
Antepartum Hemorrhage
52
Antepartum Haemorrhage By Dr Shuhaila Ahmad / A/Prof Dr Zaleha
-
Upload
babi-panggang -
Category
Documents
-
view
66 -
download
3
description
Antepartum Hemorrhage
Transcript of Antepartum Hemorrhage
Antepartum Haemorrhage
By
Dr Shuhaila Ahmad / A/Prof Dr Zaleha
Definition
Bleeding from the genital tract from 22 weeks POA until delivery of the fetus
Why 22 weeks POA?This is because fetus is considered to be salvageable
at this gestation(WHO= 22 weeks/ 500g or more)
**Lower segment starts to form at 28 weeks until 34 weeks

Incidence of APH
2 to 5 % of all pregnancies (at term)The earlier the gestation , the higher the
incidence.
Causes
Placenta praevia (30%)Abruptio placenta (22%)Indeterminate cause(42%)Local causes (5%)
– cervical polyp/ carcinoma– cervical erosion/ cervicitis– laceration
Vasa praevia -very rare
Complications of APH
an aem ia D IV C H yp ovo lu m ic sh ock P os tp artu mh aem orrh ag e
M ate rn a l
Maternal mortality
Complications Of APH
d ea th o rd is tress
an aem ia IU G R p rem atu rity
F e tu s
Fetal loss14%

PLACENTA PRAEVIA

Definition
Placenta that is situated wholly or partially in the lower segment

Types of placenta praevia
Typ e 1 Typ e 2
M in or
Typ e 3 Typ e 4
M ajo r
P lacen tap raevia
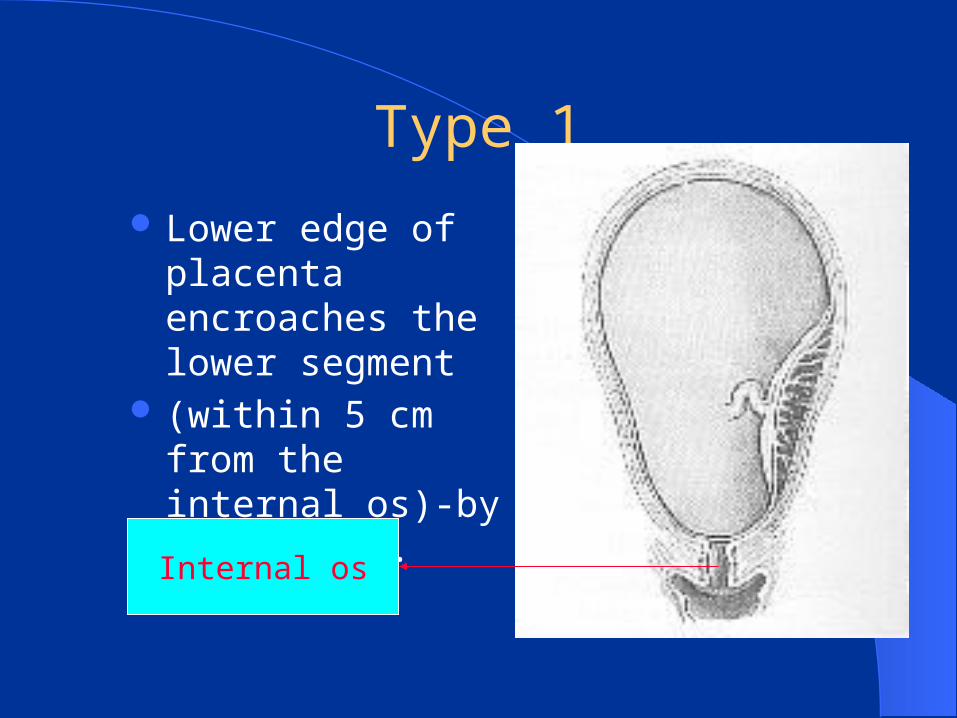
Type 1
Lower edge of placenta encroaches the lower segment
(within 5 cm from the internal os)-by ultrasound.
Internal os
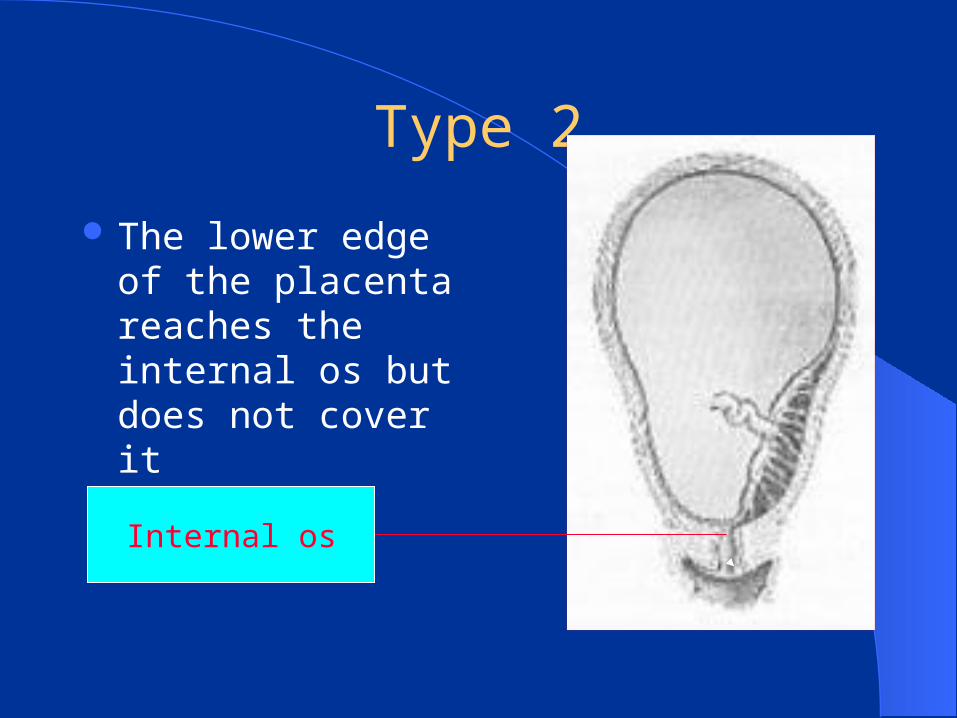
Type 2
The lower edge of the placenta reaches the internal os but does not cover it
Internal os
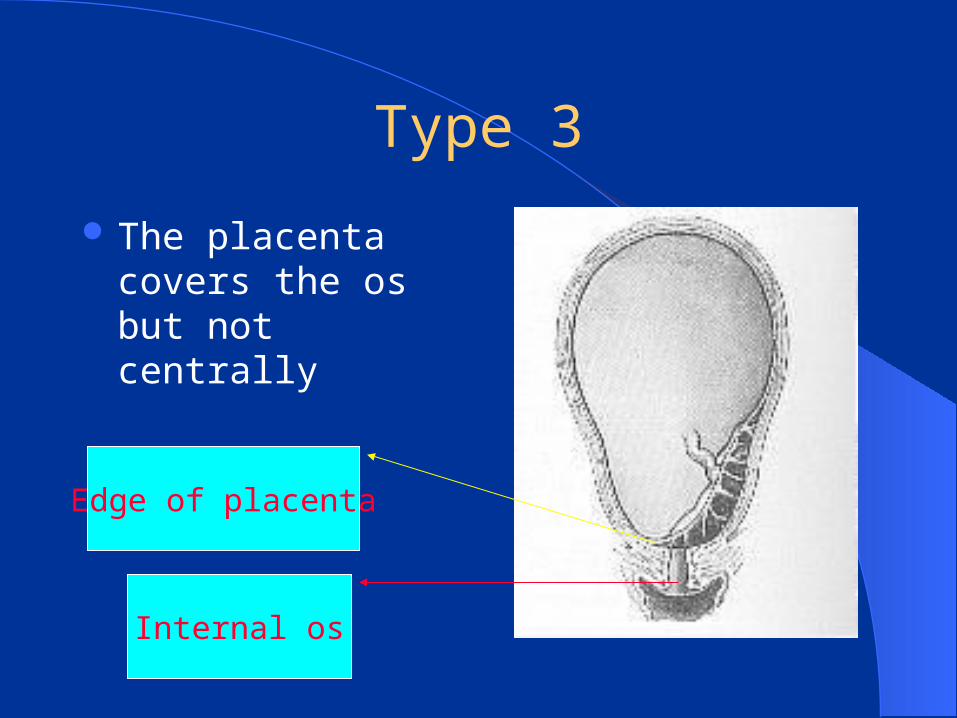
Type 3
The placenta covers the os but not centrally
Internal os
Edge of placenta

Type 4
The placenta centrally covers the os
Internal os

Cause
Unknownit is associated with:
– previous caeserean section– previous history of placenta praevia– previous h/o spontaneous abortion whereby
evacuation of uterus was performed– multiparity– multiple pregnancy
How do they present?
Classical presentation:– fetal malpresentation in late pregnancy– painless pervaginal bleeding
An unengaged head at term especially in a primigravida
Asymptomatic– diagnosis via ultrasound scan
History
Bleeding– usually painless– unprovoked e.g.. Trauma– the amount varies– fresh bleeding
Fetal movement unchanged
Physical examination
Usually vital signs stable i.e.. Not in shock (the vital signs reflect the amount of bleeding)
Abdomen is non tender and softUterus is soft and corresponding to dateFetus could be in an abnormal presentationFetal heart sound present
NO VE TO BE DONE
Until placenta praevia is ruled out
Investigation
Ultrasound scan via the abdomen – full bladder is required for better visualization– able to tell anterior or posterior– type of placenta– presentation of the fetus
Haemoglobin levelBlood group

Other methods
X-ray of the pelvis (lateral)– will show a excessive distance between the
fetal head and sacrum or symphisis pubisRadioisotope imagingMagnetic Resonance Imaging (MRI)
– expensive– not invasive

Examination under anaesthesia
Ultrasound equipment or expertise is not at hand
Patient is bleeding to a degree whereby the delay to arrange for ultrasound would be dangerous
Uncertainty between a normally situated placenta and a praevia minor
How to do it?
Preparation as if the patient is going for caesarean section
In operation theatreNot necessarily under general anaesthesiaScrub nurse and assistant fully scrubbed
and gownedInstruments for CS are laid out
EUA - how to do it?
The surgeon scrubbed and fully gowned– patient in dorsal position– vulva and vagina are inspected for active bleeding– speculum introduced to look at the os for bleeding or
placenta– finger introduced to feel for fornices– introduced into the os and feel for placenta– If no placenta, amniotomy is performed
Principle of management of APH
ResuscitationAdmit to a center with adequate facilities
such as operation theatre, blood bank and neonatal backup
After patient is stabilized, get brief history and physical examination to assess patient’s condition

Perform several investigations to look for cause and assess patient’s condition
Planned for further treatment ( to deliver or not and mode of delivery)
Management
Resuscitation of patient– 2 large bore branulas (at least 18G)– IV fluid replacement, preferably crystalloids– blood for GXM and Hb level– CBD for measuring urine output

Macafee Regime
Patient must be in a hospital with facilities for immediate CS
Blood at least 4 units must be available at all time
Anaemia must be correctedMonitoring of maternal and fetal wellbeing
– including dexamethasone for lung maturity
Delivery
Try to bring to 38 weeks POA as possibleMajor PP - CSMinor PP- vaginal delivery is possible
especially the anterior typeHowever, if the bleeding is profuse ,
delivery must be done at any gestation in order to save the maternal life.
Complications of Placenta praevia
Postpartum haemorrhage:– placenta accreta– uterine atony– poor haemostasis because lower segment has
less smooth muscle therefore contraction is poor.
Recurrence of Placenta praevia in next pregnancy


ABRUPTIO PLACENTA

DEFINITION
Premature separation of a normally situated placenta
Blood clotplacenta
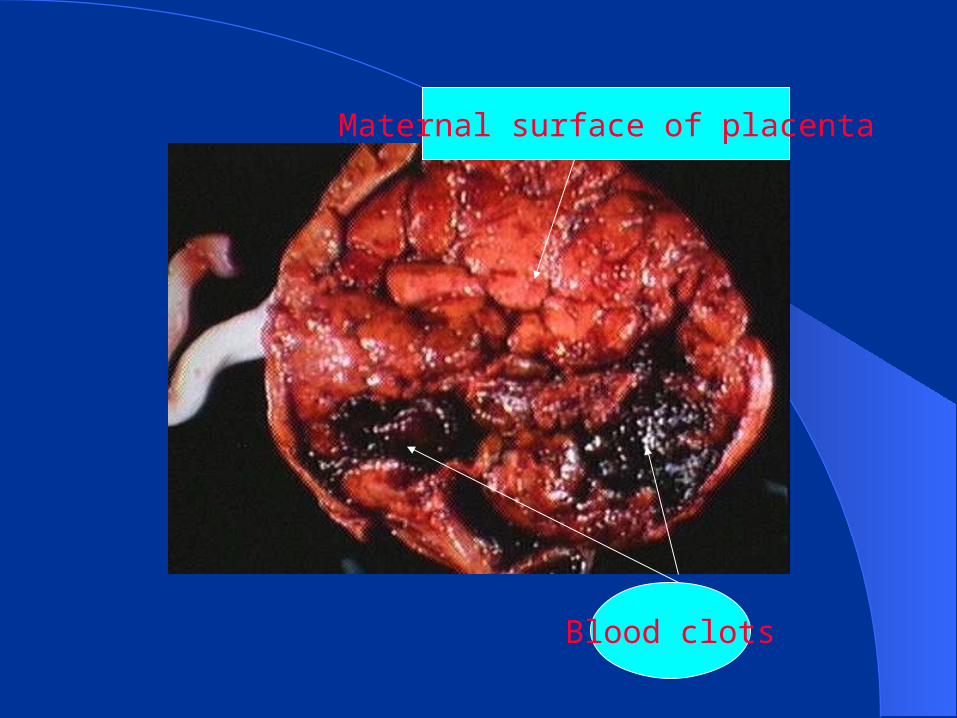
Maternal surface of placenta
Blood clots

Causes
UnknownAssociated with:
– elderly and multipara– hypertension– poor placentation (diminished adhesiveness to
the uterine wall)– trauma (to abdominal wall,external cephalic
version or cordocentesis)

Causes
– Smoking cocaine– sudden decompression of uterus i.e. in
polyhydramnios– fibroids– multiple pregnancy– ? Folate deficiency

HOW DO THEY PRESENT?
History of painful PV bleedingLoss of consciousness/syncopal attackReduced or no fetal movementMaybe history of trauma before

Physical examination
Pale not appropriate with amount of bleeding seen
Hypovolumic shockBP high or normal if it is associated with
hypertensionUterus is tender and rigidUterus can be larger or equal to date
Physical examination-cont...
Fetal parts not felt wellFetal heart absentAmniotomy noted blood stained liquor
How to diagnose?
Basically on clinical judgementUltrasound plays a small role in achieving
diagnosisIt is only confirmed by demonstrating a
retroplacental clot after delivery of placenta
Management
ResuscitationCorrect coagulopathyEarly deliveryClose monitoring of maternal vital signAdequate analgesiaAssessment of fetal condition

Delivery
C S / S V D
A live +N o D IV C
correc t D IV C +C S / S V D
A live +D IV C
C orrec t D IV C +S V D
D ead +D IV C
M od e o fd e live ry
Complications
Fetal demiseAcute renal tubular or cortical necrosisRecurrenceSevere DIVCPostpartum haemorrhage
– uterine atony– couvelaire uterus (insufficient contraction )
Indeterminate APH
Undetermined cause of bleeding Usually originating from placentaFrequently associated with circumvallate
placenta



Vasa praevia
RareUsually intrapartum rather than antepartumFetal exsanguination is rapidVelamentous insertion of cord
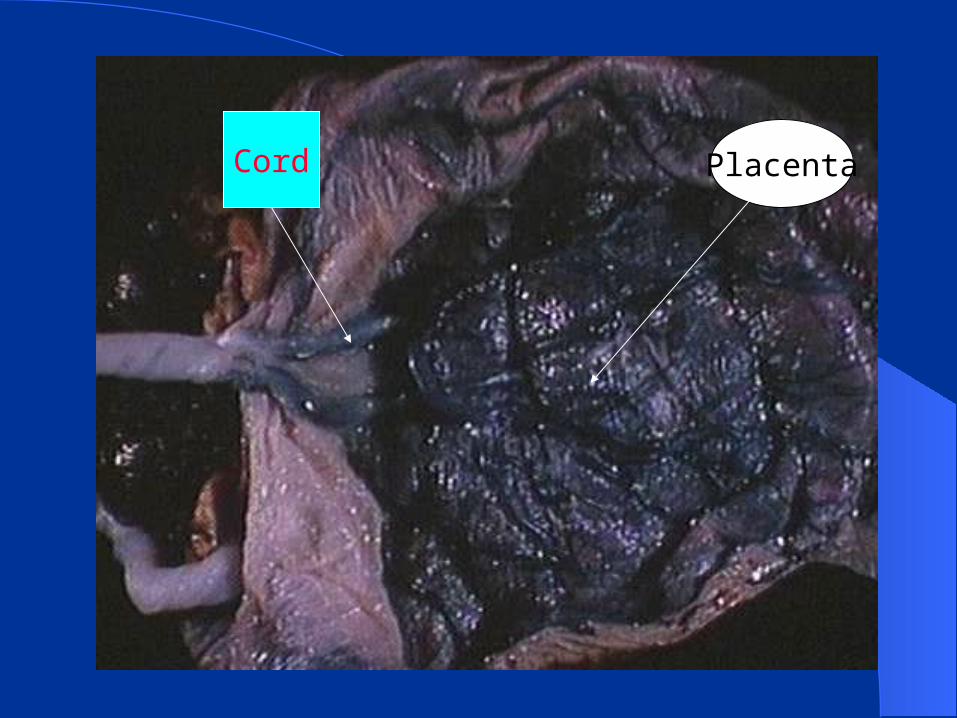
PlacentaCord
Vasa praevia_ cont…..
Fetal distressDelivery via CSDiagnosis is confirmed by Kleihaeur test

THAT’S ALL FOLKS!
The rest you read on your own
That’s all,the rest please read on your own


















