BVO UTRECHT - Workshop cloudwerken Pop-up Summerschool 8 7-16

Ion Channels and EpilepsyAssoc.Prof. Dr. Helmut Kubista
Center of Physiology and Pharmacology
Department of Neurophysiology and Neuropharmacology
Basic lecture 2020 (BVO) 860.977

Mode of Action of Anti-Epileptic Drugs

Alterpredominantly genetic causes
idiopathic epilepsies(= a “disease of its own kind”)(most often „channelopathies“)
when symptomatic than typicallydue to developmental anomalies ormetabolic dysfunction
symptomatic epilepsies(resulting form another disease
or acute damage: stroke, haemorrhage, trauma)
„translational channelopathies“
Incidence of epilepsy
Chapter 1
Chapter 2

Chapter 1
Ion Channel Dysfunction in Genetically-DeterminedEpileptic Syndromes

Idiopathic epilepsies are predominantly due to genetic factors
typically oligogenic or polygenic inheritance, only in rare cases monogenic!
Steinlein (2002), PubMed PMID: 11888238.
„Only about 2% of idiopathic epilepsies are inherited in a monogenic manner, meaning that a single mutation in one particular gene is enough to induce epilepsy with high penetrance “.
Maljevic, S., Hedrich, U. & Lerche, H. Ionenkanalerkrankungen des Gehirns – monogene Epilepsien. medgen 25, 431–439 (2013). https://doi.org/10.1007/s11825-013-0425-5
“The identification of genes (as well as of the function/dysfunction of the respective gene products), which are responsible for genetically-determined epilepsies, has crucially contributed to our understanding of the pathomechanisms of epilepsy”.
e.g. ion channel dysfunction
Steinlein (2008), PubMed PMID: 18472482.

Lerc
he e
t al. (
2013)
J P
hysio
l. 2
013,
591:7
53-7
64.
PubM
ed
PM
ID: 23090947
CACNA1H Cav3.2 (Ca2+ channel)

domain I domain II domain III domain VI
transmembrane segments S1-S6
pore-loop(„P-loop“)
N-terminus
C-terminus
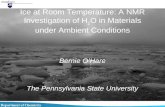
Structure: voltage-gated ion channel (e.g. Nav channels)
pore-forming α-subunit accessory
β-subunit
(S4: voltage sensor)
++++
Variants of the SCN1A gene (Nav1.1)
from: Freissmuth, Offermanns, Böhm: Pharmakologie und Toxikologie: Von den molekularen Grundlagen zur Pharmakotherapie; Springer (2016; 2. Auflage), modified!

from Stephens et al. (2015), PubMed PMID: 26042044

Cat
tera
llet
al.,
20
10
, Pu
bM
edP
MID
: 20
19
41
24
.

NaV 1.1 KO mice
Yu et al; Nat Neurosci 9, 1142, 2006
~ 75 % of INa is carried by Nav1.1 channels in hippocampal interneurons
≤ 10% INa is carried by Nav1.1 channels in hippocampal pyramidal neurons
(here, Nav1.2 and Nav1.6 predominate INa)
pyramidal bipolar

Cat
tera
llet
al.,
20
10
, Pu
bM
edP
MID
: 20
19
41
24
.

GEFS+: generalized epilepsy with febrile seizures plus
febrile seizures (FS) occur during episodes of fever, usually restricted to childhood
GEFS+: seizures persist beyond the age of 6 years
SMEI: severe myoclonic epilepsy of infancy
a severe epileptic encephalopathy, characterized by onset of febrile seizures by age 1
emergence between ages 1 and 4 of other seizure types, including myoclonic, focal,
absence and atonic seizures
developmental decline

temperature-dependent effects have been demonstrated !
[GEFS+: „generalized epilepsy with febrile seizures plus“][Dravet Syndrom = SMEI: „ severe myoclonic epilepsy of infancy“]
fro
m: C
atte
rall
(2
01
2),
Pu
bM
edP
MID
: 22
78
76
29
.
Variants of SCN1A Gen (Nav1.1) cause either „loss of function“ (LOF) or „gain of function“ (GOF)

Variants of the GABRG2 gene (γ2-subunit of the GABAA receptor) can also cause GEFS+
Mutations of the γ2 subunit lead to retention of GABAA
receptors in the endoplasmic retikulum.
This retention shows temperature-dependence! (promoted by fever, → seizures).
Kang et al. (2006), PubMed PMID: 16510738.

GABAA receptors
Sigel and Steinmann (2012), PubMed PMID: 23038269.
Cl-
γ2β2α1β2α1: the major isoform of GABAA receptors

Variants of the GABRG2 gene (γ2-subunit of the GABAA receptor) can also cause GEFS+
Forms of absence epilepsie in children (e.g. „childhood absenceepilepsy“, CAE) can be precipitated by mutations in the GABRG2 gene.
Mutations of the γ2 subunit lead to retention of GABAA
receptors in the endoplasmic retikulum.
This retention shows temperature-dependence! (promoted by fever, → seizures).
Kang et al. (2006), PubMed PMID: 16510738.

GABA-induzierte
Ströme
Kan
g et
al.
(20
06
), P
ub
Med
PM
ID: 1
65
10
73
8.
temperature-dependent retention of GABAA receptors in the endoplasmic reticulum in the presence of different mutated γ2 (R34Q, K289M, …) subunits and effects on GABA-
currents [note that α1(A322D) causes afebrile seizures!].

But γ2(R43Q) mutations also induce changes in cortical microarchitecture!
Increase in density of GABAergic interneurons
Wim
mer
et
al. (
20
15
), P
ub
Med
PM
ID: 2
57
40
86
0.

Variants in KCNQ2 und KCNQ3 genes (Kv7.2 and Kv7.3: „M-Current“)
BFNC (BFNS): Benigne familial neonatal convulsions (or seizures)
Maljevic et al., 2008 PubMed PMID: 18238816
KCNQ2 (Kv7.2) KCNQ3 (Kv7.3)

BFNS: benign familial neonatal seizures (formerly benign familial neonatal convulsions: BFNC)
onset: a few days after birth (first seizures appear on PND 2 to 3)
brief unprovoked partial or generalized seizures
seizures last from a few seconds to 3 minutes
tonic phase at the beginning (tonic posture of trunk and limbs)
then clonic phase starts with vocalisation (e.g. shrill cry), ocular symptoms
(e.g. rapid blinking of the eyes) or chewing movements, rhythmic shaking of
upper limbs
frequency of seizures as high as 20 to 30 episodes per day
progression: spontaneous remission by 16 months of age, however: increased seizure risk in later life

heart,
lung,
kidney
inner ear
CNS
CNS
CNS
KCNQ family ofpotassium channels:
KCNQ → Kv7.x
name derived from:KCNQ1-gene, which codes for Kv7.1 in cardiac tissue (mutations lead to„long-QT Syndrom“, [LQTS])
Fig. from:Robbins (2001), PubMed PMID: 11448722.(modified!)

Effect of M-current inhibition on neuronal excitability(„M“-current refers to the inhibition exerted by acetylcholine via mACh-receptors)
Jentsch (2000), PubMed PMID: 11252765.

Nig
roet
al.,
20
14
Pu
bM
edP
MID
: 2
48
28
63
4

Schroeder et al.(1998), PubMed PMID: 9872318.
BFNC mutations in red box!(heterozygous situation marked in yellow)
The moderate loss of channel function, which was postulated for BFNS patient brains,
suggested restricted availability of KCNQ2/KCNQ3 channels at this early phase of life, in
which these transient form of epilepsy occurs.
LQTS mutations in blue box!


Hedrich et al., 2019 PubMed PMID: 31904120.
a related epilepsy syndrome, benign familial neonatal/infantile seizures (BFNIS) can be caused by mutations in the SCN2A (Nav1.2) gene. In BFNIS, seizures occurin the neonatal and early infantile period; spontaneous remission in most cases before the age of 12 months.

Hedrich et al., 2013 (https://nwg-info.de/sites/nwg-info.de/files/media/pdf/neuroforum/2013-2.pdf), modified from:Liao et al., 2010 PubMed PMID: 20371507.
persistent INa+ in SCN2A mutant! replacement of Nav1.2 by Nav1.6in neurodevelopment: cause of remission?!

Mutations in the CACNA1H gene (Cav3.2, a T-type calcium channel) causeabsence epilepsy in children:
CAE: „childhood absence epilepsy“
Topology of Calcium Channels
α1 subunits and
channel nomenclature
Fig.
fro
m: H
arri
son
et
al. (
20
18
), P
ub
Med
PM
ID: 2
91
69
63
4.

Childhood absence epilepsy (CAE) typically begins between
4 and 8 years of age.
Absence seizures are the main seizure type. These are brief
staring spells during which the child is not aware or
responsive.
Each seizure lasts about 10 to 20 seconds and ends abruptly.
Without treatment, seizures typically occur many times a
day.
The seizures usually disappear by late childhood or mid-
adolescence.
Childhood Absence Epilepsy
3 Hz generalized spike wave EEG pattern!

detail of the onsetoverview of entire
electrographic seizure(duration about 8 sec)
EEG: absence seizure

LVA: low voltage-activated(T-type calcium channels, Cav3.x family)
HVA: high voltage-activated(L-type calcium channels: Cav1.x family)(P/Q-type, N-type and R-type calcium channels: Cav2.x family)
„transient“ LVA calcium currentsand
„long-lasting“ HVA-calcium currents
T-type calcium channels belong to the superfamilyof LVA calcium channels
typicalpeak current/voltage-relation
of voltage-gated calcium currents(as illustrated in the right panel).

Several mutations in the CACNA1H gene have been identified in children with CAE. (for some of these „gain of function“ was demonstrated).
This may lower the threshold for „rebound burst firing“.→ hyperexcitability, →→ seizures!
[CACNA1H mutations may also cause idiopathic generalised epilepsy (IGE)].
Fig.
fro
m: W
eier
gräb
eret
al.
(20
10
), P
ub
Med
PM
ID: 2
00
26
35
6.

The thalamus act as a rhythm generator: (a), thalamus in oscillator mode.
in which T-type calcium channels play an essential role.
The formatio reticularis (F.r.) acts in a desynchronising mode (in wakefullness),thalamus in transfer mode (b).
Fig.
fro
m: S
tep
han
Zsc
ho
cke,
Han
s-C
hri
stia
n H
anse
n (
Her
ausg
eber
):
Klin
isch
e E
lekt
roe
nze
ph
alo
grap
hie
. Sp
rin
ger;
3. A
ufl
age
(20
12
),
ISB
N-1
3: 9
78
-3-6
42
-19
94
2-4
(mo
dif
ied
!).
„gain of dunction“mutations in CACNA1H
may triggerhyperoscillatory activity!
afferent input
efferent output
synchronized desynchronized
Cortex
the thalamus: “gateway to the mind”

Variants in the CHRNA4 and CHRNB2 genes (coding for α4- and β2-subunits of thenicotinic acetylcholine-receptor) were linked to ADNFLE (autosomal dominante nocturnal frontal lobe epilepsy).
Fig.
fro
m: L
erch
e et
al.
(20
05
),
Pu
bM
edP
MID
: 16
10
14
52
.
17 subunits (α1–10, β1–4, γ, δ, and ε)are available for formation of pentameric receptors
α4β2-pentamers represent the predominante type of nAChR in the CNS!

ADNFLE: autosomal dominant nocturnal frontal lobe epilepsy
onset: 9-11 years, seizures perist through adult life
focal-onset frontal lobe seizuers
during stage 2 sleep (never in REM sleep)
duration: typically less than a minute
seizure frequency: typically 2-3 per night, not necessarily every night
seizure starts with bizarre vocalizations: moaning , gasping
or grunting
then prominent motor activity such as hyperkinetic thrashing movements with bipedal and bimanual
automatisms, …
the first epilepsy for which a monogenic cause was identified

figure from: Turnbull et al., 2005 (PMID: 16278970)
Various models have been proposed to explain the cause of epilepsy by ADNFLE
mutations in central nAChRs.
e.g.Cohen-Lester Model
(Rodrigues-Pinguet et al., 2003 (PMID: 12754307) , Rodrigues-Pinguet et al., 2005 (PMID: 15901849))
However, the finding that one of the ADNFLE mutations leads to epilepsy only when expressed embryonically
but not when expressed in adult animals questions models such as the one mentioned above, and point to
effects that occur already during development of the nervous system!
(Manfredi et al., 2009 (PubMed PMID: 19153075); Gullo et al., 2014 (PubMed PMID: 25104926)).
nAChR mutants cause a reduction in autoinhibition of nicotinic facilitation of glutamate neurotransmission that
is caused by Ca2+-depletion in the synaptic cleft, but do not alter inhibitory GABAergic transmission.

◙ Single defects in genes coding for ion channels can cause epilepsy
(e.g.SCN1A → GEFS+/SMEI, KCNQ → BFNS, CACNA1H → CAE, CHRNA4 → ADNFLE)
◙ Penetrance never 100%, → genetic defects only epileptogenic in a particular
phenotypic environment.
• allelic imbalance
•„Mosaicisms“:
penetrance ADNFLE (CHRNA4, CHRNB2): about 70%penetrance BFNS (KCNQ2, KCNQ3): about 85 %
General considerations regarding Chapter 1:

◙ differnt mutations of a particular gene may lead to differnt syndromes
(z.B.: SCN1A: GEFS+ vs. SMEI vs….)
(z.B.: GABRG2: GEFS+ vs. CAE)
(z.B. CHRNA4: ADNFLE vs. JME)
◙ one particual epilepsy syndrome can be caused by dysfunction of different genes
(z.B.: GEFS+: SCN1A vs. GABRG2)
(z.B.: CAE: CACNA1H vs. GABRG2)
(z.B. ADNFLE: CHRNA4 vs. CHRNB2)
(z.B.: BFNS: KCNQ2 vs. KCNQ3)
◙ both „loss-of-function“ as well as „gain-of-function“ channel mutations can act
in an epileptogenic manner
General considerations regarding Chapter 1:

Alterpredominantly genetic causes
idiopathic epilepsies(= a “disease of its own kind”)(most often „channelopathies“)
when symptomatic than typicallydue to developmental anomalies ormetabolic dysfunction
symptomatic epilepsies(resulting form another disease
or acute damage: stroke, haemorrhage, trauma)
„translational channelopathies“
Incidence of epilepsy
Chapter 1
Chapter 2

Chapter 2
Ion channel dysfunction in acquired(= symptomatic) forms of epilepsies

Le
rch
e e
t a
l. , 2
01
3 (
Pu
bM
ed
PM
ID: 2
30
90
947)
Ion channel dysfunction also appears to play an essential role in acquired
(= symptomatic) forms of epilepsies

from: Ferhat, Int J Cell Biol. 2012;2012:474351. PubMed PMID: 22611398.
Most of the findings were made using the status epilepticus-model of acquired epilepsy
(which employs pronconvulsant compounds such as pilocarpine or kainic acid)
Review articles regarding this model:
Löscher and Brandt (2010), PubMed PMID: 21079040.
White (2012), PubMed PMID: 22787641.

Poo
los
(20
12
), P
ub
Med
PM
ID: 2
27
87
67
7.
Loss of function of HCN channels enhances the excitability of pyramidal neurons(demonstrated using the HCN channel blocker „ZD 7288“)
but an increase of the HCN-mediated current (Ih) may also lead to seizures; forexample by causing rebound activity after inhibitory postsynaptic potentials (IPSPs).
Chen (2001), PubMed PMID: 11231632.

Fig.
fro
m: W
eier
gräb
eret
al.
(20
10
), P
ub
Med
PM
ID: 2
00
26
35
6.

If you have further questions regarding the implication of ion channels in epilepsy,
please contact me at:
„transcriptional channelopathy“ , a term coined for HCN channels in epilepsy