ARDS - principles of mechanical ventilation
101
Principii de ventilatie in ALI/ARDS SUUB Clinica Anestezie Terapie Intensiva
-
Upload
cosmin -
Category
Health & Medicine
-
view
200 -
download
5
description
ARDS - overview of principles
Transcript of ARDS - principles of mechanical ventilation

Principii de ventilatie in ALI/ARDS
SUUB
Clinica Anestezie Terapie Intensiva

ALI / ARDS – Definitie:
American-European Consensus Conference – 1994
Sindrom caracterizat prin inflamatie acuta si
persistenta, permeabilitate vasculara si alveolara
crescuta

ALI / ARDS – Definitie:
• Debut acut
• Infiltrate pulmonare bilaterale
( ˜EP) pe RxCP
• PaO2/FiO2 = 201-300 mmHg
PaO2/FiO2 ≤ 200 mmHg
• PAWP≤ 18 mmHg sau/si fara dovada clinica de LAH
-Revarsat pleural -Volum pulmonar redus -Variabilitate -CT
-PEEP? MAwP? -D.p. cu frecventa EAB, care EAB este ales -La FiO2 <0,5 – nu mai reflecta suntul
-ALI + EP – PAWP > 18 -E TOR sau MAwP , PEEP -Protocol ptr diagnostic clinic de LAH



ALI / ARDS – Dg. Diferential:
• EP cardiogen
• DAH
• Pneumonia acuta eozinofilica idiopatica
• Pneumonia lupica
• Proteinoza alveolara
• Infiltrat leucemic
• Sarcoidoza
• Pneumonia acuta interstitiala (Hamman-Rich)
• Clinica
• Istoric
• Eco
• BNP
• Swan Ganz
• Bronhoscopie
• Biopsie
• CT

DIRECT LUNG INJURY
• Pneumonia
• Aspiratia continutului gastric
• Contuzia pulmonara
• Inhalatie de toxice
• Inecul
INDIRECT LUNG INJURY
• Sepsis
• Traumatism nou toracic sever
• Bypass CP
• Pancreatita acuta
• Arsuri
• TRALI
cea mai frecventa cauza
extraspitaliceasca
cea mai frecventa cauza

Patogeneza:
• activare neutrofile, macrofage, plachete
• citokine: IL1β, TNFα, IL6, IL8
• radicali liberi, proteaze
• activare complement
• eicosanoizi: PGI2, LT, TXA2
• NO
• PAF

Consecinte morfopatologice:
- Injurie la nivelul endoteliului capilar si epiteliului alveolar
- edem interstitial si alveolar
- fluid proteinaceu, celule distruse
- pierdere surfactant
colaps alveolar

Consecinte fiziopatologice:
• Schimburi gazoase alterate - V/Q mismatch - sunt - VD fiziologic HCO2 • Complianta scazuta -- “baby lung” (Csp ~ N)
• HTP (25%) - VC hipoxica - PPV - HCO2 - subst VC (PAF ) - injurie parenchim pat vascular - IC dr acuta RAR
hO2

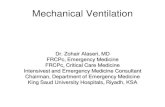
Figure: Schema representation of sponge model. In ARDS the “tissue”, likely edema in the early phase, is almost doubled in each lung level compared with normal, indicating the nongravitational distribution of edema. The increased mass, however, causes an increased superimposed pressure (SP), which in turn, leads to a “gas squeezing” from the most dependent lung regions. Superimposed pressure in expressed as cm H2O. The values indicated in the figures are taken from Pelosi and cowerkers.

1. Greutatea inimii in pozitie supina
2. Cresterea presiunii abdominale


ARDS = Heterogenitate
• Intre pacienti
• In timp, la acelasi pacient
• In acelasi plaman
-Regiuni inflate – mult, putin, mediu -Regiuni consolidate (sticky atelect) – deja proces de fibrinoformare
-Regiuni atelecto-colabate(loose atelect)- mecanism presional
Faza precoce
(0-3 zile)
Faza tardiva
(>7 zile)
Colagen
structural
puternic degradat
Atelectazie ++++ ++
Edem ++++ ++
Mecanica heterogena mai putin heterogena
VILI edem si
hemoragie
pneumotorax
pneumatocele

Factori determinanti ai presiunii de deschidere:
1. Absenta surfactantului
2. Ppl, SP mai crescute in partea dependenta
3. Reducerea compliantei toracice
4. Fibrinoformare
5. Marimea alveolei(T=Δ pr/2h)

•
• EL > N TP VILI / VALI
• EW > N TP Ppl Alterare hemodinamica


Mecanica heterogena • Deschiderea plamanului are loc la p > decat colabarea
• Deschiderea unor unitati poate presupune hiperinflatia altora


Mecanica respiratorie
ARDS pulmonar vs. ARDS extrapulmonar
• Consolidare ↑
• EL ↑↑ ↑
• Raspunde la manevre de re rutare↓
• Nu raspunde la pozitia prona
• R ~
• ERS ~
• Sticky atelectasis
• Risc de barotrauma
• IAP normal
• Ground-glass
• EW ↑↑, EL ↑
• Raspunde la manevre de re rutare ↑
• Raspunde la pozitia prona
• R ~
• ERS ~
• IAP ↑↑ ~ EW
• Edem interstitial
• Loose atelectasis
• Risc de alterare hemodinamica

Figure: Changes of static
elastances of the respiratory
system (Est,rs), lung (Est,L), and
chest wall (Est,w) as a function of
PEEP in pacients with ARDS
caused by pulmonary disease
(Group 1, top panel) with in
ARDS caused by extrapulmonary
disease (Group 2, bottom panel).
Comparison within each group:
*p<0.05 versus PEEP O cm H2O;
**p<0.01 versus PEEP O cm
H2O. Comparison between the
two groups; ^p<0.05 versus
Group 1; ^^p<0.01 versus Group 1.



VILI / VALI
Def:
“Acute lung injury that develops during mechanical ventilation is termed VALI if one cannot prove beyond any doubt a causative relationship.
VILI – a causative relationship can be proven.”

VILI / VALI Principalele cauze:
1. Barotrauma
2. Volutrauma
3. Atelectrauma
4. Toxicitatea oxigenului
5. Biotrauma

BAROTRAUMA
Cauzata de: Include:
• MAwP ↑ • PP ↑ • PEEP ↑
• Emfizem interstitial • Pneumomediastin • Pneumotorax • Embolism gazos
Odata principala cauza de VILI Astazi “doar” un accident mecanic

VOLUTRAUMA (supradistensia alveolara)
• Volumele tidal mari produc ALI
• 2 studii pe animale demonstreaza ca volumele tidal mari, nu presiunile, produc ALI
• In realitate presiunea TP explica ambele fenomene si:
-- presiunile mari nu produc tot timpul
barotrauma (Cw )
-- volumele mici pot produce ALI (CL )

Extravascular lung water (Qwl), dry lung weight, and albumin space are indicative of the development of lung injury. These abnormalities were induced in rats ventilated with high pressure and high tidal volume (HiP-HiV), low pressure and high volume (LoP-HiV), but not in those ventilated with high pressure and low volume (HiP-LoV). Redrawn from Dreyfuss, D,Soler, P,Bassett, G, Saumon, Am Rev Respir Dis 1988

The effect of limited intrathoracic expansion by means of a body cast on ventilator-induced lung injury in rabbits. Rabbits were ventilated with 15, 30, and 45 cmH20 peak inspiratory pressure for one hour. Redrawn from Hernandez, LA, Peevy, Kj, Moise, AA, Parker, JC, J Appl Physiol 1989.

Atelectazia ciclica
(atelectrauma; shear stress trauma)

ATELECTRAUMA (interdependenta alveolara)

Popping open of lung units under high pressure might be the answer





• “cyclic stress “ endotelial • Zona 2 intermitenta
• Forte de sens opus la nivelul lumenului ce uneste cele doua tipuri de vase


Toxicitatea oxigenului • Form rad. liberi
• Atelectazie de resorbtie
• Studii pe animale cu FiO2=1
• Voluntari umani respirand FiO2=1
• Target: FiO2 ≤ 0,6
• Target: PaO2 = 55-80
SpO2 = 88-95%
Importanta hipoxemiei depaseste pe cea a
toxicitatii O2
- superoxid - hidrogen peroxid - ion hidroxil
DECES IN 48-72 h (ALI/ARDS)
RASP INFLAMATOR IN 24 h

BIOTRAUMA
• Rasunet celular al unui pattern ventilator inadecvat
• Presupune mecanotransductie
• Producere excesiva si import inadecvat de mediatori
inflamatori si antiinflamatori
• Raspunsul inflamator este intra si extracompartimental
(decompartimentalizare)
• Predispune la SIRS si MODS
• Alterarea patternului de crestere bacteriana si
imunosupresie

MECANOTRANSDUCTIA

BIOTRAUMA

Lung protective ventilation
Conventional “Lung protective”
Large tidal volume Small tidal volume
Minimum PEEP “Sufficient PEEP”
Normalize PaCO2 Permissive hypercapnia
Unrestrained airway pressure
Pressure limitation
1. Open Lung Ventilation
“Open up the lung and keep
the lung open” (1992, Lachmann)
2. ARDS net

Open Lung Ventilation(1)
• Volume tidal mici (4-8 ml/kgc) (˜ ARDS net)
• Pplateau ≤ 25-30 cm H2O (˜ ARDS net)
• Manevre de recrutare
• PEEP optimizat
• RR ≤ 35/min (˜ ARDS net)
• Compromis:
HCO2, hO2 (˜ ARDS net)

Open Lung Ventilation(2)
• Nu exista un protocol universal
• Mare variabilitate
• Optimizarea PEEP-ului, manevra de recrutare, potential de recrutare – puncte de interes
• Abordare fiziopatologica
• Permite individualizarea ventilatiei
• Presupune cunoastere aprofundata a mecanicii respiratorii

Model clasic de Open Lung Ventilation (Lachmann)
Action (1) Data Comments
Pacient at day 2: volume controlled ventilation with tidal volumes of 6 ml/kg
FiO2=70%; PEEP=11cm H2O RR=32; I:E=1:2; SaO2=92% ; PAWP=26cmH2O ; TV=6 ml/kg=480 ml; PaO2=72mmHg; PaCO2=48 mmHg
Switch to pressure controlled ventilation FiO2 set to 100% I:E=1:1; RR:40 PAW 26 cm H2O PEEP 20
SaO2=100% PaO2=140 mmHg PaCO2=39 mmHg
Increase PAWP to 45 cmH2O for three breaths (5 seconds), then back to 30
PaO2=265 mmHg
1 min after stabilization increase PAWP to 50 for 5 sec, then back to 30
PaO2=350 mmHg
1 min after stabilization increase PAWP to 55 for 5 sec, then back to 30
PaO2=530 mmHg PaCO2=28 mmHg

Model clasic de Open Lung Ventilation (Lachmann)
Action (2) Data Comments
1 min after stabilization increase PAWP to 60 for 5 sec, then back to 30
PaO2=531 mmHg PaCO2=28 mmHg
PaO2 does no further increase. Opening presure=55 cmH2O.
Decrease PAWP to 28-24 No changes
Decrease PAWP to 23 PaO2=480 mmHg The lung is collapsing. Minimum required upper pressure limit = 24 cmH2O
Recruit the lung (PAWP to 55, then 24)
Reach opening pressure and airway pressure set back just above collapse pressure
PAWP 24, decrease PEEP to 18 No changes
PEEP to 17 PaO2=541 mmHg
PEEP to 16 PaO2=470 mmHg Minimum required lower pressure limit = 17 cm H2O

Model clasic de Open Lung Ventilation (Lachmann)
Action (3) Data Comments
Set PEEP to 17 Increase PAWP to 55 for 5 sec (recruit) and back to 24
PaO2=544mmHg PaCO2=34 mmHg
Optimal CO2 removal requires VCO2 of 430 ml/min; Slight hyperventilation
Increase RR to 47 I:E=3:2
PaCO2=36mmHg VCO2=435 ml/min TV=395 ml=4,9
Smaller pressure amplitude due to auto-PEEP and increased dead space ventilation
Decrease FiO2 to 30% PaO2=114 mmHg PaCO2=36 mmHg
Optimized patient ventilation at open lung

Manevre de recrutare • Nu exista “o cea mai buna”
• Cele mai folosite: 1 si 2
• 1:Cel mai mare impact hemodinamic
• 3>1 daca presiuni mai mari ca cele tolerate la 1 sunt necesare
• 1>3 pentru ca recrutarea depinde mult de MANP

Recrutam pas cu pas?
When collapse is prevalent (top), the overall pleural pressure results very low and the local transpulmonary pressures increase significantly. The risk of overdistension is very high at this condition, especially if one considers a single step – high pressure recruiting maneuver. Contrarily, we propose the application of lower pressure at this moment (top), increasing it progressively as new units get recruited.

Facilitarea recrutarii • Pozitie prona
• Presiune de inspir adecvata (40-45 cmH2O)
• PEEP adecvat
• Cel mai mic FiO2 acceptabil (in afara momentului recrutarii – Lachmann)
• Respiratie spontana posibila
(BIPAP, Autoflow, APRV)
• Minimizeaza edemul interstitial
(repletie volemica adecvata,
monitorizare EVLW-PICCO,Vigileo,
TA invaziv - ∆do +∆up)

Factori determinanti ai eficientei recrutarii (1)
• Tipul de ARDS EP>Pulm
• Stadiul ARDS
• Punctul de pornire
• PEEP postrecrutare
• Tipul de manevra
• PaO2/FiO2 < 150 (at PEEP 5 cm H2O)
• RxCP – voalat
• LIP – pe curba PV, bratul inspirator

Factori determinanti ai eficientei recrutarii (2)
• Recrutezi doar ce este recrutabil
• ↑PEEP are se s pe tru pla a ul re ruta il
• Cat de recrutabil este recrutabil?
ENGSTRÖM
> 9 % CT

Cel mai des derecrutezi prin:
• FiO2 ↑ (>0,6) pentru ∆t ↑
• Aspiratie / Bronhoscopie

Care este PEEP-ul optim?
Maximum de recrutare cu minimum de distensie
Electric impedance tomography (EIT) images are presented on the right, whereas the corresponding CT images (obtained at the same PEEP level) are represented in the left side of the figure. The EIT images represent the ventilation map during tidal breaths. Brighter areas indicate pixels with larger impedance variations (larger alveolar ventilation) during tidal breaths. Excessive, as well as insufficient PEEP levels, caused uneven ventilation. Excessive PEEP caused preferential ventilation in the dependent lung zones (because of the relative overdistention of non – dependent lung zones). Insufficient PEEP caused dependent collapse with preferential ventilation towards the patent airspaces at the non- dependent “baby lung”.

Care este PEEP-ul optim?
1. Curba P-V brat inspirator (Engstrom dynostatic curve – dynostatic algorithm, constant low flow P-V loop pe Drager (VCV))
2. DO2
3. Evaluare PaO2,PaCO2
4. Monitorizarea compliantei tidal (CRS)
5. Indexul de stress
6. CRF, volum recrutat - Engstrom
DO2>600 mlO2/min chiar cu PEEP ↓ → atele trau a ↑

Clasic: -Faza 1 – recrutare -Faza 2 – inflatie normala -Faza 3 -- supradistensie
In realitate…
CURBA P-V

Evaluare PaCO2, PaO2
A. Model Lachmann (PaO2)
B. PaCO2 -- necesita VCV (MV=const)
--la ↓ PEEP de la 5 - 20):
1. PaCO2 ~ (overdist=recr)
. PaCO ↓ re r>o erdist
. PaCO ↑ dere rutare
PEEP optim = cea mai mica PCO2
Dezavantaje redistributia sangelui intre teritorii cu V/Q
diferit

CRS
• Cea mai la indemana
• CRS d.p. cu recrutare/supradistensie
• Dezavantaje:
- CRS are Sb ↓ la ei u C ↓
- ∆CRS su t ↓↓

Stress index
• Analiza in dinamica a curbei P-T (Paw)
• Ventilatie cu flux constant (VCV)
• Permite (teoretic) optimizarea ventilatiei
- setare PEEP optim
-setare VT optim
• Vede raportul recrutare/supradistensie
• Nu vede recrutarea sau distensia
• Pp. culegerea de semnale cu frecventa ↑
• Foarte controversata
• Odata efectuata optimizarea autoflow

Stress index





Date statistice (1)
ARMA TRIAL (ARDS Network)
• Studiu prospectiv, randomizat, multicentric
• 861 pacienti cu ARDS
• 12 ml/kg (A) vs 6 ml/kg (B) volum tidal
• Grupul B: rata mortalitatii ↓ (31% vs 40%)
• Grupul B: zile fara ventilatie mecanica (12 vs 10)

Date statistice (2)
ALVEOLI TRIAL (ARDS NETWORK)
• Studiu prospectiv, randomizat, multicentric
• 768 pacienti cu ARDS ventilati conform ARMA
cu exceptia FiO2 / PEEP
• PEEP ↑ s PEEP ↓
• PEEP mediu 13 vs 8
• Rata mortalitatii: scadere nesemnificativa statistic
• NB: Nu s-au efectuat MR
• NB: Grupul PEEP ↑ -pacienti cu varste mai ↑
- PaO2/FiO2 mai ↓

Date statistice (3)
• Fara impact pe mortalitate • A – incidenta mai mica a hO2 – recuperare mai rapida • Majoritatea studiilor au limite -- potentialul de recrutare este omis -- + MR - PEEP -- + PEEP - MR -- heterogenitate dpdv al bolii de baza -- randomizare defectuoasa (pacienti mai varstnici cu PaO2/FiO2 mai in grupul A)
Recrutezi doar ce e recrutabil! Castigi doar unde poti castiga!
(A) Open Lung Ventilation MR PEEP optim/ ↑
(B) Conventional LPV ARDS net

PRO si CONTRA respiratie spontana in
managementul ventilator ALI/ARDS
PRO
• V/Q ↑in teritoriile
supradiafragmatice
• Efort inspirator
Ppl ↓ ↑TP
↑ raspu sul la MR
• CO↑ DO2 ↑
CONTRA
• VO2
• VCO2
• ITBV EVLW
EDEM
SP,Ppl
TP
Atelectazie
Efort exp ↑ Ppl↑

PRO respiratie spontana

PRO respiratie spontana

PRO respiratie spontana

Hipercapnia permisiva - Efecte
Hemodinamice si CV:
• Simpaticotonie
• MS + Catecolamine
• inotropism (pHi , direct)
• VD (direct, pHi )
• VD coronariana in teritoriile normale furt
• VC pulm prin reflex von Euler Lyljestrand
• Curba disociere O2 la dreapta SaO2 dar elib. Tis. O2
• Creste QT
• Scade injuria mitocondriala in modele de ischemie/ reperfuzie
↑HR, ↑ SV, VC


Hipercapnia permisiva - Efecte
SNC:
• VD cerebrala in teritoriile normale furt
• CBF
• ICP CPP
• Convulsii (la peste 100 mmHg)
Diverse:
• renal
• HK+

Hipercapnia permisiva
Are the effects of high PaCO2 deleterious or Protective?
CO2
Activation of signal
transduction pathways
Decreased alveolar fluid Cl
Decreased inflamatory
response
Decreased VILI/VALI

Hipercapnia permisiva – Contraindicatii
(absolute si relative)
• ICP ↑ trau a, tu ora, HTA se era
• Acidoza metabolica severa
• B. coronariana, IC, aritmii
• Tratament cu beta blocante
• HTP, IC dreapta
• Hipovolemie
• Sangerari GI
• Siclemie
• ATC – supradozaj
• Sar i a ris de FBF ↓ pri sdr. de furt datorat VD

Hipercapnia permisiva – Principii
1. Monitorizare atenta pana la stabilizarea PaCO2
2. PaCO2 gradata (≤10 mmHg/h) pt efecte adverse ( ∆t suficient pt autoreglarea pHi)
3. Limita PaCO2 – 80 mmHg (exceptional 100mmHg)
4. pH target 7,15 – 7,20 sau 7,30 – 7,45 (ARDS net)
5. Nu exista consens in privinta corectarii acidemiei datorata PaCO2
Cand? Cu ce? Cum?

Hipercapnia permisiva
• PRO pH≥7,15
• PRO pH=7,3-7,45
• CONCLUZIE: 1. Nu corectezi acidemia (pH-ul) ci acidoza 2. Acidoza este un raspuns individual la acidemie (ex – instab. hemod) Corectarea se va face individual (vezi CI) iar pH-ul este UN semnal de alarma si NU indicator al corectarii
Cand?
-Relativ bine tolerata cand PaCO2a treptat - VALI independent de VT
- pH fiziologic

Hipercapnia permisiva
1. Setarea parametrilor ventilatori (RR, VT) a.i. sa ramai in intervalul de LPV
2. Adm subst alcalinizante
-- NaHCO3 – folosit in protocolul ARDS net
-- THAM (trishidroximetilaminometan – R – NH2)
-- Carbicarb- amestec echimolar CO3/HCO3
NaHCO3+H+
H2CO3 CO2 PaCO2
CO2icel ↓pH icel
Obs: PaCO2 este temporara
pH icel este temporara VA=const – PaCO2 dp FACO2=
Adm NaHCO3 treptata are impact minim pe PaCO2, pHicel
Cu ce?
Cum?

Interventii de salvare in managementul ventilator
1. Ventilatia in pozitie prona
2. TGI (tracheal gas insufflation)
3. ECMO (extracorporeal membrane oxygenation)
4. EC CO2R (extracorporeal CO2 removal)
5. LPPPV – EC CO2 R (low frequency positive pressure vent + EC CO2 R)
6. HFV (high frequency ventilation)
7. LV (liquid ventilation)
8. ILV (independent lung ventilation)
9. PC – IRV (pressure controlled inverted ratio ventilation) clasic, APRV (airway pressure release ventilation) modern
10. Surfactant inhalator
11. Redistribuirea din teritorii de sunt inspre teritorii ventilate: NO inhalator, Almitrina iv, prostanoizi inhalator (epoprostenol, iloprost)

Ventilatia in pozitie prona – Robin Hood
SUPINA PRONA
VENTRAL (x): Va, Qa, CRFa
NON-DEPEND
DORSAL (y): Vb, Qb, CRFb
DEPEND
QbQa; Va>Vb
CRFa>CRFb
CRFa+CRFb = CRFz
Va/Qa (>N); Vb/Qb (<N)
Va+Vb=Vz
VENTRAL (y): Vd, Qb((Qa+Qb)/2),CRFd
NON-DEPEND
DORSAL (x): Vc, Qa((Qa+Qb/2)), CRFc
DEPEND
Vd>Vb(Ppl )(Vd/Qb)>(Vb/Qb)
deci Vd/Qb N
Vc<Va (Ppl ) (Vc/Qa)<(Va/Qa)
deci Vc/Qa N
Vd+Vc= Vz
CRFd>CRFb (Ppl )
CRFc<CRFa (Ppl )
CRFd+CRFc = CRFz

Ventilatia in pozitia prona
SUPIN: Cwstern – Cwcol ventilatie ventrala
(PTPventr – PTPdorsal )
PRONA: Cwstern – Cwcol ventilatie ventrala + dorsala
(PTPventr – PTPdorsal )
• Distributie diferita a VT (mai omogena)
• PTP omogenizata (Ppl omogenizata)
• Cw dar Cw e mai omogenizata
• Perfuzie putin modificata
rasp la MR

Ventilatia in pozitia prona Contraindicatii: • Trauma col. vertebrala (CI majora) • Instabilitate hemodinamica (CI relativa puternica) • Chirurgie toracica+abd (CI relativa) Riscuri: - Instab hemod 1,1 % / ciclu - Extubatie 0,4 % /ciclu - SaO2 scazuta 0,3 % / ciclu - Dislocare CVC 0,1 % / ciclu - Dislocare cat femural 0,1 % / ciclu - Obstructie sonda IOT 0,1 % / ciclu - TPSV 0,1 % / ciclu

Ventilatia prona SUMMARY AND RECOMMENDATIONS • Prone positioning appears to improve the oxygenation of most
patients with ALI or ARDS; however, a mortality benefit has not been established.
• Post-hoc analyses of multiple studies suggest that the greatest benefit of prone positioning occurs in the sickest patients if used early after the diagnosis of ALI or ARDS.
• Duration: The optimal duration of prone positioning is unknown. While many studies have used repeated sessions lasting approximately six to eight hours per day, impressive and persistent improvements in oxygenation have been noted with prone positioning of longer duration
• Routine prone positioning of all patients with ALI or ARDS is not recommended because there is substantial inconvenience associated with its use and there is insufficient data demonstrating improvement of patient-important outcomes.
• In our clinical practice, however, we implement prone positioning early in selected patients with ALI or ARDS. Specifically, we initiate prone positioning if our goals of lung-protective ventilation are not being met, or if there is persistent respiratory acidosis or tissue hypoxia despite standard ventilation in the supine position. This reflects our belief that the risks of prone positioning are minimal when properly performed and that the physiologic rationale for its use is sound.
www.UpToDate.org

Insuflatia traheala (TGI)
• Concept vechi (1969)
• Mapleson D.
• Flux secundar de O2/aer la niv carinei
• Necesar doar spre sfarsitul expirului
• Cateterul TGI spre carina sau spre circuitul ventilator ( PEEP)
• TGI flow 4-15 l / min
• Eficienta pentru Vda/Vdf 1
• Pentru siguranta trebuie sa “comunice” cu ventilatorul
TGE (Tracheal Gas Exsufflation) Sistem coaxial (5mm+8mm)

HFV (High Frequency Ventilation)
• VT<Vsma si RR>60/min
• 4 tipuri: 1. HFJV(RR=100-150)
2. HFOV(RR≤900)
3. HFPV (HFOV+PCV)
4. HFPPV

HFV - Indicatii • There are no universally accepted indications for HFV. Its use has also been
described in a variety of clinical situations. HFV should be avoided in patients with obstructive lung disease. .
• There is evidence that HFOV and HFPV improve oxygenation, although neither has been shown to improve clinical outcomes (eg, mortality, duration of mechanical ventilation, or length of ICU stay).
• HFV is not risk free. Potential harms include intrinsic positive end-expiratory pressure (auto-PEEP), dynamic hyperinflation, and related sequelae (eg, pulmonary barotrauma, hemodynamic instability). In addition, there are specific risks associated with each type of HFV.
• Bronchopleural fistula — HFJV is approved by the United States Food and Drug Administration for ventilating patients in whom a large and persistent bronchopleural fistula exists. However, the likelihood that HFJV will allow the bronchopleural fistula to close is unpredictable. While HFJV may promote fistula closure by limiting alveolar distension, this may be outweighed in some patients by increased plateau airway pressure (alveolar pressure), decreased oxygenation, or worse hypercapnia.
• ALI/ARDS — The theoretical benefit of using HFV in patients with ALI/ARDS relates to the small tidal volumes. A strategy of low tidal volume ventilation has been proven in randomized trials to improve mortality, possibly due to decreased alveolar distension and ventilator-associated lung injury. Although the trials did not use HFV, many clinicians suspect that HFV confers a similar benefit. Until this is proven, HFV should not be considered routine care for patients with ALI/ARDS. HFV is used by some clinicians when there is persistent hypoxemia during the first three days of mechanical ventilation despite maximal conventional therapy, although the data to support this are limited
www.UpToDate.org

APRV / BIPAP

PC-IRV / VC - IRV

LV (TLV+PLV) • Ventilatie cu perfluorocarbon (Ex perflubron – C,H, fluor, brom-
radioopac)
• Carrier inert de oxigen si CO2(O2=15 x plasma)
• Nontoxic, abs sistemica minima, stabil chimic
• Incolor, inodor, limpede
• PFG abs e metabolizat de macrofage
• Eliminare I prin volatilizare
Avantaje:
1. TS
2. Rezervor de oxigen
3. Deschide si mentine deschise alveolele prin presiune hidraulica ( riscul de barotrauma)
4. ∆ Q minima
5. V/Q mismatch (PFG sunt grele si “merg” in zonele dependente)
6. Favorizeaza lavajul
7. Efect antiinflamator
In theory, LV may be of benefit for numerous neonatal and adult diseases. Clinical trials, however, have shown little improvement in important clinical outcomes. As a result, LV cannot be recommended in routine clinical care. (www.UpToDate.org)

Masurarea Vds / VT pe aparatul
Drager

Indicator of the Severity of Lung
Injury and a Predictor of Mortality
•For every 0.05 increase in dead space fraction, the odds of death increased by 45%.
•Other observational studies suggest that a value of 0.60 or higher may be associated with more severe lung injury.

Indicator of the Severity of Lung
Injury and a Predictor of Mortality

Indicator of Lung Overdistension
During PEEP Titration
• Optimum End Expiratory Airway Pressure in Patients with Acute Pulmonary Failure • Suter PM, Fairley HB, Isenberg MD. NEJM 1975
• Best PEEP corresponds to the lowest dead space fraction and the highest compliance

Anatomic Vd
Alveolar Vd
Components of
Physiologic Dead Space = Anatomic + Alveolar 20 – 40 %
15 – 25 %
5 – 15 %

Douglas Bag Exhaled Gas Collection
PēCO2 VDphys = PaCO2 - PēCO2 VT PaCO2

Dead Space Fraction Measurements
on the Dräger Ventilator
Uses Fowler Method to Calculate Anatomic Dead Space Fraction
and Volume
Vds / Vt Vds (mL)
Integrated Mainstream CO2 Sensor

Dead Space Fraction Measurements
on the Dräger Ventilator
VDphys = PaCO2 - PēCO2 VT PaCO2
FēCO2 x (760 – 47) = PēCO2
VCO2 = FēCO2 MV
VCO2 Minute Ventilation

Dead Space Fraction Measurements
on the Dräger Ventilator
• Requires manually averaging
VCO2 and MV over a 5 – 10 minutes especially with large variations.
• Validation study is not
complete.
• Requires commitment by Dräger to implement software revision.