo response. Second, modern placebo research hasbeen influenced by the work by Beecher in the 1950s (36)
who, as an army doctor during the Second World War,faced the problem of the lack of strong analgesics on thebattlefield. Therefore, he treated his soldier patients withplacebos many times and found that many subjects re-sponded quite well very often. Despite several methodolog-ical flaws (44), Beechers merit was to boost the interest ofthe scientific community in the placebo effect.
Today it is not clear why some individuals respond to pla-cebos whereas some other individuals do not (see sectionVID). It should be noted that a mean change in a placebogroup might be seen in different situations, e.g., if all sub-jects in the placebo group show a moderate response or,otherwise, a small subset of subjects show a large responseand others show no response at all. These variations areresponsible for the large variability in placebo responsesthat is observed following placebo administration. For ex-ample, Levine et al. (211) found a percentage of 39%, Bene-detti (40) of 26.9%, and Petrovic et al. (257) of 56%.
Expectation seems to play a key role in placebo analgesia(188, 243, 269, 270). For example, Benedetti et al. (65)performed a pharmacological preconditioning for 2 days ina row with ketorolac, a nonopioid analgesic. On the thirdday, ketorolac was replaced with a placebo along with ver-
bal suggestions of analgesia, and a powerful placebo anal-gesic response was observed. In a second group, the sameprocedure with ketorolac was carried out to see whetherthis placebo response was due to the pharmacological pre-conditioning itself. However, on the third day, the placebowas given along with verbal suggestions that the drug was ahyperalgesic agent. Not only were these instructions suffi-cient to block placebo analgesia completely, but they alsoproduced hyperalgesia. This finding indicates that placeboanalgesia depended on expectation of pain decrease, eventhough a preconditioning procedure was performed.
The decreased effectiveness of hidden treatments representsone of the best evidences of the crucial role of expectation.In this case, a painkiller is given covertly (unexpectedly)unbeknownst to the patient, and the outcome following thehidden (unexpected) administration is compared with thatfollowing an open (expected) administration. In postoper-ative pain following the extraction of the third molar (210,213), it was found that a hidden injection of a 68 mg
intravenous dose of morphine corresponds to an open in-jection of saline solution in full view of the patient (pla-cebo). Thus a placebo is as powerful as 68 mg of mor-phine. This means that an open injection of morphine ismore effective than a hidden injection because in the hiddenadministration condition there is no placebo component. Asystematic study of the differences between open (expected)and hidden (unexpected) administrations of drugs has beenperformed for five widely used painkillers (morphine, bu-prenorphine, tramadol, ketorolac, metamizol) in the post-operative setting (19, 57, 62, 92). It was found that theanalgesic dose needed to reduce the pain by 50% (AD50)was much higher with hidden infusions than with open ones
for all five painkillers, indicating that a hidden administra-tion is less effective than an open one. In addition, it wasfound that pain ratings were much higher with a hiddeninjection than with an open one.
2. Both endogenous opioids and endocannabinoidsmay take part in placebo analgesia
The placebo effect represents today one of the most inter-esting models to understand the endogenous mechanisms ofanalgesia (42), and indeed, placebos have been found toactivate different endogenous antinociceptive systems. Thefirst study that was aimed at understanding the biologicalmechanisms of placebo analgesia used naloxone as an an-tagonist of the opioid receptors in patients with postopera-tive pain who had undergone the extraction of the thirdmolar (212). The investigators found a disruption of pla-cebo analgesia after naloxone administration, which indi-cates the involvement of endogenous opioids in the placeboanalgesic effect. The involvement of the endogenous opioidnetwork in the analgesic placebo response was then con-firmed by a number of studies (148, 210, 220).
In a long series of experiments with rigorous experimentaldesign, which were performed between 1995 and 1999,
many mechanisms were clarified and the role of endogenousopioids in placebo analgesia was better explained (FIGURE 7).With the use of experimental ischemic arm pain, it wasdefinitely clarified that the effect following naloxone ad-ministration could be attributed to the blockade of placebo-induced opioid activation (40). In addition, the effects of acholecystokinin (CCK) antagonist, proglumide, on placeboanalgesia was tested on the basis of the anti-opioid action ofCCK. It was found that proglumide potentiated placeboanalgesia, which represents a novel and indirect way to testthe opioid hypothesis (40, 51). More recent research has
FABRIZIO BENEDETTI
1222 Physiol Rev VOL 93 JULY 2013 www.prv.org
http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?- -
8/13/2019 Benedetti F. Placebo and the New Physiology of the Doctor-patient Relationship
17/40
shown that the activation of the CCK receptors by means ofthe agonist pentagastrin is capable of blocking the pla-cebo analgesic response, thus emphasizing the role ofCCK as an anti-opioid agent that may interfere withplacebo responses (53).
On the basis that the placebo analgesic effect is not alwaysmediated by endogenous opioids (147), Fields and Levine(128) suggested that different physical, psychological, andenvironmental situations could affect the endogenous opi-oid systems differently. In fact, Amanzio and Benedetti (16)showed that placebo analgesia is mediated by both expec-tation and conditioning, but whereas the former activatesthe opioid systems, the latter activates nonopioid systems.Indeed, the opioid antagonist naloxone can block thoseplacebo responses that are induced by means of strong ex-pectation cues. Similarly, if a placebo is given after repeatedadministrations of morphine (preconditioning procedure),the placebo response can be blocked by naloxone. Con-versely, if the placebo response is induced by means of priorconditioning with a nonopioid drug, such as nonsteroidanti-inflammatory drugs (NSAIDs), it is naloxone insensi-tive (16).
On the basis of these findings, Benedetti and collaborators(52) induced opioid or nonopioid placebo analgesic re-sponses and assessed the effects of the CB1 cannabinoidreceptor antagonist rimonabant. Differently from nalox-one, rimonabant had no effect on opioid-induced placeboanalgesia following morphine preconditioning, whereas itcompletely blocked placebo analgesia following nonopioidpreconditioning with the NSAID ketorolac. These findingsindicate that those placebo analgesic responses that are elic-ited by NSAIDs conditioning are mediated by CB1 canna-binoid receptors (FIGURE 7).
Since the involvement of the CB1 cannabinoid receptors inplacebo analgesia is a very recent finding, little is knownabout their localization and activation. We only knowthat they are activated following a previous exposure toNSAIDs, which suggests that these drugs, besides the inhi-bition of cyclooxygenase and prostaglandin synthesis, acti-vate an endocannabinoid pathway (52). In contrast, weknow more details about the activation and localization ofthe placebo-activated opioid systems. For example, specificplacebo analgesic responses can be obtained in differentparts of the body (242, 270), and these responses are nal-oxone-reversible (55). If four noxious stimuli are applied tothe hands and feet and a placebo cream is applied to onehand only, pain is reduced only on the hand where theplacebo cream had been applied. This highly specific effectis blocked by naloxone, suggesting that the placebo-acti-vated endogenous opioid systems have a precise and soma-totopic organization (55).
In 2002, Petrovic et al. (257) found that both a placebo andthe opioid agonist remifentanil affect the very same brainregions in the cerebral cortex and in the brain stem, whichsuggests that placebo-induced and opioid-induced analge-sia share a common mechanism. A placebo induced the
activation of the rostral anterior cingulate cortex and theorbitofrontal cortex, and there was a significant covariationin activity between the rostral anterior cingulate cortex andthe lower pons/medulla, and a subsignificant covariationbetween the rostral anterior cingulate cortex and the peri-aqueductal gray, which suggests that the descending rostralanterior cingulate/periaqueductal gray/rostral ventrome-dial medulla pain-modulating circuit is involved in placeboanalgesia. In 2005, Zubieta et al. (355) provided the firstdirect evidence of opioid-mediated placebo analgesia. Withthe use of in vivo receptor binding techniques with the ra-
Proglumide
Naloxone Rimonabant
opioid receptors CB1 cannabinoid receptors
+ +
Previousexposure to
opioids
Previousexposure to
NSAIDs
CCK
Placebo
FIGURE 7. The mechanism of the placebo analgesic response depends on the previous exposure to different
pharmacological agents, thus suggesting a memory for drug action. The previous exposure to opioids leads to
opioid-mediated placebo responses, whereas the prior exposure to nonsteroid anti-inflammatory drugs
(NSAIDs) leads to cannabinoid-mediated placebo responses. Cholecystokinin (CCK) antagonizes the opioid-mediated placebo responses. All these effects can be blocked by means of the appropriate antagonistic drugs,
such as the opioid antagonist naloxone, the cannabinoid antagonist rimonabant, and the CCK antagonist
proglumide.
PLACEBO AND THE DOCTOR-PATIENT RELATIONSHIP
122Physiol Rev VOL 93 JULY 2013 www.prv.org
-
8/13/2019 Benedetti F. Placebo and the New Physiology of the Doctor-patient Relationship
18/40
diotracer carfentanil, a -opioid agonist, it was shown thata placebo procedure activates -opioid neurotransmissionin the dorsolateral prefrontal cortex, the anterior cingulatecortex, the insula, and the nucleus accumbens. These find-ings were subsequently confirmed in a different study (335).By performing connectivity analysis with fMRI, Eippert etal. (115) found that a placebo treatment increases couplingbetween the periaqueductal gray and the rostral anterior
cingulate cortex, and that this increased coupling is dis-rupted by naloxone.
Interestingly, all these opioid-mediated placebo responseshave also been investigated in rodents, and similar mecha-nisms have been described (150, 247, 354). For example,Guo et al. (150) used the hot-plate test in an attempt tomeasure the reaction time of mice to a nociceptive stimulus(hot plate) after different types of pharmacological condi-tioning. This was performed by the combination of theconditioned cue stimulus with the unconditioned drug stim-ulus, either the opioid morphine or the nonopioid aspirin. Ifmice were conditioned with morphine, placebo analgesia
was completely antagonized by naloxone, whereas if micewere conditioned with aspirin, placebo analgesia was nal-oxone-insensitive. In addition, placebo analgesia was foundto be mediated specifically only by the -opioid receptors(354). Therefore, also in rodents, the mechanisms underly-ing placebo analgesia include both opioid and nonopioidcomponents and may depend on the previous exposure todifferent pharmacological agents.
3. Imaging the brain after placebo administration
Neuroimaging has been fundamental in the understandingof placebo analgesia, and many brain imaging studies havebeen carried out to describe the functional neuroanatomy ofthe placebo analgesic effect (70, 115, 116, 158, 196, 218,223, 224, 234, 257, 268, 288, 289, 320, 333335, 355,356). As described above, the first imaging study of placeboanalgesia showed that a subset of brain regions are similarlyaffected by either a placebo or a -opioid agonist (257).These included the rostral anterior cingulate cortex, theorbitofrontal cortex, and the anterior insula, and there wasa significant covariation in activity between the rostral an-terior cingulate cortex and the lower pons/medulla, and asubsignificant covariation between the rostral anterior cin-gulate cortex and the periaqueductal gray, which suggests a
descending pain-modulating circuit. This network may useendogenous opioids as neurotransmitters (115) and extendsdown to the spinal cord (116).
In a functional magnetic resonance imaging study of exper-imentally induced pain in healthy subjects, Wager et al.(334) found that placebo analgesia was related to neuralactivity decrease in pain-processing areas such as the thala-mus, anterior insular cortex, and anterior cingulate cortex.Importantly, a correlation was present between the magni-tudes of these decreases and the reductions in pain ratings.
Not only did Wager et al. (334) image the time period ofpain but also the time period of anticipation of pain, show-ing activations during the anticipatory phase in the orbito-frontal cortex, dorsolateral prefrontal cortex, rostral ante-rior cingulate cortex, and midbrain periaqueductal gray. Itis interesting to note that the dorsolateral prefrontal cortexis associated with cognitive control, which is a crucial ele-ment in expectation (236), and the orbitofrontal cortex
with evaluation and reward, which is consistent with a rolein affective responses during the anticipation phase of pain(104).
Differently from most of the brain imaging studies, whichwere aimed at investigating placebo analgesia in the exper-imental setting, Price et al. (268) conducted a functionalmagnetic resonance imaging study in which brain activity ofirritable bowel syndrome (IBS) patients was measured inresponse to rectal distension by a balloon barostat. A largeplacebo effect was produced by suggestions and accompa-nied by large reductions in neural activity in thalamus, pri-mary and secondary somatosensory cortex, insula, and an-terior cingulate cortex during the period of stimulation. Itwas also accompanied by increases in neural activity in therostral anterior cingulate cortex, bilateral amygdala, andperiaqueductal gray (269). This study shows that placebosact on the brain in a clinical relevant condition in the sameway as they do in the experimental setting. Therefore, theinvolvement of key areas in placebo analgesia, such as theanterior cingulate cortex, is not limited to experimentalnoxious stimuli, but it also extends to clinical pain.
Lorenz et al. (223) used high temporal resolution tech-niques (magnetoencephalography) to discriminate whether
expectations of analgesia exert their psychophysical effectduring the early phase of cortical processing, namely, in theprimary and secondary somatosensory areas, or duringlater cortical processing, such as in anterior cingulate cor-tex. These researchers found that the secondary somatosen-sory cortex was correlated to expectation-related subjectivepain rating, while the anterior cingulate cortex was associ-ated only with stimulus intensity and related attentionalengagement. In other studies with laser evoked potentials(93, 337), early nociceptive components were found to beaffected by placebos, thus indicating that later cognitivereappraisal and/or late bias-related neural activity cannot
be responsible for this early modulation.
By using both positron emission tomography and func-tional magnetic resonance imaging, Scott et al. (288) testedthe correlation between the responsiveness to placebo andthat to monetary reward, and found that placebo respon-siveness was related to the activation of dopamine in thenucleus accumbens, a region involved in reward mecha-nisms (172, 193, 285, 286) (see also section IVB). Monetaryresponses in the nucleus accumbens were assessed in thevery same subjects by means of functional magnetic reso-
FABRIZIO BENEDETTI
1224 Physiol Rev VOL 93 JULY 2013 www.prv.org
-
8/13/2019 Benedetti F. Placebo and the New Physiology of the Doctor-patient Relationship
19/40
nance imaging, and a correlation was found between theplacebo responses and the monetary responses. In fact,large nucleus accumbens responses to monetary rewardswere associated with large nucleus accumbens responses toplacebos. Therefore, placebo responsiveness may depend,at least in part, on the efficiency of the reward system. Thesame authors studied the endogenous opioid and the dopa-minergic systems by using positron emission tomography
with
11
C-labeled raclopride for the analysis of dopamineand [11C]carfentanil for the study of opioids (289). Theadministration of a placebo induced the activation of opioidreceptors in the anterior cingulate, orbitofrontal and insularcortices, nucleus accumbens, amygdala, and periaqueductalgray matter. Dopamine was activated in the nucleus accum-bens. The perceived effectiveness of the placebo was asso-
ciated with both dopamine and opioid activity. Interest-ingly, nocebo responses were associated with a deactivationof dopamine and opioid release.
Overall, these brain imaging data have been summarized byusing a meta-analysis approach with the activation likeli-hood estimation method (17). Nine functional magneticresonance studies and two positron emission tomography
studies were selected for the analysis. During the expecta-tion phase of analgesia, areas of activation were found inthe left anterior cingulate, right precentral and lateral pre-frontal cortex, and in the left periaqueductal gray (FIGURE 8, top
panel). In the phase following pain stimulation, activationswere found in the anterior cingulate and medial and lateralprefrontal cortices, in the left inferior parietal lobule and
Areas of increased activity associated with expectation
Areas of increased activity associated with early pain
Areas of decreased activity associated with early pain
FIGURE 8. Activation likelihood estimation meta-analysis of different brain imaging studies of placebo anal-
gesia in experimental pain. Red means activation areas, whereas green means deactivation areas. The
sequence of events from placebo administration to inhibition