907 GERD Alters the Functional Brain Connectivity Models Associated with Acid Stimulation
1
907 GERD Alters the Functional Brain Connectivity Models Associated with Acid Stimulation Mark Kern, Stephen J. Antonik, Rachel Mepani, Adeyemi Lawal, Reza Shaker Previous fMRI studies have documented in healthy controls and GERD patients activation of sensory/motor (SM), prefrontal (PF), anterior (AC) and posterior (PC) cingulate and insula (I) brain regions associated with esophageal acid perfusion. GERD was found to significantly amplify the volume and intensity of fMRI signals compared to controls. (Kern M, Am J Physiol 2004; 286(1):G174-81) The effects of GERD on the connectivity of cortical networks have not been studied. Aim: To compare the functional connectivity models of brain regions showing fMRI activation during esophageal acid perfusion in GERD patients and healthy controls. Methods: Structural Equation Modeling (SEM) was used to generate partial regres- sion coefficients representing the covariance among regional fMRI signals activated by eso- phageal acid perfusion. We studied 7 GERD patients (4 female, age range: 20-62 years) and 8 controls (4 female, age range: 22-40 years), during high spatial resolution fMRI scanning sequences. Brain images were acquired during alternating intervals of 0.1N HCl and saline perfusion of the distal esophagus. Grouped data was used in the SEM to yield maps showing significant (p<0.05, goodness-of-fit test) connectivity paths from a general network based on known anatomical connections among the brain regions. Results: There were substantial differences in the connectivity maps associated with esophageal acid perfusion in GERD compared to controls. As seen (Figure), arrows between regions show the direction of significant covariance. Partial regression coefficients for these paths represent a measure of the degree of correlation between the regions. For all network models, GERD connectivity was different than that of the controls. These differences were characterized by decreased connectivity between limbic and para-limbic structures like the AC and I as well as altered patterns of connectivity between PF, I and AC in GERD compared to controls. Conclusions: Models of brain connectivity associated with esophageal acid perfusion differ when comparing patients and controls suggesting alteration of the cerebral cortical networks associated with processing visceral sensory input in GERD. 908 Effects of Vagotomy On the Airway Responses to Esophageal Acidification Ivan M. Lang, Steven T. Haworth, Bidyut K. Medda, Robert Birkett, Reza Shaker In prior studies we found that esophageal acidification caused airway constriction, decreased tracheal mucociliary transport, and increased broncho-tracheal mucus output; but the mech- anisms of these responses are unknown. AIM: The aim of this study was to investigate the role of the vagus nerves in the airway responses to esophageal acidification. METHODS: Twenty seven cats were anesthetized (alpha-chloralose 50mg./kg, IP); eleven were used for investigation of airway constriction and sixteen for broncho-tracheal mucus secretion. In all cats the esophagus was cannulated at both ends, a gastric fistula was formed to drain gastric contents, and the trachea was cannulated. In 12 cats the vagus nerves were sectioned bilaterally. The esophagus was perfused at 1ml/min with either 0.1M PBS or 0.1N HCl. For airway constriction studies, the airway was dusted with tantalum powder during 5-7 ventilations at 2-3 times tidal volume. The bronchi were visualized and recorded using a micro-focal x-ray system and the diameters measured at a later date. For mucus output studies a PE50 tube was inserted into the airway through the tracheal cannula for about 12 cm and taped into position. The airway was perfused at 0.2ml/min using 0.9% NaCl and the perfusates collected every 10 minutes and analyzed at a later date for hexosamine content as a measure of mucus. RESULTS: Perfusion of the esophagus for 30 minutes with HCl significantly decreased (16 to 23%) airway diameters (P<0.05, N=5), and increased (73%) hexosamine output (P<0.05, N=10). Vagotomy (N=6) caused a significant increase (32%, P<0.05) in basal airway diameters, but had no effect (P>0.05, N=6) on basal hexosamine output. Vagotomy (N=6) significantly reduced (P<0.05) hexosamine output for the first 10 min period after HCl, but had no effect (P>0.05) on hexosamine output during the 60 min period after HCl (Table). CONCLUSIONS: The airway responses to esophageal acidification represent physiological responses. The vagus nerves mediate tonic contraction of airway smooth muscle and its response to esophageal acidification. The vagus nerves do not mediate the airway mucus secretory response to esophageal acidification. However, contraction of airway smooth mucle may facilitate the rapid output of mucus from airway mucus secreting glands and their ducts. Effect of Vagotomy on Airway Responses to HCl in Esophagus Values are mean ± SE (N); %∆, percent change; Hex, hexosamine output; Min, minutes; Dia, diameter; *, P<0.05 for effect of vagotomy using unpaired t-test. A-131 AGA Abstracts 909 Concurrent High-Resolution Impedance and Manometry: Validation of Intraluminal Pressure Gradients As a Predictor of Trans-Sphincteric Flow William J. Bulsiewicz, Sudip K. Ghosh, John E. Pandolfino, Albert Meek, Peter J. Kahrilas Background: High-resolution impedance manometry (HRIM) makes it possible to concur- rently assess esophageal motor activity and bolus transit through the esophagus and esophago- gastric junction (EGJ), providing a multi-factorial assessment of esophageal function. The focus of this study was to compare the flow permissive time determined from manometry with the interval of actual trans-EGJ flow measured using impedance. Methods: Ten 5 ml saline swallows were recorded in each of 16 asymptomatic controls with a solid state concurrent HRIM assembly (20Hz) incorporating 36 point sensors spaced at 1 cm intervals and 14 impedance recording rings (12 impedance measurements) spaced 2 cm apart (MMS, Enschede, Holland). Two impedance recording sites were positioned to record in the proximal esophagus and the transition zone, while 10 sites were positioned in the distal esophagus and across the EGJ into the stomach. Data were visualized using three modalities: (i) color isocontours of pressure overlaid with temporal line plot of impedance, (ii) color isocontours of impedance overlaid with spatial pressure variation plots to assess pressure gradients during trans-EGJ emptying, and (iii) spatial variation plots of impedance and pressure overlaid on each other to assess intrabolus pressure. The manometrically delineated flow permissive time (FPT) was defined as the interval during which a pressure gradient favorable for esophageal emptying existed across the EGJ. A new variable, the integrated flow time (IFT) was defined from the impedance data as the interval during which the maximum impedance within the EGJ reached ≤ 50% of the baseline impedance. Results: All 16 subjects tolerated the catheter without any significant discomfort. 23 of the 160 swallows had dropped peristalsis in the distal esophagus. One subject had 8 swallows with dropped peristalsis and was classified as aperistaltic. The average FPT and the IFT were calculated in the remaining 15 subjects (Figure). FPT, 3.1±0.1 s (SE) vs. IFT, 3.7±0.2 s. A strong correlation was observed between the two parameters (r 2 =0.76). The average intrabolus pressure during the IFT was 19.6±1.3 mmHg. None of the 23 swallows with impaired distal esophageal peristalsis showed complete bolus clearance. Conclusions: (i) HRIM with isocontour plots of impedance and manometry offers a novel technology to assess esophageal motor function and trans- EGJ emptying concurrently with bolus clearance. (ii) Flow permissive time calculated from trans-sphincteric pressure gradients correlates well with actual transphncteric flow as detected by high resolution impedance recordings. 910 Assessing Dysphagia During Esophageal Manometry: How Well Do Liquid and Solid Swallows Reproduce Patients' Symptoms? Daniel Pohl, Edoardo Savarino, Patrick Janiak, Michael Fried, Radu Tutuian Background: Esophageal motility abnormalities are often reported in patients with dysphagia undergoing esophageal manometry. Explaining patients symptoms based on esophageal manometry findings is challenging. Correlations between esophageal symptoms and mano- metry findings are underreported. Aim: To evaluate correlation between esophageal symp- toms and high resolution manometry findings. Methods: Patients presenting for esophageal manometry were asked to report severity and frequency of dysphagia during the last 2 weeks prior to testing (dysphagia score). Esophageal high resolution manometry (HRM) was performed using a 32-channel water-perfused system and included 10 water (10ml each) and 10 solid (bread) swallows. During esophageal manometry patients were asked after each swallow if they experienced dysphagia or not. Esophageal contractions were classified as normal, ineffective or simultaneous based on previously published criteria. Per-swallow analysis included correlation between dysphagia (yes/no) and manometric findings (normal/ ineffective/simultaneous). Per patient analysis included correlation between dysphagia score, % swallows reported as perceived and % manometric normal swallows. Results: Data from 81 manometries performed in 74 patients (43 F, 31 M, mean age 46.3; range 18-87 years) totalling 801 liquid and 782 solid swallows were included in the analysis. The per-swallow analysis for liquid swallows found manometric simultaneous and ineffective contractions more likely to be associated with symptoms (12/49; 24.5% and 21/125; 16.8% respectively) compared to manometric normal contractions (24/627; 3.8%). Similar results were noticed during solid swallow: symptomatic simultaneous contractions 30/136 (22.1%), ineffective contractions 36/208 (17.3%) and normal contractions 44/438 (10%). The per-patient analysis found significant (p<0.01) but moderate-poor correlations between dysphagia score and % swallows perceived during testing (r=0.399 liquid and r=0.409 solid swallows), between dysphagia score and % manometric normal contractions during liquid swallows (r=-0.357). Correlation between %swallows perceived during testing and % manometric normal swallows was significant (p<0.01) but poor (liquid swallows r=-0.368, solid swallows -0.268). Conclu- sion: While manometric characteristics of esophageal contractions play a role in the percep- tion of individual swallows, the proportion of manometric abnormal contractions is not solely responsible for the intensity of dysphagic symptoms. 911 In Vivo and In Vitro Characterization of Azd9343, a Novel GABA B Receptor Agonist and Reflux Inhibitor Anders Lehmann, Thomas Elebring, Jörgen Jensen, Jan P. Mattsson, Karolina A. Nilsson, Pirjo Saransaari, Sverker von Unge Transient lower esophageal sphincter relaxation (TLESR) is the predominant cause of gastroe- sophageal reflux and hence a target mechanism in the quest for new treatments for gastroeso- phageal reflux disease (GERD). Baclofen, a centrally acting GABA B receptor agonist, reduces TLESRs and inhibits reflux and GERD symptoms but is burdened by its CNS side-effect profile. This study describes the pharmacological profile of AZD9343, a novel GABA B receptor agonist. Methods: Potency and intrinsic activity were established in cells expressing human recombinant GABA B receptors, and competition with GABA in binding to native GABA B receptors was evaluated using rat brain membranes. Uptake of AZD9343 was measured in rat brain slices, and binding to the GABA transporter was studied in rat brain membranes. AGA Abstracts
Transcript of 907 GERD Alters the Functional Brain Connectivity Models Associated with Acid Stimulation

907
GERD Alters the Functional Brain Connectivity Models Associated with AcidStimulationMark Kern, Stephen J. Antonik, Rachel Mepani, Adeyemi Lawal, Reza Shaker
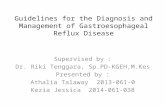
Previous fMRI studies have documented in healthy controls and GERD patients activationof sensory/motor (SM), prefrontal (PF), anterior (AC) and posterior (PC) cingulate and insula(I) brain regions associated with esophageal acid perfusion. GERD was found to significantlyamplify the volume and intensity of fMRI signals compared to controls. (Kern M, Am JPhysiol 2004; 286(1):G174-81) The effects of GERD on the connectivity of cortical networkshave not been studied. Aim: To compare the functional connectivity models of brain regionsshowing fMRI activation during esophageal acid perfusion in GERD patients and healthycontrols. Methods: Structural Equation Modeling (SEM) was used to generate partial regres-sion coefficients representing the covariance among regional fMRI signals activated by eso-phageal acid perfusion. We studied 7 GERD patients (4 female, age range: 20-62 years) and8 controls (4 female, age range: 22-40 years), during high spatial resolution fMRI scanningsequences. Brain images were acquired during alternating intervals of 0.1N HCl and salineperfusion of the distal esophagus. Grouped data was used in the SEM to yield maps showingsignificant (p<0.05, goodness-of-fit test) connectivity paths from a general network basedon known anatomical connections among the brain regions. Results: There were substantialdifferences in the connectivity maps associated with esophageal acid perfusion in GERDcompared to controls. As seen (Figure), arrows between regions show the direction ofsignificant covariance. Partial regression coefficients for these paths represent a measure ofthe degree of correlation between the regions. For all network models, GERD connectivitywas different than that of the controls. These differences were characterized by decreasedconnectivity between limbic and para-limbic structures like the AC and I as well as alteredpatterns of connectivity between PF, I and AC in GERD compared to controls. Conclusions:Models of brain connectivity associated with esophageal acid perfusion differ when comparingpatients and controls suggesting alteration of the cerebral cortical networks associated withprocessing visceral sensory input in GERD.
908
Effects of Vagotomy On the Airway Responses to Esophageal AcidificationIvan M. Lang, Steven T. Haworth, Bidyut K. Medda, Robert Birkett, Reza Shaker
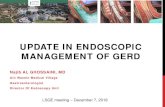
In prior studies we found that esophageal acidification caused airway constriction, decreasedtracheal mucociliary transport, and increased broncho-tracheal mucus output; but the mech-anisms of these responses are unknown. AIM: The aim of this study was to investigate therole of the vagus nerves in the airway responses to esophageal acidification. METHODS:Twenty seven cats were anesthetized (alpha-chloralose 50mg./kg, IP); eleven were used forinvestigation of airway constriction and sixteen for broncho-tracheal mucus secretion. In allcats the esophagus was cannulated at both ends, a gastric fistula was formed to drain gastriccontents, and the trachea was cannulated. In 12 cats the vagus nerves were sectionedbilaterally. The esophagus was perfused at 1ml/min with either 0.1M PBS or 0.1N HCl.For airway constriction studies, the airway was dusted with tantalum powder during 5-7ventilations at 2-3 times tidal volume. The bronchi were visualized and recorded using amicro-focal x-ray system and the diameters measured at a later date. For mucus outputstudies a PE50 tube was inserted into the airway through the tracheal cannula for about 12cm and taped into position. The airway was perfused at 0.2ml/min using 0.9% NaCl andthe perfusates collected every 10 minutes and analyzed at a later date for hexosamine contentas a measure of mucus. RESULTS: Perfusion of the esophagus for 30 minutes with HClsignificantly decreased (16 to 23%) airway diameters (P<0.05, N=5), and increased (73%)hexosamine output (P<0.05, N=10). Vagotomy (N=6) caused a significant increase (32%,P<0.05) in basal airway diameters, but had no effect (P>0.05, N=6) on basal hexosamineoutput. Vagotomy (N=6) significantly reduced (P<0.05) hexosamine output for the first 10min period after HCl, but had no effect (P>0.05) on hexosamine output during the 60 minperiod after HCl (Table). CONCLUSIONS: The airway responses to esophageal acidificationrepresent physiological responses. The vagus nerves mediate tonic contraction of airwaysmooth muscle and its response to esophageal acidification. The vagus nerves do not mediatethe airway mucus secretory response to esophageal acidification. However, contraction ofairway smooth mucle may facilitate the rapid output of mucus from airway mucus secretingglands and their ducts.Effect of Vagotomy on Airway Responses to HCl in Esophagus
Values are mean ± SE (N); %∆, percent change; Hex, hexosamine output; Min, minutes;Dia, diameter; *, P<0.05 for effect of vagotomy using unpaired t-test.
T : 11501$$CH204-02-08 16:47:05 Page 131Layout: 11501B : o
A-131 AGA Abstracts
909
Concurrent High-Resolution Impedance and Manometry: Validation ofIntraluminal Pressure Gradients As a Predictor of Trans-Sphincteric FlowWilliam J. Bulsiewicz, Sudip K. Ghosh, John E. Pandolfino, Albert Meek, Peter J. Kahrilas
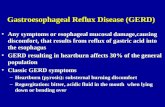
Background: High-resolution impedance manometry (HRIM) makes it possible to concur-rently assess esophageal motor activity and bolus transit through the esophagus and esophago-gastric junction (EGJ), providing a multi-factorial assessment of esophageal function. Thefocus of this study was to compare the flow permissive time determined from manometrywith the interval of actual trans-EGJ flow measured using impedance. Methods: Ten 5 mlsaline swallows were recorded in each of 16 asymptomatic controls with a solid stateconcurrent HRIM assembly (20Hz) incorporating 36 point sensors spaced at 1 cm intervalsand 14 impedance recording rings (12 impedance measurements) spaced 2 cm apart (MMS,Enschede, Holland). Two impedance recording sites were positioned to record in the proximalesophagus and the transition zone, while 10 sites were positioned in the distal esophagusand across the EGJ into the stomach. Data were visualized using three modalities: (i) colorisocontours of pressure overlaid with temporal line plot of impedance, (ii) color isocontoursof impedance overlaid with spatial pressure variation plots to assess pressure gradients duringtrans-EGJ emptying, and (iii) spatial variation plots of impedance and pressure overlaid oneach other to assess intrabolus pressure. The manometrically delineated flow permissivetime (FPT) was defined as the interval during which a pressure gradient favorable foresophageal emptying existed across the EGJ. A new variable, the integrated flow time (IFT)was defined from the impedance data as the interval during which the maximum impedancewithin the EGJ reached ≤ 50% of the baseline impedance. Results: All 16 subjects toleratedthe catheter without any significant discomfort. 23 of the 160 swallows had droppedperistalsis in the distal esophagus. One subject had 8 swallows with dropped peristalsis andwas classified as aperistaltic. The average FPT and the IFT were calculated in the remaining15 subjects (Figure). FPT, 3.1±0.1 s (SE) vs. IFT, 3.7±0.2 s. A strong correlation wasobserved between the two parameters (r2=0.76). The average intrabolus pressure during theIFT was 19.6±1.3 mmHg. None of the 23 swallows with impaired distal esophageal peristalsisshowed complete bolus clearance. Conclusions: (i) HRIM with isocontour plots of impedanceand manometry offers a novel technology to assess esophageal motor function and trans-EGJ emptying concurrently with bolus clearance. (ii) Flow permissive time calculated fromtrans-sphincteric pressure gradients correlates well with actual transphncteric flow as detectedby high resolution impedance recordings.
910
Assessing Dysphagia During Esophageal Manometry: How Well Do Liquid andSolid Swallows Reproduce Patients' Symptoms?Daniel Pohl, Edoardo Savarino, Patrick Janiak, Michael Fried, Radu Tutuian
Background: Esophageal motility abnormalities are often reported in patients with dysphagiaundergoing esophageal manometry. Explaining patients symptoms based on esophagealmanometry findings is challenging. Correlations between esophageal symptoms and mano-metry findings are underreported. Aim: To evaluate correlation between esophageal symp-toms and high resolution manometry findings. Methods: Patients presenting for esophagealmanometry were asked to report severity and frequency of dysphagia during the last 2weeks prior to testing (dysphagia score). Esophageal high resolution manometry (HRM) wasperformed using a 32-channel water-perfused system and included 10 water (10ml each)and 10 solid (bread) swallows. During esophageal manometry patients were asked after eachswallow if they experienced dysphagia or not. Esophageal contractions were classified asnormal, ineffective or simultaneous based on previously published criteria. Per-swallowanalysis included correlation between dysphagia (yes/no) and manometric findings (normal/ineffective/simultaneous). Per patient analysis included correlation between dysphagia score,% swallows reported as perceived and % manometric normal swallows. Results: Data from81 manometries performed in 74 patients (43 F, 31 M, mean age 46.3; range 18-87 years)totalling 801 liquid and 782 solid swallows were included in the analysis. The per-swallowanalysis for liquid swallows found manometric simultaneous and ineffective contractionsmore likely to be associated with symptoms (12/49; 24.5% and 21/125; 16.8% respectively)compared to manometric normal contractions (24/627; 3.8%). Similar results were noticedduring solid swallow: symptomatic simultaneous contractions 30/136 (22.1%), ineffectivecontractions 36/208 (17.3%) and normal contractions 44/438 (10%). The per-patient analysisfound significant (p<0.01) but moderate-poor correlations between dysphagia score and %swallows perceived during testing (r=0.399 liquid and r=0.409 solid swallows), betweendysphagia score and % manometric normal contractions during liquid swallows (r=-0.357).Correlation between %swallows perceived during testing and % manometric normal swallowswas significant (p<0.01) but poor (liquid swallows r=-0.368, solid swallows -0.268). Conclu-sion: While manometric characteristics of esophageal contractions play a role in the percep-tion of individual swallows, the proportion of manometric abnormal contractions is notsolely responsible for the intensity of dysphagic symptoms.
911
In Vivo and In Vitro Characterization of Azd9343, a Novel GABAB ReceptorAgonist and Reflux InhibitorAnders Lehmann, Thomas Elebring, Jörgen Jensen, Jan P. Mattsson, Karolina A. Nilsson,Pirjo Saransaari, Sverker von Unge
Transient lower esophageal sphincter relaxation (TLESR) is the predominant cause of gastroe-sophageal reflux and hence a target mechanism in the quest for new treatments for gastroeso-phageal reflux disease (GERD). Baclofen, a centrally acting GABAB receptor agonist, reducesTLESRs and inhibits reflux and GERD symptoms but is burdened by its CNS side-effectprofile. This study describes the pharmacological profile of AZD9343, a novel GABAB receptoragonist. Methods: Potency and intrinsic activity were established in cells expressing humanrecombinant GABAB receptors, and competition with GABA in binding to native GABAB
receptors was evaluated using rat brain membranes. Uptake of AZD9343 was measured inrat brain slices, and binding to the GABA transporter was studied in rat brain membranes.
AG
AA
bst
ract
s