2017 Saving Mothers Annual report - draft 12...AIDS Acquired Immune Deficiency Syndrome AF Avoidable...
96
i Contents Section Page Contents i Abbreviations ii Acknowledgements ii Foreword iii Summary and recommendations iv 1 Overview 2017 1.1. Introduction 1 1.2. Maternal deaths 2017: Comparison between DHIS and NCCEMD data 1 1.3. Maternal deaths, mortality ratios and trends 3 1.4. Underlying causes for 2017 and timing of emergency event and death 5 1.5. Comparison of underlying causes from 2011-2017 7 1.6. Comparison of underlying causes between provinces 9 1.7. Safe Caesarean delivery 14 1.8. Levels of care and mortality 15 1.9. Potentially preventable deaths 21 1.10. Avoidable factors, underlying causes and levels of care 25 1.11 Mortality ratios and level of care per province 30 1.12. Summary of findings 33 1.13. Conclusions and recommendations 34 1.14 Suggested recommendations per province 35 Appendices 1. Comparison of maternal deaths in DHIS and MaMMAS per district 39 2. Detail of underlying causes 2017 40 3. iMMR per district and province 2017 42 4. iMMR of provinces and districts ranked from highest to lowest 44 5. Number of health care professional avoidable factors per level of care 46 2 Progress report on reducing deaths associated with caesarean section 47 Appendices 1. Caesarean delivery and BLDACD CFR per province and district 58 2. Ranking of Caesarean delivery CFR per province 60 3. Ranking of CD CFR per district 61 4. Ranking of BLDACD CFR per province 62 5. Ranking of BLDACD CFR per district 63 6. Proportion of maternal deaths with CD due to BLDACD, per province and district 64 3 Managing Hypertensive Diseases in Pregnancy (HDP) 65 4 Monitoring and Evaluation of Basic Antenatal Care Plus implementation in South Africa 82 5 Saving Mothers Report 2017: Report on key decisions taken by the National Health Council; 6-7 December 2018 90
Transcript of 2017 Saving Mothers Annual report - draft 12...AIDS Acquired Immune Deficiency Syndrome AF Avoidable...

i
Contents
Section Page Contents i Abbreviations ii Acknowledgements ii Foreword iii Summary and recommendations iv 1 Overview 2017 1.1. Introduction 1 1.2. Maternal deaths 2017: Comparison between DHIS and NCCEMD data 1 1.3. Maternal deaths, mortality ratios and trends 3 1.4. Underlying causes for 2017 and timing of emergency event and death 5 1.5. Comparison of underlying causes from 2011-2017 7 1.6. Comparison of underlying causes between provinces 9 1.7. Safe Caesarean delivery 14 1.8. Levels of care and mortality 15 1.9. Potentially preventable deaths 21 1.10. Avoidable factors, underlying causes and levels of care 25 1.11 Mortality ratios and level of care per province 30 1.12. Summary of findings 33 1.13. Conclusions and recommendations 34 1.14 Suggested recommendations per province 35 Appendices 1. Comparison of maternal deaths in DHIS and MaMMAS per district 39 2. Detail of underlying causes 2017 40 3. iMMR per district and province 2017 42 4. iMMR of provinces and districts ranked from highest to lowest 44 5. Number of health care professional avoidable factors per level of care 46 2 Progress report on reducing deaths associated with caesarean section 47 Appendices 1. Caesarean delivery and BLDACD CFR per province and district 58 2. Ranking of Caesarean delivery CFR per province 60 3. Ranking of CD CFR per district 61 4. Ranking of BLDACD CFR per province 62 5. Ranking of BLDACD CFR per district 63 6. Proportion of maternal deaths with CD due to BLDACD, per province and district 64 3 Managing Hypertensive Diseases in Pregnancy (HDP) 65 4 Monitoring and Evaluation of Basic Antenatal Care Plus implementation in
South Africa 82
5 Saving Mothers Report 2017: Report on key decisions taken by the National
Health Council; 6-7 December 2018 90

ii
List of abbreviations Abbreviation Meaning AA Anaesthetic related death AC Acute collapse AIDS Acquired Immune Deficiency Syndrome AF Avoidable Factors APH Antepartum haemorrhage ARV Antiretroviral drugs BLDACD Bleeding associated with caesarean section CEMD Confidential enquiries into maternal deaths CFR Case Fatality Rate CHC Community Health Centre C Primary health care clinic CD Caesarean Delivery Decl. Declined DIC Disseminated Intravascular Coagulation DH District Hospital EC Eastern Cape Ec Ectopic pregnancy Em EMS
Embolism Emergency Medical Services
EOST Emergency Obstetric Simulation Training ESMOE Essential Steps in Managing Obstetric emergencies FS Free State Gau Gauteng HAART Highly active antiretroviral therapy HCP Health Care Professional HG Hyperemesis Gravidarum HDP Hypertensive Disorders of Pregnancy iMMR Institutional Maternal Mortality Ratio KZN KwaZulu-Natal Lim Limpopo MD Pre-existing maternal disorders Misc. Miscarriage Mpu Mpumalanga MMR Maternal Mortality Ratio NC Northern Cape NCCEMD National Committee for the Confidential Enquiries into Maternal Deaths Neg. Negative NPRI Non-pregnancy related infections NNDR Neonatal death rate NW North West Province OH Obstetric Haemorrhage PCP Pneumocystis carinii pneumonia Pos. Positive PPH Postpartum haemorrhage PRS Pregnancy related sepsis PNMR Perinatal Mortality Rate RH Regional Hospital TH Tertiary Hospital TB Tuberculosis Unk. Unknown WC Western Cape
Acknowledgements The NCCEMD would like to thank all the provincial assessors and the MCWH coordinators of all provinces and the National Department of Health’s MCWH Youth and Nutrition cluster for their hard work and cooperation in collecting and entering the data on maternal death

iii
Foreword In South Africa, the institutional maternal mortality ratio (iMMR) is approximately 134 deaths per 100 000 live births. This figure has declined considerably from a peak number of deaths recorded in 2009 when the iMMR was 188 per 100 000 live births. The National Committee on Confidential Enquiries into Maternal Deaths (NCCEMD), the Ministerial committee which began reporting on deaths since 1998 estimated that approximately 60% of these deaths were potentially preventable. South Africa is one of a few countries in which maternal deaths are reviewed at an institutional health facility in a structured formation and the information (maternal death notification form) which includes demographic data, clinical data, avoidable factors and lessons learnt are sent to independent provincial assessors for further none biased assessment. The information is finally collated and detailed Saving Mothers report are published every 3 years. In between annual reports are provided with basic demographic information and a highlight a specific issue which has been identified. In addition these reports, identify lessons learnt and target ways to prevent other deaths. In this 2017 Annual Report highlights some positives and negatives. Deaths from non- pregnancy related infections fell considerably from a peak in 2009 by over 40% and was mainly due to the introduction of ARVs irrespective of the CD cell count; the rate of decrease in deaths from this cause seems to be levelling off. A considerable amount of effort has been put into decreasing deaths from Obstetric Hemorrhage and there has been a decline in 2017 albeit about a 2% decline. However a cause for concern has been a slight increase in preventable deaths from hypertensive disorders of pregnancy. It is hoped that there will concerted effort in decreasing these deaths by instituting guidelines for all levels of health care. The 2017 Annual report provides in detail interventions to be strengthened in 2019. These include the 5 Cs viz.
C - Improve access to all forms of contraception particularly to those < 18years and those >35 years C - Strengthen access to and improve quality of antenatal care in particular history taking off previous history of preeclampsia, family history of hypertension and taking action on diagnostic findings such as slight elevations in blood pressure levels C - improve communication with communities regarding early booking for antenatal care and involve general practitioners, pharmacists to refer women who are found to be pregnant on urine pregnancy testing . C - Improve safe CD package including safe anesthesia package in all provinces C - “Quality of care“ improve attitudes of all health care professionals; train nurses and doctors on use of clinical protocols; strengthen use of DCSTs by exploring the best site in which they are placed (district office /regional hospital).
Finally I would like to thank the Minister and all the provincial MECs for supporting the NCCEMD and producing a joint report to save mothers and babies lives in South Africa
J MOODLEY Chair National Committee on the Confidential Enquiries into Maternal Deaths (Section 5 has the National Health Councils decisions on the Saving Mothers 2017 Annual Report)

iv
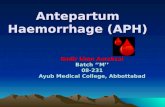
Summary and recommendations The HIV epidemic can be likened to a spring tide, the water or in this case HIV infections dominated everything; but as the tide changed (and as we have got on top of the HIV epidemic) the shore under water was revealed with rocks that were not visible before. Similarly with the receding deaths associated with HIV reducing we are left with new “rocks” and challenges. This is well illustrated in figure 1 below which looks at the proportions of potentially preventable deaths and their underlying causes.
NPRI – Non-pregnancy related infections; OH – Obstetric Haemorrhage; HDP – Hypertensive disorders of
pregnancy; M&S – Pre-existing medical and surgical conditions
In 2008-2010 non-pregnancy related infections dominated the percentage potentially preventable maternal deaths, but it’s proportion has been greatly reduced making obstetric haemorrhage (OH) the most common potentially preventable death but this is now being challenged by hypertensive disorders in pregnancy (HT) as the challenges in dealing with OH are being solved. The priorities in ending preventable maternal deaths have changed as the low hanging fruit has been plucked and now HDP is of greatest concern. Further reductions in maternal deaths will require system wide interventions which are difficult to achieve. The main finding of the 2017 Saving Mothers Annual report are:
• The decline in iMMR is plateauing • ARV programmes have been effective but need vigilance; sharp decline NPRI no longer
happening; there is a need to explore reasons for this. • It is encouraging that there is an overall decrease in obstetric haemorrhage deaths but has
not occurred in all provinces and still needs attention • Focus on reducing hypertension deaths needs to be highlighted with an action plan • Higher proportion avoidable deaths in district hospitals(DH) point to need for mentorship at
this level and the improvement of emergency transport from this level to RH or PTH where the deaths tend to occur after referral. Non Pneumatic anti shock garments (NASG) and involvement of EMS is important for this.
• There has been a 41.5% reduction in the iMMR of Provincial Tertiary Hospitals. The reason for this is not immediately clear, but there was a 2% increase in births and a 2% reduction in
0,0
5,0
10,0
15,0
20,0
25,0
30,0
35,0
2008-2010 2011-2013 2014-2016 2017
Perc
ent
Figure 1. Distribution of potential preventable deaths 2008-2017
NPRIOHHTM&S

v
maternal deaths. Perhaps the enquiry into the functioning of the PTHs had an effect on their better functioning.
• Lack of appropriately trained doctors and nurses continues to be the most frequently cited avoidable factor
• Problems with inter-facility transport of ill patients has been reduced, but there is still a large problem with women getting from home to a health facility. Innovative ways of ensuring transport at all times from townships and rural areas need to be investigated. Community involvement is very important in this aspect, as are maternity waiting areas.
• Concentration of high CFRs for CD and BLDACD in certain provinces illustrates serious inequities in maternal health care provision. It appears that these are also the provinces with the greatest reported incidents of “lack of appropriately trained staff” this needs to be explored further. It is known that some of the provinces with poorest outcomes have unacceptable deficiencies in numbers of specialists.
• Ways of reducing inequities and focussing on skills distribution and functional facilities in the poorest provinces needs to be focussed on. KwaZulu-Natal is similar to all the rural provinces, yet has a very low proportion of avoidable factors related to lack of appropriately trained staff. An investigation as to what KwaZulu-Natal is doing to ensure appropriate staffing compared to the other provinces should be performed as soon as possible to help the other provinces follow best practices.
Using managing cases of HDP as the prototype to identify and change bottlenecks in managing sick pregnant women is a good way to go to develop the system-wide interventions. HDP have evolved to be the biggest problem in ending potentially preventable maternal deaths and so must have a high priority. New detailed guidelines have been developed that affect every level of the health care system and getting these right will get the systems right for other conditions. The inequity of the distribution of health care professionals is also clearly illustrated in this report, with the poorer and more rural provinces having the biggest problems with lack of appropriately trained doctors and nurses. This must also be seen in the context that these provinces also have the least number of specialists which compounds the problems. This issue needs to be tackled if further reduction in mortality is to be achieved. The target of less than 1000 maternal deaths in 2020 will only be achieved if these issues are addressed. Recommendations The 3 Hs and 5Cs are still extremely relevant. To support this the following must be enthusiastically supported :- 1. Introduce the new guidelines in managing HDP and use these guidelines to identify barriers to
implementation and then to solve them. Improve in parallel the functioning of BANC Plus 2. Continue with the Safe CD programme and ensure all hospitals doing CD are accredited and have
accredited surgeons and anaesthetists. 3. Continue ensuring that the 90, 90, 90 programme for HIV infected pregnant women is strongly
supported. 4. Consider innovative ways to solve the lack of skills in the rural provinces. A special meeting
where KwaZulu-Natal (having a large number of rural hospitals and low lack of appropriate trained health care professionals) and the Western Cape (where there was no case of lack of trained staff recorded) can explain their methods and structures to achieve this to the other provinces should be urgently convened.
5. Engage the community in developing ways so that women with emergencies can get from home to a health facility at any time of day or night

1
Section 1. Overview 2017 1. Introduction
The aim of report is to identify new trends in maternal deaths and see if the recommendations of
the sixth Saving Mothers report 2014-2016 need to change. Data closed 31st August 2018 for the
analysis of this annual report.
2. Maternal Deaths 2017: Comparison between DHIS and NCCEMD data
Data was obtained from the District Health Information System (DHIS) for live births and maternal
deaths per district for 2017 on 23rd July 2018. The NCCEMD data was obtained from the Maternal
Morbidity and Mortality Audit System (MaMMAS) database in 7th September 2018, once all
provinces had submitted their data.
The DHIS data is almost exclusively from public hospitals (although some private hospitals do submit
data to the DHIS). The DHIS does not collect data of deaths outside of health facilities and
coincidental deaths.
Table 1 compares the number of maternal deaths recorded per province from the DHIS and
MaMMAS; private hospital births, deaths outside of health facilities and coincidental deaths are
subtracted from the MaMMAS data as shown to make the data comparable.
Table 1. Comparison of numbers of maternal deaths recorded in DHIS and MaMMAS
Provinces Live births
(DHIS) DHIS deaths MaMMAS
total deaths Pvt Outside Coincidental Comparable MaMMAS Diff.
%
diff.
Eastern Cape 99927 135 142 2 6 4 130 -5 -3,8
Free State 44559 65 69 0 5 2 62 -3 -4,8
Gauteng 213955 257 223 8 5 9 201 -56 -27,9
KwaZulu-Natal 180565 193 245 9 4 6 226 33 14,6
Limpopo 119163 150 181 7 5 7 162 12 7,4
Mpumalanga 75621 97 118 5 4 1 108 11 10,2
North West 55915 69 84 3 2 2 77 8 10,4
Northern Cape 20475 18 28 0 2 0 26 8 30,8
Western Cape 95218 53 80 2 3 7 68 15 22,1
South Africa 905398 1037 1170 36 36 38 1060 23 2,2
Table 2 illustrates the differences in the institutional maternal mortality ratio (iMMR)
Table 2. Comparison of the iMMR between DHIS and the comparable MaMMAS
iMMR DHIS Comparable MaMMAS Diff
Eastern Cape 135,10 130,09 -5,00
Free State 145,87 139,14 -6,73
Gauteng 120,12 93,94 -26,17
KwaZulu-Natal 106,89 125,16 18,28
Limpopo 125,88 135,95 10,07
Mpumalanga 128,27 142,82 14,55
North West 123,40 137,71 14,31
Northern Cape 87,91 126,98 39,07

2
Western Cape 55,66 71,42 15,75
South Africa 114,54 117,08 2,54
There are three aspects in this comparison:
1. There is agreement between DHIS and MaMMAS in 2 provinces (Eastern Cape and Free
State).
2. There are considerably less maternal deaths in MaMMAS than DHIS in Gauteng with 27,9%
more deaths in the DHIS data than MaMMAS.
3. In the remaining 6 provinces there are more deaths recorded in MaMMAS than DHIS varying
between 7 and 31%.
There is under reporting of maternal deaths in DHIS (as has mostly been the case previously). This is
due to maternal deaths being reported from other wards and sites in the hospital other than just the
maternity ward. However, in Gauteng there has been a potentially large proportion 27,9% of under-
reporting of cases to MaMMAS.
To guard against over optimism in the 2017 Annual Saving Mothers report, the MaMMAS data will
be used, except for Gauteng where the DHIS data will be used and the Gauteng data adjusted
proportionately from the MaMMAS Gauteng distribution. A ”check” should occur between the
large discrepancy between the DHIS and MaMMAS data in Gauteng. Most of the discrepancy comes
from the City of Johannesburg Metropolitan Municipality.
Appendix 1 gives the DHIS maternal deaths and the unadjusted MaMMAS maternal deaths per
district.

3
3. Maternal deaths, mortality ratios and trends
Table 3. Number of deaths during pregnancy, childbirth and the puerperium per province reported to the NCCEMD; 1998-2017
1998 1999 2000 2001 2002 2003 2004 2005 2006 2007 2008 2009 2010 2011 2012 2013 2014 2015 2016 c2017
EC 56 95 120 103 113 112 145 149 154 160 215 263 232 210 183 200 205 148 147 142
FS 94 79 96 119 100 171 161 150 170 164 139 171 120 124 72 85 92 71 70 69
cGau 131 138 171 184 213 205 251 222 257 190 268 319 293 270 339 240 283 285 253 257
KZN 188 252 238 245 238 275 209 268 354 339 366 378 385 360 326 278 281 239 220 245
Lim 27 63 88 71 72 108 101 181 199 211 222 196 198 249 245 256 216 207 200 181
Mpu 66 72 128 97 98 120 75 74 108 87 128 115 150 148 136 115 93 101 106 118
NW 58 54 115 106 80 135 111 105 100 84 97 161 134 99 96 97 116 96 84 84
NC 22 18 29 23 38 28 40 53 53 58 59 53 52 40 36 34 27 35 23 28
WC 34 34 50 42 60 67 80 61 53 73 60 110 82 60 75 79 65 68 83 80
SA 676 805 1035 990 1012 1221 1173 1263 1448 1366 1554 1766 1646 1560 1508 1384 1378 1250 1186 1222
EC – Eastern Cape; FS – Free State; cGau – Gauteng – data adjusted; KZN – KwaZuu-Natal; Lim – Limpopo; Mpu – Mpumalanga; NW – North West; NC – Northern Cape; WC
– Western Cape; SA – South Africa; c2017 – adjusted Gauteng data
Note: 2017c is Gauteng data adjusted and 2017 includes Gauteng data as given
0
200
400
600
800
1000
1200
1400
1600
1800
2000
19981999
20002001
20022003
20042005
20062007
20082009
20102011
20122013
20142015
2016
2017c2017
Nu
mb
er
Figure 2. Illustration of deaths during pregnancy, childbirth and the
puerperium reported to the NCCEMD between 1998-2017

4
Table 4. iMMR per province from 2005-2017
Province 2005 2006 2007 2008 2009 2010 2011 2012 2013 2014 2015 2016 c2017
EC 140,1 131,6 138,7 180,4 215,2 197 164,7 153,7 172,7 174,15 133,35 144,11 142,10
FS 353,8 334,1 313,1 267 350,9 263,5 246,8 149,3 185,1 203,26 162,81 172,65 154,85
Gau 136 147,6 111,9 136 160,2 159,2 136,4 163,7 115,0 136,26 138,97 125,09 128,53
KZN 152,6 187,9 181,6 183,8 194,2 208,7 197,6 170,2 146,5 140,85 125,66 124,56 135,69
Lim 150,5 167,6 182,9 176,6 160,4 166,7 196,4 192,9 201,2 169,75 168,11 170,72 151,89
Mpu 114,5 151,1 126,7 179,8 159,4 218,6 199,7 177,4 150,3 119,54 136,50 148,51 156,04
NW 174,2 144,2 121,2 161,7 279,5 256,1 173,0 164,8 168,5 200,86 167,95 151,99 150,23
NC 291,4 307,9 301,8 274,4 251,8 267,4 193,6 166,5 158,3 120,68 160,52 114,48 136,75
WC 67,7 60,1 112 61,8 113,1 88 62,6 81,8 83,9 66,50 70,59 75,78 84,02
SA 150,2 161,7 158,5 164,8 188,9 186,2 166,97 160,22 147,69 144,58 135,53 135,27 134,97
EC – Eastern Cape; FS – Free State; Gau – Gauteng; KZN – KwaZuu-Natal; Lim – Limpopo; Mpu – Mpumalanga; NW – North West; NC – Northern Cape; WC – Western Cape;
SA – South Africa: c2017 – data adjusted for Gauteng – see section 2.
120
130
140
150
160
170
180
190
200
2005 2006 2007 2008 2009 2010 2011 2012 2013 2014 2015 2016 c2017
iMM
R/10
0000
live
birt
hs
Figure 3. iMMR per year for South Africa 2005-2017

5
There are limitations of comparing data on an annual basis. Nevertheless, there appears to be a plateauing or slight increase of iMMR in all provinces compared to the sharp decline observed from 2010 (figures 2 and 3); apart from in Free state and Limpopo which have continued to decline
4. Underlying causes for 2017 and timing of emergency event and death
Table 5. Timing of emergency event and deaths per underlying causes
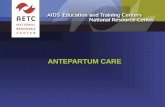
TIMING OF EMERGENCY All M&S NPRI Ec Miscr PRS OH HT AR Emb AC - Early pregnancy 18,0 20,9 19,1 92,3 50,7 1,5 2,3 6,0 6,9 8,8 6,7 - Antenatal period: 20w + 36,3 36,6 45,2 2,6 9,9 12,1 10,8 64,0 6,9 17,6 40,0 - Intrapartum period 11,4 3,9 3,2 0,0 4,2 6,1 32,4 10,0 51,7 23,5 26,7 - Postpartum period 37,3 39,9 32,9 0,0 35,2 80,3 55,1 20,0 13,8 50,0 26,7 - Anaesthesia 1,7 0,7 0,0 5,1 1,4 1,5 1,7 1,5 24,1 0,0 0,0 TIMING OF DEATH - Early pregnancy 13,5 17,0 12,4 79,5 36,6 0,0 1,1 3,5 3,4 8,8 6,7 - Antenatal period: 20w + 17,8 23,5 22,6 2,6 5,6 1,5 1,1 24,0 3,4 14,7 33,3 - Intrapartum period 4,8 3,3 0,4 0,0 2,8 3,0 8,0 4,5 31,0 14,7 13,3 - Postpartum period 64,4 54,9 64,3 10,3 54,9 95,5 85,8 65,5 20,7 58,8 46,7 - Anaesthesia 2,8 1,3 0,4 7,7 0,0 0,0 4,0 2,5 41,4 2,9 0,0
HT; 210; 18%
OH; 184; 16%
Ec; 41; 3%
Miscar.; 75; 6%
PRS; 70; 6%AR; 30; 3%Emb; 35; 3%AC; 15; 1%
ADR; 11; 1%
Miscel; 5; 0%
NPRI; 297; 25%
M&S; 161; 14%
Unk; 53; 4%
Figure 4. Distribution of maternal deaths 2017 (adjusted for Gauteng)

6
The denominator is the total of each underlying cause; e.g. 64% of emergency events in hypertension occurred
in the antenatal period, with 23,5% occurring in the postpartum period.
The denominator is the total of each underlying cause; e.g. 24% of deaths due to hypertension occurred in the
antenatal period, whereas 65,5% occurred in the postpartum period. Of note, apart from ectopic, pregnancy related sepsis and embolism, the majority of conditions present as an emergency during the antepartum or intrapartum period, notably hypertensive diseases in pregnancy (HT), non-pregnancy related infections (NPRI), Medical /Surgical disorders (M&S) and Obstetric Haemorrhage (OH which includes ante-, intra- and postpartum haemorrhages), but die in the postnatal period during which period the majority of maternal deaths occur.
0,010,020,030,040,050,060,070,080,090,0
100,0
- Earlypregnancy
- Antenatalperiod: 20w +
- Intrapartumperiod
- Postpartumperiod
- Anaesthesia
Perc
ent
Figure 5. Timing of emergency
All M&S NPRI Ec Miscr PRS OH HT AR Emb AC
0,010,020,030,040,050,060,070,080,090,0
100,0
- Earlypregnancy
- Antenatalperiod: 20w +
- Intrapartumperiod
- Postpartumperiod
- Anaesthesia
Perc
ent
Figure 6. Timing of death
All M&S NPRI Ec Miscr PRS OH HT AR Emb AC

7
5. Comparison of underlying causes from 2011-2017
Table 6. Comparison of the number of maternal deaths per underlying cause: 2011-2017
Underlying cause 2011 2012 2013 2014 2015 2016 2017 Direct 745 738 672 689 702 648 665 Hypertension 214 221 205 221 222 218 210 Obstetric haemorrhage 233 242 209 226 217 181 184 Ectopic pregnancy 38 22 42 23 36 36 41 Miscarriage 66 65 54 48 61 56 75 Pregnancy-related sepsis 84 68 74 65 65 71 70 Anaesthetic complications 41 41 23 34 28 25 30 Embolism 29 42 31 38 37 36 35 Acute collapse - cause unknown 38 36 32 26 31 20 15 Miscellaneous 2 1 2 8 5 5 5 Indirect 715 658 624 571 442 422 457 Non-pregnancy-related infections 550 509 445 395 310 263 297 Medical and surgical disorders 165 149 179 176 132 159 161 Unknown 64 65 52 57 51 61 53 Total maternal deaths 1524 1461 1348 1342 1212 1143 1186
Table 7. Comparison of the iMMR per underlying cause: 2011-2017
2011 2012 2013* 2014 2015 2016 2017 Hypertension 22,9 23,48 22,69 23,19 24,07 25,78 23,20 Obstetric haemorrhage 24,94 25,71 23,13 23,71 23,53 21,41 20,30 Ectopic pregnancy 4,07 2,34 4,65 2,41 3,9 4,26 4,50 Miscarriage 7,06 6,91 5,98 5,04 6,61 6,62 8,31 Pregnancy-related sepsis 8,99 7,22 8,19 6,82 7,05 8,4 7,71 Anaesthetic complications 4,39 4,36 2,55 3,57 3,04 2,96 3,31 Embolism 3,1 4,46 3,43 3,99 4,01 4,26 3,87 Acute collapse - cause unknown 4,07 3,82 3,54 2,73 3,36 2,37 1,68 Non-pregnancy-related infections 58,87 54,08 49,24 41,44 33,61 31,11 32,78 Medical and surgical disorders 17,66 15,83 19,81 18,47 14,31 18,81 17,73 Unknown 6,85 6,91 5,75 5,98 5,53 7,21 5,83 Total: 163,11 155,23 149,17 140,81 131,41 135,19 130,96
As mentioned in previous reports, the main change over the last 6 years has been the fall in NPRI deaths the first ‘H’, although it plateaued or increased again slightly in all provinces in 2017. This is concerning and ARV programmes need to be monitored. There is no room for complacency. For the other two ‘Hs’, it is welcome that the OH deaths are decreasing slowly but of concern that there is no change for the hypertension deaths. All other causes seem to be static. Medical and surgical disorders remain the fourth most common cause and exceed those from pregnancy related sepsis (puerperal and postabortal). Early pregnancy deaths have increased slightly.

8
0
10
20
30
40
50
60
70
HT OH Ec Misc PRS AR Emb AC NPRI M&S Unk
iMM
R/10
0000
live
birt
hs
Figure 7. Comparison iMMR per underlying cause from 2011-2017
2011
2012
2013*
2014
2015
2016*
2017#

9
6. Comparison of underlying causes between provinces
EC; 142; 12%
FS; 69; 6%
Gau; 275; 22%
KZN; 245; 20%
Lim; 181; 15%
Mpu; 118; 10%
NW; 84; 7%
NC; 28; 2%
WC; 80; 6%
Figure 8. Distribution of maternal deaths per province

10
In all provinces, NPRI is the most common cause of death, followed by deaths from hypertensive disease of pregnancy (HT), except for in Limpopo where obstetric haemorrhage (OH) is second most frequent cause; and KZN and Western Cape where Medical and Surgical disorders exceed Hypertension deaths.
Table 8. Comparison of the maternal deaths per province per underlying cause for 2017
Primary obstetric problems SA EC FS cGau KZN Lim Mpu NW NC WC Direct 665 74 49 149 108 105 76 53 16 35 Hypertension 210 27 17 50 31 29 27 17 6 6 Obstetric haemorrhage 184 20 13 39 25 40 20 13 6 8
Ectopic pregnancy 41 1 3 9 7 7 4 5 1 4
Miscarriage 75 6 6 21 14 5 13 7 3 0
Pregnancy-related sepsis 70 6 6 19 13 9 5 5 0 7
Anaesthetic complications 30 4 3 5 10 5 2 0 0 1
Embolism 35 6 1 5 6 5 4 2 0 6 Acute collapse – cause unknown 15 3 0 1 2 5 1 3 0 0
Adverse drug reactions 11 2 0 4 1 1 0 1 0 2
Miscellaneous 5 1 0 0 0 0 0 1 0 3
Indirect 457 54 13 106 116 63 36 26 10 33 Non-pregnancy-related infections 297 36 5 69 74 45 24 17 7 20
Medical and surgical disorders 161 18 8 38 42 18 12 9 3 13 Unknown 53 8 5 9 14 5 5 2 2 3
Total MD 1186 138 67 268 239 174 117 82 28 73 Coincidental cause 40 4 2 11 6 7 1 2 0 7
DDPCP 1222 142 69 275 245 181 118 84 28 80
cGau – Adjusted Gauteng data

11
Table 9. Comparison of the iMMR per underlying cause and per province 2017
Primary obstetric problems SA EC FS cGau KZN Lim Mpu NW NC WC Direct 73,44 74,05 109,97 69,59 59,81 88,11 100,50 94,79 78,14 36,76 Hypertension 23,20 27,02 38,15 23,39 17,17 24,34 35,70 30,40 29,30 6,30 Obstetric haemorrhage 20,30 20,01 29,17 18,13 13,85 33,57 26,45 23,25 29,30 8,40
Ectopic pregnancy 4,50 1,00 6,73 4,09 3,88 5,87 5,29 8,94 4,88 4,20
Miscarriage 8,31 6,00 13,47 9,94 7,75 4,20 17,19 12,52 14,65 0,00
Pregnancy-related sepsis 7,71 6,00 13,47 8,77 7,20 7,55 6,61 8,94 0,00 7,35
Anaesthetic complications 3,31 4,00 6,73 2,34 5,54 4,20 2,64 0,00 0,00 1,05
Embolism 3,87 6,00 2,24 2,34 3,32 4,20 5,29 3,58 0,00 6,30 Acute collapse - cause unknown 1,68 3,00 0,00 0,58 1,11 4,20 1,32 5,37 0,00 0,00
Adverse drug reactions 1,19 2,00 0,00 1,75 0,55 0,84 0,00 1,79 0,00 2,10
Miscellaneous 0,55 1,00 0,00 0,00 0,00 0,00 0,00 1,79 0,00 3,15
Indirect 50,51 54,04 29,17 49,70 64,24 52,87 47,61 46,50 48,84 34,66 Non-pregnancy-related infections 32,78 36,03 11,22 32,16 40,98 37,76 31,74 30,40 34,19 21,00
Medical and surgical disorders 17,73 18,01 17,95 17,54 23,26 15,11 15,87 16,10 14,65 13,65
Unknown 5,83 8,01 11,22 4,09 7,75 4,20 6,61 3,58 9,77 3,15
Total iMMR 130,96 138,10 150,36 125,14 132,36 146,02 154,72 146,65 136,75 76,67
0
50
100
150
200
250
300
350
400
450
EC FS Gau KZN Lim Mpu NW NC WC
Figure 9. Number of maternal deaths per province 1998 - 20171998
1999
2000
2001
2002
2003
2004
2005
2006
2007
2008
2009
2010
2011
2012
2013
2014
2015
2016
2017c

12
Table 10. Illustration of performance of each province per underlying cause in relation to national average
Underlying cause EC FS cGau KZN Lim Mpu NW NC WC SA <85% >115% Hypertension 27,02 38,15 23,39 17,17 24,34 35,70 30,40 29,30 6,30 23,20 19,72 26,68 Obstetric haemorrhage 20,01 29,17 18,13 13,85 33,57 26,45 23,25 29,30 8,40 20,30 17,25 23,34
Ectopic pregnancy 1,00 6,73 4,09 3,88 5,87 5,29 8,94 4,88 4,20 4,50 3,83 5,18
Miscarriage 6,00 13,47 9,94 7,75 4,20 17,19 12,52 14,65 0,00 8,31 7,07 9,56
Pregnancy-related sepsis 6,00 13,47 8,77 7,20 7,55 6,61 8,94 0,00 7,35 7,71 6,55 8,86
Anaesthetic complications 4,00 6,73 2,34 5,54 4,20 2,64 0,00 0,00 1,05 3,31 2,82 3,81
Embolism 6,00 2,24 2,34 3,32 4,20 5,29 3,58 0,00 6,30 3,87 3,29 4,45 Acute collapse - cause unknown 3,00 0,00 0,58 1,11 4,20 1,32 5,37 0,00 0,00 1,68 1,43 1,94 Non-pregnancy-related infections 36,03 11,22 32,16 40,98 37,76 31,74 30,40 34,19 21,00 32,78 27,87 37,70
Medical and surgical disorders 18,01 17,95 17,54 23,26 15,11 15,87 16,10 14,65 13,65 17,73 15,07 20,39
Total iMMR 138,10 150,36 125,14 132,36 146,02 154,72 146,65 136,75 76,67 130,96 111,32 150,61
< 85% >85% -< 115% > 115%
0
50
100
150
200
250
300
350
400
EC FS Gau KZN Lim Mpu NW NC WC SA
Figure 10. iMMR per year per province 2005-20172005
2006
2007
2008
2009
2010
2011
2012
2013
2014
2015
2016
c2017

13
Table 11. Comparison between iMMR per underlying cause per province: 2011-13; 2014-16; 2017
iMMR Eastern Cape Free State Gauteng KwaZulu-Natal Limpopo 2011-13 2014-16 2017 2011-13 2014-16 2017 2011-13 2014-16 c2017 2011-13 2014-16 2017 2011-13 2014-16 2017 HT 29,26 28,42 27,02 33,25 31,68 38,15 18,90 26,18 23,39 14,02 18,54 17,17 31,23 27,75 24,34
OH 24,29 25,40 20,01 23,55 27,82 29,17 24,12 21,95 18,13 21,65 15,19 13,85 33,59 33,47 33,57
Ec 1,66 1,81 1,00 4,85 3,86 6,73 3,91 3,90 4,09 3,73 3,53 3,88 6,30 4,63 5,87 Misc. 2,48 3,93 6,00 6,23 6,95 13,47 8,47 8,62 9,94 9,41 4,77 7,75 8,40 9,25 4,20
PRS 7,73 7,56 6,00 6,23 10,05 13,47 4,89 8,78 8,77 8,87 6,36 7,20 10,24 10,07 7,55
AR 4,14 3,93 4,00 2,77 2,32 6,73 1,47 1,63 2,34 3,73 3,35 5,54 8,92 6,53 4,20 Emb 3,31 5,14 6,00 8,31 4,64 2,24 3,75 5,04 2,34 1,95 2,12 3,32 2,10 4,90 4,20 AC 3,86 1,51 3,00 4,85 6,18 0,00 6,03 3,74 0,58 3,19 3,00 1,11 2,89 1,90 4,20 NPRI 54,92 42,94 36,03 58,88 47,91 11,22 44,97 28,45 32,16 71,70 39,20 40,98 59,84 36,73 37,76
M&S 20,98 21,77 18,01 27,71 21,64 17,95 16,29 14,63 17,54 20,23 18,36 23,26 17,32 18,77 15,11
Unk 6,90 4,23 8,01 8,31 10,05 11,22 2,44 3,90 4,09 9,76 8,83 7,75 9,97 7,35 4,20
iMMR 159,53 148,47 138,10 186,32 174,63 150,36 135,24 128,78 125,14 168,61 127,14 132,36 191,06 165,16 146,02 Mpumalanga North West Northern Cape Western Cape South Africa 2011-13 2014-16 2017 2011-13 2014-16 2017 2011-13 2014-16 2017 2011-13 2014-16 2017 2011-13 2014-16 2017 HT 30,80 28,23 35,70 30,05 30,56 30,40 21,96 26,45 29,30 12,78 9,11 6,30 22,75 24,02 23,20
OH 33,00 32,26 26,45 35,83 28,79 23,25 20,39 28,01 29,30 4,97 7,36 8,40 24,32 22,67 20,30
Ec 5,72 4,03 5,29 2,89 4,70 8,94 1,57 0,00 4,88 0,36 2,10 4,20 3,63 3,45 4,50
Misc. 6,60 4,93 17,19 5,20 7,64 12,52 1,57 1,56 14,65 1,78 1,40 0,00 6,58 6,00 8,31
PRS 12,76 4,48 6,61 11,56 7,05 8,94 7,84 1,56 0,00 5,68 4,55 7,35 8,04 7,30 7,71
AR 7,92 3,14 2,64 1,73 4,11 0,00 0,00 0,00 0,00 0,36 1,40 1,05 3,73 3,16 3,31 Emb 4,40 2,24 5,29 4,05 2,94 3,58 14,12 6,22 0,00 3,55 4,55 6,30 3,63 4,03 3,87
AC 1,32 2,24 1,32 4,62 2,94 5,37 1,57 4,67 0,00 2,49 1,40 0,00 3,77 2,80 1,68
NPRI 55,43 33,16 31,74 49,70 53,47 30,40 51,76 32,68 34,19 23,79 16,11 21,00 53,47 35,17 32,78
M&S 8,80 9,86 15,87 13,87 17,63 16,10 21,96 10,89 14,65 13,85 15,76 13,65 17,53 16,97 17,73
Unk 6,16 4,03 6,61 6,93 11,16 3,58 9,41 7,78 9,77 1,42 2,80 3,15 6,44 6,14 5,83
iMMR 172,90 132,19 154,72 166,44 172,17 146,65 152,15 121,37 136,75 71,02 68,30 76,67 154,06 134,33 130,96
HT – Hypertensive diseases in pregnancy; OH – Obstetric haemorrhage; Ec – Ectopic pregnancy; Misc – Miscarriage; PRS – Pregnancy related sepsis; AR – Anaesthetic related; Emb. – Embolism; AC – Acute collapse, cause unknown; NPRI – Non-pregnancy related infections; M&S – pre-existing medical and surgical conditions; Unk. – Unknown; iMMR – Institutional Maternal Mortality Ratio; c2017 – Adjusted morality ration for Gauteng

14
There is considerable variation between provinces in the IMMRs and trends in underlying causes. Of note Western Cape has the lowest iMMR for HDP and OH , KZN has shown the greatest reduction in OH deaths, and in all provinces NPRI is the most common cause, except the Free State where only 5 cases were recorded. The Eastern Cape has shown a consistent reduction in all causes of death.
7. Safe Caesarean Delivery See next section for detailed analysis of progress on the Safe CD project and interpretation of the 2017 Safe CD data.
Table 12. Caesarean delivery rate and case fatality rate of caesarean delivery and bleeding during or after caesarean delivery
Province Live births CD CD rate (%) MD with CD BLDACD CFR
CD/100000 CFR
BLDACD/100000 Eastern Cape 99927 29064 29,1 42 7 144,5 24,1
Free State 44559 13164 29,5 31 6 235,5 45,6 Gauteng 213955 62847 29,4 80 12 127,3 19,1
KwaZulu-Natal 180565 55734 30,9 79 10 141,7 17,9
Limpopo 119163 24487 20,5 51 17 208,3 69,4
Mpumalanga 75621 16786 22,2 32 7 190,6 41,7
North West 55915 13267 23,7 17 6 128,1 45,2
Northern Cape 20475 4471 21,8 5 1 111,8 22,4 Western Cape 95218 28561 30,0 25 3 87,5 10,5
South Africa 905398 248381 27,4 362 69 145,7 27,8
CD – Caesarean delivery; MD – Maternal Deaths; BLDACD – Bleeding during or after caesarean delivery; CFR – Case fatality rate expressed per 100000 CDs
Table 13. Comparison CD rate and CFR for CD and BLDACD
CD rate CFR CD/100000 CFR BLDACD/100000 Province 2014-2016 2017 2014-2016 2017 2014-2016 2017 Eastern Cape 27,6 29,1 168,7 144,5 25,2 24,1 Free State 25,3 29,5 170,8 235,5 21,4 45,6
Gauteng 27,1 29,4 180,9 127,3 24,6 19,1
KwaZulu-Natal 30,5 30,9 136,8 141,7 18,5 17,9
Limpopo 18,8 20,5 242,9 208,3 70,8 69,4
Mpumalanga 18,9 22,2 242,4 190,6 76,1 41,7
North West 21,4 23,7 230,2 128,1 38,4 45,2 Northern Cape 20,9 21,8 185,9 111,8 44,6 22,4
Western Cape 29,2 30,0 88,8 87,5 15,6 10,5
South Africa 25,7 27,4 169,6 145,7 30,6 27,8
CD – Caesarean delivery; MD – Maternal Deaths; BLDACD – Bleeding during or after caesarean delivery; CFR – Case fatality rate expressed per 100000 CDs
The Case fatality rates (CFR) for CD and for bleeding associated with CD (BLDACD)are highest in Limpopo, Free State, Mpumulanga and North West and show no signs of declining in these provinces. The highest CFR for BLDACD is 69.4 per 100000 CDs and the lowest is 10.5 in the Western Cape. This reflects major inequity in the safety of CD in different provinces.

15
8. Levels of care and mortality
Note: Data given as level of care; number of births; percent of births
In most provinces the majority of births occur at district level except Gauteng where the most are at Regional hospitals. This does not appear to be an appropriate use of resources and needs to be explored. The use of On-site Midwife run Birthing Units (OMBUs) must be strongly considered in these areas. Deaths outside facilities are under-represented in the NCCEMD where the focus is predominantly on institutional deaths
C; 41125; 5%
CHC; 115525; 12%
DH; 379641; 41%RH; 245483; 26%
PTH; 95757; 10%
NCH; 59093; 6%
Figure 11. Distribution of births in South Africa
0
10000
20000
30000
40000
50000
60000
70000
80000
90000
EC FS Gau KZN Lim Mpu NW NC WC
Figure 12. Numbers of Births per province per level of care
C CHC DH RH PTH NCH

16
C; 41125; 5%
CHC; 115525; 12%
DH; 379641; 41%RH; 245483; 26%
PTH; 95757; 10%
NCH; 59093; 6%
Figure 13. Distribution of births in South Africa
0,00
50,00
100,00
150,00
200,00
250,00
300,00
350,00
31156650
CHC
276379641
DH
364245483
RH
20695757PTH
17359093NCH
iMM
R/10
0000
live
bir
ths
Figure 14. Comparison of the iMMR per level of care: 2017

17
Figure 15. Distribution of births and maternal deaths per level of care: 2017
C; 41125; 5%
CHC; 115525; 12%
DH; 379641; 41%
RH; 245483; 26%
PTH; 95757; 10%
NCH; 59093; 6%
Distribution of births in South AfricaC; 0; 0%
CHC; 31; 3%
DH; 276; 25%
RH; 364; 34%
PTH; 206; 19%
NCH; 173; 16%
Pvt; 35; 3%
Distribution of maternal deaths per level of care
Figure 16. Distribution births and deaths 2014-2016
497319; 18%
1147326; 42%
703660; 26%
215166; 8%
172876; 6%Distribution of live births
CHC DH RH PT NC
75; 2%
980; 26%
1161; 31%
880; 24%
283; 8%
140; 4%178; 5%
Distribution of maternal deaths
CHC DH RH PTH NC Pvt Out

18
There was a 41.6% reduction in iMMR in the PTH This is an encouraging trend after the focus placed on PTHs after the recent triennial report.
Table 14. Comparison of the number of maternal deaths per level of care and its distribution
(Excludes deaths outside facilities and coincidental deaths)
14.a. Number of maternal deaths per underlying cause and level of care CHC District
hospital Regional hospital
Tertiary hospital
Nat central hospital
Private hospital Total
Medical and surgical disorders 5 29 42 24 33 10 143
Non-pregnancy-related infections 4 66 112 45 45 4 276
Ectopic pregnancy 1 18 11 5 2 0 37
Miscarriage 0 19 24 20 7 0 70
Pregnancy-related sepsis 1 11 19 18 14 1 64 Obstetric haemorrhage 7 52 59 29 14 9 170
Hypertension 5 34 65 47 41 3 195
Anaesthetic complications 0 19 3 2 3 2 29 Adverse drug reactions 0 1 1 3 5 0 10 Embolism 3 7 9 7 2 3 31 Acute collapse - cause unknown 2 7 2 1 0 0 12
Miscellaneous 0 0 2 1 2 0 5
Unknown 3 5 6 0 0 3 17
Maternal deaths 31 268 355 202 168 35 1059
Coincidental cause 0 8 9 6 4 0
15,1
85,4
165,0
368,1
214,6
19,79
72,70
148,28
215,13
292,76
0,0
50,0
100,0
150,0
200,0
250,0
300,0
350,0
400,0
CHC DH RH PTH NCH
iMM
R/10
0000
live
birt
hs
Figure 17. Comparison iMMR per level of care 2014-2016 and 2017
2014-2016 iMMR 2017 iMMR

19
14.b. Distribution of underlying causes of maternal deaths within level of care CHC District
hospital Regional hospital
Tertiary hospital
Nat central hospital
Private hospital Total
Medical and surgical disorders 16,1 10,8 11,8 11,9 19,6 28,6 13,5
Non-pregnancy-related infections 12,9 24,6 31,5 22,3 26,8 11,4 26,1
Ectopic pregnancy 3,2 6,7 3,1 2,5 1,2 0,0 3,5
Miscarriage 0,0 7,1 6,8 9,9 4,2 0,0 6,6
Pregnancy-related sepsis 3,2 4,1 5,4 8,9 8,3 2,9 6,0
Obstetric haemorrhage 22,6 19,4 16,6 14,4 8,3 25,7 16,1 Hypertension 16,1 12,7 18,3 23,3 24,4 8,6 18,4
Anaesthetic complications 0,0 7,1 0,8 1,0 1,8 5,7 2,7
Adverse drug reactions 0,0 0,4 0,3 1,5 3,0 0,0 0,9
Embolism 9,7 2,6 2,5 3,5 1,2 8,6 2,9
Acute collapse - cause unknown 6,5 2,6 0,6 0,5 0,0 0,0 1,1
Miscellaneous 0,0 0,0 0,6 0,5 1,2 0,0 0,5 Unknown 9,7 1,9 1,7 0,0 0,0 8,6 1,6
Maternal deaths 100,0 100,0 100,0 100,0 100,0 100,0 100,0
14.c. Distribution of underlying causes of maternal deaths across the levels of care CHC District
hospital Regional hospital
Tertiary hospital
Nat central hospital
Private hospital Total
Medical and surgical disorders 3,5 20,3 29,4 16,8 23,1 7,0 100,0
Non-pregnancy-related infections 1,4 23,9 40,6 16,3 16,3 1,4 100,0
Ectopic pregnancy 2,7 48,6 29,7 13,5 5,4 0,0 100,0
Miscarriage 0,0 27,1 34,3 28,6 10,0 0,0 100,0
Pregnancy-related sepsis 1,6 17,2 29,7 28,1 21,9 1,6 100,0 Obstetric haemorrhage 4,1 30,6 34,7 17,1 8,2 5,3 100,0
Hypertension 2,6 17,4 33,3 24,1 21,0 1,5 100,0
Anaesthetic complications 0,0 65,5 10,3 6,9 10,3 6,9 100,0
Adverse drug reactions 0,0 10,0 10,0 30,0 50,0 0,0 100,0
Embolism 9,7 22,6 29,0 22,6 6,5 9,7 100,0
Acute collapse - cause unknown 16,7 58,3 16,7 8,3 0,0 0,0 100,0 Miscellaneous 0,0 0,0 40,0 20,0 40,0 0,0 100,0
Unknown 17,6 29,4 35,3 0,0 0,0 17,6 100,0
Maternal deaths 2,9 25,3 33,5 19,1 15,9 3,3 100,0
CHC – Community Health Centre; Nat Central hospital – National Central hospital

20
Table 15. Comparison of iMMR per level of care and underlying cause
Underlying cause CHC District hospital
Regional hospital
Provincial Tertiary hospital
National Central hospital
Medical and surgical disorders 3,19 7,64 17,11 25,06 55,84 Non-pregnancy-related infections 2,55 17,38 45,62 46,99 76,15 Ectopic pregnancy 0,64 4,74 4,48 5,22 3,38 Miscarriage 0,00 5,00 9,78 20,89 11,85 Pregnancy-related sepsis 0,64 2,90 7,74 18,80 23,69 Obstetric haemorrhage 4,47 13,70 24,03 30,28 23,69 Hypertension 3,19 8,96 26,48 49,08 69,38 Anaesthetic complications 0,00 5,00 1,22 2,09 5,08 Adverse drug reactions 0,00 0,26 0,41 3,13 8,46 Embolism 1,92 1,84 3,67 7,31 3,38 Acute collapse - cause unknown 1,28 1,84 0,81 1,04 0,00 Miscellaneous 0,00 0,00 0,81 1,04 3,38 Unknown 1,92 1,32 2,44 0,00 0,00 iMMR 19,79 70,59 144,61 210,95 284,30
This table shows the referral system is working. It is important to note that in the tertiary hospitals complications of hypertensive diseases in pregnancy have the highest mortality. The distribution of mortality of NPRI also indicates the complicated cases are getting to the higher levels of care. On the other hand the greatest numbers of OH deaths are at DH and RH, reflecting that OH occurs so acutely that the patients do not survive the referral chain; dying before, during or immediately after referral.
0,00
10,00
20,00
30,00
40,00
50,00
60,00
70,00
80,00
CHC DH RH PTH NCH
iMM
R/10
0000
live
birt
hs
Figure 18. Comparison of iMMR per level of care and underlying causes
M&S NPRI Ec Miscr. PRS OH HT AR

21
9. Potentially preventable deaths
Table 16. Distribution of suboptimal care per underlying cause
IMPACT OF SUBOPTIMAL CARE M&S NPRI Ec Miscr. PRS OH HT AR Emb AC MD
(Exclude Coin)
- No suboptimal care identified 52 107 6 15 13 18 31 2 17 3 299 - Suboptimal care, no impact on outcome 19 45 3 9 3 5 18 1 2 3 114 - Suboptimal care, possible impact on outcome 54 92 4 20 21 51 65 3 9 5 340 - Suboptimal care, probable impact on outcome 28 39 26 27 29 102 86 23 6 4 379 Total 153 283 39 71 66 176 200 29 34 15 1132
IMPACT OF SUBOPTIMAL CARE (%) M&S NPRI Ec Miscr. PRS OH HT AR Emb AC MD
(Exclude Coin)
- No suboptimal care identified 34,0 37,8 15,4 21,1 19,7 10,2 15,5 6,9 50,0 20,0 26,4 - Suboptimal care, no impact on outcome 12,4 15,9 7,7 12,7 4,5 2,8 9,0 3,4 5,9 20,0 10,1 - Suboptimal care, possible impact on outcome 35,3 32,5 10,3 28,2 31,8 29,0 32,5 10,3 26,5 33,3 30,0 - Suboptimal care, probable impact on outcome 18,3 13,8 66,7 38,0 43,9 58,0 43,0 79,3 17,6 26,7 33,5
M&S – pre-existing medical and surgical conditions; NPRI – Non-pregnancy related infections; Ec – Ectopic pregnancy; Misc – Miscarriage; PRS – Pregnancy related sepsis; HT – Hypertensive disorders of pregnancy; OH – Obstetric haemorrhage; AR – Anaesthetic related; Emb. – Embolism; AC – Acute collapse, cause unknown; Unk. – Unknown; MD (Exclude Coin) – Maternal deaths excluding coincidental deaths

22
M&S – Medical and surgical disorders; NPRI – Non-pregnancy related infections; Ec – Ectopic pregnancy; Misc – Miscarriage; PRS – Pregnancy related sepsis; HT – Hypertensive disorders in pregnancy; OH – Obstetric haemorrhage; AR – Anaesthetic related; Emb. – Embolism; AC – Acute collapse, cause unknown; ALL MD – All
maternal deaths
Table 17. Distribution of potentially preventable maternal deaths from 2008-2017 per underlying cause
PP iMMR, 3 triennia M&S NPRI EC Misc. PRS OH HT AR Emb AC 2008-2010 8,37 29,48 2,08 4,40 7,10 21,41 15,97 4,21 1,50 2,01 2011-2013 9,07 23,18 3,02 4,37 6,26 21,72 15,11 3,52 1,60 1,88 2014-2016 8,21 15,12 2,87 4,07 5,81 19,91 17,01 2,94 2,29 1,20 2017 9,06 14,47 3,31 5,19 5,52 16,90 16,68 2,87 1,66 0,99
M&S – Medical and surgical disorders; NPRI – Non-pregnancy related infections; Ec – Ectopic pregnancy; Misc – Miscarriage; PRS – Pregnancy related sepsis; HT – Hypertensive disorders in pregnancy; OH – Obstetric haemorrhage; AR – Anaesthetic related; Emb. – Embolism; AC – Acute collapse, cause unknown The iMMR of potentially preventable deaths has shown considerable reductions for NPRI, OH, PRS and Anaesthetic deaths, in that order of magnitude. For all other causes there has been minimal change; and of particular concern a slight increase for hypertensive disorders in pregnancy deaths.
0,0
20,0
40,0
60,0
80,0
100,0
% potentially preventable deathsPe
rcen
t
Figure 19. Proportion of potentially preventable deaths per disease category
M&S NPRI Ec Miscr. PRS OH HT AR Emb AC All MD

23
M&S –Medical and surgical disorders; NPRI – Non-pregnancy related infections; Ec – Ectopic pregnancy; Misc – Miscarriage; PRS – Pregnancy related sepsis; HT – Hypertensive disorders in pregnancy; OH – Obstetric haemorrhage; AR – Anaesthetic related; Emb. – Embolism; AC – Acute collapse, cause unknown
0,00
5,00
10,00
15,00
20,00
25,00
30,00
35,00
M&S NPRI EC Misc. PRS OH HT AR Emb AC
iMM
R/10
0000
live
birt
hs
Figure 20. Comparison of potentially preventable maternal mortality ratio
2008-2010
2011-2013
2014-2016
2017

24
Table 18. Comparison of potentially preventable and non-preventable iMMR from 2008-2017
PP deaths/year PP iMMR NP iMMR Proportion of potentially
preventable deaths of all maternal deaths (%)
2008-2010 100 76,22 56,7 2011-2013 92,6 61,46 60,1 2014-2016 83,3 51,03 62,0 2017 79,4 49,8 61,4 PP iMMR– Potentially preventable iMMR; NP iMMR – non-preventable iMMR
M&S –Medical and surgical disorderss; NPRI – Non-pregnancy related infections; Ec – Ectopic pregnancy; Misc – Miscarriage; PRS – Pregnancy related sepsis; HT – Hypertensive disorders in pregnancy; OH – Obstetric haemorrhage; AR – Anaesthetic related; Emb. – Embolism; AC – Acute collapse, cause unknown 75% of potentially preventable deaths are due to OH (22.0%), HT (21,8%), NPRI (18,9%), M&S (11,8%)
020406080
100120140160180200
2008-2010 2011-2013 2014-2016 2017
iMM
R/10
0000
live
birt
hsFigure 21. Comparison of prevental and non-prevental maternal deaths
NP iMMR
PP iMMR
0,0
5,0
10,0
15,0
20,0
25,0
% Potentially preventable deaths
Perc
ent
Figure 22. Contibution of underlying causes to potentially preventable deaths
M&S NPRI Ec Miscr. PRS OH HT AR Emb AC

25
This graph illustrates very well the changing pattern of preventable maternal deaths in South Africa. As expected NPRI followed by haemorrhage were the major problems in 2008-2010, but as those problems have been successfully dealt with, other conditions are becoming more important, namely hypertensive diseases of pregnancy and medical and surgical conditions.
10. Avoidable factors, underlying conditions and level of care
Table 19. Distribution of avoidable factors per level of care and underlying condition
% Avoidable factor All M&S NPRI Ec Miscr PRS OH HT AR Emb AC CHC s 40,0 26,5 55,6 25,0 9,1 28,0 36,1 49,0 18,2 14,3 36,4 District Hospital 66,6 55,4 55,2 94,7 86,7 61,3 90,4 60,2 85,7 50,0 90,0 Regional Hospital 58,2 65,4 45,4 73,3 60,7 61,3 77,3 65,2 75,0 33,3 0,0 Tertiary Hospital 44,2 32,7 33,3 80,0 60,9 53,3 53,7 49,3 100,0 50,0 100,0 Private Hospitals 72,9 66,7 50,0 0,0 100,0 66,7 112,5 75,0 50,0 50,0 0,0
M&S –Medical and surgical disorders; NPRI – Non-pregnancy related infections; Ec – Ectopic pregnancy; Misc – Miscarriage; PRS – Pregnancy related sepsis; HT – Hypertensive disorders in pregnancy; OH – Obstetric haemorrhage; AR – Anaesthetic related; Emb. – Embolism; AC – Acute collapse, cause unknown; CHCs – Community health centres It is at DHs level where the highest iMMR for potentially preventable deaths is occurring.
0,0
5,0
10,0
15,0
20,0
25,0
30,0
35,0
2008-2010 2011-2013 2014-2016 2017
Perc
ent
Figure 1. Distribution of potential preventable deaths 2008-2017
NPRIOHHTM&S

26
M&S –Medical and surgical disorders; NPRI – Non-pregnancy related infections; Misc – Miscarriage; PRS –
Pregnancy related sepsis; OH – Obstetric haemorrhage; HT – Hypertensive disorders in pregnancy Miscarriage and OH stand out as problems in management in DHs. Regional hospitals stand out across the board as having a high proportion of avoidable factors for all per underlying causes. These hospitals (RH) are supposed to have specialist cover. This aspect is often lacking and this may explain the higher proportion of avoidable factors for this level of care.
0,010,020,030,040,050,060,070,080,090,0
100,0
All M&S NPRI Miscr PRS OH HT
Perc
ent
Figure 23. Proportion of avoidable factors per level of care for common conditions
CHC s District Hospital Regional Hospital Tertiary Hospital

27
Table 20. Health care professional avoidable factors per level of care
Description CHC Dist DH Dist RH Dist PTH Dist Pvt Dist Managed at this level 502 583 474 377 54 Lack of information 39 38 22 22 6 Number assessable cases 463 545 452 355 48 No avoidable factor 284 197 193 201 14 % no avoidable factor 61,3 36,1 42,7 56,6 29,2 Number cases with avoidable factor 179 348 259 154 34 % avoidable factor 38,7 63,9 57,3 43,4 70,8 Distribution of avoidable factors in cases with avoidable factors % % % % % Initial assessment 82 45,8 124 35,6 58 22,4 25 16,2 10 29,4 Problem with recognition / diagnosis 105 58,7 184 52,9 103 39,8 51 33,1 17 50,0 Delay in referring the patient 59 33,0 119 34,2 36 13,9 3 1,9 5 14,7 Managed at inappropriate level 29 16,2 93 26,7 30 11,6 1 0,6 2 5,9 Incorrect management (Wrong diagnosis) 15 8,4 68 19,5 39 15,1 21 13,6 1 2,9 Sub-standard management (Correct diagnosis) 44 24,6 177 50,9 146 56,4 96 62,3 16 47,1 Not monitored / Infrequently monitored 9 5,0 43 12,4 39 15,1 15 9,7 1 2,9 Prolonged abnormal monitoring with no action taken 14 7,8 70 20,1 33 12,7 23 14,9 5 14,7
CHC – Community health centre; Dist. – Distribution of avoidable factors in percent; DH – District Hospital; RH – Regional Hospital; PTH – Tertiary Hospital; Pvt. – Private hospital The avoidable factors shift per level of care with most of the problems at the primary level being poor initial assessment and lack of recognition of the condition; whereas in the higher level of care it is not following the standard protocols which are the most frequent avoidable factors.

28
Administrative and patient orientated avoidable factors
Table 21. Administrative avoidable factors per level of care Description All CHC DH RH PTH NC Pvt Lack of information 63 5 13 13 11 9 2 No avoidable factor 595 23 114 190 110 84 24 Assessable cases 532 26 101 177 99 75 22 Number cases with AF 600 5 175 187 140 66 13 % of MD with Administrative Avoidable Factors 53,0 16,1 63,4 51,4 58,6 46,8 37,1 Transport problem: Home to institution 20 2 5 5 2 3 0 Lack of accessibility: Barriers to entry 8 0 3 1 4 0 0 Lack of accessibility: Other 9 0 3 5 1 0 0 Delay initiating critical care (Overburdened service) 59 0 10 23 18 7 0 Lack of health care facilities: ICU 80 0 14 24 31 11 0 Lack of health care facilities: Blood/blood products 32 0 13 10 3 2 3 Lack of health care facilities: Other 29 1 5 14 7 1 0 Communication problems: Technical 19 1 5 3 8 1 1 Communication problems: Interpersonal 36 2 8 18 7 1 2 Lack of appropriately trained staff: Doctors 209 3 88 53 44 17 3 Lack of appropriately trained staff: Nurses 134 4 51 35 23 16 1 Maternal deaths 1132 31 276 364 239 141 35 Distribution of Administrative Avoidable Factors Transport problem: Home to institution 3,3 40 2,9 2,7 1,4 4,5 23,1 Lack of accessibility: Barriers to entry 1,3 0 1,7 0,5 2,9 0,0 0,0 Lack of accessibility: Other 1,5 0 1,7 2,7 0,7 0,0 7,7 Delay initiating critical care (Overburdened service) 9,8 0 5,7 12,3 12,9 10,6 15,4 Lack of health care facilities: ICU 13,3 0 8,0 12,8 22,1 16,7 269,2 Lack of health care facilities: Blood/blood products 5,3 0 7,4 5,3 2,1 3,0 0,0 Lack of health care facilities: Other 4,8 20 2,9 7,5 5,0 1,5 177,5 Communication problems: Technical 3,2 20 2,9 1,6 5,7 1,5 0,0 Communication problems: Interpersonal 6,0 40 4,6 9,6 5,0 1,5 59,2 Proportion deaths associated lack of skills Doctors 18,46 9,68 31,88 14,56 18,41 12,06 8,57 Nurses 11,84 12,90 18,48 9,62 9,62 11,35 2,86 CHC – Community health centre; Dist. – Distribution of avoidable factors in percent; DH – District Hospital; RH – Regional Hospital; PTH – Tertiary Hospital; Pvt. – Private hospital Overburdened services and lack of ICU are a problem for regional and provincial tertiary hospitals which has become a problem with more referrals from DHs. However, as in previous reports, lack of appropriately trained staff stands out as a frequently cited avoidable factors. Below is a graph of the distribution of lack of appropriately trained staff per province. It is clear from this graph that the rural provinces are those most affected by the lack of appropriately trained and skilled staff. This is an area that must be addressed if there is to be a reduction in mortality.

29
Table 22 below examines the role of inter facility transport as an avoidable factor in maternal deaths per level of care. As expected the majority of referrals of women that died is from the primary levels of care, but what is surprising is how few cases there was apparently a problem with the inter-facility transport, only 2% from CHCs and 7% from district hospitals. This is contrast to the high problems of referral problems (24%) noted in the recent triennial report when OH deaths were analysed separately. Although few cases in numbers, referral from hospitals with specialists (regional and provincial tertiary) had a higher proportion of problems; presumably due to the inability to get access to beds in national central hospitals. Lack of appropriately trained staff continues to be cited by assessors as a major avoidable factor. This is despite ESMOE training. This raises the question of whether there are inadequate staffing levels in institutions and/or incorrect deployment of appropriate level of skilled staff. It would be useful to compare this avoidable factor between provinces because there is a definite perception of inequities in skilled staffing between different provinces and districts (e.g. some provinces only have one specialist anaesthetist and some have no specialist obstetrician).
Table 22. Referral of patients from various levels of care and proportion of problems associated with transport between facilities
Referred from level n % of referred patients % of all patients
CHC 214 36,4 18,3 District Hospital 281 47,8 24
Regional Hospital 62 10,5 5,3
Tertiary Hospital 13 2,2 1,1
National Central Hospital 0 0 0 Private Hospital 18 3,1 1,5 Total 588 50,3 Problems Total transferred % Transport from CHC 4 214 1,9 Transport from DH 20 281 7,1 Transport from RH 12 62 19,4 Transport from PTH 16 16 100
CHC – Community health centre; Dist. – Distribution of avoidable factors in percent; DH – District Hospital; RH – Regional Hospital; PTH – Tertiary Hospital; Pvt. – Private hospital
0,0
10,0
20,0
30,0
40,0
50,0
60,0
EC FS Gau KZN Lim Mpu NW NC WC SA
Perc
ent
Figure 24. Lack of appropriately trained staff per province
Doctors
Nurses

30
There is a slight improvement in the transport between institutions compared with the last triennium. In the last triennium problems with transport from a CHC, DH, and RH was 2,2%, 9,5%, 25,7% respectively. Patient related avoidable factors shown in table 23 is similar to previous report. The high proportion of delay in accessing medical help is a mostly a transport problem from home to a facility, and not due to the woman or family not wanting the woman to go to a health institution.
Table 23. Patient related avoidable factors
Patient related All % of cases Lack of information 97 No avoidable factor 503 Assessable cases 1035 Cases with Avoidable Factors 532 % with Avoidable Factors 51,4 No antenatal care 198 37,2 Infrequent antenatal care 77 14,5 Delay in accessing medical help 303 57,0 Declined medication/surgery/advice 87 16,4 Family problem 14 2,6 Community problem 6 1,1 Unsafe abortion* 18 24,0 Other 64 12,0
*75 women died due to miscarriage,
Mortality ratios and level of care per province Figure 24 illustrates the number of births per level of care and the number of maternal deaths per level of care per province. The pattern varies per province depending on their structure.
Figure 24. Comparison of number of births and number of maternal deaths per level of care and per province
0
10000
20000
30000
40000
50000
60000
70000
80000
90000
EC FS Gau KZN Lim Mpu NW NC WC
Births per province per level of care
C CHC DH RH PTH NCH
0
20
40
60
80
100
120
140
EC FS Gau KZN Lim Mpu NW NC WC
Number of maternal deaths per province per level of care
CHC+C DH RH PTH NCH

31
MD – Maternal death; LOC – Level of Care; Figure 25 give the number of deaths per level of care and figure 26 gives the iMMR per level of care per province. In all provinces the higher levels, as expected, have higher mortality ratios.
Figure 27 however, compares the iMMR per level of care per province with all the other provinces (excluding national central hospitals). The red line and figure is the national average. The two outliers in the CHCs are the Northern Cape (but there were only 4 maternal deaths, but as the numbers are small the ratio is high) and KwaZulu-Natal where there were 9 maternal deaths. The rural provinces, with the exception of the Eastern Cape and Free State have the highest mortality ratios in the district hospitals, with North West and Limpopo having the highest ratios. In regional hospitals North West, Mpumalanga and the Free State have the highest ratios. Limpopo, KwaZulu-Natal, the Free State and
Figure 25. Number MD per province per LOC
0
10
20
30
40
50
60
70
CHC+C DH
CHC & DH
EC FS Gau KZN Lim Mpu NW NC WC
0
20
40
60
80
100
120
140
RH PTH NCH
RH, PTH & NCH
EC FS Gau KZN Lim Mpu NW NC WC
0,00
100,00
200,00
300,00
400,00
500,00
600,00
700,00
800,00
EC FS Gau KZN Lim Mpu NW NC WC
iMM
R/1
0000
0 liv
e bi
rths
Figure 26. iMMR per province per level of care
CHC+C DH RH PTH NCH

32
Mpumalanga have the highest provincial tertiary hospital ratios. The Western Cape has no Provincial Tertiary Hospitals.
The differences in the mortality ratios per level of care per province gives the areas where each province can concentrate their activities. The detailed recommendations and implementation process will be performed per level of care for this report and appears as an appendix.
Figure 27. iMMR per LOC and province
0,00
20,00
40,00
60,00
80,00
100,00
120,00
140,00
CHC+C DH
CHC+C and DH
EC FS Gau KZN Lim Mpu NW NC WC
72.7
0,00
100,00
200,00
300,00
400,00
500,00
600,00
700,00
800,00
RH PTH
RH and PTH
EC FS Gau KZN Lim Mpu NW NC WC
148.3
249.6
19.8

33
12. Summary of findings 2017
• The decline in iMMR is plateauing • ARV programmes have been effective but need vigilance; sharp decline NPRI no longer
happening; there is a need to explore reasons for this. • It is encouraging that there is an overall decrease in deaths rue to OH but this has not
occurred in all provinces and still needs attention • Focus on reducing deaths from HDP needs to be highlighted with an action plan which
includes strengthening BANC Plus • Higher proportion of avoidable deaths in DH point to need for mentorship at this level and
the improvement of emergency transport from this level to RH or PTH where the deaths tend to occur after referral. NASG and involvement of EMS important for this.
• There has been a marked improvement in the iMMR of Provincial Tertiary Hospitals. The reason for this is not immediately clear, but there was a 2% increase in births and a 2% reduction in maternal deaths. Perhaps the enquiry into the functioning of the PTHs has had an effect on their better functioning.
• Lack of appropriately trained doctors and nurses continues to be the most frequently cited avoidable factor
• Problems with inter-facility transport of ill patients has been reduced, but there is still a large problem with women getting from home to a health facility. Innovative ways of ensuring transport at all times from townships and rural areas needs to be investigated. Community involvement is very important in this aspect, as are maternity waiting areas.
• Concentration of high CFRs for CD and BLDACD in certain provinces illustrates serious inequities in maternal health care provision. It appears that these are also the provinces with the greatest reported incidents of “lack of appropriately trained staff”; this needs to be explored further. It is known that some of the provinces with poorest outcomes have unacceptable deficiencies in numbers of specialists.
• Ways of reducing inequities and focussing on skills distribution and functional facilities in the poorest provinces needs to be focussed on. KwaZulu-Natal is similar to all the rural provinces, yet has a very low proportion of avoidable factors related to lack of appropriately trained staff. An investigation as to what KwaZulu-Natal is doing to ensure appropriate staffing compared to the other provinces should be performed as soon as possible to help the other provinces follow best practices.

34
13. Conclusions and recommendations The low hanging fruit has been plucked and further reductions in maternal deaths will require system wide interventions which are difficult to achieve. Using managing cases of hypertensive diseases in pregnancy as the prototype to identify and change bottlenecks in managing sick pregnant women in all levels of care from primary health care clinics to tertiary hospitals and is a good way to go to develop the system wide interventions. Hypertensive disorders of pregnancy have evolved to be the biggest problem in preventing potentially preventable maternal deaths and so should have a high priority for solving. New detailed guidelines have been developed that affect every level of the health care system and getting these right will get the systems right for other conditions. This strengthening must occur in parallel with the strengthening of BANC Plus. The inequity of the distribution of health care professionals is clearly illustrated in this report, with the poorer and more rural provinces having the biggest problems with lack of appropriately trained doctors and nurses. This must also be seen in the context that these provinces also have the least number of specialists which compounds the problems. This issue needs to be tackled if further reduction in mortality is to be achieved. The target of less than 1000 maternal deaths in 2020 will only be achieved if these issues are addressed. Recommendations The 3 Hs and 5Cs are still extremely relevant. To support this the following must be enthusiastically supported. 1. Introduce the new guidelines in managing hypertensive diseases in pregnancy and use these
guidelines to identify barriers to implementation and then to solve them, especially including BANC Plus.
2. Continue with the Safe CD programme and ensure all hospitals doing CD are accredited and have accredited surgeons and anaesthetists.
3. Continue ensuring that the 90, 90, 90 programme for HIV infected pregnant women is strongly supported.
4. Consider innovative ways to solve the lack of skills in the rural provinces. 5. Engage the community in developing ways so that women with emergencies can get from home
to a health facility at any time of day or night 6. Engage with EMS about transport of women with emergencies from home; and inter-facility
transfer of women with haemorrhage including role out of the NASG for such referrals

35
14. Suggested recommendations per province
Glossary • Support – here means the DCSTs and MCWH coordinators must engage with the hospitals
mentioned • Introduce or re-enforce the Safe CD package means that the full package must be
introduced. DCSTs should oversee this. • Introduce new HDP guideline means training in the guideline at all levels of care from PHC to
National Central Hospitals. It includes BANC Plus and ESMOE. The DCSTs and MCWH coordinators should be responsible for this.
• Introduce the non-pneumatic anti-shock garment (NASG) means procuring it for the province and then having the specific one-day training programme at the sites where the NASG is available.
• Introduce the new PMTCT guidelines • Training programmes are available for NASG, HDP Guideline, BANC Plus for next level of
expertise are available • The introduction of the packages also implies that regular emergency drills concerning the
topics are conducted. • Provinces will need to interrogate their own data, discuss their challenges and devise their
own strategies for implementing the recommendations suggested by NCCEMD for their province
Overview • Further reduction in maternal mortality will be more difficult and involved all aspects of the
health system • Focus on ways of reducing inequities and focusing on skills distribution and functional
facilities in the poorest provinces • New Hypertensive Disorders in Pregnancy, postpartum haemorrhage, PMTCT guidelines and
Safe CD package need to be rigorously implemented
Eastern Cape Challenges
• Priority conditions (15% above national average): • HDP, Anaesthesia and embolism and acute collapse
• Attracting staff to district hospitals • Support for National Central hospital
Strategies • Meet with KZN and WC to develop strategies to retain staff at district hospitals • Ensure all staff giving anaesthesia go through the ESMOE anaesthetic module • Introduce new HDP guideline • Introduce the non-pneumatic anti-shock garment • Introduce new PMTCT guidelines

36
Free State Challenges
• Priority conditions (15% above national average) • HDP, OH, early pregnancy loss, pregnancy related sepsis, anaesthesia
• Surgical and anaesthetic skills Strategies
• Meet with KZN and WC to develop strategies to retain staff at district hospitals • Support regional hospitals and provincial tertiary hospitals • Introduce new HDP guideline • Re-enforce Safe CD package (surgical and anaesthetic skills) • Introduce non-pneumatic anti-shock garment • Introduce new PMTCT guidelines
Gauteng Challenges
• Priority conditions (15% above national average) • Miscarriage and pregnancy related sepsis
• Improve data collection Strategies
• Introduce On-site Midwife-run Maternity units in regional and provincial tertiary hospitals • Support regional hospitals • Introduce new HDP guideline • Introduce new PMTCT guidelines
Kwa-ZuluNatal Challenges
• Priority conditions (15% above national average) • Anaesthesia, PMTCT protocols, medical and surgical conditions
• Surgical and anaesthetic skills Strategies
• Re-enforce Safe CD package (surgical and anaesthetic skills) • Ensure all clincians giving aneasthesia have done the ESMOE Anaesthetic module • High risk clinics for medical and surgical conditions • Introduce new PMTCT guidelines
Limpopo Challenges
• Priority conditions (15% above national average) • OH, ectopic pregnancy, anaesthesia, NPRI,
• Surgical and anaesthetic skills • Lack of skilled staff in district hospitals
Strategies • Meet with KZN and WC to develop strategies to retain staff at district hospitals

37
• Introduce Safe CD package • Support regional hospitals and provincial tertiary hospitals • Introduce new HDP guideline • Introduce non-pneumatic anti-shock garment • Introduce new PMTCT guidelines
Mpumalanga Challenges
• Priority conditions (15% above national average) • HDP, OH, early pregnancy loss, embolism
• Surgical and anaesthetic skills • Lack of skills in district hospitals, regional and provincial tertiary hospitals
Strategies • Meet with KZN and WC to develop strategies to retain staff at district hospitals • Support district, regional and provincial tertiary hospitals • Introduce new HDP guideline • Re-enforce Safe CD package (surgical and anaesthetic skills) • Introduce non-pneumatic anti-shock garment • Introduce new PMTCT guidelines
North West Challenges
• Priority conditions (15% above national average): • HDP, OH, early pregnancy loss, embolism NPRI
• Surgical and anaesthetic skills • Attracting staff to district hospitals
Strategies • Meet with KZN and WC to develop strategies to retain staff at district hospitals • Ensure all staff giving anaesthesia go through the ESMOE anaesthetic module • Introduce the safe CD programme • Support for regional hospital • Introduce new HDP guideline • Introduce non-pneumatic anti-shock garment
Northern Cape Challenges
• Priority conditions (15% above national average): • HDP, OH, early pregnancy loss,
• Surgical and anaesthetic skills • Attracting staff to district hospitals
Strategies • Meet with KZN and WC to develop strategies to retain staff at district hospitals • Ensure all staff giving anaesthesia go through the ESMOE anaesthetic module • Introduce the safe CD programme • Support for district hospitals

38
• Introduce new HDP guideline • Introduce non-pneumatic anti-shock garment
Western Cape Challenges
• Priority conditions (15% above national average): • Embolism
Strategies • Ensure protocols for anti-thrombus prophylaxis are introduced and used • Introduce new HDP guideline • Introduce non-pneumatic anti-shock garment • Introduce new PMTCT guidelines

39
Appendix 1: Comparison of maternal deaths in DHIS and MaMMAS per district
Organisation unit Live births DHIS MD MaMMAS ec Alfred Nzo District Municipality 11510 6 6 ec Amathole District Municipality and ec Buffalo City Metropolitan Municipality (Combined because MaMMAS database) 21293 19 21 ec Chris Hani District Municipality 10682 17 18 ec Joe Gqabi District Municipality 4560 2 2 ec Nelson Mandela Bay Municipality 18936 25 26 ec Oliver Tambo District Municipality 27208 61 65 ec Sarah Baartman District Municipality 5738 5 4 Eastern Cape 99927 135 142 fs Fezile Dabi District Municipality 6912 12 10 fs Lejweleputswa District Municipality 9313 10 11 fs Mangaung Metropolitan Municipality 14689 29 30 fs Thabo Mofutsanyana District Municipality 12853 14 17 fs Xhariep District Municipality 792 0 1 Free State 44559 65 69 gp City of Ekurhuleni Metropolitan Municipality 62545 71 68 gp City of Johannesburg Metropolitan Municipality 69985 71 55 gp City of Tshwane Metropolitan Municipality 51330 80 73 gp Sedibeng District Municipality 14707 19 14 gp West Rand District Municipality 15388 16 14 Gauteng 213955 257 224 kz Amajuba District Municipality 8370 12 14 kz eThekwini Metropolitan Municipality 55289 55 88 kz Harry Gwala District Municipality 7453 6 7 kz iLembe District Municipality 10288 9 9 kz King Cetshwayo District Municipality 17997 27 28 kz Ugu District Municipality 12368 11 12 kz uMgungundlovu District Municipality 15965 27 33 kz Umkhanyakude District Municipality 14866 11 14 kz Umzinyathi District Municipality 10412 8 9 kz Uthukela District Municipality 11231 13 13 kz Zululand District Municipality 16326 14 18 KwaZulu-Natal 180565 193 245 lp Capricorn District Municipality 26678 70 82 lp Mopani District Municipality 24232 26 28 lp Sekhukhune District Municipality 25018 15 28 lp Vhembe District Municipality 28824 23 22 lp Waterberg District Municipality 14411 16 21 Limpopo 119163 150 181 mp Ehlanzeni District Municipality 38496 41 59 mp Gert Sibande District Municipality 17738 22 23 mp Nkangala District Municipality 19387 34 36 Mpumalanga 75621 97 118 nw Bojanala Platinum District Municipality 20328 19 25 nw Dr Kenneth Kaunda District Municipality 12645 24 26 nw Dr Ruth Segomotsi Mompati District Municipality 8119 2 3 nw Ngaka Modiri Molema District Municipality 14823 24 29 North West 55915 69 83 nc Frances Baard District Municipality 7826 9 13 nc John Taolo Gaetsewe District Municipality 4263 3 5 nc Namakwa District Municipality 1403 0 0 nc Pixley ka Seme District Municipality 2820 2 5 nc Zwelentlanga Fatman Mgcawu District Municipality 4163 4 5 Northern Cape 20475 18 28 wc Cape Winelands District Municipality 14766 8 10 wc Central Karoo District Municipality 972 1 2 wc City of Cape Town Metropolitan Municipality 62637 35 54 wc Eden District Municipality 9339 6 10 wc Overberg District Municipality 3402 2 3 wc West Coast District Municipality 4102 1 1 Western Cape 95218 53 80
South Africa 905398 1037
1170 Areas marked in yellow are districts where there is a marked discrepancy.

40
Appendix 2: Detail of underlying causes 2017
Primary obstetric problems SA % Category % all maternal deaths Coincidental cause 38 N/A - MVA 12 31,6 - Other accidents 5 13,2 - Assault 4 10,5 - Other 17 44,7 Medical and surgical disorders 153 13,5 - Cardiac disease 50 32,7 - Endocrine 6 3,9 - GIT 10 6,5 - CNS 22 14,4 - Respiratory 20 13,1 - Haematological 7 4,6 - Genito-urinary 4 2,6 - Psychiatric 9 5,9 - Neoplasm 14 9,2 - Other 11 7,2 Non-pregnancy-related infections 283 25,0 - PCP pneumonia 45 15,9 - Other pneumonia 52 18,4 - TB 94 33,2 - UTI 2 0,7 - Appendicitis 3 1,1 - Malaria 6 2,1 - Cryptococcal meningitis 14 4,9 - Other meningitis 21 7,4 - Kaposi's sarcoma 4 1,4 - Hepatitis 3 1,1 - Gastroenteritis 12 4,2 - Wasting syndrome 5 1,8 - Other 22 7,8 Ectopic pregnancy 39 3,4 - Less than 20 weeks 38 97,4 - More than 20 weeks 1 2,6 Miscarriage 71 6,3 - Septic miscarriage 50 70,4 - Haemorrhage (non-traumatic) 13 18,3 - Uterine trauma 5 7,0 - Following legal TOP 3 4,2 Pregnancy-related sepsis 66 5,8 - Chorioamnionitis (ruptured membranes) 3 4,5 - Chorioamnionitis (intact membranes) 4 6,1 - Puerperal sepsis after NVD 33 50,0 - Puerperal sepsis after C/section 23 34,8 - Bowel trauma at C/section 3 4,5

41
Primary obstetric problems SA % Category % all maternal deaths Obstetric haemorrhage 176 15,5 - Abruption with hypertension 7 4,0 - Abruption without hypertension 12 6,8 - Placenta praevia 4 2,3 - Other APH not specified 3 1,7 - Ruptured uterus with previous c/s 6 3,4 - Ruptured uterus without previous c/s 10 5,7 - Retained placenta 12 6,8 - Morbidly adherent placenta 7 4,0 - Uterine atony 11 6,3 - Vaginal trauma 5 2,8 - Cervical trauma 4 2,3 - Inverted uterus 6 3,4 - Bleeding during Caesarean section 15 8,5 - Bleeding after Caesarean section 55 31,3 - Other PPH not specified 19 10,8 Hypertension 200 17,7 - Chronic hypertension 12 6,0 - Proteinuric hypertension 49 24,5 - Eclampsia 103 51,5 - HELLP 32 16,0 - Liver rupture 4 2,0 Anaesthetic complications 29 2,6 - General anaesthetic 5 17,2 - Epidural anaesthetic 2 6,9 - Spinal anaesthetic 22 75,9 Adverse drug reactions 10 0,9 - ARV medication 3 30,0 - TB medication 1 10,0 - Other medication 2 20,0 - Herbal medication 4 40,0 Embolism 34 3,0 - Pulmonary embolism 30 88,2 - Amniotic fluid embolism 4 11,8 Acute collapse - cause unknown 15 1,3 Miscellaneous 5 0,4 - Hyperemesis gravidarum 2 40,0 - Acute fatty liver 3 60,0 Unknown 51 4,5 - Death at home or outside health services 36 70,6 - No primary cause found 4 7,8 Total: 1132 100.0

42
Appendix 3: iMMR per district and province 2017
Organisation unit Live births DHIS MD NCCEMD iMMR DHIS iMMR NCCEMD 2014-2016
ec Alfred Nzo District Municipality 11510 6 6 52,13 52,13 64,41
ec Amathole District Municipality and Buffalo City 8228 19 21 230,92 255,23 145,74
ec Chris Hani District Municipality 10682 17 18 159,15 168,51 166,14
ec Joe Gqabi District Municipality 4560 2 2 43,86 43,86 109,66
ec Nelson Mandela Bay Municipality 18936 25 26 132,02 137,30 122,29 ec Oliver Tambo District Municipality 27208 61 65 224,20 238,90 210,07
ec Sarah Baartman District Municipality 5738 5 4 87,14 69,71 103,12
Eastern Cape 99927 135 142 135,10 142,10 148,47 fs Fezile Dabi District Municipality 6912 12 10 173,61 144,68 161,57
fs Lejweleputswa District Municipality 9313 10 11 107,38 118,11 197,00 fs Mangaung Metropolitan Municipality 14689 29 30 197,43 204,23 183,67
fs Thabo Mofutsanyana District Municipality 12853 14 17 108,92 132,26 166,25
fs Xhariep District Municipality 792 0 1 0,00 126,26 0
Free State 44559 65 69 145,87 154,85 174,63 gp City of Ekurhuleni Metropolitan Municipality 62545 71 68 113,52 108,72 131,98
gp City of Johannesburg Metropolitan Municipality 69985 71 55 101,45 78,59 121,99 gp City of Tshwane Metropolitan Municipality 51330 80 73 155,85 142,22 108
gp Sedibeng District Municipality 14707 19 14 129,19 95,19 137,01
gp West Rand District Municipality 15388 16 14 103,98 90,98 135,8
Gauteng 213955 257 224 120,12 104,69 128,62 kz Amajuba District Municipality 8370 12 14 143,37 167,26 128,04 kz eThekwini Metropolitan Municipality 55289 55 88 99,48 159,16 140,57
kz Harry Gwala District Municipality 7453 6 7 80,50 93,92 106,00
kz iLembe District Municipality 10288 9 9 87,48 87,48 95,21
kz King Cetshwayo District Municipality 17997 27 28 150,03 155,58 173,57
kz Ugu District Municipality 12368 11 12 88,94 97,02 115,28
kz uMgungundlovu District Municipality 15965 27 33 169,12 206,70 192,16 kz Umkhanyakude District Municipality 14866 11 14 73,99 94,17 59,69
kz Umzinyathi District Municipality 10412 8 9 76,83 86,44 57,54
kz Uthukela District Municipality 11231 13 13 115,75 115,75 170,77
kz Zululand District Municipality 16326 14 18 85,75 110,25 70,14
KwaZulu-Natal 180565 193 245 106,89 135,69 127,14

43
Organisation unit Live births DHIS MD NCCEMD iMMR DHIS iMMR NCCEMD 2014-2016
lp Capricorn District Municipality 26678 70 82 262,39 307,37 337,64 lp Mopani District Municipality 24232 26 28 107,30 115,55 147,36
lp Sekhukhune District Municipality 25018 15 28 59,96 111,92 147,96
lp Vhembe District Municipality 28824 23 22 79,79 76,33 86,06
lp Waterberg District Municipality 14411 16 21 111,03 145,72 105,1
Limpopo 119163 150 181 125,88 151,89 168,69 mp Ehlanzeni District Municipality 38496 41 59 106,50 153,26 129,52 mp Gert Sibande District Municipality 17738 22 23 124,03 129,67 107,12
mp Nkangala District Municipality 19387 34 36 175,38 185,69 167,98
Mpumalanga 75621 97 118 128,27 156,04 134,43 nw Bojanala Platinum District Municipality 20328 19 25 93,47 122,98 153,63
nw Dr Kenneth Kaunda District Municipality 12645 24 26 189,80 205,61 203,9 nw Dr Ruth Segomotsi Mompati District Municipality 8119 2 3 24,63 36,95 148,21
nw Ngaka Modiri Molema District Municipality 14823 24 29 161,91 195,64 186,51
North West 55915 69 83 123,40 148,44 172,17 nc Frances Baard District Municipality 7826 9 13 115,00 166,11 145,43
nc John Taolo Gaetsewe District Municipality 4263 3 5 70,37 117,29 115,32
nc Namakwa District Municipality 1403 0 0 0,00 0,00 88,05 nc Pixley ka Seme District Municipality 2820 2 5 70,92 177,30 102,42
nc Zwelentlanga Fatman Mgcawu District Municipality 4163 4 5 96,08 120,11 164,88
Northern Cape 20475 18 28 87,91 136,75 132,26 wc Cape Winelands District Municipality 14766 8 10 54,18 67,72 47,47
wc Central Karoo District Municipality 972 1 2 102,88 205,76 99,3 wc City of Cape Town Metropolitan Municipality 62637 35 54 55,88 86,21 73,21
wc Eden District Municipality 9339 6 10 64,25 107,08 89,71
wc Overberg District Municipality 3402 2 3 58,79 88,18 20,26
wc West Coast District Municipality 4102 1 1 24,38 24,38 51,66
Western Cape 95218 53 80 55,66 84,02 68,3 South Africa 905398 1037 1170 114,54 129,22 135,2720039

44
Appendix 4a: iMMR of provinces ranked from highest to lowest (Deaths during pregnancy, childbirth and puerperium)
Province Live births NCCEMD iMMR NCCEMD Mpumalanga 75621 118 156,04 Free State 44559 69 154,85 Limpopo 119163 181 151,89 North West 55915 83 148,44 Eastern Cape 99927 142 142,10 Northern Cape 20475 28 136,75 KwaZulu-Natal 180565 245 135,69 South Africa 905398 1222 134,97 cGauteng 213955 275 128,53 Western Cape 95218 80 84,02

45
Appendix 4b: iMMR of districts ranked from highest to lowest (Deaths during pregnancy, childbirth and puerperium)
Organisation unit Live births Maternal
deaths NCCEMD
iMMR NCCEMD
lp Capricorn District Municipality 26678 82 307,37 ec Amathole District Municipality and Buffalo City 8228 21 255,23 ec Oliver Tambo District Municipality 27208 65 238,90 kz uMgungundlovu District Municipality 15965 33 206,70 wc Central Karoo District Municipality 972 2 205,76 nw Dr Kenneth Kaunda District Municipality 12645 26 205,61 fs Mangaung Metropolitan Municipality 14689 30 204,23 nw Ngaka Modiri Molema District Municipality 14823 29 195,64 mp Nkangala District Municipality 19387 36 185,69 nc Pixley ka Seme District Municipality 2820 5 177,30 ec Chris Hani District Municipality 10682 18 168,51 kz Amajuba District Municipality 8370 14 167,26 nc Frances Baard District Municipality 7826 13 166,11 kz eThekwini Metropolitan Municipality 55289 88 159,16 kz King Cetshwayo District Municipality 17997 28 155,58 mp Ehlanzeni District Municipality 38496 59 153,26 lp Waterberg District Municipality 14411 21 145,72 fs Fezile Dabi District Municipality 6912 10 144,68 gp City of Tshwane Metropolitan Municipality 51330 73 142,22 ec Nelson Mandela Bay Municipality 18936 26 137,30 fs Thabo Mofutsanyana District Municipality 12853 17 132,26 mp Gert Sibande District Municipality 17738 23 129,67 fs Xhariep District Municipality 792 1 126,26 nw Bojanala Platinum District Municipality 20328 25 122,98 nc Zwelentlanga Fatman Mgcawu District Municipality 4163 5 120,11 fs Lejweleputswa District Municipality 9313 11 118,11 nc John Taolo Gaetsewe District Municipality 4263 5 117,29 kz Uthukela District Municipality 11231 13 115,75 lp Mopani District Municipality 24232 28 115,55 lp Sekhukhune District Municipality 25018 28 111,92 kz Zululand District Municipality 16326 18 110,25 gp City of Ekurhuleni Metropolitan Municipality 62545 68 108,72 wc Eden District Municipality 9339 10 107,08 kz Ugu District Municipality 12368 12 97,02 gp Sedibeng District Municipality 14707 14 95,19 kz Umkhanyakude District Municipality 14866 14 94,17 kz Harry Gwala District Municipality 7453 7 93,92 gp West Rand District Municipality 15388 14 90,98 wc Overberg District Municipality 3402 3 88,18 kz iLembe District Municipality 10288 9 87,48 kz Umzinyathi District Municipality 10412 9 86,44 wc City of Cape Town Metropolitan Municipality 62637 54 86,21 gp City of Johannesburg Metropolitan Municipality 69985 55 78,59 lp Vhembe District Municipality 28824 22 76,33 ec Sarah Baartman District Municipality 5738 4 69,71 wc Cape Winelands District Municipality 14766 10 67,72 ec Alfred Nzo District Municipality 11510 6 52,13 ec Joe Gqabi District Municipality 4560 2 43,86 nw Dr Ruth Segomotsi Mompati District Municipality 8119 3 36,95 wc West Coast District Municipality 4102 1 24,38 nc Namakwa District Municipality 1403 0 0,00

46
Appendix 5. Number of health care professional avoidable factors per level of care
HEALTH CARE PROFESSIONAL All M&S NPRI Ec Miscr PRS OH HT AR Emb AC
COMMUNITY HEALTH CENTRE - Managed at this level 502 57 127 13 15 29 87 108 11 14 11 - Avoidable factors identified 185 13 65 3 1 7 30 51 2 2 4 - No avoidable factors 284 37 53 10 10 18 54 55 9 12 7 - Lack of information 39 8 10 1 4 4 4 4 0 0 0 Assessable cases 463 49 117 12 11 25 83 104 11 14 11 % Avoidable factors 40,0 26,5 55,6 25,0 9,1 28,0 36,1 49,0 18,2 14,3 36,4
DISTRICT HOSPITAL - Managed at this level 583 70 153 21 37 32 87 104 23 12 10 - Avoidable factors identified 363 36 80 18 26 19 75 59 18 6 9 - No avoidable factors 197 30 69 2 7 13 9 41 4 6 1 - Lack of information 38 5 8 2 7 1 4 6 2 0 0 Assessable cases 545 65 145 19 30 31 83 98 21 12 10 % Avoidable factors 66,6 55,4 55,2 94,7 86,7 61,3 90,4 60,2 85,7 50,0 90,0
REGIONAL HOSPITAL - Managed at this level 474 60 134 15 30 31 67 92 4 12 3 - Avoidable factors identified 263 34 59 11 17 19 51 58 3 4 0 - No avoidable factors 193 22 71 4 11 12 15 31 1 8 1 - Lack of information 22 8 4 0 2 0 1 3 0 0 2 Assessable cases 452 52 130 15 28 31 66 89 4 12 1 % Avoidable factors 58,2 65,4 45,4 73,3 60,7 61,3 77,3 65,2 75,0 33,3 0,0
TERTIARY & ABOVE - Managed at this level 377 57 96 5 27 31 43 80 4 10 2 - Avoidable factors identified 157 18 31 4 14 16 22 37 3 5 1 - No avoidable factors 201 37 64 1 9 14 20 38 0 5 0 - Lack of information 22 2 3 0 4 1 2 5 1 0 1 Assessable cases 355 55 93 5 23 30 41 75 3 10 1 % Avoidable factors 44,2 32,7 33,3 80,0 60,9 53,3 53,7 49,3 100,0 50,0 100,0
PRIVATE HOSPITAL - Managed at this level 54 13 5 0 2 3 10 8 3 4 0 - Avoidable factors identified 35 8 2 0 2 2 9 6 1 2 0 - No avoidable factors 14 4 2 0 0 1 0 2 1 2 0 - Lack of information 6 1 1 0 0 0 2 0 1 0 0 Assessable cases 48 12 4 0 2 3 8 8 2 4 0 % Avoidable factors 72,9 66,7 50,0 100,0 66,7 112,5 75,0 50,0 50,0
M&S – Medical and surgical disorders; NPRI – Non-pregnancy related infections; Ec – Ectopic pregnancy; Misc – Miscarriage; PRS – Pregnancy related sepsis; HT – Hypertensive disorders in pregnancy; OH – Obstetric haemorrhage; AR – Anaesthetic related; Emb. – Embolism; AC – Acute collapse, cause unknown;

47
Section 2. Progress report on reducing deaths associated with caesarean delivery
Sue Fawcus
Introduction
In the fifth Saving Mothers report for maternal deaths 2011-2013, the problem of caesarean delivery (CD) associated maternal mortality was first highlighted with the iMMR for women having CD being three times higher than for vaginal delivery1. This finding was also noted in the sixth Saving Mothers report for 2014-20162,. In many of these deaths, the death may have been unrelated to the CD, for example a woman dying from eclampsia who had an uncomplicated CD or a women having postpartum cardiomyopathy who had delivered by CD. However, for a substantial number, the CD contributed to the death such as in women with sepsis or thromboembolism after CD; and in others caused the death such as in women with bleeding associated with CD (BLDACD) and those with anaesthetic complications. The steep increase in maternal deaths from BLDACD from 2002 to 2015 was analysed in the interim report for 2014-20153 and highlighted in an advocacy publication in the South African Medical journal titled ‘Maternal deaths a due to bleeding associated with Caesarean section: a national emergency’4. Following this alert, the NCCEMD introduced several initiatives to address the problem of CD safety and BLDACD:
• Organising a consultation on Minimum Standards for facilities to perform Safe CD which was compiled as a published document5 .
• Developing a Safe CD package which was incorporated into a separate ESMOE module, which included tools for accrediting facilities, surgeons and anaesthetic doctors for the performance of safe CD6.
• ESMOE training on PPH and Surgical skills expanded with the distribution of training videos on difficult CD6.
• Consultation with HPCSA to ensure performance of a minimum 10 CDs under supervision is strictly adhered to and documented in intern log book as a pre-requisite for certification
It is therefore important to review the 2017 data for any progress in reducing case fatality rates (CFR = number deaths from CD/total CDs x 100,000) and CFRs from BLDACD (BLDACD CFR = number deaths from BLDACD/total CDs x 100,000)

48
Figure 1 traces the number of maternal deaths due to BLDACD from 2008 to 2017 and figure 2 gives the Case Fatality Rate (CFR) for the same time period. The deaths peaked in 2012 but now seem to be levelling off.
Mortality associated with CD and BLDACD for 2017 Table one shows the national and provincial caesarean delivery rates, CD CFRs and BLDACD CFRs for 2017. For South Africa, the CFR for CD was 145.7 deaths per 100,000 CDs and for BLDACD it was 27.8. The national CD rate for SA is 27.8 % with the lowest rate in Limpopo (20.5%) and the highest in Kwazulu Natal (30.9%). It is disappointing to see that the CD rate continues to rise, almost 2% year on year. The CFR for CD and for bleeding associated with CD (BLDACD) are highest in Limpopo, Free State, Mpumulanga and North West, and lowest in Western Cape. The highest CFR for BLDACD is 69.4
0102030405060708090
100
08 09 10 11 12 13 14 15 16 17
Num
ber
Figure 1. Number maternal deaths due to BLDACD 2008-2017
During After Total BLDACD
05
1015202530354045
08 09 10 11 12 13 14 15 16 17
CFR/
1000
00 C
D
Year
Figure 2. Case Fatality Rate (CFR) for bleeding during or after caseasean delivery (BLDACD)

49
per 100,000 CDs in Limpopo with the lowest being 10.5 in the Western Cape, indicating a six fold difference. This reflects major inequity in the safety of CD between different provinces.
Table 1 Caesarean delivery rate and case fatality rate of caesarean delivery and bleeding during or after caesarean delivery
Province Live births CD CD rate (%) MD with CD BLDACD
CFR CD/100000
CFR BLDACD/100000
Eastern Cape 99927 29064 29,1 42 7 144,5 24,1 Free State 44559 13164 29,5 31 6 235,5 45,6 Gauteng 213955 62847 29,4 80 12 127,3 19,1 KwaZulu-Natal 180565 55734 30,9 79 10 141,7 17,9 Limpopo 119163 24487 20,5 51 17 208,3 69,4 Mpumalanga 75621 16786 22,2 32 7 190,6 41,7 North West 55915 13267 23,7 17 6 128,1 45,2 Northern Cape 20475 4471 21,8 5 1 111,8 22,4 Western Cape 95218 28561 30,0 25 3 87,5 10,5 South Africa 905398 248381 27,4 362 69 145,7 27,8
CD – Caesarean delivery; MD – Maternal Deaths; BLDACD – Bleeding during or after caesarean delivery; CFR – Case fatality rate expressed per 100,000 CDs The following tables and figures compare 2017 rates with the previous triennium for different provinces
Comparison of CD and BLDACD CFR for 2017 with previous triennium (2014-2016) Table 2 compares the 2017 data for the previous triennium per province . Table 2. Comparison CD rate and CFR for CD and BLDACD
CD rate CFR CD/100000 CFR BLDACD/100000 Province 2014-2016 2017 2014-2016 2017 2014-2016 2017 Eastern Cape 27,6 29,1 168,7 144,5 25,2 24,1 Free State 25,3 29,5 170,8 235,5 21,4 45,6 Gauteng 27,1 29,4 180,9 127,3 24,6 19,1 KwaZulu-Natal 30,5 30,9 136,8 141,7 18,5 17,9 Limpopo 18,8 20,5 242,9 208,3 70,8 69,4 Mpumalanga 18,9 22,2 242,4 190,6 76,1 41,7 North West 21,4 23,7 230,2 128,1 38,4 45,2 Northern Cape 20,9 21,8 185,9 111,8 44,6 22,4 Western Cape 29,2 30,0 88,8 87,5 15,6 10,5 South Africa 25,7 27,4 169,6 145,7 30,6 27,8
CD – Caesarean delivery; MD – Maternal Deaths; BLDACD – Bleeding during or after caesarean delivery; CFR – Case fatality rate expressed per 100,000CDs Table 2 shows there has been a slight increase in CD rates in all provinces and nationally. Importantly, the national CD CFR has decreased in 2017 compared to the previous triennium (169.6 to 145.7) although caution is needed when reviewing only one year’s data. Similarly the BLADCD CFR has decreased (30.6 to 27.8). The decline has occurred in all provinces except Free State where both CD CFR and BLDACD CFR have increased markedly, KZN where the CD CFR has increased slightly, and North West where the BLDACD CFR has increased slightly. The above findings are illustrated graphically in Figures 3, and 4.

50
Appendices 1- 6 give details and rank CD CFR and BLDACD CFR per district for 2017
Underlying causes of maternal deaths in women who had CD (N=356) The underlying causes of maternal death in women who had had a CD are shown in Table 3. Nationally, of the 356 deaths, 100 (28.1%) died due to obstetric haemorrhage , 95 (26.7%) from hypertension, 45(12.6%) from NPRI , 34 (9.6%) from Medical and surgical disorders, 27 (7.6%) died from pregnancy related sepsis, 24 (6.7%) from anaesthetic complications, and 16 (4.5%) from embolism. For the 174 (48.9%) CD deaths from Hypertension, NPRI, and M&S combined it is unlikely that the CD was the main contributor to the maternal death; whereas it is likely that the CD itself was contributory in the 167 (46.9%) deaths from OH, PRS, anaesthetic and embolism combined.
0
50
100
150
200
250
300
EC FS Gau KZN Lim Mpu NW NC WC SA
CFR/
1000
00 C
DFigure 3. Comparions of Case Fatality Rate of CD per
province: 2014-16 and 2017
CFR CD 2014-16 CFR CD 2017
01020304050607080
EC FS Gau KZN Lim Mpu NW NC WC SA
CFR/
1000
00 C
D
Figure 4. Comparions of Case Fatality Rate of Bleeding During or After CD per province: 2014-16 and 2017
CFR BLDACD 2014-16 CFR BLDACD 2017

51
Table 3. Underlying cause of death in women who had CD
DH RH TH NC Pvt SA
Medical and surgical disorders 4 8 6 9 7 34
Non-pregnancy-related infections 9 17 10 5 3 45
Ectopic pregnancy 0 0 0 0 0 0
Miscarriage 0 0 0 0 0 0
Pregnancy-related sepsis 2 11 6 8 0 27
Obstetric haemorrhage 26 38 21 7 7 100
Hypertension 5 32 35 21 1 95
Anaesthetic complications 16 2 2 2 2 24
Adverse drug reactions 0 0 0 1 0 1
Embolism 6 4 3 0 2 16
Acute collapse - cause unknown 0 2 0 0 0 3
Miscellaneous 0 2 0 0 0 2
Unknown 0 2 0 0 2 9
Total MD with CD 68 118 83 53 24 356
Number of CDs 92660 91123 27682 27509 ND 238974
Coincidental cause 1 1 2 1 0 6
DH – District hospital; RH – Regional Hospital; TH – Tertiary Hospital; NC – National Central Hospital; Pvt – Private hospital; SA – Total for South Africa; ND – No denominator Of the 176 deaths from obstetric haemorrhage, 76 were after vaginal delivery and 100 had a CD. Of these 100, 15 were from bleeding during CD and 55 after CD giving a total of 70 BLDACD deaths. This forms the largest proportion of OH deaths (39.8% ), and has increased as a proportion from the previous triennium, suggesting that the main reduction of OH deaths in 2017 has been from other sub-categories of OH. Comparing subcategories of OH in 2017 with the 2014-2016 data, it is found that the proportion of OH deaths from BLDACD increased from 34.95 to 39.8%, and PPH after vaginal delivery (atony ,trauma, retained placenta etc) increased from 32.1% to 36.4%. However the proportion of deaths due to Antepartum haemorrhage (abruptio placenta, placenta praevia, unspecified) decreased from 17.3% to 14.8%) and of note the proportion of ruptured uterus decreased from 15.1% to 9.1%) Table 4 shows the relative contribution of BLDACD death to CD deaths in different provinces. This ranges from 35.3% in North West and 33.3% in Limpopo provinces to 12% in Western Cape, with a national percentage of 19.1%; illustrating large inequity between provinces. These preventable deaths are therefore highest in the more rural provinces.
Table 4. Proportion of maternal deaths with CD due to BLDACD, per province
Province % CD deaths due BLDACD North West 35,3 Limpopo 33,3 Mpumalanga 21,9 Northern Cape 20,0 Free State 19,4 South Africa 19,1 Eastern Cape 16,7 Gauteng 15,0 KwaZulu-Natal 12,7 Western Cape 12,0

52
Level of care for CD and BLDACD deaths Table 3 shows the distribution of CD deaths by level of care for the death. There were 68 (19.1%) CD deaths at District hospitals( DH), 118 (33.1%) at Regional Hospitals (RH), 83 (23.3%) at Provincial Tertiary hospitals (PTH) and 53 (14.9%) at National Central hospitals (NC) and 24 (6.7%) in private hospitals. Figure 5 shows the CFR for CD at each level of care and by underlying cause. The corresponding CFRs for CDs (Deaths per 100,000 CDs) were: 73.4 in DH, 129.5 in RH, 299.8 in PTH, and 192.7 in NC. CFR could not be calculated for private hospitals due to lack of a denominator for total CDs. It is remarkable that the CFR for hypertensive diseases in pregnancy is concentrated at the tertiary and national central hospitals. It might be that the women were referred after the CD to the tertiary levels, but analysis of the avoidable factors for hypertensive diseases in pregnancy makes this unlikely. This aspect must be further investigated. Analysing CD CFRs in this way does not reflect the level of care at which the CD was performed. Many CDs were performed at DHs and the women subsequently referred to higher levels of care (RH,PTH,NC) where they died. A more meaningful indicator would be the CD CFR for the level of cares at which the CDs were performed.
If the BLDACD deaths are considered by level of care (Figure 6), it can be seen that they constitute a higher proportion of CD deaths at District hospitals.
0,00
20,00
40,00
60,00
80,00
100,00
120,00
140,00
All CD DH RH TH NC
CFR/
1000
00 C
D
Figure 5. Comparison of CFR for underlying causes per level of care
M&S NPRI PRS OH HT AR Emb AC

53
Avoidable factors for CD and BLDACD deaths For all causes of death nationally, the most frequently cited avoidable factors were lack of appropriately trained doctors and nurses; this was particularly marked at district hospitals where 31.9% cases had lack of appropriately trained doctors and 18.5% of nurses. Figure 7 shows administrative avoidable factors for BLDACD by level of care.
Lack of appropriately skilled staff for DH, RH and PTH are the most common problems cited, followed by lack of blood at DHs. Of note the provinces with the highest CD CFR (Limpopo ,Free state, Mpumulanga and North West) have the highest proportion of maternal deaths in which ‘lack of appropriately trained doctors and nurses’ was cited as an avoidable factor, see figure 8.
0,0
20,0
40,0
60,0
80,0
All CD DH RH TH NC Pvt
Perc
ent
Figure 6. Distribution of bleeding during and after CD of all CDs per level of care
During After
0,0
10,0
20,0
30,0
40,0
50,0
60,0
70,0
80,0
Transport Fac. toFac.
Delay(overburdened
service)
Lack ICU Lack Blood/prod. Lack skilledDoctors
Lack skillednurses
Perc
ent
Figure 7. Distribution of administrative AF for BLDACD per level of care
CHC & DH = 19 RH = 18 TH = 14

54
Health care provider avoidable factors are shown in Figure 9. Problem recognition (not making a proper diagnosis) is a frequently cited problem, most frequently at DHs. This refers to not recognising the severity of shock with the bleeding and/or identifying the correct cause of the bleeding. Substandard care (not following protocols) was cited in one third of all CD deaths for DHs, RHs and THs. A similar pattern is found in BLDACD deaths (see Figure 10). (The number next to each level are the number of cases managed at some point at that level of care. They need not have died at that level).
0,0
10,0
20,0
30,0
40,0
50,0
60,0
EC FS Gau KZN Lim Mpu NW NC WC SA
Perc
ent
Figure 8. Lack of appropriately trained staff per province
Doctors Nurses
0,05,0
10,015,020,025,030,035,040,045,0
Assessment Diagnosis Delay ref. Not referred Wrong Diag. Not followprotocol
Poormonitoring
Abn. Mon.no action
Perc
ent
Figure 9. Distribution of HCP AF in women who had a CD and died
CHC=156 DH=164 RH=150 TH=133

55
Discussion In discussing CD practices in the public sector in SA, it is important to consider both CD rates as well as CD safety. CD rates These are increasing year by year in the public sector which is concerning but at 27.4%, the CD rate is much lower than the alarmingly high rate of 67% in the private sector described in the sixth triennial report. The ‘Global Epidemic’ of rising CD rates in the last two decades, has been highlighted in a recent Lancet series7. CD rates vary by world region from 44.3% in Latin America and Caribbean region, to 4.1% in the west and central Africa region. This paper draws attention to the vast inequities in access to CDs with, for example South Sudan having a rate of only 0.6%. Such rates, below 5% are too low to save mothers’ and babys’ lives, whereas CD rates such as 58.1% in the Dominican republic (and the SA private sector) are too high to be medically justifiable. Various articles in the Lancet series, including papers by WHO and FIGO, make suggestions to reduce CD rates8,9 .These include promoting the midwifery model of care, second opinion for CS, respectful effective intrapartum care , external cephalic version for breech presentation in late pregnancy, appropriate assisted vaginal delivery and other interventions . CD without medical indication should be avoided ; it is associated with an MMR three times that of vaginal delivery10.
Given that the 2015 WHO statement shows that no further reduction in maternal or perinatal mortality occurs with CD rates greater than 15%, the public sector CD rate of 28% may be a bit high 11 . However if one considers an additional purpose of CD being to reduce MORBIDITY both for mother and baby (which was mentioned in the WHO statement), then the SA public sector rates may be appropriate. It is particularly important to address inequities in access to CD which could be related to long distances to and between facilities in the poorer rural provinces, or could relate to bottlenecks at regional and provincial tertiary hospitals due to long queues of women waiting for theatre (ie overburdened services) .
The higher education training schools and continuing staff education programmes such as ESMOE in SA must be active in training doctor/midwife teams in: Respectful maternity care, more
0,0
10,0
20,0
30,0
40,0
50,0
60,0
70,0
Assessment Diagnosis Delay ref. Not referred Wrong Diag. Not followprotocol
Poormonitoring
Abn. Mon.no action
Perc
ent
Figure 10. Comparison of AF health care professionals for BLDACD per level of care
CHC=30 DH=32 RH=28 TH=18

56
appropriate management of labour, assisted vaginal deliveries, CTG training, second opinion for CS etc; in an attempt to reduce or stabilise CS rates without compromising maternal and fetal outcome.
CD safety Although, this is only one year’s data, it is encouraging that there is a trend towards reduction in CD and BLDACD case fatality rates across most provinces. The decline in CD CFR could be due to better treatment of primary conditions such as eclampsia, heart disease, HIV since these are the underlying causes in a large proportion of the CD deaths. The decline in BLDACD CFR could be due to the targeted interventions on BLDACD described in the introduction A major CONCERN is the wide variations between provinces (and mirrored in districts). The provinces with highest rates are the more rural provinces with greatest socioeconomic disadvantaged and weakest health systems (Limpopo, Mpumulanga, North West, Free State). Of note, lack of appropriately trained staff is cited most frequently in these provinces, indicating that socioeconomic disadvantage and weak health systems is accompanied by lack of skilled staff compared to other provinces with better outcomes. Can the NHI process be harnessed to assist in such provinces or is it only designed to assist where heath systems are strongest? Problem recognition/diagnosis most frequent avoidable factor at DHs, whereas substandard care/not following protocols are common at DH, RH/ and TH. This indicated the need for ongoing ESMOE and skills training which should include higher education training institutions as well as senior clinical staff and District specialist teams12,13. In addition in situations where CDs have become complicated (e.g. from BLDACD or eclampsia) that the emergency transport enables the women to arrive alive at a higher level of care. This can be facilitated by working with Emergency Medical services and the introduction of the NASG ( Non-pneumatic anti- shock garment) for shocked patients being referred from DHs14. The process of accrediting facilities for adherence to minimum standards for Safe CD has occurred in FS, KZN and EC. It still has not occurred in most provinces, including Western Cape which has the lowest CFRs from CD and BLDACD. It is important that the Safe CD package and process of accrediting facilities for safety with rationalisation of services where appropriate, continues. It will need to be accompanied, when completed, by an evaluation of its impact Summary of recommendations. 1. Implement safe CD practices: thromboprophylaxis; antibiotics, PPH management 2. Continue ESMOE training combined with in-reach/out-reach for surgical/anaesthetic training 3. Complete implementation of Safe CD package with a final evaluation 4. Develop auditable indicators for CD safety e.g. CD CFR per district/facility, BLDACD per
district/facility; and monitor CD rates 5. Address inequities between provinces; can NHI be harnessed to assist by providing skills
training? 6. Implement interventions to reduce CD rates (e.g. Second opinion for CD, respectful and effective
midwife led intrapartum care, assisted vaginal delivery where appropriate)
References 1. Gebhard GS, Fawcus S, Moodley J, Farina Z. Maternal death and caesarean section in South Africa
: Results from the 2011-2013 Saving Mothers Report of the National Committee for Confidential Enquiries into Maternal Deaths. SAMJ 2015; 105(4): 287-291.
2. Saving Mothers 2014-2016. The seventh report of the National Committee for Confidential Enquiry into Maternal Deaths in South Africa. Short report. Department Health, Pretoria 2017

57
3. NCCEMD. Saving Mothers, interim report 2014 and interim report 2015 of the National Committee for Confidential Enquiry into Maternal Deaths in South Africa. DOH, Pretoria.
4. Fawcus S, Pattinson RB, Moodley J, Schoon MG, Mhlanga RE, et al (NCCEMD).Maternal deaths from bleeding associated with Caesarean delivery: a national emergency. SAMJ 2016; 5: 472-476. OI:10.7196/SAMJ.2016.v.106i5.10821
5. N. Moran for NCCEMD. Setting minimum standards for caesarean delivery in South Africa. O&G Forum 2015; 3: 41-44
6. Essential Steps in Managing Obstetric Emergencies (ESMOE) training policy. www.ESMOE.co.za 7. Boerma T, Ronsmans T, Melesse D, Barros A, Barros F, Juan L, Moller AB et al . Global
epidemiology of use of and disparities in caesarean sections Lancet 2018; 392: 1341–48 8. Betrán AP, Temmerman M, Kingdon C, Mohiddin A, Opiyo N, Torloni M et al .Interventions to
reduce unnecessary caesarean sections in healthy women and babies.Lancet 2018; 392: 1358–68
9. Visser G, Ayres-de-Campos D, Barnea R, ,de Bernis L, Di Renzo G,Vidarte M et al . FIGO position paper: how to stop the Caesarean section epidemic. Lancet 2018; 392: 1286-7
10. Souza JP, Gulmezoglu AM, Lumbiganon P, Laopaiboom M, Carroli G, Fawole B, Ruyan P, the WHO Global survey on maternal and perinatal health research group. Caesarean section without medical indication is associated with an increased risk of adverse short-term maternal outcomes: the 2004-2008 WHO Global survey on Maternal and Perinatal Health. BMC Medicine 2010; 8: 71
11. World Health Organisation. WHO statement on Caesarean section WHO/RHR/15.02 WHO, Geneva 2015WHO
12. NCCEMD. A Monograph of the Management of Postpartum Haemorrhage. National Department of Health, Pretoria 2010.
13. NCCEMD. A monograph on Caesarean section. National Department of Health, Pretoria 2013. 14. Pileggi-Castro C, Nogueira-Pileggi V, Tuncalp O, Oladapo O, Vogel JP, Souza JP. Non-pneumatic
anti-shock garment for improving maternal survival following severe postpartum haemorrhage : a systematic review. Reproductive Health 2015; 12: 28. DOI 10.11861s2978-015-0012-

58
Appendix 1: Caesarean delivery and BLDACD CFR per province and district
Organisation unit Live births CD CD rate (%) MD with CD BLDACD CFR
CD/100000
CFR
BLDACD/100000
ec Alfred Nzo District Municipality 11510 2258 19,6 1 1 44,3 44,3 ec Amathole District Municipality and ec Buffalo City Metropolitan Municipality
21293 6383 30,0 8 0 125,3 0,0
ec Chris Hani District Municipality 10682 2373 22,2 5 1 210,7 42,1
ec Joe Gqabi District Municipality 4560 519 11,4 0 0 0,0 0,0
ec Nelson Mandela Bay Municipality 18936 7462 39,4 7 1 93,8 13,4
ec Oliver Tambo District Municipality 27208 8522 31,3 19 4 223,0 46,9
ec Sarah Baartman District Municipality 5738 1547 27,0 2 0 129,3 0,0
Eastern Cape 99927 29064 29,1 42 7 144,5 24,1 fs Fezile Dabi District Municipality 6912 1642 23,8 3 1 182,7 60,9
fs Lejweleputswa District Municipality 9313 2717 29,2 6 0 220,8 0,0
fs Mangaung Metropolitan Municipality 14689 5568 37,9 15 1 269,4 18,0
fs Thabo Mofutsanyana District Municipality 12853 3237 25,2 7 4 216,2 123,6
fs Xhariep District Municipality 792 0 0,0 0 0 0,0
Free State 44559 13164 29,5 31 6 235,5 45,6 gp City of Ekurhuleni Metropolitan Municipality 62545 17484 28,0 27 5 154,4 28,6
gp City of Johannesburg Metropolitan Municipality 69985 23025 32,9 24 2 104,2 8,7
gp City of Tshwane Metropolitan Municipality 51330 14563 28,4 18 3 123,6 20,6
gp Sedibeng District Municipality 14707 3981 27,1 4 0 100,5 0,0
gp West Rand District Municipality 15388 3794 24,7 7 2 184,5 52,7 Gauteng 213955 62847 29,4 80 12 127,3 19,1 kz Amajuba District Municipality 8370 2802 33,5 4 0 142,8 0,0
kz eThekwini Metropolitan Municipality 55289 18813 34,0 26 2 138,2 10,6
kz Harry Gwala District Municipality 7453 1764 23,7 1 0 56,7 0,0
kz iLembe District Municipality 10288 3370 32,8 3 0 89,0 0,0
kz King Cetshwayo District Municipality 17997 5886 32,7 10 2 169,9 34,0 kz Ugu District Municipality 12368 4756 38,5 7 1 147,2 21,0
kz uMgungundlovu District Municipality 15965 6277 39,3 11 0 175,2 0,0
kz Umkhanyakude District Municipality 14866 2732 18,4 3 1 109,8 36,6
kz Umzinyathi District Municipality 10412 2851 27,4 4 2 140,3 70,2
kz Uthukela District Municipality 11231 2993 26,6 4 1 133,6 33,4
kz Zululand District Municipality 16326 3490 21,4 6 1 171,9 28,7 KwaZulu-Natal 180565 55734 30,9 79 10 141,7 17,9

59
Organisation unit Live births CD CD rate (%) MD with CD BLDACD CFR
CD/100000
CFR
BLDACD/100000
lp Capricorn District Municipality 26678 6602 24,7 26 8 393,8 121,2 lp Mopani District Municipality 24232 4609 19,0 7 4 151,9 86,8
lp Sekhukhune District Municipality 25018 4913 19,6 4 0 81,4 0,0
lp Vhembe District Municipality 28824 5035 17,5 8 3 158,9 59,6
lp Waterberg District Municipality 14411 3328 23,1 6 2 180,3 60,1
Limpopo 119163 24487 20,5 51 17 208,3 69,4 mp Ehlanzeni District Municipality 38496 8404 21,8 11 3 130,9 35,7 mp Gert Sibande District Municipality 17738 4383 24,7 7 2 159,7 45,6
mp Nkangala District Municipality 19387 3999 20,6 14 2 350,1 50,0
Mpumalanga 75621 16786 22,2 32 7 190,6 41,7 nw Bojanala Platinum District Municipality 20328 4594 22,6 4 0 87,1 0,0
nw Dr Kenneth Kaunda District Municipality 12645 3763 29,8 6 3 159,4 79,7 nw Dr Ruth Segomotsi Mompati District Municipality 8119 1560 19,2 1 0 64,1 0,0
nw Ngaka Modiri Molema District Municipality 14823 3350 22,6 6 3 179,1 89,6
North West 55915 13267 23,7 17 6 128,1 45,2 nc Frances Baard District Municipality 7826 2347 30,0 3 0 127,8 0,0
nc John Taolo Gaetsewe District Municipality 4263 734 17,2 0 0 0,0 0,0
nc Namakwa District Municipality 1403 223 15,9 0 0 0,0 0,0 nc Pixley ka Seme District Municipality 2820 346 12,3 0 0 0,0 0,0
nc Zwelentlanga Fatman Mgcawu District Municipality 4163 821 19,7 2 1 243,6 121,8
Northern Cape 20475 4471 21,8 5 1 111,8 22,4 wc Cape Winelands District Municipality 14766 4606 31,2 3 1 65,1 21,7
wc Central Karoo District Municipality 972 196 20,2 1 0 510,2 0,0 wc City of Cape Town Metropolitan Municipality 62637 19366 30,9 18 2 92,9 10,3
wc Eden District Municipality 9339 2977 31,9 3 0 100,8 0,0
wc Overberg District Municipality 3402 607 17,8 0 0 0,0 0,0
wc West Coast District Municipality 4102 809 19,7 0 0 0,0 0,0
Western Cape 95218 28561 30,0 25 3 87,5 10,5 South Africa 905398 248381 27,4 362 69 145,7 27,8

60
Appendix 2: Ranking of Caesarean delivery CFR per province
Province CD CD rate (%) MD with CD CFR CD/100000
Free State 13164 29,5 31 235,5
Limpopo 24487 20,5 51 208,3
Mpumalanga 16786 22,2 32 190,6
South Africa 248381 27,4 362 145,7
Eastern Cape 29064 29,1 42 144,5
KwaZulu-Natal 55734 30,9 79 141,7
North West 13267 23,7 17 128,1
Gauteng 62847 29,4 80 127,3
Northern Cape 4471 21,8 5 111,8
Western Cape 28561 30,0 25 87,5

61
Appendix 3: Ranking of CD CFR per district
Organisation unit CD CD rate (%) MD with CD CFR
CD/100000
wc Central Karoo District Municipality 196 20,2 1 510,2
lp Capricorn District Municipality 6602 24,7 26 393,8
mp Nkangala District Municipality 3999 20,6 14 350,1
fs Mangaung Metropolitan Municipality 5568 37,9 15 269,4
nc Zwelentlanga Fatman Mgcawu District Municipality 821 19,7 2 243,6
ec Oliver Tambo District Municipality 8522 31,3 19 223,0
fs Lejweleputswa District Municipality 2717 29,2 6 220,8
fs Thabo Mofutsanyana District Municipality 3237 25,2 7 216,2
ec Chris Hani District Municipality 2373 22,2 5 210,7
gp West Rand District Municipality 3794 24,7 7 184,5
fs Fezile Dabi District Municipality 1642 23,8 3 182,7
lp Waterberg District Municipality 3328 23,1 6 180,3
nw Ngaka Modiri Molema District Municipality 3350 22,6 6 179,1
kz uMgungundlovu District Municipality 6277 39,3 11 175,2
kz Zululand District Municipality 3490 21,4 6 171,9
kz King Cetshwayo District Municipality 5886 32,7 10 169,9
mp Gert Sibande District Municipality 4383 24,7 7 159,7
nw Dr Kenneth Kaunda District Municipality 3763 29,8 6 159,4
lp Vhembe District Municipality 5035 17,5 8 158,9
gp City of Ekurhuleni Metropolitan Municipality 17484 28,0 27 154,4
lp Mopani District Municipality 4609 19,0 7 151,9
kz Ugu District Municipality 4756 38,5 7 147,2
kz Amajuba District Municipality 2802 33,5 4 142,8
kz Umzinyathi District Municipality 2851 27,4 4 140,3
kz eThekwini Metropolitan Municipality 18813 34,0 26 138,2
kz Uthukela District Municipality 2993 26,6 4 133,6
mp Ehlanzeni District Municipality 8404 21,8 11 130,9
ec Sarah Baartman District Municipality 1547 27,0 2 129,3
nc Frances Baard District Municipality 2347 30,0 3 127,8
ec Amathole District Municipality and ec Buffalo City Metropolitan
Municipality 6383 30,0 8 125,3
gp City of Tshwane Metropolitan Municipality 14563 28,4 18 123,6
kz Umkhanyakude District Municipality 2732 18,4 3 109,8
gp City of Johannesburg Metropolitan Municipality 23025 32,9 24 104,2
wc Eden District Municipality 2977 31,9 3 100,8
gp Sedibeng District Municipality 3981 27,1 4 100,5
ec Nelson Mandela Bay Municipality 7462 39,4 7 93,8
wc City of Cape Town Metropolitan Municipality 19366 30,9 18 92,9
kz iLembe District Municipality 3370 32,8 3 89,0
nw Bojanala Platinum District Municipality 4594 22,6 4 87,1
lp Sekhukhune District Municipality 4913 19,6 4 81,4
wc Cape Winelands District Municipality 4606 31,2 3 65,1
nw Dr Ruth Segomotsi Mompati District Municipality 1560 19,2 1 64,1
kz Harry Gwala District Municipality 1764 23,7 1 56,7
ec Alfred Nzo District Municipality 2258 19,6 1 44,3
ec Joe Gqabi District Municipality 519 11,4 0 0,0
fs Xhariep District Municipality 0 0,0 0 0,0
nc John Taolo Gaetsewe District Municipality 734 17,2 0 0,0
nc Namakwa District Municipality 223 15,9 0 0,0
nc Pixley ka Seme District Municipality 346 12,3 0 0,0
wc Overberg District Municipality 607 17,8 0 0,0
wc West Coast District Municipality 809 19,7 0 0,0

62
Appendix 4: Ranking of BLDACD CFR per province
Province CD CD rate (%) BLDACD CFR BLDACD/100000
Limpopo 24487 20,5 17 69,4
Free State 13164 29,5 6 45,6
North West 13267 23,7 6 45,2
Mpumalanga 16786 22,2 7 41,7
South Africa 248381 27,4 69 27,8
Eastern Cape 29064 29,1 7 24,1
Northern Cape 4471 21,8 1 22,4
Gauteng 62847 29,4 12 19,1
KwaZulu-Natal 55734 30,9 10 17,9
Western Cape 28561 30,0 3 10,5

63
Appendix 5 Ranking of BLDACD CFR per district
Organisation unit
CD CD rate (%) BLDACD CFR BLDACD/100000
fs Thabo Mofutsanyana District Municipality 3237 25,2 4 123,57
nc Zwelentlanga Fatman Mgcawu District Municipality 821 19,7 1 121,80
lp Capricorn District Municipality 6602 24,7 8 121,18
nw Ngaka Modiri Molema District Municipality 3350 22,6 3 89,55
lp Mopani District Municipality 4609 19,0 4 86,79
nw Dr Kenneth Kaunda District Municipality 3763 29,8 3 79,72
kz Umzinyathi District Municipality 2851 27,4 2 70,15
fs Fezile Dabi District Municipality 1642 23,8 1 60,90
lp Waterberg District Municipality 3328 23,1 2 60,10
lp Vhembe District Municipality 5035 17,5 3 59,58
gp West Rand District Municipality 3794 24,7 2 52,71
mp Nkangala District Municipality 3999 20,6 2 50,01
ec Oliver Tambo District Municipality 8522 31,3 4 46,94
mp Gert Sibande District Municipality 4383 24,7 2 45,63
ec Alfred Nzo District Municipality 2258 19,6 1 44,29
ec Chris Hani District Municipality 2373 22,2 1 42,14
kz Umkhanyakude District Municipality 2732 18,4 1 36,60
mp Ehlanzeni District Municipality 8404 21,8 3 35,70
kz King Cetshwayo District Municipality 5886 32,7 2 33,98
kz Uthukela District Municipality 2993 26,6 1 33,41
kz Zululand District Municipality 3490 21,4 1 28,65
gp City of Ekurhuleni Metropolitan Municipality 17484 28,0 5 28,60
wc Cape Winelands District Municipality 4606 31,2 1 21,71
kz Ugu District Municipality 4756 38,5 1 21,03
gp City of Tshwane Metropolitan Municipality 14563 28,4 3 20,60
fs Mangaung Metropolitan Municipality 5568 37,9 1 17,96
ec Nelson Mandela Bay Municipality 7462 39,4 1 13,40
kz eThekwini Metropolitan Municipality 18813 34,0 2 10,63
wc City of Cape Town Metropolitan Municipality 19366 30,9 2 10,33
gp City of Johannesburg Metropolitan Municipality 23025 32,9 2 8,69
ec Amathole District Municipality and ec Buffalo City Metropolitan
Municipality 6383 30,0 0 0,00
ec Joe Gqabi District Municipality 519 11,4 0 0,00
ec Sarah Baartman District Municipality 1547 27,0 0 0,00
fs Lejweleputswa District Municipality 2717 29,2 0 0,00
gp Sedibeng District Municipality 3981 27,1 0 0,00
kz Amajuba District Municipality 2802 33,5 0 0,00
kz Harry Gwala District Municipality 1764 23,7 0 0,00
kz iLembe District Municipality 3370 32,8 0 0,00
kz uMgungundlovu District Municipality 6277 39,3 0 0,00
lp Sekhukhune District Municipality 4913 19,6 0 0,00
nw Bojanala Platinum District Municipality 4594 22,6 0 0,00
nw Dr Ruth Segomotsi Mompati District Municipality 1560 19,2 0 0,00
nc Frances Baard District Municipality 2347 30,0 0 0,00
nc John Taolo Gaetsewe District Municipality 734 17,2 0 0,00
nc Namakwa District Municipality 223 15,9 0 0,00
nc Pixley ka Seme District Municipality 346 12,3 0 0,00
wc Central Karoo District Municipality 196 20,2 0 0,00
wc Eden District Municipality 2977 31,9 0 0,00
wc Overberg District Municipality 607 17,8 0 0,00
wc West Coast District Municipality 809 19,7 0 0,00
0fs Xhariep District Municipality 0 0,0 0

64
Appendix 6: Proportion of maternal deaths with CD due to BLDACD, per province and
district
Province % CD deaths due BLDACD
North West 35,3
Limpopo 33,3
Mpumalanga 21,9
Northern Cape 20,0
Free State 19,4
South Africa 19,1
Eastern Cape 16,7
Gauteng 15,0
KwaZulu-Natal 12,7
Western Cape 12,0
District % CD deaths due BLDACD
ec Alfred Nzo District Municipality 100,0
fs Thabo Mofutsanyana District Municipality 57,1
lp Mopani District Municipality 57,1
kz Umzinyathi District Municipality 50,0
nc Zwelentlanga Fatman Mgcawu District Municipality 50,0
nw Dr Kenneth Kaunda District Municipality 50,0
nw Ngaka Modiri Molema District Municipality 50,0
lp Vhembe District Municipality 37,5
kz Umkhanyakude District Municipality 33,3
lp Waterberg District Municipality 33,3
wc Cape Winelands District Municipality 33,3
fs Fezile Dabi District Municipality 33,3
lp Capricorn District Municipality 30,8
gp West Rand District Municipality 28,6
mp Gert Sibande District Municipality 28,6
mp Ehlanzeni District Municipality 27,3
kz Uthukela District Municipality 25,0
ec Oliver Tambo District Municipality 21,1
ec Chris Hani District Municipality 20,0
kz King Cetshwayo District Municipality 20,0
gp City of Ekurhuleni Metropolitan Municipality 18,5
gp City of Tshwane Metropolitan Municipality 16,7
kz Zululand District Municipality 16,7
mp Nkangala District Municipality 14,3
ec Nelson Mandela Bay Municipality 14,3
kz Ugu District Municipality 14,3
wc City of Cape Town Metropolitan Municipality 11,1
gp City of Johannesburg Metropolitan Municipality 8,3
kz eThekwini Metropolitan Municipality 7,7
fs Mangaung Metropolitan Municipality 6,7

65
Section 3. Managing Hypertensive
Disorders in Pregnancy (HDP)
J Moodley, P Soma-Pillay, R Pattinson
Introduction Hypertensive disorders of pregnancy (HDP) are the commonest direct cause of maternal mortality
and account for 14.8% of all maternal deaths in South Africa. Deaths from hypertensive disorders of
pregnancy occur in all categories of hypertensive disorders with eclampsia and pre-eclampsia being
the commonest final causes of deaths. The main causes leading to death were cerebral hemorrhage
and pulmonary oedema; therefore focus should be placed on the immediate lowering of acute of
severe hypertension and a policy of restrictive of fluid loading. Such steps will reduce the percentage
of preventable deaths, assessed to be approximately 70% in the period 2014-20161.
Unfortunately no progress has been made in the last decade in reducing the deaths due to HDP
(Figure 1)
The table 1 below illustrates that almost 153 (78,5%) maternal deaths due to HDP were at levels which
are supposed to have specialist care.
0
10
20
30
40
50
60
70
HT OH Ec Misc PRS AR Emb AC NPRI M&S Unk
iMM
R/1
0000
0 liv
e bi
rths
Figure 1. Comparison iMMR per underlying cause from 2011-2017
2011
2012
2013*
2014
2015
2016*
2017#

66
Figure 2 below illustrates the high iMMR due to hypertension in the regional, tertiary and national
central hospitals.
Almost 75% of the maternal deaths due to HDP were thought to be potentially preventable (Figure
3). This percentage has increased over the last few years.
Primary obstetric problem
CHCDistrict hospital
Regional hospital
Tertiary hospital
Nat.Central hospital
Private hospital
Total
Medical and surgical disorders 5 29 42 30 27 10 143Non-pregnancy-related infections 4 66 112 56 34 4 276Ectopic pregnancy 1 18 11 5 2 0 37Miscarriage 0 19 24 20 7 0 70Pregnancy-related sepsis 1 11 19 21 11 1 64Obstetric haemorrhage 7 52 59 32 11 9 170Hypertensive Diseases of Pregnancy 5 34 65 50 38 3 195Anaesthetic complications 0 19 3 3 2 2 29Adverse drug reactions 0 1 1 5 3 0 10Embolism 3 7 9 8 1 3 31Acute collapse - cause unknown 2 7 2 1 0 0 12Miscellaneous 0 0 2 2 1 0 5Unknown 3 5 6 0 0 3 17Maternal deaths 31 268 355 233 137 35 1059
Table 1. Comparison of the number of maternal deaths per level of care and its distribution (Excludes deaths outside facilities and coincidental deaths: 2017)
0,00
10,00
20,00
30,00
40,00
50,00
60,00
70,00
CHC DH RH PTH NCH
iMM
R/10
0000
live
birt
hs
Figure 2. Comparison of iMMR per level of care and underlying causes
M&S NPRI Ec Miscr. PRS OH HT AR

67
Figure 4 below illustrates that HDP is now almost the biggest contributor to potentially preventable
deaths.
Figure 5 below illustrates how HDP have increased in importance as potentially preventable deaths
as management of the two other major conditions non-pregnancy related infections and obstetric
haemorrhage has improved.
0,0
10,0
20,0
30,0
40,0
50,0
60,0
70,0
80,0
90,0
100,0
% potentially preventable deaths
Perc
ent
Figure 3. Proportion of potentially preventable deaths per disease category
M&S NPRI Ec Miscr. PRS OH HT AR Emb AC All MD
0,0
5,0
10,0
15,0
20,0
25,0
% Potentially preventable deaths
Perc
ent
Figure 4. Contribution of underlying causes to potentially preventable deaths
M&S NPRI Ec Miscr. PRS OH HT AR Emb AC

68
Figure 6 below shows that not only has the proportion of potentially preventable deaths increased,
but the actual iMMR has also increased, contrary to all other underlying causes
Figure 7below illustrates at what level of care were there avoidable factors. The MaMMAS
programme allows evaluation of the quality care at each level of care a woman who subsequently
died passed through. There were between 50% and 65% of avoidable factors at each level of care.
0,0
5,0
10,0
15,0
20,0
25,0
30,0
35,0
NPRI OH HT M&S
Perc
ent
Figure 5. Distribution of potentially preventable deaths 2008-2018
2008-20102011-20132014-20162017
0,0
5,0
10,0
15,0
20,0
25,0
30,0
35,0
2008-2010 2011-2013 2014-2016 2017
Perc
ent
Figure 6. Distribution of potential preventable deaths 2008-2017
NPRIOHHTM&S

69
Figure 8 below gives detail on what the health care professionals avoidable factors were. The
numbers in brackets next to each level of care indicate the number of women who subsequently
died due to HDP were care for at least part of the time before her death. The major problems were
lack or proper assessment and making a diagnosis at the primary level of care, but not adhering to
standard protocols was the biggest problems at regional, tertiary and national central hospitals.
Figure 9 below gives more detail on the distribution of cases where there were avoidable factors at
that level of care. Assessment and diagnosis were again the problems at the primary level of care,
but not adhering to standard protocols was the biggest problem and this was at the hospitals where
a specialist should be present.
0,0
10,0
20,0
30,0
40,0
50,0
60,0
70,0
80,0
90,0
100,0
All M&S NPRI Miscr PRS OH HT
Percen
tFigure 7. Proportion of avoidable factors per level of care for common conditions
CHC s District Hospital Regional Hospital Tertiary Hospital
0,0
5,0
10,0
15,0
20,0
25,0
30,0
35,0
40,0
45,0
Assessment Diagnosis Delay ref. Not referred Wrong Diag. Not followprotocol
Poormonitoring
Abn. Mon. noaction
Perc
ent
Figure 8. Distribution of avoidable factors per level of care for all assessable hypertensive cases managed at that level
CHC (n=108) DH (n=104) RH (n=92) TH (n=80)

70
From the above documentation it is clear that management of HDP is a problem at all levels of care.
See section 4 for monitoring and evaluation of the implementation of Basic Antenatal Care (BANC)
Plus. It is clear for this that more women are being detected with hypertension in pregnancy, but
that this has not translated into a reduction in perinatal mortality. The main reason for this is that a
number of women detected with hypertension in pregnancy are not being managed appropriately.
For these reasons the management of HDP guidelines were reviewed and re-written according to
the AGREE II format to ensure that they are comprehensive and deal with all levels of care and
specifically concentrate on the problems identified with the care outlined above.
Scope and purpose of new management guidelines for HDP • Overall objective is to improve the management of women with hypertensive diseases in
pregnancy and thereby reduce the mortality and mortality rates.
• The health question covered specifically is pregnant women with hypertension and all its
variants at all levels of care
• The target population is pregnant women with hypertension at every level of care.
Methods 1. Stakeholder involvement
a. The guideline development included individuals from the National Department of
Health (NDoH), the Colleges of Obstetrics and Gynaecology, Anaesthesiology and
family medicine, the Society of Obstetrics and Gynaecology, the Anaesthetic Society
of South Africa, the Academy of Family Practice, Departments of Obstetrics and
Gynaecology from the medical schools, the Society of Midwives in South Africa, the
Priorities in Perinatal Care Association, the Rural Doctors Association of South Africa.
b. Target users are health care professionals at primary health care clinics, district,
regional and tertiary hospitals dealing with pregnant women
2. Rigour of development
The recommendations from this guideline are based on available literature and expert
opinion. Unfortunately there is a lack of quality randomised controlled trials in the field of
0,0
10,0
20,0
30,0
40,0
50,0
60,0
70,0
80,0
Assessment Diagnosis Delay ref. Not referred Wrong Diag. Not followprotocol
Poor monitoring Abn. Mon. noaction
Perc
ent
Figure 9. Distribution of avoidable factors per level of care for health care professionals in managing hypertensive diseases of pregnancy
CHC DH RH TH

71
hypertension in pregnancy. The International Society for the Study of Hypertension in
Pregnancy (ISSHP) guideline of 2018 was used as a template for this guideline. The South
African National Department of Health maternal mortality data (Saving Mothers Report) on
deaths due to hypertensive disease in pregnancy was used to identify problem areas in the
management of hypertension in pregnancy. A guideline strategy meeting was held in
Johannesburg in June 2018. Experts from all obstetrics and gynaecology academic centres in
South Africa were invited to participate. Each expert was tasked with answering key
questions relevant to the objectives within their area of expertise. They were advised to
conduct literature searches but this was not methodically defined. The proposed content of
the guideline was interrogated and debated by those present. The discussions were based
on evidence and clinical experience of the expert group. If evidence was lacking, a consensus
among participants was adopted.
3. Editorial independence
a. The funding for the development of the guidelines was the SAMRC. They were not
involved in the discussions or development of the guideline.
b. The competing interests of guideline development group members were recorded
and addressed at each meeting.
General Issues :
• General comment – guideline should be practical and feasible to implement. Most ante-
natal care takes place at primary health care clinic and mobile points. Aim to improve quality
of care within existing resources. Should consider medico-legal consequences if clinics are
unable to follow guideline
• Should guideline be aspirational or practical so that it can be applied and is feasible. Decision
to implement a practical rather than aspirational guideline
1. International Society for the Study of Hypertension in Pregnancy (ISSHP) Classification will be used (Brown et al., 2018) (2)
2. Standard for taking BP a. Use machines validated for use in pregnancy and ensure the provision of sufficient
machines.
i. The machine used in South African clinical trials is recommended i.e. the CRADLE
VITAL SIGNS ALERT (VSA) has a traffic light algorithm and is robust and cheap. It
is made by Micro-Life (approximate cost R900.00) (3)
ii. A national tender should be considered.
iii. Machines should be regularly calibrated – should be ensured by managers
iv. Machine must be robust.
v. Committee purchasing must have specifications of machines.
(Guideline on how calibration should be done. Validation in pregnancy must be
in specifications)
(DoH – Unit in charge of health technology is different to unit in charge of
tendering process. Three types of machines have to be placed on tender
process. Tender process explained. Recommendation of 2 different machines
should be included in guideline. Recommendation will be made for pregnancy
only.)

72
b. BP to be taken in the sitting position with legs uncrossed and in relaxed position. The
arms should be free of clothing, and arm supported
c. If the MUAC > 33cm, a larger cuff size should be used. Current machines available with 2
sizes for adults – adult and obese. (2)
d. The BP should be repeated in 15 minutes if there are slight elevations in BP or BPs
between 140 – 150 mm Hg systolic
e. Level of BP agreed 140/90 mm agreed as definition of hypertension. (4)
3. Borderline blood pressure in low risk pregnant women ( 135/85-139/89…pre-hypertension: BP repeated within 30 mins – 2 hours and if still borderline asked to return within 3-7 days. If
after repeat measuring the blood pressure is normal the woman can be followed up as a low risk
patient)
4. Biochemical angiogenic tests sFlt-1 /PLGF ratio or the PLGF on its own cannot be recommended for implementation now (2)
5. Calcium supplementation should be given to all pregnant women. 500mg of elemental
calcium daily with 2-hour gap between iron and calcium intake. Start at any gestation but start
as early as possible. (5)
WHO recommendation 1,5g of elemental calcium daily based on 1 systematic review.
Repeat review done on low dose calcium – similar results to high dose trials. 1.5g is a
high dose. SA studies – women are very calcium deficient. 500mg/day of elemental
calcium is a reasonable dosage. Cost issue, larger tablet to swallow. KZN currently
recommends 1g calcium / day. However, coverage is not optimal. Some formulations
not palatable; others have very low dose of elemental calcium in each tablet. Should it
be taken after certain gestational age? Should it be prescribed to women who already
have pre-eclampsia? Calcium reduces BP in women with hypertension therefore should
not be restricted to women for prevention of hypertension. No harm described to date.
More women with HELLP in calcium group in trials but significantly less serious
outcomes in calcium group.
6. Visual dipsticks be used to test for proteinuria in a clean catch specimen of urine and that infection as a cause of the proteinuria be ruled out. This should be done at all antenatal visits. (6,7)
7. Protein/Creatinine Ratio or 24hour urine protein can be used as a test for assessing amount protein . (6,8)
8. The ISSHP high risk factors list be used during history taking for identifying patients at risk at
all levels of health care and aspirin should be started for those at risk but only if the woman books early enough to start aspirin (ideally 12-14 weeks) but can be up to 20 weeks’ gestation (with 75–162 mg/day aspirin – a quarter or half an aspirin tablet) (9,10,11)
• Prior pre-eclampsia
• Chronic hypertension
• Multiple gestation
• Pre-gestational diabetes
• Maternal BMI>35
• Anti-phospholipid syndrome/SLE
• Assisted reproduction therapies

73
These risk factors should be on the BANC Plus qualifying first visit tick sheet and in the Maternity
Case Record (MCR) (12)
9. Need clear straight forward actions that PHC nurses can follow for the first visit. History taking at PHC is done by “general nurses” not experienced in maternity care, therefore
history taking instructions need to be clear and use tick lists.
It is also important that Obesity/BMI is measured. This can be by the BMI or MUAC. A BMI of 33
and a MUAC of 35 are the critical measures. (13)
Concept of next level of expertise Facilities differ in districts and provinces throughout the country. For this reason referral from the
primary health care (PHC) clinics, community care centres (CHCs) or in some circumstances district
hospitals must be to what is termed the next level of expertise. At the next level of expertise the
woman must be seen by an advanced midwife with special training or a doctor dealing with
pregnant women and there must be the facilities to perform a haemoglobin, platelets, urea,
creatinine, ALT, urine culture and a sonar examination. The blood results must be available in a
reasonable time so that management can be planned. The next level of expertise must have a rapid
and simple means of communication to specialists. Each catchment area will need to decide for
themselves where the next level of expertise from the PHC clinics or CHCs is.
High risk antenatal clinics can be created at CHCs and should be present in all district hospitals.
Concept of catchment area All areas in South Africa have defined referral routes. These referral routes do not always follow the
district boundaries and so they are called catchment area. Each catchment area should have a
regional or tertiary hospital that it refers to. The main hospital (regional or tertiary) in your
catchment area must be involved when developing these guidelines into protocols for your hospital
or clinic. You will need to develop local solutions; e.g. developing high risk obstetric clinics at CHCs,
by passing district hospitals when dealing with severely ill pregnant women to speed up transfer to
the main hospital in the catchment area. The District Clinical Specialists of the area should be
involved and facilitate these discussions and in finalising the protocols.
Mobile clinics Should mobile clinics be used for ante-natal care. Mobile clinics currently used for women who have
no transport. Some mobile clinic goes out every 6 weeks. Some women will require ante-natal care
every 2 weeks particularly in 3rd trimester. Mobile clinic feasible for low risk patients up to 34 weeks.
If risk factor identified patient should be referred.
• Mobile clinics to follow same guidelines as for PHC

74
Guideline for managing HDP per level of care
1. Primary health care level, initial assessment and management
(Includes Primary Health Care (PHC) clinic (e.g. 8am-5pm clinic and clinics who do
not conduct planned births), mobile clinics, Community Health Centre (CHC)/
Midwife Obstetric Unit (MOU)/ 24hour clinic doing planned births):
1.1. Women with pre-hypertension (BP 130-139/85-89 mm Hg) 1.1.1. Repeat blood pressure after rest (30minutes – 2 hours), if still pre-hypertension review
in 3-7 days at PHC, if normal follow-up as low risk woman (14)
1.2. HT with no risk factors, no proteinuria and no symptoms 1.2.1. Start Alpha Methyldopa (500mg 8 hourly) and send to next level of expertise within 3
days. (15)
1.2.2. A haemoglobin, platelets, creatinine, and a sonar for fetal evaluation needs to be done
1.3. HT with risk factors (list in point 8 above) but no proteinuria 1.3.1. Refer to District hospital
1.3.2. Start low dose aspirin
1.3.3. A haemoglobin, platelets, creatinine, and a sonar for fetal evaluation needs to be
done
1.4. Women with hypertension <32 weeks 1.4.1. Refer to a district hospital for investigation for pre-eclampsia
1.5. Hypertension with proteinuria one plus or more, no severe features 1.5.1. Same day referral to nearest hospital accredited for Caesarean Delivery
1.5.1.1. Inform receiving hospital
1.5.1.2. GA ³20 weeks.(If earlier GA, case to be discussed with receiving hospital re
same day or next day referral)
1.5.1.3. Give Magnesium sulphate if receiving doctor suggests it
1.5.2. Pre-eclampsia with severe features (headache, chest/epigastric pain/discomfort/visual disturbances) OR BP>160/110 mmHg (16)
1.5.2.1. Stabilise woman as described below
1.5.2.1.1. Inform receiving hospital (regional or tertiary)
1.5.2.1.2. Start one IV line with 200ml ringers lactate/or 200ml normal saline
(whichever is available), run IV line slowly, it is just for access
1.5.2.1.3. Start magnesium sulphate (4g IVI in 200ml N Saline/Ringers lactate
over 20 minutes, 10g IMI (5g in each buttock) route (16,17)
1.5.2.1.4. Lower High Blood Pressure with 10mg quick acting Nifedipine orally.
This can be repeated every 30 minutes if the blood pressure does not drop
below 160/110mmHg. If the woman is unable to swallow put the 10mg
nifedipine under the woman’s tongue.
1.5.2.1.5. Give 1g Alpha Methyldopa orally
1.5.2.1.6. Insert a urinary catheter and monitor the urine output every hour
until the woman is transferred
1.5.2.1.7. Monitor the woman’s BP, pulse, respiratory rate, every 15 minutes
until the woman is transferred
1.5.2.1.8. Emergency transfer ideally accompanied by an experienced nurse if
available. Use SBAR form
1.5.2.1.9. Woman must be monitored and transferred in the lateral position

75
2. In District Hospital (DH) with caesarean section capability
2.1. Women with pre-hypertension (BP 135-139/85-89 mm Hg) 2.1.1. Repeat blood pressure after rest (30 minutes – 2 hours), if still pre-hypertension review
in 3 days at PHC/CHC or DH which ever most convenient
2.2. Woman with hypertension without proteinuria 2.2.1. Start 500mg Alpha Methyldopa 8 hourly, and follow-up in 3-7 days to see if BP
controlled
2.2.2. Investigate for pre-eclampsia haemoglobin, platelets, creatinine and sonar for fetal
evaluation
2.2.3. Follow-up weekly
2.3. Woman with features suggestive of pre-eclampsia (e.g. HT<32 weeks, fetal growth restriction, isolated proteinuria, hypertension and proteinuria)
2.3.1. Confirm the diagnosis
2.3.2. Estimate gestational age, fetal biometry - ultrasound scan
2.3.3. P/Cr ratio, MCS, Haemoglobin, platelets, creatinine, ALT
2.3.4. Consider delivery or transfer to a higher level of care depending on the diagnosis and
context (see below)
2.4. Woman with pre-eclampsia and severe features (referred or discovered) 2.4.1. Stabilise woman as described below
2.4.1.1. Start one IV line with 200ml ringers lactate/or 200ml normal saline
(whichever is available), run IV line slowly, it is just for access
2.4.1.2. Start magnesium sulphate (4g IVI in 200ml N Saline/Ringers lactate over 20
minutes, 10g IMI (5g in each buttock) route (2,18)
2.4.1.3. Lower High Blood Pressure with 10mg quick acting Nifedipine orally. This
can be repeated every 30 minutes if the blood pressure does not drop below
160/110mmHg. If the woman is unable to swallow put the 10mg nifedipine
under the woman’s tongue.
2.4.1.4. Give 1g Alpha Methyldopa orally
2.4.1.5. Determine if the fetus is alive. Do not monitor the fetus
2.4.1.5.1. ONLY monitor the fetus once the woman is stable and the decision
has been taken that delivery is safe in the district hospital
2.4.1.6. Insert a urinary catheter and monitor the urine output every hour until the
woman is transferred
2.4.1.7. Monitor the woman’s BP, pulse, respiratory rate, every 15 minutes until the
woman is transferred
2.4.1.8. Emergency transfer ideally accompanied by an experienced nurse if
available. Use SBAR form
2.4.1.9. Woman must be monitored and transferred in the lateral position
2.4.2. Transfer to highest available level of care (regional or tertiary – specialist O&G,
anaesthetist care available)
2.4.3. Give steroids if gestational age <34 weeks
2.4.4. If in labour, stabilise and aim for delivery in DH, then transfer
2.5. Gestational age <28 weeks pre-eclampsia with no severe features and gestational age 28-33 weeks, pre-eclampsia with no severe features
2.5.1. Stabilise woman as in 2.4.1
2.5.2. Transfer to higher level of care
2.5.3. Consult with referral hospital about steroids and magnesium sulphate
2.6. GA 34 weeks or more, pre-eclampsia with no severe features:
2.6.1. Stabilise woman as in 2.4.1
2.6.2. Ideally transfer to regional or tertiary hospital where specialist care is available

76
2.6.3. In special circumstance the woman can be managed by the district hospital if sufficient
expertise is available. This will be determined by the main hospital (regional or
tertiary) in the catchment area.
2.6.4. The woman must NOT be treated as outpatient.
2.7. Gestational hypertension (may be chronic; can only make diagnosis of chronic
hypertension 6 weeks following delivery):
2.7.1. To be seen weekly at the antenatal clinic after screening bloods (haemoglobin,
platelets, creatinine, sonar for fetal evaluation to exclude pre-eclampsia)
2.7.1.1. Uncertain of need for urine culture in absence of proteinuria
2.7.2. For delivery at 38-40 weeks at District Hospital (19)
3. Severe hypertension and pre-eclampsia with severe features (managed in regional
or tertiary hospitals – main hospital in catchment area):
3.1. Stabilise woman as in 2.4.1
3.2. Magnesium sulphate:
3.2.1. IM regimen (Pritchard),
3.2.2. IV if feasible
3.3. Preferred option for severe hypertension:
3.3.1. Antihypertensives:
3.3.1.1. Oral nifedipine (10 mg) cheaper, easier.
3.3.1.2. IV labetalol expensive, advantage forces monitoring
3.3.1.3. IV dihydralazine or hydralazine but difficult to procure
3.3.1.4. Use nifedipine or labetalol as second line if first choice not effective
3.3.1.5. Alpha methyldopa should be started on admission, if not already on it. Give
1gm loading dose and thereafter 750mg 8 hourly. This is to ensure smoother
blood pressure control later, and is NOT for immediate control of severe
hypertension.
3.3.2. Fluids:
3.3.2.1. Magnesium sulphate bolus 4g in 200 mL over 20 minutes,
3.3.2.2. Ringer’s lactate 80 mL/hour maximum (2,20)
3.3.2.3. If urine output drops to <25 ml/hour one additional bolus of 200ml can be
given.
3.3.3. Fetal monitoring
3.3.3.1. Determine if the fetus is alive on admission
3.3.3.2. ONLY monitor the fetus once the woman is stable
3.3.4. Delivery
3.3.4.1. If eclamptic or HELLP or organ dysfunction steps for delivery should be
initiated as soon as woman is stabilised.
3.3.4.2. Initiated if 34 week’s gestation
3.3.4.3. Consider giving corticosteroids and initiate delivery after 48 hours if
between 28-33 week’s provided woman is stable (no eclampsia, no HELLP,
normal platelets and creatinine, and BP controlled easily with disappearance of
symptoms)
For any pre-eclampsia at term, or preterm pre-eclampsia with serious maternal complications
(e.g. eclampsia, CVA, pulmonary oedema, uncontrollable severe hypertension, renal dysfunction
(Creatinine >120), coagulopathy (platelets <100 000 twice)), pregnancy termination
(compassionate induction of labour) should be ‘strongly advised’.

77
For pre-eclampsia preterm without serious maternal complications (>34 weeks’), termination of
pregnancy (compassionate induction of labour) should be ‘offered’ with a full explanation of the
trade-off between limiting the risk to the mother of disease progression and compromising the
baby’s health due to premature birth. (21) (Where possible the family e.g. husband, partner,
mother should be included in the discussion). When the maternal and fetal status is stable and
the gestation <34 weeks’, expectant care may be offered after careful counselling, at a tertiary
facility under specialist care. It should be emphasized that while survival is usual after 34 weeks’
gestation, preterm birth even after 34 weeks is associated with neurological impairment.
Informed consent is required for either “termination of pregnancy” or expectant management
where delivery would otherwise effect a cure from a life-threatening illness within 24 hours in
most cases
Note: It is critical to control the blood pressure and every effort must be made to do this in a
reasonable time.

78
Other issues
1. Induction of labour in pre-eclampsia or eclampsia:
1. With eclampsia, delivery is urgent and there is a time consideration (about 6 hours to get
labour established and then delivery within 12 hours from initiation of induction)
• Can be considered if cervix favourable, depending on evaluation of maternal
complications. Requires high care monitoring throughout. Availability of skilled
doctors and facilities for safe CD must also be considered. Induction of labour is
appropriate especially where CD is less safe
• All women with eclampsia should be in facilities where a safe CD can be performed
2. Without eclampsia, induction of labour reasonable even if cervix is not favourable
2. Vaginal birth in pre-eclampsia:
1. No need for elective assisted delivery
2. If the blood pressure is not controlled before pushing consider shortening second stage with
forceps or vacuum
3. Postoperative and postpartum care in pre-eclampsia:
1. Early warning monitoring chart (Coloured monitoring Charts) in a high care area must be
used
2. Consider VTE taking account appropriate clinical features i.e. weight, duration of hospital
stay, platelet counts, BP stabilisation and discuss with a specialist obstetrician and
anaesthesiologist etc.
3. Never discharge home before 24 hours
4. Continue magnesium sulphate to 24 hours after delivery or 24 hours after last fit
5. Keep eclamptic women and those with organ dysfunction for at least 3 days
6. Do not routinely stop antihypertensive drugs abruptly
7. Antihypertensive drug of choice – calcium channel blockers and or diuretic (>48 hours) ACE
Inhibitors and diuretics cab be used in combination post- partum.
8. Ensure appropriate contraception is provided
Prior to discharge all women with pre-eclampsia should have counselling especially if a
complication and pregnancy loss. information about future pregnancies and long term
outcomes ( risks of developing pre-eclampsia in the future) (22,23)
4. Long-term follow-up:
1. Depends on where the woman lives: at hospital or CHC after 1 week
2. Recommend 3-monthly follow-up
3. Psychological health – counselling and support should be provided (24)

79
Anaesthetic considerations (regional, tertiary, possibly district in special
circumstances agreed by the main hospital in the catchment area):
1. Stabilise patient – aim for BP 140/90 or less, MUST be <160/110
2. Dialogue with anaesthetist
3. Regional is anaesthetic of choice
4. Check haemoglobin, platelets
5. Platelets ordered on standby if platelet count <50000
6. GA recommended if:
i. Platelet count <75000 in last 6 hours, or platelet count not available.
This is a contentious issue, as very often the airway poses potential
difficulty. IF a specialist anaesthetist is directly involved with the case, and
pencil point spinal needles are available, a platelet count of 50000 MAY be
considered as the cut-off. In addition the time since the performance of the
platelet count may be increased to 12 hours, with the proviso that a risk-
benefit discussion occurs, particularly in severe pre-eclamptic patients,
where the platelet count may drop catastrophically, and a spinal anaesthetic
may render the management of a bleeding patient very difficult.
ii GCS <14
iii Congestive cardiac failure
7. IF GA administered:
i Magnesium to attenuate intubation response and/or opiates
ii Fluid restriction or goal directed fluid therapy; preloading is NOT recommended
iii Multimodal analgesia – local infiltration, paracetamol, opiates, not NSAIDs.
iv Lignocaine to attenuate extubation response unless CNS concerns
8. In ALL patients the syntocinon should be given at a reduced infusion rate.
9. ALL patients require an acute care bed, arranged in consultation with the obstetrician.
NOTE: These are guidelines, and each patient with PET/Eclampsia needs to be assessed on merit, taking into account the following: blood pressure control, cardiac function, neurological status, platelet count and bleeding status, and the airway.

80
References 1. Moodley J, Ngene NC. Blood pressure management and rapid acting antihypertensives for
severe hypertension in pregnancy: Review. Obstetrics and Gynaecology Forum 2016; 26: 35-
40.
2. Brown MA, Magee LA, Kenny LC, Karumanchi SA, McCarthy FP, Saito S et al. The
hypertensive disorders of pregnancy: ISSHP classification, diagnosis and management
recommendations for international practice. Pregnancy Hypertension 2018,
https://doi.org/10.1016/j.preghy.2018.05.004
3. Nathan HL, Boene H, Munguambe K, Sevene E, Akeju D, Adetoro OO et al. The CRADLE vital
signs alert: qualitative evalutation of a novel device designed for use in pregnancy by
healthcare workers in low-resource settings. Reproductive Health 2018; 15:5. DOI
10.1186/s12978-017-0450-y
4. Redman CWG, Jacobson SI, Russell R. Hypertension in pregnancy, in: R Powrie, M Greene, W
Camann (Eds), de Swiet’s Medical Disorders in Obstetric Practice, fifth ed., Blackwell
Publishing, 2010, pp.153-181.
5. Hofmeyr GJ, Atallah AN, Duley L. Calcium supplementation during pregnancy for preventing
hypertensive disorders and related problems. Cochrane Database Syst. Rev. (8)(2010).
6. Cade TJ, Gilbert SA, Polyakov A, Hotchin A. The accuracy of spot urinary protein-to-
creatinine ratio in confirming proteinuria in pre-eclampsia. Aust NZ J Obstet. Gynecol 2012;
52 (2): 179-182.
7. Phelan IK, Brown MA, Davis GK, Mangos G. A prospective study of the impact of automated
dipstick urinanalysis on the diagnosis of preeclampsia. Hypertens. Pregnancy 2004; 23(2)
:135-142.
8. Cote AM, Brown MA, Lam EM, von Dadelszen P, Firoz T, Liston RM, Magee LA. Diagnostic
accuracy of urinary spot protein:creatinine ratio for proteinuria in hypertensive pregnant
women: systematic review, BMJ 2008; 336 (7651): 1003-1006.
9. Bartsch E, Medcalf KE, Park AL, Ray JG. Clinical risk factors for pre-eclampsia determined in
early pregnancy: systematic review and meta-analysis of large cohort studies. BMJ 2016;
353: i753.
10. Rolnik DL, Wright D, Poon IC, O’Gorman N, Syngelaki A, Matallana C de Paco et al. Aspirin
versus placebo in pregnancies at high risk for preterm preeclpamsia. N England J Med 2017
null.
11. Bujold E, Roberge S, Lacasse Y, Bureau M, Audibert F, Marcoux S et al. Prevention of
preeclampsia and intrauterine growth restriction with aspirin started in early pregnancy: a
meta-analysis. Obstet Gynecol 2010; 116: 402-414
12. Hofmeyr GJ, Mentrop L. Time for “basic ante-natal care plus” in South Africa? SAMJ 2015;
105 (11); 902-903.
13. Fakier A, Petro G, Fawcus S. Mid-upper arm circumference: A surrogate for body mass index
in pregnant women. SAMJ 2017; 107(7): 606-610.
14. Magee LA, von Dadelszen P, Rey E, Ross S, Asztalos E, Murphy KE, Menzies J et al. Less-tight
versus tight control of hypeternsion in pregnancy. N Engl J Med 2015; 372 (5): 407-417.
15. Hawkins LA, Brown MA, Mangos GJ, Davis GK. Transient gestational hypertension: not
always a benign event. Pregnancy Hypertens 2012; 2 (1) 22-27.

81
16. Magee LA, von Dadelszen P, Singer J, Lee T, Rey E, Ross S et al. The CHIPS randomised
controlled trial (control of hypertension in pregnancy). Is severe hypertension just an
elevated blood pressure? Hypertension 2016; 68 (5): 1153-1159.
17. Duley L, Gulmezoglu A, Henderson-Smart DJ, Chou D. Magnesium sulphate and other
anticonvulsants for women with pre-eclampsia. Cochrane Database Syst. Rev. (11) (2010).
18. Group TMTC. Do women with pre-eclampsia and their babies benefit from magnesium
sulphate? The Magpie Trial: a randomised placebo-controlled trial. Lancet 2002; 359 (9321):
1877-1890.
19. Cruz MO, Gao W, Hibbard JU. What is the optimal time for delivery in women with
gestational hypertension? Am J Obstetr Gynecol 2012; 207 (3) 214 e1-6.
20. Brown MA, Gallery EDM. Volume homeostasis in normal pregnancy and pre-eclampsia:
physiology and clinical implications. Balliere’s Clin Obstet. Gynecol. 1994; 8 (2): 287-310.
21. Gillon TE, Pels A, von Dadelson P, MacDonell K, Magee LA. Hypertensive disorders of
pregnancy: a systematic review of international clinical practice guidelines, PLoS One (2014).
22. Bellamy L, Casas JP, Hingorani AD, Williams D. Pre-eclampsia and risk of cardiovascular disease
and cancer in later life: systematic review and meta-analysis. BMJ 2007; 335: 974.
23. Soma-Pillay P, Louw MC, Adeyemo AO, Makin J, Pattinson RC. Cardiac diastolic function after
recovery from pre-eclampsia. CVJA 2017; 28.
24. Soma-Pillay P, Makin JD, Pattinson R. Quality of life 1-year after a maternal near miss event.
Int J Obstet Gynecol 2018; Int J Gynecol Obstet 2018; 141: 133-138.

82
Section 4. Monitoring and Evaluation of
Basic Antenatal Care Plus implementation
in South Africa TMAG Hlongwane, RC Pattinson
SAMRC/UP Maternal and Infant Health Care Strategies Unit
Background
The Minister of Health accepted the new antenatal care package (called Basic Antenatal
Care Plus - BANC Plus) at the National Health Council of 24th November 2016 and instructed
the MECs to implement it starting 1st April 2017. The SAMRC/UP Maternal and Infant
Health Care Strategies unit (hence forth called SAMRC/UP unit has monitored and evaluated
the implementation of BANC Plus in 4 sites in South Africa.
Focus groups
After the introduction of the BANC Plus workshops in February and March 2017 the
SAMRC/UP unit had conducted a series of focus groups in 6 of the 9 provinces
(Mpumalanga, North West, Gauteng, Eastern Cape, Free State, and Northern Cape) which
comprise of 31 of the 52 districts in the country on antenatal care amongst other things. A
total of 22 focus groups were held with a total of 524 participants. The participants
included the provincial Maternal and Child Health (MCH) coordinators, district managers,
facility managers, CEOs of hospitals, HOD of Obstetrics and Gynaecology departments in
from larger hospitals, health care professionals from all types of facilities including PHC
facilities, emergency medical services (EMS), DCSTs and the NDOH.
The focus groups started by describing their maternal, stillbirth and neonatal death
mortality for the province, district and facility, (community health centre, district hospital
and regional/tertiary hospital). This was followed by discussion of the case on antenatal
care shown below. (Other cases were also discussed regarding transport and emergency
obstetric care).

83
Table 1. Antenatal care case scenario, challenges and solutions Scenario General issues raised by scenarios Specific
challenges identified in discussion
Proposed solutions and responsibilities
It is 09.00 at a primary health care clinic. Mrs W is a 32 year old
P3G4, she is currently 22
weeks pregnant and her
blood pressure is 145/95
mmHg. This is her first
visit.
How will you manage her antenatal care?
⁻ Assessment and diagnosis ⁻ Refer to doctor / high-risk clinic
o Visiting doctor in clinic with adequate knowledge / training / contract
o If to hospital, must ensure access (PPT)
⁻ Communication between levels ⁻ Link to WBOTs / CHWs for adherence
After the discussion information on why the antenatal care protocol was changed and the
potential effect of the change was discussed. The following figure was used to illustrate the
challenges to come.
Figure 1. Peaks in stillbirths in Mpumalanga province in South Africa
This figure illustrates the two peaks of stillbirths (at 32 and 38 week’s gestation). The peaks
correlate with the antenatal visits using the reduced visit BANC protocol at 32 and 38 weeks.
The interpretation of this was that we were diagnosing stillbirths at these times as the
women were attending clinics then and inducing labour. We were not preventing stillbirths,
just diagnosing them. This together with the new knowledge that the reduced visits could
increase the perinatal mortality by 15% was the motivation for the increased visit and other
changes for antenatal care in BANC Plus.

84
The point was made that with the increased visits there will be increased high risk referrals
as the women with babies at risk or if they develop complications like hypertension will be
referred. This had already resulted in some of the large hospital’s clinics being over-run by
women being referred for complications. The question was then asked as to how they will
deal with the increased number of women detected with high risk factors.
Summary of focus group findings
• Only one district commented on lack of staff for performing the increased antenatal
visits.
• Most districts had not developed plans to deal with the increased referrals
• In those districts where there were plans, there were four models used to manage the
increased load of high risk pregnant women
o Training an “advanced antenatal care practitioner” (advanced midwife of doctor)
to see the cold referrals at the clinic once a week. They would decide whether to
manage the women at the PHC clinic or refer to the hospital or tertiary antenatal
clinic. These practitioners had a direct line to the hospital and specialists. The
practitioners would visit about 5 PHC clinics per week.
o Training the doctors at the PHC clinics to see the cold referrals and decide to
manage at the PHC clinic or refer to the hospital or specialist. At training course
(BANC Plus consultation) was developed for this.
o Outreach from the hospital by doctors from the maternity unit to see women at
the clinic. Mostly there were at Midwife Obstetric Units that were doing over
1500 deliveries per year.
o Outreach using the DCST to see women at the PHC clinics. These were the
advanced midwife or family physician from the DCST.
• Transporting women to the high risk clinic was often a problem. The solutions were:
o Woman provide own transport (worst option)
o Planned patient transport run by EMS.
o Call an ambulance to take the woman to hospital, even though it was not an
emergency.
• Women were admitted to hospital for considerable periods because of lack of transport.
• Maternity waiting homes were used for some women with high risk antenatal factors.

85
Assessment of antenatal care in 4 catchment areas
Setting Table 2. The 4 catchment areas used for the monitoring and evaluation
Province- Hospital area Clinics and referral hospital
Gauteng: Pholosong
Nokuthela Ngwenya clinic, Kwa Thema clinic,
Pholosong hospital clinic
Northern Cape: Upington Progress clinic, Sara Strauass clinic, Loui Vaile
Clinic, Town clinic, Dr Harry Surtie Hospital
North West: Mafikeng Montshiwa Stadt clinic, Monsthioa town clinic,
Unit 9 clinic, Mafikeng Provincial hospital
Limpopo: Vhembe Thohoyandou community health centre, Sibasa
clinic, Shayandima clinic, Tshilidzini hospital
The SAMRC/UP unit offered support to the 4 catchment areas to adjust the protocol books
in line with the new guidelines, and had site visits to discuss antenatal care and the new
guidelines.The catchment areas are shown above in table 2.
The antenatal cards were photostated and outcome of pregnancy recorded of the first 50
consecutive deliveries of each quarter from each site and assessed by TH. Most deliveries
occurred in the main hospital of the catchment area.
Table 3 below details the number of antenatal card collected from each site. All cards were
collected by February 2018.
Table 3. Antenatal card and outcomes collected Hospitals March July September November February Pholosong 50 50 50 50 50
Upington 50 50 50 50 50
Mahikeng 50 50 50 50 50
Vhembe 50 50 50 50 50
Analysis of 1000 maternal cards was performed focusing on the changes in number
antenatal contacts, the detection of antenatal hypertension and the response to detecting
hypertension.

86
Results are as follows:
There was a steady increase in the number of visits over the one year period.
More women with hypertension were detected.
Results
0,0%
5,0%
10,0%
15,0%
20,0%
25,0%
30,0%
% o
f PT
with
8 o
r mor
e co
ntac
ts
Eight or more contacts (N=1000)
March July September November February
0,0%
10,0%
20,0%
30,0%
40,0%
50,0%
60,0%
70,0%
% o
f PT
with
6 o
r mor
e co
ntac
ts
Six or more contacts (N=1000)
March July September November Febrary
Results: Detection of Hypertension
• This equates to an average of 30% increase in hypertension detection from the baseline in March to February.
0
5
10
15
20
25
% o
f HT
dete
cted
Detection of HT
March July September November February

87
There has been an reduction in the number of women who did not have their blood
pressure measured at each visit. Coupled with this there has been an increase in the
number of cases where the appropriate action was taken. However, even though this
increased by 23% still about one third of women were not appropriately managed one year
after the implementation of BANC Plus.
Table 4. Percent of appropriate action taken in those detected with hypertension on during antenatal care.
Month (200 cases/month)
Number with hypertension
Number with appropriate action taken
% Appropriate action
March 25 14 56.0
July 28 17 60.7
September 24 16 66.7
November 40 27 67.5
February 36 25 69.4
Overall, the women were visiting the clinic more often, the blood pressure was taken at
most antenatal clinic visits, an increasing number of women with hypertension were
detected and an increasing number of women with hypertension detect had the
appropriate action taken. The appropriate action was not taken in just under a third of
cases at the end of the year after implementation. The appropriate action was not taken at
the clinic level.
Effect on perinatal mortality
Each site runs the Perinatal Problem Identification Program (PPIP) and data on perinatal
mortality was collated and analysed in 6 monthly tranches to assess the impact if any on
mortality.
The tranches were 6 months before the change in antenatal care protocol (October 2016-
March 2017, i.e. control group); 6 months into the change (April 2017-September 2017, i.e.
during transition) and the following 6 months (October 2017-March 2018 after transition)
we have seen a significant decrease in unexplained stillbirths, but also a significant increase
in stillbirth due to hypertension. See tables 5 and 6 below. The overall stillbirth rate and
early neonatal death rates remained similar.
Results: BP recording, actions taken
89
90
91
92
93
94
95
96
97
98
99
N of
BP
at e
ach
visit
BP at each contact (N=1000)
March July September November February
0
2
4
6
8
10
12
14
16
18
20
N of
Pat
ient
s
Appropriate action taken (145)
March July September November February

88
Table 5. PPIP indicators: Primary causes of Stillbirths
Time Period Total del.
.Del٭Unexp
SB HT APH SpD IPA
Oct 2016 - Mar 2017 9801 18 11 24 14 103 9637٭
Apr 2017 - Sep 2017 10581 30 16 28 39 65 10408٭
Oct 2017 - Mar 2018 11051 25 19 40 34 61 10866٭
Perinatal mortality indicators and avoidable factors: Hypertensive disorders (HT)), Unexplained stillbirth (Unexpl SB),Antepartum haemorrage(APH), Spontaneous Preterm delivery (SpPD), Intrapartum asphhyxia (IPA), No response to antenatal Hypertension(No response). ٭ Total deliveries more than 1000g who attended antenatal care.
Table 6. Stillbirth rates due to Hypertension, Unexplained stillbirths and Antepartum haemorrhage in antenatal care attenders. (Births and Stillbirths >1000g)
Time Period HT SBR Unexp. SBR APH SBR Oct 2016 - Mar 2017 1,5 10,7 2,5
Apr 2017 - Sep 2017 3,7 6,2 2,7
Oct 2017 - Mar 2018 3,1 5,6 3,6
SBR – Stillbirth rate; HT – hypertension; Unexp. Unexplained; APH – Antepartum haemorrhage
Table 7. Primary cause of death and avoidable factors:
Time Period Stillbirth Stillbirths and early neonatal deaths HT No response HT No response Oct 2016-March 2017 14 9 (64%) 19 9 (47%)
April 2017-Sep 2017 39 22 (56%) 48 27 (56%)
Oct 2017-March 2018 34 15 (44%) 38 18 (47%)
Primary cause of death and avoidable factors: Hypertensive disorders (HT)), No response to antenatal Hypertension (No response).
Table 7 gives the number of cases where there was a perinatal death and the avoidable
factor was “no response to antenatal hypertension”. The number of this avoidable factor
increased but proportionally there was a decrease in the three periods in the stillbirths.
Discussion
This report evaluates the implementation of BANC Plus in 4 catchment areas in South Africa.
The focus groups around the country revealed that although there were options to deal
with women with hypertension not many districts had specific plans. This is borne out by
the findings in this report.
Analysis of antenatal care per quarter found the women were visiting the clinic more often,
the blood pressure was taken at most antenatal clinic visits, an increasing number of
women with hypertension were detected and an increasing number of women with
hypertension detected had the appropriate action taken. Thus the message of increased
visits has been accepted by the community and the health care professionals have improved
their screening for hypertension in pregnancy and there was some improvement in acting
on the diagnosis of hypertension in pregnancy.
However, appropriate action was not taken in women with hypertension in pregnancy in
just under a third of cases a year after implementation. Analysis of the stillbirths for the 4
sites revealed that there was no change over the three periods in the stillbirth rate, but
there was a decrease in the number of stillbirths classified as unexplained and an increase in
the number of stillbirths where hypertension was given as the underlying cause. The most

89
common avoidable factor was “not responding to antenatal hypertension” and this
correlates with the number of antenatal cases where the appropriate action for managing
hypertension was not taken at the antenatal clinic.
The core problem in perinatal deaths due to hypertensive diseases in pregnancy is due to
the primary health care clinics not managing the woman appropriately by either referring
her on or having a more skilled attendant manage the pregnancy. Lack of recognition of the
problem and full assessment at the primary care level was also the most common health
care professional avoidable factor in women who died due to complications of hypertension
in pregnancy.
Conclusion
Targeting primary health care clinics that perform antenatal care and improving their
knowledge and ensuring a functioning and feasible referral system to the next level of
expertise is essential if maternal and perinatal deaths due to hypertensive diseases in
pregnancy are to be reduced.

90
Section 5. Saving Mothers Report 2017:
Report on key decisions taken by the
National Health Council; 6-7 December
2018
Note: Please see full Report for details Summary of key findings:
1. IMMR has levelled off since 2015
2. Impact of ARVs maximized (but NPRI still high because of deaths from TB, atypical
pneumonias)
3. Deaths from Obstetric haemorrhage have started to decline
4. Deaths from Hypertensive disorders of pregnancy (HDP) not declining (some indication that
it is climbing); HDP are also associated with high numbers of stillbirths, intrauterine and
neonatal deaths
5. The Challenge is insufficient and poorly skilled doctors and nurses, especially in district
hospitals in the more rural areas and non-use of standardized clinical protocols in tertiary
and national central hospitals
Summary of proposed interventions: • C - Improve access to all forms of contraception particularly to those below age of 18 years
and those > 35 years
• C - Strengthen access to and quality of antenatal care, in particular history taking of
hypertension in previous pregnancies and recognition of hypertension
• C- Improve communication with communities with respect of booking for antenatal care early in pregnancy and involve general practitioners to refer pregnant patients at the time of diagnosis of pregnancy. Use community service workers for this purpose also
• C - Implement safe C/S package( including the safe anaesthetic component) in all provinces
• C – Care quality of care : improve attitudes of health workers, strengthen training of nurses
and doctors and use of clinical protocols; strengthen use of DCSTs by examining the sites at
which they are placed (district office /regional hospitals etc.)
Decisions by the NHC: • Increase access to contraceptives
o Strengthen access to contraceptives to young people and those older than 35 (focus
on home, school, TVETs, universities)
o Hospitals to strengthen postpartum contraception, including tubal ligation
• Improve access to quality antenatal care o In addition to Mom Connect, CHWs must encourage pregnant women to seek
antenatal care as early as possible
o Mobilise communities through community leaders

91
• Strengthen information, diagnosis and treatment of Hypertensive Disorders of Pregnancy Ensure that all clinics have protocols and guidelines (including referral)
o DCSTs to ensure that protocols are available and are used (and provide training in
the use of protocols were necessary)
o Train nurses to manage / initiate treatment for HDP immediately especially that of
severe hypertension ) and refer pregnant women with hypertension timeously
o Ensure that functional BP machines are available at all clinics
o Provide calcium carbonate as part of antenatal care to prevent HDP and provide low
dose aspirin for those at risk of HDP
o Speak to DBE about providing information to all learners about reproductive health
matters and to ensure pregnant learners get their BP measured regularly
o Minister to issue a circular to clinical managers on the management of staff
especially sessional doctors and the availability and use of clinical protocols on
management of hypertension
• Distribution of Saving Mothers Report o Saving Mothers Report, 2017 can be distributed to provinces
o Ministerial committee to meet with officials (CEO’s, Medical and Nursing Managers)
and clinicians including DCST in each province to share the report so that province-
specific interventions can be developed (MECs were encouraged to attend)