ABC Urinary Incontinence Dr Tim Chang MBBS(SYD), FRANZCOG Gynaecologist, Endoscopic surgeon and IVF...
84
ABC Urinary Incontinence Dr Tim Chang MBBS(SYD), FRANZCOG Gynaecologist, Endoscopic surgeon and IVF Fertility specialist Dr. Christiane Mayer MD, FRANZCOG Obstetrician and Gynaecologist, 139 Dumaresq street Campbelltown
-
Upload
kristina-miller -
Category
Documents
-
view
218 -
download
4
Transcript of ABC Urinary Incontinence Dr Tim Chang MBBS(SYD), FRANZCOG Gynaecologist, Endoscopic surgeon and IVF...

ABC Urinary Incontinence
Dr Tim ChangMBBS(SYD), FRANZCOG
Gynaecologist, Endoscopic surgeon and IVF Fertility specialist
Dr. Christiane MayerMD, FRANZCOG
Obstetrician and Gynaecologist,
139 Dumaresq street
Campbelltown

ABC in Female Urinary Incontinence
Christiane MayerMD, FRANZCOG
Obstetrician & Gynaecologist

Overview
• Epidemiology
• Definition and Classification
• Etiology
• Assessment and Evaluation
• Treatment (non surgical)


Learning objectivesFeel more confidence in assessing female Pts with urinary
incontinence +/- POP Identify keyfactors in establishing a basic diagnosisUnderstand the principles of management and treatmentoptions
available for UI Ability to select which patients are appropriate for non surgical Rx
and when to refer to Specialist

Epidemiology of Urinary Incontinence
• Prevalence • Community – 8 to 41%• Nursing Home – 40 to 70%
• Incidence• 20% over a one-year period

Relationship to age
• Risk of developing incontinence increases with age:
• 10% age 45 – 49 yrs
• 20% age 60 – 64 yrs
• 32% age 70 – 74 yrs

Impact on health• QOL : depression and anxiety, low self esteem, work impairment,
social isolation
• Morbidity: perineal infections, falls and fractures, admission to hospital/nursing homes
• Sexual dysfunction: coital incontinence may affect up to one third of women with UI (Urgency UI)

Economic Impact
• Total Cost – 16.4 billion dollars • Community – 11.2 billion• Nursing Home – 5.2 billion
• Greatest cost is for care and supplies such as laundry, pads and nappies
• Less cost for diagnosis and treatment

Underreported because of….
• Embarrassment
• A belief it is part of aging
• Health care providers don’t ask!!
• Fear of treatment/therapy

Urinary incontinence is NEVER normal!!

Definition of Urinary Incontinence
• Any involuntary leakage of urine in sufficient amount or frequency to cause a social and/or healthproblem
Abrams P et al. Neurourol Urodyn 2002;21:167-78.

Types of Urinary Incontinence
• Stress Incontinence•Urgency Incontinence•Mixed Incontinence•Overflow Incontinence

Anatomy and Physiology of Micturition• 1.Filling and storage
• 2.Expulsion of urine MicturitionreflexWhen bladder volume reaches ~ 400mls, stretch receptors of the bladder wall relay a message to the brain, which returns an impulse message for voiding back to the bladder. In response the detrusor muscle contracts and the urethral sphincter relaxes to allow micturition.

• Intact lower urinary tract• Intact neurological control• Cognitive ability • Functional ability/mobility• Motivation• Environmental factors
Continence requires

Stress Urinary Incontinence
• The complaint of involuntary leakage with increased intraabdominal pressure:
exertion, sneezing, laughing or coughing
• Highest incidence in women ages 45-49

Riskfactors for Female SUIParity (Pregnancy + vaginal birth)
Obesity
Chron. constipation
Chron. cough, COPD
Aging (lower E2 levels)
High impact physical activity

Etiology of Female SUI (Anatomic)

Urethral hypermobility and bladder neck funneling
• Caused by insufficient support of urethra and bladder neck by pelvic floor muscles and vaginal connective tissue
unability of urethra to close completely
leakage (“like stepping on a hose in sand”)

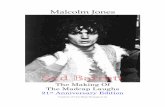
Etiology of Female SUI (ISD)
Delancey JOL. World J Urol 2007;15:268.

Mild Severe
Stress Incontinence Severity
Hypermobility Intrinsic SphincterDeficiency

ISD
• Neuromuscular damage of urethral sphincter with loss of tone
• Possibly after multiple surgeries
• Severe leakage at rest or during minimal exertion
• Challenging to treat and poor surgical outcome

Urge Urinary Incontinence
• The complaint of involuntary leakage accompanied by or immediately preceded by sudden and strong urge to void
• Detrusor overactivity DO : involuntary detrusor muscle contractions during bladder filling
• Overactive Bladder Syndrome OAB : urgency, frequency, nocturia +/- incontinence( OAB wet and OAB dry)
• Highest incidence in women > 65 yrs

Causes for UUI
• Age ( decreased ability to inhibit contractions, decreased bladder capacity, urogenital atrophia….)
• Neurologic disorders ( CNS inhibitory pathways interrupted)
• Bladder abnormalities
• idiopathic

Mixed Urinary Incontinence
• The complaint of involuntary leakage associated with urgency AND also with exertion, effort, sneezing or coughing
• Overlap of DO and impaired urethral sphincter function
• Very common

Overflow Incontinence
• Any involuntary loss of urine associated with overdistention of the bladder
• Continuos leakage or “dribbling” on B/o incomplete bladder emptying

Overflow Incontinence• Detrusor underactivity:
- older women (5-10%)
- low estrogen state
- peripheral neuropathy (DM, Vit B12 def., ETOH)
- spinal cord damage (MS, spinal stenosis…)
• Bladder outlet obstruction
- fibroids, advanced pelvic prolapse (beyond hymen), obstructing tumours….

Transient incontinence• Associated with reversible conditions (acute onset)
D I A P P E R S • Delirium• Infection• Atrophic vaginitis• Pharmaceuticals• Psychological• Excess urine output(endocrine)• Reduced mobility• Stool impaction

Evaluation of Urinary Incontinence
• Patient History !! • Voiding Diary• Physical Examination• Cough Stress Test• Urinalysis
• Post Void Residual Volume

Patient History
• Urinary Symptoms• Stress Incontinence
• 1) Do you leak urine when you cough, sneeze or laugh?• 2) Do you leak upon standing or walking?• 3) How often do you experience leakage?• 4) How much do you leak? Do you wear a pad?

Patient History
• Urinary Symptoms• Urge Incontinence
• 1) How many times a day do you void? (frequency - > 8 voids in 24 hours)• 2) Do you ever have a strong urge to void such that you feel you may leak? (urgency)• 3) Do you ever leak before reaching the toilet? (urge incontinence) • 4) How many times at night are you awakened by the need to urinate? (nocturia - > or =
to 1 time per night)• 5) Do you ever wet the bed? (nocturnal enuresis)• 6) Do you wear a pad?

Patient History
• Urinary Symptoms • Overflow Incontinence
• 1) Do you feel that your stream is adequate?• 2) Do you feel that you fully empty your bladder?• 3) Do you wear a pad?

Patient History
• Medications• Alpha-adrenergic agonists (urinary retention)• Alpha-adrenergic blockers (stress incontinence)• Anticholinergic agents (urinary retention)• Antidepressants (urinary retention)• Beta-adrenergic agonists (urinary retention)• Calcium-channel blockers (urinary retention)• Diuretics (frequency)

Patient History
• Obstetric Hx• Medical Hx• DM, CVA, dementia, MS, parkinsonism
• Past Surgical Hx• gynecologic, anti-incontinence
• Social Hx• tobacco, caffeine, occupation
Impact on QOL incl. sexual activity


Physical Examination
• Weight/BMI• Abdomen exclude mass
• VE : atrophic changes
pelvic organ prolapsepelvic massurethral caruncleperineum
• Rectal: tone of sphincter, faecal impaction
• Neurological/Mental state

UI & POP Pelvic Organ Prolapse
• POP may be seen in 50% of parous women• Common in women with UI• Symptomatic or asymptomatic• Similar RF as to Stress Incontinence: parity age/menopause obesity ( chron. increased IAP) genetics (tissue!) previous Hysterectomy

Cough Stress Test
• Performed with comfortable full bladder standing or in dorsal lithotomy
• Observation of leakage with a strong cough
• helps to confirm stress incontinence

Urinalysis
• Urine sampled to rule out the following:• UTI• haematuria
• rule out stones • rule out tumor• confirm by microscopic analysis• send for cytology!

Post Void Residual Volume
• Measurement of residual urine in bladder immediately after voiding through catheter placement or U/S
• A volume of > 150 cc may be associated with voiding dysfunction and predisposes to overflow incontinence and UTI’s
• Helpful for Pts with: severe POP/outlet obstruction
hx of retention (medication!)
neurology. diseases/neuropathy
recurrent UTIs

Urodynamics
• Not part of initial evaluation and unnecessary to initiate Rx
• Mixed incontinence
• Recurrent incontinence
• Voiding dysfunction
• Overflow incontinence
• Prior to intervention!

Initial Management
• “ A journey of a thousand miles begins with one step ” ……(or one drop) Lao-tse
• For ALL Pts with SUI/UUI/mixed UI:
• Lifestyle modifications• Pelvic floor muscle exercises PFMT

General Management
• Behavioral
• Medical
• Surgical (SUI)

Lifestyle• Loose weight
• Reduce caffeine (tea!)
• Normalise fluid intake ~ 1.5/2 l (incl. soups, watery fruits…)
• Avoid constipation
• Avoid evening fluids
• Reduce /Stop smoking
• Cranberry juice if h/o UTIs

PFMT/Kegel Contractions
• Exercises of the pelvic floor musculature
• 10 deliberate, quick, hard contractions of 10 second duration (“ same muscles as you would stop the urine flow or gas ”)
• 3 times a day
• At least 4 - 6/12

Additional support
• Supervision by Physiotherapist Cochrane 2012
• Vaginal cones
• Biofeedback• Useful if unable to isolate pelvic floor• Vaginal pressure sensor provides audible/visual feedback of strength
of pelvic contractions• Can be done using electrical stimulation• 1-2 times a week for 6 weeks

Overall Effectiveness of Conservative Therapy
• Cochrane R/V 2014
• Meta-analysis including 21 trials (n 1281)
• PFMT better than placebo
• Strong recommendation based on intermediate quality evidence
• Questionable durability of effect

Non-surgical Treatment of SUI
• Behavioural Rx :Timed voiding to maintain an empty bladder (independent of
urge)• Topical/vaginal estrogen : if atrophia in peri/postmenopausal women
• Pharmacotherapy
• Vaginal (Incontinence)Pessaries

Medical Therapy for SUI• Duloxetine Hydrochloride
Inhibits reuptake of serotonin and norepinephrine
Enhances urethral function in animal models Systematic R/V 2012 similar to placebo
• Alpha- agonists : stimulate urethral muscle
not longer recommended

Treatment of Urgency Incontinence
• Behavioural Rx = Bladder training
• Topical estrogen : if atrophia in peri/postmenopausal women
• Medical/Pharmacotherapy

Treatment of Urgency Incontinence
• Bladder Retraining:• Aim to increase again bladder capacity• Timed voiding (voiding diary) by clock• Slowly increase intervals• “freeze and squeeze”• Stop going “just in case”• At least 3/12

Medical Treatment of OAB
• Anticholinergica
• Antimuscarinics:• Blocked release of Acetylcholin during bladder filling( inhibits detrusor &
decreased urge) via muscarinic receptors• Compared to placebo >40 % rate improvement• Limited use due to S/E (dry mouth, constipation, cognitive impact)• Low dose slowly increase over few weeks• Check for urinary retention!

Medical Treatment of OAB
• Antimuscarinics:• Oxybutynin IR (Ditropan) = non selective • Oxybutynin ER 5-10 mg daily• Oxytrol (transdermal patch) twice weekly – reduced S/E
• Tolterodine(Detrol LA)= selective 2 mg daily
• Solifenacin(Vesicare) 5 mg daily

Medical Treatment of OAB
• Mirabegron (Betmiga)• Beta3 receptor- agonist• Used if bothersome S/E of Antimuscarinics• Or Contraindications (narrow angle glaucoma)• Similar effective in studies• Started 25 mg daily, up to 50 mg daily• Not to be used if severe or uncontrolled HT!

Treatment of Overflowincontinence
• Treat underlying etiology - POP pessaries/surgery- change meds- topical estrogen- DM control…..• Challenging to treat• Double voiding• Intermittent self catheterisation

UI & Pelvic Organ Prolapse
• POP-Q assessment stage 0 – 4• Treatment
conservative : PFMEtopical Estrogen(Incontinence)Pessaries
surgical repair + incontinence surgery
• Urodynamics prior to surgery!

When to refer to Specialist
• Uncertain diagnosis• Haematuria in absence of UTI• Significant POP• Failed initial Rx• Pelvic pain• B/o complex neurological conditions• Recurrent UI after incontinence surgery• Post radiation, suspected fistula

Summary


Thank you !

Surgical Management of Urinary Incontinence
Tim ChangMBBS(SYD), FRANZCOG
Gynaecologist, Endoscopic surgeon and IVF Fertility specialist
139 Dumaresq street
Campbelltown

Management of Incontinence
• Cause• Severity• Patient expectations• Patient risk factors / co morbidities
Benefits and risks need to be aligned with patient expectations

Management of Incontinence
Womens perception of success of IC treatment based predominantly on reduction in IC episodes and other QoL measures rather than any
special testing

Indications for referral
• Failed conservative therapy and contemplating surgery• Haematuria without infection• Elevated PVR• Significant pain• Significant prolapse or pelvic masses• Suspected fistula• Suspected neurological condition• Uncertain diagnosis

Stress Incontinence

Conservative therapy
• Mild/moderate Incontinence• Motivated patient• Desires future pregnancies• Unsuitable for surgery

Surgery
• Severe Urinary Stress Incontinece• Failed conservative therapy• Patient preference

Surgery for Stress IC
• Surgery offers high rates of cure for USI (80-90% vs 40-60% with conservative treatments)• Minimal invasive sling procedures have lead to increase surgical
treatment for IC from 0.8/1000 women in 1979 to 1.0/1000 women 2006.• Ideally women should finished childbearing prior to anti-incontinence
surgery

Choice of Surgery for Stress IC
• Need for other procedures e.g hysterectomy• Coexisting prolapse• ISD• Medical status patient including age• Previous anti-incontinence surgery• Skill surgeon

Factors associated with failure of surgery
• DI present (60% success for overall IC cure)• ISD (retropubic sling preferred)• Obesity• Chronic lung disease• Previous surgery • Hypoestrogenism/Poor nutrition/Advanced age

Types of surgery
• Mid Urethral Slings• Colposuspension • Bladder neck slings

Midurethral Slings
• Revolutionised surgical treatment IC• Polypropylene tape• Vaginal procedure• Sling placed using trocars• Support the midurethra

Midurethral sling types
• Retropubic • Transobturator• Minislings

Retropubic slings
• Introduced 1990s• Vagina up or Suprapubic down
approach• Surgical time 30 minutes• Hospital stay day surgery -1 day• Return normal activities 2 weeks

Complications Retropubic tapes
• Haemorrhage• Venous plexus 2%• Vascular 1/1000
• Viscus injury• Bladder 4%• Bowel 1/1000
• Retention 2%• Voiding dysfunction 5%• UTI 5%• DI 7%• Erosion 1%

Transobturator slings

Transobturator sling
• Introduced 2001• Similar efficacy• Inside out or outside in approaches• Reduced viscus + visceral injury• Decreased retention / voiding dysfunction• Groin pain

Minislings
• Microinvasive ( single incision) surgery• Aim to further reduced morbidity of
surgery• Day surgery• Return to normal activities after 48 hours• 90% efficacy (follow up data 18 months)

Intrinsic Urethral Sphincter deficiency (ISD)
• Urodynamic diagnosis• MUCP <20cm H20 VLPP <60• Retropubic approach preferred to transobturator• Periurethral injections• Artifical Urinary Sphincter

Detrusor Instability
• Bladder retraining• Estrogens• Antimuscarinics• Selective β agonist• Botox• Sacral Modulation• Cystoplasty

Botox DI
• Failed drug therapy• Improved urinary symptoms 70% • Continence rates 60% • Voiding dysfunction 40% (up to 10% symptomatic)• Lasts 6-9 months• On PBS urogynaecologist or urologist

Mixed Incontinece
• Behavioural therapy• Add drug therapy to maximally treat DI• Sling surgery
• 90% improves SI• 50% improves DI• 70% improves incontinence symptoms

Overflow Incontinece
• Bladder obstruction vs hypoactivebladder• Treat the aetiology if possible eg prolapse• SNM may be an option• Intermittent self catheterisation• Urine diversions

Summary
• Align patient expectations efficacy compared to morbidity• Midurethra slings treatment of choice• Botox management DI