Rheumatic fever & acute rheumatic heart disease Rheumatic fever & acute rheumatic heart disease

Acute rheumatic fever
Index
1. Definition
2. Prevalance
3. Causes
4. Pathology
5. Clinical manifestation
6. Diagnosis
7. Differential diagnosis
8. Clinical course
9. Management
10. Prognosis
11. Prevention
DEFINITION
1. Rheumatic fever is the leading cause of acquired heart disease in children worldwide.
2. Initiated by a pharyngeal infection with group A beta-hemolytic streptococci (GAS)
3. latent period of approximately 2 to 3 weeks,
4. characterized by acute inflammation of the heart, joints, skin, subcutaneous tissue, and
central nervous system.
5. Pathologically, the inflammatory process causes damage to collagen fibrils and
connective tissue ground substance (i.e., fibrinoid degeneration),
6. connective tissue or collagen vascular disease.
Disease burden
1. incidence varies by socioeconomic development
2. annual incidence ranges between 8 and 51/1,00,000 among children and young people
3. Incidence remains high in the South Pacific, Australia and New Zealand
4. Not known in large parts of Africa and Asia because of the absence of regional data


True incidence of ARF
1. Needs systematic and active surveillance of children and young people in the community
2. Active disease specific surveillance is costly
3. SUBCLINICAL RHD detected by ECHO -> intermediate stage before development of
clinical disease
4. Also correlates with ARF incidence
5. Less costly, more feasible, repeatable, can be used as screening for locally representative
data and for targeted implementation of preventive programmes
Nomenclature of cardiac involvement in acute rheumatic fever and RHD 1. SUBCLINICAL CARDITIS - e/o valvular involvement by ECHO within 12 weeks of
onset of symptoms of ARF
2. SUBCLINICAL RHD - Rheumatic valvular HD detected on ECHO screening of
asymptomatic population
3. MISSED CLINICAL RHD – moderate and severe lesions detected incidentally but
evident on clinical examination
4. CLINICAL RHD – when symptomatic patients seek medical care.

Cause
1. Attributes of GABHS
2. GABHS M serotypes 1,3,5,6,14,18,19,24,27,29
a. Not associated with M 2,4,28
3. Only throat infection/ pharyngitis
4. Strains rich in M protein induce marked immune response and probably share
epitopes with human tissue
5. Recently, mucoid producing strains were found to be more rheumatogenic
Group A Streptococci: Cell wall Components of Clinical Interest
1. Capsule: Hyaluronic Acid: Non antigenic
2. Cell Wall:
I. Surface Protein:
i. M protein: Type Specific Antigen: Virulence factor
II. Group A carbohydrate: N acetyl glucosamine+ Rhamnose: Group specific
antigen: Lancefield classification
3. Mucopeptides: common to many bacteriae
I. N Acetyl glucosamine
II. N Acetyl muramic acid
PATHOGENESIS
• Incompletely understood
• An autoimmune response to pharyngeal infection with GAS in genetically predisposed
individuals, mediated through molecular mimicry
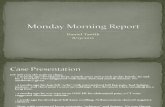
Conjunctivitis
Coryza
Hoarseness,
cough
Diarrhoea
Characteristic exanthems

Sudden onset
sore throat
Pain on swallowing
Fever
Tonsillo
Pharyngeal
exudates
Soft palate
petechiae
Red swollen
Uvula
Tender anterior
cervical nodes
• The theory of molecular mimicry holds that GAS pharyngitis triggers an
autoimmune response to epitopes in the organism that cross-react with similar
epitopes in the heart, brain, joints and skin, and repeated episodes of rheumatic
fever lead to RHD
• Inflammation leads to neovascularisation and healing by fibrosis, causing characteristic
valve lesions of RHD.
• Antibodies against GAS N-acetyl-beta-D-glucosamine cross react with neuronal cells in
basal ganglia causing excess release of dopamine -> chorea
• Accumulation of immune complexes cause transient, migratory joint manifestations
PATHOLOGY OF HUMAN TISSUE INVOLVEMENT
Skin, synovium, brain:
1. Inflammation is self limiting and heal without residua
2. Edema, inflammation and infiltration with predominant lymphocytes, few
neutrophils.
3. Perivascular inflammatory lesions
4. Subcutaneous nodules have central fibrinoid necrosis surrounded by inflammatory
reaction

CARDIAC INVOLVEMENT
1. The histopathologic findings in myocardium include the “pathognomonic” Aschoff
nodule
a. -found in the subendocardial or perivascular regions in the myocardium.
2. Little histopathologic damage to the myocardium, even in patients with florid clinical
carditis and heart failure.
3. Myocyte necrosis is uncommon, and the cellular infiltrate is confined to the interstitium.
4. This correlates with the lack of troponin leaks even in patients with frank rheumatic
myocarditis.
5. Progresses from exudative phase to fibrotic phase over 6 months
6. no marker is useful for active carditis
RISK FACTORS
1. People between 5 – 14 years
2. Incidence highest among children 10-14 years f/b 5-9 years
3. Poverty and social disadvantage- strongest predisposing factors
(OVERCROWDING)
4. Males = females (ARF) , Females > males (RHD)
5. Virulence of the strain and host susceptibility-important determinants


DIAGNOSIS OF ARF
1. MAJOR CRITERIA
2. MINOR CRITERIA
3. ESSENTIAL CRITERIA (e/o preceding GABHS infection)
Initial RF: 2 major / 1major + 2 minor
Recurrent RF: 2 Major/ 1 major + 2 minor / 3 minor
DIAGNOSIS
1. No single lab test or clinical feature is diagnostic
2. Most present with combination of FEVER, JOINT manifestations, and CARDIAC
involvement
3. Original JONES CRITERIA revised – to improve specificity
I. Risk stratification based on disease endemicity
II. Different implications of joint manifestations for different population
III. Acceptance of ECHO e/o carditis (SUBCLINICAL carditis)
IV. Diagnosing recurrent ARF
Essential criteria NOT required if:
• Chorea – Late presentation
• Indolent carditis – Late recognition
Risk stratification
• LOW RISK population
– Prevalence: ARF ≤ 2/100,000 school children.
- RHD < 1/1000 (all ages)
• Non-low risk: Considered as HIGH/MODERATE risk
• High sensitivity and High specificity




POSSIBLE” ARF

1. Clinical presentation may not fulfill the updated Jones criteria, but the clinician may still
have good reason to suspect ARF
2. High-incidence settings à use clinical judgement
3. AHA 2015 Guideline: “…. genuine uncertainty, it is reasonable to consider offering 12
months of secondary prophylaxis followed by reevaluation … include…. history and
physical examination in addition to a repeat echocardiogram.”
A retrospective study in North Queensland, Australia, investigated the impact of the
addition of subclinical carditis, monoarthritis, and low-grade fever (>37.5°C) to the 1992
revised Jones criteria
1. Of the 98 cases with a clinical diagnosis of ARF, only 71.4% met the revised Jones
criteria.
2. Modification of the criteria, as discussed above, increased the proportion of the cases
that satisfied diagnostic criteria to 91.8%.
3. Of the 28 people who did not meet the traditional Jones criteria, 12 (42%) developed
evidence of chronic RHD.
4. Addition of monoarthritis and subclinical carditis as major manifestations and low-grade
fever as a minor manifestation to the Jones criteria could increase sensitivity when
applied specifically to high-risk populations.
Carditis
1. major criteria
2. Most serious manifestation of ARF
3. May lead to RHD and complications like AF, Stroke, IE, CHF and death
4. 90-92% in <3years, 50% in 3-6, 32% in 14-17 and 15% in adults
5. Signs and symptoms depend upon involvement of pericardium, myocardium and heart
valves
6. Occurs in first 2 weeks of ARF
7. PAN-Carditis:
• Endocardium
• Myocardium

• Epicardium
8. Frequency:
• 60-90%
• Method of eval – clinical/echo doppler
• First attack - recurrent
9. Clinical Carditis
10. Subclinical Carditis (Echo Carditis)
11. Indolent Carditis
12. Recurrent Carditis
13. Symptoms
14. Tachycardia – out of proportion to fever
• 10C à 10bpm
15. Auscultation – Regurgitation murmurs
MR/TR/AR
• Echo-doppler: sub-clinical (echo carditis)
• 92 – 95% : MV involvement
• 70 – 75% : Isolated MV
• 20 – 25% : Aortic valve involvement (along with MV)
• 5 – 8 % : Isolated AV
• Involvement of TV : Rare (<10%)
• Always along with MV
• Involvement of all cardiac valves
• Reported, but extremely rare
• Severity of carditis – clinical:
• Cardiac murmurs

• Cardiomegaly
• CHF
• Pericardial rub
• Diagnostic/Therapeutic relevance
• Long term prognosis on valvular status & CRHD
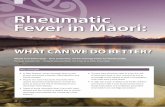
CARDITIS THROUGH THE YEARS
2015 AHA Update to Jones Criteria for diagnosis of RF. Circ 2015

INDOLENT CARDITIS
• Evidence of Carditis:
» Insidious onset
» Slow progression (less aggressive)
» Milder forms (asymptomatic/Mild symptoms)
» Active inflammation
– Not recognised/late recognition during routine check-up for incidental illness
– Essential criteria NOT required – Late presentation
RECURRENT CARDITIS
• Established CRHD
• Recurrence of ARF – Carditis
– Onset of new cardiac murmur

– Pericarditis
– Onset of heart failure (worsening of valvular lesion)
• Signs of inflammation +
• Essential criteria is mandatory
• r/o SBE
ARF- PERCARDITIS
• 6 – 15% ARF
• Clinical diagnosis – symptoms
• Always associated with valvulitis – MR/AR
• Effusion – infrequent
• Tampondae – rare
• Indicates severe carditis
– Regression of valve disease less likely
ARF MYOCARDITIS
• No Evidence of myocarditis
– Cardiac biomarkers
– Systolic function – Echo
– Cardiac biopsy: No e/o cellular necrosis
– CE – due to severe valvular regurgitation, not due to myocarditis – surgical
correction of MR – reversal of CE


What do we do when abnormal Echo Doppler findings are picked up during screening/
health survey/ Epidemiological study: Guide lines
• Definite RHD
• Borderline RHD
• WHY : In endemic areas, even in absence of past ARF, echo features of RHD call for
secondary prophylaxis against rheumatic fever, as prevention of repeated attacks of ARF
can protect the individual from severe / continuing valve damage and is cost effective
Migratory Polyarthritis
• Earliest manifestation
• Sequential involvement of joint with inflammation resolving in one and beginning in
other
• May be additive
• If not treated, may involve 6-16 joints

• If persists for >4weeks, consider other diagnosis
• Co-relate with peak ASO titre
• 75% patient larger joint ( knee,ankle,wrist,elbow)
• Responds promptly to low dose of salicylates
• Joints are never deforming (exception- JACCOUD’s arthritis)
• Inverse relationship b/w severity of arthritis and cardiac involvement
JACCOUD’s arthritis or Arthropathy
• Chronic post rheumatic fever arthropathy
• After repeated attacks of ARF, recurrent inflammation of fibrous articular capsule
• Ulnar deviation of fourth and fifth fingers, flexion of MCP, hyper extension of PIP
• Correctable
• No true erosions on radiography
• RA factor negative
Differential Diagnosis:
• Post streptococcal reactive arthritis
• Septic arthritis
• Infective Endocarditis
• Lyme’s disease
• Leukaemia/lymphoma
• Viral arthropathy
• Sickle cell disease
Chorea
• 10-15% patient
• More common in females, even more after puberty

• Latent period is longer ( GAS infection to chorea) 6-8 weeks
• Involuntary, purposeless, jerky movements of hands, arms, shoulders, feet, legs, face and
trunk a/w hypotonia and weakness
• Interferes with voluntary activity and disappears during sleep
• May be unilateral (hemichorea)
Evaluation of chorea – MOTOR IMPERSISTENCE
• Demonstration of milkmaid grip- repetitive, irregular squeezes
• Spooning & pronation of hands
• Wormian darting movement of tongue upon pronation- involuntarily, intermittently
withdrawing the tongue when attempted to protrude for 30 seconds (JACK-IN-BOX)
• Emotional lability – inappropriate behaviour, personality changes, restlessness, outbursts
of laughter and crying
• May last for 1week to 2 years but usually 8-15 weeks
• When only manifestation – CRP, ESR, Ab titres are normal
• D/D – involuntary jerks of Tourette’s syndrome, PANDAS
Erythema marginatum
• Rare , only in 1% of patient
• Characteristics rash of ARF
• Evanascent, pink, extends centrifugally whole centre returns to normal, serpiginous
border
• Non pruritic
• Mainly on the trunk& extremities , not on face
• May become prominent after hot shower

Sub cutaneous nodules
• < 1 % of patient
• Along the extensor surface of tendon near bony prominence
• With prolonged active carditis rather than acute stages of ARF
• Firm, painless, app. 1cm, freely movable over subcutaneous tissue
• May persist for weeks
• Multiple crops are related to severity
Supporting evidence of antecedent group A streptococcal infection
• Positive throat culture or rapid streptococcal antigen test
• Elevated or increasing streptococcal antibody titre
Treatment
• Bed rest
• Monitoring for evidence of carditis
• ANTIBIOTIC THERAPY :
1. 10 days of oral penicillin or amoxicillin
2. Single intramuscular injection of benzathine
If allergic to penicillin give erythromycin( 10), azithromycin (5)

• Without secondary prophylaxis, recurrence is maximum in first five years and minimal beyond
15 years.
– < 5 years : 20%
– 5 – 10 years : 10%
– 10 – 15 years : 5%
– > 15 years : 2%
• Duration of secondary prophylaxis depends on:
– Presence of carditis during initial attack of RF
– Age of patient – infrequent > 45 yrs
– Severity of valve disease
– Duration after last episode of RF

RECURRENCE DESPITE PROPHYLAXIS
ANTI-INFLAMMATORY THERAPY
• Patient with typical migratory polyarthritis & carditis without cardiomegaly or CHF
• Aspirin 50-70mg/kg/day in 4 divided dose for 3-5 days
• f/b 50mg/kg/day for 3 week then half dose for another 2-4 week
• Patient with carditis & more than minimal cardiomegaly & or CHF
• Prednisone -2mg/kg/day in QID foe 2-3 wks f/b half dose for 2-3 wks
• Then tapering dose by 5mg/24hour every 2-3 days and along with this aspirin should be
started to prevent rebound inflammation

Sydenham chorea
• It occurs as isolated manifestation after acute phase
• Sedatives may be given
• Phenobarbitol is DOC
• Haloperidol or chlorpromazine
Complication
• Arthritis and chorea resolve completely without sequelae
Prevention
• Primary prevention : Prevention of initial attack, appropriate antibiotics should be given
before 9th day of symptoms of acute GAS pharyngitis.

• Secondary prevention- Prevention of acute GAS pharyngitis in patients at substantial
risk of ARF
Anti Streptococcal Vaccines
For mass primary prophylaxis against GABHS
• Target Antigen: M-Protein
• Type specific: N-Terminal region
• Protects against specific serotype
• Devoid of homology with human myocardial tissue
• Need polyvalent vaccine to cover all possible serological groups
• Carboxy terminal region( highly conserved): Protects against multiple serological groups
• Cross reaction with human tissue uncertain
Vaccine using Non M protein moieties
• Streptococcal C5a peptidase( similar antigen in several serotypes)
• Low risk of cross reactivity with human tissue
• Protects against several M serotypes
• Streptococcal extra cellular protease vaccine using strep. Pyrogenic exotoxin