APH and multiples - Wikispaces and multiples... · mately 20% of all cases of antepartum hemorrhage...
15
Antepartum haemorrhage & Multiple pregnancy Dr. Wajeih ALAali, SSCOG, ABOG, MFM Consultant OBGYN and Fetal medicine 1 Antepartum haemorrhage Bleeding from or in to the genital tract, occurring from 24+0 weeks of pregnancy and prior to the birth of the baby. 2 Antepartum haemorrhage CAUSES OF ANTEPARTUM HEMORRHAGE (APH) Common Placenta previa Preterm labor (marginal separation of placenta) Uncommon Uterine rupture Fetal (chorionic) vessel rupture Cervical or vaginal lacerations Cervical or vaginal lesions, including cancer Congenital bleeding disorder Unknown (by exclusion of the above) 3 Antepartum haemorrhage 4 APH and multiples - November 3, 2016
Transcript of APH and multiples - Wikispaces and multiples... · mately 20% of all cases of antepartum hemorrhage...
Antepartum haemorrhage & Multiple pregnancy
Dr. Wajeih ALAali, SSCOG, ABOG, MFMConsultant OBGYN and Fetal medicine
1
Antepartum haemorrhage
Bleeding from or in to the genital tract, occurring from 24+0 weeks of pregnancy and prior to the birth of the baby.
2
Antepartum haemorrhage CHAPTER 10 Obstetric Hemorrhage 137
obtaining a platelet count, serum fibrinogen level, pro-thrombin time (PT), and partial thromboplastin time. Additionally, the patient should be typed and cross-hatched for at least 4 units of blood (packed cells). A rapid but subjective method to test for coagulopathy is to partially fill a “red-top” tube with blood. If a clot does not form, or once formed does not stay clotted, the patient most likely has disseminated intravascular coagulation (DIC).
An important and accurate method of determin-ing the cause of bleeding in the late second trimester and the third trimester is ultrasonography. This eval-uation should include not only the location and extent of the placenta (initial ultrasonic assessment to rule out placenta previa) but also an assessment of gesta-tional age, an estimate of fetal weight, determination of the fetal presentation, and screening for fetal anom-alies. Uterine activity and the fetal heart rate should be assessed with a monitored strip to rule out labor and to establish fetal well-being (see Chapter 9).
Abnormal Placentation: Placenta Previa and Placenta AccretaPLACENTA PREVIAThe incidence of placenta previa, the most common type of abnormal placentation, is 0.5%. Approxi-mately 20% of all cases of antepartum hemorrhage are due to placenta previa. Seventy percent of patients with placenta previa present with painless vaginal bleeding in the third trimester, 20% have contractions associated with bleeding, and 10% have the diagnosis made incidentally on the basis of ultrasonography or at term.
Predisposing FactorsFactors that have been associated with a higher inci-dence of placenta previa include (1) multiparity, which is associated with changes in the size and shape of the uterus, providing more space in the lower uterine segment for implantation; (2) increased maternal age; (3) prior placenta previa; (4) multiple gestation; and (5) cesarean delivery, which also changes the shape of the lower uterine segment. Patients with a prior pla-centa previa have a 4-8% risk of having placenta previa in a subsequent pregnancy.
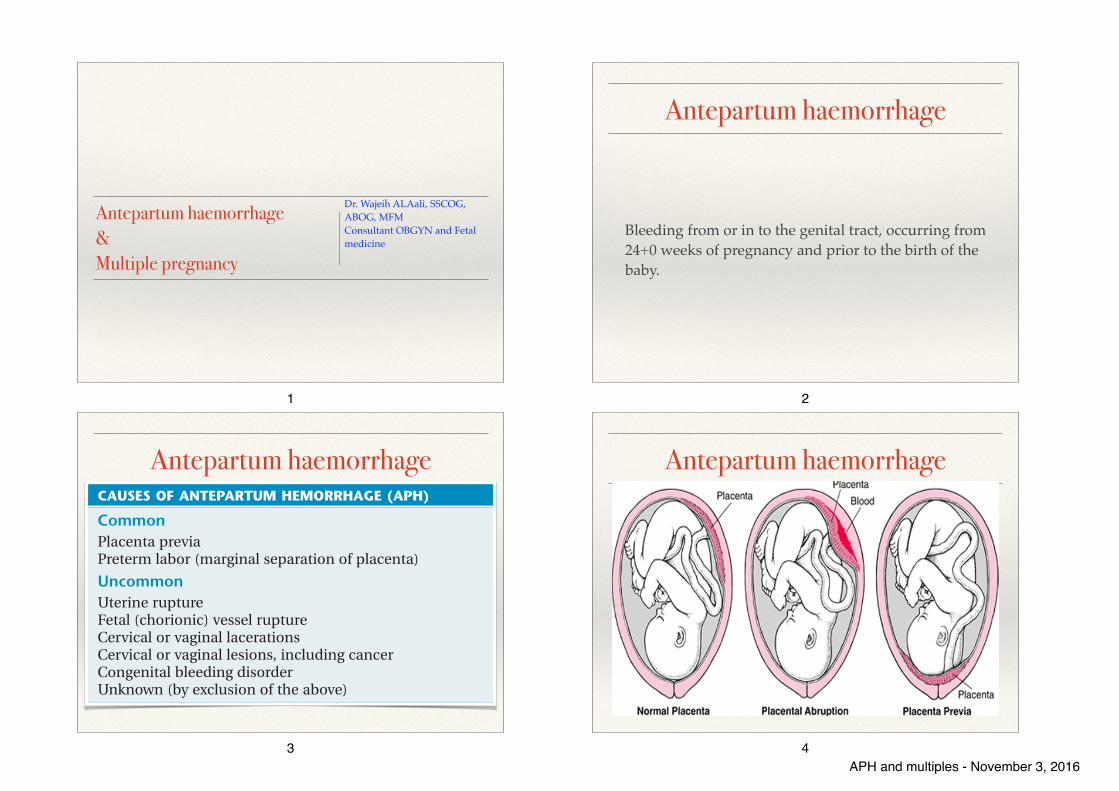
ClassificationPlacenta previa is classified according to the relation-ship of the placenta to the internal cervical os (Figure 10-1). Complete placenta previa implies that the pla-centa totally covers the cervical os. A complete pla-centa previa may be central, anterior, or posterior, depending on where the center of the placenta is located relative to the os. Partial placenta previa implies that the placenta partially covers the internal
well-being of both the mother and the fetus that the patient who presents with bleeding in the late second trimester and the third trimester be evaluated and managed emergently.
INITIAL EVALUATIONAfter a complete history has been taken, physical examination is performed, but a pelvic examination is usually postponed until an abdominal ultrasound has been obtained to rule out placenta previa. The differ-ential diagnosis of second- and third-trimester bleed-ing is listed in Box 10-1.
The vital signs and amount of bleeding should be checked immediately, as should the patient’s mental status. The patient’s medical history should be checked for known bleeding disorders or liver disease, which predispose the patient to coagulopathy. Once placenta previa has been excluded by abdominal ultrasound, a sterile speculum examination can safely be done to rule out genital tears or lesions (e.g., cervical cancer) that may be responsible for the bleeding. If none are identified, a digital examination or pelvic ultrasound may be performed to determine whether cervical dila-tion is present.
If a patient is bleeding profusely, a team approach to the assessment and management should be insti-tuted to establish hemodynamic stability. This team should include an obstetrician, an anesthesiologist, and nurses who are knowledgeable about the manage-ment of a potentially critically ill patient. At least two large-bore peripheral intravenous (IV) lines should be placed, as they allow the most rapid replacement of fluid and blood volume. A central venous pressure line, or preferably a pulmonary artery catheter, is helpful in the management of hypovolemic shock.
A complete blood count should be obtained and compared with previous evaluations to help assess the amount of blood loss, although acute blood loss may not be reflected in the hemoglobin level until homeostasis has been reestablished. An assessment of the patient’s coagulation profile should be done by
BOX 10-1
CAUSES OF ANTEPARTUM HEMORRHAGE (APH)
CommonPlacenta previaPreterm labor (marginal separation of placenta)
UncommonUterine ruptureFetal (chorionic) vessel ruptureCervical or vaginal lacerationsCervical or vaginal lesions, including cancerCongenital bleeding disorderUnknown (by exclusion of the above)
3
Antepartum haemorrhage
4APH and multiples - November 3, 2016
Antepartum haemorrhage Initial Evaluation
❖ Complete history:
✓ Bleeding disorder
✓ Liver disease
✓ Review previous US reports
❖ physical examination:
✓ Vital signs
✓ Amount of bleeding, Mental status
✓ Sterile speculum examination
❖ Abdominal ultrasound
❖ Digital examination !
5
Antepartum haemorrhage Initial Evaluation
❖ 2 large bore IV cannula
❖ Laboratory
✓ Complete blood count: Hb, HCT, platelets
✓ Coagulation profile: PT, PTT, Fibrinogen
✓ Blood group and cross match
❖ Ultrasound
6
Placenta previa
7
Placenta previa
❖ Incidence: 0.5% (1/200)
❖ Most common type of abnormal placentation
❖ 20% of all cases of antepartum haemorrhage
❖ Painless vaginal bleeding in the third trimester 70%
❖ Contractions associated with bleeding 20%
8APH and multiples - November 3, 2016
Placenta previa
❖ Maternal mortality(<1%)/morbidity
❖ Preterm birth
❖ Malpresentation 30%
9
Placenta previa
Risk factors:
❖ Multiparity
❖ Increased maternal age
❖ Prior placenta previa
❖ Multiple gestation
❖ Cesarean delivery
10
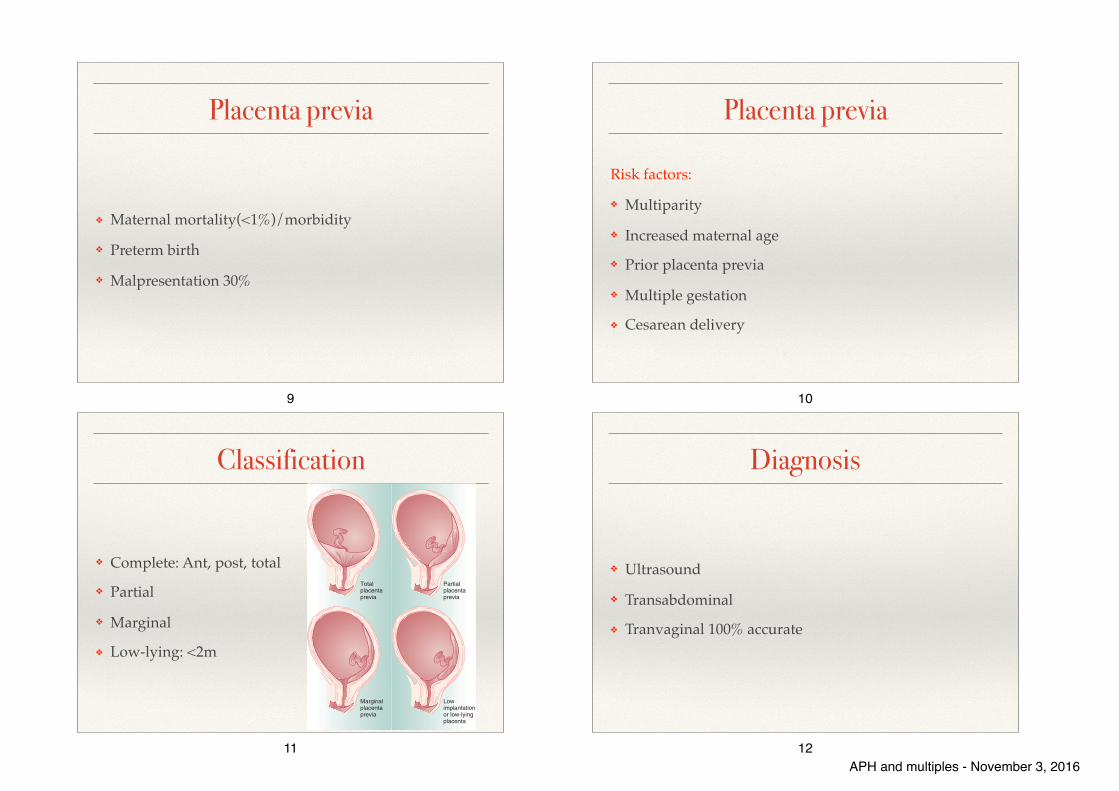
Classification
❖ Complete: Ant, post, total
❖ Partial
❖ Marginal
❖ Low-lying: <2m
PART 2 Obstetrics138
lower margin of the placenta may be obscured and the diagnosis of placenta previa missed. Transvaginal ultrasonography can accurately diagnose placenta previa in virtually 100% of cases.
ManagementOnce the diagnosis of placenta previa is established, management decisions depend on the gestational age of the fetus and the extent of the vaginal bleeding. With a preterm pregnancy, the goal is to attempt to obtain fetal maturation without compromising the mother’s health. If bleeding is excessive, delivery must be accomplished by cesarean, regardless of gestational age. When the bleeding episode is not profuse or repet-itive, the patient is managed expectantly in the hospital on bed rest. With expectant management, 70% of patients will have recurrent vaginal bleeding before completion of 36 weeks’ gestation and will require delivery. If the patient reaches 36 weeks, fetal lung maturity should be determined by amniocentesis and the patient delivered by cesarean if the fetal lungs are mature. Elective delivery is preferable, as sponta-neous labor places the mother at greater risk for hem-orrhage and the fetus at risk for hypovolemia and anemia.
LOW-LYING PLACENTAA patient with a low-lying placenta (placental margin within 2 cm of the endocervical os) may present in the same way as a patient with placenta previa. It may be difficult to distinguish a low-lying placenta from a mar-ginal placenta previa, but a transvaginal ultrasound is typically diagnostic. Vaginal delivery is not contrain-dicated, because during labor the fetal head com-presses the edge of the placenta, decreasing the risk of bleeding. The same level of monitoring should be maintained for maternal hemodynamic stability and fetal well-being.
MATERNAL-FETAL RISKSMaternal mortality from placenta previa has dropped from 30% to less than 1% over the past 60 years. This has primarily been due to the liberal use of cesarean delivery and careful expectant management. The rare maternal death is generally associated with compli-cations of cesarean delivery or uncontrolled hemor-rhage from the placental site. The lower uterine segment does not contract well, especially after a lower uterine incision. DIC may also result if a massive hemorrhage or an associated abruption occurs.
The risk of antepartum or intrapartum hemorrhage, or both, is a constant threat to the patient with placenta previa. Bleeding may be exacerbated by an associated placenta accreta or uterine atony. Placenta previa pre-disposes the patient to preterm delivery, which poses the greatest risk to the fetus. As a result of advances in obstetric and neonatal care, the perinatal mortality rate (PMR) for patients with placenta previa has
cervical os. A marginal placenta previa is one in which the edge of the placenta extends to the margin of the internal cervical os.
DiagnosisThe classic presentation of placenta previa is painless vaginal bleeding in a previously normal pregnancy. The mean gestational age at onset of bleeding is 30 weeks, with one-third presenting before 30 weeks. Placenta previa is almost exclusively diagnosed on the basis of ultrasonography. Between 4% and 6% of patients have some degree of placenta previa on ultra-sonic examination before 20 weeks’ gestation. With the development of the lower uterine segment, a relative upward placental migration occurs, with 90% of these resolving by the third trimester. Complete placenta previa is the least likely to resolve, with only 10% of cases resolving by the third trimester. When placenta previa is diagnosed in the second trimester, a repeat sonogram is indicated at 30 to 32 weeks for follow-up evaluation.
Transabdominal ultrasonography has an accuracy of 95% for placenta previa detection. If the placenta is implanted posteriorly and the fetal vertex is low, the
FIGURE 10-1 Types of placenta previa.
Partialplacentaprevia
Totalplacentaprevia
Lowimplantationor low-lyingplacenta
Marginalplacentaprevia
11
Diagnosis
❖ Ultrasound
❖ Transabdominal
❖ Tranvaginal 100% accurate
12APH and multiples - November 3, 2016
Management
❖ Cesarean delivery
❖ Expectant management
❖ Gestational age:
➡ Preterm Term/near term
❖ Fetal lung maturation/Steroids
❖ Recurrent episodes of bleeding 70%
13
Management
❖ 2 large bore IV cannula
❖ Laboratory
✓ Complete blood count: Hb, HCT, platelets
✓ Coagulation profile: PT, PTT, Fibrinogen
✓ Blood group and cross match
❖ Ultrasound
14
Placenta accreta ❖ Abnormal attachment of the placenta through the uterine
myometrium as a result of defective decidual formation
✓ Superficial (accreta)
✓ Deep (increta)
✓ Extend through to the uterine serosa (percreta).
❖ Previous uterine surgery
❖ Cesarean hystrectomy
15
Abruptio Placentae
16APH and multiples - November 3, 2016
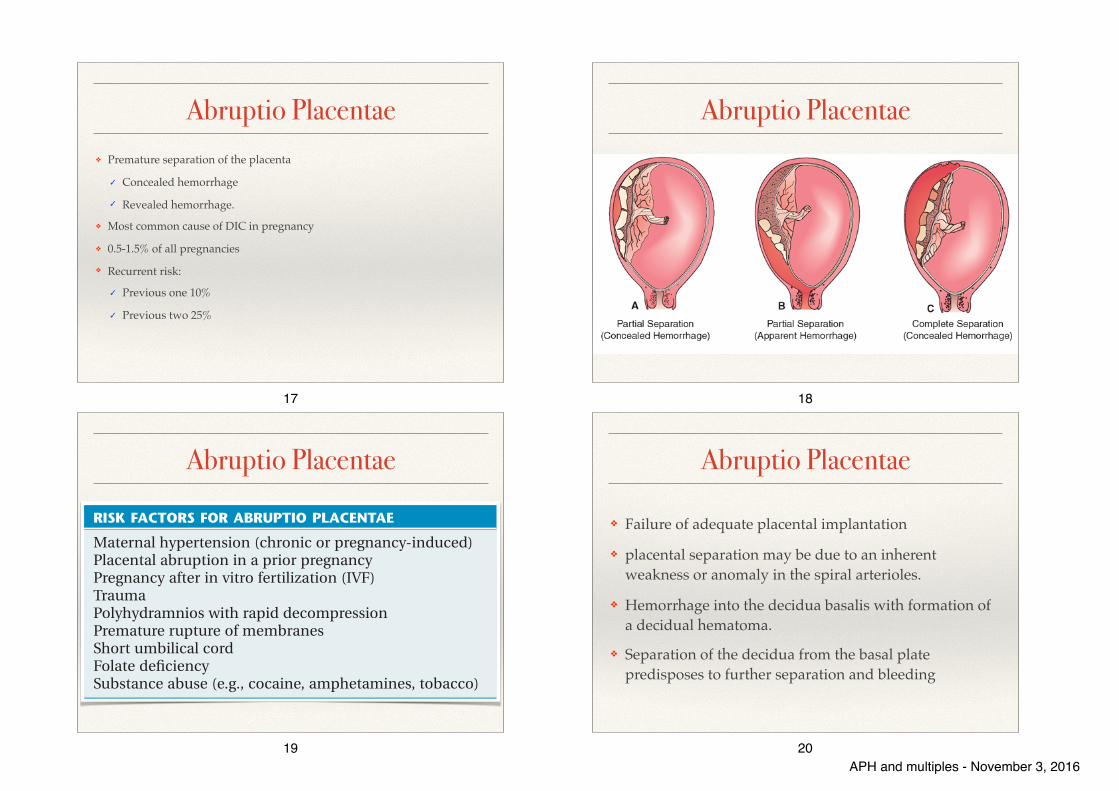
Abruptio Placentae ❖ Premature separation of the placenta
✓ Concealed hemorrhage
✓ Revealed hemorrhage.
❖ Most common cause of DIC in pregnancy
❖ 0.5-1.5% of all pregnancies
❖ Recurrent risk:
✓ Previous one 10%
✓ Previous two 25%
17
Abruptio Placentae
18
Abruptio Placentae
CHAPTER 10 Obstetric Hemorrhage 139
25% after two. The etiology may be the opposite of that for placenta accreta. Because abruption is associated with maternal hypertension or preeclampsia, there may be a failure of adequate placental implantation. Its inciting cause is unknown, but placental separation may be due to an inherent weakness or anomaly in the spiral arterioles. Placental separation is initiated by hemorrhage into the decidua basalis with formation of a decidual hematoma. The resulting separation of the decidua from the basal plate predisposes to further separation and bleeding, as well as to compression and destruction of placental tissue. Blood may either dissect upward toward the fundus, resulting in a concealed hemorrhage, or extend downward toward the cervix, resulting in an external or revealed hemorrhage.
DIAGNOSIS AND MANAGEMENTClinically, the diagnosis of a placental abruption is entertained if a patient presents with painful vaginal bleeding in association with uterine tenderness, hyperactivity, and increased tone. The signs and symptoms of placental abruption are variable, however. The most common finding is vaginal bleeding, which is seen in 80% of cases. Abdominal pain and uterine tenderness are present in 66% of cases, fetal distress in 60%, uterine hyperactivity and increased uterine tone in 34%, and fetal death in 15%.
The diagnosis of placental abruption is made clini-cally. Ultrasonography may detect only 2% of abrup-tions. Because placental abruption may coexist with a placenta previa, the reason for doing an initial ultra-sonic examination is to exclude the previa.
Management of the patient with an abruption includes careful maternal hemodynamic and fetal monitoring, serial evaluation of the hematocrit and coagulation profile, and delivery. Intensive monitor-ing of both the mother and the fetus is essential because rapid deterioration of the condition of either one can occur. Blood products for replacement should always be available, and a large-bore (16- to 18-gauge) IV line must be secured. Red blood cells should be given liberally if indicated. In the setting of placental abruption, the use of tocolytics or uterine relaxants is not advisable. Uterine tone must be maintained to control bleeding following delivery, or at least to control the bleeding sufficiently to allow a safe hysterectomy to be performed, if necessary.
MATERNAL-FETAL RISKSAbruption places the fetus at significant risk of hypoxia and, ultimately, death. The PMR due to placental abruption is 35%, and the condition accounts for 15% of third-trimester stillbirths. Fifteen percent of live-born infants have significant neurologic impairment.
Placental abruption is the most common cause of DIC in pregnancy. This results from release into the maternal circulation of thromboplastin from the dis-rupted placenta and subplacental decidua, causing a
declined over the past decade. The incidence of mal-presentation with placenta previa is 30%, presumably due to the mass effect of the placenta and distortion of the lower uterine segment.
PLACENTA ACCRETAPlacenta accreta implies an abnormal attachment of the placenta through the uterine myometrium as a result of defective decidual formation (absent Nita-buch layer). This abnormal myometrial attachment of the placental villi is usually superficial (accreta), but the villi may invade more deeply into the myome-trium (increta) or extend through to the uterine serosa (percreta). Two-thirds of patients with this complica-tion require hysterectomy when an attempt to remove the placenta leads to severe hemorrhage intrapar-tum. Patients with a history of uterine surgery are at greatest risk of developing an accreta. In fact, those with prior cesarean delivery have a 10-50% risk of abnormal implantation. If ultrasonic imaging shows accreta prior to delivery, elective hysterectomy may be performed to prevent hemorrhage. The etiology of placenta accreta is complex, but recent evidence sug-gests the aggressive invasion of the placenta into the spiral arteries is a process unique to primates that has been conserved through evolution. It ensures that invasion of the uterine arteries is complete to maxi-mize fetal access to the maternal circulation for maximal nutrition.
Abruptio PlacentaeAbruptio placentae, or premature separation of the normally implanted placenta, complicates 0.5-1.5% of all pregnancies (1 in 120 births). Abruption severe enough to result in fetal death occurs in 1 in 500 deliveries.
PREDISPOSING FACTORS AND PATHOPHYSIOLOGYFactors associated with an increased incidence of abruption are noted in Box 10-2. The most common of these risk factors is maternal hypertension, either chronic or as a result of preeclampsia. The risk of recurrent abruption is 10% after one abruption and
BOX 10-2
RISK FACTORS FOR ABRUPTIO PLACENTAE
Maternal hypertension (chronic or pregnancy-induced)Placental abruption in a prior pregnancyPregnancy after in vitro fertilization (IVF)TraumaPolyhydramnios with rapid decompressionPremature rupture of membranesShort umbilical cordFolate deficiencySubstance abuse (e.g., cocaine, amphetamines, tobacco)
19
Abruptio Placentae
❖ Failure of adequate placental implantation
❖ placental separation may be due to an inherent weakness or anomaly in the spiral arterioles.
❖ Hemorrhage into the decidua basalis with formation of a decidual hematoma.
❖ Separation of the decidua from the basal plate predisposes to further separation and bleeding
20APH and multiples - November 3, 2016
DiagnosisClinical diagnosis
❖ Painful vaginal bleeding 80%
❖ Uterine tenderness 66%
❖ Uterine hyperactivity
❖ Increased uterine tone 34%
❖ Fetal distress 60%
❖ Fetal death 15%
21
Management
❖ 2 large bore IV cannula
❖ Laboratory
✓ Complete blood count: Hb, HCT, platelets
✓ Coagulation profile: PT, PTT, Fibrinogen
✓ Blood group and cross match
❖ Ultrasound !
22
Management
❖ Delivery
❖ Expectant management
❖ Steroids, if preterm!
❖ Consider blood products transfusion
❖ Tocolysis is contraindicated
23
Complications
❖ PMR 35%
❖ Third-trimester stillbirths 15%
❖ DIC complicates 20%
❖ Hypovolemic shock
❖ Acute renal failure
❖ Sheehan syndrome
24APH and multiples - November 3, 2016
Multiple pregnancy
25
Multiple pregnancy
Account for only 3% of all live births
❖ 17% of all PTB
❖ 23% of early PTB(<32 wks)
❖ 25% of low and very low PTB.
26
EPIDEMIOLOGY/INCIDENCEThe natural incidence of multiple gestations:
❖ MZ twining occurs at a constant rate of about 4 per 1000 (1/250).
❖ DZ twining rates:
✓ Race (low in Asians, high in blacks)
✓ Age (increases with advanced maternal age)
✓ Parity (increases with parity)
✓ Family history (especially on maternal side)
27
Actual incidence of multiple gestations
❖ Heavily influenced by the use of assisted reproductive technologies (ART)
❖ >50% of multiple gestations in developed countries are from ART.
28APH and multiples - November 3, 2016
29 30
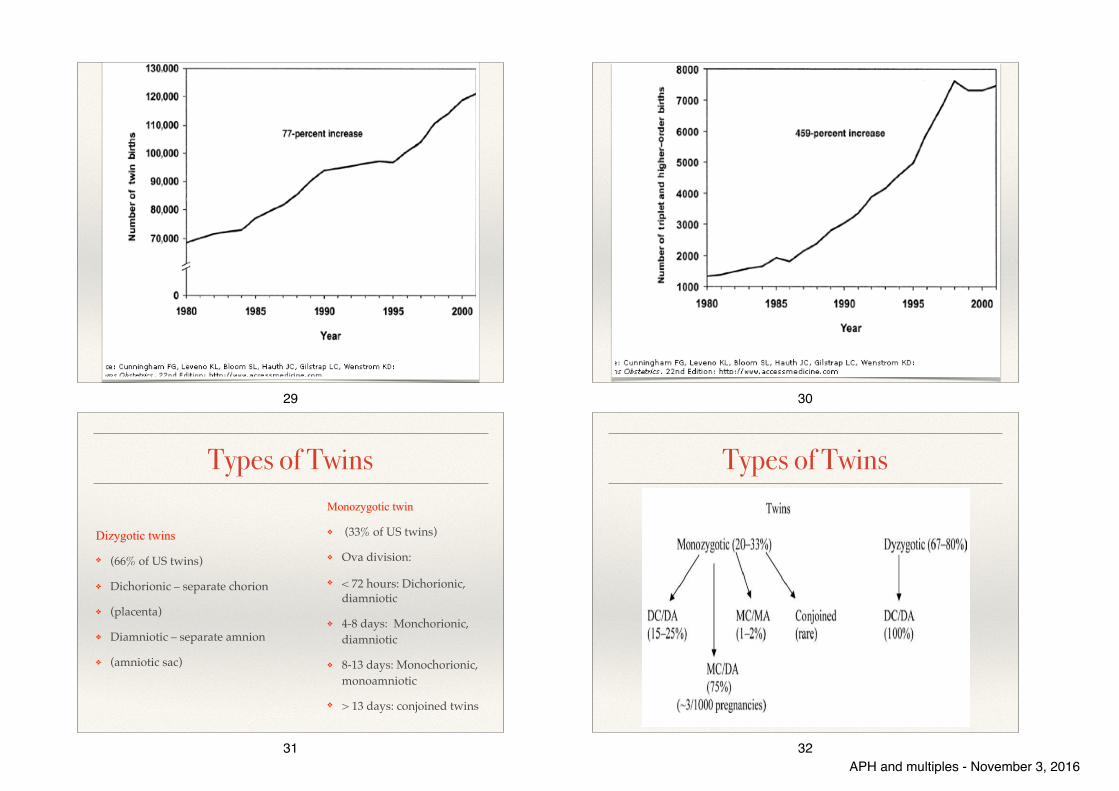
Types of Twins
Dizygotic twins
❖ (66% of US twins)
❖ Dichorionic – separate chorion
❖ (placenta)
❖ Diamniotic – separate amnion
❖ (amniotic sac)
Monozygotic twin
❖ (33% of US twins)
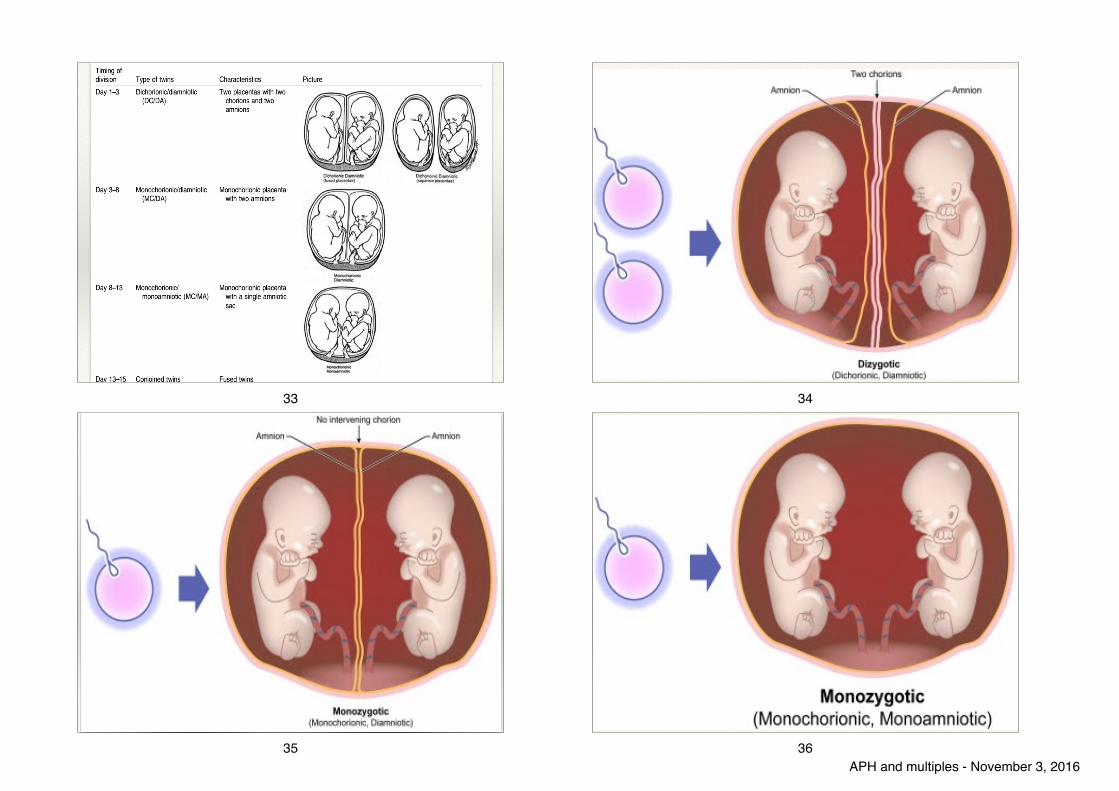
❖ Ova division:
❖ < 72 hours: Dichorionic, diamniotic
❖ 4-8 days: Monchorionic, diamniotic
❖ 8-13 days: Monochorionic, monoamniotic
❖ > 13 days: conjoined twins
31
Types of Twins
32APH and multiples - November 3, 2016
33 34
35 36APH and multiples - November 3, 2016
Zygosity & chorionicity Zygosity:
Refer to type of conception or genetic identity.
2/3 of twin are dizygotic
25% of monozygotic are dichorionic.
Chorionicity:
Refer to type placenta.
37
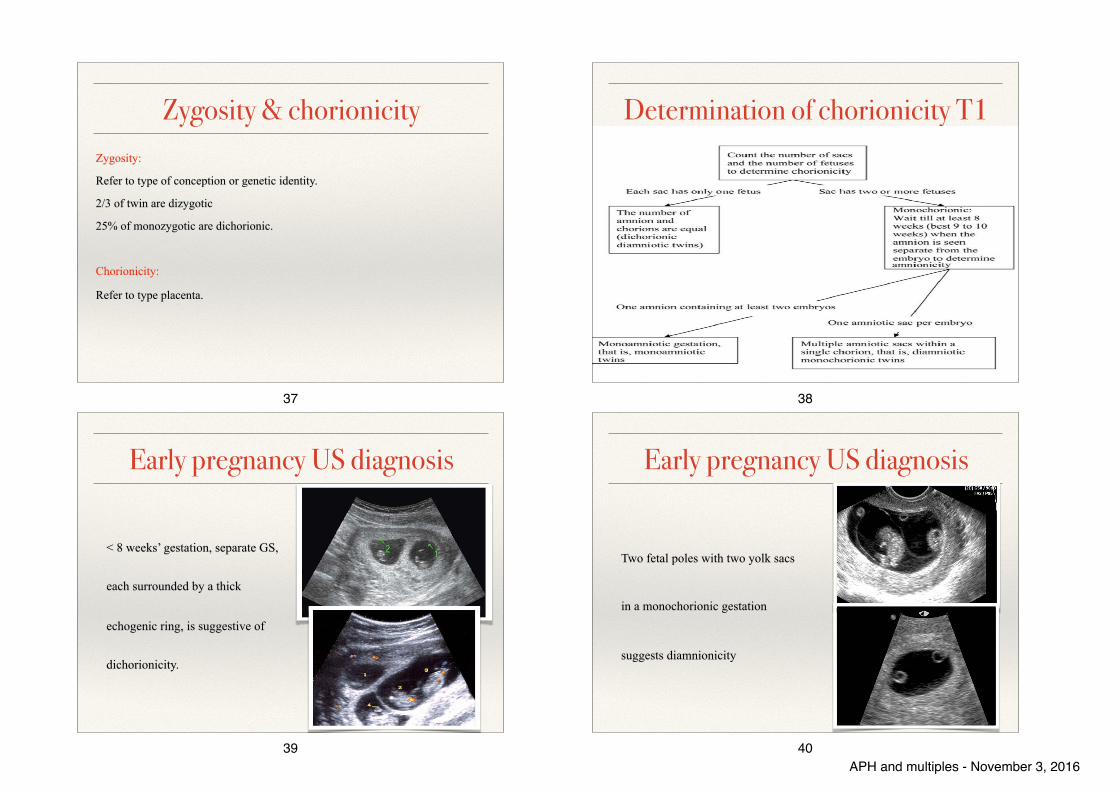
Determination of chorionicity T1
38
Early pregnancy US diagnosis
< 8 weeks’ gestation, separate GS,
each surrounded by a thick
echogenic ring, is suggestive of
dichorionicity.
39
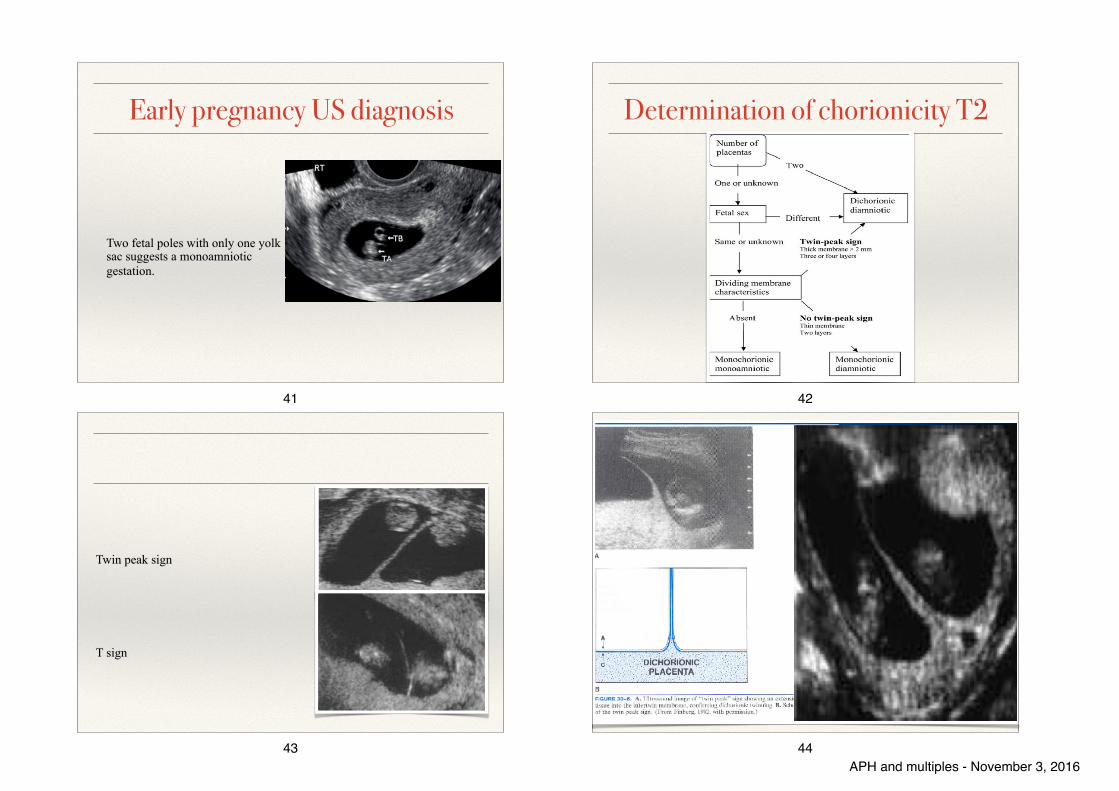
Early pregnancy US diagnosis
Two fetal poles with two yolk sacs
in a monochorionic gestation
suggests diamnionicity
40APH and multiples - November 3, 2016
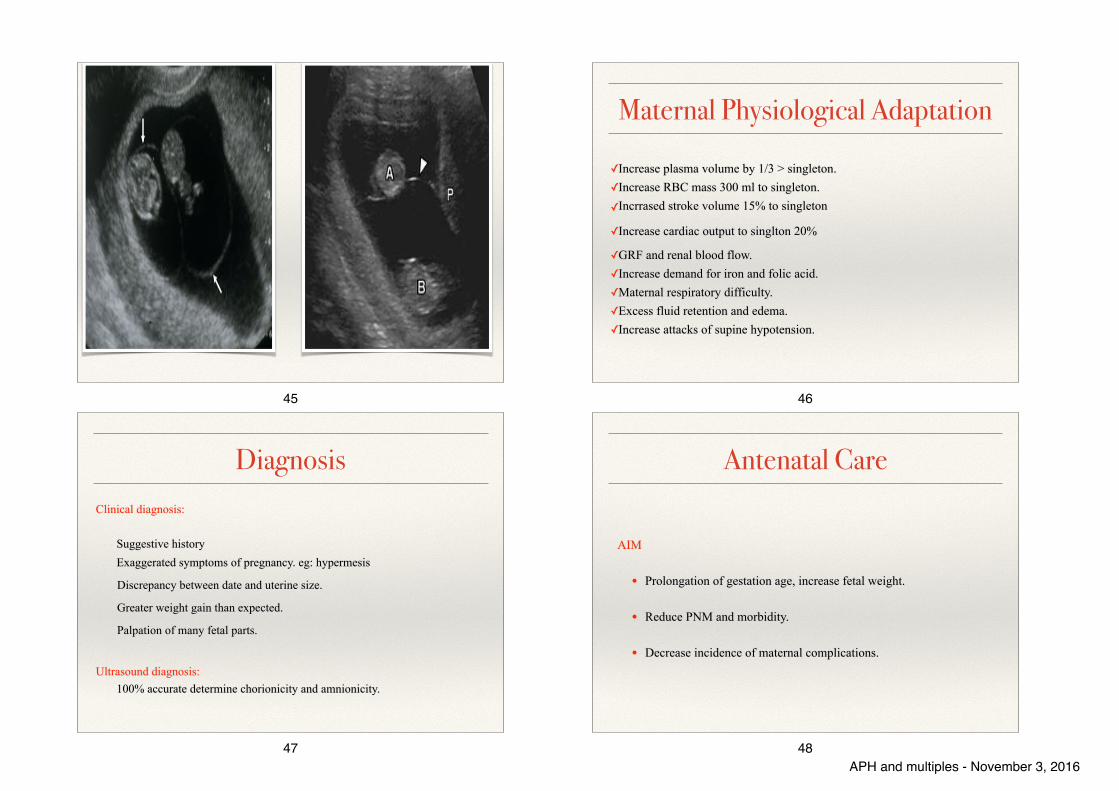
Early pregnancy US diagnosis
Two fetal poles with only one yolk sac suggests a monoamniotic gestation.
41
Determination of chorionicity T2
42
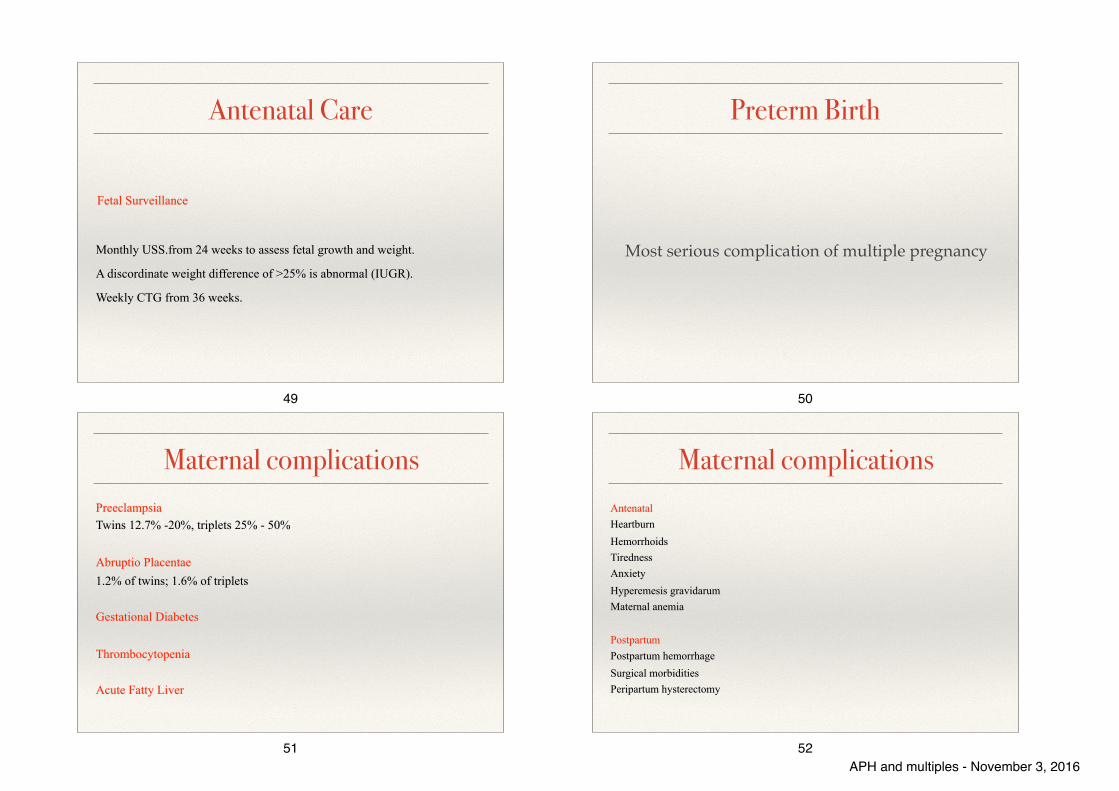
Twin peak sign
T sign
43 44APH and multiples - November 3, 2016
45
Maternal Physiological Adaptation
✓Increase plasma volume by 1/3 > singleton. ✓Increase RBC mass 300 ml to singleton. ✓Incrrased stroke volume 15% to singleton
✓Increase cardiac output to singlton 20%
✓GRF and renal blood flow. ✓Increase demand for iron and folic acid. ✓Maternal respiratory difficulty. ✓Excess fluid retention and edema. ✓Increase attacks of supine hypotension.
46
DiagnosisClinical diagnosis:
Suggestive history Exaggerated symptoms of pregnancy. eg: hypermesis
Discrepancy between date and uterine size.
Greater weight gain than expected.
Palpation of many fetal parts.
Ultrasound diagnosis: 100% accurate determine chorionicity and amnionicity.
47
Antenatal Care
AIM
• Prolongation of gestation age, increase fetal weight.
• Reduce PNM and morbidity.
• Decrease incidence of maternal complications.
48APH and multiples - November 3, 2016
Antenatal Care
Fetal Surveillance
Monthly USS.from 24 weeks to assess fetal growth and weight.
A discordinate weight difference of >25% is abnormal (IUGR).
Weekly CTG from 36 weeks.
49
Preterm Birth
Most serious complication of multiple pregnancy
50
Maternal complicationsPreeclampsia Twins 12.7% -20%, triplets 25% - 50%
Abruptio Placentae 1.2% of twins; 1.6% of triplets
Gestational Diabetes
Thrombocytopenia
Acute Fatty Liver
51
Maternal complicationsAntenatal Heartburn Hemorrhoids Tiredness Anxiety Hyperemesis gravidarum Maternal anemia
Postpartum Postpartum hemorrhage Surgical morbidities Peripartum hysterectomy
52APH and multiples - November 3, 2016
Fetal complications
Spontaneous Reduction Chromosomal abnormalities Congenital Anomalies Fetal Growth Restriction and Discordant Growth Perinatal Mortality
53
PART 2 Obstetrics174
First and Second TrimestersBetween 16 and 22 weeks, the patient is seen every 2 weeks for ultrasonic cervical length assessment, because incompetent cervix is more common with multiple gestations. A suture (cerclage) can be placed in the cervix if marked shortening is noted in the absence of contractions, though the benefit of a cervi-cal cerclage has been under scrutiny recently and is the subject of multiple clinical studies with conflicting findings. Adequacy of maternal diet is assessed due to the increased need for overall calories, iron, vitamins, and folate. The Institute of Medicine (IOM) recom-mends women with twins gain a total of 16.0 to 20.5 kg (35 to 45 lb) during the pregnancy. However, optimal weight gain is somewhat dependent on prepregnancy maternal body mass index (BMI), because obese women (BMI > 30) have better outcomes with less weight gain than women who are of normal weight before pregnancy.
Third TrimesterDuring the third trimester, prevention of prematurity is of utmost importance. The cervix is monitored closely with ultrasonic measurements for early efface-ment and dilation that may precede frank premature labor. A cervical length less than 25 mm at 24 to 28 weeks is associated with a doubling of the risk of pre-mature birth. Interventions to prolong the length of twin pregnancy, such as bed rest, serial uterine activity monitoring, hospitalization, and prophylactic vaginal progesterone, have been carried out but have not been
Retained Dead Fetus SyndromeIt is not unusual for one twin to die in utero remote from term, whereas the remaining twin and the preg-nancy continue to be viable. Over time (after 3 weeks or more in pregnancies that have progressed beyond 20 weeks), the retained dead fetus syndrome can develop, which involves disseminated intravascular coagulopathy in the mother as a result of the transfer of nonviable fetal material with thromboplastin-like activity into the maternal circulation. In such cases, the maternal platelet count and fibrinogen levels should be checked once a week to identify possible coagula-tion abnormalities. The dead fetus will be reabsorbed if the demise occurs before 12 weeks’ gestation. Beyond this time, the fetus will shrink and become dehydrated and flattened (fetus papyraceus).
ALTERED MATERNAL PHYSIOLOGIC ADAPTATION WITH MULTIPLE FETUSESA number of normal maternal physiologic responses to pregnancy are exaggerated with multiple gestations. Whereas in normal pregnancy, maternal blood volume is augmented by 40% (2 L over the nonpregnant base-line), in twins this increase may be 3 L or more. The increased blood volume and demand for iron and folate increase the risk of anemia in the mother and make the patient less able to tolerate the stresses of infection, labor, and premature labor. Preeclampsia and gestational hypertension are almost doubled in multifetal gestation. The increased uterine size associ-ated with multiple fetuses can cause maternal respira-tory embarrassment, orthostatic hypotension due to compression of the vena cava, and compromised renal function due to compression of the ureters.
DIAGNOSISHistorical factors such as a maternal family history of dizygotic twinning, the use of fertility drugs, a maternal sensation of feeling larger than with previous pregnan-cies, or a sensation of excessive fetal movements should raise the suspicion of twins. Physical signs, including excessive weight gain, excessive uterine fundal growth, and auscultation of fetal hearts in separate quadrants of the uterus are suggestive but not diagnostic. An obstetric ultrasound should be performed when a mul-tiple gestation is suspected. The diagnosis of multiple gestations requires a sonographic examination dem-onstrating two separate fetuses and heart activities, and can be made as early as 6 weeks’ gestation.
ANTEPARTUM MANAGEMENTBecause of the high risk of preterm birth, intensive antepartum management schemes should be directed at prolonging gestation and increasing birth weight, in order to decrease perinatal morbidity and mortality. The complications of multiple gestations are shown in Box 13-1.
BOX 13-1
COMPLICATIONS OF MULTIPLE GESTATIONS
MaternalAnemiaHydramniosHypertensionPremature laborPostpartum uterine atonyPostpartum hemorrhagePreeclampsiaCesarean delivery
FetalMalpresentationPlacenta previaAbruptio placentaePremature rupture of the membranesPrematurityUmbilical cord prolapseIntrauterine growth restrictionCongenital anomaliesIncreased perinatal morbidityIncreased perinatal mortality
54
Delivery Fetal and neonatal morbidity and mortality begin to increase in twins at 37 completed weeks and triplets at 35 completed weeks.
✓ Uncomplicated Di/Di: 38 weeks of gestation
✓ Uncomplicated Mono/Di between 34 weeks and 37 6/7 weeks
✓ Uncomplicated monoamniotic twin at 32–34 weeks of gestation.
55
Route of delivery
Depends on type of twins, fetal presentations, gestational age, and experience of the clinician
Vertex/Vertex: 40% to 45% Vertex/Non vertex: 35% to 40%, Consider: (1) the size of the second twin, (2) the presence of growth discordance (estimated weight of second twin at least 25% greater than first twin) (3) the availability of obstetric staff skilled in assisted breech delivery, internal podalic version, and total breech extraction. Nonvertex first twin: 15% to 20%
56APH and multiples - November 3, 2016
Questions ?
57
APH and multiples - November 3, 2016