59 - Roche4cf03e98-fb44-4f1f... · •Primary endpoint CR by PET-CT by IRC after primary assessment...
42
Transcript of 59 - Roche4cf03e98-fb44-4f1f... · •Primary endpoint CR by PET-CT by IRC after primary assessment...


59th ASH Annual Meeting, Atlanta
Roche Conference Call Wednesday, 13 December 2017
3
This presentation contains certain forward-looking statements. These forward-looking
statements may be identified by words such as ‘believes’, ‘expects’, ‘anticipates’, ‘projects’,
‘intends’, ‘should’, ‘seeks’, ‘estimates’, ‘future’ or similar expressions or by discussion of, among
other things, strategy, goals, plans or intentions. Various factors may cause actual results to
differ materially in the future from those reflected in forward-looking statements contained in
this presentation, among others:
1 pricing and product initiatives of competitors;
2 legislative and regulatory developments and economic conditions;
3 delay or inability in obtaining regulatory approvals or bringing products to market;
4 fluctuations in currency exchange rates and general financial market conditions;
5 uncertainties in the discovery, development or marketing of new products or new uses of existing products, including without limitation negative results of clinical trials or research projects, unexpected side-effects of pipeline or marketed products;
6 increased government pricing pressures;
7 interruptions in production;
8 loss of or inability to obtain adequate protection for intellectual property rights;
9 litigation;
10 loss of key executives or other employees; and
11 adverse publicity and news coverage.
Any statements regarding earnings per share growth is not a profit forecast and should not be interpreted to
mean that Roche’s earnings or earnings per share for this year or any subsequent period will necessarily
match or exceed the historical published earnings or earnings per share of Roche.
For marketed products discussed in this presentation, please see full prescribing information on our website
www.roche.com
All mentioned trademarks are legally protected.

Introduction
Karl Mahler Head of Investor Relations

Agenda
Welcome
Karl Mahler, Head of Investor Relations
Roche hematology portfolio: ASH update
Sandra Horning, M.D., Chief Medical Officer and Head Global Product Development
Hemlibra: Changing the standard of care in hemophilia A
Gallia Levy, M.D., Ph.D., Global Development Team Leader, Hemlibra
Q&A
Karl Mahler, Head of Investor Relations
5

Highlights from ASH
6
Venclexta
Polatuzumab vedotin
Emicizumab
Ph 3 MURANO sets a new
standard of care in R/R CLL
Ph 3 trials ongoing in 1L
CLL, AML, and MM: novel
combinations (idasanutlin)
Ph 2 results in R/R DLBCL show
strong benefit over Rituxan + benda
Moving into 1L DLBCL with
Ph 3 POLARIX trial
Updated data in Hemophilia A
patients with inhibitors shows bleed
rates continue to improve, q4w data
Positive results in patients
without inhibitors and for
monthly dosing
Data presented at ASH Future program developments
DLBCL=diffuse large B cell lymphoma; AML=acute myeloid leukemia; CLL=chronic lymphocytic leukemia, R/R = relapsed/refractory

Recognition for innovation 2013-present
7 Breakthrough designations for 4 NMEs in hematology
7
Rank Company #
1 Roche 18
2 Novartis 15
3 BMS 10
4 Merck 9
4 Pfizer 9
18 Breakthrough Therapy Designations
Source: http://www.focr.org/breakthrough-therapies as of October 2017; NME=new molecular entity; BR=bendamustin+Rituxan; DLBCL=diffuse large B cell lymphoma;
LDAC=low dose cytarabine; AML=acute myeloid leukemia; ECD=Erdheim-Chester disease; NSCLC=non-small cell lung cancer; PPMS=primary progressive multiple
sclerosis; HMA=hypomethylating agent; CLL=chronic lymphocytic leukemia; IPF=idiopathic pulmonary fibrosis
= BTDs in hematology

Roche hematology portfolio: ASH update
Sandra Horning, M.D. Executive VP Chief Medical Officer and Head Global Product Development

Late-stage portfolio: Improving the standard of
care and new indications in malignant hematology
9
¹Datamonitor; incidence rates includes the 7 major markets (US, Japan, France, Germany, Italy, Spain, UK); CLL=chronic lymphoid leukemia; DLBCL (aNHL)=diffuse
large B-cell lymphoma; iNHL=indolent non-hodgkin`s lymphoma; AML=acute myeloid leukemia; MM=multiple myeloma; MDS=myelodysplastic syndrome; ALL=acute
lymphoblastic leukemia; Venclexta in collaboration with AbbVie; Gazyva in collaboration with Biogen; Polatuzumab vedotin in collaboration with Seattle Genetics; Rituxan
HYCELA (Rituxan SC) partnered with Halozyme, BTD for R/R CLL and R/R DLBCL
Incidence rates (330,000 pts1)
Ph III 1L (CLL14)
Ph III R/R (MURANO)
Ph III
Ph III
Polatuzumab
vedotin
+
Ph II R/R (GO29365)
Ph III 1L (POLARIX) +
Ph III Idasanutlin

Late-stage portfolio:
Polatuzumab vedotin in DLBCL
10 ¹Datamonitor; incidence rates includes the 7 major markets (US, Japan, France, Germany, Italy, Spain, UK); CLL=chronic lymphoid leukemia; DLBCL (aNHL)=diffuse
large B-cell lymphoma; iNHL=indolent non-hodgkin`s lymphoma; AML=acute myeloid leukemia; MM=multiple myeloma; MDS=myelodysplastic syndrome; ALL=acute
lymphoblastic leukemia; Gazyva in collaboration with Biogen; Polatuzumab vedotin in collaboration with Seattle Genetics
Incidence rates (330,000 pts1)
Polatuzumab
vedotin
Ph II R/R (GO29365)
Ph III 1L (POLARIX) +
11
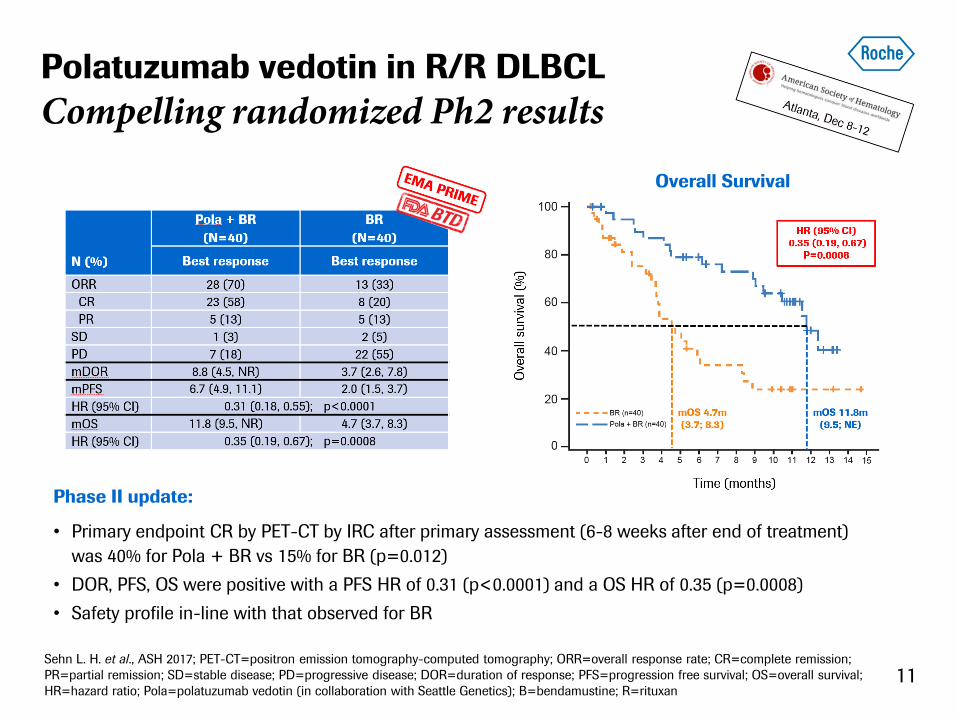
Polatuzumab vedotin in R/R DLBCL
Compelling randomized Ph2 results
Overall Survival
Phase II update:
• Primary endpoint CR by PET-CT by IRC after primary assessment (6-8 weeks after end of treatment)
was 40% for Pola + BR vs 15% for BR (p=0.012)
• DOR, PFS, OS were positive with a PFS HR of 0.31 (p<0.0001) and a OS HR of 0.35 (p=0.0008)
• Safety profile in-line with that observed for BR
Sehn L. H. et al., ASH 2017; PET-CT=positron emission tomography-computed tomography; ORR=overall response rate; CR=complete remission;
PR=partial remission; SD=stable disease; PD=progressive disease; DOR=duration of response; PFS=progression free survival; OS=overall survival;
HR=hazard ratio; Pola=polatuzumab vedotin (in collaboration with Seattle Genetics); B=bendamustine; R=rituxan

12
Polatuzumab vedotin in R/R DLBCL
Ph3 study of polatuzumab + R-CHP started
Phase II update:
• PET-CT data show that Pola+BR improved responses in both ABC and GCB
• Based on these results BTD and PRIME status awarded by FDA and EMA
• Ph3 study (POLARIX) of Pola+R-CHP vs R-CHP in 1L DLBCL initiated (First-patient-in Nov 17)
OR and CR by PET-CT*
Sehn L. H. et al., ASH 2017; PET-CT=positron emission tomography-computed tomography; OR= overall response; CR=complete remission; INV=investigator;
IRC=independent review committee; Pola=polatuzumab vedotin (in collaboration with Seattle Genetics); B=bendamustin; R=rituxan
* at primary response assessment (6–8 weeks after Cycle 6 Day 1 or last dose of therapy); + conducted in subset with available data
Armitage J., Blood 2011;118:2-3
PET-CT as endpoint
Pretreatment Posttretreatment

Late-stage portfolio:
Venclexta in CLL
13 ¹ Datamonitor; incidence rates includes the 7 major markets (US, Japan, France, Germany, Italy, Spain, UK); CLL=chronic lymphoid leukemia; DLBCL (aNHL)=diffuse
large B-cell lymphoma; iNHL=indolent non-hodgkin`s lymphoma; AML=acute myeloid leukemia; MM=multiple myeloma; MDS=myelodysplastic syndrome; ALL=acute
lymphoblastic leukemia; Venclexta in collaboration with AbbVie; Gazyva in collaboration with Biogen
Incidence rates (330,000 pts1)
Ph III 1L (CLL14)
Ph III R/R (MURANO) +

14
Venclexta in R/R CLL
MURANO supports new standard therapeutic option
Seymour J. et al., ASH 2017; INV=investigator; PFS=progression free survival; HR=hazard ratio; V=Venclexta in collaboration with
AbbVie
Trial design
Phase III interim results (MURANO):
• Primary PFS endpoint met (HR of 0.17) with benefit across all sub-groups, including high-risk patients
• Safety consistent with known safety profile of R/R CLL patients
INV assessed PFS
HR (95% CI)
0.17 (0.11-0.25)
P<0.0001

15 Seymour J. et al., ASH 2017; * descriptive P value; INV=investigator; IRC=independent review committee; ORR=overall response rate;
CR=complete remission; CRi=complete remission with incomplete marrow recovery; PR=partial remission; nPR=nodular partial remission;
SD=stable disease; PD=progressive disease; HR=hazard ratio; V=venclexta (in collaboration with AbbVie); R=rituxan; B=bendamustine
Venclexta in R/R CLL Strong response rates, encouraging OS
Response rates
Phase III interim results (MURANO):
• Investigator assessed ORR of 93.3% with 26.8% of patients showing a CR or CRi
• OS HR of 0.48 with a descriptive p-value of 0.0186
• Landmark 2Y OS at 91.9% for V+R vs 86.6% for B+R
Overall Survival (OS)
HR (95% CI)
0.48 (0.25-0.90)
P=0.0186*
16 16
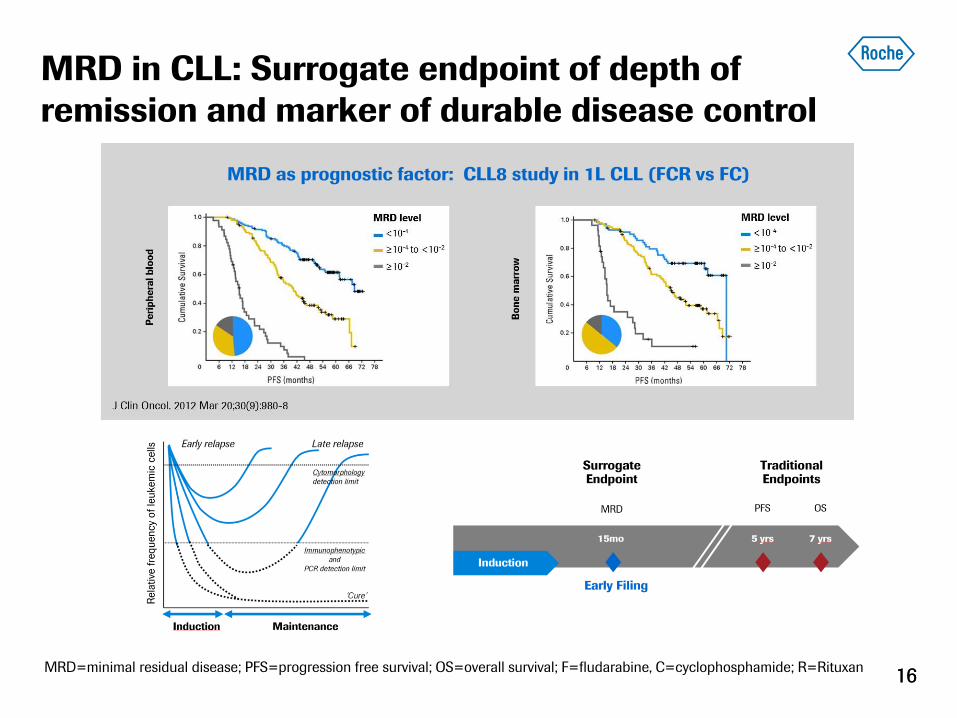
MRD in CLL: Surrogate endpoint of depth of
remission and marker of durable disease control
MRD=minimal residual disease; PFS=progression free survival; OS=overall survival; F=fludarabine, C=cyclophosphamide; R=Rituxan
MRD as prognostic factor: CLL8 study in 1L CLL (FCR vs FC)
Venclexta in R/R CLL
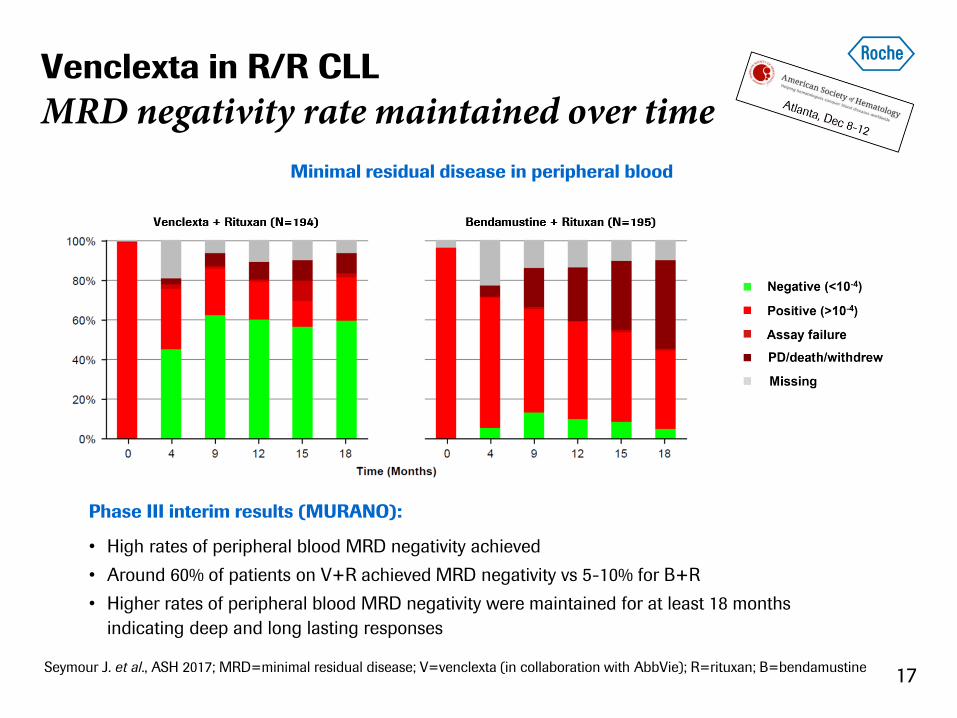
MRD negativity rate maintained over time
17 Seymour J. et al., ASH 2017; MRD=minimal residual disease; V=venclexta (in collaboration with AbbVie); R=rituxan; B=bendamustine
Phase III interim results (MURANO):
• High rates of peripheral blood MRD negativity achieved
• Around 60% of patients on V+R achieved MRD negativity vs 5-10% for B+R
• Higher rates of peripheral blood MRD negativity were maintained for at least 18 months
indicating deep and long lasting responses
Minimal residual disease in peripheral blood

18 18
R/R CLL: Cross trial comparison
Venclexta to induce deep responses
1.Stilgenbauer S, et al. ASH 2015 LBA-6; 2. Seymour JF, et al. ASCO 2014 Abs 7015; 3.Roberts NEJM 2016; 4. Byrd ASCO 2017 P7510; 5.Brown, JCO 2013;
6.Seymour ASH 2017 LBA2; 7.Chanan-Khan Lancet Oncol. 2016; 8.Burger Lancet 2014; 9. Jain CCR 2017; 10. Furman NEJM 2014; 11. Robak, JCO 2010;
Cross-trial comparisons have inherent limitations. Therefore, any such comparison should be taken with its limitations in consideration. Different
trials can potentially include different patient populations and may have different methodologies for data collection/data analysis.
ORR=overall response rate; CR=complete remission; MRD=minimal residual disease; mPFS=medium progression free survival; mOS=medium overall
survival; HR=hazard ratio; VEN=Venclexta (in collaboration with AbbVie); Ibr=ibrutinib; Idela=idelalisib; B=bendamustine; R=rituxan; IRC=independent
review committee; PB=peripheral blood; NR=not reached; est=estimated from graph

Venclexta + Gazyva in 1L CLL
Ph1 study design
19 Flinn I. W. et al., ASH 2017; Gazyva dosing schedule: C1D1=Cycle 1 day 1; VEN=venclexta (in collaboration with AbbVie);
G=Gazyva (in collaboration with Biogen)
Phase I update (GP28331/NCT01685892):
• 6 cycles of VEN+G combination therapy followed by 6 months of VEN monotherapy
• 1 cycle of G completed prior to VEN ramp up phase; 6 patients were started on a different schedule
• Ph3 study (CLL14) ongoing; First-patient-in in Nov 2016
Study design

Venclexta + Gazyva in 1L CLL
Strong response rates and lasting MRD negativity
20 Flinn I. W. et al., ASH 2017; MRD=minimal residual disease; VEN=venclexta (in collaboration with AbbVie); G=Gazyva (in collaboration with Biogen);
ORR=overall response rates; CR=complete remission; CRi=complete remission with incomplete marrow recovery; PR=partial remission
MRD negativity in peripheral blood
Phase I interim results (GP28331/NCT01685892):
• 32 patients with 100% ORR (72% CR/CRi and 28% PR), including high-risk patients
• Highly durable MRD negativity rates
• Favorable benefit/risk profile in previously untreated CLL
Response rates

Late-stage portfolio:
Venclexta in AML
21 ¹ Datamonitor; incidence rates includes the 7 major markets (US, Japan, France, Germany, Italy, Spain, UK); CLL=chronic lymphoid leukemia; DLBCL (aNHL)=diffuse
large B-cell lymphoma; iNHL=indolent non-hodgkin`s lymphoma; AML=acute myeloid leukemia; MM=multiple myeloma; MDS=myelodysplastic syndrome; ALL=acute
lymphoblastic leukemia; Venclexta in collaboration with AbbVie; Gazyva in collaboration with Biogen
Incidence rates (330,000 pts1)
Ph III

Venclexta + AZA/DEC in 1L elderly AML
Encouraging response rates and mOS
22
Phase Ib update (NCT02203773):
• ORR of 65%, compares favorably to historic results
• mOS of 17.5 months obtained for the 800mg VEN dose; not reached for the 400mg VEN dose
• 400mg VEN combination dose established due to best benefit-risk profile
• Ph3 study (NCT02993523) of VEN+AZA in 1L AML on-going (First-patient-in in Q1 17)
DiNardo C. D. et al., ASH 2017; AZA=azacitidine; DEC=decitabine; ORR=overall response rate; CR=complete remission; CRi=complete
remission with incomplete marrow recovery; DOR=duration of response; NR=not reached; VEN=Venclexta (in collaboration with AbbVie)
Overall Survival (OS)

23
20 Years of improving the standard of care
ADCC=antibody-dependent cellular cytotoxicity; ADCP=antibody-dependent cellular phagocytosis
Hemlibra: Changing the standard of care in
hemophilia A
Gallia Levy, M.D., Ph.D. Global Development Team Leader, Hemlibra

Hemlibra now approved in hemophilia A with
factor VIII inhibitors
Approved in US, updated data presented at ASH, data
currently under review by EMA (accelerated assessment)
Trial met primary endpoint and key secondary endpoints
HAVEN 1 Adult/adolescent inhibitor, QW dosing
Positive interim results
• Label contains no limitations
on age
• First treatment in hemophilia
to compare to prophylaxis
• Statistically significant
quality-of-life improvement
included in label.1
• Boxed warning and dosing
guidance important for
patient safety
FDA approval November 2017
3 months prior to PDUFA date
1 Physical Health Score of the Hemophilia-specific Quality of Life Score ,
HAVEN 2 Pediatric inhibitor, QW dosing
HAVEN 3 Non-inhibitor, QW/Q2W dosing
HAVEN 4 Inhibitor/Non-inhibitor Q4W dosing
✔
✔
Approved in US, updated data presented at ASH, data
currently under review by EMA (accelerated assessment)
25

15.7
1.8 0
2
4
6
8
10
12
14
16
18
Prior BPA
prophylaxis
Emicizumab
prophylaxis
Annualliz
ed b
leedin
g r
ate
1
88% reduction P<0.0001
HAVEN 1: Bleed rates have continued to
improve over time
Prophylactic
BPA’s
Prior
prophylactic
BPA
Emicizumab
NIS Haven1, Arm C
Treated bleeds with emicizumab prophylaxis
vs. prior BPA prophylaxis
HAVEN 1 intra-individual comparison
Mancuso M.E. et al., ASH 2017; ABR=Annualized bleeding rate; BPA=Bypassing agent; NIS=Non-interventional study, IQR = interquartile range 1Negative binomial model 2 Primary analysis data cutoff: Oct 25, 2016; Updated analysis data cutoff: Sep 8, 2017
Interval (weeks)
1-24 25-48 49-72
Mean ABR (95% CI)
Median ABR (IQR)
0 0 0 0.5
Calc
ula
ted A
BR
for
24 w
k inte
rval
HAVEN 1 emicizumab bleed rates over time
Treated bleeds with emicizumab prophylaxis over 24 wk intervals
1-24 25-48 49-72
Interval (weeks)
Proportion of patients with zero bleeds over 24 wk intervals Patients
with z
ero
ble
eds
for
24-w
eek inte
rval (%
)
88%
26
Nearly 10 months additional follow-up2

HAVEN 2: Ph3 update in pediatric patients with
inhibitors
Young G. et al., ASH 2017; ABR = Annualized Bleeding Rate, BPA = Bypassing agent, QOL= Quality of Life, IQR = interquartile range, 1Interim analysis data
cutoff: Oct 28, 2016; Updated analysis data cutoff: May 8, 2017, *Aged <12 years, † Primary efficacy results (ABR analysis) based only on patients aged < 12 yrs
on study for ≥12 wks, ‡ Negative binomial regression model
• 54/57 (94.7%) of children with zero treated bleeds on emicizumab prophylaxis
• Quality of life improvement seen in pediatric patients on emicizumab prophylaxis
• No thromboembolic or thrombotic microangiopathy events reported
40 additional patients and ~6m of additional follow-up confirm earlier analysis1
27

HAVEN 2: Ph3 update in pediatric patients with
inhibitors in intra-patient analysis
Young G. et al., ASH 2017; ABR = Annualized Bleeding Rate, BPA = Bypassing agent, QOL= Quality of Life, Interim analysis data cutoff: Oct 28, 2016; Updated
analysis data cutoff: May 8, 2017,
HAVEN 2 intra-individual comparison emicizumab prophylaxis vs prior BPA treatment
31.8
12.4
2.5
18.0
0
24.4
14.3
34.2 31.8
9.3
17.9
11.5 11.0
1.4 1.3 0 0 0 0 0 0 0 0 0 0 0 0
10
20
30
40
1 2 3 4 5 6 7 8 9 10 11 12 13
Patient
Calc
ula
ted
AB
R
(tre
ate
d b
leed
s)
Emicizumab Prophylaxis Prior BPA, episodic Prior BPA prophylaxis
99% reduction in treated bleeds vs. prior BPA treatment in intra-patient analysis
28
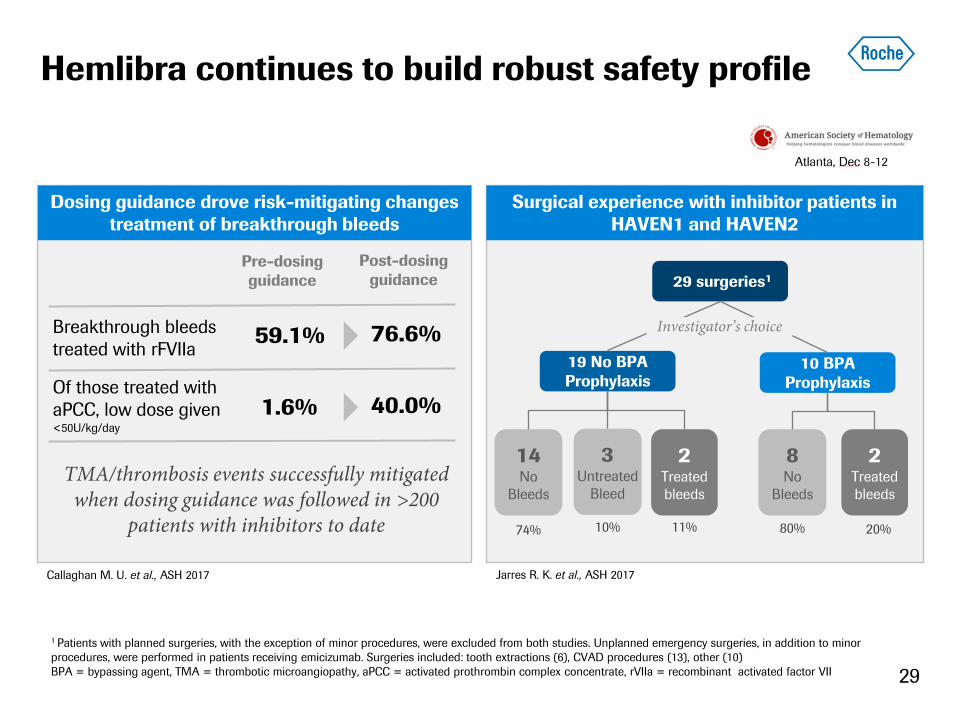
Hemlibra continues to build robust safety profile
29 surgeries1
1 Patients with planned surgeries, with the exception of minor procedures, were excluded from both studies. Unplanned emergency surgeries, in addition to minor
procedures, were performed in patients receiving emicizumab. Surgeries included: tooth extractions (6), CVAD procedures (13), other (10)
BPA = bypassing agent, TMA = thrombotic microangiopathy, aPCC = activated prothrombin complex concentrate, rVIIa = recombinant activated factor VII
19 No BPA
Prophylaxis
10 BPA
Prophylaxis
Surgical experience with inhibitor patients in
HAVEN1 and HAVEN2
3 Untreated
Bleed
2 Treated
bleeds
14 No
Bleeds
2 Treated
bleeds
8 No
Bleeds
Dosing guidance drove risk-mitigating changes
treatment of breakthrough bleeds
Investigator’s choice
74% 10% 11% 80% 20%
Pre-dosing
guidance
Post-dosing
guidance
59.1% 76.6% Breakthrough bleeds
treated with rFVIIa
Of those treated with
aPCC, low dose given <50U/kg/day
1.6% 40.0%
TMA/thrombosis events successfully mitigated when dosing guidance was followed in >200
patients with inhibitors to date
Callaghan M. U. et al., ASH 2017 Jarres R. K. et al., ASH 2017
29

HAVEN 3: Positive trial in non-inhibitor patients
• Met primary endpoint: reduction in treated bleeds vs. no prophylaxis (Arm A vs. C)
• Q2W dosing achieved: secondary endpoint met (Arm B vs. C)
• Intra-Patient Comparison: emicizumab prophylaxis superior to FVIII prophylaxis (Arm D)
• No new safety signals observed: no TMA or thrombotic events occurred in this study.
• Plan to submit for filing: data to be presented at an upcoming medical congress.
FVIII = factor VIII, TMA = thrombotic micro angiopathy
ARM A: Emicizumab 1.5mg/kg/wk maintenance
Screening Severe Hemophilia A
Pre-study episodic FVIII
Pre-study FVIII prophylaxis
R 2:2:1
ARM B: Emicizumab 3.0mg/kg/2wks maintenance
ARM C: No prophylaxis
ARM D: Emicizumab 1.5mg/kg/wk maintenance
24 w
eek p
rim
ary
eff
icacy
analy
sis
Em
iciz
um
ab
continuation
n=34
n=34
n=17
n=40-60 Intra-patient comparison
HAVEN3 Study Design: Adult and adolescent non-inhibitor patients
✔
✔
✔
30

Clinical data from weekly and monthly dosing
consistent with PK modeling
31
weekly
dosing
Modeled ABR
q2w
dosing
q4w
dosing
HAVEN 1/2/3 Data consistent with
PK modeling
HAVEN 3
Data consistent with
PK modeling
HAVEN 4 Preliminary data
consistent with PK
modeling
PK Modeling (plasma conc.)
✔
✔
Clin. Pharmacokinetics 2017 Dec 06, Selected phase III dosing regimens: repeated subcutaneous loading dose of 3 mg/kg once weekly for first 4 weeks followed
by subcutaneous maintenance doses of 1.5 mg/kg once weekly (a), 3 mg/kg every 2 weeks (b), and 6 mg/kg every 4 weeks (c).

HAVEN 4: Positive interim results for q4w dosing
HAVEN 4 PK run-in data
PK run-in cohort
(n=7)
Expansion cohort
(n=41)
PK, safety Efficacy, safety, PK/PD
• Hemlibra q4w prophylaxis showed a
clinically meaningful control of bleeding
• Preliminary findings are consistent with
results from previous studies of Hemlibra
dosed once weekly or every two weeks
• Levels of Hemlibra in the blood
(pharmacokinetics) are maintained in a
clinically effective range
• HAVEN 4 fully enrolled, interim results to
be presented at an upcoming meeting
HAVEN 4 positive interim results
✔
Jiménez-Yuste V. et al., ASH 2017, Dosing regimens: repeated subcutaneous loading dose of 3 mg/kg once weekly for first 4 weeks followed by subcutaneous
maintenance doses of 6 mg/kg every 4 weeks (c).
32

33
Appendix

34
Hematology pipeline progress in 2017
13 molecules in combination testing
* Venclexta in collaboration with AbbVie; Polatuzumab vedotin in collaboration with Seattle Genetics; Cotellic in collaboration with Exelixis; ChK1i in collaboration with
Array BioPharma; NHL=non-hodgkin`s lymphoma; CLL=chronic lymphoid leukemia; MM=multiple myeloma; MDS=myelodysplastic syndrom; AML=acute myeloid
leukemia
= progress in 2017
2x
2x

Indication Relapsed or refractory
FL and DLBCL 1L DLBCL
Phase/study Phase Ib/II Phase III
POLARIX
# of patients N=224 N=875
Design
PIb: Dose escalation
PhII: Polatuzumab vedotin plus BR vs. BR
PhII expansion: Polatuzumab vedotin plus Gazyva, non-
randomized
ARM A: Polatuzumab vedotin plus R-CHP
ARM B: R-CHOP
Primary
endpoint
Safety and response by PET/CT Progression-free survival
Status
FPI Q4 2014
Recruitment completed Q3 2016
Updated data presented at ASH 2016, ICML and EHA 2017
PRIME designation (Q2 2017) and Breakthrough Therapy
Designation granted (Q3 2017) for r/r DLBCL
FPI expected Q4 2017
CT Identifier
NCT02257567 NCT03274492
35
Polatuzumab vedotin (RG7596)
ADC targeting CD79b to treat B cell malignancies
In collaboration with Seattle Genetics
ADC=antibody–drug conjugate; DLBCL=diffuse large B cell lymphoma; FL=follicular lymphoma; ASH=American Society of Hematology;
ICML=international Conference on Malignant Lymphoma; EHA=European Hematology Association; BR=bendamustine and Rituxan; R-CHP=Rituxan,
cyclophosphamide, hydroxydoxorubicin, prednisone; R-CHOP=Rituxan, cyclophosphamide, doxorubicin, vincristine, and prednisone

Venclexta (venetoclax, RG7601, ABT-199)
Novel small molecule Bcl-2 selective inhibitor – CLL
36 Joint project with AbbVie, in collaboration with The Walter and Eliza Hall Institute
CLL=chronic lymphocytic leukemia
Indication Untreated CLL patients with
coexisting medical conditions Relapsed or refractory CLL
Relapsed or refractory CLL
with 17p deletion
Phase/study Phase III
CLL14
Phase III
MURANO Phase II
# of patients N=432 N=391 N=100
Design
ARM A: Venclexta plus Gazyva
ARM B: Chlorambucil plus Gazyva
ARM A: Venclexta plus Rituxan
ARM B: Rituxan plus bendamustine
Single-agent Venclexta
Primary
endpoint
Progression-free survival Progression-free survival Safety and maximum tolerated dose
(MTD)
Status
FPI Q4 2014
Recruitment completed Q3 2016
Recruitment completed Q3 2015
Study met primary endpoint at interim
analysis
Breakthrough designation granted by FDA
Q2 2015, priority review granted, US
approval Q2 2016
Approved in EU Q4 2016
CT Identifier NCT02242942 NCT02005471 NCT01889186
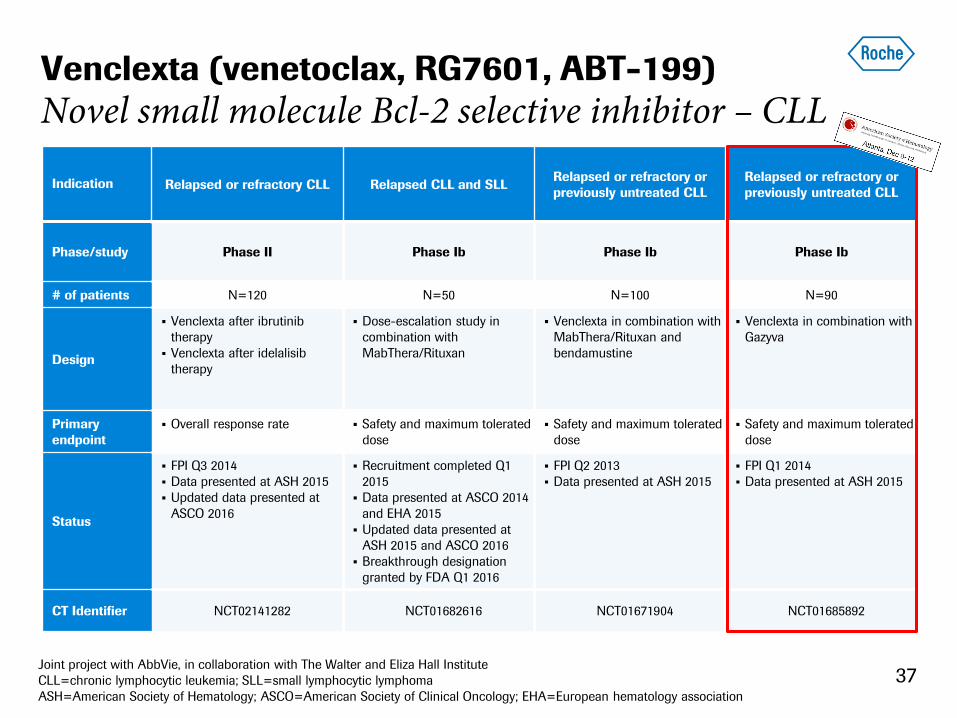
37 Joint project with AbbVie, in collaboration with The Walter and Eliza Hall Institute
CLL=chronic lymphocytic leukemia; SLL=small lymphocytic lymphoma
ASH=American Society of Hematology; ASCO=American Society of Clinical Oncology; EHA=European hematology association
Venclexta (venetoclax, RG7601, ABT-199)
Novel small molecule Bcl-2 selective inhibitor – CLL
Indication Relapsed or refractory CLL Relapsed CLL and SLL Relapsed or refractory or
previously untreated CLL
Relapsed or refractory or
previously untreated CLL
Phase/study Phase II Phase Ib Phase Ib Phase Ib
# of patients N=120 N=50 N=100 N=90
Design
Venclexta after ibrutinib
therapy
Venclexta after idelalisib
therapy
Dose-escalation study in
combination with
MabThera/Rituxan
Venclexta in combination with
MabThera/Rituxan and
bendamustine
Venclexta in combination with
Gazyva
Primary
endpoint
Overall response rate Safety and maximum tolerated
dose
Safety and maximum tolerated
dose
Safety and maximum tolerated
dose
Status
FPI Q3 2014
Data presented at ASH 2015
Updated data presented at
ASCO 2016
Recruitment completed Q1
2015
Data presented at ASCO 2014
and EHA 2015
Updated data presented at
ASH 2015 and ASCO 2016
Breakthrough designation
granted by FDA Q1 2016
FPI Q2 2013
Data presented at ASH 2015
FPI Q1 2014
Data presented at ASH 2015
CT Identifier NCT02141282 NCT01682616 NCT01671904 NCT01685892

Indication Treatment-naïve AML not eligible for standard induction therapy
Phase/study Phase Ib Phase I/II Phase III
# of patients N=160 N=65 N=400
Design
Venclexta (dose escalation) plus
decitabine
Venclexta (dose escalation) plus
azacitidine
Venclexta (dose escalation) plus
decitabine plus posaconazole
Venclexta (dose escalation) plus low-dose
cytarabine
• ARM A: Venclexta plus azacitidine
• ARM B: Azacitidine
Primary
endpoint
Safety Safety, PK, PD and efficacy Percentage of participants with CR,
Overall survival
Status
FPI Q4 2014
Data presented at ASH 2015
Breakthrough designation granted by FDA
Q1 2016
Updated data presented at ASCO 2016
FPI Q1 2015
Initial data presented at ASCO 2016
Updated data presented at ASH 2016
FPI Q1 2017
CT Identifier NCT02203773 NCT02287233 NCT02993523
38 Joint project with AbbVie, in collaboration with The Walter and Eliza Hall Institute
AML=acute myelogenous leukemia; ASH=American Society of Hematology; ASCO=American Society of Clinical Oncology
Venclexta (venetoclax, RG7601, ABT-199)
Novel small molecule Bcl-2 selective inhibitor – AML

Indication Relapsed or refractory multiple myeloma
Phase/study Phase III
BELLINI Phase I Phase I
# of patients N=240 N=66 N=84
Design
ARM A: Venclexta plus bortezomib plus
dexamethasone
ARM B: Placebo plus bortezomib plus
dexamethasone
Patients receiving bortezomib and
dexamethasone as standard therapy:
Dose escalation cohort: Venclexta plus
bortezomib plus dexamethasone
Safety expansion cohort: Venclexta
plus bortezomib plus dexamethasone
Dose escalation cohort:
Venclexta dose escalation
Safety expansion cohort:
Venclexta expansion
Combination:
Venclexta plus dexamethasone
Primary
endpoint
Progression-free survival Safety and maximum tolerated dose Safety and maximum tolerated dose
Status
FPI Q3 2016 FPI Q4 2012
Data presented at ASCO 2015
Updated data presented at ASCO 2016
and ASH 2016
FPI Q4 2012
Data presented at ASCO 2015
Updated data presented at ASCO 2016
and ASH 2016
CT Identifier NCT02755597 NCT01794507 NCT01794520
39 Joint project with AbbVie, in collaboration with The Walter and Eliza Hall Institute
MM=multiple myleloma; ASCO=American Society of Clinical Oncology; ASH=American Society of Hematology
Venclexta (venetoclax, RG7601, ABT-199)
Novel small molecule Bcl-2 selective inhibitor – MM

Oncology development programs
Small molecules
40
Molecule Idasanutlin
(MDM2 antagonist, RG7388)
Indication Relapsed/refractory AML
MIRROS
Refractory AML
not eligible for cytotoxic therapy
Phase/study Phase III Phase I
# of patients N=440 N=140
Design
ARM A: Idasanutlin plus cytarabine
ARM B: Placebo plus cytarabine
Phase I (dose escalation)
ARM A: Cotellic1 plus Venclexta2
ARM B: Idasanutlin plus Venclexta2
Phase II (expansion)
ARM A: Cotellic1 plus Venclexta2
ARM B: Idasanutlin plus Venclexta2
Primary
endpoint
Overall survival Safety and efficacy
Status FPI Q4 2015 FPI Q1 2016
CT Identifier NCT02545283 NCT02670044
1 Cotellic in collaboration with Exelixis; 2 Joint project with AbbVie, in collaboration with The Walter and Eliza Hall Institute
AML=acute myeloid leukemia; ASCO=American Society of Clinical Oncology; ECC=European Cancer Congress; ESMO=European Society for Medical Oncology

41 41
Un-classified ABC GCB
~15% ~55% ~30%
Lenalidomide (RELEVANCE)
Ibrutinib (PHOENIX)
Polatuzumab vedotin backbone
* 46% of ABC patients are double positive (Hu S et l. Blood, 2013); Source: Roche internal data presented during REFORCE F2F Feb-2015; Johnson N et al, JCO 2012;
Hu S et al, Blood 2013; Iqbal J et al. Clin Can Res 2011; Iqbal J et al. JCO, 2006; Davis et al. Nature 2010; Haberman T et al, JCO 2006; Thieblemont C et al. JCO 2011
~50%
~50%
Elevated BCL-2
Double Positive
BCL-2 and myc* Double Hit
BCL-2
and myc
Increasing Segmentation in 1L DLBCL
Rituxan backbone

Doing now what patients need next