130266099752028203_VR-VTH Breast Cancer tab online
16
DECODING BREAST CANCER Whether it’s a perfectly healthy woman volunteering for a biopsy, an 8-year-old girl allowing her habits to be tracked or Hollywood shining its bright lights on gene testing, the fight to crack the deadly code of breast cancer is leaving no stone unturned. Special Section Sunday, October 20, 2013 INSIDE THE SILVER SCREEN: “DECODING ANNIE PARKER” A GUIDE TO BRCA GENE TESTING HOW AN 8-YEAR-OLD COULD HELP CURE BREAST CANCER KAISER: EARLY DETECTION IS KEY STATISTICS DON’T TELL THE WHOLE SOLANO GROUP OFFERS 3-D IMAGING
-
Upload
jordan-cabrera -
Category
Documents
-
view
106 -
download
0
Transcript of 130266099752028203_VR-VTH Breast Cancer tab online
16 The Reporter • Times Herald • Sunday, October 20, 2013
DECODING BREAST CANCER
Whether it’s a perfectly healthy woman volunteering for a biopsy, an 8-year-old girl allowing her habits to be tracked
or Hollywood shining its bright lights on gene testing, the fight to crack the deadly code of breast cancer
is leaving no stone unturned.
Special SectionSunday, October 20, 2013
INSIDE
COURTESY NORTHBAYHEALTCARE
Thanks to an investmentin some high-tech software,Solano DiagnosticsImaging in Vacavilleis now the onlyentity in SolanoCounty that cur-rently offers 3-Dmammography, atool that is especial-ly helpful in diag-nosing or ruling outcancer in womenwith dense breasts.
In April, California passeda law requiring patients with“Heterogeneously DenseBreasts” or “ExtremelyDense Breasts” be notified oftheir density score and pos-sible risk for breast cancer. Itis estimated that nearly 50percent of all women whocurrently receive mammo-grams will soon learn theyhave dense breasts.
“If a woman knows shehas dense breasts, she canelect to come to SDI inVacaville for a 3-D mammo-gram instead of relying on astandard mammogram,”explains Adrian Riggs, direc-tor. “If she gets a standardmammogram, there’s a goodchance her doctor will referher to have images takenusing the 3-D technology.
She might as well go rightfor the best technology first.”
Rather than taking twoimages, as is done in stan-
dard mammography,breast tomosynthesistakes multiple low-dose images of thebreast and synthe-sizes them into athree-dimensionalimage. This allowsradiologists to exam-ine the breast in very
thin layers. The digital image allows
the radiologist to rotate thetissue in front of or behindan abnormality, makingdetection easier. In addition,overlapping tissue that mayappear abnormal on a stan-dard mammogram can bedetermined to be benign ina 3-D image.
Breasts are composed offatty tissue, milk lobules,milk ducts and connectivetissue. The greater theamount of milk ducts, milklobules and connective tis-sue, the denser the breast.
On a mammogram,denser breast tissue appearswhite, while fatty tissue isgray, explains Dr. JasonMarengo, an oncoplasticsurgeon with the NorthBayCenter for Specialty Care.“Typically when a cancer is
found on a mammogram, itis also white. With verydense breasts, it can be diffi-cult to clearly see cancer. It’slike trying to find a whitesnowflake against a whitebackground,”
For the patient, getting a3-D mammogram firsttranslates into fewer “callbacks” for additional mam-mographic views, fewerunnecessary biopsies, detec-tion of concerning massesthat may have beenobscured by surroundingbreast tissue and fewersleepless nights, says Dr.Marengo.
A patient doesn’t have tobe associated with NorthBayHealthcare patient to get a3D screening at SDI inVacaville, notes Riggs. “Justask your doctor for a refer-ral.”
Solano County facilityoffers mammography
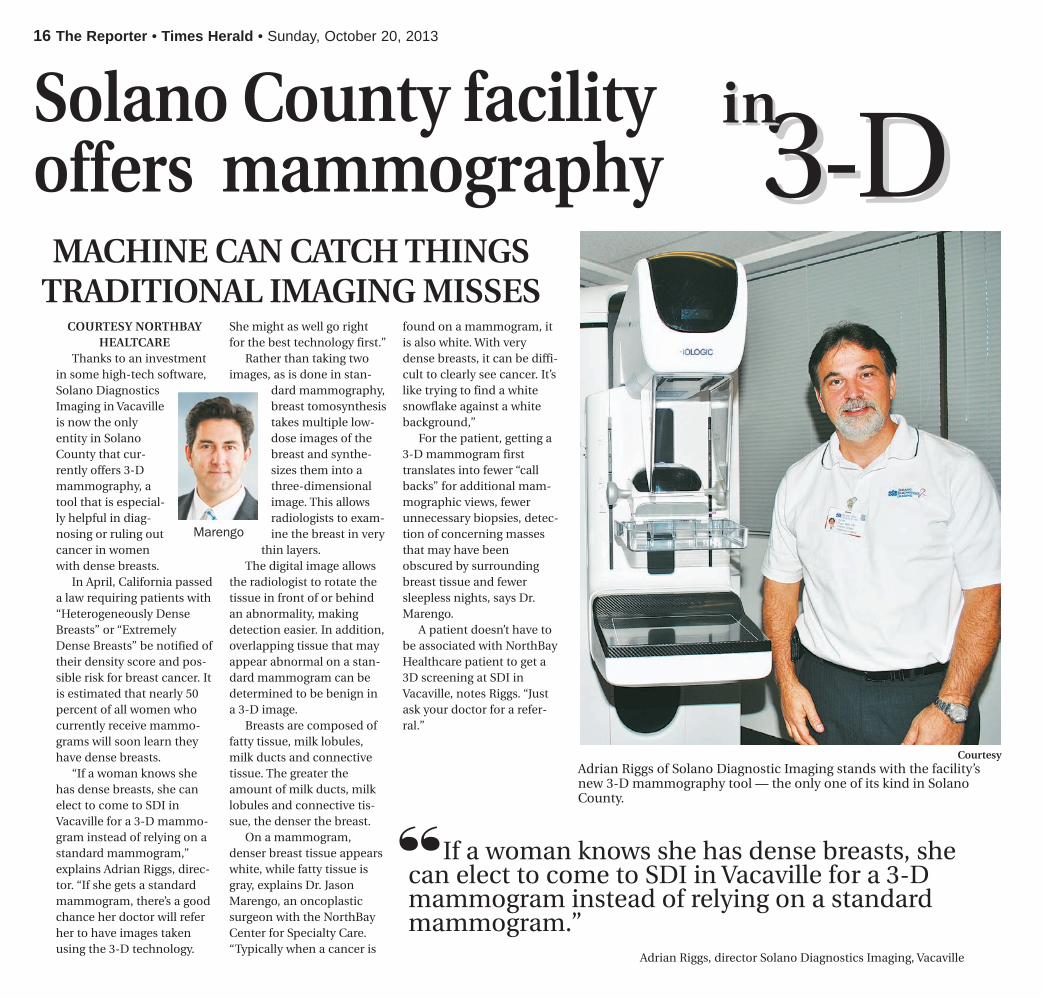
CourtesyAdrian Riggs of Solano Diagnostic Imaging stands with the facility’snew 3-D mammography tool — the only one of its kind in SolanoCounty.
Marengo
33--DDinin
MACHINE CAN CATCH THINGSTRADITIONAL IMAGING MISSES
If a woman knows she has dense breasts, shecan elect to come to SDI in Vacaville for a 3-Dmammogram instead of relying on a standardmammogram.”
Adrian Riggs, director Solano Diagnostics Imaging, Vacaville
“THE SILVER SCREEN:“DECODING ANNIEPARKER”
A GUIDE TOBRCA GENETESTING
HOW AN 8-YEAR-OLDCOULD HELP CUREBREAST CANCER
KAISER: EARLYDETECTIONIS KEY
STATISTICSDON’T TELL THE WHOLE
SOLANO GROUPOFFERS 3-DIMAGING

14 The Reporter • Times Herald • Sunday, October 20, 2013 Sunday, October 20, 2013 • Times Herald • The Reporter 3
BY RACHEL RASKIN-ZRIHENTimes-Herald staff writer
It was just before Thanksgiving threeyears ago that I had my last radiationtreatment, against doctor’s orders.
Sort of.I had undergone, I think, six chemo
treatments after my surgery to remove avery small, very earlycancerous tumor frommy left breast, and,what seemed like sev-eral thousand dailydoses of radiation.
I drove myself tothese treatments afterwork every day atNapa’s Queen of the
Valley Hospital, and then home, fightingthe infamous traffic on Highway 29through American Canyon at rush hour— a serious misnomer, since it lasts sig-nificantly longer than an hour.
Though everyone was lovely at theQueen, I only got through the wholething with my sanity by counting downthe days until it was over. I had figuredout — and bear in mind that figuring outanything was a real feat during this men-tal Swiss-cheese time of my life — that
the last treatment was going to be theday before Thanksgiving, and I wascounting on that. It seemed appropriate,somehow; like a message.
However, on the day that was sup-posed to be my last treatment, I wasinformed that their radiation machinehad malfunctioned in some way and Ineeded to come back one more time,after the holiday.
Not going to happen.“I planned on today being the last
one and that’s what it’s going to be,” Isaid. “Not that I don’t love you guys, but,
no offense, I never want to see any ofyou again in a professional capacity.”
And so far, I haven’t.Since my diagnosis in May, 2010, I’ve
spoken with a lot of people, some ofthem experts, and done a lot of readingon the issue, and have learned that acertain percentage of people with thesame thing I had elect different coursesof treatment. I went with the mostaggressive form because I was told itgave me the best chance to avoid arecurrence, and that’s what I want. Norepeat.
But I know people who have optedfor surgery alone, and some who havechosen chemo only or just radiation, orsome combination. I chose to go wholehog, so to speak.
So far, all but one of the way-too-many of my friends who have had thisdisease, are all still alive, thank God. But,we did lose one very important personto this crummy disease, and it wasbecause by the time she caught it, it hadalready spread. She lived a decade withit — long enough to see her daughtermarried and to meet her grandson — ahuge blessing.
Fahni was an inspiration to everyonewho knew her and a living testament tohow far medicine has come in the treat-ment of breast cancer.
But, hers is also a cautionary tale,with the moral of the story being, checkyourself. No one knows your body aswell as you do. And if you think you feelsomething, get it checked. Don’t wait. It’sprobably nothing, but, as the sayinggoes, better safe than sorry.
Contact staff writer Rachel Raskin-Zrihen at 553-6824 [email protected].
Vallejo writer recalls own battleLESSONS LEARNED, FRIENDS
LOST TO BREAST CANER
Raskin-Zrihen
I had figured out — and bear in mind that fig-uring out anything was a real feat during this men-tal Swiss-cheese time of my life — that the last treat-ment was going to be the day before Thanksgiving,and I was counting on that. It seemed appropriate,somehow; like a message.”
WASHINGTON (AP) — Abiotech drug that Roche makesat Vacaville’s Genentech facility,has become the first medicineapproved to treat breast cancerbefore surgery, offering an earli-er approach against one of thedeadliest forms of the disease.
Earlier this month, the Foodand Drug Administrationapproved Perjeta for womenwith a form of early-stage breastcancer who face a high risk ofhaving their cancer spread toother parts of the body.
Surgery to remove tumors isusually the first step in treating
most forms of cancer. Perjeta isthe first drug to be approved asa pre-surgical step. Doctorshope that using cancer drugsearlier could help shrink tumors,making them easier to remove.In some cases, that could allowwomen to keep their breasts,rather than having a full mastec-tomy. Doctors also say thattreating the disease at its earlieststages could prevent tumorsfrom returning later, thoughstudies have not yet establishedthat benefit.
“By making effective thera-pies available to high-risk
patients in the earliest diseasesetting, we may delay or preventcancer recurrences,” said FDA’sDr. Richard Pazdur, who directsthe agency’s office of cancerproducts.
Cancer specialists already useseveral chemotherapy drugs asinitial treatments for cancer, butthey are not formally approvedfor the use. The FDA originallyapproved Perjeta to treat breastcancer that has spread to otherparts of the body after surgery.
The FDA granted the drugaccelerated approval for its newuse based on a study showingwomen who received the drug
as an initial treatment weremore likely to be cancer-free 12weeks later than women whoreceived older drug combina-tions. Accelerated approval isreserved for drugs that showgroundbreaking results for treat-ing life-threatening diseases inearly studies.
As a condition of approval,Roche’s Genentech unit mustconduct a larger follow-up studyshowing the drug’s long-termbenefits for patients. Generallythat means showing thatpatients lived longer or had ahigher quality of life due to tak-ing the drug. Genentech, based
in South San Francisco, Calif.,has already enrolled about 4,800patients in the follow-up study,with results expected in 2016.
Dr. Paula Klein, a breast can-cer specialist, said she will startprescribing the drug for early-stage patients immediately, butstressed the importance of fol-low-up data on patient survival.
“This does not yet proveto us that using the antibody inthis setting will result in morecures. That is still a hypothesis,”said Klein, who directs thebreast cancer program atContinuum Cancer Centers ofNew York.
Pre-surgery breast cancer drug made in Vacaville
“
heavy emotional and health burden if you carry this mutation, but in my mind, I was also given the gift of knowl-edge. That knowledge has enabled me to be more proactive with my health.”
Schlager, who lives near Washington, D.C., decided to get tested after an aunt found out she was BRCA positive and approached Schlager about consid-ering a gene test. Though Schlager had some breast cancer in her family history, she never thought it enough to be a troubling pattern.
“Not knowing much about BRCA mutations at all, I agreed to get tested,” she said. “I, too, came back positive for the BRCA1 mutation.”
Schlager decided to do surveillance for eight years before moving forward with surgeries to remove her ovaries, fallopian tubes and breasts. At the time of her diagnosis, the field of heredi-tary cancer research was still brand new. Schlager didn’t know anyone confronting the same health decisions she faced. FORCE, a national non-profit devoted to fighting hereditary breast cancer and ovarian cancer, had just been founded. Today, Schlager is FORCE’s spokeswoman. She is passionate about sharing her story and connecting women with resources and with one another.
“Every woman finds her path,” Schlager said. “Ultimately, although I thought I would never do it, I did go forward with surgery. I don’t regret it, and I don’t wish I had done it earlier. I think it was the perfect path for me.”
The right path may be different --even for women in the same family. JudyPollak, 64, was diagnosed with breastcancer when she was 25, around thetime of Annie Parker’s diagnosis andlong before the genetic links in breastcancer were understood. The Maryland
optical storeowner survived her cancerand went on to have two daughters, bothof whom also carry the mutation.
Pollak’s daughters, now 29 and 27, opted for different preventative measures after their BRCA tests. One chose a prophylactic mastectomy and the other chose surveillance.
“It’s very hard for me because I wor-ry,” Pollak said. “But mothers worry no matter what. Life is not ending, it’s just a different route that you’re taking. You look at yourself and say, ‘I’ll beat this.’ And you meet these women, we are phenomenal women that are survivors, that could accomplish anything.”
Pollak didn’t find out about her faulty BRCA gene until years after her diagnosis when, in the early 1980s, she participated in a study that sought women who had been diagnosed with breast cancer at a young age.
“I had never heard the word BRCA,”Pollak said. “I always thought my breastcancer came from my mother, who atage 70 had a mastectomy, but now Iknow it was totally unrelated. My BRCAis from my father, not from my mother.”
Even today, science is at the “tip of the iceberg” in understanding BRCA mutations and the link to cancer, according to Deborah Armstrong, a professor of oncology, gynecology and obstetrics at Maryland’s Johns Hopkins Kimmel Cancer Center and director of the hospital’s breast and ovarian genet-ic counseling and screening service.
“One of the biggest issues that has remained is that BRCA1 and BRCA2 only explain about half of familial breast cancers,” Armstrong said. “As the 1990s went on, (after the initial discovery of those gene mutations), we expected that we would have a BRCA3 and BRCA4 that would explain a pretty big chunk of these women at risk who
What is BRCA gene testing?
Everyone has BRCA genes that produce
tumor-suppressing proteins. But risky BRCA1
and BRCA2 gene mutations leave a person
more susceptible to cancers, including breast
and ovarian cancers. BRCA testing is used
to determine whether a person has such a
mutation, which can be inherited from either
parent. Each child of a parent who has a mu-
tation in one of these genes has a 50 percent
chance of inheriting the mutation.
What does the test entail?
BRCA gene mutations are detectable
through DNA from a blood or saliva sample.
It usually takes about a month to get results
once your sample is sent to a lab for analysis.
What does a positive result mean?
A woman’s lifetime risk of developing can-
cer is “greatly increased,” if she has a harmful
BRCA mutation, according to the National
Institutes of Health. About 12 percent of
women will develop breast cancer at some
point compared with up to 65 percent of
women who inherit a harmful BRCA1 muta-
tion. Other cancers are linked to mutations in
BRCA1 and BRCA2, including fallopian tube,
abdominal and pancreatic cancers. Men with
harmful BRCA gene mutations face higher
risk of prostate cancer.
How common are high-risk BRCA
gene mutations?
The likelihood of carrying a BRCA gene
mutation is extremely low for people with no
family history of breast or ovarian cancer. Only
about 10 percent of all breast cancers and 15
percent of all ovarian cancers can be traced
back to inherited genetic mutations.
Who should take the test?
Because BRCA gene mutations are
relatively rare, many doctors agree only those
who have specific family patterns of cancer
should consider the test. Such patterns
include having multiple family members who
have been diagnosed with breast or ovarian
cancer, especially at a young age; cases of
male breast cancer; and two or more cancers
in one family member.
For anyone thinking about such testing,
experts strongly recommend genetic counsel-
ing by someone who is experienced in cancer
genetics. Counseling can help assess the need
for testing in the first place, as well as facilitate
discussion about what kinds of decisions a
person faces once she gets her results.
What kinds of decisions should you
be prepared to make?
A person who finds out she has a BRCA
gene mutation faces some difficult decisions.
Some women choose enhanced cancer
screening, beginning with regular mam-
mograms in their 20s, for example. Others
choose risk-reducing surgeries like mas-
tectomies or the removal of the ovaries and
fallopian tubes. People also consider chemo-
prevention regimens of drugs and vitamins to
delay or reduce cancer risk. Finding out you
have a harmful BRCA mutation indicates a
higher risk for your siblings, too, so what you
learn can affect multiple family members.
How much does it cost?
Some insurance companies cover BRCA
testing, which can range in cost from hun-
dreds to thousands of dollars. The National
Cancer Institute urges people to contact their
insurance companies to discuss cost before
getting the test. For those without insurance,
some genetic testing companies offer free
or discounted pricing for individuals who
meet certain medical or financial eligibility
standards.
Who can help?
There are myriad resources for people
considering BRCA gene testing, including the
Cancer Information Service at the National
Institutes of Health (NIH) and many nonprofit
organizations. Live and anonymous online
chatting is available from the NIH weekdays
from 8 a.m. to 11 p.m. ET (5 a.m. to 8 p.m. PT
at http://livehelp.cancer.gov. You can also call
1-800-4-CANCER.— Adrienne LaFrance
A guide to BRCA gene testing
“It’s very hard for me because I worry (about herdaughters). But mothers worry no matter what.
Life is not ending, it’s just a different route that you’retaking. You look at yourself and say, ‘I’ll beat this.’ Andyou meet these women, we are phenomenal womenthat are survivors, that could accomplish anything.”Judy Pollak, 64, diagnosed with breast cancer when she was 25, around the time of Annie Parker’s diagnosis. She survived her cancer and went on to have two daughters, both of whom also carry the mutation.
Continued from page X
Continued on page X
4 The Reporter • Times Herald • Sunday, October 20, 2013 Sunday, October 20, 2013 • Times Herald • The Reporter 13
Continued from page 2
Continued on page 5
Sutter Fairfield Imaging willhost a free mammography day forpre-registered, uninsured womenage 40 and older on Oct. 26.
Space is limited, that’s whywomen are asked to call inadvance for the free digital screen-ing mammogram.
Women will receive theirresults from Sutter FairfieldImaging within several days aftertheir visit. Sutter Fairfield Imagingwill connect women who have anabnormal result to local not-for-profit agencies with which Sutterregularly partners so patients maytake next steps and receive follow-up care.
The free mammograms will beconducted from 8 a.m. to 3:30p.m. Oct. 26 at Sutter FairfieldImaging, 2700 Low Court inFairfield. Call 432-2500 to register.
Sutter’s Free MammographyDays was spearheaded at SutterAuburn Faith Hospital in 2009,where in two years’ time about 70uninsured women were given freemammograms. Inspired by thefeedback and success of the pro-gram, Sutter Diagnostic Imagingexpanded it to its other locationsin Davis, Elk Grove, Roseville andSacramento in 2011, and inFairfield, Jackson and Vallejo in2012. Sutter was able to give 358uninsured women free digitalscreening mammograms last year.
For more information aboutSutter Diagnostic Imaging centers,call 1-877-515-0053 or visitwww.checksutterfirst.org/imaging.
Sutteroffers free
exams
BY KATIE RASILA, M.D.Sutter Medical Group
Statistics regarding breast cancerfrom the American CancerSociety paint a positive picture:
incidence was stable from 2005-2009and deaths have been steadily decreas-ing since 1989. Still, the ACS estimatesthat more than 232,000 new cases ofbreast cancer will be diagnosed thisyear, and nearly 40,000 women will diefrom it-making it the second deadliestcancer for women (after lung cancer).
No one is immune from breast can-cer. Many of the risk factors —beingfemale, advancing age, family history,early menarche and late menopause-can’t be changed. Risk factors that canbe changed include obesity, use of hor-mone replacement therapy, physicalinactivity and alcohol consumption.
As is true for all cancers, earlydetection is key to successful treat-ment. The ACS recommends annualmammograms beginning at age 40. Inaddition, MRI scans may be appropri-ate for some women who are at highrisk.
Solano County women diagnosedwith breast cancer are fortunate tohave state-of-the-art treatment avail-able at the Sutter Solano CancerCenter in Vallejo. Our multidisciplinaryteam includes professionals to treatand guide patients throughout theircancer odyssey: surgeons, medicaloncologists and radiation oncologists,social workers, psychologists, nutri-tionists and patient navigators. Inaddition, several support groups areavailable for patients and their families
— helping heal them as a whole.Being under one roof helps our
team’s ability to communicate and beon the same page, which leads to ahigher level of personalized care. Weunderstand how anxious patients areafter receiving a cancer diagnosis andtake the time to ensure they under-stand all their options and can makethoughtful decisions about the righttreatment plan for them.
The treatment of breast cancer isindividualized; a number of factors willdetermine the recommended course ofaction for each patient, including thesize, grade, node status and stage ofthe tumor and whether it’s hormonereceptor positive or negative.Treatment alternatives may includemastectomy, breast-conserving sur-gery (lumpectomy), radiation,chemotherapy, hormone-blockingtherapy and targeted/biologic therapy.As an American College of Surgeons-accredited cancer treatment facility,the Sutter Solano Cancer Center teamis well equipped to provide patientswith the tools, information and
resources they need to make decisionsregarding their treatment.
Dr. Rasila, a member of Sutter MedicalGroup and the Sutter Solano CancerCenter medical team, specializes in med-ical oncology and hematology. She seespatients in Fairfield and Vacaville andcan be reached at 427-4900.
Statistics don’t tellthe whole story
No one is immune from breast cancer.Many of the risk factors — being female,advancing age, family history, early menarcheand late menopause-can’t be changed. Riskfactors that can be changed include obesity,use of hormone replacement therapy, physicalinactivity and alcohol consumption.”
Katie Rasila, M.D., Sutter Medical Group.
EARLY DETECTION VITAL TOSUCCESSFUL TREATMENT
“

had familial inheritance patterns. But we haven’t.”
Meantime, medicine is becomingmore and more personalized. The ideaof treatment plans tailored to a person’sunique genes is gaining popularity, es-pecially after a Supreme Court decisionearlier this year said naturally occurringgenes are no longer patentable. Thedecision paves the way for cheapergene testing by more companies, whichmakes it more important than everfor people to seek reliable informationbefore considering a gene test.
“In terms of what’s changing over time is, first, just the uptake of testing, but also the types of tests we can do now,” said Rebecca Nagy, president of the National Society of Genetic Counselors. “When I first started, and even just 5 years ago, we really focused on one or two genes at a time. Now we can test for 20 or 30 genes at a time for the same cost as two or three genes. Technology has changed the game.”
While testing tools evolve at a break-neck pace, many women are actively working to increase awareness about testing. Doctors and cancer survivors strongly urge people considering a gene test to seek genetic counseling first. Counselors help a person de-termine whether a test is advisable, which test to take and what decisions she might have to make depending
on results. While BRCA1 and BRCA2 mutations are relatively rare, those who are at risk might not necessarily realize it.
“I got my gene through my father’s father’s father. I found out in January of 2006 that the mutation was present in my family and in February of 2006 I had the first symptom (of ovarian cancer) so there wasn’t time for me to really do anything with that infor-mation,” said Carey Fitzmaurice, a 45-year-old senior policy analyst at the Environmental Protection Agency in Washington, D.C., who has a BRCA gene mutation and battled both breast cancer and ovarian cancer. “That’s one of the reasons why I am determined to make people aware of this.
Raising that awareness is one of the main goals that Parker has for “Decod-ing Annie Parker.” The film’s unique distribution model means it’s getting screened with partner charities around the country. Half of the revenue from each event goes back to the charities, already nearly half a million dollars, according to the film’s director Steve Bernstein.
While “Decoding Annie Parker” tells the story of Parker and the race to identify the BRCA gene, the film is ul-timately about something much bigger, even though much of it is funny.
“The first three-quarters of the film
are essentially a comedy,” Bernsteinsaid. “It’s about people overcoming ob-stacles, the indomitable human spirit. Alot of times the audience is laughing, andat the end of the film it’s life affirming.Are there a few tears along the way? Ab-solutely. We’ve shown the film 20 times,and we’ve had 18 standing ovations.”
Above all, Bernstein says he set out to explore what happens to people when day-to-day comforts are stripped away in the face of real adversity. Of-ten, he says, human beings are capable of more strength and empathy than anyone might believe possible.
“We get to the real essence of self,” Bernstein said. “Annie’s a very charm-ing person who had to face cancer not once but has been diagnosed with can-cer three separate times. This woman, who has repeatedly faced death, is someone who refuses to find
death depressing. The Annie Parkers of the world believe that if they will themselves to live, they can live.”
Parker, now 62, still embodies that spirit. She recalls getting the news that she had ovarian cancer, eight years after her breast cancer diagnosis. Doc-tors were pessimistic.
“I was well into the third stage and almost the fourth stage, so I was told to go home and get my things in order,” Parker recalls. “Well, if somebody tells me that, I’m up for the challenge.”
Today, Parker’s health is good. And as she travels the country to screen the film, she takes the memories of her mother and sister with her.
“I have them on my shoulder at every screening, my mom sitting on one and my sister on the other,” Parker said. “This is my family story, but it’s many families’ story.”
“Decoding’s” Samantha Morton, left, stars as Annie Parker, who, with geneticist Mary-Claire King (Played by Helen Hunt, right), uncovered a hereditary cause for some breast cancers and spearheaded research that led to the identification of the BRCA gene mutation. Jeff Berline, Berline Creative
“Annie’s a very charming person who had to facecancer not once but has been diagnosed with
cancer three separate times. This woman, who hasrepeatedly faced death, is someone who refuses tofind death depressing. The Annie Parkers of theworld believe that if they will themselves to live,they can live.” Director Steve Bernstein.
Continued from page X
12 The Reporter • Times Herald • Sunday, October 20, 2013 Sunday, October 20, 2013 • Times Herald • The Reporter 5
Continued from page 4
6 The Reporter • Times Herald • Sunday, October 20, 2013 Sunday, October 20, 2013 • Times Herald • The Reporter 11
He didn’t say ‘treatable’ but‘curable’ and that was animportant distinction forme.”
“Understanding one’srisk for developing breastcancer is very important,”said Dr. Marzban Rad, sub-chief for Breast Imaging forKaiser Permanente in theNapa Solano area. “It isimportant for women tounderstand that ‘risk’ is thechance that something willhappen, not that it defi-nitely will happen.”
According to Rad theprimary risk factors fordeveloping breast cancerare being a woman andgetting older. Other impor-tant risk factors includehaving a first degree rela-tive (a mother, daughter orsister) with breast cancer,and pregnancy (having kidsversus not). Maintaining ahealthy weight, having anactive lifestyle and decreas-ing alcohol consumptionare all important in reduc-ing risk as well.
“Kaiser Permanente iscommitted to offeringcomprehensive breast care.That is why we offer same-day mammogram service,’”added Dr. Rad. “If a patientis called back from herscreening mammogramand needs further review,
she can have everything,like a second mammogramand biopsy, done with justone trip, which helps alle-viate anxiety for thepatient.”
In the Napa Solano area,Kaiser Permanente diag-noses eight cases of breastcancers for every 1,000mammograms they per-form.
“We take a multi-disci-plinary team approach tobreast cancer treatment,”explained Rad. “EveryTuesday we have a medicalconference at our VallejoMedical Center with breastimaging radiologists, breastsurgeons, oncologists, radi-ation oncologists, patholo-gy and nursing to discusseach individual case to cre-ate the most effective treat-ment plan for ourpatients.”
“My experience at KaiserPermanente made a hugedifference in my care,” saidWick. “Some of my friendsdon’t have Kaiser and aren’tconnected like I am. I reallylove being connected andgetting emails from mydoctor — even on week-ends. They really lookedout for me and you couldtell the care here is allabout the person.”
Continued from page 4
Ryan Chalk/[email protected] Velasquez smiles gratefully at Jordan Cabrera, the Kaiser employee who she credits with savingher life. He called to remind her she was past due for a mammogram. When she got the proceduredone, Velasquez learned she had breast cancer but it was caught early enough to be successfullytreated.Velasquez and Cabrera met face-to-face for the first time in May — just in time for Mother’sDay.
They caught it early because ofthat call. Had it been seen six monthslater it could have been a very differentstory.”
Breast cancer survivor Sarah Velasquez
“

BY KIRSTEN STEWARTSalt Lake Tribune
Cindy Solomon chuckles while she watches 8-year-old Ella pour a packet of sugar into her own mouth, stimu-lating her salivary glands to produce a “spit sample” for testing at Huntsman Cancer Institute.
For Ella, the sugar is a rare treat. For her health-conscious mom, it’s a nutritional sacrifice for science.
The Solomons are among 1,000 moth-er-and-daughter duos from the UnitedStates and Canada taking part in a long-term study of environmental, dietaryand family links to breast cancer.
Funded by the U.S. National Insti-tutes for Health, the “Legacy” study represents a shift in the focus of cancer research from diagnosis and treatment to prevention. And it’s one of the few involving girls so young, between ages 6 and 13.
Ella has no significant family history of cancer. Her mom heard about the study through a neighbor.
“We talked about how it would help scientists better understand cancer,” said Cindy, who told Ella that even though she’s not at risk, “You know people who have had the disease, and if you can help scientists and it’s fun, why not do it?”
Traditionally, researchers have focused on older women, asking them to recall details about their lives that may have predisposed them to breast cancer, said Saundra Buys, a principal investigator and co-director of the High Risk Breast Clinic at Huntsman.
“But more and more younger women are being diagnosed,” said Buys.
And increasingly risk factors are be-ing traced back to our early years, she
said. “As we follow these girls along, we’ll hopefully come up with some interesting hypotheses for things we can do in childhood or even in prenatal life to decrease the risk.”
Legacy — an acronym for Lessons in Epidemiology and Genetics of Adult Cancer from Youth — is being done at Breast Cancer Registry sites in San Francisco, New York, Philadelphia, Toronto and Salt Lake.
The Solomons are among 150 en-rolled through Huntsman.
Every six months for at least five years they will answer detailed ques-tionnaires about their exercise habits, the food they eat and the cosmetics,
hair gels and perfumes they use. Ella will be measured and weighed
and will volunteer saliva and urine for testing hormonal and genetic changes.
She also agreed to give blood — it’s optional — which didn’t seem to bother the wiggly, giggly girl at her last clinic appointment in August.
Clinic visits are kept upbeat. Many of the participants have lost close rela-tives, such as an aunt, grandmother or older sibling, but none of the girls will be tested for the breast cancer genes, BRCA1 or BRCA2.
“A lot of them had a mom who died of breast cancer and they’re coming in with their dad. That’s why there was a
lot of talk up front about how to frame this,” said Buys.
After Ella’s visit, she got to pick a plush toy to take home. The girls also get snacks and gift certificates. Adorn-ing the clinic’s walls are photos of puppies, kittens and teen heartthrobs like Justin Bieber.
“My daughter knows what cancer is, but I don’t think she associates the study with cancer. They don’t talk about cancer or dying. It’s more like, ‘What are you girls doing to keep your bodies healthy?’” said a 32-year-old study participant whose mother died six months ago from cancer.
She asked to be kept anonymous toprotect her 10-year-old daughter againstprejudice from employers and insurers.
“My mother didn’t find out she had the genetic mutation until after she was diagnosed with stage 4 ovarian cancer. She also had breast cancer at a young age, in her 30s,” said the Salt Lake County woman. “It’s definitely something I’m concerned about for me, my daughter and her children.
“I would rather not sit and wait and wonder, but be as proactive as I can. If finding better detection and prevention options means schlepping my daughter and her friends up to Huntsman, so be it,” she added.
By comparing girls from shared en-vironments researchers hope to better understand why some get cancer and others don’t.
They’d like to follow the girls for10 years or more, though the study iscurrently only funded for five — notlong enough to see if any of the girlsdevelop cancer.
“We can’t look at breast cancer outcomes,” said Esther John, another principal investigator who works at
How an 8-year-old could help cure breast cancer
SCIENTISTS HOPE BY STUDYING THE HABITS OF ADOLESCENT GIRLSTHEY CAN SHED LIGHT ON WHY WOMEN GET BREAST CANCER.
Cindy Solomon laughs as her 8-year-old daughter, Ella Solomon, eats a bag of sugar in order to produce saliva that will be tested during her visit to the Huntsman Cancer Institute office in Research Park in Salt Lake City, Utah. Steve Griffin, The Salt Lake Tribune
Continued on page X
10 The Reporter • Times Herald • Sunday, October 20, 2013 Sunday, October 20, 2013 • Times Herald • The Reporter 7
Continued on page 8
COURTESY KAISER PERMANENTEFor Sarah Velasquez it was a call
reminding her she was overdue for hermammogram. For Paula Wick it was aroutine mammogram that warranted acloser look. Both women never expect-ed what came next: breast cancer.
“I was so surprised,” Wick saidwhile addressing a roomful of KaiserPermanente staff and physicians inAugust as part of health care organiza-tion’s “I Saved A Life Program” —which recognizes staff who helpenhance patient care by schedulingmembers who are overdue for healthscreenings. The 64-year-old Napa resi-dent wasn’t expecting a cancer diagno-sis. “We don’t have any breast cancerin my family so it was a real surprise.You could have knocked me over witha feather.”
“You never think it will be you,”said Velasquez back in May. The 43-year-old Vacaville school teacher wasoverdue for her mammogram, and aKaiser Permanente employee calledand nudged her to make that appoint-ment. “They caught it early because ofthat call. Had it been seen six monthslater it could have been a very differ-ent story.”
Both Velasquez and Paula are nowbig believers of early detection and aregrateful for the care they received.
“I remember my radiologist tellingme that this is ‘fixable and curable,’”recalled Velasquez. “I really liked that.
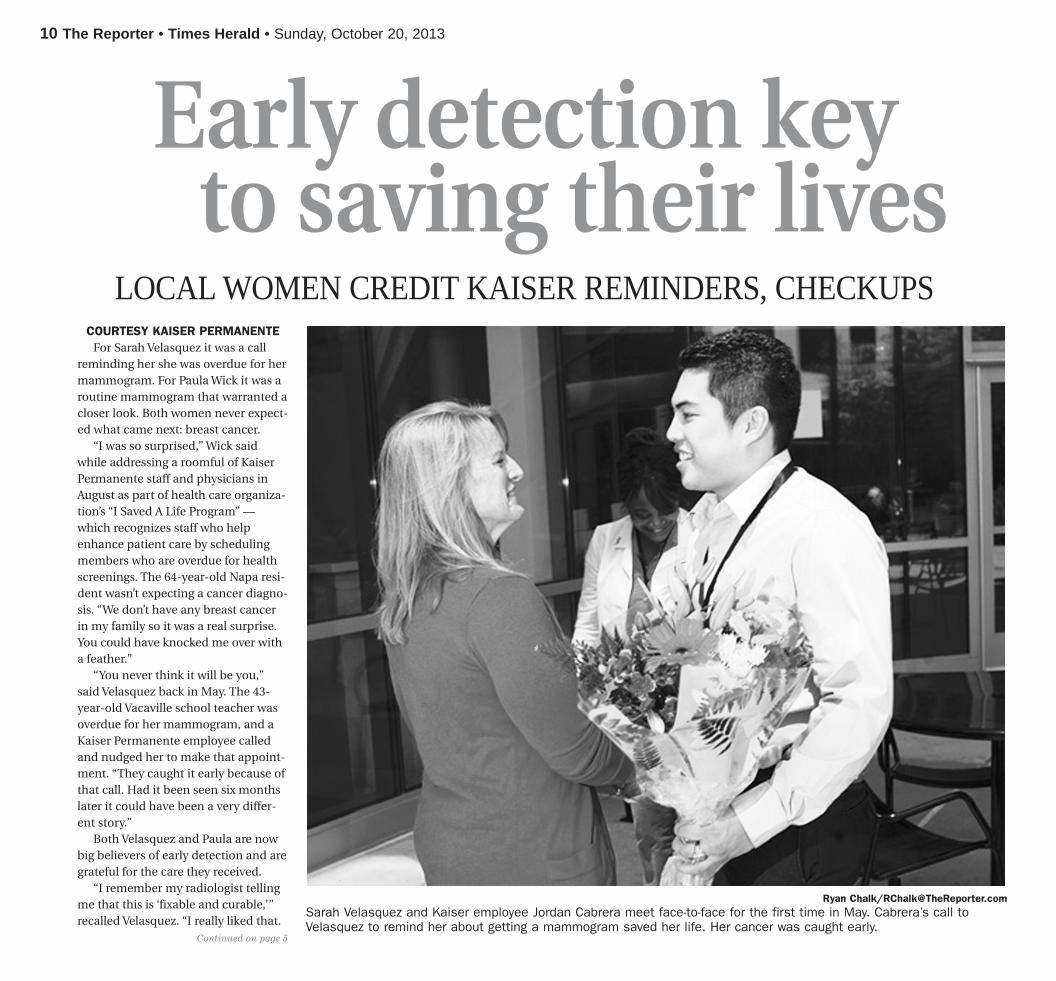
Early detection keyto saving their lives
LOCAL WOMEN CREDIT KAISER REMINDERS, CHECKUPS
Ryan Chalk/[email protected] Velasquez and Kaiser employee Jordan Cabrera meet face-to-face for the first time in May. Cabrera’s call toVelasquez to remind her about getting a mammogram saved her life. Her cancer was caught early.
Continued on page 5

the Cancer Prevention Institute of California. But the group can learn how lifestyle and environmental exposures trigger changes in the girls’ bodies that make them more prone to breast cancer, she said.
John is interested in examining how exercise and body size effect puberty. Girls in the U.S. are hitting puberty at younger ages, prolonging the exposure of their developing breasts to hor-mones that raise their cancer risk.
Researchers will also look at hormonessuch as insulin and melatonin, thought toreduce the risks of some cancers.
The team in Toronto will be using optical spectroscopy to shine a light into the girls’ breast tissue to measure fatty tissue and oxygenated blood, said Buys. It’s a way to divine breast density, another risk factor, without exposing the girls to radiation, she said.
“We could ask, are these girls the oneswho are most likely to be consuming alot of foods in plastic containers, or to beexposed to endocrine disruptors in theform of hair sprays?” she said.
Other teams will delve into behav-ioral factors, asking how families talk
and think about breast cancer. How do they cope with stress? Do they live in walkable communities with easy access to grocery stores and healthy food?
There’s no disputing that cancer has a strong genetic component. But a large majority of breast cancer cases happen in women with no family histo-ry of the disease.
Worldwide it is the most commonly diagnosed malignancy and the leading cause of cancer death among women. In 2012, an estimated 229,000 Amer-icans will be diagnosed with breast cancer and 40,000 will die from it, according to the Interagency Breast Cancer and Environmental Research Coordinating Committee (IBCERCC).
Yet only about 10 percent of govern-ment-funded research has focused on environmental causes, according to a 2013 report by IBCERCC, which calls for a different approach.
“How we do research matters,” said Jeanne Rizzo, IBCERCC co-chair-woman and president of the national advocacy group, the Breast Cancer Fund. “We need to study people in real-life scenarios, multiple exposures over time and not just ask, ‘Are we 95 percent sure that this one chemical caused this one disease in most people who were exposed to it?’”
The value of studies like Legacy, said Rizzo, is the broad sweep of data collected.
“When you go to the doctor, they mayask if you smoke or drink alcohol, butthey don’t ask anything about workplaceexposures or what chemicals you use,”she said. “So when we turn around andtry to understand how a person getssick, we don’t have the data.”
Cancer registries, traditionallydevoted to tracking diagnoses anddeaths, have begun collecting environ-mental data.
The shift stems from a long overdue recognition by scientists that “the absence of certainty does not give you permission to do nothing,” Rizzo said.
Long-term studies involving children, however, do pose ethical quandaries. Under routine research rules, Legacy researchers won’t be able to tell par-ents if they spot potential or existing health problems in the girls.
“I don’t expect to ever receive infor-mation about my daughter’s health or future risk of cancer from this study,” reasoned Cindy. “But I’m happy to help researchers identify things that may decrease breast cancer risk in general.”
Top: Eight-year-old Ella Solomon picks out a stuffed animal after Karen O’Toole, a regis-tered nurse and coordinator on the Legacy Girls Study, took a blood sample at the Hunts-man Cancer Institute office. The Huntsman Cancer Institute is part of the national study measuring and comparing girls from breast cancer families to girls from families with no breast cancer. Ella and her mother, Cindy Sol-omon, have committed to making such visits every six months for five years.Steve Griffin, The Salt Lake Tribune
Continued from page X
8 The Reporter • Times Herald • Sunday, October 20, 2013 Sunday, October 20, 2013 • Times Herald • The Reporter 9
Continued from page 7
the Cancer Prevention Institute of California. But the group can learn how lifestyle and environmental exposures trigger changes in the girls’ bodies that make them more prone to breast cancer, she said.
John is interested in examining how exercise and body size effect puberty. Girls in the U.S. are hitting puberty at younger ages, prolonging the exposure of their developing breasts to hor-mones that raise their cancer risk.
Researchers will also look at hormonessuch as insulin and melatonin, thought toreduce the risks of some cancers.
The team in Toronto will be using optical spectroscopy to shine a light into the girls’ breast tissue to measure fatty tissue and oxygenated blood, said Buys. It’s a way to divine breast density, another risk factor, without exposing the girls to radiation, she said.
“We could ask, are these girls the oneswho are most likely to be consuming alot of foods in plastic containers, or to beexposed to endocrine disruptors in theform of hair sprays?” she said.
Other teams will delve into behav-ioral factors, asking how families talk
and think about breast cancer. How do they cope with stress? Do they live in walkable communities with easy access to grocery stores and healthy food?
There’s no disputing that cancer has a strong genetic component. But a large majority of breast cancer cases happen in women with no family histo-ry of the disease.
Worldwide it is the most commonly diagnosed malignancy and the leading cause of cancer death among women. In 2012, an estimated 229,000 Amer-icans will be diagnosed with breast cancer and 40,000 will die from it, according to the Interagency Breast Cancer and Environmental Research Coordinating Committee (IBCERCC).
Yet only about 10 percent of govern-ment-funded research has focused on environmental causes, according to a 2013 report by IBCERCC, which calls for a different approach.
“How we do research matters,” said Jeanne Rizzo, IBCERCC co-chair-woman and president of the national advocacy group, the Breast Cancer Fund. “We need to study people in real-life scenarios, multiple exposures over time and not just ask, ‘Are we 95 percent sure that this one chemical caused this one disease in most people who were exposed to it?’”
The value of studies like Legacy, said Rizzo, is the broad sweep of data collected.
“When you go to the doctor, they mayask if you smoke or drink alcohol, butthey don’t ask anything about workplaceexposures or what chemicals you use,”she said. “So when we turn around andtry to understand how a person getssick, we don’t have the data.”
Cancer registries, traditionallydevoted to tracking diagnoses anddeaths, have begun collecting environ-mental data.
The shift stems from a long overdue recognition by scientists that “the absence of certainty does not give you permission to do nothing,” Rizzo said.
Long-term studies involving children, however, do pose ethical quandaries. Under routine research rules, Legacy researchers won’t be able to tell par-ents if they spot potential or existing health problems in the girls.
“I don’t expect to ever receive infor-mation about my daughter’s health or future risk of cancer from this study,” reasoned Cindy. “But I’m happy to help researchers identify things that may decrease breast cancer risk in general.”
Top: Eight-year-old Ella Solomon picks out a stuffed animal after Karen O’Toole, a regis-tered nurse and coordinator on the Legacy Girls Study, took a blood sample at the Hunts-man Cancer Institute office. The Huntsman Cancer Institute is part of the national study measuring and comparing girls from breast cancer families to girls from families with no breast cancer. Ella and her mother, Cindy Sol-omon, have committed to making such visits every six months for five years.Steve Griffin, The Salt Lake Tribune
Continued from page X
8 The Reporter • Times Herald • Sunday, October 20, 2013 Sunday, October 20, 2013 • Times Herald • The Reporter 9
Continued from page 7
BY KIRSTEN STEWARTSalt Lake Tribune
Cindy Solomon chuckles while she watches 8-year-old Ella pour a packet of sugar into her own mouth, stimu-lating her salivary glands to produce a “spit sample” for testing at Huntsman Cancer Institute.
For Ella, the sugar is a rare treat. For her health-conscious mom, it’s a nutritional sacrifice for science.
The Solomons are among 1,000 moth-er-and-daughter duos from the UnitedStates and Canada taking part in a long-term study of environmental, dietaryand family links to breast cancer.
Funded by the U.S. National Insti-tutes for Health, the “Legacy” study represents a shift in the focus of cancer research from diagnosis and treatment to prevention. And it’s one of the few involving girls so young, between ages 6 and 13.
Ella has no significant family history of cancer. Her mom heard about the study through a neighbor.
“We talked about how it would help scientists better understand cancer,” said Cindy, who told Ella that even though she’s not at risk, “You know people who have had the disease, and if you can help scientists and it’s fun, why not do it?”
Traditionally, researchers have focused on older women, asking them to recall details about their lives that may have predisposed them to breast cancer, said Saundra Buys, a principal investigator and co-director of the High Risk Breast Clinic at Huntsman.
“But more and more younger women are being diagnosed,” said Buys.
And increasingly risk factors are be-ing traced back to our early years, she
said. “As we follow these girls along, we’ll hopefully come up with some interesting hypotheses for things we can do in childhood or even in prenatal life to decrease the risk.”
Legacy — an acronym for Lessons in Epidemiology and Genetics of Adult Cancer from Youth — is being done at Breast Cancer Registry sites in San Francisco, New York, Philadelphia, Toronto and Salt Lake.
The Solomons are among 150 en-rolled through Huntsman.
Every six months for at least five years they will answer detailed ques-tionnaires about their exercise habits, the food they eat and the cosmetics,
hair gels and perfumes they use. Ella will be measured and weighed
and will volunteer saliva and urine for testing hormonal and genetic changes.
She also agreed to give blood — it’s optional — which didn’t seem to bother the wiggly, giggly girl at her last clinic appointment in August.
Clinic visits are kept upbeat. Many of the participants have lost close rela-tives, such as an aunt, grandmother or older sibling, but none of the girls will be tested for the breast cancer genes, BRCA1 or BRCA2.
“A lot of them had a mom who died of breast cancer and they’re coming in with their dad. That’s why there was a
lot of talk up front about how to frame this,” said Buys.
After Ella’s visit, she got to pick a plush toy to take home. The girls also get snacks and gift certificates. Adorn-ing the clinic’s walls are photos of puppies, kittens and teen heartthrobs like Justin Bieber.
“My daughter knows what cancer is, but I don’t think she associates the study with cancer. They don’t talk about cancer or dying. It’s more like, ‘What are you girls doing to keep your bodies healthy?’” said a 32-year-old study participant whose mother died six months ago from cancer.
She asked to be kept anonymous toprotect her 10-year-old daughter againstprejudice from employers and insurers.
“My mother didn’t find out she had the genetic mutation until after she was diagnosed with stage 4 ovarian cancer. She also had breast cancer at a young age, in her 30s,” said the Salt Lake County woman. “It’s definitely something I’m concerned about for me, my daughter and her children.
“I would rather not sit and wait and wonder, but be as proactive as I can. If finding better detection and prevention options means schlepping my daughter and her friends up to Huntsman, so be it,” she added.
By comparing girls from shared en-vironments researchers hope to better understand why some get cancer and others don’t.
They’d like to follow the girls for10 years or more, though the study iscurrently only funded for five — notlong enough to see if any of the girlsdevelop cancer.
“We can’t look at breast cancer outcomes,” said Esther John, another principal investigator who works at
How an 8-year-old could help cure breast cancer
SCIENTISTS HOPE BY STUDYING THE HABITS OF ADOLESCENT GIRLSTHEY CAN SHED LIGHT ON WHY WOMEN GET BREAST CANCER.
Cindy Solomon laughs as her 8-year-old daughter, Ella Solomon, eats a bag of sugar in order to produce saliva that will be tested during her visit to the Huntsman Cancer Institute office in Research Park in Salt Lake City, Utah. Steve Griffin, The Salt Lake Tribune
Continued on page X
10 The Reporter • Times Herald • Sunday, October 20, 2013 Sunday, October 20, 2013 • Times Herald • The Reporter 7
Continued on page 8
COURTESY KAISER PERMANENTEFor Sarah Velasquez it was a call
reminding her she was overdue for hermammogram. For Paula Wick it was aroutine mammogram that warranted acloser look. Both women never expect-ed what came next: breast cancer.
“I was so surprised,” Wick saidwhile addressing a roomful of KaiserPermanente staff and physicians inAugust as part of health care organiza-tion’s “I Saved A Life Program” —which recognizes staff who helpenhance patient care by schedulingmembers who are overdue for healthscreenings. The 64-year-old Napa resi-dent wasn’t expecting a cancer diagno-sis. “We don’t have any breast cancerin my family so it was a real surprise.You could have knocked me over witha feather.”
“You never think it will be you,”said Velasquez back in May. The 43-year-old Vacaville school teacher wasoverdue for her mammogram, and aKaiser Permanente employee calledand nudged her to make that appoint-ment. “They caught it early because ofthat call. Had it been seen six monthslater it could have been a very differ-ent story.”
Both Velasquez and Paula are nowbig believers of early detection and aregrateful for the care they received.
“I remember my radiologist tellingme that this is ‘fixable and curable,’”recalled Velasquez. “I really liked that.
Early detection keyto saving their lives
LOCAL WOMEN CREDIT KAISER REMINDERS, CHECKUPS
Ryan Chalk/[email protected] Velasquez and Kaiser employee Jordan Cabrera meet face-to-face for the first time in May. Cabrera’s call toVelasquez to remind her about getting a mammogram saved her life. Her cancer was caught early.
Continued on page 5

6 The Reporter • Times Herald • Sunday, October 20, 2013 Sunday, October 20, 2013 • Times Herald • The Reporter 11
He didn’t say ‘treatable’ but‘curable’ and that was animportant distinction forme.”
“Understanding one’srisk for developing breastcancer is very important,”said Dr. Marzban Rad, sub-chief for Breast Imaging forKaiser Permanente in theNapa Solano area. “It isimportant for women tounderstand that ‘risk’ is thechance that something willhappen, not that it defi-nitely will happen.”
According to Rad theprimary risk factors fordeveloping breast cancerare being a woman andgetting older. Other impor-tant risk factors includehaving a first degree rela-tive (a mother, daughter orsister) with breast cancer,and pregnancy (having kidsversus not). Maintaining ahealthy weight, having anactive lifestyle and decreas-ing alcohol consumptionare all important in reduc-ing risk as well.
“Kaiser Permanente iscommitted to offeringcomprehensive breast care.That is why we offer same-day mammogram service,’”added Dr. Rad. “If a patientis called back from herscreening mammogramand needs further review,
she can have everything,like a second mammogramand biopsy, done with justone trip, which helps alle-viate anxiety for thepatient.”
In the Napa Solano area,Kaiser Permanente diag-noses eight cases of breastcancers for every 1,000mammograms they per-form.
“We take a multi-disci-plinary team approach tobreast cancer treatment,”explained Rad. “EveryTuesday we have a medicalconference at our VallejoMedical Center with breastimaging radiologists, breastsurgeons, oncologists, radi-ation oncologists, patholo-gy and nursing to discusseach individual case to cre-ate the most effective treat-ment plan for ourpatients.”
“My experience at KaiserPermanente made a hugedifference in my care,” saidWick. “Some of my friendsdon’t have Kaiser and aren’tconnected like I am. I reallylove being connected andgetting emails from mydoctor — even on week-ends. They really lookedout for me and you couldtell the care here is allabout the person.”
Continued from page 4
Ryan Chalk/[email protected] Velasquez smiles gratefully at Jordan Cabrera, the Kaiser employee who she credits with savingher life. He called to remind her she was past due for a mammogram. When she got the proceduredone, Velasquez learned she had breast cancer but it was caught early enough to be successfullytreated.Velasquez and Cabrera met face-to-face for the first time in May — just in time for Mother’sDay.
They caught it early because ofthat call. Had it been seen six monthslater it could have been a very differentstory.”
Breast cancer survivor Sarah Velasquez
“
had familial inheritance patterns. But we haven’t.”
Meantime, medicine is becomingmore and more personalized. The ideaof treatment plans tailored to a person’sunique genes is gaining popularity, es-pecially after a Supreme Court decisionearlier this year said naturally occurringgenes are no longer patentable. Thedecision paves the way for cheapergene testing by more companies, whichmakes it more important than everfor people to seek reliable informationbefore considering a gene test.
“In terms of what’s changing over time is, first, just the uptake of testing, but also the types of tests we can do now,” said Rebecca Nagy, president of the National Society of Genetic Counselors. “When I first started, and even just 5 years ago, we really focused on one or two genes at a time. Now we can test for 20 or 30 genes at a time for the same cost as two or three genes. Technology has changed the game.”
While testing tools evolve at a break-neck pace, many women are actively working to increase awareness about testing. Doctors and cancer survivors strongly urge people considering a gene test to seek genetic counseling first. Counselors help a person de-termine whether a test is advisable, which test to take and what decisions she might have to make depending
on results. While BRCA1 and BRCA2 mutations are relatively rare, those who are at risk might not necessarily realize it.
“I got my gene through my father’s father’s father. I found out in January of 2006 that the mutation was present in my family and in February of 2006 I had the first symptom (of ovarian cancer) so there wasn’t time for me to really do anything with that infor-mation,” said Carey Fitzmaurice, a 45-year-old senior policy analyst at the Environmental Protection Agency in Washington, D.C., who has a BRCA gene mutation and battled both breast cancer and ovarian cancer. “That’s one of the reasons why I am determined to make people aware of this.
Raising that awareness is one of the main goals that Parker has for “Decod-ing Annie Parker.” The film’s unique distribution model means it’s getting screened with partner charities around the country. Half of the revenue from each event goes back to the charities, already nearly half a million dollars, according to the film’s director Steve Bernstein.
While “Decoding Annie Parker” tells the story of Parker and the race to identify the BRCA gene, the film is ul-timately about something much bigger, even though much of it is funny.
“The first three-quarters of the film
are essentially a comedy,” Bernsteinsaid. “It’s about people overcoming ob-stacles, the indomitable human spirit. Alot of times the audience is laughing, andat the end of the film it’s life affirming.Are there a few tears along the way? Ab-solutely. We’ve shown the film 20 times,and we’ve had 18 standing ovations.”
Above all, Bernstein says he set out to explore what happens to people when day-to-day comforts are stripped away in the face of real adversity. Of-ten, he says, human beings are capable of more strength and empathy than anyone might believe possible.
“We get to the real essence of self,” Bernstein said. “Annie’s a very charm-ing person who had to face cancer not once but has been diagnosed with can-cer three separate times. This woman, who has repeatedly faced death, is someone who refuses to find
death depressing. The Annie Parkers of the world believe that if they will themselves to live, they can live.”
Parker, now 62, still embodies that spirit. She recalls getting the news that she had ovarian cancer, eight years after her breast cancer diagnosis. Doc-tors were pessimistic.
“I was well into the third stage and almost the fourth stage, so I was told to go home and get my things in order,” Parker recalls. “Well, if somebody tells me that, I’m up for the challenge.”
Today, Parker’s health is good. And as she travels the country to screen the film, she takes the memories of her mother and sister with her.
“I have them on my shoulder at every screening, my mom sitting on one and my sister on the other,” Parker said. “This is my family story, but it’s many families’ story.”
“Decoding’s” Samantha Morton, left, stars as Annie Parker, who, with geneticist Mary-Claire King (Played by Helen Hunt, right), uncovered a hereditary cause for some breast cancers and spearheaded research that led to the identification of the BRCA gene mutation. Jeff Berline, Berline Creative
“Annie’s a very charming person who had to facecancer not once but has been diagnosed with
cancer three separate times. This woman, who hasrepeatedly faced death, is someone who refuses tofind death depressing. The Annie Parkers of theworld believe that if they will themselves to live,they can live.” Director Steve Bernstein.
Continued from page X
12 The Reporter • Times Herald • Sunday, October 20, 2013 Sunday, October 20, 2013 • Times Herald • The Reporter 5
Continued from page 4
heavy emotional and health burden if you carry this mutation, but in my mind, I was also given the gift of knowl-edge. That knowledge has enabled me to be more proactive with my health.”
Schlager, who lives near Washington, D.C., decided to get tested after an aunt found out she was BRCA positive and approached Schlager about consid-ering a gene test. Though Schlager had some breast cancer in her family history, she never thought it enough to be a troubling pattern.
“Not knowing much about BRCA mutations at all, I agreed to get tested,” she said. “I, too, came back positive for the BRCA1 mutation.”
Schlager decided to do surveillance for eight years before moving forward with surgeries to remove her ovaries, fallopian tubes and breasts. At the time of her diagnosis, the field of heredi-tary cancer research was still brand new. Schlager didn’t know anyone confronting the same health decisions she faced. FORCE, a national non-profit devoted to fighting hereditary breast cancer and ovarian cancer, had just been founded. Today, Schlager is FORCE’s spokeswoman. She is passionate about sharing her story and connecting women with resources and with one another.
“Every woman finds her path,” Schlager said. “Ultimately, although I thought I would never do it, I did go forward with surgery. I don’t regret it, and I don’t wish I had done it earlier. I think it was the perfect path for me.”
The right path may be different --even for women in the same family. JudyPollak, 64, was diagnosed with breastcancer when she was 25, around thetime of Annie Parker’s diagnosis andlong before the genetic links in breastcancer were understood. The Maryland
optical storeowner survived her cancerand went on to have two daughters, bothof whom also carry the mutation.
Pollak’s daughters, now 29 and 27, opted for different preventative measures after their BRCA tests. One chose a prophylactic mastectomy and the other chose surveillance.
“It’s very hard for me because I wor-ry,” Pollak said. “But mothers worry no matter what. Life is not ending, it’s just a different route that you’re taking. You look at yourself and say, ‘I’ll beat this.’ And you meet these women, we are phenomenal women that are survivors, that could accomplish anything.”
Pollak didn’t find out about her faulty BRCA gene until years after her diagnosis when, in the early 1980s, she participated in a study that sought women who had been diagnosed with breast cancer at a young age.
“I had never heard the word BRCA,”Pollak said. “I always thought my breastcancer came from my mother, who atage 70 had a mastectomy, but now Iknow it was totally unrelated. My BRCAis from my father, not from my mother.”
Even today, science is at the “tip of the iceberg” in understanding BRCA mutations and the link to cancer, according to Deborah Armstrong, a professor of oncology, gynecology and obstetrics at Maryland’s Johns Hopkins Kimmel Cancer Center and director of the hospital’s breast and ovarian genet-ic counseling and screening service.
“One of the biggest issues that has remained is that BRCA1 and BRCA2 only explain about half of familial breast cancers,” Armstrong said. “As the 1990s went on, (after the initial discovery of those gene mutations), we expected that we would have a BRCA3 and BRCA4 that would explain a pretty big chunk of these women at risk who
What is BRCA gene testing?
Everyone has BRCA genes that produce
tumor-suppressing proteins. But risky BRCA1
and BRCA2 gene mutations leave a person
more susceptible to cancers, including breast
and ovarian cancers. BRCA testing is used
to determine whether a person has such a
mutation, which can be inherited from either
parent. Each child of a parent who has a mu-
tation in one of these genes has a 50 percent
chance of inheriting the mutation.
What does the test entail?
BRCA gene mutations are detectable
through DNA from a blood or saliva sample.
It usually takes about a month to get results
once your sample is sent to a lab for analysis.
What does a positive result mean?
A woman’s lifetime risk of developing can-
cer is “greatly increased,” if she has a harmful
BRCA mutation, according to the National
Institutes of Health. About 12 percent of
women will develop breast cancer at some
point compared with up to 65 percent of
women who inherit a harmful BRCA1 muta-
tion. Other cancers are linked to mutations in
BRCA1 and BRCA2, including fallopian tube,
abdominal and pancreatic cancers. Men with
harmful BRCA gene mutations face higher
risk of prostate cancer.
How common are high-risk BRCA
gene mutations?
The likelihood of carrying a BRCA gene
mutation is extremely low for people with no
family history of breast or ovarian cancer. Only
about 10 percent of all breast cancers and 15
percent of all ovarian cancers can be traced
back to inherited genetic mutations.
Who should take the test?
Because BRCA gene mutations are
relatively rare, many doctors agree only those
who have specific family patterns of cancer
should consider the test. Such patterns
include having multiple family members who
have been diagnosed with breast or ovarian
cancer, especially at a young age; cases of
male breast cancer; and two or more cancers
in one family member.
For anyone thinking about such testing,
experts strongly recommend genetic counsel-
ing by someone who is experienced in cancer
genetics. Counseling can help assess the need
for testing in the first place, as well as facilitate
discussion about what kinds of decisions a
person faces once she gets her results.
What kinds of decisions should you
be prepared to make?
A person who finds out she has a BRCA
gene mutation faces some difficult decisions.
Some women choose enhanced cancer
screening, beginning with regular mam-
mograms in their 20s, for example. Others
choose risk-reducing surgeries like mas-
tectomies or the removal of the ovaries and
fallopian tubes. People also consider chemo-
prevention regimens of drugs and vitamins to
delay or reduce cancer risk. Finding out you
have a harmful BRCA mutation indicates a
higher risk for your siblings, too, so what you
learn can affect multiple family members.
How much does it cost?
Some insurance companies cover BRCA
testing, which can range in cost from hun-
dreds to thousands of dollars. The National
Cancer Institute urges people to contact their
insurance companies to discuss cost before
getting the test. For those without insurance,
some genetic testing companies offer free
or discounted pricing for individuals who
meet certain medical or financial eligibility
standards.
Who can help?
There are myriad resources for people
considering BRCA gene testing, including the
Cancer Information Service at the National
Institutes of Health (NIH) and many nonprofit
organizations. Live and anonymous online
chatting is available from the NIH weekdays
from 8 a.m. to 11 p.m. ET (5 a.m. to 8 p.m. PT
at http://livehelp.cancer.gov. You can also call
1-800-4-CANCER.— Adrienne LaFrance
A guide to BRCA gene testing
“It’s very hard for me because I worry (about herdaughters). But mothers worry no matter what.
Life is not ending, it’s just a different route that you’retaking. You look at yourself and say, ‘I’ll beat this.’ Andyou meet these women, we are phenomenal womenthat are survivors, that could accomplish anything.”Judy Pollak, 64, diagnosed with breast cancer when she was 25, around the time of Annie Parker’s diagnosis. She survived her cancer and went on to have two daughters, both of whom also carry the mutation.
Continued from page X
Continued on page X
4 The Reporter • Times Herald • Sunday, October 20, 2013 Sunday, October 20, 2013 • Times Herald • The Reporter 13
Continued from page 2
Continued on page 5
Sutter Fairfield Imaging willhost a free mammography day forpre-registered, uninsured womenage 40 and older on Oct. 26.
Space is limited, that’s whywomen are asked to call inadvance for the free digital screen-ing mammogram.
Women will receive theirresults from Sutter FairfieldImaging within several days aftertheir visit. Sutter Fairfield Imagingwill connect women who have anabnormal result to local not-for-profit agencies with which Sutterregularly partners so patients maytake next steps and receive follow-up care.
The free mammograms will beconducted from 8 a.m. to 3:30p.m. Oct. 26 at Sutter FairfieldImaging, 2700 Low Court inFairfield. Call 432-2500 to register.
Sutter’s Free MammographyDays was spearheaded at SutterAuburn Faith Hospital in 2009,where in two years’ time about 70uninsured women were given freemammograms. Inspired by thefeedback and success of the pro-gram, Sutter Diagnostic Imagingexpanded it to its other locationsin Davis, Elk Grove, Roseville andSacramento in 2011, and inFairfield, Jackson and Vallejo in2012. Sutter was able to give 358uninsured women free digitalscreening mammograms last year.
For more information aboutSutter Diagnostic Imaging centers,call 1-877-515-0053 or visitwww.checksutterfirst.org/imaging.
Sutteroffers free
exams
BY KATIE RASILA, M.D.Sutter Medical Group
Statistics regarding breast cancerfrom the American CancerSociety paint a positive picture:
incidence was stable from 2005-2009and deaths have been steadily decreas-ing since 1989. Still, the ACS estimatesthat more than 232,000 new cases ofbreast cancer will be diagnosed thisyear, and nearly 40,000 women will diefrom it-making it the second deadliestcancer for women (after lung cancer).
No one is immune from breast can-cer. Many of the risk factors —beingfemale, advancing age, family history,early menarche and late menopause-can’t be changed. Risk factors that canbe changed include obesity, use of hor-mone replacement therapy, physicalinactivity and alcohol consumption.
As is true for all cancers, earlydetection is key to successful treat-ment. The ACS recommends annualmammograms beginning at age 40. Inaddition, MRI scans may be appropri-ate for some women who are at highrisk.
Solano County women diagnosedwith breast cancer are fortunate tohave state-of-the-art treatment avail-able at the Sutter Solano CancerCenter in Vallejo. Our multidisciplinaryteam includes professionals to treatand guide patients throughout theircancer odyssey: surgeons, medicaloncologists and radiation oncologists,social workers, psychologists, nutri-tionists and patient navigators. Inaddition, several support groups areavailable for patients and their families
— helping heal them as a whole.Being under one roof helps our
team’s ability to communicate and beon the same page, which leads to ahigher level of personalized care. Weunderstand how anxious patients areafter receiving a cancer diagnosis andtake the time to ensure they under-stand all their options and can makethoughtful decisions about the righttreatment plan for them.
The treatment of breast cancer isindividualized; a number of factors willdetermine the recommended course ofaction for each patient, including thesize, grade, node status and stage ofthe tumor and whether it’s hormonereceptor positive or negative.Treatment alternatives may includemastectomy, breast-conserving sur-gery (lumpectomy), radiation,chemotherapy, hormone-blockingtherapy and targeted/biologic therapy.As an American College of Surgeons-accredited cancer treatment facility,the Sutter Solano Cancer Center teamis well equipped to provide patientswith the tools, information and
resources they need to make decisionsregarding their treatment.
Dr. Rasila, a member of Sutter MedicalGroup and the Sutter Solano CancerCenter medical team, specializes in med-ical oncology and hematology. She seespatients in Fairfield and Vacaville andcan be reached at 427-4900.
Statistics don’t tellthe whole story
No one is immune from breast cancer.Many of the risk factors — being female,advancing age, family history, early menarcheand late menopause-can’t be changed. Riskfactors that can be changed include obesity,use of hormone replacement therapy, physicalinactivity and alcohol consumption.”
Katie Rasila, M.D., Sutter Medical Group.
EARLY DETECTION VITAL TOSUCCESSFUL TREATMENT
“
14 The Reporter • Times Herald • Sunday, October 20, 2013 Sunday, October 20, 2013 • Times Herald • The Reporter 3
BY RACHEL RASKIN-ZRIHENTimes-Herald staff writer
It was just before Thanksgiving threeyears ago that I had my last radiationtreatment, against doctor’s orders.
Sort of.I had undergone, I think, six chemo
treatments after my surgery to remove avery small, very earlycancerous tumor frommy left breast, and,what seemed like sev-eral thousand dailydoses of radiation.
I drove myself tothese treatments afterwork every day atNapa’s Queen of the
Valley Hospital, and then home, fightingthe infamous traffic on Highway 29through American Canyon at rush hour— a serious misnomer, since it lasts sig-nificantly longer than an hour.
Though everyone was lovely at theQueen, I only got through the wholething with my sanity by counting downthe days until it was over. I had figuredout — and bear in mind that figuring outanything was a real feat during this men-tal Swiss-cheese time of my life — that
the last treatment was going to be theday before Thanksgiving, and I wascounting on that. It seemed appropriate,somehow; like a message.
However, on the day that was sup-posed to be my last treatment, I wasinformed that their radiation machinehad malfunctioned in some way and Ineeded to come back one more time,after the holiday.
Not going to happen.“I planned on today being the last
one and that’s what it’s going to be,” Isaid. “Not that I don’t love you guys, but,
no offense, I never want to see any ofyou again in a professional capacity.”
And so far, I haven’t.Since my diagnosis in May, 2010, I’ve
spoken with a lot of people, some ofthem experts, and done a lot of readingon the issue, and have learned that acertain percentage of people with thesame thing I had elect different coursesof treatment. I went with the mostaggressive form because I was told itgave me the best chance to avoid arecurrence, and that’s what I want. Norepeat.
But I know people who have optedfor surgery alone, and some who havechosen chemo only or just radiation, orsome combination. I chose to go wholehog, so to speak.
So far, all but one of the way-too-many of my friends who have had thisdisease, are all still alive, thank God. But,we did lose one very important personto this crummy disease, and it wasbecause by the time she caught it, it hadalready spread. She lived a decade withit — long enough to see her daughtermarried and to meet her grandson — ahuge blessing.
Fahni was an inspiration to everyonewho knew her and a living testament tohow far medicine has come in the treat-ment of breast cancer.
But, hers is also a cautionary tale,with the moral of the story being, checkyourself. No one knows your body aswell as you do. And if you think you feelsomething, get it checked. Don’t wait. It’sprobably nothing, but, as the sayinggoes, better safe than sorry.
Contact staff writer Rachel Raskin-Zrihen at 553-6824 [email protected].
Vallejo writer recalls own battleLESSONS LEARNED, FRIENDS
LOST TO BREAST CANER
Raskin-Zrihen
I had figured out — and bear in mind that fig-uring out anything was a real feat during this men-tal Swiss-cheese time of my life — that the last treat-ment was going to be the day before Thanksgiving,and I was counting on that. It seemed appropriate,somehow; like a message.”
WASHINGTON (AP) — Abiotech drug that Roche makesat Vacaville’s Genentech facility,has become the first medicineapproved to treat breast cancerbefore surgery, offering an earli-er approach against one of thedeadliest forms of the disease.
Earlier this month, the Foodand Drug Administrationapproved Perjeta for womenwith a form of early-stage breastcancer who face a high risk ofhaving their cancer spread toother parts of the body.
Surgery to remove tumors isusually the first step in treating
most forms of cancer. Perjeta isthe first drug to be approved asa pre-surgical step. Doctorshope that using cancer drugsearlier could help shrink tumors,making them easier to remove.In some cases, that could allowwomen to keep their breasts,rather than having a full mastec-tomy. Doctors also say thattreating the disease at its earlieststages could prevent tumorsfrom returning later, thoughstudies have not yet establishedthat benefit.
“By making effective thera-pies available to high-risk
patients in the earliest diseasesetting, we may delay or preventcancer recurrences,” said FDA’sDr. Richard Pazdur, who directsthe agency’s office of cancerproducts.
Cancer specialists already useseveral chemotherapy drugs asinitial treatments for cancer, butthey are not formally approvedfor the use. The FDA originallyapproved Perjeta to treat breastcancer that has spread to otherparts of the body after surgery.
The FDA granted the drugaccelerated approval for its newuse based on a study showingwomen who received the drug
as an initial treatment weremore likely to be cancer-free 12weeks later than women whoreceived older drug combina-tions. Accelerated approval isreserved for drugs that showgroundbreaking results for treat-ing life-threatening diseases inearly studies.
As a condition of approval,Roche’s Genentech unit mustconduct a larger follow-up studyshowing the drug’s long-termbenefits for patients. Generallythat means showing thatpatients lived longer or had ahigher quality of life due to tak-ing the drug. Genentech, based
in South San Francisco, Calif.,has already enrolled about 4,800patients in the follow-up study,with results expected in 2016.
Dr. Paula Klein, a breast can-cer specialist, said she will startprescribing the drug for early-stage patients immediately, butstressed the importance of fol-low-up data on patient survival.
“This does not yet proveto us that using the antibody inthis setting will result in morecures. That is still a hypothesis,”said Klein, who directs thebreast cancer program atContinuum Cancer Centers ofNew York.
Pre-surgery breast cancer drug made in Vacaville
“
16 The Reporter • Times Herald • Sunday, October 20, 2013
DECODING BREAST CANCER
Whether it’s a perfectly healthy woman volunteering for a biopsy, an 8-year-old girl allowing her habits to be tracked
or Hollywood shining its bright lights on gene testing, the fight to crack the deadly code of breast cancer
is leaving no stone unturned.
Special SectionSunday, October 20, 2013
INSIDE
COURTESY NORTHBAYHEALTCARE
Thanks to an investmentin some high-tech software,Solano DiagnosticsImaging in Vacavilleis now the onlyentity in SolanoCounty that cur-rently offers 3-Dmammography, atool that is especial-ly helpful in diag-nosing or ruling outcancer in womenwith dense breasts.
In April, California passeda law requiring patients with“Heterogeneously DenseBreasts” or “ExtremelyDense Breasts” be notified oftheir density score and pos-sible risk for breast cancer. Itis estimated that nearly 50percent of all women whocurrently receive mammo-grams will soon learn theyhave dense breasts.
“If a woman knows shehas dense breasts, she canelect to come to SDI inVacaville for a 3-D mammo-gram instead of relying on astandard mammogram,”explains Adrian Riggs, direc-tor. “If she gets a standardmammogram, there’s a goodchance her doctor will referher to have images takenusing the 3-D technology.
She might as well go rightfor the best technology first.”
Rather than taking twoimages, as is done in stan-
dard mammography,breast tomosynthesistakes multiple low-dose images of thebreast and synthe-sizes them into athree-dimensionalimage. This allowsradiologists to exam-ine the breast in very
thin layers. The digital image allows
the radiologist to rotate thetissue in front of or behindan abnormality, makingdetection easier. In addition,overlapping tissue that mayappear abnormal on a stan-dard mammogram can bedetermined to be benign ina 3-D image.
Breasts are composed offatty tissue, milk lobules,milk ducts and connectivetissue. The greater theamount of milk ducts, milklobules and connective tis-sue, the denser the breast.
On a mammogram,denser breast tissue appearswhite, while fatty tissue isgray, explains Dr. JasonMarengo, an oncoplasticsurgeon with the NorthBayCenter for Specialty Care.“Typically when a cancer is
found on a mammogram, itis also white. With verydense breasts, it can be diffi-cult to clearly see cancer. It’slike trying to find a whitesnowflake against a whitebackground,”
For the patient, getting a3-D mammogram firsttranslates into fewer “callbacks” for additional mam-mographic views, fewerunnecessary biopsies, detec-tion of concerning massesthat may have beenobscured by surroundingbreast tissue and fewersleepless nights, says Dr.Marengo.
A patient doesn’t have tobe associated with NorthBayHealthcare patient to get a3D screening at SDI inVacaville, notes Riggs. “Justask your doctor for a refer-ral.”
Solano County facilityoffers mammography
CourtesyAdrian Riggs of Solano Diagnostic Imaging stands with the facility’snew 3-D mammography tool — the only one of its kind in SolanoCounty.
Marengo
33--DDinin
MACHINE CAN CATCH THINGSTRADITIONAL IMAGING MISSES
If a woman knows she has dense breasts, shecan elect to come to SDI in Vacaville for a 3-Dmammogram instead of relying on a standardmammogram.”
Adrian Riggs, director Solano Diagnostics Imaging, Vacaville
“THE SILVER SCREEN:“DECODING ANNIEPARKER”
A GUIDE TOBRCA GENETESTING
HOW AN 8-YEAR-OLDCOULD HELP CUREBREAST CANCER
KAISER: EARLYDETECTIONIS KEY
STATISTICSDON’T TELL THE WHOLE
SOLANO GROUPOFFERS 3-DIMAGING