1941-3084 · Luminal Esophageal Temperature Monitoring With a Deflectable Esophageal Temperature...
10
1941-3084 American Heart Association. All rights reserved. Print ISSN: 1941-3149. Online ISSN: 2011 Copyright © Greenville Avenue, Dallas, TX 72514 Circulation: Arrhythmia and Electrophysiology is published by the American Heart Association. 7272 DOI: 10.1161/CIRCEP.110.960328 2011; 2011;4;149-156; originally published online February 15, Circ Arrhythm Electrophysiol Barreto, Fabrício Vassalo, Andre d'Avila and Sheldon M. Singh Anderson Oliverira, André R. Zanatta, Ayrton K. Peres, Clarissa Novakoski, Jose R. Luiz R. Leite, Simone N. Santos, Henrique Maia, Benhur D. Henz, Fábio Giuseppin, Injury During Atrial Fibrillation Ablation Procedures : Results of a Pilot Study Temperature Probe and Intracardiac Echocardiography May Reduce Esophageal Luminal Esophageal Temperature Monitoring With a Deflectable Esophageal http://circep.ahajournals.org/content/4/2/149.full on the World Wide Web at: The online version of this article, along with updated information and services, is located http://circep.ahajournals.org/content/suppl/2011/02/15/CIRCEP.110.960328.DC1.html Data Supplement (unedited) at: http://www.lww.com/reprints Reprints: Information about reprints can be found online at [email protected] 410-528-8550. E-mail: Health, 351 West Camden Street, Baltimore, MD 21201-2436. Phone: 410-528-4050. Fax: Permissions: Permissions & Rights Desk, Lippincott Williams & Wilkins, a division of Wolters Kluwer http://circep.ahajournals.org/site/subscriptions/ at Subscriptions: Information about subscribing to Circulation: Arrhythmia and Electrophysiology is online by guest on May 27, 2013 circep.ahajournals.org Downloaded from
Transcript of 1941-3084 · Luminal Esophageal Temperature Monitoring With a Deflectable Esophageal Temperature...

1941-3084American Heart Association. All rights reserved. Print ISSN: 1941-3149. Online ISSN: 2011 Copyright ©
Greenville Avenue, Dallas, TX 72514Circulation: Arrhythmia and Electrophysiology is published by the American Heart Association. 7272
DOI: 10.1161/CIRCEP.110.9603282011;
2011;4;149-156; originally published online February 15,Circ Arrhythm ElectrophysiolBarreto, Fabrício Vassalo, Andre d'Avila and Sheldon M. Singh
Anderson Oliverira, André R. Zanatta, Ayrton K. Peres, Clarissa Novakoski, Jose R. Luiz R. Leite, Simone N. Santos, Henrique Maia, Benhur D. Henz, Fábio Giuseppin,Injury During Atrial Fibrillation Ablation Procedures : Results of a Pilot Study
Temperature Probe and Intracardiac Echocardiography May Reduce Esophageal Luminal Esophageal Temperature Monitoring With a Deflectable Esophageal
http://circep.ahajournals.org/content/4/2/149.full
on the World Wide Web at: The online version of this article, along with updated information and services, is located
http://circep.ahajournals.org/content/suppl/2011/02/15/CIRCEP.110.960328.DC1.html Data Supplement (unedited) at:
http://www.lww.com/reprintsReprints: Information about reprints can be found online at
[email protected]. E-mail:Health, 351 West Camden Street, Baltimore, MD 21201-2436. Phone: 410-528-4050. Fax: Permissions: Permissions & Rights Desk, Lippincott Williams & Wilkins, a division of Wolters Kluwer
http://circep.ahajournals.org/site/subscriptions/atSubscriptions: Information about subscribing to Circulation: Arrhythmia and Electrophysiology is online
by guest on May 27, 2013circep.ahajournals.orgDownloaded from

Luminal Esophageal Temperature Monitoring With aDeflectable Esophageal Temperature Probe and Intracardiac
Echocardiography May Reduce Esophageal Injury DuringAtrial Fibrillation Ablation Procedures
Results of a Pilot Study
Luiz R. Leite, MD; Simone N. Santos, MD; Henrique Maia, MD; Benhur D. Henz, MD;Fabio Giuseppin, MD; Anderson Oliverira, MD; Andre R. Zanatta, MD; Ayrton K. Peres, MD;
Clarissa Novakoski, MD; Jose R. Barreto, MD; Fabrício Vassalo, MD;Andre d’Avila, MD, PhD; Sheldon M. Singh, MD
Background—Luminal esophageal temperature (LET) monitoring is one strategy to minimize esophageal injury duringatrial fibrillation ablation procedures. However, esophageal ulceration and fistulas have been reported despite adequateLET monitoring. The objective of this study was to assess a novel approach to LET monitoring with a deflectable LETprobe on the rate of esophageal injury in patients undergoing atrial fibrillation ablation.
Methods and Results—Forty-five consecutive patients undergoing an atrial fibrillation ablation procedure followed byesophageal endoscopy were included in this prospective observational pilot study. LET monitoring was performed with a 7Fdeflectable ablation catheter that was positioned as close as possible to the site of left atrial ablation using the deflectablecomponent of the catheter guided by visualization of its position on intracardiac echocardiography. Ablation in the posteriorleft atrial was limited to 25 W and terminated when the LET increased 2°C from baseline. Endoscopy was performed 1 to2 days after the procedure. All patients had at least 1 LET elevation �2°C necessitating cessation of ablation. Deflection ofthe LET probe was needed to accurately measure LET in 5% of patients when ablating near the left pulmonary veins, whereasdeflection of the LET probe was necessary in 88% of patients when ablating near the right pulmonary veins. The averagemaximum increase in LET was 2.5�1.5°C. No patients had esophageal thermal injury on follow-up endoscopy.
Conclusions—A strategy of optimal LET probe placement using a deflectable LET probe and intracardiac echocardiog-raphy guidance, combined with cessation of radiofrequency ablation with a 2°C rise in LET, may reduce esophagealthermal injury during left atrial ablation procedures. (Circ Arrhythm Electrophysiol. 2011;4:149-156.)
Key Words: catheter ablation � atrial fibrillation � complications � esophageal injury � temperature monitoring
Catheter ablation procedures for the treatment of atrialfibrillation (AF) may involve extensive radiofrequency
ablation of the left atrial (LA) posterior wall with the potentialrisk of collateral damage to adjacent structures including theesophagus. Although the incidence of LA-esophageal fistula inpatients undergoing AF ablation procedures has been reported tobe approximately 0.04%,1 esophageal ulceration, the purportedprecursor to LA-esophageal fistula, has been reported to occur inas many as 48% of patients.2 Thus, strategies to minimize therisk of esophageal thermal injury may reduce the likelihood ofdeveloping this rare but devastating complication. Currently, areduction in the magnitude and duration of radiofrequency
power applied in the vicinity of the esophagus is performed in anattempt to minimize esophageal injury. However, interindividualvariability in LA and esophageal wall thickness as well as thepresence and extent of intervening fibrofatty tissue3 prevents thisapproach from uniformly minimizing the risk of thermal esoph-ageal injury in all patients.
Clinical Perspective on p 156
Luminal esophageal temperature (LET) monitoring hasalso been suggested as one method of assessing the risk ofesophageal thermal injury with a strategy of cessation ofradiofrequency ablation once a prespecified LET is obtained
Received October 17, 2010; accepted February 3, 2011.From the Instituto Brasília de Arritmia (L.R.L., S.N.S., H.M., B.D.H., F.G., A.O., A.R.Z., A.K.P., C.N., J.R.B., F.V.), Brasilia, Brasil; Cardiac
Arrhythmia Service–Mount Sinai School of Medicine (A.d’A.), New York, NY; and Schulich Heart Program (S.M.S.), Division of Cardiology,Sunnybrook Health Sciences Center, Faculty of Medicine, University of Toronto, Toronto, Ontario, Canada.
The online-only Data Supplement is available at http://circep.ahajournals.org/cgi/content/full/CIRCEP.110.960328/DC1.Correspondence to Sheldon M. Singh, MD, Schulich Heart Program, Sunnybrook Health Sciences Center, 2075 Bayview Ave, Room A222, Toronto,
ON, Canada, M4N 3M5. E-mail [email protected]© 2011 American Heart Association, Inc.
Circ Arrhythm Electrophysiol is available at http://circep.ahajournals.org DOI: 10.1161/CIRCEP.110.960328
149 by guest on May 27, 2013circep.ahajournals.orgDownloaded from

possibly minimizing this risk.4 Despite the use of LETmonitoring, esophageal ulcerations have been reported tooccur in 6% to 26%2,4,5 of patients undergoing AF ablation.Additionally, and somewhat more worrisome, at least 2 casesof LA-esophageal fistula have been reported in patientsundergoing AF ablation procedures with LET monitoring.6,7
The ongoing high rate of esophageal thermal injury despiteLET monitoring probably is related to the limitations of thecurrent technique used for LET monitoring. Specifically,suboptimal orientation and positioning of the LET probe inrelationship to the site of radiofrequency application mayresult in an underestimation of the true LET at the site closestto the area of radiofrequency application. It is possible thatthis limitation may be overcome with the use of imaging toposition the LET probe in as close proximity as possible tothe location of the radiofrequency catheter during ablation,thereby improving the accuracy of the LET value obtained,and allowing one to better estimate the risk of local esopha-geal thermal injury. Thus, the aim of this pilot study was toassess the impact of LET monitoring using intracardiacechocardiography (ICE) guidance to visualize and positionthe LET probe in as close proximity to the radiofrequencyablation catheter as possible, on the prevalence of esophagealinjury in patients undergoing AF ablation procedures.
MethodsPatient PopulationForty-five consecutive patients with symptomatic drug refractory AFplanned to undergo a first-ever AF ablation procedure, were includedin this prospective observational pilot study. All patients wereidentified and all procedures performed at the Instituto Brasília deArritmia, Brasília, Brazil, between December 2008 and April 2009.All patients provided verbal and written informed consent as per thelocal institutional guidelines. The study was approved by the EthicsCommittee of the Instituto Brasília de Arritmia, Brasilia, Brasil.
Patient demographics (age, sex, and body mass index) and diseasecharacteristics (paroxysmal AF, LA volume, and left ventricularejection fraction) were obtained from all patients in this cohort.
Ablation ProcedureCoumadin therapy was discontinued 3 days before the ablationprocedure, and all patients bridged with low-molecular-weight hep-arin. Conscious sedation (n�2) or general anesthesia (n�43) wasavailable for all cases and used according to patient’s preference andphysician discretion. Internal jugular venous access was obtained inall patients and used to place a decapolar catheter within the coronarysinus. Additionally, an ICE catheter (10F, 5.5 to 10 MHz phasedarray, AcuNav Ultrasound Catheter, Biosense Webster, DiamondBar, CA) was placed in the right atrium in all patients and used toguide transseptal puncture as well as position the LET probe (seedescription below). Double transseptal punctures were performed inall patients, and a 20-mm circular mapping catheter and 3.5-mmopen irrigated tip ablation catheter (Navistar Thermocool or CelciusThermocool, Biosense Webster) were placed within the LA via eachtransseptal sheath.
Preprocedural imaging with CT or MRI was not performed in anypatient. The ablation procedure was performed with fluoroscopy, andICE guided movements of the circular mapping catheter in 25patients, whereas an electroanatomic mapping system (CARTO XPand CARTOSOUND, Biosense Webster) was used in the remainingpatients. LA geometry was created in a point-by-point fashion usingthe ablation catheter and fluoroscopic and ICE guidance when theCARTO XP (Biosense Webster) electroanatomic mapping systemwas used (n�9). LA geometry was created with the CARTOSOUND
module by tracing the LA contours obtained with ICE imaging(n�11).
Ablation was performed in the antral region of all pulmonary veins(PV) guided by the presence of PV potentials on the circularmapping catheter with the aim of achieving pulmonary vein isola-tion. Additional LA substrate modification was performed at thediscretion of the operator.
The radiofrequency generator (Stockert, Biosense Webster) wasset to deliver a maximum of 30 W and 42°C. Power was limited to25 W and radiofrequency applications approximately 30 seconds induration when ablating on the posterior wall. Further reductions inradiofrequency power were undertaken with rises in LET (seebelow). The flow rate was 17 mL/min during radiofrequencyablation. Ablation lesions were delivered by “dragging” the catheter.
LET MonitoringLET monitoring was achieved with a standard curve, 7F steerablesymmetrical bidirectional 5-mm-tip ablation catheter (EPT Blazer II,Boston Scientific, Natick, MA). The thermistor of the ablationcatheter is located at its tip. A cable adapter from the ablationcatheter was plugged directly into the electrophysiology recordingsystem (EP-Tracer, Cardiotek, Maastrich, The Netherlands), and thechanges in LET from baseline were displayed on the recordingsystem and also documented. Any rise in LET of 2°C from thebaseline LET resulted in a red flashing light to be displayed on therecording system, thereby alerting the operator to an absolute 2°Crise in LET during the current radiofrequency application. Radiofre-quency applications were discontinued when an absolute rise in LET�2°C above the baseline occurred—this value (2°C) was selectedbased on our prior experiences (selecting a rise of only 1°C resultedin frequent premature termination of radiofrequency applications),desire to account for variations in baseline LET among patients, andrecognition that an elevation in LET of �2°C would correspond toa greater rise in intramural esophageal temperature that may bedetrimental. In general a LET rise �2°C usually occurs beforeachieving an absolute LET of 39°C. Additional ablation was permit-ted at a reduced power output (15 to 20 W) once the LET hadreturned to baseline.
Use of ICE to Aid LET Probe PositioningAt the start of the ablation procedure, the deflectable ablationcatheter (ie, the LET probe) was inserted into the lumen ofesophagus in an undeflected manner (Figure 1). The ICE catheterwas placed within the right atrium (RA) and manipulated to visualizethe esophagus (Figure 1). ICE manipulation was performed by 1 of2 operators with extensive experience in cardiac ultrasound imaging.The echocardiographic relationship between the esophagus and PVswas also documented. Occasionally, when the CARTOSOUNDmodule was used, the esophagus was traced and displayed on theelectroanatomic map to illustrate its relationship to the LA.
If the esophagus was visualized with ICE at a targeted site ofablation, then the LET probe was manipulated such that it was alsovisualized on ICE at a site as close as possible to the targeted ablationsite (hereafter called the optimal site) (Figure 2 and online-onlySupplement Video 1 and Video 2). To achieve this, the LET probewas frequently advanced or retracted in a craniocaudal fashion, or,using the deflectable feature of the LET probe, deflected to the rightor the left (Figure 2), or, turned in a clockwise or counterclockwisefashion to be positioned more anterior or posterior in the esophagus(Figure 3). LET probe manipulation was performed exclusively by acirculating nurse in the electrophysiology laboratory. Any distensionin the esophagus during LET probe manipulation (Figure 4, online-only Supplement Video 1) was annotated.
Esophageal EvaluationAll patients underwent a non–symptom-driven esophageal endos-copy within 2 days of the AF ablation procedure. All procedureswere performed by a single gastroenterologist. Particular attentionwas made to visualizing the region of the midesophagus adjacent to
150 Circ Arrhythm Electrophysiol April 2011
by guest on May 27, 2013circep.ahajournals.orgDownloaded from

the pulsating heart where ablation related thermal injury would beexpected to occur.
Follow-UpAll patients were discharged after the endoscopy procedure. Atherapeutic international normalized ratio was maintained for at least4 months after the ablation procedure. Antiarrhythmic agents wereinitiated or continued at the discretion of the patient’s physician. Allpatients were prescribed the proton-pump inhibitor pantoprazole for1 week after the procedure. During the first year of follow-up, ECGswere recorded monthly, Holter monitoring performed at the 3rd, 6th,and 12th months, and exercise testing performed during the 6thmonth of follow-up. Recurrence was defined as any AF recorded byECG, Holter monitoring, or exercise testing.
Statistical AnalysisContinuous variables were reported as mean�standard deviation anddiscrete variables reported in percentages. Two-by-two contingencytables were created for discrete variables and frequencies comparedwith the �2 test. The proportion of patients in this series withesophageal ulceration was reported, and the Zar method was used to
determine the confidence interval associated with this proportion.8
Probability values (probability values) �0.05 were considered sig-nificant. All statistical analysis was performed with SPSS 15 forWindows (SPSS Inc, Chicago, IL).
ResultsPatient and Procedural CharacteristicsThe Table summarizes the patient and procedural character-istics of the study cohort. No patient had a history ofesophageal disease. All patients had an international normal-ized ratio �2.0 on the day of the procedure. Generalanesthesia was used in all but 2 patients (n�43, 96%).Orogastric or nasogastric tubes were not placed in anypatient. The average procedure time for the entire cohort was255�67 minutes.
Esophageal VisualizationThe course of the esophagus in relation to the LA wasvisualized with ICE in 98% (n�44) of patients in this cohort.The esophagus was not visualized in one patient with aseverely dilated LA (LA volume�240 mL/m2). This patientwas excluded from the current analysis.
Using ICE, the esophagus was visualized solely in prox-imity to the left PVs in 41% (n�18) of patients, solely inproximity to the right PVs in 9% (n�4) of patients, and inproximity to both the right and left veins in 50% (n�22)patients. There was no change in the esophageal locationduring the ablation procedure with either ICE or fluoroscopicvisualization.
Positioning of the LET ProbeWhen the esophagus was in contact with the left PVs (n�40),the optimal LET probe position was achieved with the LETprobe undeflected in 95% (n�38) of patients. That is, simplyadvancing or retracting the LET probe in a craniocaudalfashion guided by fluoroscopy was sufficient to position theLET probe as close as possible to the radiofrequency ablationcatheter in 95% of the patients in this cohort. In the remaining2 patients, the optimal LET probe position could not simplybe achieved with manipulating the LET probe in a craniocaudaldirection. In these 2 patients, deflection of the LET probe to theleft guided by ICE allowed it to be in a position nearest to theradiofrequency ablation catheter, which resulted in further risesin LET during radiofrequency application.
When the esophagus was in contact with the right PVs(n�26), an optimal LET probe positioning was achieved withthe LET probe undeflected in 12% (n�3) of patients. That is,simply advancing or retracting the LET probe in a craniocau-dal fashion guided by fluoroscopy alone was sufficient toposition the LET probe as close to the radiofrequencyablation catheter in only 12% of patients. Deflection of theLET probe guided by ICE was necessary to position the LETprobe as close as possible to the radiofrequency ablationcatheter in the remaining 88% of cases (Figure 2). Deflectionof the LET probe to achieve an optimal position was morenecessary when the esophagus was near the right than leftsided PVs (P�0.001).
In addition to optimizing the position of the LET probe ina lateral direction (that is, right to left), ICE aided optimiza-
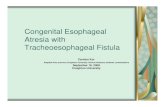
Figure 1. Visualization of the luminal esophageal temperature(LET) probe with intracardiac echocardiography (ICE). A, Crosssection of a cadaver demonstrating the relationship between theleft atrium (LA) and esophagus. On this cadaveric specimen, noLET probe is placed in the esophagus. The ICE probe is in theright atrium (RA) and indicated by the asterisk. The red triangleapproximates the field of view of the ICE probe. B, ICE imagingfrom the RA visualizing the LA and aorta. As in A, no LET probeis placed in the esophagus, hence the esophagus is visualizedwith ICE, whereas the LET probe is not visualized. C, Crosssection of a cadaver demonstrating the relationship between theLA and esophagus. On this cadaveric specimen, a LET probe(arrow) is placed in the esophagus. The ICE probe is in the RAand indicated by the asterisk. The red triangle approximates thefield of view of the ICE probe. D, ICE imaging from the RA visu-alizing the LA and aorta. As in C, a LET probe is now visualizedin the esophagus (arrow). Ao indicates aorta; Eo, esophagus.Arrow corresponds to the LET probe; asterisk corresponds tothe ICE probe.
Leite et al LET Monitoring Guided by ICE During AF Ablation 151
by guest on May 27, 2013circep.ahajournals.orgDownloaded from

tion of the LET probe position in an anteroposterior directionin 5 patients (Figure 3). For example, occasionally the LETprobe would be located adjacent to the posterior wall of theesophagus; such an orientation may result in underestimationof LET due to the inability to accurately detect anterioresophageal wall heating during posterior LA ablation. Inaddition, distension of the anterior esophageal wall into theposterior LA by the LET probe (Figure 4 and online-onlySupplement Video 1) was noted with ICE at some pointduring 27% of the procedures. In these situations, the LETprobe was repositioned as this orientation may facilitate
esophageal heating (Figure 4 and online-only SupplementVideo 2).
LET MonitoringThe average baseline LET in this cohort was 35.8�0.7°C. Allpatients had at least 1 LET elevation �2°C during radiofre-quency ablation that necessitated termination of radiofre-quency ablation (Figure 5). Radiofrequency lesions that wereterminated achieved, on average, a maximum LET rise of2.5�1.5°C from the baseline LET with the maximum LEToccurring approximately 11�8 seconds after termination of
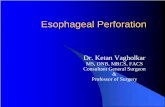
Figure 2. Deflection of the luminal esophageal temperature (LET) probe during ablation of the right pulmonary veins (PVs). A, Intracar-diac echocardiography (ICE) demonstrating the presence and location of the esophagus in relation to the left atrium (LA). The greentracing highlights the esophagus and is used to illustrate the esophagus with CARTOSOUND. B, CARTO electroanatomic map demon-strating the left atrium (LA) and the esophagus (gray structure). Of note, the esophagus in this patient is wide and borders the posterioraspect of the LA near the right and left-sided PVs. C, CARTO electroanatomic map. Esophageal temperature rises �2°C, noted by theblack points. Note elevated LET were present near both the left- and right-sided veins. LET probe deflection was required to appreciateLET rises adjacent to the right PVs. D, At baseline, the LET probe is inserted in a neutral or undeflected position. On fluoroscopy, theLET probe is distant from the ablation (ABL) catheter, which is adjacent to the right PVs. E, On fluoroscopy, the LET probe is deflectedto the right. The LET probe now appears closer to the ABL catheter with fluoroscopy. F, ICE visualization of the right PVs correspond-ing to the fluoroscopic image in D. Note the esophagus is located in this region (dashed outline); however, on fluoroscopy, the LETprobe is at the corresponding level of interest but not visualized at the location of interest (ie, near the ABL catheter) using ICE. G, ICEvisualization demonstrating the esophagus in relation to the right PVs after deflection of the LET probe shown in E. The ablation cathe-ter is noted (arrow). The newly positioned/deflected LET probe can be seen with ICE (arrow) in close proximity to the ablation catheter.It is unlikely that the esophagus was moved with deflection of the LET probe because the esophagus is noted to be in the same posi-tion now with the LET probe compared with before placement of the LET probe, which is shown in D. MAP indicates circular mappingcatheter; CS, coronary sinus catheter; Eso, esophagus; and RIPV, right inferior pulmonary vein. Single arrow indicates ablation catheterwithin the LA; double arrow, LET probe.
152 Circ Arrhythm Electrophysiol April 2011
by guest on May 27, 2013circep.ahajournals.orgDownloaded from

radiofrequency ablation. The LET returned to the baselinepreablation temperature approximately 18�9 seconds afterthe maximum LET was achieved.
During ablation of the left PVs, deflection of the LETprobe resulted in detection of at least 1 significant LET rise in2 of 40 patients. However, during ablation of the right PVs,deflection of the LET resulted in detection of at least 1significant LET rise in 23 of 26 patients. An associationbetween deflection of the LET probe and LET rises wasobserved when ablation was performed near the right com-pared with the left PVs (P�0.001).
Of note, compared with prior experiences, we did notobserve any unusual change in impedance during ablationwhen the deflectable LET probe was used with the averageimpedance during ablation being 113�10 ohms.
EndoscopyAll patients underwent esophageal endoscopy within 2 daysafter ablation procedure (68% on day 1). No esophagealmucosal abnormalities (ie, erythema or ulceration) werenoted in any patient. No evidence of trauma related to the useof the LET probe was noted. The 95% confidence interval forthe observed event proportion was 0% to 8%.
Follow-UpPatients were followed up for an average of 13�3 months.No patients had esophageal symptoms (dysphagia) or LA-esophageal fistula during the follow-up period. AF recurrencewas 25% after a single procedure during the follow-up period(14.3% for paroxysmal and 35% for nonparoxysmal AF),with 14% of patients free of AF still on an antiarrhythmicagent for the duration of the follow-up period.
DiscussionThe results of this pilot study suggest that a strategy ofoptimal LET probe placement guided by real-time esophagealimaging, combined with the cessation of radiofrequencyablation after a 2°C rise in LET, may be considered anothertool to reduce esophageal thermal injury during AF ablationprocedures.
Efficacy of Current Methods of LET MonitoringAs esophageal thermal injury may be the precursor to the rarebut devastating complication of LA-esophageal fistula, it isimperative that strategies minimizing esophageal heatingduring AF ablation be developed. LET monitoring during AFablation has been proposed as one such strategy. Singh et al4
demonstrated that LET monitoring during AF ablation pro-cedures (with cessation of radiofrequency at LET �38.5°C)was associated with an 83% relative risk reduction in esoph-ageal ulcer formation compared to performing AF ablationwithout LET monitoring. Despite this, 6% of patients in thisseries had esophageal ulceration. Di Biase et al2 reported ona series of patients undergoing AF ablation with cessation ofradiofrequency ablation with any increase in LET �39°C—esophageal ulceration was noted in 26% of patients. Rillig etal5 performed AF ablation with a remote robotic navigationsystem. Esophageal ulceration was present in 14.3% ofpatients despite termination of radiofrequency ablation withLET rises �39°C. Additionally, we are aware of at least 2cases of LA-esophageal fistula formation after AF ablationperformed with LET monitoring.6,7 Thus, current methods ofLET monitoring during AF ablation procedures may reducebut not eliminate the risk of esophageal injury.
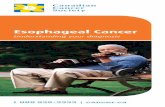
Figure 3. Repositioning the luminalesophageal temperature (LET) probe froma posterior to anterior esophageal posi-tion. A, LET probe (arrow) located awayfrom the anterior esophagus and hencefurther away from the left atrial (LA) site ofablation. B, Repositioning of the LETprobe such that it is now positioned closeto the anterior aspect of the esophagus(double arrow), closer to the LA site ofablation. Ao indicates aorta.
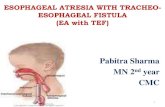
Figure 4. Indentation of the posterior leftatrium (LA) with the luminal esophagealtemperature (LET) probe. A, The LETprobe is deflected toward the anterioresophagus near the left inferior pulmonaryvein such that it indents the anterioresophageal wall into the LA (asterisk)(online-only Supplement Video 1). B, TheLET probe is repositioned not to indentthe anterior esophageal wall into the LA,thereby minimizing heat transfer to theesophagus (online-only Supplement Video2). Abl indicates ablation catheter.
Leite et al LET Monitoring Guided by ICE During AF Ablation 153
by guest on May 27, 2013circep.ahajournals.orgDownloaded from

Role of Real-Time Esophageal ImagingGiven the complex anatomy and dynamic nature of theesophagus, it is no surprise that current methods of LETmonitoring with LET probe placement guided solely byfluoroscopy are unable to eliminate esophageal injury. Theability to visualize the location of the LET probe with ICEand subsequently deflect the probe to optimize its placementprobably improves the accuracy of local LET measurements.In our series of patients, adjusting the LET probe in acraniocaudal manner, similar to what is currently performedwith fluoroscopy, resulted in optimal LET probe positioningin less than half of all patients, with this approach beingparticularly suboptimal for patients with an esophagus adja-cent to the right PVs. One may speculate that should optimalLET probe positioning not be achieved then a falsely lowLET or slow rise in LET may occur during radiofrequencyablation placing the patient at risk for esophageal injury. Theapproach we describe stresses the importance of adequateLET probe placement. The ability to visualize the entireextent of the esophageal-posterior LA wall relationship andboth visualize and manipulate the LET probe in real-time in3 dimensions is a significant improvement compared tocurrent methods of simply advancing and retracting the LETprobe with the aid of fluoroscopy. These improvements willallow for more accurate LET measurements to be obtained.Additionally, the use of ICE allowed for visualization ofanterior displacement of the esophagus into the posterior wallof the LA with the LET probe—a situation that may increasethermal conduction to the esophagus and esophageal injury.
It is important to recognize that simply visualizing theesophagus alone is necessary but unlikely sufficient to avoidesophageal thermal injury deflection of the LET probe to
optimize its position also necessary. This latter point is bestillustrated in the report by Vijayraman,7 where LA-esophageal fistula occurred despite appropriate LET monitor-ing with a nondeflectable LET probe as well as the use of ICEand barium to visualize the esophagus. Thus, a combinationof visualization of the esophagus and deflection of the LETprobe to optimize its position is vital.
Choice of LET GuidingRadiofrequency TerminationRather than terminate radiofrequency applications after anabsolute LET was achieved as described in previous stud-ies.2,4,5 Radiofrequency applications were terminated after anincrease in LET of 2°C, based on our prior experiences,desire to account for variations in baseline LET amongpatients, and recognition than a rise in LET �2°C would beassociated with a greater rise in intramural esophageal tem-perature that may be detrimental. Because the average base-line LET of patients in this study was 35.8°C, radiofrequencyapplications were generally terminated at a lower LET than inprevious studies (38.5° to 39°C).2,4,5 Additionally, this ap-proach resulted in only a small rise in LET above the actualLET temperature at which radiofrequency was terminated,and required a short time for the LET to return to baseline—the latter more indicative of less esophageal heating. Theseparameters compare quite favorably to a previously reportedsubseries of patients undergoing AF ablation with generalanesthesia and conventional LET monitoring.2 In their series,Di Biase et al terminated radiofrequency ablation after a LET of39°C was achieved. On average, the maximum LET continuedto rise approximately 1.6°C above the cutoff LET (comparedwith 0.5°C in our cohort) with the LET returning to baselineafter approximately 29 seconds (compared with 18 seconds inour cohort). These differences probably contributed to thedramatic difference in the rate of esophageal injury betweenDi Biase’s and our cohort (48% versus 0%). We speculatethat discontinuation of radiofrequency after a change in LETof 2°C rather than after an absolute temperature is achievedwill account for variability in baseline LET and thermalconduction among patients thereby minimizing esophagealheating.
Table. Patient Demographics
Male sex, n (%) 35 (78)
Age, y, mean�SD 55�14
Left atrial volume, mL, mean�SD 33�11
Left ventricular ejection fraction, %, mean�SD 68�18
Body mass index, kg/m2, mean�SD 29�4
Paroxysmal AF, n (%) 21 (47)
Figure 5. Example of the rise in luminalesophageal temperature during radiofre-quency ablation requiring termination of abla-tion. The y-axis illustrates the increase in LETabove baseline measured with the deflectableLET probe. LET begins to rise approximately9 seconds after the onset of radiofrequencyablation. Point A demonstrates the time pointwhere the LET is 2°C above baseline resultingin termination of radiofrequency ablation. Thisoccurs approximately 1 second after the LETbegins to rise and 10 seconds after radiofre-quency energy was initiated. Point B demon-strates the time that the LET continues to riseafter radiofrequency termination (consistentwith thermal latency). LET continues to risefor approximately 0.5 seconds after RF termi-nation. In this example, 7 seconds of time isrequired for the LET to return to baseline fromthe maximum achieved LET.
154 Circ Arrhythm Electrophysiol April 2011
by guest on May 27, 2013circep.ahajournals.orgDownloaded from

Theoretical Hazards of LET MonitoringCare must be exercised during esophageal instrumentation.For example, manipulation of the LET probe may result intraumatic injury to the esophagus. Distortion of the esophagusmay facilitate heating. Finally, esophageal probes may alterthe current density during ablation facilitating heating. Thelatter concern is not unfounded—for example, Martinekdescribed a high rate of esophageal ulceration in patientsundergoing ablation procedures with nasogastric tubes,9 andMohr reported atrio-esophageal fistulas in 3 patients under-going surgical ablation procedures with concomitantly placedtransesophageal echocardiogram probes.10 However, thesafety of LET monitoring in this study, the increasing supportfor the relationship between LET and esophageal injury, andthe fact that an atrio-esophageal fistula has been reported in apatient without esophageal instrumentation,11 suggests thatthe benefits of LET monitoring outweigh its theoretical risks.
LimitationsLimitations of our work must be acknowledged. First, oursample size was small and may underestimate the frequencyof esophageal thermal injury. Additionally, given the rarity ofLA-esophageal fistula, we cannot definitely conclude that thisstrategy will prevent this complication. Although true, oursample size is similar to that of other series assessingesophageal protection strategies, and the finding of no ulcer-ation in a series of consecutive patients undergoing AFablation, the majority of whom had the procedure performedwith general anesthesia—a known high risk for esophagealinjury,2 is compelling, and has not been reported with otherstrategies. Second, luminal esophageal temperature may notbe representative of intramural esophageal temperature.12
However, there are currently no clinically available methodsof determining intramural esophageal temperature. Third,only the presence of esophageal mucosal injury was assessed.Injury to adjacent structures, which may be detected withmore sophisticated imaging modalities such as MRI13 oresophageal endosonography,14 may be underestimated. Webelieve that the presence of esophageal mucosal injury iscritical to report as this is the presumed precursor to thedevelopment of the LA-esophageal fistula. Fourth, we did notdocument whether there was a specific duration of time afterradiofrequency was applied when LET rises occurred. Al-though one may argue for limiting radiofrequency durationbelow a certain time to avoid temperature rises and hence theneed for LET monitoring, this approach is unlikely to beapplicable to all patients as some patient may have LET risealmost immediately after radiofrequency was applied. Fifth,premature termination of radiofrequency energy may preventadequate LA lesion formation thereby increasing the likeli-hood of PV reconnection. Although theoretically possible,this was not noted in our cohort where rates of freedom fromAF were similar to that reported by others. Sixth, this strategymay not be widely adopted by all electrophysiologists, giventhe cost of using an ablation catheter as a LET probe and ICEcatheter to visualize the esophagus, and comfort with usingICE. Although true, should this strategy be proven to bereproducible then efforts must be made to ensure that acost-effective alternative is available given the potential
benefits associated with elimination of esophageal thermalinjury. Finally, there was no control group in our series ofpatients which may prevent one from commenting on the trueefficacy of this approach. Although true, the rate of esopha-geal ulceration in our cohort was lower than that historicallyreported by others.2,4,5
Further work is necessary to determine (1) the optimal LETrise from baseline at which radiofrequency should be termi-nated, (2) whether other methods of real-time visualization ofthe esophagus (for example barium ingestion) are an accept-able alternative to the use of ICE imaging and useful insituations in which the esophagus is unable to be visualizedon ICE (such as the case of our patient with severe LAdilation), (3) whether this approach will be tolerated inpatients undergoing AF ablation procedures with conscioussedation, and (4) whether there is additional merit to physi-cally deflecting the esophagus away from the LA with thedeflectable LET probe during ablation at sites associated withLET rises. It is important to note that we did not intend toactively deflect the esophagus when the deflecting the LETprobe—the fact that the esophagus was visualized on ICEbefore positioning or deflecting the LET probe (Figure 2) isconsistent with simply placing the LET probe in positionrather than deflecting the esophagus to that location. Finally,given the importance of this topic, confounders relating topatient and ablation strategies, we strongly encourage con-ducting a large multicenter, randomized study to adequatelyassess the merits of LET on reducing esophageal injury.
In conclusion, a strategy of optimal LET probe placementusing a deflectable LET probe and ICE guidance, combinedwith cessation of radiofrequency ablation with a 2°C rise inLET, is another tool which may reduce esophageal thermalinjury during AF ablation procedures.
DisclosuresNone.
References1. Cappato R, Calkins H, Chen SA, Davies W, Iesaka Y, Kalman J, Kim
YH, Klein G, Natale A, Packer D, Skanes A, Ambrogi F, Biganzoli E.Updated worldwide survey on the methods, efficacy and safety of catheterablation for human atrial fibrillation. Circ Arrhythm Electrophysiol.2010;3:32–38.
2. Di Biase L, Saenz LC, Burkhardt DJ, Vacca M, Elayi CS, Barrett CD,Horton R, Bai R, Siu A, Fahmy TS, Patel D, Armaganijan L, Tung C, KaiS, Ching CK, Phillips K, Sckweikert RA, Cummings JE, Arruda M,Saliba WI, Dodig M, Natale A. Esophageal capsule endoscopy afterradiofrequency catheter ablation for atrial fibrillation: documented higherrisk of luminal esophageal damage with general anesthesia as comparedwith conscious sedation. Circ Arrhythm Electrophysiol. 2009;2:108–112.
3. Sanchez-Quintana D, Cabrera JA, Climent V, Farre J, de Mendonca MC,Ho SY. Anatomic relations between the esophagus and left atrium andrelevance for ablation of atrial fibrillation. Circulation. 2005;112:1400–1405.
4. Singh SM, d’Avila A, Doshi SK, Brugge WR, Bedford RA, Mela T,Ruskin JN, Reddy VY. Esophageal injury and temperature monitoringduring atrial fibrillation ablation. Circ Arrhythm Electrophysiol. 2008;1:162–168.
5. Rillig A, Meyerfeldt U, Birkmeyer R, Wiest S, Sauer BM, Staritz M, JungW. Oesophageal temperature monitoring and incidence of oesophageallesions after pulmonary vein isolation using a remote navigation system.Europace. 2010;12:655–661.
6. Pinherio M, Ferreira O, Deseta D, Francisquini A, Abufaiad B, Bron-chtein AI, Araujo N, Tavares F, Bronchtein S, Scanavacca M, D’Or R.Case report of an atrio-esophageal fistula after atrial fibrillation catheter
Leite et al LET Monitoring Guided by ICE During AF Ablation 155
by guest on May 27, 2013circep.ahajournals.orgDownloaded from

ablation occurring in a patient with esophageal temperature monitoring[Abstract]. Heart Rhythm. 2010;7:S194.
7. Vijayaraman P, Netrebeko P, Geyfman V, Dandamudi G, Casey K,Ellenbogen K. Esophageal fistula formation despite esophageal moni-toring and low-power radiofrequency catheter ablation for atrial fibril-lation. Circ Arrhythm Electrophysiol. 2009;5:e31–e33.
8. Zar JH. Biostatistical Analysis. 2nd edition. Englewood Cliffs, NJ:Prentice Hall, 1984;378.
9. Martinek M, Bencsik G, Aichinger J, Hassanein S, Schoefl R, Kuchinka P,Nesser HJ, Purerfellner H. Esophageal damage during radiofrequencyablation of atrial fibrillation: impace of energy settings, lesions sets, andesophageal visualization. J Cardiovasc Electrophysiol. 2009;20:726–733.
10. Mohr FW, Fabricius AM, Falk V, Autschbach R, Doll N, von Oppell U,Diegeler A, Kottkamp H, Hendricks G. Esophageal injury during radio-frequency ablation for atrial fibrillation. J Thorac Cardiovasc Surg.2002;123:919–927.
11. Gillinov AM, Pettersson G, Rice TW. Esophageal injury during radio-frequency ablation of atrial fibrillation. J Thorac Cardiovasc Surg. 2001;122:1239–1240.
12. Cummings JE, Barrett CD, Litwak KN, Di Biase L, Chowdhury P, OhS, Ching CK, Saliba WI, Schweikert RA, Burkhrdt JD, De Marco S,Armaganijan L, Natale A. Esophageal luminal temperature mea-surement underestimates esophageal tissue temperature during radio-frequency ablation within the canine left atrium: comparison between8mm tip and open irrigation catheters. J Cardiovasc Electrophysiol.2008;19:641– 644.
13. Badger TJ, Adjei-Poku YA, Burgon NS, Kalvaitis S, Shaaban A,Sommers DN, Blauer JEJ, Fish EN, Akoum N, Haslem TS, Khol-movski EG, MacLeod RS, Adler DG, Marrouche NF. Initial expe-rience of assessing esophageal tissue injury and recovery usingdelayed-enhancement MRI after atrial fibrillation ablation. CircArrhythm Electrophysiol. 2009;2:620 – 625.
14. Zellerhoff S, Ullerich H, Lenze F, Meister T, Wasmer K, Monnig G,Kobe J, Milberg P, Bittner A, Domschke W, Breitherdt G, Echardt L.Damage to the esophagus after atrial fibrillation ablation: just the tipof the iceberg? High prevalence of mediastinal changes diagnosed byendosonography. Circ Arrhythm Electrophysiol. 2010;3:155–159.
CLINICAL PERSPECTIVEThe close proximity of the esophagus to the left atrium places it at risk for thermal injury during atrial fibrillation ablationprocedures. Luminal esophageal temperature monitoring has been proposed as one method of reducing esophageal thermalinjury. However, esophageal ulceration and atrio-esophageal fistula have been reported with the current methods used tomonitor luminal esophageal temperature. In these situations, the esophageal probe can only be manipulated in acraniocaudal direction. The inability to laterally deflect current esophageal temperature probes limits their ability to detectthe “hot test” spots within the esophagus. In this pilot study, we report a novel method of esophageal temperaturemonitoring with the use of a deflectable esophageal temperature probe, which, using intracardiac echocardiographyguidance, was positioned in the esophageal lumen at the site closest to that where left atrial catheter ablation wasperformed. This approach, combined with cessation of radiofrequency catheter ablation with any 2°C rise in esophagealtemperature, was used in a series of 45 patients, all of whom underwent non–symptom-driven esophageal endoscopy within48 hours of the catheter ablation procedure. No patient had esophageal injury in this series. These results suggest thataccurate esophageal temperature monitoring with the use a deflectable esophageal temperature probe positioned withintracardiac echocardiography guidance, combined with cessation of radiofrequency ablation with a rise in luminalesophageal temperature of 2°C, may prevent esophageal thermal injury.
156 Circ Arrhythm Electrophysiol April 2011
by guest on May 27, 2013circep.ahajournals.orgDownloaded from

SUPPLEMENTAL MATERIAL
Supplemental Online Video 1: Distortion of the esophagus by the LET probe.
Supplemental Online Video 2: Repositioning of the LET probe which no longer distorts
the esophagus.
by guest on May 27, 2013circep.ahajournals.orgDownloaded from